{kind=link}
Contents
Thromboembolism
Thromboembolism is a term referring to blood clot that forms inside a blood vessel (a thrombus) blocking most or all of the oxygen-carrying blood from flowing to that part of your body or an embolus which is a blood clot, piece of fat or atherosclrotic plaque which has broken off and been carried in the bloodstream to lodge in a distant blood vessel causing local death of the tissue (infarction). When the blood clot travels from the site where it formed to another location in the body, it is called an embolism or thromboembolism. Thromboembolism may occur in your veins which is called venous thromboembolism or “VTE” or in your arteries which is called arterial thromboembolism.
When a blood vessel (a vein or an artery) is injured, the damaged cells in the vessel wall send out chemical signals. These signals cause clots that slow or stop bleeding.
A blood clot forms through several steps 1:
- The blood vessel narrows. First, chemical signals cause the injured vessels to narrow to prevent more blood from leaking out.
- Platelets travel to the site of the injury. The chemical signals travel through your blood to the spleen, where many platelets (thrombocytes) are stored. The signals tell your spleen to release the platelets into your blood. Back at the injury site, the vessel walls become sticky and capture the platelets as they float past.
- A platelet plug forms. The platelets change shape and become stickier. This allows them to attach to the vessel wall and clump together into a plug.
- The blood clot forms. Clotting factors in your blood are normally turned off so that you do not form abnormal blood clots. When there is an injury, platelets release molecules into the blood that help turn on clotting factors. One important clotting factor is fibrin, a long, thin, and sticky protein. When it is turned on, it forms a mesh to hold the platelet plug in place. This is called a fibrin clot. The mesh also traps red blood cells to form a blood clot. The platelets contract to pull the two sides of the damaged vessel closer together, so it is easier to repair.
Once the blood clot is formed, your body’s immune system repairs the injury. At this point in the process, factors in your blood start to break down the blood clot.
If you do not have enough platelets (thrombocytes) or clotting factors in your blood, your blood will not be able to clot as well.
In other cases, your blood may clot too easily. Some conditions cause overactive clotting so that blood clots form in blood vessels throughout your body. Eventually, the platelets in your body are used up, which can then lead to bleeding. These conditions include:
- Antiphospholipid syndrome
- Disseminated intravascular coagulation (DIC)
- Thrombotic thrombocytopenic purpura
What is venous thromboembolism?
Venous thromboembolism also called “VTE” is a term referring to blood clot (a thrombus) that forms in a vein. Venous thromboembolism describes two related conditions: deep vein thrombosis (DVT) and a more serious complication called pulmonary embolism (PE), which is an emergency. A deep vein thrombosis (DVT) occurs when a blood clot forms in a deep vein, usually in your lower leg, thigh, or pelvis. Deep vein thrombosis (DVT) can also occur in your arms, especially if there is a large intravenous central line in the vein. A pulmonary embolism (PE) occurs when a clot breaks loose and travels through the bloodstream to your lungs. Both are blood clots in the veins and highly preventable. Venous thromboembolism (VTE) is common with many as 600,000 venous thromboembolism events occur each year in the United States 2. There are ways to prevent and treat venous thromboembolism (VTE), but you can help identify the warning signs of venous thromboembolism to save lives. Swelling, redness, and pain are some of the signs and symptoms of deep vein thrombosis (DVT). A pulmonary embolism can cause sudden chest pain and shortness of breath. Sometimes venous thromboembolism (VTE) occurs without any obvious signs, which can make it harder to diagnose. Medicines that help prevent further blood clots from forming or that dissolve serious vein blockages are the main treatments for venous thromboembolism. Without treatment, venous thromboembolism can restrict or block blood flow and oxygen, which can damage the body’s tissue or organs. This can be especially serious in the case of a pulmonary embolism, which blocks blood flow to the lungs. If a blood clot is large or there are many clots, a pulmonary embolism can cause death.
Many factors can put you at risk for venous thromboembolism. The risk of developing venous thromboembolism is highest after major surgery, major injury, or during periods of infection and inflammation or when you have heart failure, cancer, or a heart attack. This is because blood clots can develop in veins damaged by surgery or injury. Lack of movement after surgery or while traveling long distances can raise the likelihood of blood clotting. Inflammation and serious infection also raise the likelihood of blood clots.
Some of these risk factors seem obvious, such as lengthy surgery (especially orthopedic), pregnancy, being over age 40 and not exercising, cancer, obesity, use of birth control pills, hormone replacement therapy, family history of deep vein thrombosis (DVT), long distance travel (especially on airplanes) and spinal cord injuries. Others may not be as obvious such as heart failure, some types of lung disease, kidney disease, infections and other inflammatory diseases increase your risk. Smoking increases clotting risk as do obesity and inherited clotting conditions. These risk factors are additive: the more you have, the greater your risk. If you have several risk factors, such as a planned or a recent surgery, a fracture, been on bed rest, or will be immobilized for any length of time, you may want to discuss venous thromboembolism with your health care provider and develop a plan for preventing blood clots.
If you have recently had surgery or have other risk factors of venous thromboembolism, talk to your doctor about your risk and how to prevent blood clots. Your doctor will do tests to find out whether you have venous thromboembolism (VTE).
If you have venous thromboembolism, your doctor may prescribe medicines to treat serious vein blockages and help prevent further blood clots from forming.
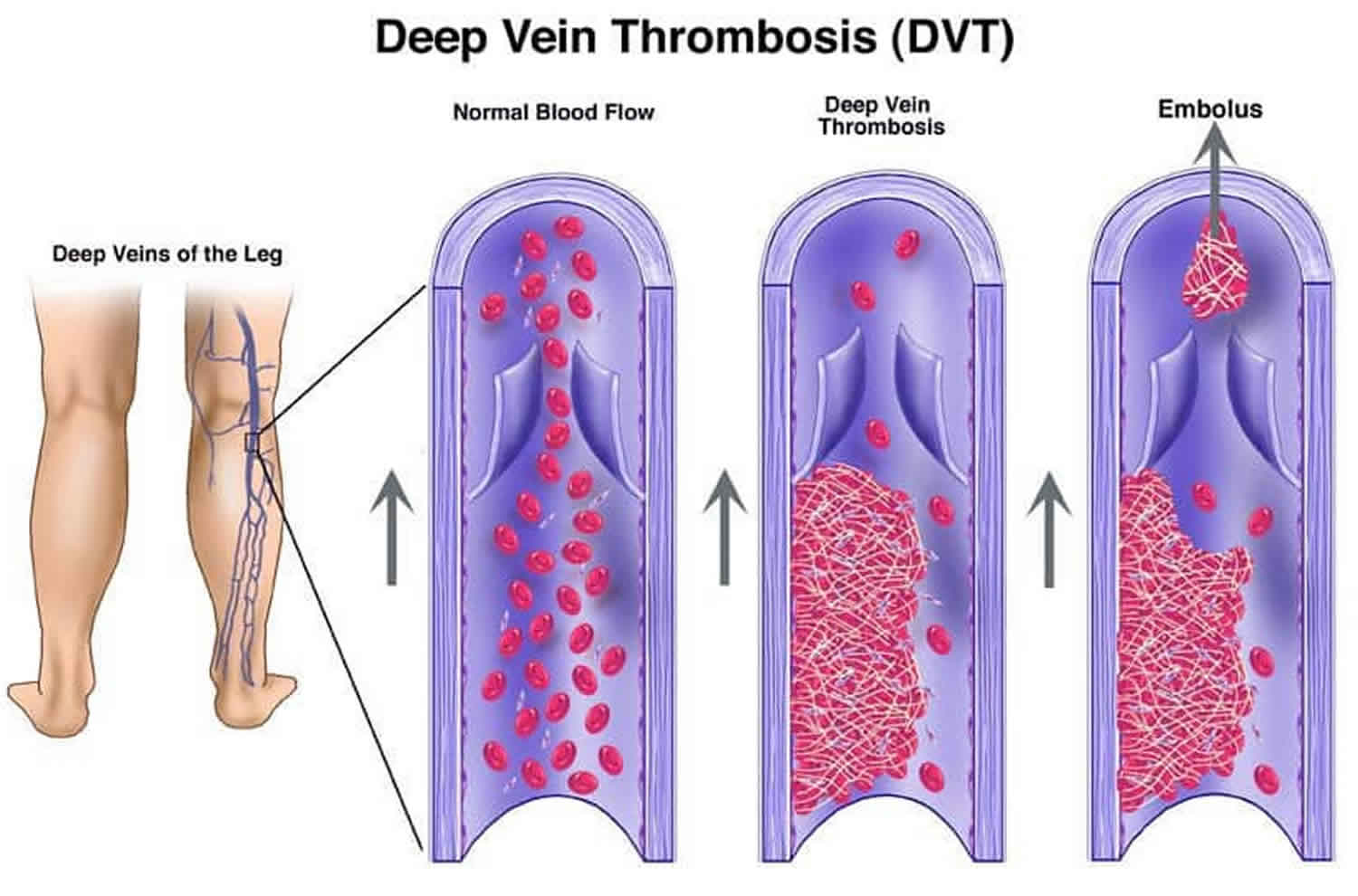
Deep vein thrombosis (DVT)
Deep vein thrombosis (DVT) is a medical condition that occurs when a blood clot forms in a deep vein. These blood clots usually develop in your lower leg or calf and can extend to involve the large deep veins of the upper legs, thighs or pelvis, but they can also occur in your arm. Only rarely does DVT occur in your arm and usually occurs because of intravenous (IV) access lines, or in athletic individuals due to repetitive injury. It is important to know about DVT because it can happen to anybody and can cause serious illness, disability, and in some cases, death. The good news is that DVT is preventable and treatable if discovered early.
Your legs and arms have two major types of veins: superficial and deep. The superficial veins are near the surface of the skin where they are sometimes visible, whereas the deep veins are located near the bones and are surrounded by muscle. Contraction or squeezing of the muscles around the deep veins sends blood back to the heart. A blood clot that develops in a deep vein can block this flow of blood and may or may not cause symptoms. DVT is not usually life threatening, but it can be if the blood clots break loose and go into your lungs. This condition is known as pulmonary embolism (PE) which can be fatal if the traveling blood clot, called an “embolus,” clogs the main lung arteries blocking their blood flow. Many people die in the first hour from a pulmonary embolism (PE), about 100,000 death in the United States each year, making it the third most common cause of vascular death. When deep vein thrombosis (DVT) and pulmonary embolism (PE) occur together, it’s called venous thromboembolism (VTE).
DVT can cause leg swelling that is usually treated with 3-6 months of a blood thinner. A long-term side effect of DVT is the development of the postthrombotic syndrome. About one-third of patients who experience a DVT (a higher percentage if the clot goes into the large veins in the pelvis or abdomen) can develop postthrombotic syndrome even after treatment with blood thinners. This condition can show up months to years later as chronic pain, swelling and discoloration of the leg, as well as the development of open sores or ulcers, caused by damage that is done by the clot to valves in the veins. The effects of postthrombotic syndrome can be long lasting and can lessen one’s quality of life.
DVT signs and symptoms
You may notice these symptoms of deep vein thrombosis (DVT) around the area of a blood clot in your leg:
- Swelling
- Pain or tenderness
- Cramping, aching, or increased warmth
- Red, purple or discolored skin, depending on the color of your skin
Deep vein thrombosis (DVT) can occur without noticeable symptoms.
DVT causes
Anything that prevents the blood from flowing or properly clotting can cause a blood clot. The main causes of deep vein thrombosis (DVT) are damage to a vein from surgery or inflammation and damage due to infection or injury.
Risk factors for DVT
Almost anyone can have a DVT. However, certain factors can increase the chance of having this condition. The chance increases even more for someone who has more than one of these factors at the same time.
Following is a list of factors that increase your risk of developing DVT:
- Injury to a vein, often caused by:
- Fractures,
- Severe muscle injury, or
- Major surgery (particularly involving the abdomen, pelvis, hip, or legs).
- Slow blood flow, often caused by:
- Confinement to bed (e.g., due to a medical condition or after surgery);
- Limited movement (e.g., a cast on a leg to help heal an injured bone). When your legs don’t move for a long time, the calf muscles don’t squeeze (contract). Muscle contractions help blood flow;
- Sitting for a long time, such as when driving or flying, especially with crossed legs, increases the risk of DVT; or
- Paralysis.
- Increased estrogen, often caused by:
- Birth control pills (oral contraceptives) or hormone replacement therapy. Both can increase the blood’s ability to clot.
- Hormone replacement therapy, sometimes used after menopause
- Pregnancy, for up to 3 months after giving birth. Pregnancy increases the pressure in the veins in the pelvis and legs. The risk of blood clots from pregnancy can continue for up to six weeks after a baby is born. People with an inherited clotting disorder are especially at risk.
- Certain chronic medical illnesses, such as:
- Heart disease. Heart failure. Heart failure increases the risk of DVT and pulmonary embolism. Because the heart and lungs don’t work well in people with heart failure, the symptoms caused by even a small pulmonary embolism are more noticeable.
- Lung disease
- Cancer and its treatment. Some cancers increase substances in the blood that cause the blood to clot. Some types of cancer treatment also increase the risk of blood clots.
- Inflammatory bowel disease (Crohn’s disease or ulcerative colitis)
- Other factors that increase the risk of DVT include:
- Previous personal history of DVT or pulmonary embolism (PE)
- Family history of DVT or pulmonary embolism (PE). If you or someone in your family has had one or both of these conditions, you might be at greater risk of developing DVT.
- Age (risk increases as age increases). Being older than 60 increases the risk of DVT. But DVT can occur at any age.
- Being overweight or obese. Being overweight increases the pressure in the veins in the pelvis and legs.
- A catheter located in a central vein
- Inherited clotting disorders. Some people have DNA changes that cause the blood to clot more easily. One example is factor V Leiden. This inherited disorder changes one of the clotting factors in the blood. An inherited disorder on its own might not cause blood clots unless combined with other risk factors.
- Smoking. Smoking affects how blood flows and clots, which can increase the risk of DVT.
Sometimes, a blood clot in a vein can occur with no identifiable risk factor. This is called an unprovoked venous thromboembolism (VTE).
DVT prevention
Lifestyle changes may help prevent deep vein thrombosis. Try these strategies:
- Move your legs. If you’ve had surgery or have been on bed rest, try to move as soon as possible. Don’t cross your legs while sitting. Doing so can block blood flow. When traveling, take frequent breaks to stretch your legs. When on a plane, stand or walk occasionally. If you’re traveling by car, stop every hour or so and walk around. If you can’t walk, do lower leg exercises. Raise and lower your heels while keeping your toes on the floor. Then raise your toes while keeping your heels on the floor.
- Don’t smoke. Smoking increases the risk of DVT.
- Manage your weight. Obesity is a risk factor for DVT. Regular exercise lowers the risk of blood clots. As a general goal, aim for at least 30 minutes of moderate physical activity every day. If you want to lose weight, maintain weight loss or meet specific fitness goals, you may need to exercise more.
DVT complications
Complications of DVT can include:
- Pulmonary embolism (PE). Pulmonary embolism is a potentially life-threatening complication associated with DVT. It occurs when a blood clot (thrombus) in a leg or other body area breaks free and gets stuck in a blood vessel in a lung. Get immediate medical help if you have symptoms of pulmonary embolism. They include sudden shortness of breath, chest pain while breathing in or coughing, rapid breathing, rapid pulse, feeling faint or fainting, and coughing up blood.
- Postphlebitic syndrome. Damage to the veins from the blood clot reduces blood flow in the affected areas. Symptoms include leg pain, leg swelling, skin color changes and skin sores.
- Treatment complications. Blood thinners are often used to treat DVT. Bleeding (hemorrhage) is a worrisome side effect of blood thinners. It’s important to have regular blood tests while taking blood-thinning drugs.
DVT diagnosis
To diagnose DVT, your health care provider will do a physical exam and ask questions about your symptoms. The provider will check the legs for swelling, tenderness or changes in skin color.
The tests you have depend on whether your doctor thinks you are at a low or a high risk of DVT.
Tests used to diagnose or rule out DVT include:
- D-dimer blood test. D dimer is a type of protein produced by blood clots. Almost all people with severe DVT have increased blood levels of D dimer. This test often can help rule out PE.
- Duplex ultrasound. This noninvasive test uses sound waves to create pictures of how blood flows through the veins. It’s the standard test for diagnosing DVT. For the test, a care provider gently moves a small hand-held device (transducer) on the skin over the body area being studied. Additional ultrasounds may be done over several days to check for new blood clots or to see if an existing one is growing.
- Venography. This test uses X-rays and dye to create a picture of the veins in the legs and feet. The dye is injected into a large vein in the foot or ankle. It helps blood vessels show up more clearly on X-rays. The test is invasive, so it’s rarely done. Other tests, such as ultrasound, often are done first.
- Magnetic resonance imaging (MRI) scan. This test may be done to diagnose DVT in veins of the belly (abdomen).
DVT treatment
There are three main goals to DVT treatment.
- Prevent the clot from getting bigger.
- Prevent the clot from breaking loose and traveling to the lungs.
- Reduce the chances of another DVT.
DVT treatment options include:
- Blood thinners. These medicines, also called anticoagulants, help prevent blood clots from getting bigger. Blood thinners reduce the risk of developing more clots. Blood thinners may be taken by mouth or given by IV or an injection under the skin. There are many different types of blood-thinning drugs used to treat DVT. Together, you and your health care provider will discuss their benefits and risks to determine the best one for you. You might need to take blood thinner pills for three months or longer. It’s important to take them exactly as prescribed to prevent serious side effects. People who take a blood thinner called warfarin (Jantoven) need regular blood tests to monitor levels of the drug in the body. Certain blood-thinning medications are not safe to take during pregnancy.
- Clot busters (thrombolytics). These drugs are used for more-serious types of DVT or PE, or if other medications aren’t working. Clot busters are given by IV or through a tube (catheter) placed directly into the clot. They can cause serious bleeding, so they’re usually only used for people with severe blood clots.
- Filters. If you can’t take medicines to thin your blood, a filter may be placed into a large vein — the vena cava — in your belly (abdomen). A vena cava filter prevents clots that break loose from lodging in the lungs.
- Support stockings (compression stockings). These special knee socks help prevent blood from pooling in the legs. They help reduce leg swelling. Wear them on your legs from your feet to about the level of your knees. For DVT, you typically wear these stockings during the day for a few years, if possible.
Pulmonary embolism
Pulmonary embolism occurs when a clump of material, most often a blood clot (thrombus or embolus), gets wedged in one of the pulmonary arteries in your lungs. These blood clots most commonly come from the deep veins of your legs and rarely from other parts of your body. This condition is known as deep vein thrombosis (DVT).
In most cases, multiple clots are involved but not necessarily all at once. The portions of lung served by each blocked artery are robbed of blood and may die. This is known as pulmonary infarction. This makes it more difficult for your lungs to provide oxygen to the rest of your body.
Occasionally, blockages in the blood vessels are caused by substances other than blood clots, such as:
- Fat from the marrow of a broken long bone
- Collagen or other tissue
- Part of a tumor
- Air bubbles
Because the clots block blood flow to the lungs, pulmonary embolism can be life-threatening. About one-third of people with undiagnosed and untreated pulmonary embolism don’t survive. When the condition is diagnosed and treated promptly, however, that number drops dramatically.
Pulmonary embolism can also lead to pulmonary hypertension, a condition in which the blood pressure in your lungs and in the right side of the heart is too high. When you have obstructions in the arteries inside your lungs, your heart must work harder to push blood through those vessels. This increases the blood pressure within these vessels and the right side of the heart, which can weaken your heart.
In rare cases, small emboli occur frequently and develop over time, resulting in chronic pulmonary hypertension, also known as chronic thromboembolic pulmonary hypertension.
Pulmonary embolism symptoms can vary greatly, depending on how much of your lung is involved, the size of the clots, and whether you have underlying lung or heart disease.
Pulmonary embolism common signs and symptoms include:
- Shortness of breath. This symptom typically appears suddenly and always gets worse with exertion.
- Chest pain. You may feel like you’re having a heart attack. The pain may become worse when you breathe deeply (pleurisy), cough, eat, bend or stoop. The pain will get worse with exertion but won’t go away when you rest.
- Fainting. You may pass out if your heart rate or blood pressure drops suddenly. This is called syncope.
- Cough. The cough may produce bloody or blood-streaked sputum.
Other signs and symptoms that can occur with pulmonary embolism include:
- Leg pain or swelling, or both, usually in the calf
- Clammy or discolored skin (cyanosis)
- Fever
- Excessive sweating
- Rapid or irregular heartbeat
- Lightheadedness or dizziness.
Pulmonary embolism causes
A pulmonary embolism occurs when a clump of material, most often a blood clot, gets stuck in an artery in the lungs, blocking the flow of blood. Blood clots most commonly come from the deep veins of your legs, a condition known as deep vein thrombosis.
In many cases, multiple clots are involved. The portions of lung served by each blocked artery can’t get blood and may die. This is known as a pulmonary infarction. This makes it more difficult for your lungs to provide oxygen to the rest of your body.
Occasionally, blockages in the blood vessels are caused by substances other than blood clots, such as:
- Fat from the inside of a broken long bone
- Part of a tumor
- Air bubbles
Risk factors for getting pulmonary embolism
Although anyone can develop blood clots and subsequent pulmonary embolism, certain factors can increase your risk.
You’re at higher risk if you or any of your family members have had venous blood clots or pulmonary embolism in the past. This may be due to inherited disorders that affect blood, making it more prone to clot.
In addition, some medical conditions and treatments put you at risk, such as:
- Heart disease. Cardiovascular disease, specifically heart failure, makes clot formation more likely.
- Cancer. Certain cancers — especially pancreatic, ovarian and lung cancers, and many cancers with metastasis — can increase levels of substances that help blood clot, and chemotherapy further increases the risk. Women with a personal or family history of breast cancer who are taking tamoxifen or raloxifene also are at higher risk of blood clots.
- Surgery. Surgery is one of the leading causes of problem blood clots. For this reason, medication to prevent clots may be given before and after major surgery such as joint replacement.
Prolonged immobility
Blood clots are more likely to form during periods of inactivity, such as:
- Bed rest. Being confined to bed for an extended period after surgery, a heart attack, leg fracture, trauma or any serious illness makes you more vulnerable to blood clots. When the lower extremities are horizontal for long periods, the flow of venous blood slows and blood can pool in the legs.
- Long trips. Sitting in a cramped position during lengthy plane or car trips slows blood flow in the legs, which contributes to the formation of clots.
Other risk factors
- Smoking. For reasons that aren’t well-understood, tobacco use predisposes some people to blood clot formation, especially when combined with other risk factors.
- Being overweight. Excess weight increases the risk of blood clots — particularly in women who smoke or have high blood pressure.
- Supplemental estrogen. The estrogen in birth control pills and in hormone replacement therapy can increase clotting factors in your blood, especially if you smoke or are overweight.
- Pregnancy. The weight of the baby pressing on veins in the pelvis can slow blood return from the legs. Clots are more likely to form when blood slows or pools.
Pulmonary embolism prevention
Preventing blood clots in the deep veins in your legs will help prevent pulmonary embolisms. For this reason, most hospitals are aggressive about taking measures to prevent blood clots, including:
- Blood thinners (anticoagulants). These medicines are often given to people at risk of clots before and after surgery. Also, they’re often given to people admitted to the hospital with certain medical conditions, such as heart attack, stroke or complications of cancer.
- Compression stockings. Compression stockings steadily squeeze the legs, helping veins and leg muscles move blood more efficiently. They offer a safe, simple and inexpensive way to keep blood from pooling in the legs during and after surgery.
- Leg elevation. Elevating your legs when possible and during the night can be very effective. Raise the bottom of your bed 4 to 6 inches (10 to 15 cm) with blocks or books.
- Physical activity. Moving as soon as possible after surgery can help prevent pulmonary embolism and hasten recovery overall. This is one of the main reasons your nurse may push you to get up, even on your day of surgery, and walk despite pain at the site of your surgical incision.
- Pneumatic compression. This treatment uses thigh-high or calf-high cuffs that automatically inflate with air and deflate every few minutes. This massages and squeezes the veins in your legs and improves blood flow.
Prevention while traveling
The risk of blood clots developing while traveling is low but increases as long-haul travel increases. If you have risk factors for blood clots and you’re concerned about travel, talk with your doctor.
Your doctor might suggest the following to help prevent blood clots during travel:
- Drink plenty of fluids. Water is the best liquid for preventing dehydration, which can contribute to the development of blood clots. Avoid alcohol, which contributes to fluid loss.
- Take a break from sitting. Move around the airplane cabin once an hour or so. If you’re driving, stop every so often and walk around the car a couple of times. Do a few deep knee bends.
- Move in your seat. Bend and make circle movements with your ankles and raise your toes up and down every 15 to 30 minutes.
- Wear support stockings. Your provider may recommend these to help promote circulation and fluid movement in your legs. Compression stockings are available in a range of stylish colors and textures. There are even devices, called stocking butlers, to help you put on the stockings.
Pulmonary embolism complications
A pulmonary embolism can be life-threatening. About one-third of people with an undiagnosed and untreated pulmonary embolism don’t survive. When the condition is diagnosed and treated promptly, however, that number drops dramatically.
Pulmonary embolisms also can lead to pulmonary hypertension, a condition in which the blood pressure in the lungs and in the right side of the heart is too high. When you have blockages in the arteries inside your lungs, your heart must work harder to push blood through those vessels. This increases blood pressure and eventually weakens your heart.
In rare cases, small clots called emboli remain in the lungs and scarring develops in the pulmonary arteries over time. This restricts blood flow and results in chronic pulmonary hypertension.
Pulmonary embolism diagnosis
A pulmonary embolism can be difficult to diagnose, especially if you have underlying heart or lung disease. For that reason, your health care provider will likely discuss your medical history, do a physical exam, and order tests that may include one or more of the following.
- Blood tests. Your doctor may order a blood test for the clot-dissolving substance D dimer. High levels may suggest an increased likelihood of blood clots, although many other factors can cause high D dimer levels. Blood tests also can measure the amount of oxygen and carbon dioxide in your blood. A clot in a blood vessel in your lungs may lower the level of oxygen in your blood. In addition, blood tests may be done to determine whether you have an inherited clotting disorder.
Chest X-ray. Chest X-ray shows images of your heart and lungs on film. Although X-rays can’t diagnose a pulmonary embolism and may even appear fine when a pulmonary embolism exists, they can rule out other conditions with similar symptoms. - Ultrasound. A noninvasive test known as duplex ultrasonography, sometimes called a duplex scan or compression ultrasonography, uses sound waves to scan veins to check for deep vein blood clots. This test can look at veins in the thigh, knee and calf, and sometimes the arms. A wand-shaped device called a transducer is moved over the skin, directing the sound waves to the veins being tested. These waves are then reflected back to the transducer to create a moving image on a computer. The absence of clots reduces the likelihood of deep vein thrombosis. If clots are present, treatment likely will be started immediately.
- CT pulmonary angiography (CTPA) also called a CT pulmonary embolism study. Computed tomography pulmonary angiography (CTPA) takes pictures of your blood vessels and looks for blood clots in the lungs. CT pulmonary angiography creates 3D images that can find changes such as a pulmonary embolism within the arteries in your lungs. In some cases, contrast material is given through a vein in the hand or arm during the CT scan to outline the pulmonary arteries. Computed tomography pulmonary angiography (CTPA) is the main test to diagnose pulmonary embolism.
- Ventilation-perfusion (V/Q) scan. When there is a need to avoid radiation exposure or contrast from a CT scan due to a medical condition, a V/Q scan may be done. In this test, a small amount of a radioactive substance called a tracer is injected into a vein in your arm. The tracer maps blood flow, called perfusion, and compares it with the airflow to your lungs, called ventilation. This test can be used to see if blood clots are causing symptoms of pulmonary hypertension.
- Pulmonary angiogram. This test provides a clear picture of the blood flow in the arteries of your lungs. It’s the most accurate way to diagnose a pulmonary embolism. But because it requires a high degree of skill to perform and has potentially serious risks, it’s usually done when other tests fail to provide a definite diagnosis. In a pulmonary angiogram, a thin, flexible tube called a catheter is inserted into a large vein — usually in your groin — and threaded through your heart and into the pulmonary arteries. A special dye is then injected into the catheter. X-rays are taken as the dye travels along the arteries in your lungs. In some people, this procedure may cause a temporary change in heart rhythm. In addition, the dye may cause increased risk of kidney damage in people with reduced kidney function.
- MRI scan. MRI is a medical imaging technique that uses a magnetic field and computer-generated radio waves to create detailed images of the organs and tissues in your body. MRI is usually only done in those who are pregnant ⸺ to avoid radiation to the baby ⸺ and in people whose kidneys may be harmed by dyes used in other tests.
Pulmonary embolism treatment
Treatment of a pulmonary embolism focuses on keeping the blood clot from getting bigger and preventing new clots from forming. Prompt treatment is essential to prevent serious complications or death. Most people can treat blood clots with medicines at home. Sometimes, more serious blood clots require you to stay in the hospital for treatment.
Treatment can include medicines, surgery and other procedures, and ongoing care.
Medicines. Medicines include different types of blood thinners (anticoagulants) and clot dissolvers (thrombolytics).
- Blood thinners or anticoagulants. Blood-thinning medicines or anticoagulants prevent existing clots from getting bigger and new clots from forming while your body works to break up the clots. Heparin is a frequently used anticoagulant that can be given through a vein or injected under the skin. It acts quickly and is often given along with an oral anticoagulant, such as warfarin (Jantovin), until the oral medicine becomes effective. This can take several days. Newer oral anticoagulants work more quickly and have fewer interactions with other medicines. Some have the advantage of being given by mouth until they’re effective, without the need for heparin. However, all anticoagulants have side effects, and bleeding is the most common.
- Clot dissolvers or thrombolytics. While clots usually dissolve on their own, sometimes thrombolytics ⸺ medicines that dissolve clots ⸺ given through a vein can dissolve clots quickly. Because these clot-busting medicines can cause sudden and severe bleeding, they usually are reserved for life-threatening situations.
Surgical and other procedures
- Clot removal. If you have a large, life-threatening clot in your lung, your health care provider may remove it using a thin, flexible catheter threaded through your blood vessels.
- Vein filter. A catheter also can be used to position a filter in the body’s main vein, the inferior vena cava, that leads from your legs to the right side of your heart. The filter can help keep clots from going to your lungs. This procedure is usually only used for people who can’t take anticoagulant drugs or those who get blood clots even with the use of anticoagulants. Some filters can be removed when no longer needed.
Ongoing care
Because you may be at risk of another deep vein thrombosis or pulmonary embolism, it’s important to continue treatment, such as remaining on anticoagulants and being monitored as often as suggested by your doctor. Also, keep regular visits with your doctor to prevent or treat complications.
Venous thromboembolism prophylaxis
The following tips can help prevent DVT (deep vein thrombosis):
- Move around as soon as possible after having been confined to bed, such as after surgery, illness, or injury.
- If you’re at risk for DVT, talk to your doctor about:
- Graduated compression stockings (sometimes called “medical compression stockings”)
- Medication (anticoagulants) to prevent DVT.
- When sitting for long periods of time, such as when traveling for more than four hours:
- Get up and walk around every 2 to 3 hours.
- Exercise your legs while you’re sitting by:
- Raising and lowering your heels while keeping your toes on the floor
- Raising and lowering your toes while keeping your heels on the floor
- Tightening and releasing your leg muscles
- Wear loose-fitting clothes.
- You can reduce your risk by maintaining a healthy weight, avoiding a sedentary lifestyle, and following your doctor’s recommendations based on your individual risk factors.
Preventing clots in the deep veins in your legs (deep vein thrombosis) will help prevent pulmonary embolism. For this reason, most hospitals are aggressive about taking measures to prevent blood clots, including:
- Blood thinners (anticoagulants). These medications are often given to people at risk of clots before and after an operation — as well as to people admitted to the hospital with a heart attack, stroke or complications of cancer.
- Compression stockings. Compression stockings steadily squeeze your legs, helping your veins and leg muscles move blood more efficiently. They offer a safe, simple and inexpensive way to keep blood from stagnating during and after general surgery.
- Leg elevation. Elevating your legs when possible and during the night also can be very effective. Raise the bottom of your bed 4 to 6 inches with blocks or books.
- Physical activity. Moving as soon as possible after surgery can help prevent pulmonary embolism and hasten recovery overall. This is one of the main reasons your nurse may push you to get up, even on your day of surgery, and walk despite pain at the site of your surgical incision.
- Pneumatic compression. This treatment uses thigh-high or calf-high cuffs that automatically inflate with air and deflate every few minutes to massage and squeeze the veins in your legs and improve blood flow.
Venous thromboembolism prevention while traveling
The risk of blood clots developing while traveling is low, but increases as travel increases. If you have risk factors for blood clots and you’re concerned about traveling, talk with your doctor.
Your doctor might suggest the following to help prevent blood clots during travel:
- Drink plenty of fluids. Water is the best liquid for preventing dehydration, which can contribute to the development of blood clots. Avoid alcohol, which contributes to fluid loss.
- Take a break from sitting. Move around the airplane cabin once an hour or so. If you’re driving, stop every hour and walk around the car a couple of times.
- Do a few deep knee bends.
- Fidget in your seat. Flex your ankles every 15 to 30 minutes.
- Wear support stockings. Your doctor may recommend these to help promote circulation and fluid movement in your legs. Compression stockings are available in a range of stylish colors and textures. There are even devices, called stocking butlers, to help you put on the stockings.
Venous thromboembolism symptoms
Deep vein thrombosis (DVT) signs and symptoms
People with DVT may develop pain, swelling and tenderness. Only about half the people with DVT have typical symptoms, so diagnosis is difficult. A big misconception is that there should be something visible with DVT. Most DVTs are associated with leg pain or mild swelling only, and the perception that there should be obvious symptoms has likely resulted in many delayed or missed diagnoses of venous thromboembolism. It is the combination of risk factors and these symptoms that is important.
When symptoms do occur the most common are:
- Sudden swelling of one leg. Rarely, there’s swelling in both legs.
- Pain or tenderness in the calf muscle or groin. The pain often starts in your calf and can feel like cramping or soreness.
- Skin that is warm to the touch on the legs
- Fullness of the veins just beneath the skin (seeing these veins more easily or if they look swollen)
- Changes in skin color (blue, red or very pale)
Symptoms like these can develop slowly, but can also develop suddenly. These symptoms are not unique to DVT and can be associated with other conditions. If you have these symptoms you should contact your health care provider immediately.
Pulmonary embolism signs and symptoms
Signs and symptoms of pulmonary embolism occur quickly and need prompt attention. The symptoms of pulmonary embolism are different than for DVT.
Pulmonary embolism symptoms include:
- Shortness of breath
- Sharp chest pain usually with breathing in or when taking a deep breath
- A feeling of apprehension
- Sudden collapse or fainting
- Rapid pulse
- Coughing
- Sweating
- Bloody phlegm (coughing up blood)
These symptoms are not unique to pulmonary embolism and can be associated with many other conditions. Unfortunately, a majority of people with pulmonary embolism, unlike DVT, will experience uncommon symptoms such as dizziness, back pain or wheezing. However, because pulmonary embolism can be fatal, if you experience these signs or symptoms seek medical attention right away.
Venous thromboembolism diagnosis
To diagnose deep vein thrombosis, your doctor will ask you about your symptoms. You’ll also have a physical exam so that your doctor can check for areas of swelling, tenderness or discoloration on your skin. Depending on how likely you are to have a blood clot, your doctor might suggest tests, including:
- Ultrasound. The easiest and most reliable method for diagnosing deep vein thrombosis is an ultrasound exam. This test is simple, painless, safe and widely available. A wandlike device (transducer) placed over the part of your body where there’s a clot sends sound waves into the area. As the sound waves travel through your tissue and reflect back, a computer transforms the waves into a moving image on a video screen. A clot might be visible in the image. Sometimes a series of ultrasounds are done over several days to determine whether a blood clot is growing or to check for a new one.
- Blood test. Almost all people who develop severe deep vein thrombosis have an elevated blood level of a substance called “D-dimer”. A specific blood test may be performed to measure “D-dimer” which is a sign of recent and active clotting. When this test is negative, it is very unlikely that you have suffered a DVT.
- Venography. A dye is injected into a large vein in your foot or ankle. An X-ray creates an image of the veins in your legs and feet, to look for clots. However, less invasive methods of diagnosis, such as ultrasound, can usually confirm the diagnosis.
- CT or MRI scans. Either can provide visual images of your veins and might show if you have a clot. Sometimes these scans performed for other reasons reveal a clot.
Pulmonary embolism may be diagnosed by a special type of chest CT scan, a lung scan or less commonly by an invasive procedure known as a pulmonary angiogram.
- Spiral CT scan: In a spiral (helical) CT scan, the scanner rotates around your body in a spiral — like the stripe on a candy cane — to create 3-D images. This type of CT can detect abnormalities within the arteries in your lungs with much greater precision than conventional CT scans. In some cases, contrast material is given intravenously during the CT scan to outline the pulmonary arteries.
- Pulmonary angiogram: Pulmonary angiogram test provides a clear picture of the blood flow in the arteries of your lungs. It’s the most accurate way to diagnose pulmonary embolism, but because it requires a high degree of skill to administer and has potentially serious risks, it’s usually performed when other tests fail to provide a definitive diagnosis. In a pulmonary angiogram, a flexible tube (catheter) is inserted into a large vein — usually in your groin — and threaded through into your heart and on into the pulmonary arteries. A special dye is then injected into the catheter, and X-rays are taken as the dye travels along the arteries in your lungs. One risk of this procedure is a temporary change in your heart rhythm. In addition, the dye may cause kidney damage in people with decreased kidney function.
- MRI scan: MRI scans use radio waves and a powerful magnetic field to produce detailed images of internal structures. Because MRI is expensive, it’s usually reserved for pregnant women (to avoid radiation to the fetus) and people whose kidneys may be harmed by dyes used in other tests.
Venous thromboembolism treatment
Deep vein thrombosis (DVT) treatment
Deep vein thrombosis (DVT) treatment is aimed at preventing the clot from getting bigger and preventing it from breaking loose and causing a pulmonary embolism. Then the goal becomes reducing your chances of deep vein thrombosis happening again.
Deep vein thrombosis treatment options include:
- Blood thinners. Deep vein thrombosis is most commonly treated with anticoagulants, also called blood thinners. These drugs, which can be injected or taken as pills, decrease your blood’s ability to clot. They don’t break up existing blood clots, but they can prevent clots from getting bigger and reduce your risk of developing more clots. The injectable medications can be given as a shot under the skin or by injection into your arm vein (intravenous). Heparin is typically given intravenously. Other similar blood thinners, such as enoxaparin (Lovenox), dalteparin (Fragmin) or fondaparinux (Arixtra), are injected under the skin. You might receive an injectable blood thinner for a few days, after which pills such as warfarin (Coumadin, Jantoven) or dabigatran (Pradaxa) are started. Once warfarin has thinned your blood, the injectable blood thinners are stopped. Other blood thinners can be given in pill form without the need for an injectable blood thinner. These include rivaroxaban (Xarelto), apixaban (Eliquis) or edoxaban (Savaysa). You might need to take blood thinner pills for three months or longer. It’s important to take them exactly as your doctor instructs because taking too much or too little can cause serious side effects. If you take warfarin, you’ll need periodic blood tests to check how long it takes your blood to clot. Pregnant women shouldn’t take certain blood-thinning medications.
- Clot busters. If you have a more serious type of deep vein thrombosis or pulmonary embolism, or if other medications aren’t working, your doctor might prescribe drugs that break up clots quickly, called clot busters or thrombolytics. These drugs are either given through an IV line to break up blood clots or through a catheter placed directly into the clot. These drugs can cause serious bleeding, so they’re generally reserved for severe cases of blood clots.
- Filters. If you can’t take medicines to thin your blood, you might have a filter inserted into a large vein — the vena cava — in your abdomen. A vena cava filter prevents clots that break loose from lodging in your lungs.
- Compression stockings. To help prevent swelling associated with deep vein thrombosis, these are worn on your legs from your feet to about the level of your knees. This pressure helps reduce the chances that your blood will pool and clot. You should wear these stockings during the day for at least two years, if possible.
Once you receive treatment for deep vein thrombosis (DVT), you need to watch your diet and watch for signs of excessive bleeding, as well as take steps to prevent another DVT. Some things you can do include:
- Check in with your doctor regularly to see if your treatment needs to be modified. If you’re taking warfarin (Coumadin, Jantoven), you’ll need a blood test to see how well your blood is clotting.
- Take your blood thinners as directed. If you’ve had DVT, you’ll be on blood thinners for at least three to six months.
- Watch for excessive bleeding, which can be a side effect of taking blood thinners. Talk to your doctor about activities that could cause you to bruise or get cut, as even a minor injury could become serious if you’re taking blood thinners.
- Move. If you’ve been on bed rest because of surgery or other factors, the sooner you get moving, the less likely blood clots will develop.
- Wear compression stockings to help prevent blood clots in the legs if your doctor recommends them.
Pulmonary embolism treatment
Pulmonary embolism treatment is aimed at keeping the blood clot from getting bigger and preventing new clots from forming. Prompt treatment is essential to prevent serious complications or death.
Medications
- Blood thinners (anticoagulants). These drugs prevent new clots from forming while your body works to break up the clots. Heparin is a frequently used anticoagulant that can be given through the vein or injected under the skin. It acts quickly and is often overlapped for several days with an oral anticoagulant, such as warfarin, until it becomes effective, which can take days. A newer class of anticoagulants, referred to as novel oral anticoagulants (NOACs), has been tested and approved for treatment of venous thromboembolism, including pulmonary embolism. These medications work quickly and have fewer interactions with other medications. Some NOACs have the advantage of being given by mouth, without the need for overlap with heparin. However, all anticoagulants have side effects, with bleeding being the most common.
- Clot dissolvers (thrombolytics). While clots usually dissolve on their own, there are medications given through the vein that can dissolve clots quickly. Because these clot-busting drugs can cause sudden and severe bleeding, they usually are reserved for life-threatening situations.
Surgical and other procedures
- Clot removal (thrombectomy or embolectomy). If you have a very large, life-threatening clot in your lung, your doctor may suggest removing it via a thin, flexible tube (catheter) threaded through your blood vessels.
- Vein filter. A catheter can also be used to position a filter in the body’s main vein — called the inferior vena cava — that leads from your legs to the right side of your heart. This filter can help keep clots from being carried into your lungs. This procedure is typically reserved for people who can’t take anticoagulant drugs or when anticoagulant drugs don’t work well enough or fast enough. Some filters can be removed when they are no longer needed.
What is arterial thromboembolism
Arterial thromboembolism is a term referring to blood clot (a thrombus) that forms in an artery. Arterial thromboembolism is the major cause of obstruction of the blood supply to an organ or region of tissue, typically by a thrombus (blood clot in an artery) or embolus (a blood clot, piece of fat or atheromatous plaque or atheroma which has broken off and been carried in the bloodstream to lodge in a distant blood vessel), causing local death of the tissue (infarction). The blockage starves tissues of blood and oxygen. This can result in damage or tissue death (necrosis). Most arteries are blood vessels that takes oxygen-rich blood away from your heart to your entire body (tissues, lungs, brain etc.) 3. Arteries are part of the circulatory system, that is responsible for the delivery of oxygen and nutrients to all cells, as well as the removal of carbon dioxide and waste products, the maintenance of optimum blood pH, and the circulation of proteins and cells of the immune system. With the exception of the pulmonary and the umbilical arteries, which carry oxygen-poor blood (deoxygenated blood) to the organs that oxygenate it (lungs and placenta, respectively). In contrast, veins are blood vessels that carry oxygen-poor blood (deoxygenated blood) back towards your heart.
Arterial thromboembolism often occur in your legs and feet. Some may occur in your brain causing a stroke, or in your heart causing a heart attack (myocardial infarction). Less common sites include the kidneys, intestines, and eyes 4.
Arterial thromboembolism signs and symptoms may begin quickly or slowly depending on the size of the embolus and how much it blocks the blood flow 4. Symptoms of embolization in an organ vary with the organ involved but commonly include:
- Pain in the involved body part
- Temporarily decreased organ function
Later symptoms are closely related to infarction (death) of the affected tissue. This may cause permanently decreased organ function. For example, symptoms of heart attack (myocardial infarction) mainly include chest pain, shortness of breath (dyspnea), excessive sweating (diaphoresis), weakness, light-headedness, nausea, vomiting, and palpitations (rapid heart rate). Symptoms of limb infarction include coldness, decreased or no pulse beyond the site of blockage, pain, muscle spasm, numbness and tingling, pallor and muscle weakness, possibly to paralysis in the affected limb.
Arterial thromboembolism causes
An arterial thromboembolism is caused by one or more emboli getting stuck in an artery and blocking blood flow, causing ischemia, possibly resulting in infarction with tissue death (necrosis). The most common cause of arterial thromboembolism is due to cholesterol-containing deposits called plaques. Plaques can build up in the walls of the arteries, reducing blood flow. If a plaque breaks open, it can cause a blood clot (thrombus) in the artery blocking most or all of the oxygen-carrying blood from flowing to that part of your body. An “embolus” is a blood clot or a piece of plaque that acts like a clot. When the blood clot travels from the site where it formed to another location in the body, it is called an embolism.
An arterial embolism may be caused by one or more blood clots. The blood clots can get stuck in the main artery or one of the smaller arteries blocking their blood flow. The blockage starves tissues of blood and oxygen. This can result in damage or tissue death (necrosis).
Arterial emboli often occur in the legs and feet. Emboli that occur in the brain cause a stroke. Ones that occur in the heart cause a heart attack. Less common sites include the kidneys, intestines, and eyes.
Risk factors for arterial thromboembolism
Risk factors for arterial thromboembolism include:
- Abnormal heart rhythms causing disturbed blood flow in your heart such as atrial fibrillation
- Injury or damage to an artery wall
- Conditions that increase blood clotting (hypercoagulability state) or blood clotting disorders
- Advanced age
- Cigarette smoking. Smoking and long-term exposure to secondhand smoke can damage the inside walls of arteries. The damage can allow deposits of cholesterol and other substances to collect and slow blood flow in the coronary arteries. Smoking causes the coronary arteries to spasm and may also increase the risk of blood clots.
- Cancer 5, 6
- Hypertension (high blood pressure). Over time, high blood pressure can accelerate atherosclerosis, resulting in damage to the coronary arteries and other arteries in your body.
- Obesity. Obesity is associated with diabetes, high blood pressure and high blood cholesterol levels.
- Hyperlipidemia, e.g. hypercholesterolemia, hypertriglyceridemia, elevated lipoprotein A or apolipoprotein B, or decreased levels of HDL cholesterol). Cholesterol is a major part of the deposits that can narrow your coronary arteries. A high level of “bad” (low-density lipoprotein, or LDL) cholesterol in your blood may be due to an inherited condition or a diet high in saturated fats and cholesterol. Triglycerides, another type of blood fat, also may contribute to atherosclerosis.
- Diabetes. Type 1 and type 2 diabetes are linked to an increased risk of myocardial ischemia, heart attack and other heart problems.
- Sedentary lifestyle
- Lack of physical activity. Not getting enough exercise contributes to obesity and is linked to higher cholesterol and triglyceride levels. People who get regular aerobic exercise have better heart health, which is associated with a lower risk of myocardial ischemia and heart attack. Exercise also reduces blood pressure.
- Stress. Stress can include:
- Losing a job (or starting a new one).
- Your child leaving or returning home.
- The death of your spouse or love one.
- Divorce or marriage.
- Illness or injury for you or a close family member.
- Money problems.
- Having or adopting a baby.
- Recent surgery (both for thromboembolism and air embolism)
- Previous stroke or cardiovascular disease
- A history of long-term intravenous therapy (for air embolism)
- Bone fracture (for fat embolism)
Another condition that poses a high risk for embolization (especially to the brain) is mitral stenosis. Endocarditis (infection of the inside of the heart) can also cause arterial thromboembolism.
A common source for an embolus is from areas of atherosclerosis in the aorta and other large blood vessels. These blood clots can break loose and flow down to your legs and feet.
Paradoxical embolization can take place when a clot in a vein enters the right side of the heart and passes through a hole into the left side of the heart. The blood clot can then move to an artery and block blood flow to the brain (stroke) or other organs.
If a clot travels and lodges in the arteries supplying blood flow to the lungs, it is called a pulmonary embolus.
Arterial thromboembolism prevention
Prevention begins with finding possible sources of a blood clot. Your doctor may prescribe blood thinners (such as warfarin or heparin) to prevent clots from forming. Antiplatelet drugs may also be needed. If your blood cholesterol is high your doctor may prescribe a healthy diet, regular exercise and sometimes medication to help reduce high cholesterol.
The same lifestyle habits that can help treat arterial thromboembolism can also help prevent it from developing in the first place. Leading a healthy lifestyle can help keep your arteries strong, elastic and smooth, and allow for maximum blood flow.
A healthy lifestyle can help prevent arterial thromboembolism includes:
- Quitting smoking if you smoke and avoiding secondhand smoke
- Following a healthy diet that is low in fat and cholesterol
- Losing weight if you’re overweight or obese
- Exercising regularly
- Managing stress. To reduce your stress you can:
- Get enough sleep. It’s important to get enough sleep so your body has time to repair itself.
- Meditate. Meditation is a form of guided thought. It can take many forms. You can do it with exercise that uses the same motions over and over, like walking or swimming. You can meditate by practicing relaxation training, by stretching, or by breathing deeply.
- Do relaxation training. Start with one muscle. Hold it tight for a few seconds and then relax. Do this with each of your muscles, beginning with the toes and feet and working your way up through the rest of your body.
- Do stretching can also help relieve tension. Roll your head in a gentle circle. Reach toward the ceiling and bend side to side slowly. Roll your shoulders.
- Do deep, relaxed breathing by itself may help relieve stress. This helps you get plenty of oxygen and activates your body’s relaxation response.
- Let go. Don’t worry about things you can’t control, such as the weather.
- Don’t sweat the small stuff. Solve the little problems. This can help you gain a feeling of control.
- Be ready. Prepare to the best of your ability for events you know may be stressful, such as a job interview.
- Chin up. Try to look at change as a positive challenge, not as a threat.
- Work it out. Resolve conflicts with other people.
- Talk it out. Discuss what’s bothering you with a trusted friend, family member, or counselor.
- Keep it real. Set realistic goals at home and at work. Avoid over scheduling.
- Have some fun. Participate in something you don’t find stressful, such as sports, social events, or hobbies.
- Just say no. Stay away from drugs and alcohol. They can actually increase your stress levels.
- Talk with a friend, family member, or health care professional.
- Controlling your blood pressure
- Managing your blood sugar (if you have diabetes)
- Seeing your doctor regularly for check-ups
Arterial thromboembolism signs and symptoms
Arterial thromboembolism signs and symptoms may begin quickly or slowly depending on the size of the embolus and how much it blocks the blood flow 4.
Symptoms of an arterial embolism in the arms or legs may include:
- Cold arm or leg
- Decreased or no pulse in an arm or leg
- Lack of movement in the arm or leg
- Pain in the affected area
- Numbness and tingling in the arm or leg
- Pale color of the arm or leg (pallor)
- Weakness of an arm or leg
Later symptoms:
- Blisters of the skin fed by the affected artery
- Shedding (sloughing) of skin
- Skin erosion (ulcer)
- Tissue death (necrosis; skin is dark and damaged)
Symptoms of a clot in an organ vary with the organ involved but may include:
- Pain in the part of the body that is involved
- Temporarily decreased organ function
Arterial thromboembolism complications
Arterial thromboembolism may include:
- Acute myocardial infarction or heart attack. If a coronary artery becomes completely blocked, the lack of blood and oxygen can lead to a heart attack that destroys part of the heart muscle. The damage can be serious and sometimes fatal. Over time, repeated episodes of heart ischemia may lead to heart failure.
- Infection in the affected tissue
- Septic shock
- Stroke (CVA)
- Temporary or permanent decrease or loss of other organ functions
- Temporary or permanent kidney failure
- Tissue death (necrosis) and gangrene
- Transient ischemic attack (TIA)
Arterial thromboembolism diagnosis
Your doctor may find decreased or no pulse, and decreased or no blood pressure in the arm or leg. There may also be signs of tissue death or gangrene.
Tests to diagnose arterial embolism or reveal the source of emboli may include:
- Angiography of the affected extremity or organ
- Doppler ultrasound exam of an extremity
- Duplex Doppler ultrasound exam of extremity
- Duplex Doppler ultrasound exam of arteries to the brain
- Echocardiogram
- MRI of the arm or leg
- Myocardial contrast echocardiography (MCE)
- Plethysmography
- Transcranial Doppler exam of arteries to the brain
- Transesophageal echocardiography (TEE)
This disease may also affect the results of the following tests:
- D-dimer
- Factor VIII assay
- Isotope study of the affected organ
- Plasminogen activator inhibitor-1 (PAI-1) activity
- Platelet aggregation test
- Tissue-type plasminogen activator (t-PA) levels
Arterial thromboembolism treatment
Arterial embolism requires prompt treatment at a hospital. The goals of treatment are to control symptoms and to improve the interrupted blood flow to the affected area of the body. The cause of the clot, if found, should be treated to prevent further problems.
Medicines include:
- Anticoagulants (such as warfarin or heparin or one of the newer blood thinners such as apixaban, rivaroxaban, edoxaban, or dabigatran) can prevent new clots from forming
- Antiplatelet medicines (such as aspirin or clopidogrel) can prevent new clots from forming
- Painkillers given through a vein (by IV)
- Thrombolytics (such as streptokinase) can dissolve clots
Some people need surgery. Procedures include:
- Bypass of the artery (arterial bypass) to create a second source of blood supply
- Clot removal through a balloon catheter placed into the affected artery or through open surgery on the artery (embolectomy)
- Opening of the artery with a balloon catheter (angioplasty) with or without a stent
Arterial thromboembolism prognosis
How well a person does depends on the location of the blood clot and how much the clot has blocked blood flow and for how long the blockage has been present. Arterial thromboembolism can be very serious if not treated promptly. The affected area can be permanently damaged. Amputation is needed in up to 1 in 4 cases. Arterial emboli can come back even after successful treatment.
- How Does Blood Clot? https://www.nhlbi.nih.gov/health/clotting-disorders/how-blood-clots[↩]
- What Is Venous Thromboembolism? https://www.nhlbi.nih.gov/health/venous-thromboembolism[↩]
- Mercadante AA, Raja A. Anatomy, Arteries. [Updated 2023 Mar 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK547743[↩]
- Arterial embolism. https://medlineplus.gov/ency/article/001102.htm[↩][↩][↩]
- Mulder FI, Horváth-Puhó E, van Es N, Pedersen L, Büller HR, Bøtker HE, Sørensen HT. Arterial Thromboembolism in Cancer Patients: A Danish Population-Based Cohort Study. JACC CardioOncol. 2021 Apr 20;3(2):205-218. doi: 10.1016/j.jaccao.2021.02.007[↩]
- Navi BB, Reiner AS, Kamel H, Iadecola C, Okin PM, Elkind MSV, Panageas KS, DeAngelis LM. Risk of Arterial Thromboembolism in Patients With Cancer. J Am Coll Cardiol. 2017 Aug 22;70(8):926-938. doi: 10.1016/j.jacc.2017.06.047[↩]