Contents
What is a thoracotomy
Thoracotomy is surgery done through a cut (incision) in the chest wall between the ribs, your doctor may make the cut in your chest wall through your front, side, or back. Your doctor is able to operate inside your chest through the thoracotomy. A thoracotomy may be used for surgery on the lungs, esophagus, trachea, heart, aorta, or diaphragm. The exact place where your doctor makes the incision depends on the reason for your surgery. It is usually across the side of the mid-chest.
In order to spread the ribs far enough to do the surgery, your doctor may need to cut through a rib or the breastbone (sternum). When the surgery is finished, the doctor will close the incision with stitches or staples. If a rib or the breastbone was cut, the doctor will use wire to hold the pieces of bone together as they heal.
Most people spend 3 to 7 days in the hospital after this type of surgery. You will be quite sore after chest surgery. You will get medicine to help with this. Even though you will be sore, it is very important to breathe deeply and be as active as possible after surgery. This will help your lungs expand again and help you heal more quickly. It is important not to smoke after surgery.
The amount of time you will need to recover at home depends on the type of surgery you had. You will probably need to take at least 1 to 2 months off work.
Preparing for thoracotomy surgery
Bring a list of questions to ask your doctors. It is important that you understand exactly what surgery is planned, the risks, benefits, and other options before your surgery.
Tell your doctors ALL the medicines and natural health products you take. Some of these can increase the risk of bleeding or interact with anesthesia. Your doctor will tell you which medicines to take or stop before your surgery.
If you take blood thinners, such as warfarin (Coumadin), clopidogrel (Plavix), or aspirin, be sure to talk to your doctor. He or she will tell you if you should stop taking these medicines before your surgery. Make sure that you understand exactly what your doctor wants you to do.
You may need to stop taking certain medicines a week or more before surgery, so talk to your doctor as soon as you can.
Before your surgery, you will speak with an anesthesia provider to discuss your anesthetic options, including the risks, benefits, and alternatives to each. This may be on the phone or in person.
Taking care of yourself before surgery
- Build healthy habits into your life. Changes are best made several weeks before surgery, since your body may react to sudden changes in your habits.
- Stay as active as you can.
- Eat a healthy diet.
- Cut back or quit alcohol and tobacco.
- If you have an advance care plan, let your doctor know. If you do not have one, you may want to prepare one so your doctor and loved ones know your health care wishes. Doctors recommend that everyone prepare these papers before surgery, regardless of the type of surgery or condition.
Thoracotomy procedure
- Before thoracotomy surgery you will be asked to repeat your full name, what surgery you are having, and what part of your body is being operated on. The area for surgery may be marked.
- A small tube (IV) will be placed in a vein, to give you fluids and medicine to help you relax. Because of the combination of medicines given to keep you comfortable, you may not remember much about the operating room.
- You will be kept comfortable and safe by your anesthesia provider. You will be asleep during the surgery.
- The thoracotomy surgery will take about 2 to 4 hours.
- You may stay in the ICU for the first 1 or 2 days after thoracotomy surgery.
- As you wake up in the recovery room, the nurse will check to be sure you are stable and comfortable. It is important for you to tell your doctor and nurse how you feel and ask questions about any concerns you may have.
- You will have a tube down your throat during surgery to help you breathe. This will probably be removed before you are fully awake.
- You will probably have one or two tubes coming out of your chest to drain fluid and air so that your lungs can expand again after surgery. The chest tubes will be removed before you go home.
- You will have a tube in your vein, called an IV, to give you fluids and medicines.
- You may have a tube in your wrist, called an arterial line, to measure your blood pressure.
- You may have a tube that drains urine from your bladder (urinary catheter) for a few days.
- You may have an epidural catheter, which is a tiny tube that delivers pain medicine directly into the area in your back around your spinal cord. The epidural will help prevent pain after surgery.
Clamshell thoracotomy
Clamshell thoracotomy is a large transverse incision that spans across the entire chest wall 1. It is also known as a bilateral thoracotomy and is used during massive chest trauma, lung transplant, or resection of tumors in the chest. The incision extends through the sternum, between the fourth and fifth ribs bilaterally, and extends to the mid-axillary line. Mammary vessels will be interrupted as well as intercostal muscles with associated intercostal nerves and vessels 2.
Figure 1. Clamshell thoracotomy
Thoracotomy recovery
Going home
- Be sure you have someone to drive you home.
- Ask your doctor when you can drive again.
- Arrange for extra help at home after surgery, especially if you live alone or provide care for another person.
- You will be given more specific instructions about recovering from your surgery, including activity and when you may return to work.
It is common to feel tired for 6 to 8 weeks after thoracotomy surgery. Your chest may hurt and be swollen for up to 6 weeks. It may ache or feel stiff for up to 3 months. You may also feel tightness, itching, numbness, or tingling around the incision for up to 3 months. Your doctor will give you medicine to help with pain.
You will have stitches or staples in the incision. You may have one or more tubes coming out of your chest to drain fluid and air that can build up after thoracotomy surgery. The tubes are often removed before you leave the hospital. Your doctor will remove the stitches or staples at your follow-up visit.
You may feel short of breath at first after the thoracotomy surgery. Your doctor, nurse, or respiratory therapist will teach you deep-breathing and coughing exercises to help your body get as much oxygen as possible. You also may need to get extra oxygen through a mask or a plastic tube in your nostrils (nasal cannula). This is called oxygen therapy.
The amount of time you will need to recover depends on the surgery you had. You probably will need to take at least 1 to 2 months off work.
Call your local emergency number anytime you think you may need emergency care. For example, call if:
- You passed out (lost consciousness).
- You have severe trouble breathing.
- You have sudden chest pain and shortness of breath, or you cough up blood.
Call your doctor or seek immediate medical care if:
- You are sick to your stomach or cannot keep fluids down.
- You have pain that does not get better after you take pain medicine.
- You have a fever over 100.4 °F (38°C).
- You have loose stitches, or your incision comes open.
- Bright red blood has soaked through the bandage over your incision.
- You have signs of infection, such as:
- Increased pain, swelling, warmth, or redness.
- Red streaks leading from the incision.
- Pus draining from the incision.
- Swollen lymph nodes in your neck, armpits, or groin.
- A fever.
- You cough up a lot more mucus than normal, or your mucus changes color.
Watch closely for changes in your health, and be sure to contact your doctor or nurse call line if you have any problems.
How to you care for yourself at home
Medicines
- Your doctor will tell you if and when you can restart your medicines. He or she will also give you instructions about taking any new medicines.
- If you take blood thinners, such as warfarin (Coumadin), clopidogrel (Plavix), or aspirin, be sure to talk to your doctor. He or she will tell you if and when to start taking those medicines again. Make sure that you understand exactly what your doctor wants you to do.
- Take pain medicines exactly as directed.
- If the doctor gave you a prescription medicine for pain, take it as prescribed.
- If you are not taking a prescription pain medicine, ask your doctor if you can take an over-the-counter medicine.
- Do not take two or more pain medicines at the same time unless the doctor told you to. Many pain medicines have acetaminophen, which is Tylenol.
- Too much acetaminophen (Tylenol) can be harmful.
- If you think your pain medicine is making you sick to your stomach:
- Take your medicine after meals (unless your doctor has told you not to).
- Ask your doctor for a different pain medicine.
- If your doctor prescribed antibiotics, take them as directed. Do not stop taking them just because you feel better. You need to take the full course of antibiotics.
Incision care
- If you have strips of tape on the incision, leave the tape on for a week or until it falls off.
- Wash the area daily with warm, soapy water, and pat it dry. Don’t use hydrogen peroxide or alcohol, which may delay healing. You may cover the area with a gauze bandage if it weeps or rubs against clothing. Change the bandage every day.
- Keep the area clean and dry.
Diet
- You can eat your normal diet. If your stomach is upset, try bland, low-fat foods like plain rice, broiled chicken, toast, and yogurt.
- Drink plenty of fluids (unless your doctor tells you not to).
- You may notice that your bowel movements are not regular right after your surgery. This is common. Try to avoid constipation and straining with bowel movements. You may want to take a fiber supplement every day. If you have not had a bowel movement after a couple of days, ask your doctor about taking a mild laxative.
Activity
- Rest when you feel tired. Getting enough sleep will help you recover.
- Try to walk each day. Start by walking a little more than you did the day before. Bit by bit, increase the amount you walk. Walking boosts blood flow and helps prevent pneumonia and constipation.
- Do not smoke or allow others to smoke around you. If you need help quitting, talk to your doctor about stop-smoking programs and medicines. These can increase your chances of quitting for good.
- Try to avoid being around people who you know have a cold, the flu, or other illness.
- Avoid strenuous activities, such as bicycle riding, jogging, weight lifting, or aerobic exercise, until your doctor says it is okay. Also avoid swimming, tennis, golf, or other activities that could strain your arm and shoulder muscles, until your doctor says it is okay.
- Until your doctor says it is okay, avoid lifting anything that would make you strain. This may include a child, heavy grocery bags and milk containers, a heavy briefcase or backpack, cat litter or dog food bags, or a vacuum cleaner.
- If your incision is in the front or the side of your chest, hold a pillow over the incision when you cough or take deep breaths. This will support your chest and decrease your pain.
- Ask your doctor when it is safe to you to drive or fly. You probably will not be able to drive for at least 4 weeks. This is because your arm and shoulder muscles may be stiff after surgery and could make it difficult to steer.
- You may be able to take showers (unless you have a drain near your incision). If you have a drain near your incision, follow your doctor’s instructions to empty and care for it. Do not take a bath for the first 2 weeks, or until your doctor tells you it is okay.
- Ask your doctor when it is okay for you to have sex.
- You will probably need to take at least 1 to 2 months off from work. It depends on the surgery you had and the type of work you do.
Exercise
- To help keep your lungs clear, cough and do deep breathing exercises as you are told by your doctor, nurse, or respiratory therapist.
- Your doctor may send you home with an incentive spirometer. This device helps you practise taking deep breaths, which can help keep your lungs healthy.
- Ask your doctor about exercises to keep your arm and shoulder muscles strong and flexible while you recover.
Emergency thoracotomy
Emergency thoracotomy also known as emergency department thoracotomy, sometimes referred to as emergency resuscitative thoracotomy, is a drastic, last-ditch effort to save the life of a patient in extremis due to injury 3. Although some studies boast a 60% survival rate, others have argued that emergency thoracotomy is a futile and expensive procedure that only places health care providers at significant personal risk 4. Further, indications for emergency thoracotomy have widely varied. For these reasons, the emergency thoracotomy remains a controversial but potentially lifesaving procedure in a select group of patients 5.
The causes of acute circulatory arrest after chest injury include hemorrhagic shock due to injury to the heart or intrathoracic vasculature, cardiac tamponade, and tension pneumothorax.
The primary goals of emergency thoracotomy include the following 6:
- Hemorrhage control
- Release of cardiac tamponade 7
- Facilitation of internal/open cardiac massage 8
- Prevention of air embolism
- Exposure of the descending thoracic aorta for cross-clamping
- Repair cardiac or pulmonary injury
Emergent thoracotomy typically takes place in the emergency department or operating room. It is crucial for the emergency provider to consult a surgeon upon the patient’s arrival to facilitate with the procedure if possible or to manage the patient subsequent to the thoracotomy.
Most patients undergoing emergency thoracotomy are comatose or medically sedated and/or paralyzed from airway management.
The first consideration should be to intubate the patient for adequate control and comfort. If orotracheal intubation is not possible (eg, unsuccessful intubation or anticipated difficult intubation), adequate analgesic and amnestic agents are indicated. Ideally, agents that have minimal effects on the cardiovascular system should be used.
Emergent thoracotomies have been successfully performed in the prehospital setting by physicians and emergency medical service teams 9. Rapid transport to the emergency department is associated with higher survival rates in thoracic injury 10.
Survival after emergency thoracotomy in blunt trauma patients is much lower than with penetrating injury 11. Some recommend not performing emergency thoracotomy in patients with blunt trauma, owing to the particularly low survival rates 12. Of penetrating injuries, survival after emergency thoracotomy is higher in stab wounds than gunshot wounds 13. Patients who sustain a single penetrating wound to the chest have the best survivability after a resuscitative thoracotomy 14. Outcomes are similar in adult and pediatric patients 15.
Control of the airway via standard orotracheal intubation technique is strongly advised prior to performing emergency thoracotomy. Selective intubation of the right mainstem bronchus is the preferred method. This allows for both ventilation and oxygenation of the patient via the right lung as well as decreased risk of injury to the left lung via decreased left lung expansion during a left-sided anterolateral thoracotomy. To intubate the right mainstem bronchus, directly visualize the vocal cords to pass the endotracheal (ET) tube into the trachea, and then blindly pass the ET tube to approximately 30 cm.
Either prior to emergency thoracotomy or while the procedure is being performed, an assistant should pass a nasogastric tube to help distinguish the esophagus from the aorta upon exploration of the thoracic contents.
Immediately obtain a surgical consult. If the patient survives the emergency thoracotomy, they need to be taken expediently to the operating room.
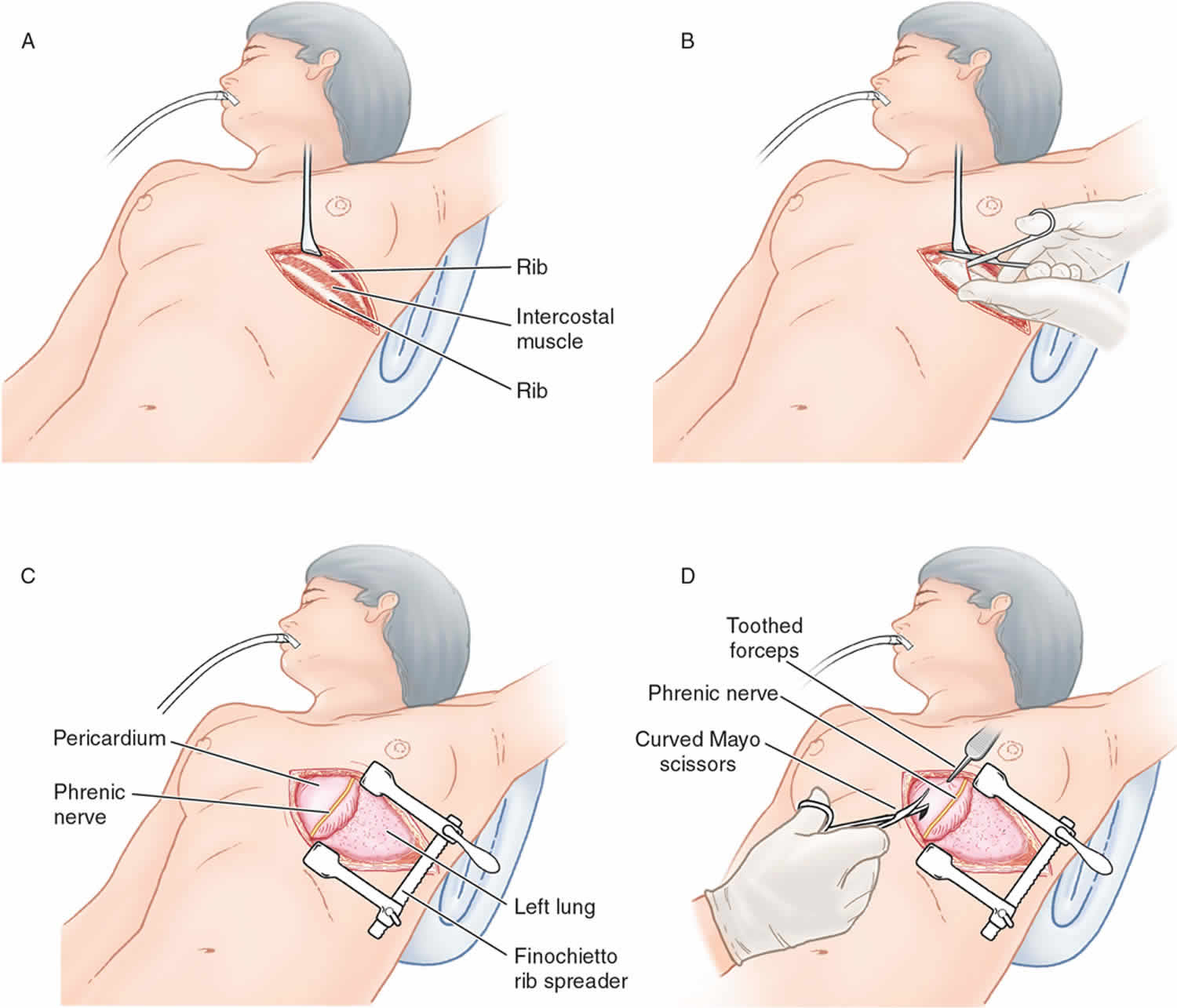
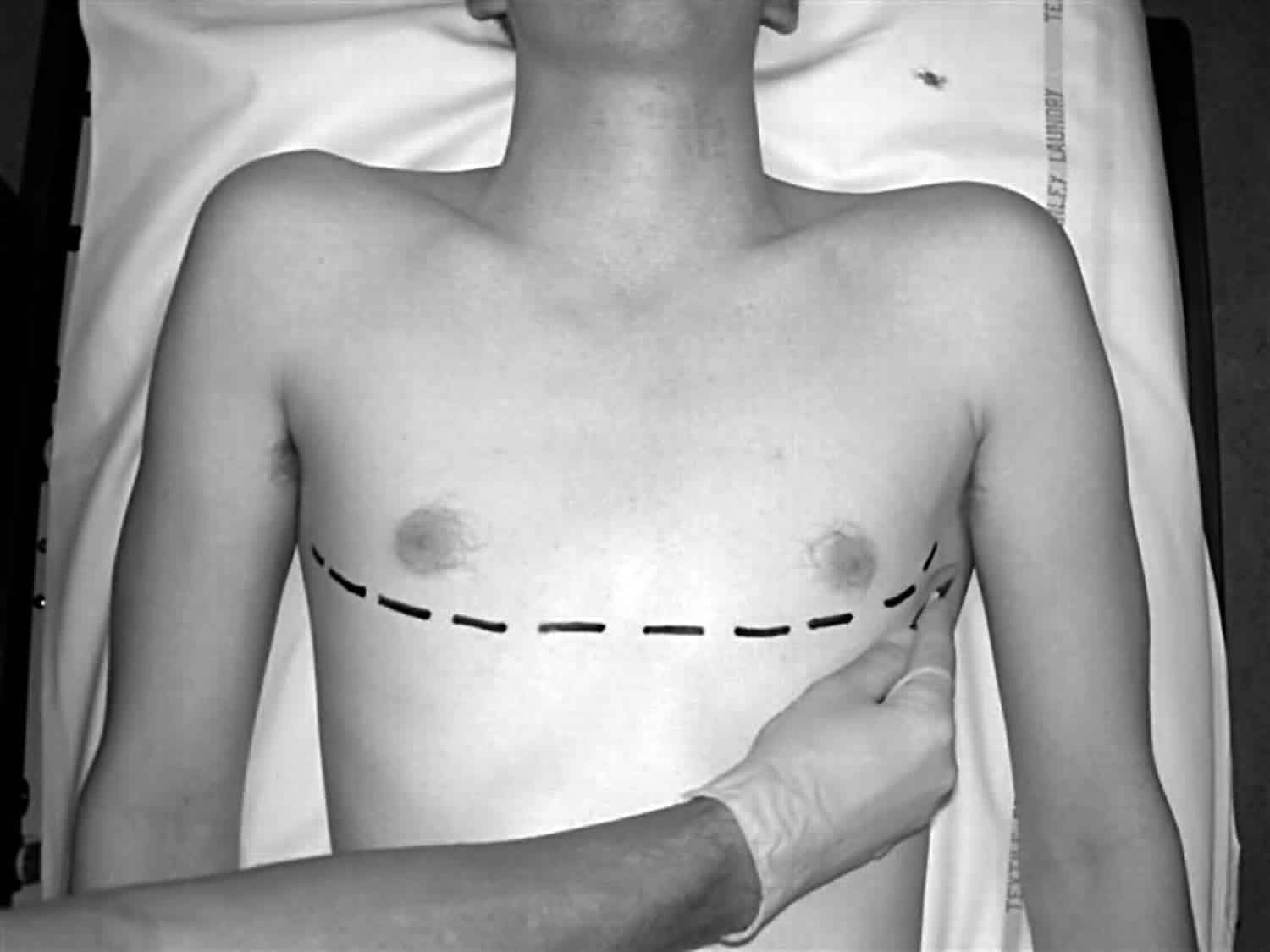
Use the left anterolateral thoracotomy approach when the site of the injury is unknown and the patient’s status requires immediate intervention for possible intrathoracic injuries.
Incision over the fifth rib with dissection into the fourth intercostal space provides the best access to the heart and great vessels. This incision is just beneath the nipple in men or along the inframammary fold in women.
The rib spreaders should be placed with the handle downward to permit for extension of the incision into the right chest if necessary.
Avoid making the incision too low. The location of the heart is commonly thought of as lower than it actually is.
The incision should be made just above the rib to avoid injury to the intercostals neurovascular bundle.
Gaining access to the thoracic cavity should take no longer than 1-2 minutes.
Use nontoothed forceps to lift the pericardium, and use small dressing scissors to open it in order to avoid ventricular laceration 16.
When the patients clinical status allows, urgent rather than emergent thoracotomy can be performed to minimize the dangers incumbent to this procedure in the emergency department 17.
Large amounts of blood products are typically required in the resuscitation of patients undergoing emergency thoracotomy.
Consider potential organ donor rescue after emergency thoracotomy arrest 18.
Emergency thoracotomy indications
The indications for emergency thoracotomy have been much debated.
To simplify the issue, the American College of Surgeons Committee on Trauma has instituted general guidelines on this subject 19.
The decision to perform an emergency thoracotomy is determined by the presence of signs of life and the mechanism and location of injury.
Increased thoracotomy survival rates are associated with signs of life in the emergency department, including the following:
- Pupillary response
- Spontaneous ventilation
- Presence of carotid pulse
- Measurable or palpable blood pressure
- Extremity movement
- Cardiac electrical activity
Thoracic injuries (as opposed to abdominal injuries) can be identified and treated during emergency thoracotomy.
Survival for blunt injury is significantly lower than for penetrating injury due to conditions such as cardiac contusion, cardiac rupture, and aortic rupture 20. Many consider an attempt to resuscitate a blunt trauma patient in cardiac arrest futile 21. However, some have a different view, reporting better outcomes from emergency thoracotomy in European countries where blunt trauma predominates 22.
Stab wounds (as opposed to gunshot wounds [GSWs]) are associated with a higher success rate. Gunshot wound injuries are usually unable to spontaneously seal because of the large nature of the missile injury pattern 23.
The following are also associated with increased survival:
- Higher blood pressure
- Higher respiratory rates
- Higher Glasgow coma scale scores
Accepted indications for emergency thoracotomy
- Penetrating thoracic injury with the following conditions:
- Previously witnessed cardiac activity (prehospital or in-hospital)
- Unresponsive hypotension 24
- Blunt thoracic injury with the following conditions:
- Previously witnessed cardiac activity (prehospital or in-hospital)
- Rapid exsanguination from the chest tube (>1,500 mL immediately returned)
- Unresponsive hypotension (systolic blood pressure <70 mm Hg) despite vigorous resuscitation
American College of Surgeons Committee on Trauma indications for emergency thoracotomy are as follows 25:
- Precordial wound in a patient with prehospital cardiac arrest
- Trauma patient with cardiac arest after arrival to emergency department
- Profound hypotension (<70 mm Hg) in a patient with a truncal wound who is either unconscious or an operating room is unavailable
Relative indications for emergency thoracotomy
- Penetrating thoracic injury with traumatic arrest without previously witnessed cardiac activity
- Penetrating nonthoracic injury (eg, abdominal, peripheral) with traumatic arrest with previously witnessed cardiac activity (prehospital or in-hospital)
- Blunt thoracic injuries with traumatic arrest with previously witnessed cardiac activity (pre-hospital or in-hospital).
The decision to perform an emergency thoracotomy should be made on a case-by-case basis, owing to exceptions and reported survivors who exceeded the above thresholds 26.
Previous studies have suggested that in order to maximize neurologic outcomes, resuscitation should occur within 10 minutes for blunt trauma and 10-15 minutes for penetrating trauma 27.
The Eastern Association for the Surgery of Trauma sought to provide evidence-based recommendations for emergency thoracotomy based on common clinical scenarios based on a systematic data search. Their conclusions are summarized as follows 28:
- Patient presents pulseless to the emergency department with signs of life after penetrating thoracic injury – Resuscitative emergency thoracotomy strongly recommended
- Patient presents pulseless to the emergency department without signs of life after penetrating thoracic injury – Resuscitative emergency thoracotomy conditionally recommended
- Patient presents pulseless to the emergency department with signs of life after penetrating extrathoracic injury – Resuscitative emergency thoracotomy conditionally recommended
- Patient presents pulseless to the emergency department without signs of life after penetrating extrathoracic injury – Resuscitative emergency thoracotomy conditionally recommended
- Patient presents pulseless to the emergency department with signs of life after blunt injury – Resuscitative emergency thoracotomy conditionally recommended
- Patient presents pulseless to the emergency department without signs of life after blunt injury – Conditionally recommend against resuscitative emergency thoracotomy
Emergency thoracotomy contraindications
Emergency thoracotomy should not be performed in patients under the following conditions:
- Blunt injury without witnessed cardiac activity (prehospital) 29
- Penetrating abdominal trauma without cardiac activity (prehospital)
- Nontraumatic arrest
- Severe head injury
- Severe multisystem injury
- Improperly trained team
- Insufficient equipment
A 2011 prospective multicenter study suggests that emergency thoracotomy does not yield survival if the following are noted 30:
- Blunt trauma with more than 10 minutes of prehospital cardiopulmonary resuscitation (CPR) without response
- Penetrating trauma with more than 15 minutes of prehospital CPR without response
- Asystole without cardiac tamponade
As mentioned, the decision to perform emergency thoracotomy should be made on a case-by-case basis because the literature demonstrates rare survival even in patients with relatively favorable parameters 21.
Equipment
Personal protective equipment and preparation
- Gloves
- Sterile gloves
- Gown
- Face shield
- Povidone iodine (Betadine)
- Sterile drapes
Thoracotomy tray
To enter the chest cavity:
- Scalpel, No. 10 or No. 20 blade
- Mayo scissors (alternatively, Metzenbaum scissors)
- Rib spreaders (eg, Finochietto)
- Trauma shears or saw (eg, Gigli)
To control hemorrhage and repair injury:
- Tissue/tooth forceps
- Satinsky vascular clamps (large and small)
- Long and short needle holders (eg, Hegar)
- Nonabsorbable sutures (silk), 2-0 or larger, on large round-body needle
- Cardiovascular Ethibond sutures, 3-0
- Teflon pledgets plus polypropylene or large braided sutures
- Suture scissors
- Aortic clamp instrument
- Kelly clamp
- Skin stapler
- High-volume suction device
- Laparotomy packs
- Tonsil clamps
- Foley catheter, 20F with 30-mL balloon
- Laparotomy pads
- Teflon patches
- Internal defibrillator (charge to 10 J to start)
- Chest tube, 30F
- Advanced cardiac life support medications
A simplified approach has been suggested in performing a “clamshell” thoracotomy to maximize exposure and minimize time of performance, requiring only a scalpel, nontoothed forceps, dressing scissors, and Plaster-of-Paris shears 31.
Thoracotomy vs Thoracostomy
A thoracostomy is a small incision of the chest wall for insertion of a chest tube into the pleural space to drain air or fluid from the chest 32. The tube may be attached to a suction device to remove excess fluid or air. Or, it may be used in a procedure called pleurodesis in which medication is delivered into the space to decrease the likelihood that fluid will accumulate. Thoracostomy is most commonly used for the treatment of a pneumothorax. This is performed by physicians, and paramedics, usually via needle thoracostomy or with a thoracostomy tube (chest tube).
Thoracostomy indications are as follows:
- Pneumothorax 33: Open or closed; simple or tension 34
- Hemothorax 33
- Hemopneumothorax
- Hydrothorax
- Chylothorax 35
- Empyema
- Pleural effusion 36
- Patients with penetrating chest wall injury who are intubated or about to be intubated
- Considered for those about to undergo air transport who are at risk for pneumothorax
- Workup and diagnosis of idiopathic pleural effusions
- Staging of lung cancer 37
- Pleurodesis
- Site-directed biopsy of parietal pleura
- Staging for mesothelioma
- Jelinek LA, Jones MW. Surgical Access Incisions. [Updated 2019 May 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK541018[↩]
- Dumas RP, Chreiman KM, Seamon MJ, Cannon JW, Reilly PM, Christie JD, Holena DN. Benchmarking emergency department thoracotomy: Using trauma video review to generate procedural norms. Injury. 2018 Sep;49(9):1687-1692[↩]
- Siram, Suryanarayana, Oyetunji T, Johnson SM, Khoury, AL, et al. Predictors for survival of penetrating trauma using emergency department thoracotomy in an urban trauma center: the Cardiac Instability Score. Journal of the National Medical Association. Feb 2010. 102(2):126-130[↩]
- Emergency Bedside Thoracotomy. https://emedicine.medscape.com/article/82584-overview[↩]
- Hunt PA, Greaves I, Owens WA. Emergency thoracotomy in thoracic trauma-a review. Injury. 2006 Jan. 37(1):1-19[↩]
- Kirkpatrick AW, Ball CG, D’Amours SK, Zygun D. Acute resuscitation of the unstable adult trauma patient: bedside diagnosis and therapy. Can J Surg. 2008 Feb. 51(1):57-69[↩]
- Menaker J, Cushman J, Vermillion JM, Rosenthal RE, Scalea TM. Ultrasound-diagnosed cardiac tamponade after blunt abdominal trauma-treated with emergent thoracotomy. J Emerg Med. 2007 Jan. 32(1):99-103[↩]
- Boczar ME, Howard MA, Rivers EP, Martin GB, Horst HM, Lewandowski C. A technique revisited: hemodynamic comparison of closed- and open-chest cardiac massage during human cardiopulmonary resuscitation. Crit Care Med. 1995 Mar. 23(3):498-503[↩]
- Davies GE, Lockey DJ. Thirteen survivors of prehospital thoracotomy for penetrating trauma: a prehospital physician-performed resuscitation procedure that can yield good results. J Trauma. 2011 May. 70(5):E75-8.[↩]
- Kidher E, Krasopoulos G, Coats T, Charitou A, Magee P, Uppal R, et al. The effect of prehospital time related variables on mortality following severe thoracic trauma. Injury. 2012 Sep. 43 (9):1386-92[↩]
- Hoth JJ, Scott MJ, Bullock TK, Stassen NA, Franklin GA, Richardson JD. Thoracotomy for blunt trauma: traditional indications may not apply. Am Surg. 2003 Dec. 69(12):1108-11.[↩]
- Lustenberger T, Labler L, Stover JF, Keel MJ. Resuscitative emergency thoracotomy in a Swiss trauma centre. Br J Surg. 2012 Apr. 99(4):541-8[↩]
- Tan BK, Pothiawala S, Ong ME. Emergency thoracotomy: a review of its role in severe chest trauma. Minerva Chir. 2013 Jun. 68 (3):241-50[↩]
- Cipolle M, Rhodes M, Tinkoff G. Deadly dozen: dealing with the 12 types of thoracic injuries. JEMS. 2012 Sep. 37 (9):60-5[↩]
- Easter JS, Vinton DT, Haukoos JS. Emergent pediatric thoracotomy following traumatic arrest. Resuscitation. 2012 Dec. 83 (12):1521-4[↩]
- Puchwein P, Sommerauer F, Clement HG, Matzi V, Tesch NP, Hallmann B, et al. Clamshell thoracotomy and open heart massage–A potential life-saving procedure can be taught to emergency physicians: An educational cadaveric pilot study. Injury. 2015 Sep. 46 (9):1738-42[↩]
- Kremer H, Wilson J. Penetrating cardiac injury with urgent not emergent thoracotomy. Missouri Medicine. Sept-Oct2010. 107(5):328-330.[↩]
- Schnuriger B, Inaba K, Branco BC, Salim A, Russell K, Lam L, et al. Organ donation: an important outcome after resuscitative thoracotomy. Journal of the American College of Surgeons. Oct 2010. 211(4):450-455[↩]
- Working Group, Ad Hoc Subcommittee on Outcomes, American College of Surgeons-Committee on Trauma. Practice management guidelines for emergency department thoracotomy. J Am Coll Surg. 2001 Sep. 193(3):303-9[↩]
- Velmahos GC, Degiannis E, Souter I, Allwood AC, Saadia R. Outcome of a strict policy on emergency department thoracotomies. Arch Surg. 1995 Jul. 130(7):774-7[↩]
- Moriwaki Y, Sugiyama M, Yamamoto T, Tahara Y, Toyoda H, Kosuge T, et al. Outcomes from prehospital cardiac arrestin blunt trauma patients. World Journal of Surgery. Jan 2011. 35:34-45[↩][↩]
- Narvestad JK, Meskinfamfard M, Søreide K. Emergency resuscitative thoracotomy performed in European civilian trauma patients with blunt or penetrating injuries: a systematic review. Eur J Trauma Emerg Surg. 2016 Dec. 42 (6):677-685[↩]
- Siram, Suryanarayana, Oyetunji T, Johnson SM, Khoury, AL, et al. Predictors for survival of penetrating trauma using emergency department thoracotomy in an urban trauma center: the Cardiac Instability Score. Journal of the National Medical Association. Feb 2010. 102(2):126-130.[↩]
- Iwata T, Inoue K, Hige M, Yamazaki K, Kawata Y, Suehiro S. Multiple thoracoabdominal gunshot wounds with complicated trajectories. Jpn J Thorac Cardiovasc Surg. 2006 Oct. 54(10):444-7.[↩]
- American College of Surgeons Committee on Trauma. Advanced trauma life support. 7th ed. Chicago, Ill: American College of Surgeons Committee on Trauma; 2004.[↩]
- Seamon MJ, Fischer CA, Gaughan JP, Kulp H, Dempsey DT, Goldberg AJ. Emergency department thoracotomy: survivial of the least expected. World J Surg. 2008. 32:604-612[↩]
- Millin MG, Galvagno SM, Khandker SR, et al. Withholding and termination of resuscitation of adult cardiopulmonary arrest secondary to trauma: resource document to the joint NAEMSP-ACSCOT position statements. J Trauma Acute Care Surg. 2013 Sep. 75 (3):459-67.[↩]
- Seamon, Mark J. MD; Haut, Elliott R. MD, PhD, et al. Emergency Department Thoracotomy. Journal of Trauma. July 2015. 79(1):159-173.[↩]
- Kavolius J, Golocovsky M, Champion HR. Predictors of outcome in patients who have sustained trauma and who undergo emergency thoracotomy. Arch Surg. 1993 Oct. 128(10):1158-62[↩]
- Moore EE, Knudson MM, Burlew CC, Inaba K, Dicker RA, Biffl WL, et al. Defining the limits of resuscitative emergency department thoracotomy: a contemporary Western Trauma Association perspective. Journal of Trauma-Injury Infection and Critical Care. Feb 2011. 70(2):334-339[↩]
- Puchwein P, Sommerauer F, Clement HG, Matzi V, Tesch NP, Hallmann B, et al. Clamshell thoracotomy and open heart massage–A potential life-saving procedure can be taught to emergency physicians: An educational cadaveric pilot study. Injury. 2015 Sep. 46 (9):1738-42.[↩]
- Mattox KL, Allen MK. Systematic approach to pneumothorax, haemothorax, pneumomediastinum and subcutaneous emphysema. Injury. 1986 Sep. 17(5):309-12[↩]
- Bailey RC. Complications of tube thoracostomy in trauma. J Accid Emerg Med. 2000 Mar. 17(2):111-4[↩][↩]
- Leigh-Smith S, Harris T. Tension pneumothorax–time for a re-think?. Emerg Med J. 2005 Jan. 22(1):8-16[↩]
- Tsukahara K, Kawabata K, Mitani H, Yoshimoto S, Sugitani I, Yonekawa H, et al. Three cases of bilateral chylothorax developing after neck dissection. Auris Nasus Larynx. 2007 Dec. 34(4):573-6[↩]
- Muzumdar H, Arens R. Pleural fluid. Pediatr Rev. 2007 Dec. 28(12):462-4[↩]
- Vial MR, Eapen GA, Casal RF, Sarkiss MG, Ost DE, Vakil E, et al. Combined pleuroscopy and endobronchial ultrasound for diagnosis and staging of suspected lung cancer. Respir Med Case Rep. 2018. 23:49-51.[↩]





{kind=link}