
Contents
Slipping rib syndrome
Slipping rib syndrome also called 12th rib syndrome, clicking rib syndrome, slipping-rib-cartilage syndrome, interchondral subluxation, painful rib syndrome, displaced ribs, rib-tip syndrome, rib subluxation, chest pain-slipping rib or Cyriax syndrome, refers to pain in your lower chest or upper abdomen which may be present when your lower ribs move a little more than normal 1, 2, 3, 4, 5, 6, 7, 8, 9, 10. Your ribs are the bones in your chest that wrap around your upper body. Your ribs connect your breastbone (manubrium and sternum) to your spine (vertebrae). Slipping rib syndrome usually involves the 8th, 9th and 10th ribs (also known as “false ribs”) at the lower part of your rib cage. These ribs are not connected to the chest bone (sternum). Fibrous tissue (ligaments), connect these ribs to each other to help keep them stable. The relative weakness in the ligaments can allow the ribs to move a little more than normal and cause pain. Slipping rib syndrome was first described in 1919 by Cyriax as an anterior rib dislocation causing pain due to impingement of the intercostal nerves 11, 5. It was hypothesized that the terminal nerves, which run at the inferior border of each cartilage, were irritated due to the abnormally subluxing rib 12.
Slipping rib syndrome can occur at any age with cases have been reported in children as young as 12 years, but it is more common in middle-aged adults. Females may be more affected than males 8, 13, 14.
Slipping rib syndrome usually occurs on one side 15. Rarely, it may occur on both sides 16, 12. The pain of slipping rib syndrome usually goes away in few weeks.
Slipping rib syndrome symptoms include:
- Severe pain in the lower chest or upper abdomen. The pain may come and go and get better with time.
- A popping, clicking, or slipping sensation.
- Pain when applying pressure to the affected area.
- Coughing, laughing, lifting, twisting, and bending may make the pain worse.
Slipping rib syndrome symptoms are similar to other medical conditions. Slipping rib syndrome must be differentiated from conditions with similar clinical characteristics such as costochondritis, rib fractures, cholecystitis, esophagitis, gastric ulcer, hepatosplenic abnormalities, stress fracture, inflammation of the chondral cartilage, pleuritic chest pain, cancers, heart or gastrointestinal conditions 5, 17. This makes slipping rib syndrome difficult to diagnose. As it is a commonly missed diagnosis of upper abdominal pain, many cases have been reported of patients suffering from pain and discomfort for months to years without an established diagnosis 18. A quick way to rule out these other conditions is to look for an association between certain movements or postures and pain intensity, determine if the patient has experienced recent trauma (although not always present), and reproduce the symptoms (e.g, pain, clicking) with the hooking maneuver.
The hooking maneuver, a relatively simple clinical test, which involves the examiner placing his or her fingers under the lower costal margin and pulls the hand with an upward lift 19. Pain or “clicking” sensation indicates a positive test and confirms the diagnosis. It is recommended that the hooking maneuver be followed with a rib block to see if the pain can be relieved 20. Radiologic imaging is generally not useful in the diagnosis of slipping rib syndrome but may be of value in ruling out other conditions in the differential diagnosis 21.
Hooking maneuver test:
- You will be asked to lie on your back.
- Your doctor will hook their fingers under the lower ribs and pull them outward.
- Pain and a clicking sensation confirms slipped rib.
Simple reassurance (eg, “there is nothing seriously wrong with you”) and the avoidance of movements or postures that exacerbate symptoms may be sufficient in eliciting a successful outcome 8. Slipping rib syndrome treatment focuses on relieving your pain 12. Rest from the inciting activity, along with ice, non-steroidal anti-inflammatory drugs (e.g., ibuprofen (Advil, Motrin) or naproxen (Aleve, Naprosyn) for pain relief), and topical analgesics may be enough to alleviate the symptoms completely 5. For mild pain, you can use ibuprofen (Advil, Motrin) or naproxen (Aleve, Naprosyn). You can buy these pain medicines at the store. Talk with your doctor before using these medicines if you have heart disease, high blood pressure, kidney disease, liver disease, or have had stomach ulcers or internal bleeding in the past. Take the dose as advised by your doctor. Do not take more than the amount recommended on the bottle or advised by your doctor. Carefully read the warnings on the label before taking any medicine. Your doctor may also prescribe pain medicines to relieve pain. For severe pain, your doctor may give you a single intercostal nerve block and corticosteroid injection at the site of your pain.
You may be asked to:
- Apply heat or ice at the site of pain. Wrap the ice in a cloth. Do not put ice directly on the skin.
- Avoid activities that makes the pain worse, such as heavy lifting, twisting, pushing, and pulling.
- Wear a chest binder to stabilize the ribs.
- Consult a physical therapist.
If your pain persists, surgery may be done to remove the cartilage and lower ribs, although it is not a commonly performed procedure 18.
Figure 1. Ribs anatomy

Figure 2. Slipping rib syndrome diagnostic and treatment algorithm
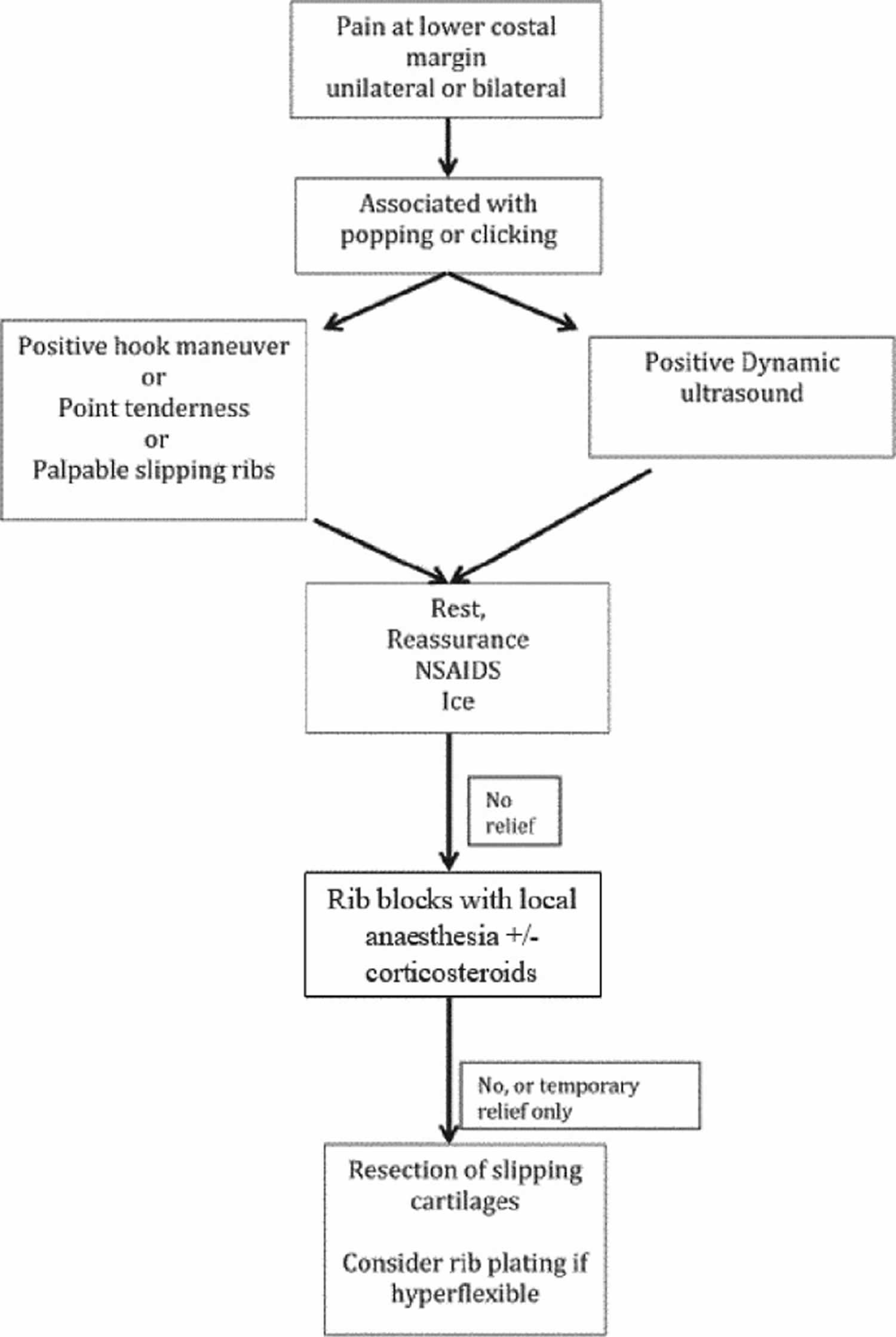
Footnotes: Algorithm for the evaluation, diagnosis and treatment of slipping rib syndrome.
Abbreviation: NSAID = non-steroidal anti-inflammatory drug.
[Source 6 ]You should contact your doctor right away if you have:
- An injury to your chest
- Pain in your lower chest or upper abdomen
- Difficulty breathing or shortness of breath
- Pain during daily activities
Call your local emergency services number if:
- You have sudden crushing, squeezing, tightening, or pressure in your chest.
- Pain spreads (radiates) to your jaw, left arm, or between your shoulder blades.
- You have nausea, dizziness, sweating, a racing heart, or shortness of breath.
Ribs anatomy
Your chest (thoracic wall) or rib cage encloses and protects your heart, lungs, and great vessels as well as some abdominal organs 22, 23. You have 12 sets of rib pairs and their corresponding attachments to the sternum (breastbone) and the vertebral column make up your chest or rib cage. Ribs number 1 to 9 curve around the lateral thoracic wall and attach to the manubrium and sternum via the hyaline or costal cartilage 24. Ribs number 10 to 12 are relatively short, due to their short course, do not reach the sternum and are known as floating ribs 22. Posteriorly, ribs attach to costovertebral articulations of the spine 25, 23. Ribs number 2 through 9 all have 2 facets on their heads; the superior facet articulates with the vertebra above the rib, while the inferior facet articulates with the respectively named vertebra 23. In addition, ribs 1 through 10 have tubercles with facets that articulate with the costal facet of the transverse process of each respective vertebra 26. Ribs 11 and 12 have no tubercle and therefore do not articulate with the transverse process of their respective vertebra.
Anteriorly ribs articulate with the hyaline, or costal, the cartilage of the adjacent rib. Ribs number 1 to 7 are true ribs and connect anteriorly by pliable cartilages called costal cartilages to the sternum, including the sternal notch, manubrium, and sternal body. Ribs 8, 9, and 10 attach anteriorly to the hyaline cartilage of the rib above them and are known as false ribs 23. False ribs do not have a bone-to-bone anterior articulation. Ribs 11 and 12 are floating ribs, denoting there is no anterior articular attachment to hyaline cartilage or the sternum, the floating ribs, have their cartilages ending in the muscle in the abdominal wall 23. Ribs 11 and 12 are otherwise known as caliper ribs because of their lack of anterior attachment.
Muscular attachments to the ribs include the scalenes, internal intercostals, external intercostals, and the diaphragm 27. During inhalation and exhalation, the ribs move up and down as levers when pulled by their muscular attachments to expand the thoracic cavity, creating a negative pressure space, activating airflow into the lungs 28. During the inhalation and exhalation, ribs 1 to 4 move in pump handle motion, meaning they are moving up (nuchal) or cephalad and down (caudal) or caudad. Ribs 1 to 4 on their anterior articulations move up and down. Ribs 5 to 10 are called bucket handle ribs because the shaft of the rib body on the lateral aspect of the chest wall moves up and down.
Each rib has muscular attachments to facilitate inhalation and exhalation 28. The first rib has muscular attachments at is base of the anterior and middle scalene, which elevate the first rib during inspiration 28. The anterior scalene muscle originates from the C3-C6 transverse processes and attaches to the first rib 28. The posterior and middle scalene originate from the posterior tubercles of C2-C6 and attach posteriorly to the subclavian groove on the first rib. The posterior scalene attaches to C2, elevating it during inspiration. Together with the first rib, they create the inter-scalene triangle. The scalenes side bend and flex the neck to their side of attachment. Intercostal muscles include the external, internal, innermost, and subcostal muscles.
The diaphragm moves in inspiration and expiration by expanding and re-doming as the diaphragm contracts and relaxes 29. It is composed of two muscles, costal and crural, with innervation from the phrenic nerve C3-C5 29. When the costal muscle of the diaphragm contracts, it expands the thoracic cage in the coronal plane with the pump handle ribs and sagittal plane with inhalation of bucket handle ribs 29, 30. During inhalation, the diaphragm relaxed the dome shape of the muscle flattens, allowing for decreased intra-thoracic pressure and air to fill the lungs 31. The diaphragm is key in returning lymph and venous blood to the heart 29. This action moves lymph through the body from the subcutaneous tissues bringing it back into the intravascular system.
Slipping rib syndrome causes
Slipping rib syndrome is caused by hypermobility of the anterior 8th, 9th and 10th ribs (false ribs) due to the disruption of the interchondral fibrous attachments. This disruption permits the costal cartilage tips to shift and impinge on the intercostal nerves and the surrounding muscles and tissues, passing along the undersurface of the adjacent rib, resulting in severe pain and inflammation in the area 32. This impingement causes severe pain and a slipping sensation and is provoked by respiratory movements, bending and external influences e.g. palpation by the examiner or hooking maneuver 16.
Rib hypermobility caused by weakness of the rib-sternum (sternocostal), rib-cartilage (costochondral), and/or rib-vertebral (costovertebral/costotransverse) ligaments, allowing rib hypermobility, is thought to be the primary cause of slipping rib syndrome 20. Ribs 8, 9 and 10 (false ribs), which are not connected to the sternum but are connected to each other via a cartilaginous cap or fibrous band, tend to be the most mobile and susceptible to trauma. Because of this, slipping rib syndrome is usually caused by hypermobility of 8th, 9th or 10th rib. Anterior rib hypermobility is also likely to cause problems in the posterior thoracic area as well because in a closed system (in this case, the rib cage) it is difficult for motion to occur at 1 site (the anterior portion of the rib) without causing motion to occur elsewhere (the posterior portion of the rib) 20.
Slipping rib syndrome can occur as a result of 33, 20, 10:
- Injury to your chest while playing contact sports such as football, ice hockey, wrestling, and rugby.
- A fall or direct trauma to your chest.
- Rapid twisting, pushing, or lifting motions, such as throwing a baseball or swimming.
More often, a direct traumatic incident is not remembered by the patient, but an insidious insult may have occurred that was overlooked. Sudden extension or flexion, repeated one-sided weight bearing or exercise such as throwing a ball, vigorous swimming, or swinging a bat may be implicated.
Slipping rib syndrome symptoms
Slipping rib syndrome usually occurs on one side. Rarely, it may occur on both sides. Slipping rib syndrome symptoms include:
- Severe pain in the lower chest or upper abdomen. The pain may come and go and get better with time.
- A popping, clicking, or slipping sensation.
- Pain when applying pressure to the affected area.
- Coughing, laughing, lifting, twisting, and bending may make the pain worse.
Slipping rib syndrome complications
Slipping rib syndrome complications may include:
- Difficulty breathing.
- Pneumothorax (a collapsed lung that occurs when air leaks into the space between the lungs and chest wall) from an injury during an injection.
There are usually no long-term complications.
Slipping rib syndrome diagnosis
Your doctor will take your medical history and ask about your symptoms. You will be asked questions such as:
- How did the pain start?
- Was there an injury?
- What makes your pain worse?
- Does anything help relieve the pain?
Your doctor will perform a physical exam. The hooking maneuver test may be done to confirm the diagnosis. In the hooking maneuver test:
- You will be asked to lie on your back.
- Your doctor will hook their fingers under the lower ribs and pull them outward.
- Pain and a clicking sensation confirms slipped rib.
It is recommended that the hooking maneuver be followed with a rib block to see if the pain can be relieved 20. If a hooking maneuver is followed by an intercostal nerve block which releases the pain, the diagnosis slipping rib syndrome is highly plausible 34. If intercostal nerve block does not relieve symptoms, it is necessary to consider a missed fracture, a muscle tear, or another source of pain.
On the basis of your exam, an X-ray, ultrasound, MRI, bone scan or blood tests may be done to check for other conditions 21. For example, a bone scan can be useful to diagnose costochondritis 18, 20.
Slipping rib syndrome treatment
Simple reassurance (e.g, “there is nothing seriously wrong with you”) and the avoidance of movements or postures that worsen the symptoms may be sufficient in eliciting a successful outcome 8. Rest from the inciting activity, along with ice, non-steroidal anti-inflammatory drugs (e.g., ibuprofen (Advil, Motrin) or naproxen (Aleve, Naprosyn) for pain relief), and topical analgesics may be enough to alleviate the symptoms completely 5. Other conservative treatments include heat, physical therapy, massage, topical NSAIDs, chiropractic manipulation and electronic stimulation, all of which focus on symptom control 34. However, in patients with moderate to severe pain and dysfunction, an intercostal nerve block with local anesthetic with or without corticosteroid for relief of symptoms 35. If the pain returns after the nerve block, the next step is to consider surgical resection as the pain is likely to continue to recur 36. Lastly, those with severe pain or refractory cases to conservative management can undergo surgical intervention with resection of the slipping rib and the connected costal cartilage may be necessary 5, 37, 18. Most recently in 2019, McMahon implemented a novel technique in patients for whom rib excision was not curative 38. In 3 separate cases, bioabsorbable rib plating techniques traditionally used for fracture repair were utilized to vertically plate ribs 8 to 10 and mechanically separate the hypermobile ribs 38. Symptom reduction was achieved in all three patients, but given the singularity of this case report, further research into this technique is required 38.
The outcomes of both conservative and surgical management have been shown to be favourable 39.
Slipping rib syndrome prognosis
Slipping rib syndrome is a benign condition. Slipping rib syndrome pain often goes away completely over time, although the pain may become chronic. In the almost 400 cases reported in the literature since 1919, the majority of patients are reported to have pain relief after treatment 16, 18. Scott described 76 patients with painful rib syndrome. This was defined as pain in the lower chest or upper abdomen, a tender spot on the lower costal margin and reproduction of the pain with palpation 5. Their treatment protocol was reassurance and acetaminophen (paracetamol). Five patients went to a pain clinic for treatment without relief. Injections or surgery may be required in some cases 40.
- Madeka I, Alaparthi S, Moreta M, Peterson S, Mojica JJ, Roedl J, Okusanya O. A Review of Slipping Rib Syndrome: Diagnostic and Treatment Updates to a Rare and Challenging Problem. J Clin Med. 2023 Dec 14;12(24):7671. doi: 10.3390/jcm12247671[↩]
- Gress K, Charipova K, Kassem H, Berger AA, Cornett EM, Hasoon J, Schwartz R, Kaye AD, Viswanath O, Urits I. A Comprehensive Review of Slipping Rib Syndrome: Treatment and Management. Psychopharmacol Bull. 2020 Oct 15;50(4 Suppl 1):189-196. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7901126[↩]
- Mazzella A, Fournel L, Bobbio A, Janet-Vendroux A, Lococo F, Hamelin EC, Icard P, Alifano M. Costal cartilage resection for the treatment of slipping rib syndrome (Cyriax syndrome) in adults. J Thorac Dis. 2020 Jan;12(1):10-16. doi: 10.21037/jtd.2019.07.83[↩]
- Álvarez-Muñoz V, Prado Á, Vega N, Crehuet D, Sánchez L, Vega L. Slipping rib syndrome in childhood. A case series. Arch Argent Pediatr. 2024 Aug 1;122(4):e202310141. English, Spanish. https://www.sap.org.ar/docs/publicaciones/archivosarg/2024/v122n4a12e.pdf[↩]
- McMahon LE. Slipping Rib Syndrome: A review of evaluation, diagnosis and treatment. Semin Pediatr Surg. 2018 Jun;27(3):183-188. doi: 10.1053/j.sempedsurg.2018.05.009[↩][↩][↩][↩][↩][↩][↩]
- Chhipa I, Cheesman Q. Slipping rib syndrome in an adolescent wrestler. BMJ Case Rep. 2020 Jan 12;13(1):e232514. doi: 10.1136/bcr-2019-232514[↩][↩]
- Porter GE. Slipping rib syndrome: an infrequently recognized entity in children: a report of three cases and review of the literature. Pediatrics. 1985 Nov;76(5):810-3.[↩]
- Wright JT. Slipping-rib syndrome. Lancet. 1980 Sep 20;2(8195 pt 1):632-4. doi: 10.1016/s0140-6736(80)90294-9[↩][↩][↩][↩]
- Davies-Colley R. SLIPPING RIB. Br Med J. 1922 Mar 18;1(3194):432. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2415737/pdf/brmedj06708-0014.pdf[↩]
- Udermann BE, Cavanaugh DG, Gibson MH, Doberstein ST, Mayer JM, Murray SR. Slipping Rib Syndrome in a Collegiate Swimmer: A Case Report. J Athl Train. 2005 Jun;40(2):120-122. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1150226[↩][↩]
- Cyriax EF. On various conditions that may stimulate the referred pain of visceral diseases and a consideration of these from the point of view of cause and effect. Practitioner. 1919;102:314–322.[↩]
- Mooney DP, Shorter NA. Slipping rib syndrome in childhood. J Pediatr Surg. 1997 Jul;32(7):1081-2. doi: 10.1016/s0022-3468(97)90403-6[↩][↩][↩]
- Parry W, Breckenridge I, Khalil YF. Bilateral clicking ribs. Thorax. 1989 Jan;44(1):72-3. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC461670/pdf/thorax00277-0086.pdf[↩]
- Scott EM, Scott BB. Painful rib syndrome–a review of 76 cases. Gut. 1993 Jul;34(7):1006-8. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1374244/pdf/gut00558-0160.pdf[↩]
- Gould JL, Rentea RM, Poola AS, Aguayo P, St Peter SD. The effectiveness of costal cartilage excision in children for slipping rib syndrome. J Pediatr Surg. 2016 Dec;51(12):2030-2032. doi: 10.1016/j.jpedsurg.2016.09.032[↩]
- Saltzman DA, Schmitz ML, Smith SD, Wagner CW, Jackson RJ, Harp S. The slipping rib syndrome in children. Paediatr Anaesth. 2001 Nov;11(6):740-3. doi: 10.1046/j.1460-9592.2001.00754.x[↩][↩][↩]
- Arroyo JF, Vine R, Reynaud C, Michel JP. Slipping rib syndrome: don’t be fooled. Geriatrics. 1995 Mar;50(3):46-9.[↩]
- Copeland GP, Machin DG, Shennan JM. Surgical treatment of the ‘slipping rib syndrome’. Br J Surg. 1984 Jul;71(7):522-3. doi: 10.1002/bjs.1800710716[↩][↩][↩][↩][↩]
- Heinz GJ, Zavala DC. Slipping rib syndrome. JAMA. 1977 Feb 21;237(8):794-5.[↩]
- Peterson LL, Cavanaugh DG. Two years of debilitating pain in a football spearing victim: slipping rib syndrome. Med Sci Sports Exerc. 2003 Oct;35(10):1634-7. doi: 10.1249/01.MSS.0000089249.00206.04[↩][↩][↩][↩][↩][↩]
- Gregory PL, Biswas AC, Batt ME. Musculoskeletal problems of the chest wall in athletes. Sports Med. 2002;32(4):235-50. doi: 10.2165/00007256-200232040-00003[↩][↩]
- Hussain A, Burns B. Anatomy, Thorax, Wall. [Updated 2023 Jul 30]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK535414[↩][↩]
- Donley ER, Holme MR, Loyd JW. Anatomy, Thorax, Wall Movements. [Updated 2024 Mar 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526023[↩][↩][↩][↩][↩]
- Flodine TE, Thomas M. Osteopathic Manipulative Treatment: Inhaled Rib Dysfunction. [Updated 2023 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560751[↩]
- Mortola JP, Sant’Ambrogio G. Motion of the rib cage and the abdomen in tetraplegic patients. Clin Sci Mol Med. 1978 Jan;54(1):25-32. doi: 10.1042/cs0540025[↩]
- Waxenbaum JA, Reddy V, Futterman B. Anatomy, Back, Thoracic Vertebrae. [Updated 2023 Aug 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459153[↩]
- Dobrusin R. An osteopathic approach to conservative management of thoracic outlet syndromes. J Am Osteopath Assoc. 1989 Aug;89(8):1046-50, 1053-7.[↩]
- Georgakopoulos B, Lasrado S. Anatomy, Head and Neck: Inter-scalene Triangle. [Updated 2022 Nov 9]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK544222[↩][↩][↩][↩]
- De Troyer A, Sampson M, Sigrist S, Macklem PT. The diaphragm: two muscles. Science. 1981 Jul 10;213(4504):237-8. doi: 10.1126/science.7244632[↩][↩][↩][↩]
- Germanovich A, Ferrante FM. Multi-Modal Treatment Approach to Painful Rib Syndrome: Case Series and Review of the Literature. Pain Physician. 2016 Mar;19(3):E465-71.[↩]
- Urmey W, Loring S, Mead J, Slutsky AS, Sarkarati M, Rossier A, Brown R. Upper and lower rib cage deformation during breathing in quadriplegics. J Appl Physiol (1985). 1986 Feb;60(2):618-22. doi: 10.1152/jappl.1986.60.2.618[↩]
- van Delft EAK, van Pul KM, Bloemers FW. The slipping rib syndrome: a case report. Int J Surg Case Rep 2016;23:23–4. 10.1016/j.ijscr.2016.04.009[↩]
- Foley Davelaar CM. A Clinical Review of Slipping Rib Syndrome. Curr Sports Med Rep. 2021 Mar 1;20(3):164-168. doi: 10.1249/JSR.0000000000000821[↩]
- Udermann BE, Cavanaugh DG, Gibson MH, Doberstein ST, Mayer JM, Murray SR. Slipping Rib Syndrome in a Collegiate Swimmer: A Case Report. J Athl Train. 2005 Jun;40(2):120-122. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1150226/[↩][↩]
- Migliore M, Signorelli M, Caltabiano R, Aguglia E. Flank pain caused by slipping rib syndrome. Lancet. 2014 Mar 1;383(9919):844. doi: 10.1016/S0140-6736(14)60156-2[↩]
- van Delft EA, van Pul KM, Bloemers FW. The slipping rib syndrome: A case report. Int J Surg Case Rep. 2016;23:23-4. doi: 10.1016/j.ijscr.2016.04.009[↩]
- Turcios NL. Slipping rib syndrome in an adolescent: an elusive diagnosis. Clin Pediatr (Phila). 2013 Sep;52(9):879-81. doi: 10.1177/0009922812469290[↩]
- McMahon LE. Recurrent Slipping Rib Syndrome: Initial Experience with Vertical Rib Stabilization Using Bioabsorbable Plating. J Laparoendosc Adv Surg Tech A. 2020 Mar;30(3):334-337. doi: 10.1089/lap.2019.0519[↩][↩][↩]
- Khan NAJ, Waseem S, Ullah S, Mehmood H. Slipping Rib Syndrome in a Female Adult with Longstanding Intractable Upper Abdominal Pain. Case Rep Med. 2018 Jul 2;2018:7484560. doi: 10.1155/2018/7484560[↩]
- Polycarpou A, Chopko TC, Glasgow AE, McCarthy SR, Hilliker DR, Wilder RT, Klinkner DB. One-year Results of Minimally Invasive Sutured Fixation of the Slipped Ribs in the Pediatric Population. J Pediatr Surg. 2024 Feb 29:S0022-3468(24)00109-X. doi: 10.1016/j.jpedsurg.2024.02.027[↩]





{kind=link}