
Contents
What is trichinosis
Trichinosis also called Trichinellosis, is a disease that people can get by eating raw or undercooked meat from animals infected with the microscopic roundworms parasite (nematodes) Trichinella. Infection occurs commonly in certain wild carnivorous (meat-eating) animals such as bear or cougar, or omnivorous (meat and plant-eating) animals such as domestic pigs or wild boar.
When a human or animal eats meat that contains infective Trichinella cysts, the acid in the stomach dissolves the hard covering of the cyst and releases the worms. The worms pass into the small intestine and in 1-2 days, become mature. After mating, adult females lay eggs. Eggs develop into immature worms, travel through the arteries and are transported to muscles. Within the muscles, the worms curl into a ball and encyst (become enclosed in a capsule). The life cycle repeats when meat containing these encysted worms is consumed by another human or animal.
The incubation period ranges from 1-2 days (enteral phase) to 2 to 8 weeks (parenteral phase) or more, depending on the infectious dose and possibly the species of parasite. The parasite larvae are released from meat during digestion and then penetrate the intestinal mucosa where they mature into adult worms. The adult worms mate and new larvae are produced which then migrate via the bloodstream to skeletal muscle throughout the body. The host immune response leads to expulsion of the adult worms after several weeks; the larvae, once in the striated muscle cells, can persist for months or years, although clinical signs and symptoms typically wane after several months.
If you eat raw or undercooked meats, particularly bear, pork, wild feline (such as a cougar), fox, dog, wolf, horse, seal, or walrus, you are at risk for trichinosis.
See your healthcare provider who can order tests and treat symptoms of trichinosis infection. If you have eaten raw or undercooked meat, you should tell your health care provider.
How common is trichinosis?
Trichinosis (trichinellosis) infection used to be more common and was usually caused by ingestion of undercooked pork. However, trichinosis infection is now relatively rare. During 2008–2012, 15 cases were reported per year on average 1. The number of cases decreased beginning in the mid-20th century because of legislation prohibiting the feeding of raw-meat garbage to hogs, commercial and home freezing of pork and the public awareness of the danger of eating raw or undercooked pork products. Cases are less commonly associated with pork products and more often associated with eating raw or undercooked wild game meats.
Worldwide, an estimated 10,000 cases of trichinosis occur every year. Several different species of Trichinella can cause human disease; the most common species is Trichinella spiralis, which has a global distribution and is the species most commonly found in pigs. Other Trichinella species are less commonly reported as the cause of human disease and may be found in different parts of the world, usually infecting wild animals.
What are the symptoms of trichinosis?
The signs, symptoms, severity and duration of trichinosis (trichinellosis) vary. Nausea, diarrhea, vomiting, fatigue, fever, and abdominal discomfort are often the first symptoms of trichinosis. Headaches, fevers, chills, cough, swelling of the face and eyes, aching joints and muscle pains, itchy skin, diarrhea, or constipation may follow the first symptoms. If the infection is heavy, patients may experience difficulty coordinating movements, and have heart and breathing problems. In severe cases, death can occur.
For mild to moderate infections, most symptoms subside within a few months. Fatigue, weakness, muscle pain, and diarrhea may last for months.
How soon after infection will symptoms appear?
Abdominal symptoms can occur 1-2 days after infection. Further symptoms usually start 2-8 weeks after eating contaminated meat. Symptoms may range from very mild to severe and relate to the number of infectious worms consumed in meat. Often, mild cases of trichinosis are never specifically diagnosed and are assumed to be the flu or other common illnesses.
The earlier signs of trichinosis – diarrhea, fever, myalgia and edema, especially of the face – correspond to the new larvae migration through the body and can persist days to weeks. In addition to physical damage to affected tissues, larval penetration and tissue migration causes an immune-mediated inflammatory reaction and stimulates the development of eosinophilia. More severe manifestations include myocarditis, encephalitis, and thromboembolic disease.
Can I spread trichinellosis to others?
No. Infection can only occur by eating raw or undercooked meat containing Trichinella worms.
Trichinosis lifecycle
Trichinosis (trichinellosis) is caused by nematodes (roundworms) of the genus Trichinella. In addition to the classical agent Trichinella spiralis (found worldwide in many carnivorous and omnivorous animals), several other species of Trichinella are now recognized, including Trichinella pseudospiralis (mammals and birds worldwide), Trichinella nativa (Arctic bears), Trichinella nelsoni (African predators and scavengers), and Trichinella britovi (carnivores of Europe and western Asia).
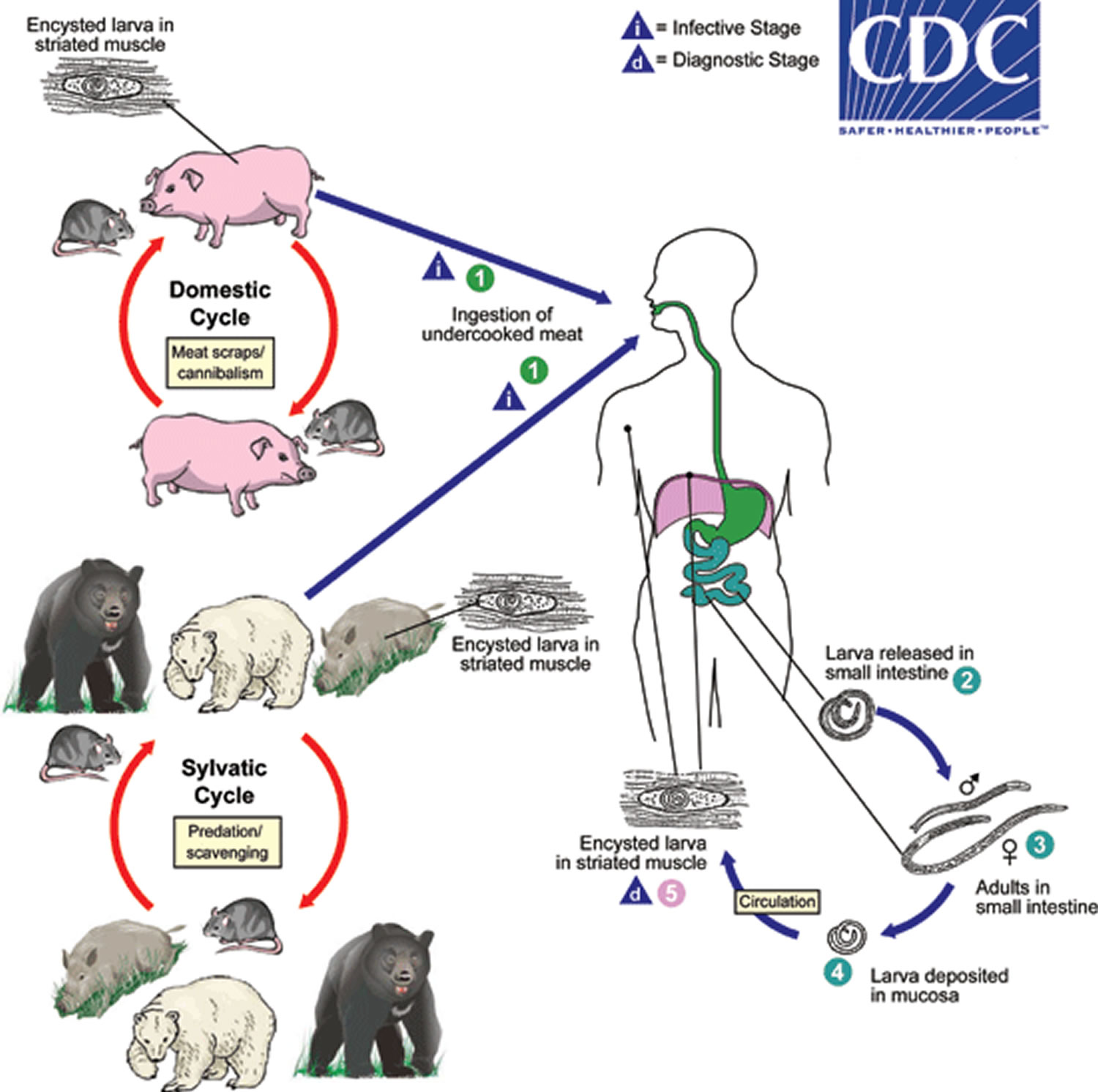
Trichinosis is acquired by ingesting meat containing cysts (encysted larvae) (1) of Trichinella. After exposure to gastric acid and pepsin, the larvae are released (2) from the cysts and invade the small bowel mucosa where they develop into adult worms (3) (female 2.2 mm in length, males 1.2 mm; life span in the small bowel: 4 weeks). After 1 week, the females release larvae (4) that migrate to the striated muscles where they encyst (5). Trichinella pseudospiralis, however, does not encyst. Encystment is completed in 4 to 5 weeks and the encysted larvae may remain viable for several years. Ingestion of the encysted larvae perpetuates the cycle. Rats and rodents are primarily responsible for maintaining the endemicity of this infection. Carnivorous/omnivorous animals, such as pigs or bears, feed on infected rodents or meat from other animals. Different animal hosts are implicated in the life cycle of the different species of Trichinella. Humans are accidentally infected when eating improperly processed meat of these carnivorous animals (or eating food contaminated with such meat).
Figure 1. Trichinosis lifecycle
Trichinosis complications
Except in severe cases, complications related to trichinosis are rare. In cases of heavy infestation, larvae can migrate to vital organs, causing potentially dangerous, even fatal, complications, including:
- Myocarditis — an inflammation of the myocardium, the thick muscular layer of your heart wall
- Encephalitis — an inflammation of your brain
- Meningitis — an inflammation of the membranes (meninges) and cerebrospinal fluid surrounding your brain and spinal cord
- Pneumonia — an inflammation of your lungs
Trichinosis causes
People get trichinosis when they eat undercooked meat — such as pork, bear, walrus or horse — that is infected with the immature form (larvae) of the trichinella roundworm. In nature, animals are infected when they feed on other infected animals. Pigs and horses can become infected with trichinosis when they feed on garbage containing infected meat scraps. Cattle don’t eat meat, but some cases have been linked to eating beef that was mixed with infected pork or ground in a grinder previously used for contaminated pork.
Due to increased regulation of pork feed and products in the United States, pigs have become a less common source of infection. Wild animals, including bear, continue to be sources of infection.
Risk factors for trichinosis
Risk factors for trichinosis include:
- Improper food preparation. Trichinosis infects humans when they eat undercooked infected meat, such as pork, bear or walrus, or other meat contaminated by grinders or other equipment.
- Rural areas. Trichinosis is more common in rural areas. In the United States, higher rates of infection are found in hog-raising regions.
- Consumption of wild or noncommercial meats. Public health measures have greatly decreased the incidence of trichinosis in commercial meats, but noncommercial, farm-raised animals have higher rates of infection — particularly those with access to wild-animal carcasses. Wild animals, such as bears and walruses, are still a common source of infection.
Trichinosis prevention
To help prevent Trichinella infection in animal populations, do not allow pigs or wild animals to eat uncooked meat, scraps, or carcasses of any animals, including rats, which may be infected with Trichinella.
People acquire trichinosis by consuming raw or undercooked meat infected with the Trichinella parasite, particularly wild game meat or pork. Even tasting very small amounts of undercooked meat during preparation or cooking puts you at risk for infection. Outbreaks occur in settings where multiple people consume the same Trichinella-infected meat.
The best way to prevent trichinosis (trichinellosis) is to cook meat to safe temperatures. A food thermometer should be used to measure the internal temperature of cooked meat. Do not sample meat until it is cooked. USDA recommends the following for meat preparation.
For Whole Cuts of Meat (excluding poultry and wild game)
- Cook to at least 145° F (63° C) as measured with a food thermometer placed in the thickest part of the meat, then allow the meat to rest* for three minutes before carving or consuming.
For Ground Meat (excluding poultry and wild game)
- Cook to at least 160° F (71° C); ground meats do not require a rest* time.
For Wild Game (whole cuts and ground)
- Cook to at least 160° F (71° C).
For All Poultry (whole cuts and ground)
- Cook to at least 165° F (74° C), and for whole poultry allow the meat to rest* for three minutes before carving or consuming.
*According to USDA, “A ‘rest time’ is the amount of time the product remains at the final temperature, after it has been removed from a grill, oven, or other heat source. During the three minutes after meat is removed from the heat source, its temperature remains constant or continues to rise, which destroys pathogens.”
- Avoid undercooked meat. Be sure whole cuts of meat other than poultry and wild game are cooked to an internal temperature of 145 F (63 C) throughout, and don’t cut or eat the meat for at least three minutes after you’ve removed it from the heat. Cook ground pork and beef to at least 160 F (71 C). They can be eaten immediately after cooking. Using a meat thermometer is the best way to ensure the meat is thoroughly cooked.
- Avoid undercooked wild game. For both whole cuts and ground varieties, cook to an internal temperature of at least 160 F (71 C).
- Avoid undercooked poultry. For whole cuts and ground varieties, cook to a temperature of at least 165 F (74 C). For whole cuts, let the poultry sit for three minutes before cutting or eating.
- Curing (salting), drying, smoking, or microwaving meat alone does NOT consistently kill infective worms; homemade jerky and sausage were the cause of many cases of trichinosis reported to the Centers for Disease Control and Prevention in recent years.
- Know that other processing methods don’t kill parasites. Other methods of meat processing or preserving, such as smoking and pickling, don’t kill trichinella parasites in infected meat.
- Freeze pork less than 6 inches thick for 20 days at 5°F (-15°C) to kill any worms.
- Freezing wild game meats, unlike freezing pork products, may NOT effectively kill all worms because some worm species that infect wild game animals are freeze-resistant.
- Clean meat grinders thoroughly after each use.
- Have wild-animal meat frozen or irradiated. Irradiation will kill parasites in wild-animal meat, and deep-freezing for three weeks kills trichinella in some meats. However, trichinella in bear meat does not die by freezing, even over a long period. Neither irradiation nor freezing is necessary if you ensure that the meat is thoroughly cooked.
Trichinosis signs and symptoms
Symptoms may range from very mild to severe and relate to the number of infectious worms consumed in the meat. Many mild cases of trichinosis are never specifically diagnosed because they are assumed to be the flu or other common illnesses. Furthermore, many people with Trichinella infection do not experience any symptoms at all. The severity of symptoms usually depends on the number of larvae consumed in the infected meat.
Possibly no signs or symptoms
Mild cases of trichinosis — those with only a small number of parasites in your body — may cause no recognizable signs or symptoms. Symptoms can develop with moderate or heavy infestation, sometimes progressing as the parasite travels through your body.
The severity of disease is related to the infectious dose and host characteristics, such as age of the patient or immunological priming as a result of previous Trichinella infection. Some reports have linked severity of trichinosis to the infecting species of Trichinella, suggesting that certain species are more likely to cause severe disease than others. However, the pathogenicity of various species is difficult to define clinically without quantifying infectious dose.
If the infection is heavy, persons may have trouble coordinating movements, and have heart and breathing problems. Although rare, death can occur in severe cases. For mild to moderate infections, most symptoms go away within a few months.
The first symptoms of trichinosis are gastrointestinal, usually occurring 1-2 days after a person consumes raw or undercooked meat from a Trichinella-infected animal. You swallow trichinella larvae encased in a cyst. Your digestive juices dissolve the cyst, releasing the parasite into your body. The larvae then penetrate the wall of the small intestine, where they mature into adult worms and mate.
At this stage, you may experience:
- Nausea
- Diarrhea
- Vomiting
- Abdominal pain
The classic trichinosis symptoms often occur within 2 weeks after eating contaminated meat, and can last up to 8 weeks. About a week after infection, the adult female worms produce larvae that go through the intestinal wall, enter your bloodstream, and eventually burrow into muscle or other tissue.
This tissue invasion can cause:
- Muscle pain and tenderness
- Fever
- Swelling of the face, particularly the eyelids
- Pink eye (conjunctivitis)
- Sensitivity to light
- Weakness or fatigue
- Headache
- Chills
- Itchy skin or rash
- Cough
- Diarrhea
- Constipation
Trichinosis diagnosis
Trichinella larvae bury themselves inside muscle tissue rather than remain in the intestine as in other roundworm infections, so stool sample tests don’t often show evidence of the parasite. The initial diagnosis relies on the classic signs and symptoms — swelling around the eyes, muscle inflammation and fever.
A diagnosis of trichinosis is made in patients whose signs and symptoms are compatible with trichinosis, have a positive laboratory test for Trichinella, and who can recall eating raw or undercooked pork or wild game meat.
Laboratory diagnosis of Trichinella infection is most often made by a Trichinella antibody test. In some cases a muscle biopsy may be performed.
To confirm the diagnosis, your doctor might use these tests:
- Blood tests. Your doctor may take a blood sample and test it for signs suggesting trichinosis — an increase in the number of a certain type of white blood cell (eosinophils) or the formation of antibodies against the parasite after several weeks.
- Muscle biopsy. While the blood test typically is enough to establish a diagnosis, your doctor might also recommend a muscle biopsy. A small piece of muscle is removed and examined under a microscope to look for trichinella larvae.
For outbreak-associated infections, the diagnosis can be made in asymptomatic persons on the basis of positive results on laboratory testing and history of consumption of an implicated meat. Diagnosis can be challenging, particularly in non-outbreak settings. In the early stages of disease, signs and symptoms are non-specific (see Disease) and mimic those of many other illnesses. For example, the diarrhea that can occur in the first weeks of Trichinella infection is also a common symptom of other foodborne diseases such as salmonellosis, and the fever and myalgia in the acute phase of Trichinella infection are also suggestive of influenza virus infection.
Trichinella infections are most often diagnosed in the laboratory based on detection of antibodies to excretory/secretory Trichinella antigen in enzyme immunoassays (EIA) format. This antigen preparation will react with antibodies from other Trichinella species but may also cross react with non-specific antibodies. IgG antibodies can be detected approximately 12 to 60 days post-infection. Antibody development depends on the amount of infective Trichinella larvae that are consumed. Levels peak in the second or third month post-infection and then decline, but may be detectable for 10 years or more following infection. At least two serum specimens should be drawn and tested weeks apart to demonstrate seroconversion in patients with suspected trichinellosis whose initial results were negative or weakly positive. Immunologic tests for Trichinella infection have the potential for cross-reactivity with sera from patients with other conditions, especially other parasitic infections. One commercial enzyme immunoassays (EIA) kit for trichinosis antibody detection is available in the United States.
Antibody levels are often not detectable until 3 to 5 weeks post-infection, well after the onset of acute-stage illness. Antibody development is also affected by the infecting dose of larvae: the higher the infecting dose, the faster the patient’s antibody response will develop. Multiple serum specimens should be drawn several weeks apart to demonstrate seroconversion in patients whose initial specimen was negative. IgG, IgM, and IgE antibodies are detectable in many patients; however, tests based on IgG antibodies are most sensitive. Antibody levels peak in the second or third month post-infection and then decline slowly for several years. In our experience at CDC, EIAs with ES antigens detect antibodies earlier than bentonite flocculation in 25% of serum specimens from patients with acute infection, but EIAs also remain positive for longer periods after infection than the bentonite flocculation, and are reactive in a larger proportion of persons with no clinical evidence of trichinellosis.
Muscle biopsies are infrequently performed, but they allow for the molecular identification of the Trichinella species or genotype, which is not possible with antibody testing. Usually, 0.2 to 0.5 grams of human or animal skeletal muscle tissue is collected and examined for Trichinella larvae via artificial digestion or histological analysis.
Trichinosis treatment
Several safe and effective prescription drugs are available to treat trichinosis. Treatment should begin as soon as possible and the decision to treat is based upon symptoms, exposure to raw or undercooked meat, and laboratory test results.
Prompt treatment with antiparasitic drugs can help prevent the progression of trichinosis by killing the adult worms and so preventing further release of larvae. Once the larvae have become established in skeletal muscle cells, usually by 3 to 4 weeks post infection, treatment may not completely eliminate the infection and associated symptoms. Treatment with either mebendazole or albendazole is recommended. If treatment is not initiated within the first several days of infection, more prolonged or repeated courses of treatment may be necessary. Both drugs are considered relatively safe but have been associated with side effects including bone marrow suppression. Patients on longer courses of therapy should be monitored by serial complete blood counts to detect any adverse effects promptly and discontinue treatment. Albendazole and mebendazole are not approved for use in pregnant women or children under the age of 2 years. In addition to antiparasitic medication, treatment with steroids is sometimes required in more severe cases to control inflammation during larval migration. Some cases of trichinosis cause allergic reactions when the parasite enters muscle tissue or when dead or dying larvae release chemicals in your muscle tissue.
Pain relievers. After muscle invasion, pain relievers may be given for muscle aches. Eventually, the larvae cysts in your muscles tend to calcify, resulting in destruction of the larvae and the end of muscle aches and fatigue.
| Drug | Adult and pediatric dose |
|---|---|
| Albendazole | 400 mg twice a day by mouth for 8 to 14 days |
| Mebendazole | 200 to 400 mg three times a day by mouth for 3 days, then 400 to 500 mg three times a day by mouth for 10 days |
Oral albendazole is available for human use in the United States.
Mebendazole is available in the United States only through compounding pharmacies.
Albendazole
Treatment in Pregnancy
Albendazole is pregnancy category C. Data on the use of albendazole in pregnant women are limited, though the available evidence suggests no difference in congenital abnormalities in the children of women who were accidentally treated with albendazole during mass prevention campaigns compared with those who were not. In mass prevention campaigns for which the World Health Organization (WHO) has determined that the benefit of treatment outweighs the risk, WHO allows use of albendazole in the 2nd and 3rd trimesters of pregnancy. However, the risk of treatment in pregnant women who are known to have an infection needs to be balanced with the risk of disease progression in the absence of treatment.
Pregnancy Category C: Either studies in animals have revealed adverse effects on the fetus (teratogenic or embryocidal, or other) and there are no controlled studies in women or studies in women and animals are not available. Drugs should be given only if the potential benefit justifies the potential risk to the fetus.
Treatment During Lactation
It is not known whether albendazole is excreted in human milk. Albendazole should be used with caution in breastfeeding women.
Treatment in Pediatric Patients
The safety of albendazole in children less than 6 years old is not certain. Studies of the use of albendazole in children as young as one year old suggest that its use is safe. According to WHO guidelines for mass prevention campaigns, albendazole can be used in children as young as 1 year old. Many children less than 6 years old have been treated in these campaigns with albendazole, albeit at a reduced dose.
Mebendazole
Treatment in Pregnancy
Mebendazole is in pregnancy category C. Data on the use of mebendazole in pregnant women are limited. The available evidence suggests no difference in congenital anomalies in the children of women who were treated with mebendazole during mass treatment programs compared with those who were not. In mass treatment programs for which the World Health Organization (WHO) has determined that the benefit of treatment outweighs the risk, WHO allows use of mebendazole in the 2nd and 3rd trimesters of pregnancy. The risk of treatment in pregnant women who are known to have an infection needs to be balanced with the risk of disease progression in the absence of treatment.
Pregnancy Category C: Either studies in animals have revealed adverse effects on the fetus (teratogenic or embryocidal, or other) and there are no controlled studies in women or studies in women and animals are not available. Drugs should be given only if the potential benefit justifies the potential risk to the fetus.
Treatment During Lactation
It is not known whether mebendazole is excreted in breast milk. The WHO classifies mebendazole as compatible with breastfeeding and allows the use of mebendazole in lactating women.
Treatment in Pediatric Patients
The safety of mebendazole in children has not been established. There is limited data in children age 2 years and younger. Mebendazole is listed as an intestinal antihelminthic medicine on the WHO Model List of Essential Medicines for Children, intended for the use of children up to 12 years of age.
- Trichinellosis FAQs. https://www.cdc.gov/parasites/trichinellosis/gen_info/faqs.html[↩]





{kind=link}