Contents
What is trichiasis
Trichiasis is an acquired misdirection of the eyelashes in which normal eyelashes grow in a posterior direction toward the corneal surface. In trichiasis, the lash follicle is normal, but the direction of eyelash growth is abnormal 1. In the presence of inflammation, there may be a misdirection of the eyelash hair follicle with the eyelash growing inwards towards the cornea, but the cause is not entropion. Some authors have divided trichiasis into primary where the eyelash is misdirected by abnormal direction of the shaft of the hair and secondary trichiasis where there is a misdirection of the hair follicle. Some eye experts have found this division less useful in clinical practice. Others have classified trichiasis as minor (less than five cilia) and major (more than five cilia). Mostly, trichiasis affects the lower eyelid.
Trichiasis can present similar to entropion (a condition in which the eyelid is turned inward), but management is different, as the problem is the direction of eyelash growth and not a margin malposition 2.
Trichiasis develops most commonly some time after chronic blepharitis (inflammation of the edges of the eyelids) or injury or damage to the eyelid or conjunctiva. Some people are born with an extra eyelid skinfold (epiblepharon) that causes the eyelashes to grow straight up into the eye or with an extra row of eyelashes (distichiasis).
Trichiasis can be asymptomatic or cause pain, foreign body sensation, red eye, tearing, and corneal scratches leading to infection and scarring.
The method used for treating trichiasis is usually dictated by the pattern (segmental or diffuse) of the misdirected lashes and the quality of the posterior lamella of the involved eyelid. Inturned lashes not associated with involutional entropion are usually seen in cases of posterior lamellar scarring (marginal cicatricial entropion). If the eyelid margin is misdirected, treatment should be directed at correcting the entropion.
In people with trichiasis, an eye doctor can remove the eyelashes with forceps. If eyelashes grow back, other methods can be used to remove them, such as electrolysis (use of heat and electrical current to destroy the hair follicle) or cryosurgery (use of extreme cold to destroy the hair follicle).
There is no fool proof way to remove trichiatic lashes (misdirected eyelashes that grow inwards and rub against the eye). The choices are recurrent epilation (plucking eyelashes), cryo (freezing) therapy, laser therapy (for dark lashes only) or a split thickness lid surgery where the lashes are removed follicle by follicle. None of these procedures are fool proof. With time and perseverance, however, the trichiatic condition can be improved.
Figure 1. Normal versus trichiasis
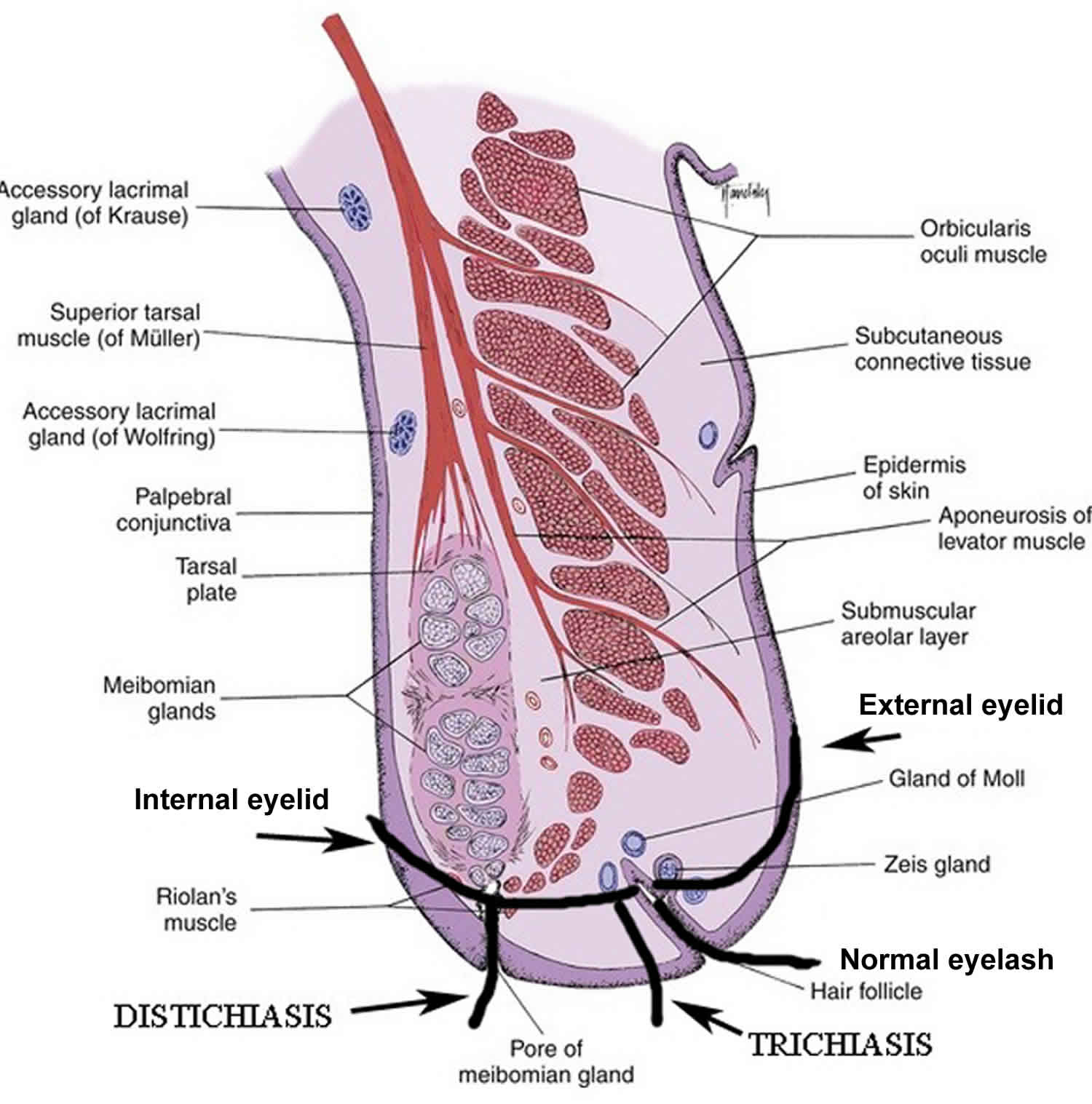 Figure 2. Trichiasis
Figure 2. Trichiasis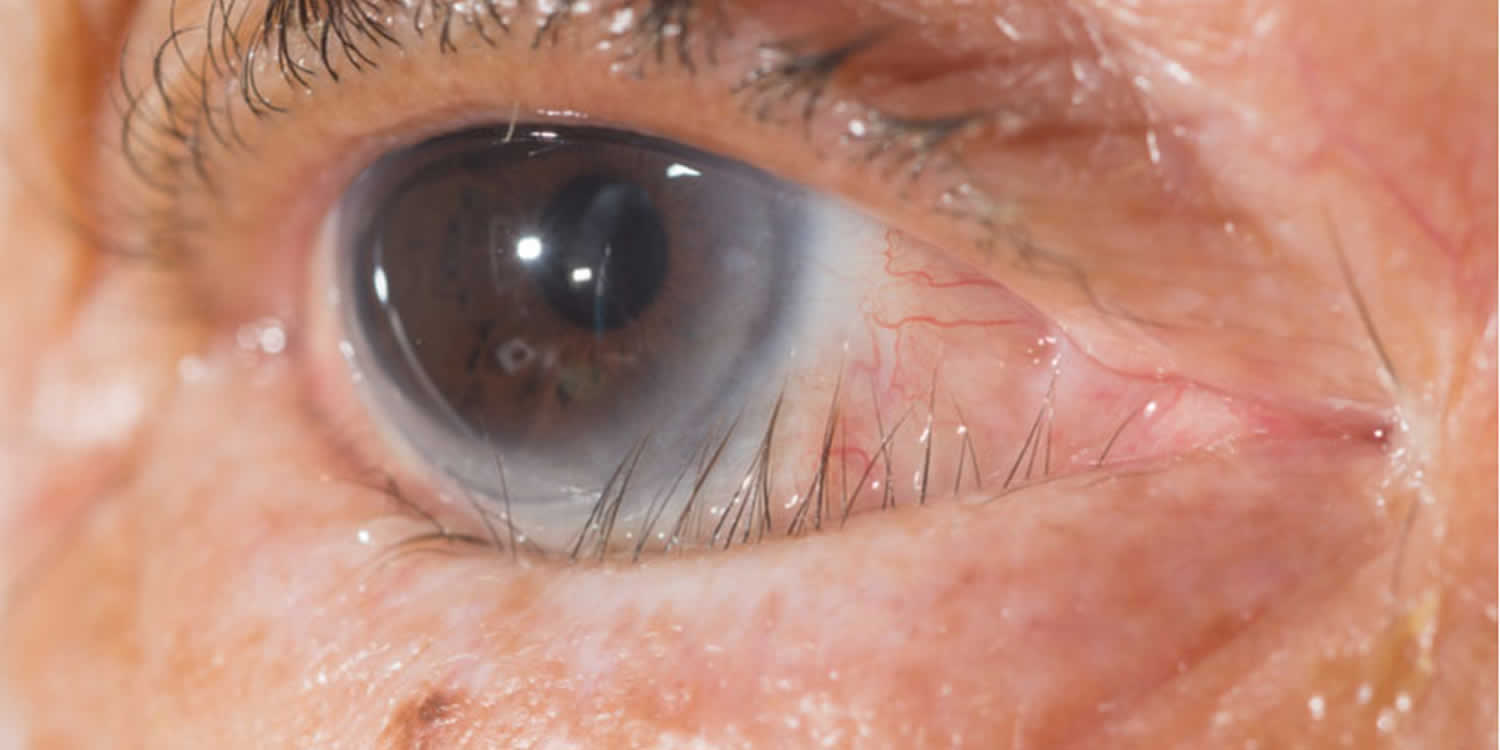
Trichiasis causes
Trichiasis causes:
- Chronic blepharitis
- Vernal keratoconjunctivitis
- Chemical burns
- Thermal injury
- Eczema
- Herpes zoster
- Atopic diseases
- Ocular cicatricial pemphigoid disease
- Cicatrizing conjunctival disease
- Eyelid trauma
- Eyelid surgery
- Meibomitis
- Stevens-Johnson syndrome
- Leprosy
- Eyelid tumors
- Trachoma
- Chalazia: Sometimes one will see trichiasis at a site of a prior chalazion which may or may not have been surgically drained: the collapsed meibomian gland can cause a local change in the architecture with lashes turning in.
Mostly, trichiasis affects the lower eyelid, except in chemical burns (where both lids are affected) or trachoma, where the upper eyelid is more severely affected. Chlamydia trachomatis causes trachoma: the disease is endemic in sub-Saharan Africa. In trachoma, inflammation of the eyelid margin and conjunctiva will cause a combination of trichiasis as well as cicatricial entropion. Corneal scarring and eventual corneal opacification can occur 3.
Trichiasis symptoms
In people with trichiasis, the eye becomes red and irritated, feels as though something is in it (foreign body sensation), and develops tearing and sensitivity and sometimes pain when exposed to light. If the condition persists, scarring of the cornea can occur.
Trichiasis diagnosis
A doctor bases the diagnosis of trichiasis on the symptoms and examination findings. Examination under the biomicroscope should assess the lid margin, the posterior lamella, and fornices (looking for symblepharon or scarring). An examination will reveal lashes pointing backward rubbing against the conjunctiva or the cornea. The lashes may be in their normal position may be growing from behind the normal eyelashes. Scarring of the eyelid margin secondary to inflammation should be looked for. Trichiasis is differentiated from involutional entropion, where the eyelid margin turns in and causes normal lashes to rub against the cornea. This is often termed secondary trichiasis or pseudo-trichiasis.
Trichiasis treatment
Artificial tear ointment will protect the surface of your eye. If there is a scratch on the eye, antibiotic drops may be necessary. The misdirected lashes can be pulled, but they typically grow back short and stiff in 6-8 weeks and can be more irritating. If there are signs of infection, scarring or vision loss, the lash follicles can be destroyed in the operating room. If the cause is epiblepharon, surgery can be done to remove the excess skin and rotate the eyelid.
Short-term relief may be obtained by epilating the eyelashes or inserting a bandage contact lens. Surgical treatment should only be undertaken after active inflammation is brought under control 1. Permanent destruction of the roots of the offending eyelashes is achieved using numerous techniques, including argon laser, electrolysis, radiofrequency epilation, trephination, eyelash bulb extirpation, resection of the lash follicle, cryotherapy, and surgical repositioning. Some eye doctors use the radiofrequency needle to the depth of the root of the lashes (2.4 mm deep in the upper lid and 1.4 mm in the lower lid) to kill the offending lash roots. Monopolar electrocautery is used less often now as it causes more collateral thermal injury to the eyelid margin.
- Patel BC, Joos ZP. Diseases of the Eyelashes. [Updated 2019 Apr 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537100[↩][↩]
- Cahill KV, Foster JA. 2012. Trichiasis. In: Black EH, Nesi FA, Calvano CJ, Gladstone GJ, Levine MR editors. Smith and Nesi’s Ophthalmic Plastic and Reconstructive Surgery. 3rd ed. New York (NY): Springer. p.317-321.[↩]
- Burton M, Habtamu E, Ho D, Gower EW. Interventions for trachoma trichiasis. Cochrane Database Syst Rev. 2015 Nov 13;(11):CD004008[↩]





{kind=link}