Contents
What is spina bifida
Spina bifida is a neural tube defect. The neural tube is that part of the very young fetus which later develops into the central nervous system and the structures surrounding it. The neural tube comprises the brain and spinal cord, their three layers of lining called the meninges as well as the vertebrae (backbone) and skull. The baby’s brain and spine develop from a neural tube in the first four weeks of pregnancy. Spina bifida is caused when the neural tube does not fully develop, leaving a gap or split in the spine. Spina bifida can affect how your baby’s brain, spine, spinal cord and meninges develop. Meninges are the tissues that cover and protect the brain and the spinal cord. Most neural tube defects can be prevented by taking folic acid before and after conception.
The total incidence of neural tube defects is approximately 1 in 700 live births in Caucasian people. The incidence amongst African-Americans is less than 1 in 3000 live births. There is no particular predominance for male or female newborns.
Spina bifida can range from mild to severe, depending on the type of defect, size, location and complications. When early treatment for spina bifida is necessary, it’s done surgically, although such treatment doesn’t always completely resolve the problem.
Figure 1. Neural tube development
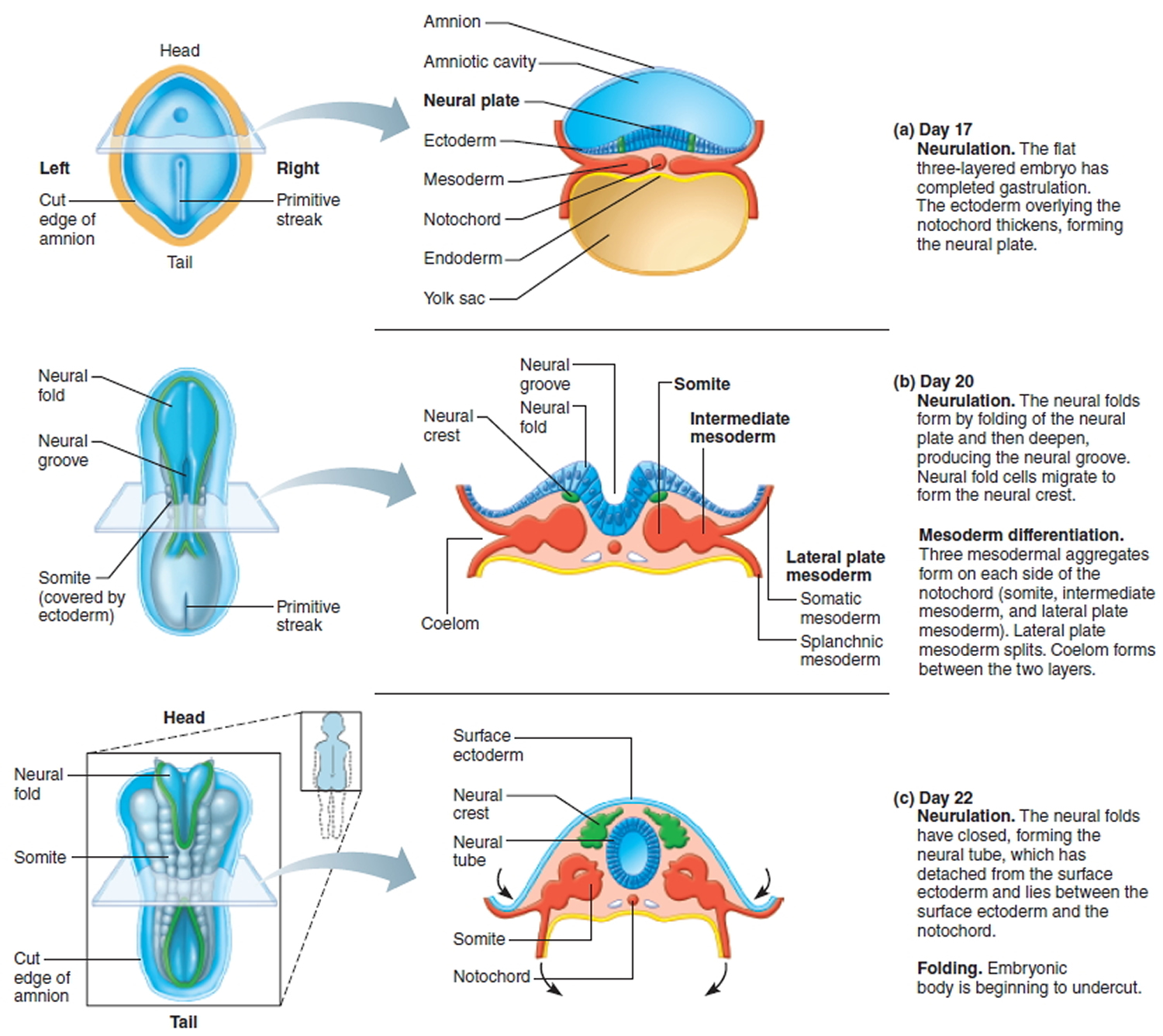
Around the third week of pregnancy a flat sheet of cells called the neural plate starts to change shape and forms a groove. The process continues until a tube is formed. This tube is called the neural tube. If the process does not complete and an opening is left somewhere along the length of the neural tube then the result is what is called a neural tube defect. If the opening is in the top part of the tube which later forms the brain and skull, the defect is called anencephaly and it is always fatal.
If the opening is in the bottom part of the tube the defect is spina bifida. Because the bottom part of the neural tube develops into the spinal cord, meninges (linings) and vertebrae, any or all of these structures can be involved in the spina bifida.
Risk Factors
- Maternal folic acid deficiency has a strong correlation with neural tube defects.
- Maternal use of valproate in the 1st trimester may be associated with spina bifida, however the risk of epilepsy in pregnancy outweighs not using medication in most cases.
- Previous children with spina bifida is associated with an increased risk of spia bifida – this suggests there may be some genetic component to this disease (in the absence of ongoing environmental factors).
- It should be noted that over ninety percent of cases of spina bifida, the pregnancy is classified ‘low risk’.
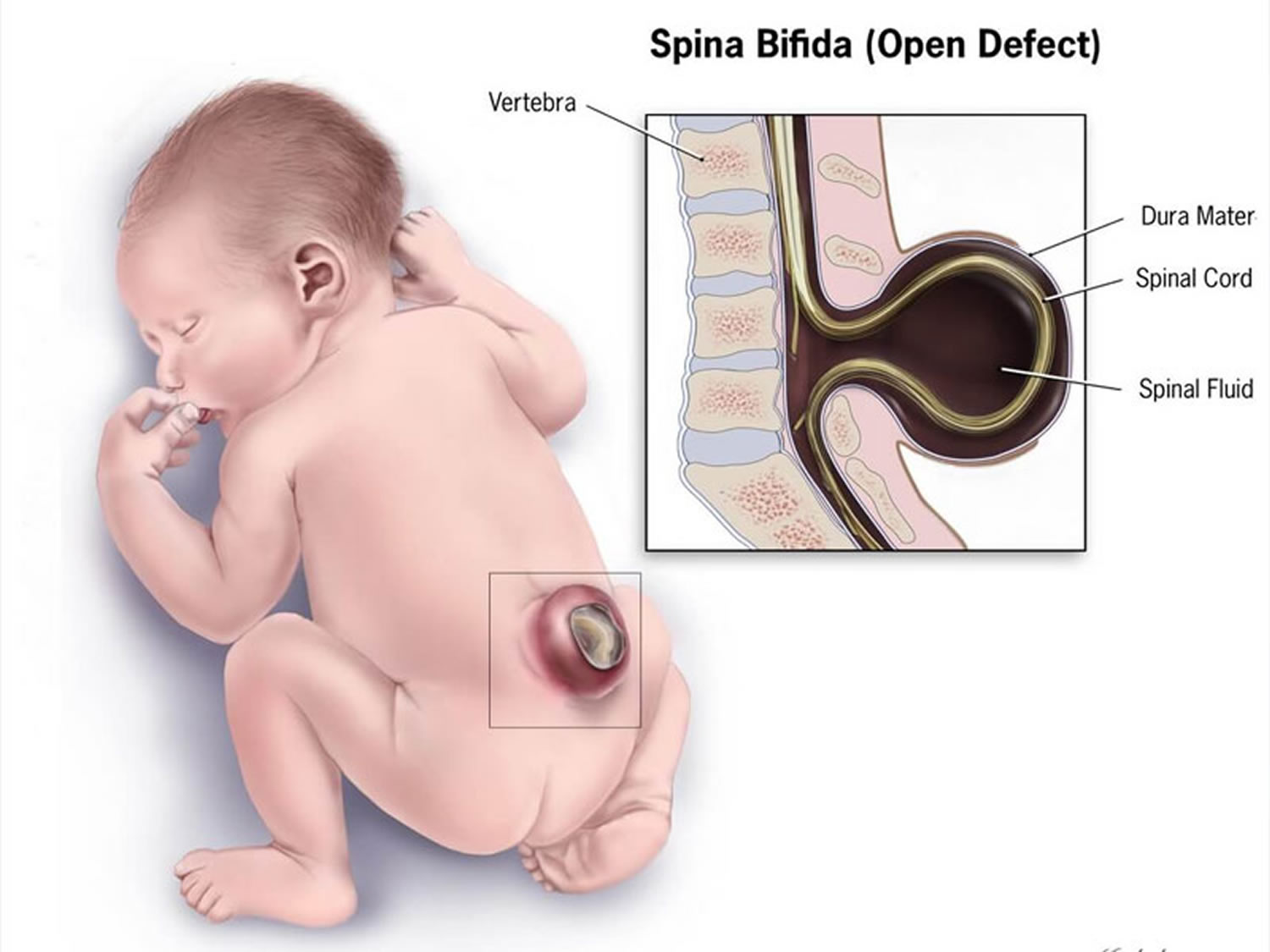
Where the spinal cord and meninges (linings) protrude into a sac on the back which is exposed, it is called meningomyelocele or sometimes myelomeningocoele.
Where the meninges, but not the spinal cord, protrude through the opening in the vertebrae into an exposed sac, the condition is called meningocele. The sac is exposed (not covered by skin) when the baby is born so these forms of spina bifida are very obvious at birth. They are also usually detected by ultrasound when scans are taken in the 18th week of pregnancy.
Where there is no exposed sac and the lesion is covered by skin the condition is called spina bifida occulta. The spinal cord and meninges are usually not affected. However the skin may show some unusual signs of underlying problems and this will be discussed later. Spina bifida occulta almost always occurs at the bottom of the spine – in the lumbar or sacral area.
Spina bifida can result in varying degrees of paralysis, loss of sensation, incontinence, spine and limb problems and in some cases cognitive impairment. However it should be noted that more than eighty percent of patients with spina bifida have a normal intelligence.
Early problems that may occur predominantly involve infection at the source of the lesion. The infection may spread to the central nervous system if left untreated. The spinal cord may also tether causing further neurological deterioration. Treatment may involve surgery, but it depends on the severity of the condition.
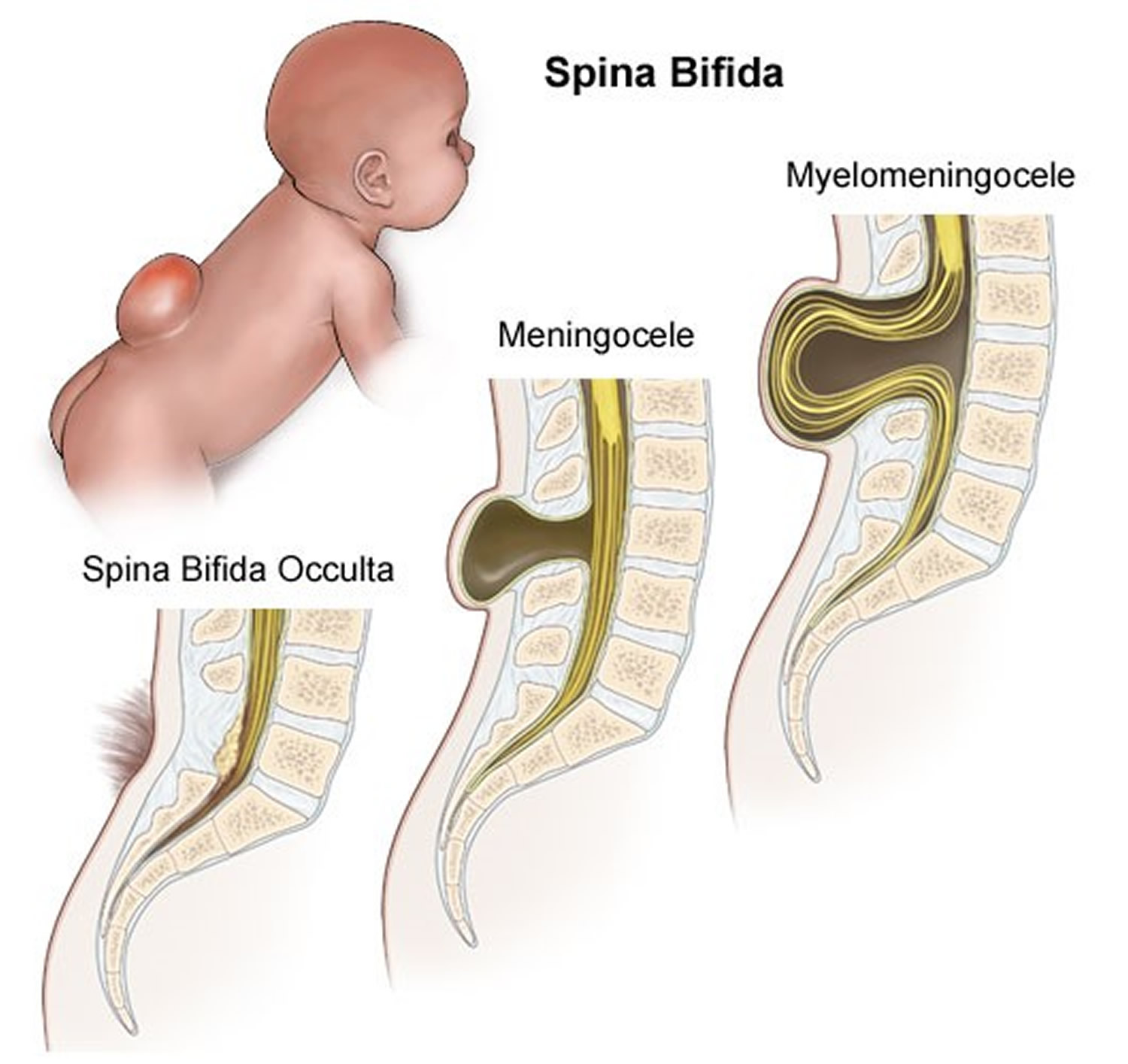
Figure 2. Spina bifida
 Spina bifida types
Spina bifida types
Spina bifida can occur in different forms:
- spina bifida occulta,
- meningocele
- myelomeningocele (spina bifida cystica).
The severity of spina bifida depends on the type, size, location and complications.
Spina bifida occulta
The term spina bifida occulta covers two different conditions and this can be very confusing. One of them is relatively harmless and common – an anatomical anomaly rather than a medical condition. The other condition is much less common but it can cause significant problems. It is similar to a mild form of spina bifida.
Spina bifida is Latin for split spine and occulta means hidden. So spina bifida occulta is a split in the spine hidden by skin. What this means is that at least one vertebra is malformed or has not developed fully. Nobody knows for sure but it is assumed that spina bifida occulta develops in a similar way to spina bifida.
Spina bifida occulta – the common form
Spina bifida occulta where the spinal cord or meninges are not involved is quite common. A few recent medical studies show that about 22% of people have spina bifida occulta. In this form of spina bifida occulta it is usually only one vertebra which has not formed completely and the opening is usually very narrow.
In theory, because the spinal cord and meninges are not involved in any way, this form of spina bifida should cause no problems. However, there is some medical evidence that older children with urinary problems and adults with spondylolysis are over-represented in the group of people with this type of spina bifida occulta. Spondyloysis is a crack or stress fracture of the back part of one of the vertebra and it is reasonably common.
The association between spina bifida occulta and these conditions does not necessarily mean that the spina bifida occulta causes urinary problems or spondylolysis. It might mean that some of the things which caused the neural tube to not close fully have also caused other things to happen and these have led to the other conditions. This is one of the areas regarding spina bifida occulta that medical research has yet to provide an answer.
Spina bifida occulta – a mild spina bifida type
This type of spina bifida occulta is sometimes called occult spinal dysraphism or closed spina bifida. For clarity, this type will be referred to as occult spinal dysraphism from this point on.
Occult spinal dysraphism differs from the common type of spina bifida occulta in that the spinal nerves and or meninges are mixed up in some way with their surrounding structures and this involvement causes complications. Unfortunately, it is not always easy to say with any certainty which type a person has. There seems to be a range of lesions with very obvious cases of harmless spina bifida occulta at one end and very obvious cases of occult spinal dysraphism at the other and a grey area in the middle. While MRI technology has gone a long way to shed light on what is happening at the site, it seems that there are a number of people with no apparent involvement of nerve tissue who do have complications.
While spina bifida occulta is very common, there are much fewer people who have occult spinal dysraphism. Estimations of the incidence vary from 1 in 250 to 1 in 5,000 of the general population. However, these figures may change as medical technology improves and the ability to detect what is happening at the lesion site improves. The condition may also be undiagnosed in many people. The incidence of occult spinal dysraphism may be found to be similar to the incidence of spina bifida in the way that it varies from one geographic area to another and from one racial group to another. It is usually just one vertebra that is involved with the common spina bifida occulta and if there are more involved then the diagnosis is more likely to be occult spinal dysraphism. Apart from the size of the defect and the number of vertebrae involved, there can be some telltale signs on the skin which are visible at birth which might give a clue that something unusual is going on underneath.
Spina bifida is caused by both environmental and genetic factors. Even though 9 out of 10 children with spina bifida are born to parents with no family history of spina bifida, there is a higher risk of a pregnancy being affected by a neural tube defect (anencephaly or spina bifida) where there is a family history. The risk is higher when the family relationship is closer. The same seems to be true for occult spinal dysraphism.
In a family where one child has some form of occult spinal dysraphism, any future children seem to have a similar risk (3.5%) of developing a neural tube defect. It is not clear whether the risk is only for occult spinal dysraphism or any type of neural tube defect.
As many as 80% of people with occult spinal dysraphism have at least one of these outward signs or herald marks. The signs include:
- A hairy patch in the middle of the lower back
- A fatty lump over the bottom of the spine
- A stork bite or hemangioma (a reddish or purple spot) on the skin
- A dimple or sinus (hole) above the level of the crease in the buttocks (Dimples below the level of the crease are common in newborns and are usually no cause for alarm)
- A pigmented area or birthmark over the bottom of the spine.
- A small tail
Occult spinal dysraphism can be very complex because it is not just one condition. It represents a number of conditions which can occur separately or in combination. Some of these conditions are:
- A tethered spinal cord where the lower end of the spinal cord is stuck or attached to surrounding bone or other structures. The spinal cord is usually free (to some extent) to move up and down within the spinal canal.
- A lipoma which is a fatty lump whose tissues are often interwoven with those of the spinal cord, making them very difficult to separate. Lipomas can also tether the spinal cord.
- Diastematomyelia where the spinal cord is split in two usually by a piece of abnormal bone or cartilage. This can also tether the spinal cord.
- A dermal sinus which is a connection between the spinal canal and the skin of the back.
All of these conditions can affect the functioning of the spinal cord i.e. its ability to send messages to and from the brain. The cord can become stretched which causes pain and the blood supply to the cells in the spinal cord can be affected with the result that the nerves lose their ability to function properly.
Complications of occult spinal dysraphism
Not everyone with occult spinal dysraphism will have complications. Sometimes the onset of signs and symptoms will be so gradual that they may not appear until adulthood. For most though, there will be some indications early in the person’s life that the nerves in the spine are not working as they should.
Some of these are:
- Foot deformity
- Weakness in the legs
- Reduced feeling or numbness in the legs or feet
- Back or leg pain
- Bladder infections
- Bladder incontinence
- Constipation
- Scoliosis or other orthopedic deformities.
All of these symptoms can be caused by conditions other than occult spinal dysraphism so it is important to see your doctor for thorough testing and an accurate diagnosis.
It is especially important to seek medical advice where the symptoms are progressing or getting worse. These changes may indicate that the spinal cord is tethered and an operation to untether the cord might be required.
Prevention
It has been known for a few decades that folic acid (vitamin B-9) when taken for a month prior to conception and for 3 months afterwards can reduce the risk of the baby developing a neural tube defect by up to 70%. For women with no family history of a neural tube defect the recommended dose is 600 micrograms (600 mcg) a day. For women with a family history, including them or their partner, the recommended dose is 4 milligrams a day.
Folic acid (called folate in its natural form) is available naturally in leafy green vegetables and some other foods. The levels consumed naturally do not always reach the recommended level for lowering the risk of a neural tube defect in affected pregnancy, so it is important for women of child bearing age to take a daily folic acid supplement. Because about half of all pregnancies in the US are unplanned, the recommendation is for all women of child bearing age to supplement their diet with a folic acid tablet.
Medical treatment
If is felt that medical intervention is required then treatment may involve untethering of the spinal cord. This procedure is performed by a neurosurgeon. Because of the way that the nerves are arranged in the lower spinal cord, it is very complex surgery and there is always a risk that some nerves or the spinal cord itself may be damaged. Because of this risk and the fact that there is no guarantee that the operation will be successful in removing the symptoms or even reducing them, many neurosurgeons will wait until the symptoms become relatively serious before operating. On the other hand some neurosurgeons will operate early to try to prevent symptoms from progressing. At the moment there does not seem to be any clear evidence that one approach is better than the other.
Depending on the type or severity of complications, it may be necessary to be treated by another specialist such as a urologist or orthopedic surgeon.
The procedure to untether the spinal cord creates scar tissue at the site which increases the risk for further tethering. There are a number of ways neurosurgeons try to avoid this, but it is a complicating factor that you and your neurosurgeon must take into consideration.
Meningocele
This is the rarest form of spina bifida. In this form of spina bifida called meningocele, the protective membranes around the spinal cord (meninges) push out through the opening in the vertebrae, forming a sac filled with fluid. But this sac doesn’t include the spinal cord, so nerve damage is less likely, but some babies may have problems controlling their bladder and bowels and later complications are possible. Surgery can remove the meningocele.
Spina bifida cystica
This is the most severe and the most common form of spina bifida. Spina bifida cystica also known as myelomeningocele or open spina bifida, is the most severe form of spina bifida and it refers to the meninges and spinal cord protruding through a cleft. The spinal cord is usually damaged and has not developed properly. The spinal canal is open along several vertebrae in the lower or middle back. The membranes and spinal nerves push through this opening at birth, forming a sac on the baby’s back, typically exposing tissues and nerves. This makes the baby prone to life-threatening infections. This is usually associated with paralysis and loss of sensation below the level of the lesion. Babies with this condition need surgery before birth or within the first few days of life. During surgery, a surgeon tucks the spinal cord and nerves back into the spine and covers them with muscle and skin. This can help prevent new nerve damage and infection. But the surgery can’t undo any damage that’s already happened. Even with surgery, babies with this condition have lasting disabilities, like problems walking and going to the bathroom.
Figure 3. Spina bifida cystica

Spina bifida Complications
Spina bifida may cause minimal symptoms or only minor physical disabilities. If the spina bifida is severe, sometimes it leads to more significant physical disabilities. Severity is affected by:
- The size and location of the neural tube defect
- Whether skin covers the affected area
- Which spinal nerves come out of the affected area of the spinal cord
This list of possible complications may seem overwhelming, but not all children with spina bifida get all these complications. And these conditions can be treated.
- Walking and mobility problems. The nerves that control the leg muscles don’t work properly below the area of the spina bifida defect, causing muscle weakness of the legs, sometimes involving paralysis. Whether a child can walk typically depends on where the defect is, its size, and the care received before and after birth.
- Paralysis. People with spina bifida higher on the spine may have paralyzed legs or feet and need to use wheelchairs. Those with spina bifida lower on the spine (near the hips) may have more use of their legs. They may be able to walk on their own or use crutches, braces or walkers to help them walk. Some babies can start exercises for the legs and feet at an early age to help them walk with braces or crutches when they get older.
- Orthopedic complications. Children with myelomeningocele can have a variety of problems in the legs and spine because of weak muscles in the legs and back. The types of problems depend on the level of the defect. Possible problems include a curved spine (scoliosis), abnormal growth or dislocation of the hip, bone and joint deformities, muscle contractures and other orthopedic concerns.
- Bowel and bladder problems. Nerves that supply the bladder and bowels usually don’t work properly when children have myelomeningocele. This is because the nerves that supply the bowel and bladder come from the lowest level of the spinal cord.
- Accumulation of fluid in the brain (hydrocephalus). Babies born with myelomeningocele commonly experience accumulation of fluid in the brain, a condition known as hydrocephalus. Extra fluid can cause the head to swell and put pressure on the brain. Hydrocephalus can cause intellectual and developmental disabilities. These are problems with how the brain works that can cause a person to have trouble or delays in physical development, learning, communicating, taking care of himself or getting along with others. In some cases, a surgeon needs to drain the extra fluid from a baby’s brain.
- Shunt malfunction. Shunts can stop working or become infected. Warning signs may vary. Some of the warning signs of a shunt that isn’t working include headaches, vomiting, sleepiness, irritability, swelling or redness along the shunt, confusion, changes in the eyes (fixed downward gaze), trouble feeding, or seizures.
- Chiari malformation type II. Chiari malformation type II is a common brain abnormality in children with the myelomeningocele form of spina bifida. The brainstem, or lowest part of the brain above the spinal cord, is elongated and positioned lower than usual. This can cause problems with breathing and swallowing. Rarely, compression on this area of the brain occurs and surgery is needed to relieve the pressure.
- Infection in the tissues surrounding the brain (meningitis). Some babies with myelomeningocele may develop meningitis, an infection in the tissues surrounding the brain. This potentially life-threatening infection may cause brain injury.
- Tethered spinal cord. Tethered spinal cord results when the spinal nerves become bound to the scar where the defect was closed surgically, making the spinal cord less able to grow as the child grows. This progressive tethering can cause loss of muscle function to the legs, bowel or bladder. Surgery can limit the degree of disability.
- Sleep-disordered breathing. Both children and adults with spina bifida, particularly myelomeningocele, may have sleep apnea or other sleep disorders. Assessment for a sleep disorder in those with myelomeningocele helps detect sleep-disordered breathing, such as sleep apnea, which warrants treatment to improve health and quality of life.
- Skin problems. Children with spina bifida may get wounds on their feet, legs, buttocks or back. They can’t feel when they get a blister or sore. Sores or blisters can turn into deep wounds or foot infections that are hard to treat. Children with myelomeningocele have a higher risk of wound problems in casts.
- Latex allergy. Children with spina bifida have a higher risk of latex allergy, an allergic reaction to natural rubber or latex products. Latex allergy may cause rash, sneezing, itching, watery eyes and a runny nose. It can also cause anaphylaxis, a potentially life-threatening condition in which swelling of the face and airways can make breathing difficult. So it’s best to use latex-free gloves and equipment at delivery time and when caring for a child with spina bifida.
- Other complications. More problems may arise as children with spina bifida get older, such as urinary tract infections, gastrointestinal (GI) disorders and depression. Children with myelomeningocele may develop learning disabilities, such as problems paying attention, and difficulty learning reading and math.
- Skin problems. People with spina bifida can develop sores, calluses, blisters and burns on their feet, ankles and hips. But they may not know they have these problems because they may not be able to feel certain parts of their body. Your baby’s provider can recommend ways to help prevent skin problems.
- Tethered spinal cord. This condition happens when the spinal cord is held tightly in place, causing the cord to stretch as your baby grows. The stretching can cause nerve damage in the spine. Babies with tethered spinal cord may have problems like back pain and a curved spine (also called scoliosis). Tethered spinal cord can be treated with surgery. This condition affects babies with myelomeningocele, meningocele and spina bifida occulta.
- Urinary tract infections (also called UTIs). The urinary tract is the system of organs (including the kidneys and bladder) that helps your body get rid of waste and extra fluids in the urine. Babies with spina bifida often can’t control when they go to the bathroom because the nerves that help a baby’s bladder and bowels work are damaged. If your baby has problems emptying the bladder completely, this can cause UTIs and kidney problems. Your baby’s health care provider can teach you how to use a plastic tube called a catheter to empty your baby’s bladder.
- Other conditions. Some people with spina bifida have problems with:
- Obesity (being very overweight)
- Digestion, the process of how your body breaks down food after you eat it
- Having sex
- Social and emotional conditions, including depression
- Vision
Spina bifida life expectancy
There is no cure for spina bifida. The prognosis of spina bifida has greatly improved thanks to advances in multidiscplinary care. Depending on the degree of disability, including paralysis, incontinence and the loss of sensation, spina bifida can be effectively managed in many cases.
Spina bifida in adults
- Many adults living with Spina Bifida lead happy, productive and independent lives. There are just a few things that need attention.
- Find a good doctor that you can talk to. Link in to a Spina Bifida Service or Rehabilitation Specialist. The Spina Bifida Adult Resource team are a great resource in the community for people over 18. You can self-refer to them at Northcott. Try to have an annual review to stay ahead of any issues related to your Spina Bifida.
- Monitor your mobility. Be open to changing your mobility equipment to support your body, this may mean that you are able to be more independent for longer.
- See medical specialists urgently if you experience worsening spasms or loss of strength in legs or arms, and it is affecting your ability to walk or transfer.
- Check your skin but in particular your feet and bottom daily. Use a pressure cushion and wear shoes. If you develop pressure injuries or swelling on the legs see your doctor and follow up with your rehabilitation specialist. You should attend daily to self-skin checks and take good care with your hygiene. Use a podiatrist for managing your foot care.
- If you have orthoses remember to check them on a daily basis. They should be reviewed by an orthotist at least once a year. They need to be cleaned regularly & inspected for any signs of wear & tear. Although rare, sometimes the plastic or componentry of the orthoses may break and this could result in a fall. If ill fitting, they could contribute to pressure injury also.
- Have a renal ultrasound every year. Keep up your clean intermittent self-catheterisation program. You might require repeat urodynamic testing and a cystoscopy if you have had an indwelling catheter for more than 15 years. The frequency of testing will be decided by your treating urologist.
- Eat a balanced diet with sufficient fibre (eg. cereals, grain, fruit & vegetables). Remember that you will gain weight more easily so dietary advice may be necessary if you are gaining weight. Exercise regularly to maintain a healthy body weight.
- Ensure you have a regular shunt review by either a neurosurgeon or the Spina Bifida Service.
- Minimise alcohol consumption, recreational drugs and don’t smoke cigarettes.
- Know the reason why you are taking different medications and keep track of any changes.
- For women, be aware of the normal look and feel of your breast and see your doctor immediately if you notice any new or unusual changes.
- Women over 18 need second yearly pap smear and gynaecological review. Men need regular prostate cancer and related screening. It is important not to neglect aspects of your sexual health.
- Important general health reviews as you age include blood pressure and cholesterol checks, eye tests and blood sugar tests.
- It is important to have regular 6 monthly or 12 monthly dental reviews. In between dental visits good oral hygiene practices need to be maintained.
- Try to find social activities that you enjoy. Get out and about and have lots of fun.
Things to remember:
- Living well with Spina Bifida includes weight control, exercise, regular health and equipment reviews and vigilance to any warning symptoms.
- Know your body and be proactive in managing any changes.
- Make sure you tell new health care professionals about any allergies you may have.
- Use services and supports available to you to maintain your independence.
- Review your equipment on a daily basis. Remember to clean your equipment and keep up with maintenance needs.
Spina bifida causes
What causes spina bifida
Doctors aren’t certain what causes spina bifida. As with many other problems, it appears to result from a combination of genetic and environmental risk factors, such as a family history of neural tube defects and folate deficiency.
Risk factors for spina bifida
Spina bifida is more common among whites and Hispanics, and females are affected more often than males. Although doctors and researchers don’t know for sure why spina bifida occurs, they have identified some risk factors:
- Folate deficiency. Folate (vitamin B-9) is important to the healthy development of a baby. Folate is the natural form of vitamin B-9. The synthetic form, found in supplements and fortified foods, is called folic acid. A folate deficiency increases the risk of spina bifida and other neural tube defects. During pregnancy, take a prenatal vitamin each day that has 600 micrograms of folic acid in it.
- Family history of neural tube defects. Couples who’ve had one child with a neural tube defect have a slightly higher chance of having another baby with the same defect. That risk increases if two previous children have been affected by the condition. In addition, a woman who was born with a neural tube defect has a greater chance of giving birth to a child with spina bifida. However, most babies with spina bifida are born to parents with no known family history of the condition.
- You may be more likely than others to have a baby with spina bifida if:
- You or your partner has spina bifida. When one parent has spina bifida, there’s a 1 in 25 (4 percent) chance of passing spina bifida to your baby.
- You already have a child with spina bifida. In this case, there’s a 1 in 25 (4 percent) chance of having another baby with spina bifida.
- In these cases, you may want to see a genetic counselor. This is a person who is trained to help you understand how genes, birth defects and other medical conditions run in families, and how they can affect your health and your baby’s health. In most cases, spina bifida happens without any family history of the condition. This means no one in your family or your partner’s family has spina bifida.
- You may be more likely than others to have a baby with spina bifida if:
- Some medications. For example, anti-seizure medications, such as valproic acid (Depakene) and and carbamazepine, seem to cause neural tube defects when taken during pregnancy, possibly because they interfere with the body’s ability to use folate and folic acid. Doctors will try to avoid prescribing these medications if there’s a chance you could get pregnant while taking them, but they may be needed if the alternatives aren’t effective. It’s advisable to use a reliable form of contraception if you need to take one of these medications and aren’t trying to get pregnant. Tell your doctor if you’re thinking about trying for a baby and you need to take one of these medications. They may be able to lower the dose and prescribe folic acid supplements at a higher than normal dose, to reduce the risk of problems.
- Diabetes. Women with diabetes who don’t control their blood sugar well have a higher risk of having a baby with spina bifida.
- Obesity. Pre-pregnancy obesity is associated with an increased risk of neural tube birth defects, including spina bifida.
- Increased body temperature. Some evidence suggests that increased body temperature (hyperthermia) in the early weeks of pregnancy may increase the risk of spina bifida. Elevating your core body temperature, due to fever or the use of saunas or hot tubs, has been associated with a possible slight increased risk of spina bifida. If you have a fever, take acetaminophen (Tylenol®) right away and call your provider.
- Genetic conditions: Very rarely, spina bifida can occur alongside a genetic condition such as Patau’s syndrome, Edwards’ syndrome or Down’s syndrome. If your baby is found to have spina bifida and it’s thought they may also have one of these syndromes, you’ll be offered a diagnostic test, such as amniocentesis or chorionic villus sampling that can tell for certain if your baby has one of these genetic conditions.
If you have known risk factors for spina bifida, talk with your doctor to determine if you need a larger dose or prescription dose of folic acid, even before a pregnancy begins.
If you take medications, tell your doctor. Some medications can be adjusted to diminish the potential risk of spina bifida, if plans are made ahead of time.
Spina bifida prevention
Folic acid, taken in supplement form starting at least one month before conception and continuing through the first trimester of pregnancy, greatly reduces the risk of spina bifida and other neural tube defects.
Due to folic acid role in the synthesis of DNA and other critical cell components, folate is especially important during phases of rapid cell growth 1. Clear clinical trial evidence shows that when women take folic acid periconceptionally, a substantial proportion of neural tube defects is prevented 2. Scientists estimate that periconceptional folic acid use could reduce neural tube defects by 50% to 60% 3.
Since 1998, when the mandatory folic acid fortification program took effect in the United States, neural tube defect rates have declined by 25% to 30% 3. However, significant racial and ethnic disparities exist. Spina bifida and anencephaly rates have declined significantly among Hispanic and non-Hispanic white births in the United States, but not among non-Hispanic black births 4. Differences in dietary habits and supplement-taking practices could be a factor in these disparities 4. In addition, factors other than folate status—such as maternal diabetes, obesity, and intake of other nutrients such as vitamin B12—are believed to affect the risk of neural tube defects 5.
Because approximately 50% of pregnancies in the United States are unplanned, adequate folate status is especially important during the periconceptual period before a woman might be aware that she is pregnant. The Food and Nutrition Board at the Institute of Medicine advises women capable of becoming pregnant to “consume 400 mcg of folate daily from supplements, fortified foods, or both in addition to consuming food folate from a varied diet”6. The U.S. Public Health Service and the Centers for Disease Control and Prevention have published similar recommendations 7.
The Food and Nutrition Board at the Institute of Medicine has not issued recommendations for women who have had a previous neural tube defect and are planning to become pregnant again. However, other experts recommend that women obtain 4,000 to 5,000 mcg (4 – 5 mg) supplemental folic acid daily starting at least 1 to 3 months prior to conception and continuing for 2½ to 3 months after conception 8. These doses exceed the Tolerable Upper Intake Level (maximum daily intake unlikely to cause adverse health effects) and should be taken only under the supervision of a physician 9.
Get folic acid first
It’s critical to have enough folic acid in your system by the early weeks of pregnancy to prevent spina bifida. Because many women don’t discover that they’re pregnant until this time, experts recommend that all women of childbearing age take a daily supplement of folic acid. During pregnancy, demands for folate increase due to its role in nucleic acid synthesis 10. To accommodate this need, the Food and Nutrition Board at the Institute of Medicine increased the folate Recommended Dietary Allowance (RDA) from 400 mcg/day for nonpregnant women to 600 mcg/day during pregnancy 6. This level of intake might be difficult for many women to achieve through diet alone. The American College of Obstetricians and Gynecologists recommends a prenatal vitamin supplement for most pregnant women to ensure that they obtain adequate amounts of folic acid and other nutrients 11.
Several foods, including enriched bread, pasta, rice and some breakfast cereals, are fortified with 400 mcg of folic acid per serving. Folic acid may be listed on food packages as folate, which is the natural form of folic acid found in foods.
Planning pregnancy
If you’re actively trying to conceive, most pregnancy experts believe supplementation of at least 400 mcg of folic acid a day is the best approach for women planning pregnancy.
Your body doesn’t absorb folate as easily as it absorbs synthetic folic acid, and most people don’t get the recommended amount of folate through diet alone, so vitamin supplements are necessary to prevent spina bifida. And, it’s possible that folic acid will also help reduce the risk of other birth defects, including cleft lip, cleft palate and some congenital heart defects.
It’s also a good idea to eat a healthy diet, including foods rich in folate or enriched with folic acid. This vitamin is present naturally in many foods, including:
- Beans
- Citrus fruits and juices
- Egg yolks
- Dark green vegetables, such as broccoli and spinach
When higher doses are needed
If you have spina bifida or if you’ve given birth to a child with spina bifida, you’ll need extra folic acid before you become pregnant. If you’re taking anti-seizure medications or you have diabetes, you may also benefit from a higher dose of this B-9 vitamin. But check with your doctor before taking additional folic acid supplements.
Spina bifida symptoms
Signs and symptoms of spina bifida vary by type and severity. Symptoms can also differ for each person.
Spina bifida can cause a wide range of symptoms, including problems with movement, bladder and bowel problems, and problems associated with hydrocephalus (excess fluid on the brain).
The severity of the symptoms of spina bifida varies considerably, largely depending on the location of the gap in the spine.
A gap higher up the spine is more likely to cause paralysis of the legs and mobility difficulties compared with gaps in the middle or at the base of the spine, which may only cause continence issues.
A baby is more likely to have learning difficulties if they develop hydrocephalus.
- Spina bifida occulta. Because the spinal nerves usually aren’t involved, typically there are no signs or symptoms. But visible indications can sometimes be seen on the newborn’s skin above the spinal defect, including an abnormal tuft of hair, or a small dimple or birthmark.
- Meningocele. The membranes around the spinal cord push out through an opening in the vertebrae, forming a sac filled with fluid, but this sac doesn’t include the spinal cord.
- Myelomeningocele (spina bifida cystica). In this severe form of spina bifida:
- The spinal canal remains open along several vertebrae in the lower or middle back.
- Both the membranes and the spinal cord or nerves protrude at birth, forming a sac.
- Tissues and nerves usually are exposed, though sometimes skin covers the sac.
Spina bifida cystica (myelomeningocele) symptoms
Movement problems
The brain controls all the muscles in the body with the nerves that run through the spinal cord. Any damage to the nerves can result in problems controlling the muscles.
Most children with spina bifida have some degree of weakness or paralysis in their lower limbs. They may need to use ankle supports or crutches to help them move around. If they have severe paralysis, they’ll need a wheelchair.
Paralysis can also cause other, associated problems. For example, as the muscles in the legs aren’t being used regularly, they can become very weak.
As the muscles support the bones, muscle weakness can affect bone development. This can cause dislocated or deformed joints, bone fractures, misshapen bones and an abnormal curvature of the spine (scoliosis).
Bladder problems
Many people with spina bifida have problems storing and passing urine. This is caused by the nerves that control the bladder not forming properly. It can lead to problems such as:
- urinary incontinence
- urinary tract infections (UTIs)
- hydronephrosis – where one or both kidneys become stretched and swollen due to a build-up of urine inside them
- kidney scarring
- kidney stones
Due to the risk of infection, the bladder and kidneys will need to be regularly monitored. Ultrasound scans may be needed, as well as tests to measure the bladder’s volume and the pressure inside it.
Bowel problems
The nerves that run through the spinal cord also control the bowel and the sphincter muscles that keep stools in the bowel.
Many people with spina bifida have limited or no control over their sphincter muscles and have bowel incontinence.
Bowel incontinence often leads to periods of constipation followed by episodes of diarrhoea or soiling.
Hydrocephalus
Some babies with spina bifida have hydrocephalus (excess fluid on the brain), which can damage the brain and cause further problems.
Many people with spina bifida and hydrocephalus will have normal intelligence, although some will have learning difficulties, such as:
- a short attention span
- difficulty solving problems
- difficulty reading
- difficulty understanding some spoken language – particularly fast conversations between a group of people
- difficulty organising activities or making detailed plans
They may also have problems with visual and physical co-ordination – for example, tasks such as tying shoelaces or fastening buttons.
Some babies have a problem where the lower parts of the brain are pushed downwards towards the spinal cord. This is known as type 2 Arnold-Chiari malformation and is linked to hydrocephalus.
Hydrocephalus can cause additional symptoms soon after birth, such as irritability, seizures, drowsiness, vomiting and poor feeding.
Other problems
Other problems associated with spina bifida include:
- skin problems – reduced sensation can make it difficult to tell when the skin on the legs has been damaged – for example, if the skin gets burnt on a radiator; if a person with spina bifida injures their legs without realising, the skin could become infected or an ulcer could develop; it’s important to check the skin regularly for signs of injury
- latex allergy – people with spina bifida can develop an allergy to latex; symptoms can range from a mild allergic reaction – watery eyes and skin rashes – to a severe allergic reaction, known as anaphylactic shock, which requires an immediate injection of adrenalin; tell medical staff if you or your child is allergic to latex
Spina bifida diagnosis
Spina bifida can be diagnosed during pregnancy or after your baby is born. Spina bifida occulta may not be diagnosed until later in life.
If you’re pregnant, you’ll be offered prenatal screening tests to check for spina bifida and other birth defects. The tests aren’t perfect. Some mothers who have positive blood tests have normal babies. Even if the results are negative, there’s still a small chance that spina bifida is present. Talk to your doctor about prenatal testing, its risks and how you might handle the results.
Blood tests
Your doctor will most likely check for spina bifida by first performing these tests:
- Maternal serum alpha-fetoprotein (MSAFP) test. For the maternal serum alpha-fetoprotein test, a sample of the mother’s blood is drawn and tested for alpha-fetoprotein (AFP) — a protein produced by the baby. The test is done at 15 to 20 weeks of pregnancy. It’s normal for a small amount of AFP to cross the placenta and enter the mother’s bloodstream. But abnormally high levels of AFP suggest that the baby has a neural tube defect, such as spina bifida, though some spina bifida cases don’t produce high levels of AFP.
- Test to confirm high AFP levels. Varying levels of AFP can be caused by other factors — including a miscalculation in fetal age or multiple babies — so your doctor may order a follow-up blood test for confirmation. If the results are still high, you’ll need further evaluation, including an ultrasound exam.
- Other blood tests. Your doctor may perform the maternal serum alpha-fetoprotein test with two or three other blood tests. These tests are commonly done with the maternal serum alpha-fetoprotein test, but their objective is to screen for other abnormalities, such as trisomy 21 (Down syndrome), not neural tube defects.
Ultrasound
Many obstetricians rely on ultrasonography to screen for spina bifida. If blood tests indicate high AFP levels, your doctor will suggest an ultrasound exam to help determine why. The most common ultrasound exams bounce high-frequency sound waves off tissues in your body to form images on a video monitor.
The information these images provide can help establish whether there’s more than one baby and can help confirm gestational age, two factors that can affect AFP levels. An advanced ultrasound also can detect signs of spina bifida, such as an open spine or particular features in your baby’s brain that indicate spina bifida.
Amniocentesis
If a blood test shows high levels of AFP in your blood but the ultrasound is normal, your doctor may offer amniocentesis. During amniocentesis, your doctor uses a needle to remove a sample of fluid from the amniotic sac that surrounds the baby.
An analysis of the sample indicates the level of AFP present in the amniotic fluid. A small amount of AFP is normally found in amniotic fluid. However, when an open neural tube defect is present, the amniotic fluid contains an elevated amount of AFP because the skin surrounding the baby’s spine is gone and AFP leaks into the amniotic sac.
Discuss the risks of amniocentesis, including a slight risk of loss of the pregnancy, with your doctor.
After your baby is born
In some cases, providers diagnose a baby’s spina bifida after birth. A hairy patch of skin or a dimple on your baby’s back may be the first sign of spina bifida. If your provider thinks your baby has spina bifida, she may use one of these tests to get a clearer view of your baby’s spine:
- Computed tomography (also called CT or CAT scan). CT scans use special X-ray equipment and powerful computers to make pictures of the inside of your body.
- Magnetic resonance imaging (also called MRI). MRI is a medical test that makes a detailed picture of the inside of your body.
- X-ray. X-rays use radiation to make a picture of your baby’s body on film.
Spina bifida treatment
Spina bifida treatment depends on the severity of the condition. Spina bifida occulta often doesn’t require treatment at all, but other types of spina bifida do.
If your child is diagnosed with spina bifida, they’ll be referred to a specialist team who will be involved in their care.
A care plan may be drawn up to address your child’s needs and any problems they have. As your child gets older, the care plan will be reassessed to take into account changes to their needs and situation.
There are several different treatments for the various problems spina bifida can cause. These are described below.
Surgery before birth
Nerve function in babies with spina bifida can worsen after birth if it’s not treated. Prenatal surgery for spina bifida (fetal surgery) takes place before the 26th week of pregnancy. Surgeons expose a pregnant mother’s uterus surgically, open the uterus and repair the baby’s spinal cord.
Research suggests that children with spina bifida who had fetal surgery may have reduced disability and be less likely to need crutches or other walking devices. In addition, fetal surgery may reduce the risk of hydrocephalus. Ask your doctor whether this procedure may be appropriate for you. Discuss the risks, such as possible premature delivery and other complications, and potential benefits for you and your baby.
It’s important to have a comprehensive evaluation to determine whether fetal surgery is feasible. This specialized surgery should only be done at a health care facility that has experienced fetal surgery experts, a multispecialty team approach and neonatal intensive care. Typically the team includes a fetal surgeon, pediatric neurosurgeon, maternal-fetal medicine specialist, fetal cardiologist and neonatologist.
Cesarean birth
Many babies with myelomeningocele tend to be in a feet-first (breech) position. If your baby is in this position or if your doctor has detected a large cyst or sac, cesarean birth may be a safer way to deliver your baby.
Surgery after birth
Meningocele involves surgery to put the meninges back in place and close the opening in the vertebrae. Because the spinal cord develops normally in babies with meningocele, these membranes often can be removed by surgery with little or no damage to nerve pathways.
Myelomeningocele also requires surgery. Performing the surgery early can help minimize risk of infection that’s associated with the exposed nerves and may also help protect the spinal cord from more trauma.
During the procedure, a neurosurgeon places the spinal cord and exposed tissue inside the baby’s body and covers them with muscle and skin. Sometimes a shunt to control hydrocephalus in the baby’s brain is placed during the operation on the spinal cord.
Treatment for complications
In babies with myelomeningocele, irreparable nerve damage has likely already occurred and ongoing care from a multispecialty team of surgeons, physicians and therapists is usually needed. Babies with myelomeningocele may need more surgery for a variety of complications. Treatment for complications — such as weak legs, bladder and bowel problems or hydrocephalus — typically begins soon after birth.
Depending on the severity of spina bifida and the complications, treatment may include, for example:
- Walking and mobility aids. Some babies may start exercises to prepare their legs for walking with braces or crutches when they’re older. Some children may need walkers or a wheelchair. Mobility aids, along with regular physical therapy, can help a child become independent.
- Bowel and bladder management. Routine bowel and bladder evaluations and management plans help reduce the risk of organ damage and illness. Evaluations include X-rays, kidney scans, ultrasounds, blood tests and bladder function studies. These evaluations will be more frequent in the first few years of life, but less often as children grow.
- Bowel management may include oral medications, suppositories, enemas, surgery, or a combination of these approaches.
- Bladder management may include medications, using catheters to empty the bladder, surgery, or a combination.
- For children, a specialist in pediatric urology with experience in evaluating and performing surgery on children with spina bifida is the best choice.
- Surgery for hydrocephalus. Most babies with myelomeningocele will need a ventricular shunt — a surgically placed tube that allows fluid in the brain to drain into the abdomen. This tube might be placed just after birth, during the surgery to close the sac on the lower back or later as fluid accumulates. A less invasive procedure, called endoscopic third ventriculostomy, may be used, but candidates must be carefully chosen and meet certain criteria. The surgeon uses a small video camera to see inside the brain and makes a hole in the bottom of or between the ventricles so cerebrospinal fluid can flow out of the brain.
- Treatment and management of other complications. To help with functioning, special equipment such as bath chairs, commode chairs and standing frames may be needed. Whatever the issue — orthopedic complications, tethered spinal cord, GI issues, skin problems, or others — most spina bifida complications can be treated or at least managed to improve quality of life.
Ongoing care
Children with spina bifida need close follow-up care and observation. Their primary care doctors follow growth, the need for immunizations and general medical issues. They coordinate your child’s medical care.
Parents and other caregivers are a key part of the team, learning how to help manage their child’s condition and how to encourage and support their child emotionally and socially. Keep in mind that children with spina bifida can go on to college, hold jobs and have families. Special accommodations may be necessary along the way, but encourage your child to be as independent as possible.
Children with spina bifida also often need treatment and ongoing care from:
- Physical medicine and rehabilitation
- Neurology
- Neurosurgery
- Urology
- Orthopedics
- Physical therapy
- Occupational therapy
- Special education teachers
- Social workers
- Dietitians
Physiotherapy
Physiotherapy is an important way of helping someone with spina bifida to become as independent as possible. The main aim is to help with movement, prevent deformity, and stop the leg muscles weakening further.
This may involve daily exercises to help maintain strength in the leg muscles, as well as wearing special splints to support the legs.
Occupational therapy
Occupational therapy can help people find ways to carry out everyday activities and become more independent.
An occupational therapist can help work out practical solutions to problem areas such as getting dressed. They may for example provide equipment, such as handrails, to make the activity easier.
Mobility aids
People who are unable to use their legs at all will usually require a wheelchair. Electric wheelchairs are available, but using a manual wheelchair can help to maintain good upper body strength.
Leg braces, splints and other walking aids can be used by people who have weak leg muscles.
Treating bone and joint problems
Further corrective surgery may be needed if there are problems with bone development, such as hip dislocation or club foot (a deformity of the foot and ankle). This type of surgery is known as orthopaedic surgery.
Treating bladder problems
Many people with spina bifida have problems controlling their bladder.
Treatments for bladder problems include:
- antibiotics – lifelong antibiotics are sometimes needed to help prevent kidney and urinary infections
- medicines – that help relax the bladder so it can store more urine
- urinary catheterisation – an intermittent urinary catheter is usually needed to drain urine from the bladder several times a day to help prevent infection
- bladder surgery – may involve enlarging the bladder so it can hold more urine, or connecting the appendix to the bladder and making an opening in the belly so that a catheter can be used more easily
Treating bowel problems
Bowel problems, particularly constipation, are often a problem for people with spina bifida.
Treatments for bowel problems include:
- laxatives – a type of medicine to help empty the bowels
- suppositories and enemas – medicines put into the bottom to help stimulate the bowels and relieve constipation
- anal irrigation – where using special equipment, you pump water through a tube into your bottom to clean out your bowels; this can be done at home once you’ve been trained in using the equipment
- antegrade continence enema – an operation to create a channel between the bowel and a small opening (stoma) on the surface of the tummy; this means liquids can be passed through the opening in the tummy to flush stools out of the bottom
- colostomy – surgery to divert one end of the large bowel through an opening in the tummy; a pouch is placed over the opening to collect stools; a colostomy may be recommended if other treatments don’t work
Coping and support
News that your newborn child has a condition such as spina bifida can naturally cause you to feel grief, anger, frustration, fear and sadness. There’s good reason to hope, however, because most people with spina bifida live active, productive and full lives — especially with encouragement and support from loved ones.
Independent mobility is an important and appropriate goal for all children with spina bifida. This may mean walking with or without braces, using walking aids (such as canes or crutches) or exclusively using a wheelchair. They benefit from encouragement to participate in activities with their peers, and caregivers can help adjust activities to accommodate physical limitations.
Many children with spina bifida have normal intelligence, but some may need educational intervention for learning problems. Some children experience difficulty with attention, concentration or language that requires treatment from professionals outside of school.
As for any child with a chronic medical condition, children with spina bifida may benefit from meeting with mental health professionals, such as a child psychologist, to assist with adjustment and coping. Most children with spina bifida are resilient and adapt to their challenges with support from their parents, teachers and other caregivers.
If your child has spina bifida, you may benefit from finding a support group of other parents who are dealing with the condition. Talking with others who understand the challenges of living with spina bifida can be helpful.
Support at school
Most children with spina bifida have a normal level of intelligence and are often be able to attend a mainstream school.
However, they may need support to help with any learning disabilities they have, as well as any physical problems, such as incontinence.
If you think your child may need extra support at school or nursery, talk to their teacher or the special educational needs co-ordinator.
- Lamers Y (2011). Folate recommendations for pregnancy, lactation, and infancy. Ann Nutr Metab 59(1): 32-37. https://www.karger.com/Article/Abstract/332073[↩]
- Wilson RD, Johnson JA, Wyatt P, Allen V, Gagnon A, Langlois S, et al. (2007). Pre-conceptional vitamin/folic acid supplementation 2007: the use of folic acid in combination with a multivitamin supplement for the prevention of neural tube defects and other congenital anomalies. J Obstet Gynaecol Can 29(12): 1003-1026. https://www.ncbi.nlm.nih.gov/pubmed/18053387[↩]
- Pitkin RM (2007). Folate and neural tube defects. Am J Clin Nutr 85(1): 285S-288S. https://www.ncbi.nlm.nih.gov/pubmed/17209211[↩][↩]
- Williams LJ, Rasmussen SA, Flores A, Kirby RS, Edmonds LD (2005). Decline in the prevalence of spina bifida and anencephaly by race/ethnicity: 1995-2002. Pediatrics 116(3): 580-586. https://www.ncbi.nlm.nih.gov/pubmed/16140696[↩][↩]
- Shane B (2012). Folate-responsive birth defects: of mice and women. Am J Clin Nutr 95(1): 1-2. https://academic.oup.com/ajcn/article/95/1/1/4576483[↩]
- Dietary Reference Intakes for Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline. https://www.nap.edu/catalog/6015/dietary-reference-intakes-for-thiamin-riboflavin-niacin-vitamin-b6-folate-vitamin-b12-pantothenic-acid-biotin-and-choline[↩][↩]
- Centers for Disease Control and Prevention. Folic Acid, Recommendations, Occurrence Prevention. https://www.cdc.gov/ncbddd/folicacid/recommendations.html[↩]
- Centers for Disease Control and Prevention (2010). CDC Grand Rounds: additional opportunities to prevent neural tube defects with folic acid fortification. MMWR Morb Mortal Wkly Rep 59(31): 980-984. https://www.cdc.gov/mmwr/preview/mmwrhtml/mm5931a2.htm[↩]
- Centers for Disease Control (1991). Use of folic acid for prevention of spina bifida and other neural tube defects–1983-1991. MMWR Morb Mortal Wkly Rep 40(30): 513-516. https://www.ncbi.nlm.nih.gov/pubmed/2072886[↩]
- Scholl TO, Johnson WG (2000). Folic acid: influence on the outcome of pregnancy. Am J Clin Nutr 71(5 Suppl): 1295S-1303S. https://www.ncbi.nlm.nih.gov/pubmed/10799405[↩]
- American College of Obstetricians and Gynecologists. (2011). https://www.acog.org/~/media/For%20Patients/faq001.pdf?dmc=1&ts=20120515T1154495022[↩]





{kind=link}