
Contents
What is antiphospholipid syndrome
Antiphospholipid antibody syndrome also known as Hughes syndrome, is an immune disorder characterized by the presence of abnormal antibodies (antiphospholipid antibodies) in the blood associated with abnormal blood clotting, migraine headaches, recurrent pregnancy losses (repeat spontaneous abortions), and low blood platelet counts (thrombocytopenia). The antiphospholipid abnormal antibodies are directed against phospholipids. Phospholipids are fats that contains phosphorous). Antiphospholipid antibody syndrome can occur by itself (primary) or be caused by an underlying condition (secondary), such as systemic lupus erythematosus. About a third of persons with primary antiphospholipid antibody syndrome have heart valve abnormalities. Antiphospholipid antibodies reduce the levels of annexin V, a protein that binds phospholipids and has potent anticoagulant activity. The reduction of annexin V levels is thought to be a possible mechanism underlying the increased tendency of blood to clot and the propensity to pregnancy loss characteristic of the antiphospholipid antibody syndrome.
This means people with antiphospholipid syndrome are at greater risk of developing conditions such as:
- Deep vein thrombosis (DVT), a blood clot that usually develops in the leg
- Arterial thrombosis (a clot in an artery), which can cause a stroke or heart attack
- Blood clots in the brain, leading to problems with balance, mobility, vision, speech and memory
- Recurrent pregnancy loss (miscarriage)
- A decrease in the number of blood platelets (thrombocytopenia)
Pregnant women with antiphospholipid syndrome also have an increased risk of having a miscarriage, although the exact reasons for this are uncertain.
Antiphospholipid syndrome doesn’t always cause noticeable problems, but some people have general symptoms that can be similar to those of multiple sclerosis (a common condition affecting the central nervous system).
Antiphospholipid syndrome can affect people of all ages, including children and babies. However, most people are diagnosed with antiphospholipid syndrome between 20 and 50 years of age, and it affects three to five times as many women as men. Actual frequency of antiphospholipid syndrome in the general population is unknown. On the other hand, antiphospholipid antibody tends to occur more frequently in elderly individuals.
People with antiphospholipid syndrome are at increased risk from an early age of death or disability caused by stroke, heart attack, pulmonary embolism and renal failure.
There are a number of classifcations of antiphospholipid antibody syndrome:
- Primary antiphospholipid syndrome: No associated disorder;
- Secondary antiphospholipid syndrome: Those clearly exhibiting features of an autoimmune disease such as systemic lupus erythematosus (SLE);
- Catastrophic antiphospholipid syndrome: Formation of many thrombi in multiple locations in a short space of time.
Antiphospholipid antibody syndrome may be found in the blood of up to 50% of people affected by systemic lupus erythematosus. However these antibodies have also been found in 1-5% of apparently healthy individuals.
Antiphospholipid antibody syndrome prognosis
Most individuals with primary antiphospholipid syndrome lead normal healthy lives with appropriate medication and lifestyle modifications. However, subsets of patients continue to have thrombotic events despite aggressive therapies. For these patients, the disease course can be devastating, often leading to significant morbidity or early mortality. Patients with secondary antiphospholipid syndrome carry a similar prognosis; however, morbidity and mortality may also be influenced by their underlying autoimmune or rheumatic condition.
Antiphospholipid syndrome complications
Depending on which organ is affected by a blood clot and how severe the obstruction of blood flow to that organ is, untreated antiphospholipid syndrome can lead to permanent organ damage or death. Complications include:
- Kidney failure. This can result from decreased blood flow to your kidneys.
- Stroke. Decreased blood flow to a part of your brain can cause a stroke, which can result in permanent neurological damage, such as partial paralysis and loss of speech (aphasia).
- Cardiovascular problems. A blood clot in your leg can damage the valves in the veins, which keep blood flowing to your heart. This can result in chronic swelling and discoloration in your lower legs (chronic venous insufficiency). Another possible complication is heart damage.
- Lung problems. These can include high blood pressure in your lungs (pulmonary hypertension) and pulmonary embolism.
- Pregnancy complications. These can include miscarriages, stillbirths, premature delivery, slow fetal growth and high blood pressure during pregnancy (preeclampsia).
Rarely, a person can have repeated clotting events in a short time, leading to progressive damage in multiple organs (catastrophic antiphospholipid syndrome).
Catastrophic antiphospholipid syndrome
In very rare cases, in people who develop catastrophic antiphospholipid syndrome, blood clots suddenly form throughout the body, resulting in multiple organ failure. This is known as catastrophic antiphospholipid syndrome.
Catastrophic antiphospholipid syndrome is a rare but serious complication of antiphospholipid syndrome. It occurs in less than 1% of people with antiphospholipid syndrome.
Catastrophic antiphospholipid syndrome requires immediate emergency treatment in hospital with high-dose anticoagulants.
It’s not clear what causes catastrophic antiphospholipid syndrome, but one case in five occurs after an infection, trauma or surgery.
The initial symptoms can be wide-ranging, depending on which organs are involved. Symptoms may include:
- loss of blood supply to the tips of your fingers or toes, causing them to go dark blue or black
- swollen ankles, feet or hands
- increasing breathlessness
- abdominal (tummy) pain
- blood in your urine
- confusion
- seizures (fits)
- coma
The symptoms usually develop suddenly and rapidly get worse.
Immediate admission to an intensive care unit (ICU) is required for people with catastrophic antiphospholipid syndrome so the body’s functions can be supported. High-dose anticoagulants are used to stop the blood clots getting bigger while they are slowly absorbed by the body.
However, even with the best available treatment, an estimated 50% of people die as a result of the condition.
Antiphospholipid syndrome causes
It’s not known what causes the immune system to produce abnormal antibodies. As with other autoimmune conditions, genetic, hormonal and environmental factors are thought to play a part.
In antiphospholipid syndrome, the immune system produces abnormal antibodies called antiphospholipid antibodies. The main antiphospholipid antibodies associated with antiphospholipid syndrome include lupus anticoagulant, cardiolipin antibody and beta-2 glycoprotein 1 (β2GP1) antibody. These target proteins attached to fat molecules (phospholipids), which makes the blood more likely to clot. These antibodies increase an affected person’s risk of developing recurrent inappropriate blood clots in both veins and arteries. Those with antiphospholipid syndrome may experience a single thrombotic episode or have multiple occurrences. Symptoms and complications may range from mild to critical. Blood clots that form can obstruct blood flow and can damage tissues and organs. If they are carried to the lungs, heart, brain or kidneys, they can cause a pulmonary embolism, heart attack, stroke and/or kidney damage. A small subset of people with antiphospholipid syndrome may have widespread thrombotic disease with damage to many of the large internal organs of the body (viscera), referred to as catastrophic antiphospholipid syndrome.
Those with antiphospholipid antibodies may have antiphospholipid syndrome and another co-existing autoimmune disorder such as systemic lupus erythematosus (SLE) or may have one or more of the antibodies present with no associated symptoms. Antiphospholipid antibodies may be seen in those with HIV, some cancers, in the elderly and temporarily, with infections (e.g. Q fever) and with drugs such as phenothiazines and procainamide. They may also be found in 1 per cent to 5 per cent of healthy people.
Antiphospholipid syndrome may affect anyone but is most frequently seen in women of child-bearing age and in those with another autoimmune disorder.
This increases the risk of blood clots developing in the blood vessels, which can lead to serious health problems, such as:
- deep vein thrombosis (DVT)
- strokes
- heart attacks
It’s not clear why these abnormal antibodies are produced, or why many people have antiphospholipid antibodies but don’t develop blood clots.
A combination of genetic and environmental factors is thought to be responsible.
Antiphospholipid antibodies
Antibodies are proteins produced by the immune system to help fight off infection and illness.
They’re part of the body’s defence system and produced to help protect against ‘foreign invaders’, such as bacteria and viruses. Antibodies signal the immune system to release chemicals to kill these bacteria and viruses and to prevent infection spreading.
In antiphospholipid syndrome, the immune system produces abnormal antibodies which, rather than attacking bacteria and viruses, mistakenly attack proteins found on the outside of cells in the blood and blood vessels.
It’s not known how this causes the blood to clot more easily. However, most experts believe that keeping your blood at the correct consistency (not too runny and not too sticky) is a delicate balancing act that relies on different types of proteins and fats working together. This balance may be disrupted by the abnormal antibodies in people with antiphospholipid syndrome.
Genetic factors
Research into the genetics around antiphospholipid syndrome is still at an early stage, but it seems the genes you inherit from your parents may play a role in the development of abnormal antiphospholipid antibodies.
Antiphospholipid syndrome isn’t passed down directly from parents to children in the same way as other conditions, such as hemophilia and sickle cell anemia. However, having a family member with antiphospholipid antibodies increases the chance of your immune system also producing them.
Studies have shown that some people with antiphospholipid syndrome have a faulty gene that plays a role in other autoimmune conditions, such as lupus. This may explain why some people develop antiphospholipid syndrome alongside another immune system condition.
Environmental factors
It’s thought that one or more environmental triggers may be needed to trigger antiphospholipid syndrome in some people.
Environmental factors that may be responsible include:
- viral infections, such as the cytomegalovirus (CMV) or parvovirus B19
- bacterial infections, such as E. coli (a bacteria often associated with food poisoning) or leptospirosis (an infection usually spread by certain animals)
- certain medications, such as anti-epileptic medicine or the oral contraceptive pill
Another theory is that many people with abnormal antiphospholipid antibodies only go on to develop antiphospholipid syndrome if they have a higher risk of developing blood clots. For example, if they:
- eat an unhealthy diet, leading to high cholesterol levels in the blood
- don’t do enough exercise
- take the contraceptive pill or hormone replacement therapy (HRT)
- smoke
- are obese
However, this doesn’t explain why some children and adults who don’t have any of these risk factors still develop antiphospholipid syndrome.
Risk factors for antiphospholipid antibody syndrome
Antiphospholipid syndrome affects women much more than it does men. Other risk factors include:
- Having an autoimmune condition, such as systemic lupus erythematosus or Sjogren’s syndrome
- Having certain infections, such as syphilis, HIV/AIDS, hepatitis C or Lyme disease
- Taking certain medications, such as hydralazine for high blood pressure, the heart rhythm-regulating medication quinidine, the anti-seizure medication phenytoin (Dilantin) and the antibiotic amoxicillin
- Having a family member with antiphospholipid syndrome
Risk factors for developing symptoms
It’s possible to have the antibodies associated with antiphospholipid syndrome without developing signs or symptoms. However, having these antibodies increases your risk of developing blood clots, particularly if you:
- Become pregnant
- Are immobile for a time, such as being on bed rest or sitting during a long flight
- Have surgery
- Smoke cigarettes
- Take oral contraceptives or estrogen therapy for menopause
- Have high cholesterol and triglycerides levels.
Antiphospholipid syndrome symptoms
In antiphospholipid syndrome, your immune system produces abnormal antibodies that make the blood ‘stickier’ than normal.
The symptoms associated with antiphospholipid syndrome will vary from person to person and with each thrombotic episode. With pregnant women, antiphospholipid syndrome may cause recurrent miscarriages, pre-eclampsia and premature births but no distinguishable symptoms. Symptoms associated with a blood clot depend on where the clot forms in the body and the damage that occurs.
Antiphospholipid syndrome signs and symptoms may include:
- High blood pressure
- Deep vein thrombosis (DVT)
- A stroke or a transient ischemic attack (TIA) or ‘mini-stroke’
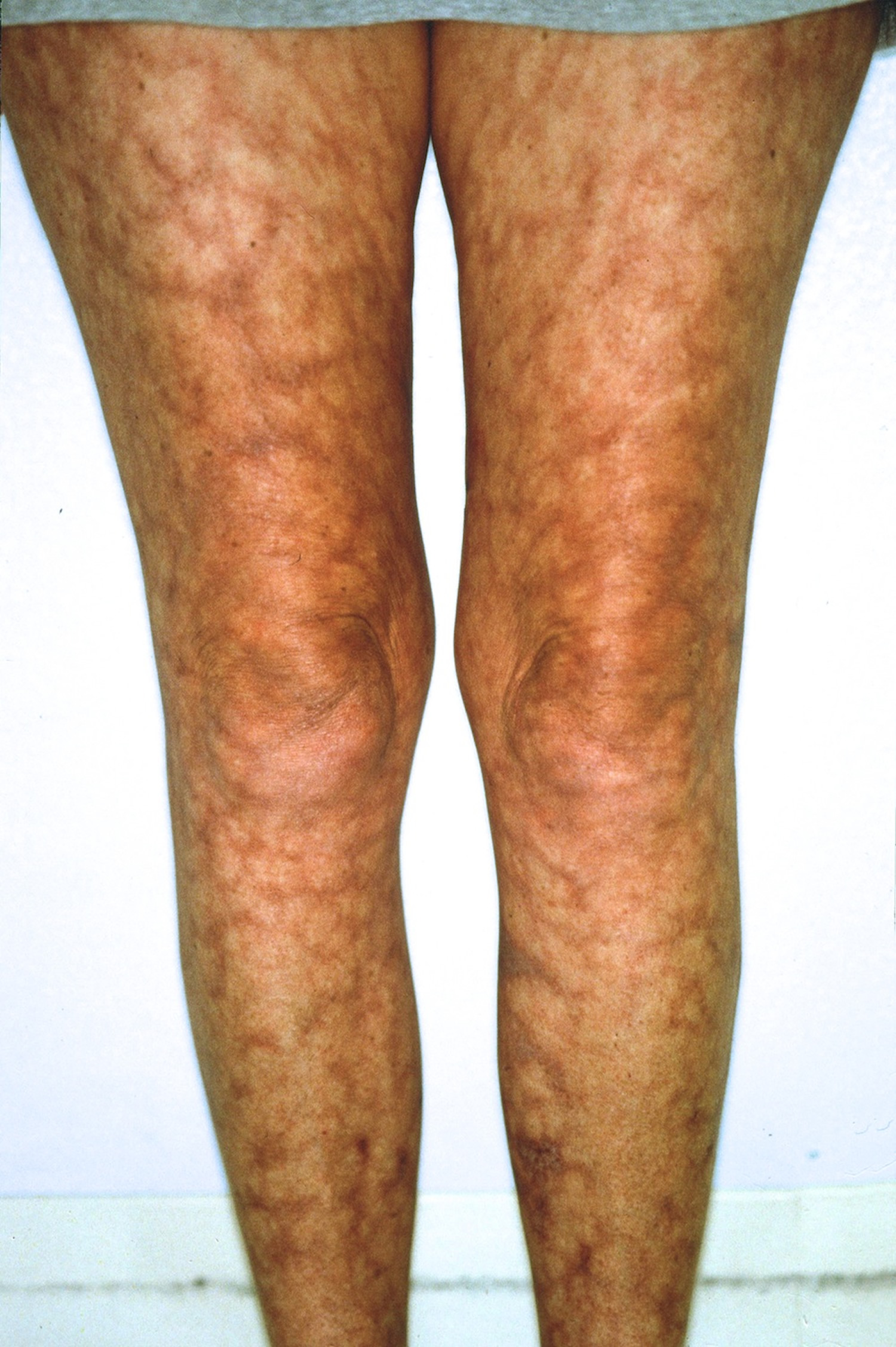
- A red lacy rash on the arms or legs (livedo reticularis) (see Figure 1)
- Heart attacks
- Pulmonary embolism – a blockage in one of the blood vessels in the lungs
- Persistent headaches
- Chest pain
- Shortness of breath
- Nausea
- Speech and/or cognitive changes
- Seizures
- Redness, swelling, and pain in a leg or arm
- Skin ulcers
- Mild to severe bleeding (with significant thrombocytopenia)
Less common signs and symptoms include:
- Neurological symptoms. Chronic headaches, including migraines; dementia and seizures are possible when a blood clot blocks blood flow to parts of your brain.
- Cardiovascular disease. Antiphospholipid syndrome can damage heart valves.
- Bleeding. Some people have a decrease in blood cells needed for clotting (platelets). If you have this condition (thrombocytopenia), you might have few or no symptoms.
However, if your platelet count drops too low, you might have episodes of bleeding, particularly from your nose and gums. You can also bleed into your skin, which will appear as patches of small red spots (petechiae).
People with antiphospholipid syndrome may also experience any of the following symptoms:
- balance and mobility problems
- vision problems, such as double vision
- speech and memory problems
- a tingling sensation or pins and needles in your arms or legs
- fatigue (extreme tiredness)
- repeated headaches or migraines
Livedo reticularis
Livedo reticularis is a skin condition caused by small blood clots that develop inside the blood vessels of the skin.
It causes the skin to take on a blotchy red or blue appearance. Some people also develop ulcers (sores) and nodules (bumps). These symptoms are often more severe in cold weather.
Figure 1. Livedo reticularis
Superficial thrombophlebitis
Superficial thrombophlebitis is inflammation of the veins just under your skin, usually in your leg. The symptoms are similar to DVT but they’re not usually as severe.
The symptoms of superficial thrombophlebitis include:
- swelling
- redness and tenderness along the affected vein
- a high temperature of 100.4 °F (38 °C) or above (although this is less common)
The symptoms usually resolve within two to six weeks.
Figure 2. Superficial thrombophlebitis

Antiphospholipid syndrome pregnancy
Women with antiphospholipid syndrome have a much higher risk of developing complications during pregnancy, particularly if it’s not treated. Possible complications include:
- recurrent (three or more) early miscarriages, usually during the first 10 weeks of pregnancy
- one or more later miscarriages, usually after week 10 of pregnancy
- premature birth, usually at or before week 34 of pregnancy, which may be caused by pre-eclampsia (where a woman develops high blood pressure during pregnancy)
If you have antiphospholipid syndrome and you’re thinking about getting pregnant, ask your doctor what treatments are available during your pregnancy.
Antiphospholipid syndrome diagnosis
Diagnosing antiphospholipid syndrome can sometimes be tricky, as some of the symptoms are similar to multiple sclerosis.
An accurate diagnosis of antiphospholipid syndrome (antiphospholipid syndrome) is important because blood clots can have serious consequences.
Therefore, blood tests to identify the antibodies responsible for antiphospholipid syndrome are essential in diagnosing the condition.
Diagnosis of antiphospholipid syndrome is based on the results of specific blood tests and a medical assessment.
If antiphospholipid syndrome is suspected, you’ll usually be referred to hospital to see either:
- a hematologist (specialist in conditions affecting the blood)
- a rheumatologist (specialist in conditions affecting the immune system)
Specific blood tests
To diagnose antiphospholipid syndrome, the blood needs to be tested for the abnormal antiphospholipid antibodies that increase the risk of blood clots. This requires a blood test specifically designed for look for these antibodies.
A diagnosis of antiphospholipid syndrome can only be made after two abnormal blood test results, with at least a 12-week gap between them.
This is because harmless antiphospholipid antibodies can sometimes develop in the body for short periods of time. Usually this is a result of an infection or a side effect of medication, such as antibiotics.
If antiphospholipid antibodies are identified during the first blood test, another test will be needed at a later date to confirm whether the abnormal antibodies are still present.
Blood tests that are used to detect the presence of autoantibodies include:
- Lupus anticoagulant testing (e.g. DRVVT)
- Cardiolipin antibodies
- Beta2 glycoprotein 1 (β2GP1) antibodies
Other tests that may be ordered include:
- Activated partial thromboplastin time (PTT, to evaluate blood clotting)
- Full blood count (FBC, to evaluate blood cells and platelets)
- A variety of additional tests to evaluate other causes for a person’s symptoms, such as 1:1 Mix study (dilute PTT) to detect lupus anticoagulant activity
Table 1. Revised Classification Criteria for the Antiphospholipid Antibody Syndrome*
| Clinical criteria | Laboratory criteria |
|---|---|
Vascular thrombosis:
Pregnancy complications:
| Positive test for one of the autoantibodies must be present on two or more occasions at least 12 weeks apart:
|
| *Established in 2006 by the 11th International Congress on Antiphospholipid Antibodies | |
Medical assessment
If blood tests confirm you have antiphospholipid syndrome, your medical history will be carefully assessed to check whether you’ve experienced any previous symptoms that may be caused by antiphospholipid syndrome.
A diagnosis of antiphospholipid syndrome can usually be confirmed if you’ve had:
- one or more confirmed blood clots
- one or more unexplained late miscarriages, at or after week 10 of your pregnancy
- one or more premature births, at or before week 34 of your pregnancy
- three or more unexplained early miscarriages, before week 10 of your pregnancy.
Non-Laboratory Tests
Imaging scans may be performed to confirm a thrombotic episode, to locate a blood clot, evaluate organ damage, and to monitor a fetus. These may include:
- CT scan
- MRI
- Ultrasounds to detect blood clots and to monitor fetal health and growth
- Echocardiograph to detect heart valve abnormalities that can occur with antiphospholipid syndrome
Antiphospholipid syndrome treatment
Antiphospholipid antibody syndrome treatment
Although there’s no cure for antiphospholipid syndrome, the risk of developing blood clots can be greatly reduced if it’s correctly diagnosed.
Treatment for antiphospholipid syndrome aims to reduce your risk of developing more blood clots.
An anticoagulant medicine such as warfarin or an antiplatelet such as low-dose aspirin is usually prescribed. These reduce the likelihood of unnecessary blood clots forming but still allow clots to form when you cut yourself.
Treatment with these medications can also improve a pregnant woman’s chance of having a successful pregnancy. With treatment, it’s estimated there’s about an 80% chance of having a successful pregnancy.
Most people respond well to treatment and can lead normal, healthy lives. However, a small number of people with antiphospholipid syndrome continue to experience blood clots despite extensive treatment.
Medication
As part of your treatment you’ll be prescribed anticoagulant medicine such as warfarin, or an antiplatelet medication such as low-dose aspirin.
These work by interrupting the process of blood clot formation. This means blood clots are less likely to form when they’re not needed.
Your treatment plan
Most people with antiphospholipid syndrome need to take anticoagulant or antiplatelet medication daily for the rest of their life.
If blood tests show you have abnormal antiphospholipid antibodies, but you don’t have a history of blood clots, low-dose aspirin tablets are usually recommended. If you can’t take aspirin, you may be prescribed an alternative antiplatelet tablet called clopidogrel.
Warfarin tablets are usually recommended if you have antiphospholipid syndrome and a history of blood clots, such as previously having deep vein thrombosis (DVT) or a stroke. However, this needs to be changed if you become pregnant or are planning a pregnancy (see below). Tell your doctor if this is the case.
If you develop a blood clot or your symptoms suddenly become severe, injections of an anticoagulant called heparin may be needed. These injections may be given in hospital, or you may be trained to give them yourself.
Standard initial treatment
If you have thrombosis, standard initial treatment involves a combination of blood-thinning (anticoagulant) medications.
- Heparin. Typically, you’ll first be given an injection of the blood thinner heparin, combined with another blood thinner in pill form, likely warfarin (Coumadin, Jantoven).
- Warfarin. After several days of combined heparin and warfarin, your doctor might discontinue the heparin and continue the warfarin, possibly for the rest of your life.
- Aspirin. In some cases, your doctor might recommend adding low-dose aspirin to your treatment plan.
Side effects
Side effects of these medications are uncommon and generally mild, such as indigestion or feeling sick (nausea).
However, there’s a risk that the disruption to the blood’s ability to clot can cause excessive bleeding (a hemorrhage).
Symptoms of excessive bleeding can include:
- blood in your urine or feces
- black feces
- severe bruising
- prolonged nosebleeds (lasting longer than 10 minutes)
- blood in your vomit
- coughing up blood
Treatment during pregnancy
Women diagnosed with antiphospholipid syndrome are strongly advised to plan for any future pregnancy. This is because treatment to improve the outcome of a pregnancy is most effective when it begins as soon as possible after an attempt to conceive. Some medications used to treat antiphospholipid syndrome can also harm an unborn baby.
If you don’t plan your pregnancy, it may be several weeks before you realize you’re pregnant. This may increase the risk of treatment to safeguard the pregnancy being unsuccessful.
Treatment during pregnancy involves taking daily doses of aspirin or heparin, or a combination of both. This depends on whether you have a history of blood clots and previous complications during pregnancy. Warfarin isn’t recommended during pregnancy because it carries a small risk of causing birth defects.
Treatment with aspirin and/or heparin is usually started at the beginning of the pregnancy and may continue for one to six weeks after you have given birth.
- Heparin. Some forms of heparin — enoxaparin (Lovenox) and dalteparin (Fragmin) — are known as low-molecular-weight heparin, which you can inject yourself under your skin (subcutaneously). Heparin is considered safe to take during pregnancy.
- Aspirin. If you’re pregnant, your doctor might recommend taking one tablet of aspirin daily in addition to the heparin, to increase your chances of a successful pregnancy.
Possible future treatments
Several new treatments are being considered for antiphospholipid syndrome, including:
- New blood thinners (anticoagulants). A number of oral blood thinners — dabigatran (Pradaxa), rivaroxaban (Xarelto) and apixaban (Eliquis) — have recently been approved to treat other conditions. It’s not clear yet if these drugs are appropriate for treating antiphospholipid syndrome. None is recommended for use during pregnancy or breast-feeding.
- Rituximab (Rituxan). This drug has been used successfully to treat conditions affecting the immune system. But there isn’t yet enough evidence of benefit to recommend rituximab as a treatment for antiphospholipid syndrome.
Lifestyle changes
If you’re diagnosed with antiphospholipid syndrome, it’s important to take all possible steps to reduce your risk of developing blood clots. Effective ways of achieving this include:
- not smoking
- eating a healthy, balanced diet – low in fat and sugar and containing plenty of fruit and vegetables
- taking regular exercise
- maintaining a healthy weight and losing weight if you are obese (have a body mass index of 30 or more)
If you take anticoagulants
Take extra care to keep from injuring yourself and to avoid bleeding.
- Avoid contact sports or other activities that could cause bruising or injury or cause you to fall.
- Use a soft toothbrush and waxed floss.
- Shave with an electric razor.
- Take extra care when using knives, scissors and other sharp tools.
Certain foods and medications may affect how well your anticoagulants work. Ask your doctor for guidance about:
- Safe dietary choices. Vitamin K can lessen the effectiveness of warfarin, but not other anticoagulants. Eating small amounts of vitamin K-rich foods might not be harmful, but avoid eating large amounts of avocado, broccoli, Brussels sprouts, cabbage, leafy greens and garbanzo beans. On the other hand, cranberry juice and alcohol can increase warfarin’s blood-thinning effect. Ask your doctor if you need to limit or avoid these drinks.
- Safe medications and dietary supplements. Certain medications, vitamins and herbal products can interact dangerously with warfarin. These include some over-the-counter pain relievers, cold medicines, stomach remedies or multivitamins, as well as garlic, ginkgo and green tea products.





{kind=link}