Contents
Snake bite
It can be difficult to know if a bite from a snake is dangerous or not. However, most North American snakes aren’t dangerous to humans. Some exceptions include the rattlesnake, coral snake, water moccasin and copperhead. Their bites can be life-threatening. If the snake is dead, be careful of the head — a snake can actually bite (from a reflex) for several hours after it’s dead. Do not rely on visual identification of snakes as non-venomous, as appearances and coloration may vary considerably within species.
Most snakes will avoid people if possible, but all snakes will bite as a last resort when threatened or surprised. If you are bitten by any snake, treat it seriously.
It’s important to be aware that snake bites can cause a severe allergic reaction (anaphylaxis) in some people. Learn more about first aid treatment for severe allergic reactions in the ‘anaphylaxis’ section below.
If you are bitten by a venomous snake, call your local emergency services number immediately, especially if the area changes color, begins to swell or is painful. Many emergency rooms stock antivenom drugs, which may help you.
If possible, take these steps while waiting for medical help:
- Remain calm and move beyond the snake’s striking distance.
- Remove jewelry and tight clothing before you start to swell.
- Position yourself, if possible, so that the bite is at or below the level of your heart.
- Clean the wound, but don’t flush it with water. Cover it with a clean, dry dressing.
Caution
- Don’t use a tourniquet or apply ice.
- Don’t cut the wound or attempt to remove the venom.
- Don’t drink caffeine or alcohol, which could speed your body’s absorption of venom.
- Don’t try to capture the snake. Try to remember its color and shape so that you can describe it, which will help in your treatment.
Venomous snakes in North America
Most venomous snakes in North America have eyes like slits and are known as pit vipers. Their heads are triangular with a pit between the eye and nostril on either side of the head.
Venomous snake bites include bites by any of the following:
- Cobra
- Copperhead
- Coral snake
- Cottonmouth (water moccasin)
- Rattlesnake
- Various snakes found at zoos
Other characteristics are unique to certain venomous snakes:
- Rattlesnakes rattle by shaking the rings at the end of their tails.
- Water moccasins’ mouths have a white, cottony lining.
- Coral snakes have red, yellow and black rings along the length of their bodies. Their heads aren’t triangular and the pupils are round.
- Copperhead snakes have a copper-colored head and reddish brown bodies with dark bands.
Snake identification
Identification of venomous snakes can be made from venom present on clothing or the skin using a so called ‘venom detection’ kit. For this reason do not wash or suck the bite or discard clothing.
It’s not recommended to kill the snake for purposes of identification, because medical services do not rely on visual identification of the snake species.
What does a snake bite look like?
You may not always know you were bitten by a snake, especially if you were bitten in water or tall grass. Signs and symptoms of a snakebite may include the following:
- two puncture marks at the wound
- redness or swelling around the wound
- severe pain at the site of snake bite
- nausea
- vomiting
- difficulty breathing (in extreme cases, breathing may stop altogether)
- fever-like symptoms, such as sweating
- increased salivation and sweating
- numbness or tingling sensation in the fingers, toes or area around the wound
- blurry vision
- diarrhea
- fainting
- convulsions
- rapid pulse.
What should I do if I get a snakebite?
- Remain calm and call for help.
- If you are alone, try to get to the nearest hospital as soon as you can.
- Restrict movement as much as possible and try to keep the wound just below the level of your heart. This will reduce the spread of venom.
- Take off any jewelry or tight clothing near the bite before swelling starts.
- Try to remember what the snake looked like: its color, shape and markings. This will help with your treatment.
- Cover the bite with a clean, dry bandage.
Bull snake bite
Bull snake (Pituophis catenifer sayi) is a large non-venomous colubrid snake. It is currently considered a subspecies of the gopher snake (Pituophis catenifer).
Clinical effects
Not likely to cause significant effects.
- Rate of Envenoming: Non-venomous, so essentially all bites should be “dry”.
- General: Untreated Lethality Rate: No lethal potential, non-venomous bite
- Local Effects: Insufficient clinical reports to know, but most likely no local effects, possibly, at most, minor local pain & swelling only
- Local Necrosis: Insufficient clinical reports to know, but local necrosis most unlikely
- General Systemic Effects: Insufficient clinical reports to know, but systemic effects not expected
- General: Neurotoxic Paralysis
- Insufficient clinical reports to know, but unlikely to occur
- General: Myotoxicity
- Insufficient clinical reports to know, but unlikely to occur
- Coagulopathy and Hemorrhages: Insufficient clinical reports to know, but unlikely to occur
- General: Renal Damage
- Insufficient clinical reports to know, but unlikely to occur
- General: Cardiotoxicity
- Insufficient clinical reports to know, but unlikely to occur
- General: Other
- Insufficient clinical reports to know
Treatment
Bites by this species are not expected to cause medically significant effects and the only risk, probably small, is local secondary infection. Patients presenting with bites by these snakes do not require medical attention, other than to check for infection and ensure tetanus immune status. Patients should be advised to return if local symptoms develop, suggesting secondary infection.
Key Diagnostic Features
- Either no effects or minimal local pain & swelling only. No systemic effects.
- While most cases will be minor, not requiring admission, some cases will be more severe, requiring admission and treatment, so assess carefully before early discharge.
Antivenom Therapy
- No antivenom available
Copperhead snake bite
Clinical Effects 1)
Moderate envenoming possible. All cases should be treated as urgent and potentially lethal. Rapid assessment and commencement of treatment including appropriate antivenom (if indicated & available) is mandatory. Admit all cases.
- Rate of Envenoming: Unknown but likely to be moderate
- Untreated Lethality Rate: Unlikely to prove lethal
- Local Effects: Mild to no pain, mild swelling, no bruising, blistering
- Local Necrosis: Not likely to occur
- General Systemic Effects: General systemic symptoms usually absent
- Neurotoxic Paralysis: Does not occur, based on current clinical evidence
- Myotoxicity: Does not occur, based on current clinical evidence
- Coagulopathy and Hemorrhages: May cause mild coagulopathy, but pathologic bleeding not likely
- Renal Damage: Does not occur, based on current clinical evidence
- Cardiotoxicity: Does not occur, based on current clinical evidence
- Other: Insufficient clinical reports to know
Treatment
Bites by copperhead snake species vary from only minor local effects to moderate, rarely severe local effects, the latter potentially including hypovolaemic shock. Major systemic effects are likely to be confined to coagulopathy, though systemic myolysis is a theoretical risk, but not paralysis. Cases with major local or systemic envenoming should receive antivenom IV.
Key Diagnostic Features
Local pain, swelling, ecchymosis ± coagulopathy & haemorrhage
General Approach to Management
- All cases should be treated as urgent and potentially lethal. Rapid assessment and commencement of treatment including appropriate antivenom (if indicated & available) is mandatory. Admit all cases.
Antivenom Therapy
Antivenom Name: Polyvalent crotalid antivenom ( CroFab ), Ovine, Fab. Only antivenoms available are for related species, but should be used for significant envenoming.
Coral snake bite
Major coral snake bite symptoms may not develop for hours. DO NOT make the mistake of thinking you will be fine if the bite area looks good and you are not in a lot of pain. Untreated coral snake bites can be deadly. Symptoms may include:
- Blurred vision
- Breathing difficulty
- Convulsions
- Drowsiness
- Eyelid drooping
- Headache
- Low blood pressure
- Mouth watering (excessive salivation)
- Nausea and vomiting
- Numbness
- Pain and swelling at site of bite
- Paralysis
- Shock
- Slurred speech
- Swallowing difficulty
- Swelling of tongue and throat
- Weakness
- Skin color changes
- Skin tissue damage
- Stomach or abdominal pain
- Weak pulse
Cottonmouth snake bite
Clinical Effects 2):
Moderate envenoming possible and potentially lethal
- Rate of Envenoming: Unknown but likely to be moderate
- Untreated Lethality Rate: Unknown but lethal potential cannot be excluded
- Local Effects: Local pain, swelling, bruising & blistering
- Local Necrosis: Potentially may occur
- General Systemic Effects: Insufficient clinical reports to know, but might develop systemic symptoms in severe cases; headache, nausea, vomiting, abdominal pain, collapse
- Neurotoxic Paralysis: Does not occur, based on current clinical evidence
- Myotoxicity: Does not occur, based on current clinical evidence
- Coagulopathy and Hemorrhages: Insufficient clinical reports to know, but coagulopathy & haemorrhage might occur
- Renal Damage: Does not occur, based on current clinical evidence
- Cardiotoxicity: Does not occur, based on current clinical evidence
- Other: Insufficient clinical reports to know
Treatment
Bites by cottonmouth snake species vary from only minor local effects to moderate, rarely severe local effects, the latter potentially including hypovolemic shock. Major systemic effects are likely to be confined to coagulopathy, though systemic myolysis is a theoretical risk, but not paralysis. Cases with major local or systemic envenoming should receive antivenom IV.
Key Diagnostic Features
- Local pain, swelling, ecchymosis ± coagulopathy and hamorrhage
General Approach to Management
All cases should be treated as urgent & potentially lethal. Rapid assessment and commencement of treatment including appropriate antivenom (if indicated & available) is mandatory. Admit all cases.
Antivenom Therapy
- Only antivenoms available are for related species, but should be used for significant envenoming
Antivenom Name: Polyvalent crotalid antivenom ( CroFab ), Ovine, Fab
Garden snake bite
Clinical Effects 3):
Bite most unlikely to cause fatality, but death from constriction possible, but rare.
- Rate of Envenoming: Zero
- Untreated Lethality Rate: Very low
- Local Effects: Can cause numerous tooth punctures, with local pain & swelling, potential for secondary infection.
- Local Necrosis: Does not occur, based on current clinical evidence
- General Systemic Effects: Does not occur, based on current clinical evidence
- Neurotoxic Paralysis: Does not occur
- Myotoxicity: Does not occur
- Coagulopathy and Hemorrhages: Does not occur
- Renal Damage: Does not occur
- Cardiotoxicity: Does not occur
- Other: Does not occur
Treatment
Bites by boas and pythons do not cause envenoming, but can cause local pain, swelling, secondary infection, or rarely, more extensive injury from constriction. The wound should be washed thoroughly. If infection develops, commence targeted antibiotic therapy orally, or in more severe cases, IV. No antivenom is available, nor is it needed, because these snakes are non-venomous.
Key Diagnostic Features
- Local teeth marks, pain, swelling
General Approach to Management
- Most cases will be minor and not require admission.
Antivenom Therapy
- No antivenom available
Snake bite first aid
For all snake bites, provide emergency care including cardiopulmonary resuscitation (CPR) if needed. Call your local emergency services number for an ambulance. Apply a pressure immobilization bandage and keep the person calm and as still as possible until medical help arrives.
Avoid washing the bite area because any venom left on the skin can help identify the snake.
DO NOT apply a tourniquet, cut the wound or attempt to suck the venom out.
NOTE: If resuscitation is needed it takes precedence over the pressure immobilization bandage. However the resuscitation team should apply pressure immobilization bandage as soon as possible to potentially minimize further venom flow.
- DO NOT cut or excise the bitten area, or attempt to suck venom from the bite site.
- DO NOT wash the bitten area.
- DO NOT apply an arterial tourniquet. (Arterial tourniquets that cut off circulation to the limb, are potentially dangerous
- DO NOT pick up the snake or try to trap it.
- DO NOT wait for symptoms to appear if bitten. Seek immediate medical attention.
- DO NOT allow the person to become over-exerted. If necessary, carry the person to safety.
- DO NOT apply cold compresses to a snake bite.
- DO NOT apply ice or soak the wound in water.
- DO NOT cut into a snake bite with a knife or razor.
- DO NOT try to suck out the venom by mouth.
- DO NOT give the person stimulants or pain medicines unless a doctor tells you to do so.
- DO NOT give the person anything by mouth.
- DO NOT raise the site of the bite above the level of the person’s heart.
Pressure immobilization bandage
A pressure immobilization bandage is recommended for anyone bitten by a venomous snake. This involves firmly bandaging the area of the body involved, such as the arm or leg, and keeping the person calm and still until medical help arrives.
Follow these steps to apply a pressure immobilization bandage:
- First remove any rings or constricting items, because the affected area may swell.
- Secondly put a pressure bandage over the bite itself. If on a limb, apply a broad pressure bandage over the bite site as soon as possible. The bandage should be firm and tight and you should not be able to easily slide a finger between the bandage and the skin. Elasticized bandages (10-15cm wide) are preferred over crepe bandages, if neither are available, clothing or other material should be used 4).
- Then use a heavy crepe or elasticized roller bandage to immobilize the whole limb. In order to further restrict lymphatic flow and to assist in immobilization of the limb. Start at the fingers or toes of the bitten limb and moving upwards on the limb as far as the body, covering as much of the limb as possible 5). Splint the limb including joints on either side of the bite, to restrict limb movement. The bandage should be applied over existing clothing if possible. The purpose of this bandage is to further restrict lymphatic flow and assist immobilization. (Alternatively, a single bandage may be used to achieve both pressure on the bite site and immobilization of the limb. In this method, the bandage is initially applied to the fingers or toes and extended up the limb as far as possible including the bite site) 6).
- Keep the person and the limb completely at rest. If possible, mark the site of the bite on the bandage with a pen.
- Monitor the person’s vital signs — temperature, pulse, rate of breathing, and blood pressure — if possible. If there are signs of shock (such as paleness), lay the person flat, raise the feet about a foot (30 centimeters), and cover the person with a blanket.
If the bite is not on the limb, firm direct pressure on the bite site may be useful. Do not restrict breathing or chest movement and do not apply firm pressure to the neck or head.
Keep the victim and the limb completely at rest. Bring transport to the victim if possible. Transport the victim to medical care, preferably by ambulance. If alone, the victim should apply the pressure immobilization bandage as completely as possible over the bite site and affected limb. They should keep immobile until medical assistance arrives. If they are unable to obtain urgent help to come to them, then apply local pressure if possible, immobilization is contraindicated and they should move themselves to seek urgent help. Do not remove the bandages or splints before evaluation in an appropriate hospital environment.
Figure 1. Snake bite pressure immobilization bandage


Cardiopulmonary resuscitation (CPR)
How to perform a Cardiopulmonary Resuscitation (CPR) for for children over 1 year
- Step 1: If a child is unconscious, the first step is to check his mouth for anything blocking the airway. This could include his tongue, food, vomit or blood.
- Step 2: If you find a blockage, roll him onto his side, keeping his top leg bent. This is the recovery position. Clear blockages with your fingers, then check for breathing.
- Step 3: If you find no blockages, check for breathing and look for chest movements. Listen for breathing sounds, or feel for breath on your cheek.
- Step 4: If the child is breathing, gently roll him onto his side and into the recovery position. Phone your local emergency services number and check regularly for breathing and response until the ambulance arrives. If the child is not breathing and responding, send for help. Phone local emergency services number and start CPR: 30 chest compressions, 2 breaths.
- Step 5: Put the heels of your hands in the center of the child’s chest. Using the heel of your hand, give 30 compressions. Each compression should depress the chest by about one third.
- Step 6: After 30 compressions, take a deep breath, seal your mouth over the child’s mouth, pinch his nose and give two steady breaths. Make sure the child’s head is tilted back to open his airway.
- Step 7: Keep giving 30 compressions then 2 breaths until medical help arrives. If the child starts breathing and responding, turn him into the recovery position. Keep watching his breathing and be ready to start CPR again at any time.
Figure 2. CPR for for children over 1 year

How to perform a Cardiopulmonary Resuscitation (CPR) on Adults
Hands-only CPR
To carry out a chest compression:
- Place the heel of your hand on the breastbone at the centre of the person’s chest. Place your other hand on top of your first hand and interlock your fingers.
- Position yourself with your shoulders above your hands.
- Using your body weight (not just your arms), press straight down by 5-6cm (2-2.5 inches) on their chest.
- Keeping your hands on their chest, release the compression and allow the chest to return to its original position.
- Repeat these compressions at a rate of 100 to 120 times per minute until an ambulance arrives or you become exhausted.
When you call for an ambulance, telephone systems now exist that can give basic life-saving instructions, including advice about CPR. These are now common and are easily accessible with mobile phones.
Cardiopulmonary Resuscitation (CPR) with rescue breaths
If you’ve been trained in CPR, including rescue breaths, and feel confident using your skills, you should give chest compressions with rescue breaths. If you’re not completely confident, attempt hands-only CPR instead (see above).
Adults
- Place the heel of your hand on the center of the person’s chest, then place the other hand on top and press down by 5-6cm (2-2.5 inches) at a steady rate of 100 to 120 compressions per minute.
- After every 30 chest compressions, give two rescue breaths.
- Tilt the casualty’s head gently and lift the chin up with two fingers. Pinch the person’s nose. Seal your mouth over their mouth and blow steadily and firmly into their mouth for about one second. Check that their chest rises. Give two rescue breaths.
- Continue with cycles of 30 chest compressions and two rescue breaths until they begin to recover or emergency help arrives.
Anaphylactic shock
Snake bites can be painful. Occasionally some people have a severe allergic reaction to being bitten. In cases of severe allergic reaction, the whole body can react within minutes to the bite which can lead to anaphylactic shock. Anaphylactic shock is very serious and can be fatal.
Anaphylaxis is a severe and potentially life-threatening reaction to a trigger such as an allergy.
- Anaphylaxis is a medical emergency that requires immediate medical assistance and treatment.
- Anaphylaxis can occur within seconds or minutes of exposure to something you’re allergic to, such as peanuts or bee stings.
Anaphylaxis causes your immune system to release a flood of chemicals that can cause you to go into shock — your blood pressure drops suddenly and your airways narrow, blocking breathing. Signs and symptoms include a rapid, weak pulse; a skin rash; and nausea and vomiting. Common triggers include certain foods, some medications, insect venom and latex.
Anaphylaxis requires an injection of epinephrine and a follow-up trip to an emergency room. If you don’t have epinephrine, you need to go to an emergency room immediately. If anaphylaxis isn’t treated right away, it can be fatal.
Symptoms of anaphylactic shock may include:
- Trouble breathing or noisy breathing
- Difficulty talking more than a few words and/or hoarse voice
- Wheeze
- Cough
- Swelling and tightness of the throat
- Collapse
- Light-headedness or dizziness
- Diarrhea
- Tingling in the hands, feet, lips or scalp
- Swelling of tongue
- Pale and floppy (in young children)
Call your local emergency services number for an ambulance. If the person has a ‘personal action plan’ to manage a known severe allergy, they may need assistance to follow their plan. This may include administering adrenaline to the person via an autoinjector (such as an Epipen®) if one is available.
How to use Adrenaline auto-injectors
People with potentially serious allergies will often be given an adrenaline auto-injector to carry at all times. This can help stop an anaphylactic reaction becoming life threatening.
This should be used as soon as a serious reaction is suspected, either by the person experiencing anaphylaxis or someone helping them.
If you’ve been given an auto-injector, make sure you’re aware how to use it correctly.
There are three main types of adrenaline auto-injector, which are used in slightly different ways.
These are:
- EpiPen – see Figure 1 on how to use Epipen
- Jext
- Emerade
Instructions are also included on the side of each injector if you forget how to use it or someone else needs to give you the injection.
Figure 3. How to use the Epipen
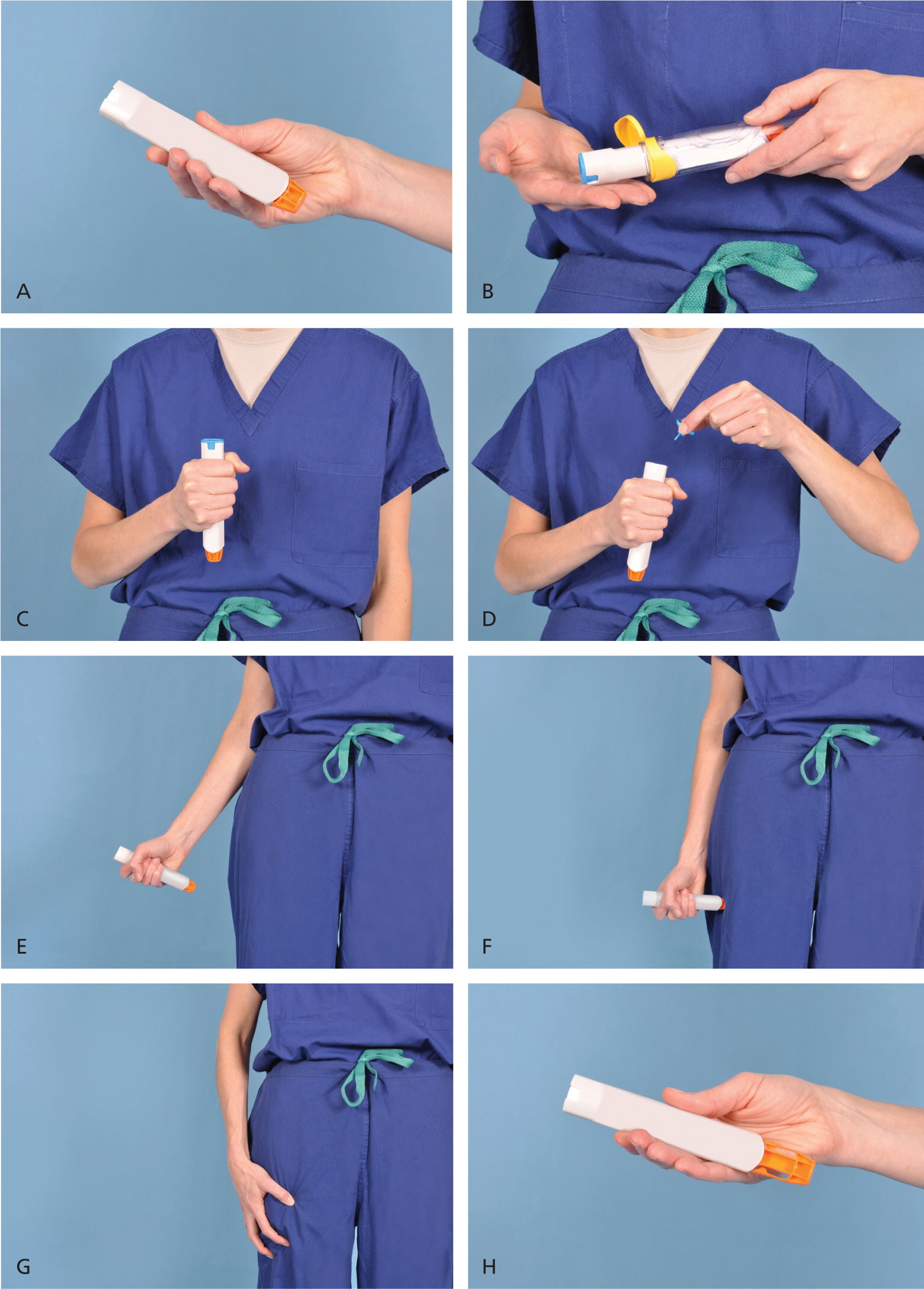
Demonstration of appropriate deployment of the (A) Epipen (released in 2008). For demonstration purposes, a trainer device is being used instead of a live device; however, the coloring of key components is the same as the actual adult device. (B) Open the yellow cap of the carrying case and remove the device from its storage tube (the Epipen Jr. has a green cap). (C) Grasp and form a fist around the unit with the orange tip facing down. (D) With the other hand, remove the blue safety release. (E) Aim the orange tip toward the outer thigh. (F) Swing the arm and jab the device firmly into the outer thigh, at a 90-degree angle, until the device clicks. The needle will deploy at this time into thigh (the autoinjector is designed to work through clothing). Hold the device firmly against the thigh for 10 seconds, so the entire dose will be delivered. (G) Remove the device from the thigh and massage the injection area for 10 seconds. (H) The safety feature of the device, extension of the orange tip that locks into place, will completely cover the needle immediately after use. The used device should be taken to the hospital emergency department with the patient for disposal.
Different types of snake bites
Dry bites
A dry bite is when the snake strikes but no venom is released. Dry bites will be painful and may cause swelling and redness around the area of the snake bite.
Because you can’t tell if a snake’s bite is a dry bite always assume that you have been injected with venom, and manage the bite as a medical emergency. Once medically assessed, there is usually no need for further treatment, such as with antivenoms. Many snake bites in Australia do not result in envenomation, and so they can be managed without antivenom.
Venomous bites
Venomous bites are when the snake bites and releases venom (poison) into a wound. Snake venom contains poisons which are designed to stun, numb, or kill other animals. A bite by a venomous snake can cause local tissue death (necrosis), bleeding and destruction of blood cells (hematological problems), and nerve (neurological) damage (coma, paralysis).
Symptoms of a venomous bite include:
- severe pain around the bite, this might come on later
- swelling, bruising or bleeding from the bite
- bite marks on the skin (these might be obvious puncture wounds or almost invisible small scratches)
- swollen and tender glands in the armpit or groin of the limb that has been bitten
- tingling, stinging, burning or abnormal feelings of the skin
- feeling anxious
- nausea (feeling sick) or vomiting (being sick)
- dizziness
- blurred vision
- headache
- breathing difficulties
- problems swallowing
- stomach pain
- irregular heartbeat
- muscle weakness
- confusion
- blood oozing from the site or gums
- collapse
- paralysis, coma or death (in the most severe cases)
Snake bite symptoms
Most snakebites occur on the extremities. If the bite is from a nonvenomous snake, typical symptoms are pain and scratches at the site.
Usually, after a bite from a poisonous snake, there is severe burning pain at the site, within 15 to 30 minutes. This can progress to swelling and bruising at the wound, and all the way up the arm or leg. Other symptoms include nausea and a general sense of weakness, as well as an odd taste in the mouth.
Some snakes, such as coral snakes, have toxins that cause neurological symptoms, such as tingling, difficulty speaking and weakness.
Symptoms depend on the type of snake, but may include:
- Bleeding from wound
- Blurred vision
- Burning of the skin
- Convulsions
- Diarrhea
- Dizziness
- Excessive sweating
- Fainting
- Fang marks in the skin
- Fever
- Increased thirst
- Loss of muscle coordination
- Nausea and vomiting
- Numbness and tingling
- Rapid pulse
- Tissue death
- Severe pain
- Skin discoloration
- Swelling at the site of the bite
- Weakness
Rattlesnake bites are painful when they occur.
Rattlesnake bite symptoms usually begin right away and may include:
- Bleeding
- Breathing difficulty
- Blurred vision
- Eyelid drooping
- Low blood pressure
- Nausea and vomiting
- Numbness
- Pain at site of bite
- Paralysis
- Rapid pulse
- Skin color changes
- Swelling
- Tingling
- Tissue damage
- Thirst
- Tiredness
- Weakness
- Weak pulse
Cottonmouth and copperhead bites are painful right when they occur.
Cottonmouth and copperhead bite symptoms, which usually begin right away, may include:
- Bleeding
- Breathing difficulty
- Low blood pressure
- Nausea and vomiting
- Numbness and tingling
- Pain at site of bite
- Shock
- Skin color changes
- Swelling
- Thirst
- Tiredness
- Tissue damage
- Weakness
- Weak pulse
Coral snake bites may be painless at first.
Major coral snake bite symptoms may not develop for hours. DO NOT make the mistake of thinking you will be fine if the bite area looks good and you are not in a lot of pain. Untreated coral snake bites can be deadly. Symptoms may include:
- Blurred vision
- Breathing difficulty
- Convulsions
- Drowsiness
- Eyelid drooping
- Headache
- Low blood pressure
- Mouth watering (excessive salivation)
- Nausea and vomiting
- Numbness
- Pain and swelling at site of bite
- Paralysis
- Shock
- Slurred speech
- Swallowing difficulty
- Swelling of tongue and throat
- Weakness
- Skin color changes
- Skin tissue damage
- Stomach or abdominal pain
- Weak pulse
Anaphylaxis
In a small number of people, a snake bite can trigger a severe reaction, known as anaphylaxis or anaphylactic shock. This can occur immediately after a bite or several hours later.
Anaphylaxis should always be treated as a medical emergency. Left untreated, anaphylaxis can be life threatening.
Symptoms of anaphylaxis include:
- itchy skin with hives and redness
- swollen face, lips, tongue and throat
- swelling in the throat that can cause breathing difficulties
- wheezing and difficulty breathing
- rapid heartbeat
- nausea, vomiting and diarrhea
Anaphylaxis can also cause a drop in blood pressure, which can lead to shock and cause symptoms such as:
- dizziness or mental confusion
- faintness, loss of consciousness or collapsing
- cold and clammy skin
- blindness
Shock
Someone who’s been bitten by a snake may go into shock. Shock is a life-threatening condition that occurs when there’s an insufficient supply of oxygen to the body.
Shock should always be treated as a medical emergency – you should dial your local emergency services number to request an ambulance immediately.
Symptoms of shock include:
- faintness or collapsing
pale, cold, clammy skin - sweating
- rapid, shallow breathing
- weakness and dizziness
- blindness
- feeling sick and possibly vomiting
- drowsiness or loss of consciousness
After calling an ambulance, lay the person down and raise and support their legs. Use a coat or blanket to keep them warm.
Snake bite prevention
To prevent snake bites:
- Leave snakes alone.
Do not attempt to catch or handle snakes. - Avoid areas where snakes may be hiding, such as under rocks and logs.
- Even though most snakes are not venomous, avoid picking up or playing with any snake unless you have been properly trained.
- Don’t provoke a snake. That is when many serious snake bites occur.
- Tap ahead of you with a walking stick before entering an area where you can’t see your feet. Snakes will try to avoid you if given enough warning.
- When hiking in an area known to have snakes, wear long pants and boots if possible.
- Never put hands in hollow logs or thick grass or under woodpiles, building material etc without prior inspection.
- When stepping over logs, carefully inspect the ground on the other side.
- Keep barns and sheds free of mice and rats as they may attract snakes.
- Keep grass well cut – particularly in playgrounds, around houses etc.
- Take care around houses, barns etc on warm nights, as snakes may be active at this time. Use a torch and wear adequate footwear.
- Do not handle snakes whilst intoxicated.
- Educate children in the above precautions.
Traveling abroad
If you’re bitten by a snake while abroad, you should assume it’s a medical emergency and contact the relevant emergency medical services.
If you’re traveling to an area where there’s a risk of being bitten by a snake, make sure you know how to contact emergency medical services in that country.
When traveling abroad, carry a first aid kit that contains medications, such as painkillers, antacids (for indigestion) and rehydration sachets (for diarrhea). It should also include plasters, non-adherent dressings and bandages, insect repellent, and sun cream.
Snake bite treatment
Only 1 in 20 snake bites require active emergency treatment or the administration of antivenom (antidote to snake venom), but every snake bite should be managed as a medical emergency until resolved, even if the person seems well on presentation. Medical management depends on the degree of systemic envenomation, the effectiveness of first aid bandaging, and the type of venom.
Antivenoms contain antibodies, which are proteins that neutralise the effects of the snake’s venom toxins.
Antivenom should be given to all patients who exhibit signs of systemic spread. In some people, antivenoms can trigger a severe reaction called anaphylaxis, so it’s important you’re closely monitored after receiving this treatment. Anaphylaxis is treated with adrenaline. Because of the risk of anaphylaxis, antivenom should only be given by a qualified healthcare professional.
General treatment considerations:
Compartment syndrome requiring surgical intervention is a relatively uncommon complication of pit viper envenomation that may be confused with direct venom-induced muscle necrosis. Wick catheter or other intracompartmental pressure measurement > 30 mm Hg is required for diagnosis. If compartment syndrome is present, urgent surgical consultation is required 7).
Additional treatments may include nonsedating analgesia, coagulation factor and platelet replacement (controversial; currently under investigation), dialysis for established renal failure, urine alkalinization for myoglobinuria (uncertain value), and respiratory support as indicated 8).
After administration of antivenom, a short, nontapered course of prednisone (40 to 60 mg daily for five days) should be given to decrease the incidence of type III immune complex disease. Wound care and tetanus prophylaxis should be provided as indicated. Antibiotics are indicated only if evidence of infection is present.
Critically ill patients
- Maintain immobilization, splint and bandage until the situation is under control!
- Support airway, breathing and circulation.
- Intubate and ventilate with 100% Oxygen if airway or respiration fail.
- Give antivenom immediately. Intravenous adrenaline should be given only for lifethreatening hypotension or anaphylaxis – its use has been associated with cerebral hemorrhage.
- Volume expansion may be necessary.
- Severe coagulation disturbances, electrolyte abnormalities, and muscle damage leading to acute renal failure are likely.
- Repeat antivenom as clinically indicated.
- General management as for less seriously ill patients as well (see below).
Less seriously ill patients – no signs of systemic spread
- Admit to ICU for non-invasive monitoring, strict bedrest and full head injury observations (wake hourly).
- Leave bandages in place.
- Obtain appropriate antivenoms and venom detection kit.
- Obtain intravenous access.
- Take blood for group and X-match, coagulation screen (including APTT, fibrinogen levels, CK and tests for DIC), full blood count, electrolytes and calcium, creatinine kinase and arterial blood gases. Perform ECG. Repeat at appropriate intervals.
- Collect urine for microscopy to detect hematuria and for free protein, hemoglobin and myoglobin measurement. Record urine output. Freeze the first sample for venom detection.
- Draw up adrenaline, antihistamine, and steroids in case of anaphylaxis to antivenom.
- When ready, cut a hole over the wound site, inspect and take swabs for use with the venom detection kit.
- Once the results of the venom detection kit are known, slowly and progressively remove the bandages. Don’t rush!
If systemic symptoms ensue:
- Re-apply bandages and give antivenom as clinically indicated.
- Ensure the patient is well hydrated (to reduce the risk of acute renal failure due to rhabdomyolysis).
- Repeat blood tests, ECG, etc at clinically relevant intervals.
- Correct abnormal coagulation; look out for disseminated intravascular coagulation (heparin probably contra-indicated in disseminated intravascular coagulation (DIC) from snake bite).
- Analgesia and sedation – be cautious.
- Correct hypotension, if present, with volume expansion and vasopressors (exclude occult bleeding).
- Watch for development of renal failure – monitor urine output and composition.
- Tetanus prohylaxis is recommended.
Usually, if there are no signs of envenomation four hours after removal of the bandages, and if repeat blood tests taken at that time are normal, then it is probable that significant envenomation has not occurred. If laboratory tests are not available, 12 to 24 hours is a reasonable period of observation.
Recovery is usually complete, though the patient usually develops a sensitivity to equine immunoglobulin.
If the patient develops serum sickness (see below), the severity is reduced by steroid administration (e.g., prednisolone 1mg/kg every 8 hours) until resolution occurs. A course of steroids is recommended in all patients who receive polyvalent antivenoms.
Snake bite shot
Antivenom indications:
A grading system may be used to approximate the degree of envenomation, but should be balanced with individual presentation and comorbidities:
0 = nonenvenomation (“dry” bite). Fang marks may or may not be visible; no local or systemic effects. Antivenom is not indicated.
1 = minimal envenomation. Local effects (pain, edema) are limited to the bite site; no systemic effects or laboratory abnormalities. Antivenom is not usually needed, but may be given if clinical progression occurs.
2 = moderate envenomation. Extension of local effects, but the entire bitten extremity is not involved; systemic signs (e.g., nausea, vomiting, metallic taste); some laboratory abnormalities (e.g., thrombocytopenia, prolonged INR, elevated CPK level). Antivenom is required.
3 = severe envenomation. Rapidly progressing edema; blistering and ecchymoses; shock; altered sensorium; multiple laboratory abnormalities (e.g., markedly prolonged INR, severe thrombocytopenia [platelet count < 20,000 mm3]); fibrin degradation products; renal insufficiency or failure. Antivenom is required with a high initial dose. Large subsequent doses are often required.
Antivenom dosing and administration 9):
- Give Crotalidae polyvalent immune Fab (ovine): 4 to 6 vials, each reconstituted (10 mL saline) and diluted in 250 mL saline, IV administration.
- Initial infusion of 20 to 60 mL per minute; increase to 250 mL per hour if no adverse reactions occur.
- Give additional 4 to 6 vials, followed by 2 vials every six hours for 18 hours (14 to 18 vials total) as indicated; higher doses may be required for severe envenomations.
Presynaptic envenomation by species such as Mojave rattlesnakes may require higher doses and may be ineffective in late presentations, requiring intubation and ventilation.
Delayed absorption of sequestered venom is possible; because of the variably short half-life of the antivenom (12 to 23 hours), serial assessment of INR is essential (e.g., reversal of prolonged INR is sufficient to withhold further antivenom, but INR must be monitored for 24 to 48 hours [sometimes longer]).
Crotalidae polyvalent immune Fab (ovine) is approved for mild to moderate envenomation by rattlesnakes (Crotalus species), but published clinical experience indicates that it is also effective for severe envenomation 10). It has been used for copperhead (Agkistrodon contortrix) envenomations, but controlled trials with long-term follow-up are needed to evaluate its use in these cases 11). Its effectiveness for envenomations by water moccasins (Agkistrodon piscivorus), pygmy rattlesnakes (Sistrurus miliarius), and massasaugas (Sistrurus catenatus) requires formal clinical assessment. Coral snake envenomation requires specific anti-coral snake anti-venom. Although the coral snake antivenom formerly manufactured by Wyeth is no longer in production, an alternative formulation from Mexico (Coralmyn) is being tested 12). An antivenom for serious scorpion stings in the Southwest is also being tested (Centruroides F(ab)2); initial results indicate promising effectiveness 13).
All antivenoms have the potential to cause early and late adverse effects, including anaphylactic reactions on first exposure. For this reason, antivenom should be given only in a setting where resources to manage anaphylaxis are immediately available. Pretesting for allergy to antivenom is no longer recommended 14). The use of premedication before administration of antivenom is controversial and not widely practiced; evidence indicates that neither steroids nor antihistamines provide benefit. Pre-treatment with a non-sedating anti-histamine (i.e,, promethazine 0.25 mg/kg), subcutaneous adrenaline (0.25mg for adults, 0.01mg/kg for children), and IV steroids (hydrocortisone 2mg/kg) is still recommended, athough severe reactions are rare. In general the risk from the snake toxins is much greater than the risk of administering the antivenom.
All patients with serious envenomation must be counseled about the risk of antivenom anaphylaxis, immune complex disease, and possible loss of function, regardless of treatment effectiveness. If an antivenom is administered, patients are advised of the possibility of delayed serum sickness (up to 14 days later). This is characterized by fever, rash, generalized lymphadenopathy, aching joints and renal impairment. The likelihood of developing this depends on the volume of antivenom required. It occurs in about 10% of patients who are given polyvalent antivenoms. Treatment with steroids is usually all that is needed.
Antivenoms are prepared from horse serum. The risk of anaphylaxis is very low (less than 1% even for polyvalent antivenoms), but is increased in people who have had prior exposure to horses, equine tetanus vaccines, and a general allergic history. This increased risk is much more common in people aged 50 years or more. About 4% of all administrations are associated with minor reactions.
Recovery from snake bite
Recovery times for snake bites can vary depending on the species of snake involved.
In most cases, children bitten by an adder will make a full recovery in one to two weeks.
Adults usually take more than three weeks to recover fully, with a quarter taking between one to nine months. Early treatment with antivenom can reduce these times.
During the recovery period, you may experience episodes of pain and swelling in the area that’s been bitten.
These symptoms can usually be controlled by taking over-the-counter painkillers, such as paracetamol, and continuing to exercise the limb.
References [ + ]


{kind=link}