
Contents
What is thumb arthritis
Basal thumb arthritis is a common condition seen in hand clinics across the US and is often associated with other pathological conditions such as carpal tunnel syndrome and scaphotrapezial arthritis. The base of the thumb, primarily the trapeziometacarpal joint [also known as the carpometacarpal joint] (see Figures 1, 2 and 3), is the second most common site affected by primary idiopathic arthritis in the hand behind only the distal joints of the fingers. Typically, patients complain of pain localized to the base of the thumb. This pain is often activity related, particularly after excessive use involving forceful pinch.
In a normal thumb joint, cartilage covers the ends of the bones — acting as a cushion and allowing the bones to glide smoothly against each other. With thumb arthritis, the cartilage that covers the ends of the bones deteriorates, and its smooth surface roughens. The body reacts to loss of the joint surface by forming bone spurs (osteophytes). The bones then rub against each other, resulting in friction and joint damage.
The damage to the joint might result in growth of new bone along the sides of the existing bone (bone spurs), which can produce noticeable lumps on your thumb joint.
Thumb arthritis can cause severe pain, swelling, and decreased strength and range of motion, making it difficult to do simple tasks, such as turning doorknobs and opening jars.
The prevalence of basal thumb arthritis increases with age and is seen predominantly in postmenopausal women 1. The female:male ratio is 6:1. No conclusive environmental or genetic factors that lead to the expression of this disease have been identified.
A detailed history and examination is normally all that is needed to make the diagnosis. Provocative manoeuvres may be helpful in localizing symptoms to the basal joint with degenerative changes or synovitis. Radiographs are useful for confirming the diagnosis and staging the disease in order to plan for surgery. The mainstay of initial treatment of basal thumb arthritis of any stage is activity modifications, rest, nonsteroidal anti‐inflammatory drugs, exercises and splinting. A variety of surgical procedures are available to treat the condition when conservative measures have failed, in order to control symptoms and improve function.
Figure 1. Thumb joint (trapeziometacarpal joint of the thumb)
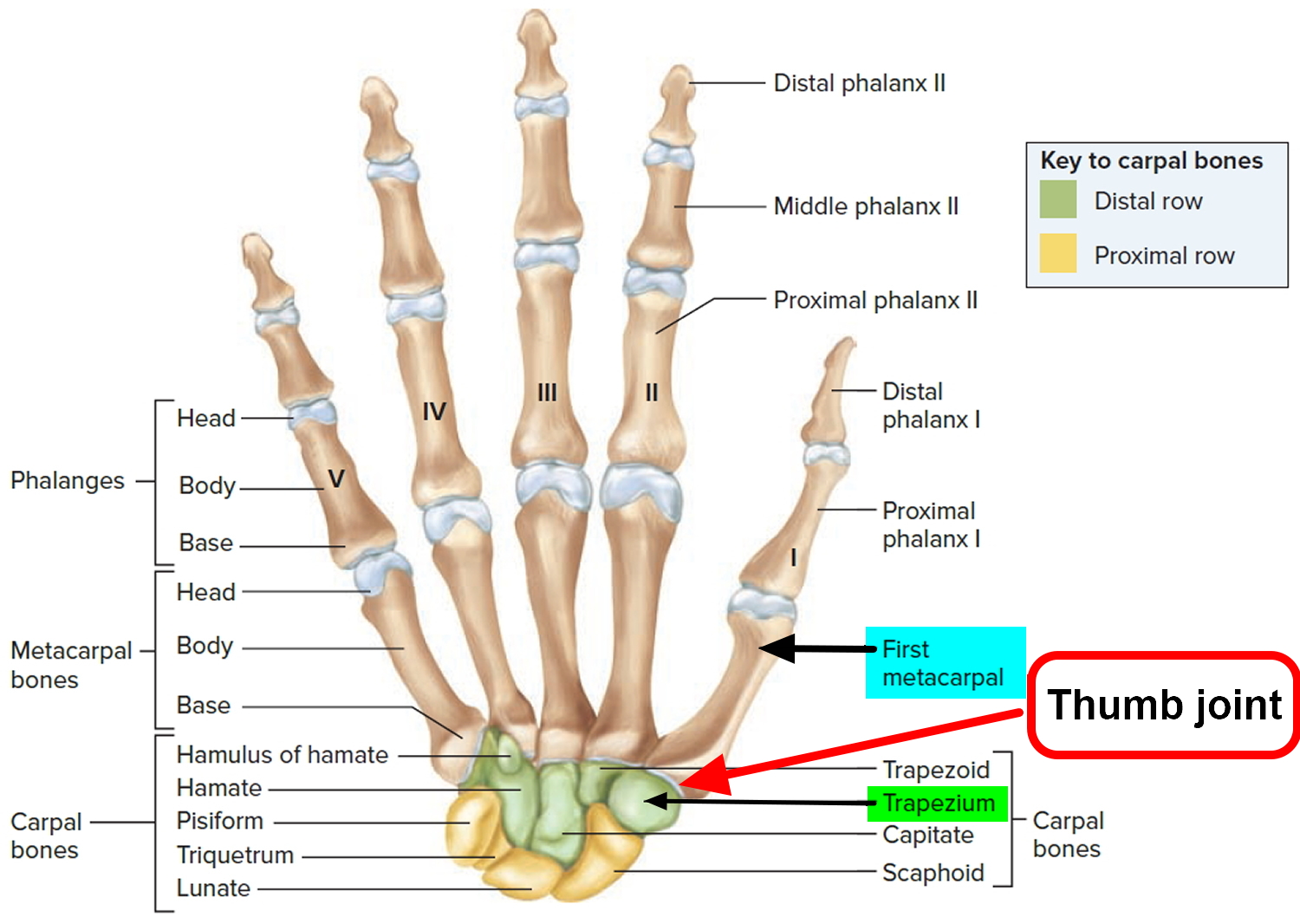
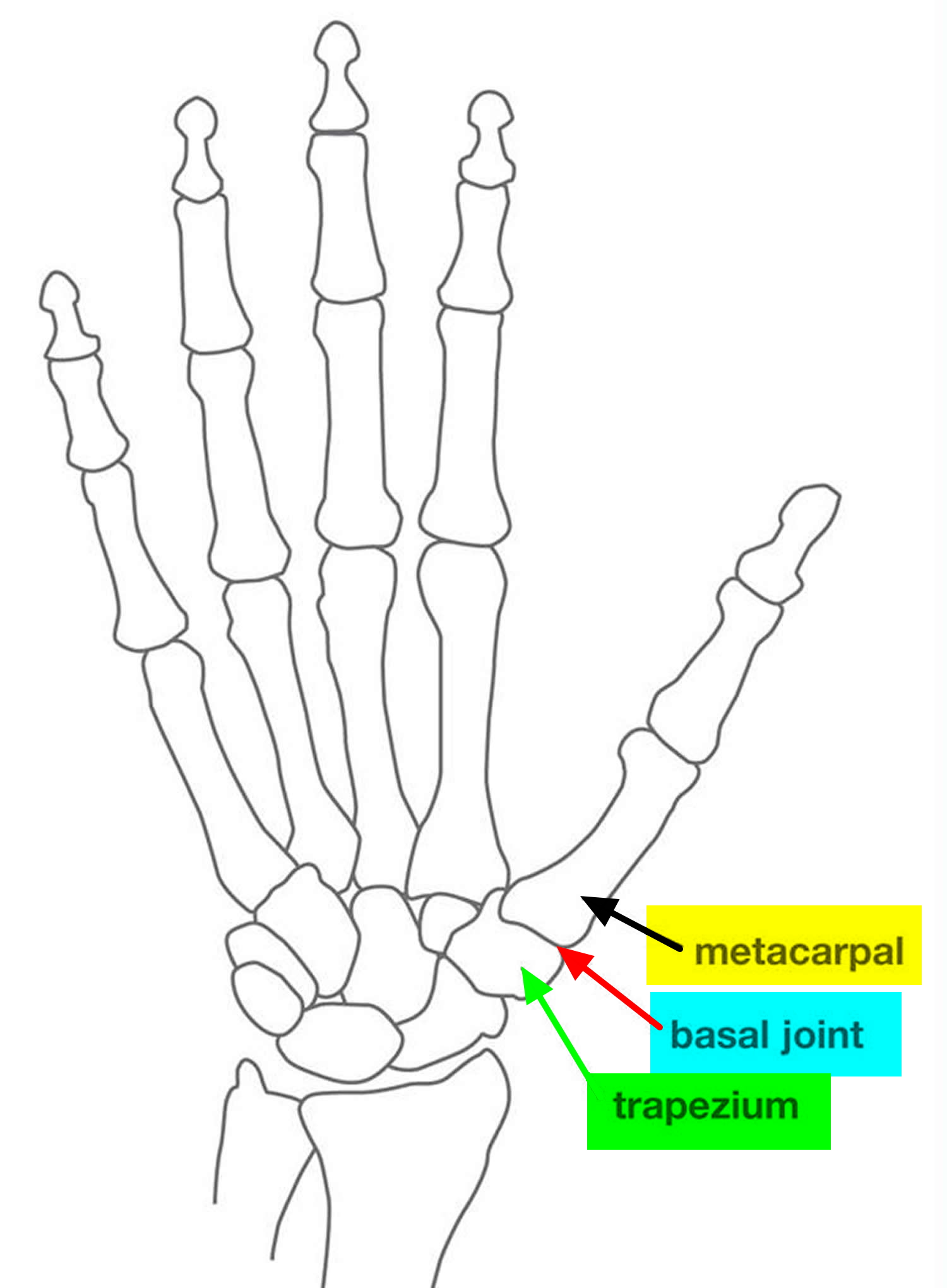 Figure 3. X-ray of arthritis in thumb joint (stage IV basal thumb arthritis)
Figure 3. X-ray of arthritis in thumb joint (stage IV basal thumb arthritis)
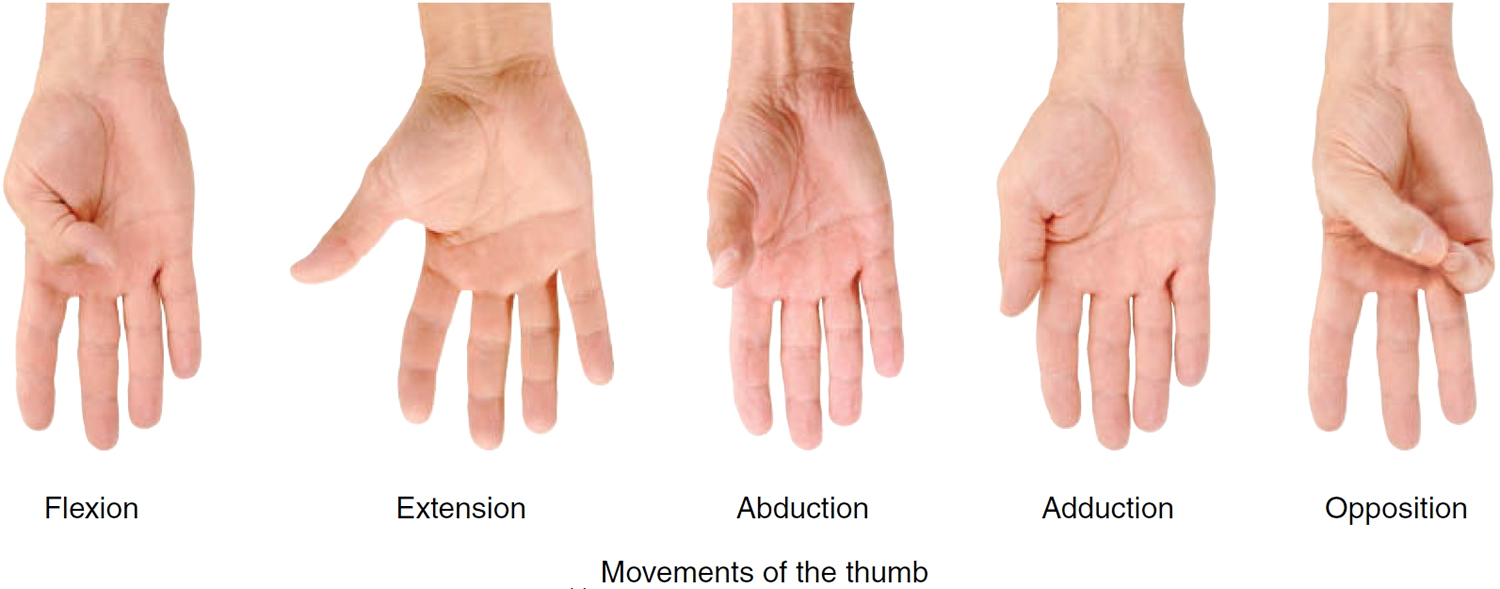
The carpometacarpal or trapeziometacarpal joint of the thumb is known as nature’s universal joint. It is a saddle‐shaped joint and allows a wide range of movement in three planes. Movements of the thumb are very important in the precise activities of the hand, and they are defined in different planes from comparable movements of other digits because the thumb is positioned at a right angle to the other digits. The five principal movements of the thumb are illustrated in Figure 3 and include flexion (movement of the thumb medially across the palm), extension (movement of the thumb laterally away from the palm), abduction (movement of the thumb in an anteroposterior plane away from the palm), adduction (movement of the thumb in an anteroposterior plane toward the palm), and opposition (movement of the thumb across the palm so that the tip of the thumb meets the tip of a finger). Opposition is the single most distinctive digital movement that gives humans and other primates the ability to grasp and manipulate objects precisely. This increase in mobility, however, renders the thumb joint prone to degeneration.
Figure 4. Thumb movements
Associated conditions
Other conditions may also be associated with basal thumb arthritis, such as carpal tunnel syndrome, scaphotrapezial arthrosis, trigger digits, metacarpophalangeal hyperextension and tenosynovitis of the wrist 2. Florack et al 3 noted that 43% of their patients who underwent surgery for arthritis to the base of the thumb had carpal tunnel syndrome. The prevalence of compression neuropathy was found to be higher in women and in patients with diabetes. The basal joint is in close proximity to the carpal tunnel and hence inflammation in one site can spread to a neighboring site. In addition, the skeletal changes that occur at the basal joint can affect the dimensions of the carpal tunnel, leading to reduced volume for the median nerve.16 It is therefore important to inquire about these conditions to make a comprehensive diagnosis and tailor the treatment accordingly.
Basal thumb arthritis causes
The most common cause for symptomatic basal joint arthritis, is idiopathic (unknown) 4.
Scientists found a strong association between excessive basal joint laxity and the development of premature degenerative changes in the thumb joint 5. Ligamentous laxity is common in young women. Repeated loading of subluxed joints in the 20s, 30s and 40s may be the reason why one third of women >50 years show some radiological evidence of degenerative change 6.
Previous trauma to the thumb can predispose the patient to basal joint arthritis.
Fractures that involve the articular base of the metacarpal are commonly known as Rolando or Bennett fractures, and if left to heal in a malunited position, can lead to degeneration 7.
Inflammatory arthritis, such as rheumatoid arthritis, is another predisposing condition. The most common site of upper extremity involvement in the population with rheumatoid arthritis is the distal radioulnar joint and one third of these patients will have basal joint involvement 8.
Risk factors for thumb arthritis
Factors that can increase your risk of thumb arthritis include:
- Female sex.
- Age above 40 years.
- Obesity.
- Certain hereditary conditions, such as joint ligament laxity and malformed joints.
- Injuries to your thumb joint, such as fractures and sprains.
- Diseases that change the normal structure and function of cartilage, such as rheumatoid arthritis. Although osteoarthritis is the most common cause of thumb arthritis, rheumatoid arthritis can also affect the CMC joint, usually to a lesser extent than other joints of the hand.
- Activities and jobs that put high stress on the thumb joint.
Thumb arthritis signs and symptoms
Patients with thumb arthritis report pain and weakness with pinching, gripping and grasping or or use your thumb to apply force. For instance, opening jars, turning doorknobs or keys, and writing are often painful. Typically, patients have pain localized to the base of the thumb, often radiating to the thenar eminence and the metacarpophalangeal joint 9. The pain in basal thumb arthritis is often activity related, particularly after excessive use involving forceful pinch. Daily activities such as grasping large objects, unscrewing jar tops, turning doorknobs and writing can exacerbate symptoms 10. As the arthritis progresses, pain may become constant. In addition to pain, weakness or loss of motion are commonly reported 2. These symptoms are a protective mechanism to prevent excessive use of a damaged joint. In the later stages of the disease when instability and subluxation (partial dislocation) of the joint occurs, patients report an inability to abduct the thumb, weakness of pinch grip and a deterioration of hand function 11. As a result, the thumb cannot be brought far enough away from the index finger to grasp large objects. Collapse of the thumb may eventually occur, producing a swan‐neck deformity with progressive adduction of the first metacarpal and compensatory hyperextension of the metacarpophalangeal joint (Figure 5).
Other signs and symptoms might include:
- Swelling, stiffness and tenderness at the base of your thumb
- Decreased strength when pinching or grasping objects
- Decreased range of motion
- Enlarged or bony appearance of the joint at the base of your thumb
Figure 5. Zig-zag deformity in severe cases of thumb arthritis due to a collapse into the palm

Thumb arthritis diagnosis
The diagnosis is made by talking with you and examining you. The appearance of the thumb can change with the development of bone spurs and stretching of soft tissues (ligaments) (see X-ray in Figure 3 and Z deformity in Figure 5).
Tenderness is usually well localized over the joint, and this can be reproduced with thumb and finger pressure applied directly over the affected joint. Crepitus evident on examination implies erosion of the articular cartilage 12.
Provocative manoeuvres may be helpful in localizing symptoms to the basal joint with degenerative changes or synovitis. The“grind” test is performed by rotating the thumb metacarpal base while applying axial compression (i.e, compression along the plane of the metacarpal bone) 13. When the test is positive, the resulting pain is suggestive of degenerative disease. A grinding sensation may also be present at the joint (see Figure 3). The “distraction” or “torque” test is performed by rotating the thumb metacarpal base while applying gentle axial traction. A positive test is indicative of synovitis associated with milder disease as a result of traction on an inflamed joint capsule 13. These tests, however, are more commonly used in a specialist hand surgery setting.
X-rays are not necessary to make the diagnosis, but they can help you understand the disease and they can help when surgery is being considered.
Table 1. Classification system for basal joint arthritis of the thumb
| Stage | Radiographic changes |
|---|---|
| I | Normal trapeziometacarpal joint contours with <1/3 joint subluxation |
| II | Trapeziometacarpal joint narrowing and osteophytes or loose bodies <2 mm. Instability apparent on stress views. ⩾1/3 joint subluxation |
| III | Trapeziometacarpal joint narrowing, subchondral sclerosis, osteophytes or loose bodies >2 mm. ⩾1/3 joint subluxation |
| IV | Advanced disease of trapeziometacarpal and scaphotrapezial joint |
Thumb arthritis treatment
As with other aspects of aging, we adapt to thumb arthritis and treatment is often unnecessary. Options for treatment include non-surgical methods and surgery. Treatments without surgery range from ice/heat, pain medicines, splinting, and injections.
The mainstay of initial treatment of basal thumb arthritis of any stage is activity modifications, rest, non‐steroidal anti‐inflammatory drugs, and thenar intrinsic and extrinsic muscle strengthening exercises 14.
Examples of activity modification include less forceful pinching, alternate hand use and switching to larger‐diameter writing instruments.
Thumb arthritis Splint
The hand is rested by immobilising the base of the thumb in a splint 15. A splint can support your joint and limit the movement of your thumb and wrist. You might wear a splint just at night or throughout the day and night.
Splints can help:
- Decrease pain
- Encourage proper positioning of your joint while you complete tasks
- Rest your joint
Patients may already be wearing a splint obtained from a chemist, which is often a standard wrist immobiliser that leaves the thumb free to move, thereby exacerbating the symptoms. The most effective splint for immobilising and resting the basal joint is a well‐fitted custom‐made splint fashioned by a qualified hand therapist (see Figures 6 and 7). This is usually in the form of a long opponens or thumb spica splint 15. Initially, splinting is usually continuous for 3 or 4 weeks, and in combination with non‐steroidal anti‐inflammatory drugs (NSAIDs). If there is improvement after this, the splint can be worn during the day and the patients gradually wean themselves from the splint over the course of 1 month, or make intermittent use thereafter when the thumb is symptomatic or under heavy load. If there is no improvement of symptoms after 2 months, surgical options can be discussed.
Use of a long thumb splint (Figure 7) to immobilize the wrist and thumb for 6 weeks has been found to have a greater degree of symptom relief in early stage disease as compared to later stage disease, but is recommended as an initial treatment for all patients 16. A shorter splint that allows freedom of wrist motion may be better tolerated by some patients and can be effective in resting the Trapeziometacarpal joint as well (Figure 6). In one recent study of 33 patients followed over 7 years hand therapy and splinting helped 70% avoid surgery altogether 17.
Figure 6. Thumb arthritis spica splint

Figure 7. Custom molded long thumb splint

Medication
To relieve pain, your doctor might recommend:
- Over-the counter pain relievers, such as acetaminophen (Tylenol, others), ibuprofen (Advil, Motrin IB, others) or naproxen (Aleve)
- Prescription pain relievers, such as celecoxib (Celebrex) or tramadol (Conzip, Ultram)
Hand therapy
Therapy for early stage disease may also include thenar muscle strengthening and education in how to modify pinch-grasp activities, so as to load the joint without undue shear stress. Modalities such as heat and massage may offer temporary relief of symptoms. Aside from the fabrication of custom molded splints, the hand therapist has little to offer patients with late stage arthritis.
Injections
If pain relievers and a splint aren’t effective, your doctor might recommend injecting a long-acting corticosteroid into your thumb joint. Corticosteroid injections can offer temporary pain relief and reduce inflammation.
Corticosteroid injections of the trapeziometacarpal joint can be useful when conservative measures have not worked 18. Pain relief can be effective and last from a few days to several months. Repetitive injections, however, have a diminishing effect and can theoretically weaken the capsular support of the joint and further compromise the articular cartilage 12.
Thumb arthritis surgery
If you don’t respond to other treatments or if you’re barely able to bend and twist your thumb, your doctor might recommend surgery.
Surgery consists of removing the joint either by removing a bone or connecting the bones together.
There are options for moving one of your tendons to secure or cushion the bone, and each hand surgeon has a different opinion on whether this is helpful.
Options include:
- Joint fusion (arthrodesis). The bones in the affected joint are permanently fused. The fused joint can bear weight without pain, but has no flexibility.
- Osteotomy. The bones in the affected joint are repositioned to help correct deformities.
- Trapeziectomy. One of the bones in your thumb joint (trapezium) is removed.
- Joint replacement (arthroplasty). All or part of the affected joint is removed and replaced with a graft from one of your tendons.
These surgeries can all be done on an outpatient basis. After surgery, you can expect to wear a cast or splint over your thumb and wrist for up to six weeks. Once the cast is removed, you might have physical therapy to help you regain hand strength and movement.
Lifestyle and home remedies
To ease pain and improve joint mobility, try to:
- Modify hand tools. Consider purchasing adaptive equipment — such as jar openers, key turners and large zipper pulls — designed for people with limited hand strength. Replace traditional door handles, which you must grasp with your thumb, with levers.
- Apply cold. Icing the joint for five to 15 minutes several times a day can help relieve swelling and pain.
Thumb arthritis exercises
Start with your hand in a neutral, relaxed position with your fingers and thumb straightened. Next, bend your thumb across your palm, touching the tip of your thumb to the bottom of your small finger. If you can’t make your thumb touch, just stretch as far as you can. Return your thumb to the starting position. Repeat this exercise multiple times with each hand.

Hand exercises can help improve joint flexibility and range of motion in people who have arthritis. Start by holding your hand and fingers straight and close together. Bend the end and middle joints of your fingers. Keep your knuckles straight. Moving slowly and smoothly, return your hand to the starting position. If you can, perform multiple repetitions of this exercise on each hand.



- Topography of the osteoarthritic thumb carpometacarpal joint and its variations with regard to gender, age, site, and osteoarthritic stage. Xu L, Strauch RJ, Ateshian GA, Pawluk RJ, Mow VC, Rosenwasser MP. J Hand Surg Am. 1998 May; 23(3):454-64. https://www.ncbi.nlm.nih.gov/pubmed/9620186/[↩]
- Melone C P, Beavers B, Isani A. The basal joint pain syndrome. Clin Orthop Relat Res 198722058–67. https://www.ncbi.nlm.nih.gov/pubmed/3595011[↩][↩]
- Florack T M, Miller R J, Pelligrini V D. et al The prevalence of carpal tunnel syndrome in patients with basal joint arthritis of the thumb. J Hand Surg [Am] 199217624–630. https://www.ncbi.nlm.nih.gov/pubmed/1629540[↩]
- Pellegrini V D., Jr Osteoarthritis of the trapeziometacarpal joint: the pathophysiology of articular cartilage degeneration. I. Anatomy and pathology of the aging joint. J Hand Surg 199116967–974. https://www.ncbi.nlm.nih.gov/pubmed/1748767[↩]
- Pellegrini V D., Jr The basal articulations of the thumb: pain, instability, and osteoarthritis. In: Peimer CA, ed. Surgery of the hand and upper extremity. New York: McGraw‐Hill, 19961019–1039.[↩]
- Kirk J A, Ansell B M, Bywaters E G L. The hypermobility syndrome: musculoskeletal complaints associated with generalized joint hypermobility. Ann Rheum Dis 196726419–425. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1031347/pdf/annrheumd00226-0048.pdf[↩]
- Cannon R, Dowd G, William D. et al A long‐term study following Bennett’s fracture. J Hand Surg [Br] 198611426–431. https://www.ncbi.nlm.nih.gov/pubmed/3794490[↩]
- Papp S R, Athwal G S, Pichora D R. The rheumatoid wrist. J Am Acad Orthop Surg 20061465–77. https://www.ncbi.nlm.nih.gov/pubmed/16467182[↩]
- Eaton R G, Glickel S Z. Trapeziometacarpal osteoarthritis: staging as a rationale for treatment. Hand Clin 19873455–469. https://www.ncbi.nlm.nih.gov/pubmed/3693416[↩]
- Marmor L, Peter J. Osteoarthritis of the carpometacarpal joint of the thumb. Am J Surg 1969117632–636. https://www.ncbi.nlm.nih.gov/pubmed/5791031[↩]
- Burton R I. Basal joint implant arthroplasty in osteoarthritis. Indications, techniques, pitfalls, and problems. Hand Clin 19873473–487. https://www.ncbi.nlm.nih.gov/pubmed/3693417[↩]
- Glickel S Z. Clinical assessment of the thumb trapeziometacarpal joint. Hand Clin 200117185–195. https://www.ncbi.nlm.nih.gov/pubmed/11478041[↩][↩]
- Burton R I. Basal joint arthrosis of the thumb. Orthop Clin North Am 19734331–348. https://www.ncbi.nlm.nih.gov/pubmed/4707436[↩][↩]
- Pomerance J F. Painful basal joint arthritis of the thumb. Part II: treatment. Am J Orthop 199524466–472. https://www.ncbi.nlm.nih.gov/pubmed/7670869[↩]
- Swigart C R, Eaton R G, Glickel S Z. et al Splinting in the treatment of arthritis of the first carpometacarpal joint. J Hand Surg 19992486–91. https://www.ncbi.nlm.nih.gov/pubmed/10048521[↩][↩]
- Splinting in the treatment of arthritis of the first carpometacarpal joint. Swigart CR, Eaton RG, Glickel SZ, Johnson C. J Hand Surg Am. 1999 Jan; 24(1):86-91. https://www.ncbi.nlm.nih.gov/pubmed/10048521/[↩]
- Reduction in the need for operation after conservative treatment of osteoarthritis of the first carpometacarpal joint: a seven year prospective study. Berggren M, Joost-Davidsson A, Lindstrand J, Nylander G, Povlsen B. Scand J Plast Reconstr Surg Hand Surg. 2001 Dec; 35(4):415-7. https://www.ncbi.nlm.nih.gov/pubmed/11878178[↩]
- Pellegrini V D., Jr Osteoarthritis at the base of the thumb. Orthop Clin North Am 19922383–102. https://www.ncbi.nlm.nih.gov/pubmed/1729673[↩]





{kind=link}