
Contents
Snoring
Snoring is a loud or harsh sound made by vibrations of the soft palate and other tissue in the mouth, nose and throat (upper airway) that can occur as you sleep. Snoring is caused by turbulence inside the airway during inspiration. The turbulence is caused by a partial blockage that may be located anywhere from the tip of your nose to the vocal chords. The restriction may occur only during sleep, or it may persist all the time and be worse when you are asleep. This is because your muscle tone is reduced during sleep and there may be insufficient muscle tone to prevent the airway tissue vibrating. During waking hours muscle tone keeps the airway in good shape; that’s why you don’t snore when awake.
- There is not a cure for snoring.
- Snoring can however, be successfully controlled. The sound you know as snoring is caused by a physical abnormality that needs to be identified before a control can be found.
- There are many thousands of web sites offering products that claim to cure snoring, with many offering nothing more than snake oil. If you are serious about wanting to stop snoring, then we encourage you to read about the many different causes of snoring.
Snoring can originate from the nose, oropharynx or the base of the tongue. In recent years it has been found that the tongue plays a far more important role in the incidence of snoring than was once thought.
Snoring is very common and usually isn’t caused by anything serious. About half of people snore at some point in their lives. Snoring is more common in men, though many women snore. Snoring appears to run in families and becomes more common as you get older. About 40 percent of adult men and 24 percent of adult women are habitual snorers. Men become less likely to snore after the age of 70.
Sleeping on your back may make you more likely to snore. It may also occur as your throat muscles relax from use of alcohol or other depressants. Congestion from a cold or allergies can also cause you to snore.
Snoring can be a nuisance to your partner and anyone else nearby. You may even snore loudly enough to wake yourself up. Though, in many cases people do not realize that they snore. Snoring can also cause you to have a dry mouth or sore or irritated throat when you wake up.
Light snoring may not disrupt your overall sleep quality. Heavy snoring may be associated with obstructive sleep apnea, a serious sleep disorder and a risk factor for heart disease, stroke, diabetes and many other health problems.
Snoring is something that cannot be stopped at will, neither is it something that can be ‘cured’. It can however, be successfully controlled. Snoring is caused by a physical abnormality that needs to be identified before a control can be found. This is not as difficult as it seems and the good news is there is a control for everybody. Finding the cause is the key to finding a solution. In most instances snoring can be controlled by simple self-help remedies.
Most snorers tend to take the ‘hit and miss’ route to finding a solution, with the inevitable disappointing result. They are often lured into buying products that claim to have exceedingly high success rates. Sadly, for many snorers, they become so despondent that they give up on their quest to stop.
Snoring is caused by a physical abnormality that needs to be identified before a control can be found. This is not as difficult as it seems and the good news is there is a control for everybody.
- Fat deposits around the neck – double chin
- Obstruction at the back of the tongue caused by a ‘weak chin’
- Small or collapsing nostrils
- Deviated septum
- Nasal congestion and catarrh
- Enlarged nasal turbinates and nasal polyps
- Large soft palate or uvula
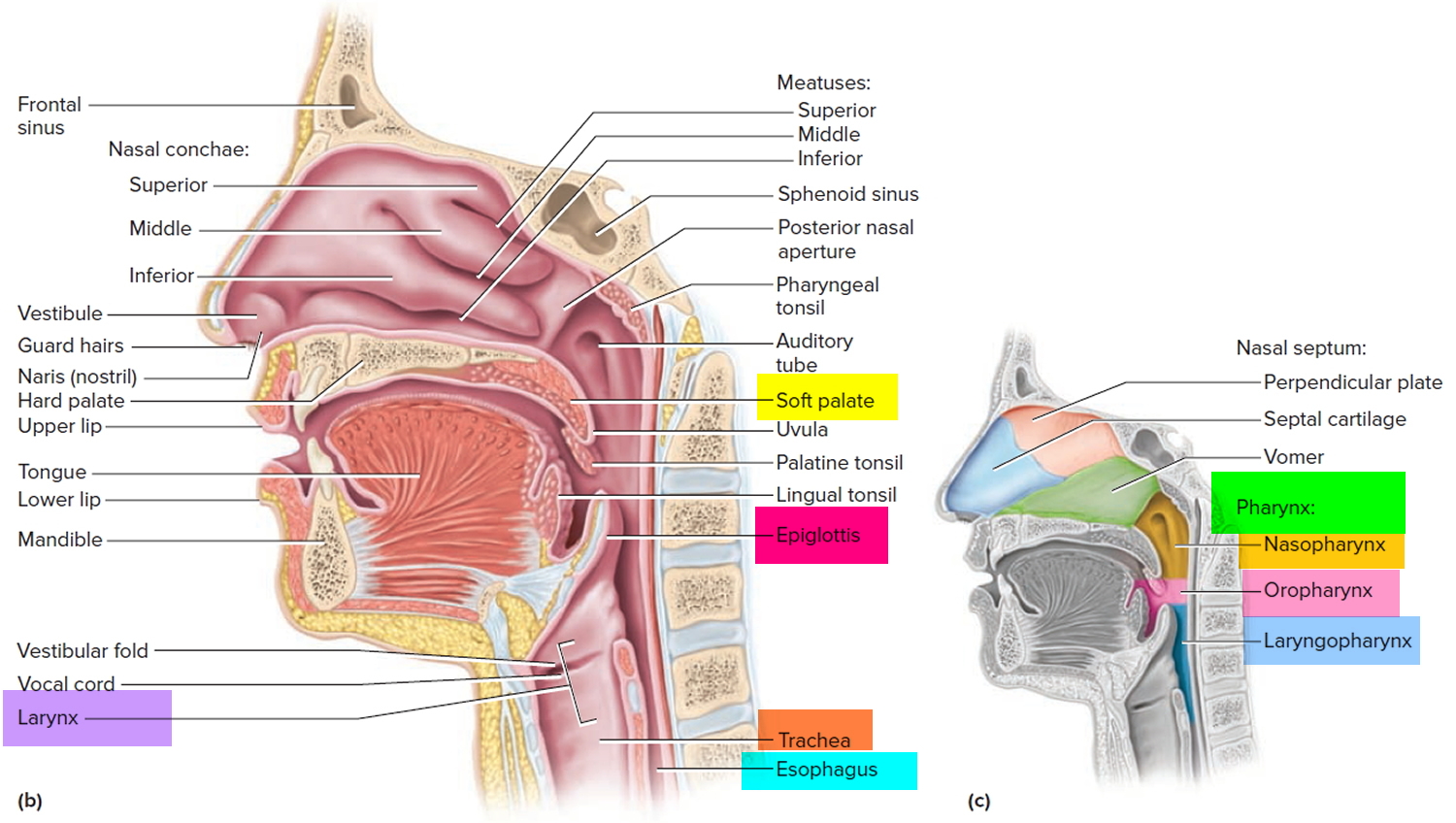
Figure 1. Pharynx and larynx anatomy
See your doctor if you have any of the following symptoms. These may indicate your snoring is associated with obstructive sleep apnea (OSA).
- Witnessed breathing pauses during sleep
- Excessive daytime sleepiness
- Difficulty concentrating
- Morning headaches
- Sore throat upon awakening
- Restless sleep
- Moodiness, irritability or depression
- Gasping or choking at night
- High blood pressure
- Chest pain at night
- Your snoring is so loud it’s disrupting your partner’s sleep
- Frequent need to urinate during the night
- In children, poor attention span, behavioral issues or poor performance in school
If your child snores, ask your pediatrician about it. Children can have obstructive sleep apnea (OSA), too. Nose and throat problems — such as enlarged tonsils — and obesity often can narrow a child’s airway, which can lead to your child developing obstructive sleep apnea (OSA).
Snoring vs. Sleep Apnea
Snoring can be a symptom of obstructive sleep apnea but not everyone who snores has the sleep disorder. Obstructive sleep apnea is a serious sleep disorder that causes you to temporarily stop breathing when you are asleep. These periods of ‘stopping breathing’ only become clinically significant if the cessation lasts for more than 10 seconds each time and occur more than 5 times every hour. When you experience an episode of apnoea during sleep your brain will automatically wake you up, usually with a very loud snore or snort, in order to breathe again. People with obstructive sleep apnea will experience these wakening episodes many times during the night and consequently feel very sleepy during the day: they have an airway that is more likely to collapse than normal. If you are regularly tired during the day even though you have had sufficient sleep or if your snoring is paired with choking or gasping sound, you may have sleep apnea. A sleep medicine physician is trained to detect and diagnose sleep apnea using an in-lab sleep study or home sleep testing. Sleep apnea is manageable using several approaches including CPAP (continuous positive airway pressure), oral appliance therapy and surgery.
Obstructive sleep apnea (OSA) is the commonest form of sleep apnea, affecting about 4% of men and 2% of women, but there is also a condition called Central Sleep Apnea (CSA). This is a condition when the brain does not send the right signals to tell you to breathe when you are asleep. In other words the brain ‘forgets’ to make you breathe. It can also be associated with weakness of the breathing muscles. The assessment for Central Sleep Apnoea (CSA) is often more complicated than for obstructive sleep apnea and the treatment has to be carefully matched to the patient’s requirements. There is also a condition called Mixed Sleep Apnea that is a combination of both obstructive and central sleep apnea.
How do you know if you have sleep apnea?
People with sleep apnea may complain of excessive daytime sleepiness often with irritability or restlessness. But it is normally the bed partner, family or friends who notice the symptoms first. Sufferers may experience some of the following:
- Extremely loud heavy snoring, often interrupted by pauses and gasps
- Excessive daytime sleepiness, e.g., falling asleep at work, whilst driving, during conversation or when watching TV. (This should not be confused with excessive tiredness with which we all suffer from time to time)
- Irritability, short temper
- Morning headaches
- Forgetfulness
- Changes in mood or behavior
- Anxiety or depression
- Decreased interest in sex
Remember, not everyone who has these symptoms will necessarily have sleep apnea. Most possibly all suffer from these symptoms from time to time but people with sleep apnea demonstrate some or all of these symptoms all the time.
Diagnosing Sleep Apnea
To determine whether you are suffering from sleep apnoea you must first undergo a specialist ‘sleep study’. This will usually involve a night in hospital where equipment will be used to monitor the quality of your sleep. The results will enable a specialist to decide on your best course of treatment. The ultimate investigation is polysomnography, which will include:
- Electro-encephalography (EEG) – brain wave monitoring
- Electromyography (EMG) – muscle tone monitoring
- Recording thoracic-abdominal movements – chest and abdomen movements
- Recording oro-nasal airflow – mouth and nose airflow
- Pulse oximetry – heart rate and blood oxygen level monitoring
- Electrocardiography (ECG) – heart monitoring
- Sound and video recording
This is a very expensive investigation, with few centers able to offer it routinely for all suspected sleep apnea patients. A ‘mini’ sleep study is more usual, consisting of pulse oximetry and nursing observation. Home sleep study is becoming more popular.
Treating Sleep Apnea
There are several forms of treatment for sleep apnoea. In mild and moderate cases weight loss and the use of mandibular advancement devices can be wholly successful. In moderate and severe cases mandibular advancement device or nasal continuous positive airway pressure (CPAP) are normally prescribed. CPAP is the gold standard treatment for obstructive sleep apnea.
What causes snoring
Snoring is caused by things such as your tongue, mouth, throat or airways in your nose vibrating as you breathe.
When you doze off and progress from a light sleep to a deep sleep, the muscles in the roof of your mouth (soft palate), tongue and throat relax. The tissues in your throat can relax enough that they partially block your airway and vibrate.
The more narrowed your airway, the more forceful the airflow becomes. This increases tissue vibration, which causes your snoring to grow louder.
The following are the causes of snoring and by controlling them, you can become quiet at night:
- Overweight/obesity and/or Lack of Exercise. Obesity and/or lack of exercise leads to an increase in fat around the throat. If you have fatty tissue around your neck you will find that during sleep it squeezes the airway and prevents air from flowing in and out freely. If you have a collar size of 16½ inches or greater, you may not have the muscle tone needed to keep the airway open sufficiently at night to allow normal breathing, and the narrow airway is more likely to vibrate. A person with a short fat neck is at an increased risk of snoring. Excess body fat seems to be more of a problem for men than women.
- Pregnancy.
- Alcohol
- Sleeping Pills
- Smoking. Cigarette smoke irritates the lining of the nasal cavity and throat causing swelling and catarrh. If the nasal passages become congested it is difficult to breathe through your nose because the airflow is decreased. The likelihood of snoring increases as more cigarettes are smoked per day because the congestion increases with each cigarette. Even passive smoking can cause inflammation of the nose and throat passages, thus increasing the risk of snoring. Children of parents who smoke are more likely to be affected by snoring than children of non smoking parents.
- Sleeping on your back. Several studies have found that individuals who sleep in the supine position (on the back) are more likely to snore or have increased sleep apneas than those who sleep in the lateral position (on the side).
- Allergy. Allergies and in particular allergic rhinitis are increasing in prevalence and currently affect between 10-25% of the population. The most common symptoms include: nasal congestion, rhinorrhea (runny nose), itching, postnasal drip and sneezing. Congestion in the nasal airway can lead to sleep disordered breathing and snoring.
- Nasal Stuffiness. Nasal stuffiness is another common reason for mouth breathing, because we tend to breathe with our mouths open to compensate for not being able to breathe through our noses. It is essential that you find out what is causing the nasal stuffiness and treat it.
- Mouth Breather. If you are a ‘mouth breather’ and sleep with your mouth open you will probably snore. When we breathe in through the nose the air passes over the curved part of the soft palate in a gentle flow into the throat without creating unnecessary turbulence. When we breathe in through the mouth however, the air hits the back of the throat ‘head on’ and can create enormous vibrations in the soft tissue.
- Small or Collapsing Nostrils.
- During sleep we are designed to breathe through the nose. If for any reason nasal breathing is not possible our body’s self-preservation mechanism forces us to breathe through the mouth. There are several reasons as to why some people find it difficult to breathe through the nose during sleep.
- Size of nostrils
- Nasal collapse (alar collapse)
- Nocturnal nasal congestion (rhinitis)
- Nasal obstruction (anatomic abnormalities)
- These features increase nasal resistance, commonly known simply as ‘nasal resistance’. Nasal resistance may be a contributing factor in the occurrence of sleep disordered breathing, upper airway resistance syndrome, snoring and obstructive sleep apnea (OSA).
- During sleep we are designed to breathe through the nose. If for any reason nasal breathing is not possible our body’s self-preservation mechanism forces us to breathe through the mouth. There are several reasons as to why some people find it difficult to breathe through the nose during sleep.
- Tongue Base Snorer. If you are a ‘tongue base snorer’, this means that you snore because your airway is liable to vibrate at the base of the tongue. Turbulent air is trying to get into your lungs through this restricted airway and in doing so it vibrates the tissues of the tongue. The tongue may partially or completely block the airway preventing you from breathing.
- Medications e.g. muscle relaxants and other medications
- Multifactoral Snoring e.g. genetic factors,
Sometimes snoring is caused by a condition like obstructive sleep apnea (OSA), which is when your airways become temporarily blocked as you sleep.
Risk factors for snoring
Risk factors that may contribute to snoring include:
- Being a man. Men are more likely to snore or have sleep apnea than are women.
- Being overweight. People who are overweight or obese are more likely to snore or have obstructive sleep apnea.
- Having a narrow airway. Some people may have a long soft palate, or large tonsils or adenoids, which can narrow the airway and cause snoring.
- Drinking alcohol. Alcohol relaxes your throat muscles, increasing the risk of snoring.
- Having nasal problems. If you have a structural defect in your airway, such as a deviated septum, or your nose is chronically congested, your risk of snoring is greater.
- Having a family history of snoring or obstructive sleep apnea. Heredity is a potential risk factor for OSA.
How to prevent snoring
- Losing weight. Weight loss can help reduce or eliminate your snoring for some people. If you are overweight or obese losing weight should be a priority. Weight gain can make snoring worse, and may even lead to sleep apnea.
- Do regular exercise. Weak muscles around your airway are more likely to collapse while you sleep, triggering snoring. But surprise: Just like regular exercise can tone your arms, legs, and belly, it also tones the muscles of your throat, which can help you stop snoring.
- Avoiding alcohol close to bedtime.
- Avoid muscle relaxants and certain medications like sedatives and sleeping pills.
- Avoid or quit smoking.
- Treating nasal congestion. You’ll be less likely to snore if your nasal passages are unobstructed, because that’ll provide an open passage for the air you breathe. Try a warm shower before bed, use a neti pot or saline spray to flush out your nose, try nasal strips to widen your nostrils, and consider keeping a humidifier in your bedroom to keep the air moist (aim for 50% humidity in the bedroom).
- Get enough sleep. Late nights plus early mornings can spell snore-filled slumber. That’s because when your head finally hits the pillow, you’re overtired and your throat’s muscles are slack and prone to snoring.
- Avoiding sleeping on your back. For some people, snoring mostly occurs while they sleep on their back. If you are one of these types of snorers, you may be able to improve your snoring by changing your sleep position. There are a variety of products that you can wear when you go to sleep that prevent you from sleeping on your back. You can also attach a tennis ball to the back of your shirt or pajamas. This does not work for everyone.
- Raise the head of your bed. Raising the head of your bed by about 4 inches may help. Propping up the head of your mattress with small blocks can help to take pressure off your airway so that it’s easier to breathe while you sleep. Just make sure to prop up your whole upper body since lifting just your head can actually have the opposite effect.
- Get Rid of Allergens. Dust your ceiling fans, wash your sheets and blankets, and throw your pillows in the dryer on fluff every few weeks to help rid your bedroom of dust mites, dander, and other airway-aggravating allergens. Another trigger to consider banishing from the bed: pets. Fluffy may be none too happy, but if less pet dander yields silent nights, it may be well worth it.
Snoring symptoms
Snoring is often associated with a sleep disorder called obstructive sleep apnea (OSA). Not all snorers have obstructive sleep apnea (OSA), but if snoring is accompanied by any of the following symptoms, it may be an indication to see a doctor for further evaluation for obstructive sleep apnea:
- Witnessed breathing pauses during sleep
- Excessive daytime sleepiness
- Difficulty concentrating
- Morning headaches
- Sore throat upon awakening
- Restless sleep
- Moodiness, irritability or depression
- Gasping or choking at night
- High blood pressure
- Chest pain at night
- Your snoring is so loud it’s disrupting your partner’s sleep
- Frequent need to urinate during the night
- In children, poor attention span, behavioral issues or poor performance in school
Obstructive sleep apnea (OSA) often is characterized by loud snoring followed by periods of silence when breathing stops or nearly stops. Eventually, this reduction or pause in breathing may signal you to wake up, and you may awaken with a loud snort or gasping sound.
You may sleep lightly due to disrupted sleep. This pattern of breathing pauses may be repeated many times during the night.
People with obstructive sleep apnea usually experience periods when breathing slows or stops at least five times during every hour of sleep.
Snoring complications
Habitual snoring may be more than just a nuisance. Aside from disrupting a bed partner’s sleep, if snoring is associated with OSA, you may be at risk for other complications, including:
- Daytime sleepiness
- Frequent frustration or anger
- Difficulty concentrating
- A greater risk of high blood pressure, heart conditions and stroke
- An increased risk of behavior problems, such as aggression or learning problems, in children with OSA
- An increased risk of motor vehicle accidents due to lack of sleep
Snoring diagnosis
To diagnose your condition, your doctor will review your signs and symptoms, and your medical history. Your doctor will also perform a physical examination.
Your doctor may ask your partner some questions about when and how you snore to help assess the severity of the problem. If your child snores, you’ll be asked about the severity of your child’s snoring.
Imaging
Your doctor may request an imaging test, such as an X-ray, a computerized tomography scan or magnetic resonance imaging. These tests check the structure of your airway for problems, such as a deviated septum.
Sleep study
Depending on the severity of your snoring and other symptoms, your doctor may want to conduct a sleep study. Sleep studies may sometimes be done at home.
However, depending upon your other medical problems and other sleep symptoms, you may need to stay overnight at a sleep center to undergo an in-depth analysis of your breathing during sleep by a study, called a polysomnography.
In a polysomnography, you’re connected to many sensors and observed overnight. During the sleep study, the following information is recorded:
- Brain waves
- Blood oxygen level
- Heart rate
- Breathing rate
- Sleep stages
- Eye and leg movements.
How to stop snoring
Treatment for snoring depends on the cause.
Talk to your doctor about the best treatment for you.
- Tongue partially blocking the back of your throat: anti snoring device you wear in your mouth to bring your tongue forward (mandibular advancement device)
- Mouth falling open when you’re asleep: a chin strap for snoring to hold your mouth closed or a device you wear in your mouth to make you breathe through your nose while you sleep (vestibular shield)
- Blocked or narrow airways in your nose: special devices (nasal dilators) or strips that hold your nose open while you sleep, or sprays to reduce swelling inside your nose.
- Snoring mouth guard. An oral appliance is a small plastic device that fits in your mouth over your teeth while you sleep that stops you from snoring. It may resemble a sports mouth guard or an orthodontic retainer. The device prevents the airway from collapsing by holding the tongue in position or by sliding your jaw forward so that you can breathe when you are asleep. A dentist trained in dental sleep medicine can fit you with an oral appliance.
Home remedies for snoring
Simple lifestyle changes can help stop or reduce snoring.
DO
- Lose weight if you’re overweight
- Exercise. Weak muscles around your airway are more likely to collapse while you sleep, triggering snoring. But surprise: Just like regular exercise can tone your arms, legs, and belly, it also tones the muscles of your throat, which can help you stop snoring.
- Sleep on your side – try taping a tennis ball to the back of your sleepwear, or buy a special pillow or bed wedge to help keep you on your side
- Consider asking your partner to use ear plugs if your snoring affects their sleep
- Raise the head of your bed. Raising the head of your bed by about 4 inches may help.
- Nasal strips or an external nasal dilator. Adhesive strips applied to the bridge of the nose help many people increase the area of their nasal passage, enhancing their breathing. A nasal dilator is a stiffened adhesive strip applied externally across the nostrils that may help decrease airflow resistance so you breathe easier. Nasal strips and external nasal dilators aren’t effective for people with OSA, however.
- Treat nasal congestion or obstruction. Having allergies or a deviated septum can limit airflow through your nose. This forces you to breathe through your mouth, increasing the likelihood of snoring. Ask your doctor about a prescription steroid spray if you have chronic congestion. To correct a structural defect in your airway, such as a deviated septum, you may need surgery.
- Limit or avoid alcohol and sedatives. Avoid drinking alcoholic beverages at least two hours before bedtime, and let your doctor know about your snoring before taking sedatives. Sedatives and alcohol depress your central nervous system, causing excessive relaxation of muscles, including the tissues in your throat.
- Quit smoking. Smoking cessation may reduce snoring, in addition to having numerous other health benefits.
- Get enough sleep. Adults should aim for at least seven hours of sleep per night. The recommended hours of sleep for children vary by age. Preschool-aged children should get 10 to 13 hours a day. School-age children need nine to 12 hours a day, and teens should have eight to 10 hours a day.
DON’T
- smoke
- drink too much alcohol
- take sleeping pills – these can sometimes cause snoring.
For snoring accompanied by sleep apnea
For snoring accompanied by OSA, your doctor may suggest:
Oral appliances. Oral appliances are form-fitting dental mouthpieces that help advance the position of your jaw, tongue and soft palate to keep your air passage open.
If you choose to use an oral appliance, you’ll work with your dental specialist to optimize the fit and position of the appliance. You’ll also work with your sleep specialist to make sure the oral appliance is working as intended. Dental visits may be necessary at least once every six months during the first year, and then at least annually after that, to have the fit checked and to assess your oral health.
Excessive salivation, dry mouth, jaw pain and facial discomfort are possible side effects from wearing these devices.
Continuous positive airway pressure (CPAP). This approach involves wearing a mask over your nose or mouth while you sleep. The mask directs pressurized air from a small bedside pump to your airway to keep it open during sleep.
CPAP eliminates snoring and is most often used to treating snoring when associated with OSA.
Although CPAP is the most reliable and effective method of treating OSA, some people find it uncomfortable or have trouble adjusting to the noise or feel of the machine.
Upper airway surgery. There are a number of procedures that seek to open the upper airway and prevent significant narrowing during sleep through a variety of techniques.
For example, in a procedure called uvulopalatopharyngoplasty, you’re given general anesthetics and your surgeon tightens and trims excess tissues from your throat — a type of face-lift for your throat. Another procedure called maxillomandibular advancement involves moving the upper and lower jaws forward, which helps open the airway. Radiofrequency tissue ablation employs a low-intensity radiofrequency signal to shrink tissue in the soft palate, tongue or nose.
A newer surgical technique called hypoglossal nerve stimulation employs a stimulus applied to the nerve that controls forward movement of the tongue so the tongue does not block the airway when you take a breath.
The effectiveness of these surgeries varies and the response can be challenging to predict.
Snoring surgery
Surgery for snoring is a treatment of last resort and should only be considered if the simple non-surgical alternatives have been tried (and failed). Before embarking on palatal surgery you should be sure that the snoring originates from the palate as opposed to the base of the tongue. If you have nasal abnormalities these should also be addressed before contemplating palatal surgery.
The aim of palatal surgery is to reduce or stop the collapsibility of the oropharyngeal segment (area around the throat). This is usually done by reducing the amount of soft palate and/or removing the tonsils. Surgery is also undertaken to remove the chief vibratory tissue (the uvula).
Some surgeons advocate sleep nasendoscopy before surgery is undertaken to determine the level of obstruction. Here the patient is sedated to a state of sleep. The surgeon can then examine the upper airway through a narrow flexible endoscope to see where the collapsing is occurring. This procedure however is not widely available as it is time consuming and costly.
There are four basic surgical procedures:
- Uvulopalatopharyngoplasty
- Laser-assisted uvuloplatoplasty
- Platal stiffening operations
- Radio-frequency ablation (Somnoplasty)
Other procedures include:
- Injection Snoreplasty
- Septoplasty
- Pillar Procedure
The choice of which operation is less important as there are arguments for and against each method. What is more important is that surgery is the right treatment for you.
Some important points that you should remember before undertaking surgery:
- After the operation you will experience pain.
- Surgery for snoring should never be carried out without a prior sleep study.
- Surgery is a treatment of last resort; try everything else first.
- There is no guarantee of success.
- Even if initially successful, snoring can return after a few months.
- Snoring may not be associated with the soft palate at all. It could occur at the base of the tongue. Without full diagnostic procedures it is not possible to differentiate. Surgery will not eradicate tongue based snoring.
- Following a sleep study, surgery should not be considered unless you fit the following criteria: low alcohol intake, non-obese, tonsils still present, and correct jaw shape.
- Even if you do comply with the above, you are advised that there are many short and long term limitations to such procedures.
- If you put on weight after your surgery especially around the neck area you are likely to resume your snoring.
- Remember, you may still go on to develop sleep apnoea in the future especially if you put on weight. Surgery may mask the development of sleep apnea.
- Surgery is not always effective in patients with a deep oropharynx where the side walls tend to collapse towards each other.
- Once you have undergone a surgical procedure it cannot be reversed. You may experience unwanted side effects as a result of the surgery.
- Surgery is very rarely undertaken for the treatment of sleep apnea. Continuous positive airway pressure (CPAP) therapy is the recommended course of treatment for sleep apnea, but it is also effective for snoring if the simple remedies have not worked for you.





{kind=link}