
Contents
What is TSH
TSH is short for thyroid-stimulating hormone also called thyrotropin, is produced by the anterior pituitary gland, a tiny organ located below your brain and behind the sinus cavities. TSH interacts with specific cell receptors on the thyroid cell surface and gives rise to 2 main actions. First, TSH stimulates cell reproduction and hypertrophy. Second, TSH stimulates the thyroid gland to synthesize and secrete the hormones thyroxine (T4) and triiodothyronine (T3) into the blood. These thyroid hormones help control the rate at which the body uses energy. TSH is synthesized and secreted by the anterior pituitary in response to a negative feedback mechanism involving concentrations of free triiodothyronine (T3) and free thyroxine (T4). Additionally, the hypothalamic tripeptide, thyrotropin-releasing hormone (TRH), directly stimulates TSH production.
Serum TSH concentrations exhibit a diurnal variation with the peak occurring during the night and the nadir occurring between 10 a.m. and 4 p.m. This biological variation does not influence the interpretation of the TSH test result since most clinical TSH measurements are performed on ambulatory patients between 8 a.m. and 6 p.m.
When hypothalamic-pituitary function is normal, a log/linear inverse relationship between serum TSH and free thyroxine exists.
TSH, along with its regulatory hormone thyrotropin releasing hormone (TRH), which comes from the hypothalamus, is part of the feedback system that the body uses to maintain stable amounts of thyroid hormones in your blood. When thyroid hormone concentrations decrease, the production of TSH by the anterior pituitary gland is increased. TSH in turn stimulates the production and release of thyroxine (T4) and triiodothyronine (T3) by the thyroid gland, a small butterfly-shaped gland that lies at the base of the throat flat against the windpipe. When all three organs are functioning normally, thyroid production turns on and off to maintain relatively stable levels of thyroid hormones in the blood.
If the thyroid releases inappropriately large amounts of thyroxine (T4) and triiodothyronine (T3), the affected person may experience symptoms associated with hyperthyroidism, such as rapid heart rate, weight loss, nervousness, hand tremors, irritated eyes, and difficulty sleeping. Graves disease is the most common cause of hyperthyroidism. It is a chronic autoimmune disorder in which the affected person’s immune system produces antibodies that act like TSH, leading to the production of excessive amounts of thyroid hormone. In response, the pituitary may produce less TSH, usually leading to a low level in the blood.
If there is decreased production of thyroid hormones by the thyroid (hypothyroidism), the person may experience symptoms such as weight gain, dry skin, constipation, cold intolerance, and fatigue. Hashimoto thyroiditis is the most common cause of hypothyroidism in the U.S. It is a chronic autoimmune condition in which the immune response causes inflammation and damage to the thyroid as well as the production of autoantibodies. With Hashimoto thyroiditis, the thyroid produces low levels of thyroid hormone. The anterior pituitary gland may produce more TSH, usually resulting in a high level in the blood.
However, the level of TSH does not always predict or reflect thyroid hormone levels. Some people produce an abnormal form of TSH that does not function properly. They often have hypothyroidism despite having normal or even mildly elevated TSH levels. In a variety of thyroid diseases, thyroid hormone levels may be high or low, regardless of the amount of TSH present in the blood.
Rarely, pituitary dysfunction may result in increased or decreased amounts of TSH. In addition to pituitary dysfunction, hyperthyroidism or hypothyroidism can occur if there is a problem with the hypothalamus due to insufficient or excessive thyrotropin releasing hormone (TRH).
Thyroid disease is much more common in women and most often occurs under the age of 40. It also tend to run in families. You may need a thyroxine test if a family member has ever had thyroid disease or if you have symptoms of having too much thyroid hormone in your blood, a condition called hyperthyroidism, or symptoms of having too little thyroid hormone, a condition called hypothyroidism.
Signs and symptoms of hypothyroidism may include:
- Weight gain
- Dry skin
- Constipation
- Cold intolerance
- Puffy skin
- Hair loss
- Fatigue
- Menstrual irregularity in women
- Enlarged thyroid gland (goiter)
Signs and symptoms of hyperthyroidism may include:
- Increased heart rate
- Anxiety
- Weight loss
- Difficulty sleeping
- Tremors in the hands
- Weakness
- Diarrhea
- Puffiness around the eyes, dryness, irritation, or bulging of the eyes
Figure 1. The pituitary gland location

Figure 2. The hypothalamus and pituitary gland (anterior and posterior) endocrine pathways and target organs
 Figure 3. Thyroid stimulating hormone (TSH)
Figure 3. Thyroid stimulating hormone (TSH)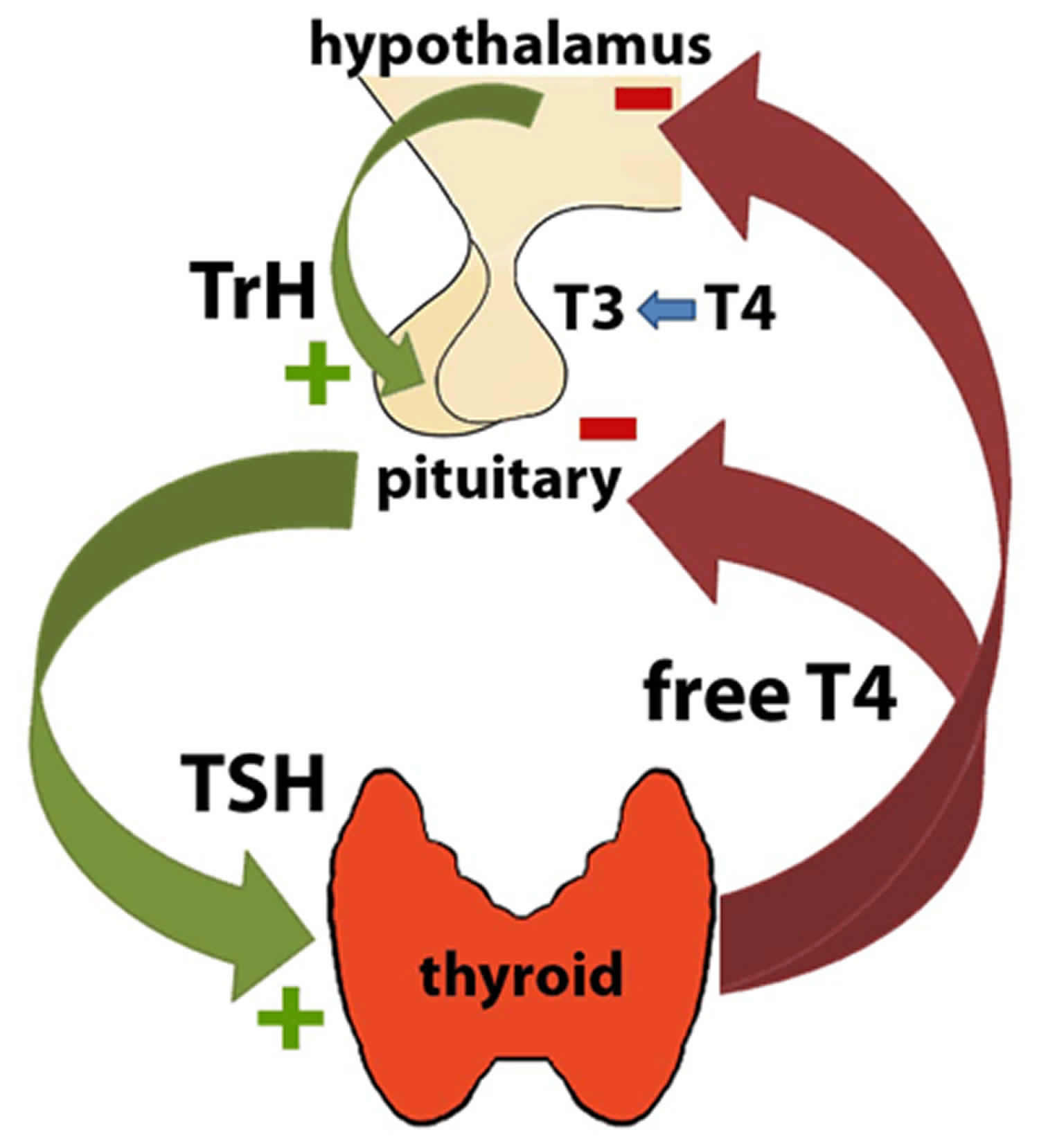
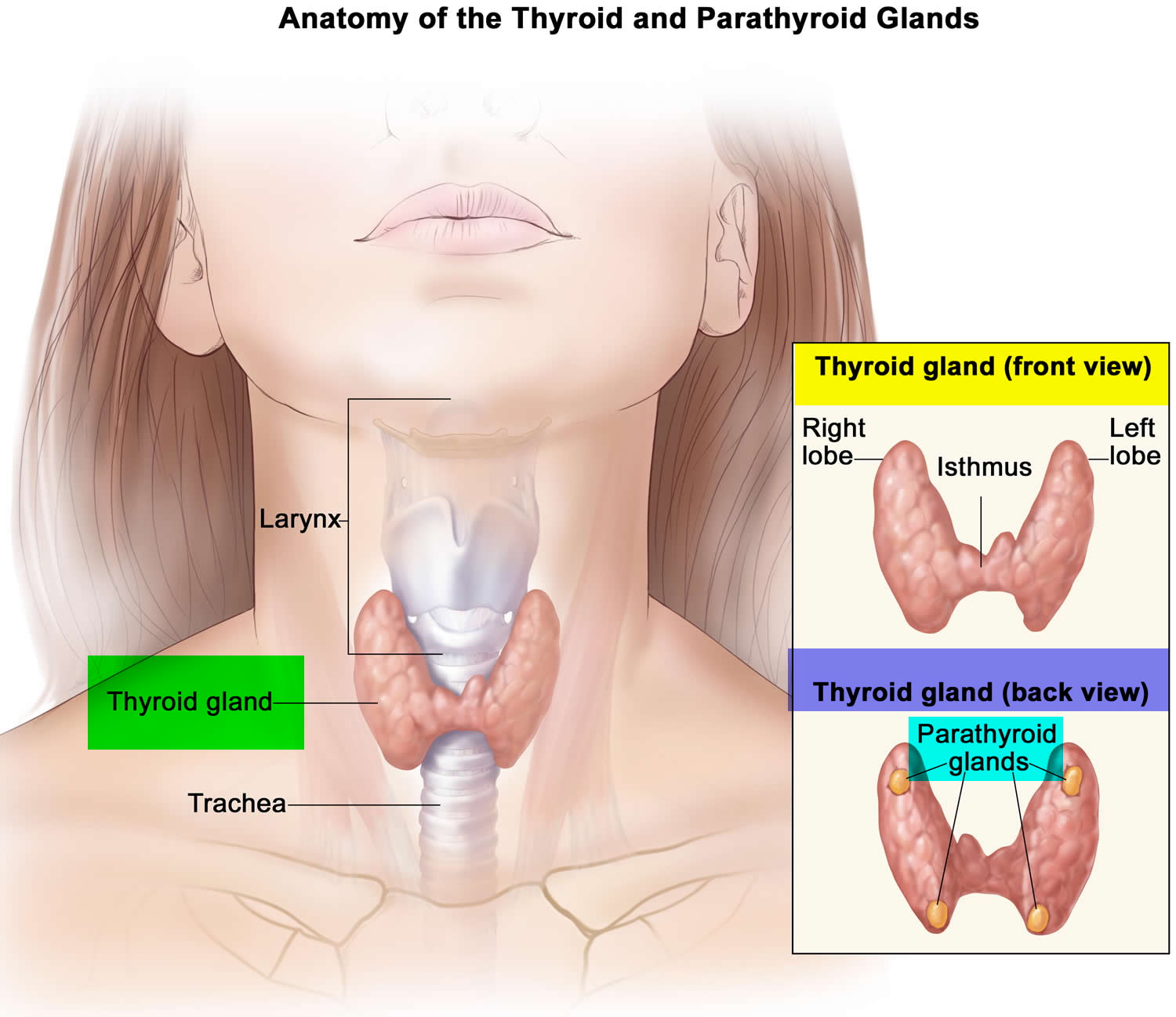
Figure 4. Thyroid gland location
What is TSH test?
The TSH (thyroid-stimulating hormone) blood test is often the test of choice for evaluating thyroid function and/or symptoms of a thyroid disorder, including hyperthyroidism or hypothyroidism.
TSH is produced by the anterior pituitary gland, a tiny organ located below the brain and behind the sinus cavities. It is part of the body’s feedback system to maintain stable amounts of the thyroid hormones thyroxine (T4) and triiodothyronine (T3) in the blood and to help control the rate at which the body uses energy.
A TSH test is frequently ordered along with or preceding a free T4 test. Other thyroid tests that may be ordered include a free T3 test and thyroid antibodies (if autoimmune-related thyroid disease is suspected). Sometimes TSH, free T4 and free T3 are ordered together as a thyroid panel.
TSH testing is used to:
- Diagnose a thyroid disorder in a person with symptoms
- Screen newborns for an underactive thyroid
- Monitor thyroid replacement therapy in people with hypothyroidism
- Monitor anti-thyroid treatment in people with hyperthyroidism
- Help diagnose and monitor infertility problems in women
- Help evaluate the function of the pituitary gland (occasionally)
- Screen adults for thyroid disorders, although expert opinions vary on who can benefit from screening and at what age to begin
TSH normal range
Normal TSH levels
- Age 0-5 days: 0.7-15.2 mIU/L
- Age 6 days-2 months: 0.7-11.0 mIU/L
- Age 3-11 months: 0.7-8.4 mIU/L
- Age 1-5 years: 0.7-6.0 mIU/L
- Age 6-10 years: 0.6-4.8 mIU/L
- Age 11-19 years: 0.5-4.3 mIU/L
- Age > or =20 years: 0.3-4.2 mIU/L
When is TSH test ordered?
A health practitioner may order a TSH test when someone has symptoms of hyperthyroidism or hypothyroidism and/or when a person has an enlarged thyroid gland (goiter).
Signs and symptoms of hyperthyroidism may include:
- Increased heart rate
- Anxiety
- Weight loss
- Difficulty sleeping
- Tremors in the hands
- Weakness
- Diarrhea (sometimes)
- Light sensitivity, visual disturbances
- The eyes may be affected: puffiness around the eyes, dryness, irritation, and, in some cases, bulging of the eyes.
Signs and symptoms of hypothyroidism may include:
- Weight gain
- Dry skin
- Constipation
- Cold intolerance
- Puffy skin
- Hair loss
- Fatigue
- Menstrual irregularity in women
- Enlarged thyroid gland (goiter)
TSH may be ordered at regular intervals when an individual is being treated for a known thyroid disorder. When a person’s dose of thyroid medication is adjusted, the American Thyroid Association recommends waiting 6-8 weeks before testing the level of TSH again.
TSH screening is routinely performed in the United States on newborns soon after birth as part of each state’s newborn screening program.
In 2004, the U.S. Preventive Services Task Force found insufficient evidence to recommend for or against routine screening for thyroid disease in asymptomatic adults. However, the American Thyroid Association and the American Association of Clinical Endocrinologists released clinical practice guidelines in 2012 that recommend that screening for hypothyroidism should be considered in people over the age of 60. Because the signs and symptoms of both hypothyroidism and hyperthyroidism are so similar to those seen in many common disorders, health practitioners often need to rule out thyroid disease even though the patient has another problem.
What does abnormal TSH test result mean?
Whether high or low, an abnormal TSH indicates an excess or deficiency in the amount of thyroid hormone available to the body, but it does not indicate the reason why. An abnormal TSH test result is usually followed by additional testing to investigate the cause of the increase or decrease.
- In primary hypothyroidism, thyroid-stimulating hormone (TSH) levels will be elevated.
- In primary hyperthyroidism, TSH levels will be low.
The ability to quantitate circulating levels of TSH is important in evaluating thyroid function. It is especially useful in the differential diagnosis of primary (thyroid) from secondary (pituitary) and tertiary (hypothalamus) hypothyroidism. In primary hypothyroidism, TSH levels are significantly elevated, while in secondary and tertiary hypothyroidism, TSH levels are low or normal.
Elevated or low TSH in the context of normal free thyroxine (free T4) is often referred to as subclinical hypo- or hyperthyroidism, respectively.
Thyrotropin-releasing hormone (TRH) stimulation differentiates all types of hypothyroidism by observing the change in patient TSH levels in response to TRH (thyrotropin-releasing hormone). Typically, the TSH response to TRH stimulation is exaggerated in cases of primary hypothyroidism, absent in secondary hypothyroidism, and delayed in tertiary hypothyroidism. Most individuals with primary hyperthyroidism have TSH suppression and do not respond to TRH stimulation with an increase in TSH over their basal value.
Sick, hospitalized patients may have falsely low or transiently elevated TSH.
The following table summarizes some examples of typical test results and their potential meaning.
| TSH | Free T4 | Free or total T3 | Interpretation |
|---|---|---|---|
| High | Normal | Normal | Mild (subclinical) hypothyroidism |
| High | Low | Low or normal | Hypothyroidism |
| Low | Normal | Normal | Mild (subclinical) hyperthyroidism |
| Low | High or normal | High or normal | Hyperthyroidism |
| Low | Low or normal | Low or normal | Nonthyroidal illness; pituitary (secondary) hypothyroidism |
| Normal | High | High | Thyroid hormone resistance syndrome (a mutation in the thyroid hormone receptor decreases thyroid hormone function) |
The above test results alone are not diagnostic but will prompt a health practitioner to perform additional testing to investigate the cause of the elevated or low TSH. As examples, the most common cause of hyperthyroidism is Graves disease and the most common cause of hypothyroidism is Hashimoto thyroiditis.
When used for monitoring treatment for thyroid or pituitary disorders, results of thyroid tests will inform the health practitioner whether treatment is effective and/or whether an adjustment to dose is necessary. For example, in people with hyperthyroidism, free T4, free T3, and TSH are regularly checked while they are on anti-thyroid drugs to assure that the drugs are working and to decrease doses if thyroid hormone levels get too low. In people with hypothyroidism, TSH and free T4 are regularly checked to assure that the right dose of thyroid hormone is being given to make TSH normal.
Thyroid Function Ordering Algorithm
In nonhospitalized patients without known or suspected pituitary disease.
- If in adult TSH <0.10 mIU/L (low TSH)
- Suspect: Hyperthyroidism
- Order Free T4 (Thyroxine):
- If Free T4 is normal
- Order Total T3 (Triiodothyronine). In hyperthyroidism, both T4 and T3 levels are usually elevated, but in a small subset of hyperthyroid patients only T3 is elevated (T3 toxicosis).
- If Free T4 is normal
- Order Free T4 (Thyroxine):
- Suspect: Hyperthyroidism
- If in adult TSH 0.10–0.29 mIU/L
- Suspect: Borderline low TSH
- Order Free T4 (Thyroxine)
- Suspect: Borderline low TSH
- If in adult TSH 0.30–4.2 mIU/L
- No further testing unless clinically indicated.
- If in adult TSH >4.2 mIU/L (high TSH)
- Suspect: Hypothyroidism
- Order Free T4 (Thyroxine) and Thyroperoxidase antibodies. In hypothyroidism T4 and T3 levels are decreased. To aid in the diagnosis of thyroid autoimmune disorders (e.g., Hashimoto thyroiditis, idiopathic myxedema, and Graves disease). The highest thyroperoxidase antibody levels are observed in patients suffering from Hashimoto thyroiditis. In this disease, the prevalence of thyroperoxidase antibodies is about 90% of cases, confirming the autoimmune origin of the disease. These autoantibodies also frequently occur (60%–80%) in the course of Graves disease. In patients with subclinical hypothyroidism, the presence of thyroperoxidase antibodies is associated with an increased risk of developing overt hypothyroidism. Many clinical endocrinologists use the thyroperoxidase antibody test as a diagnostic tool in deciding whether to treat a patient with subclinical hypothyroidism.
- Suspect: Hypothyroidism
High TSH levels
A elevated TSH may mean that:
- The person tested has an underactive thyroid gland that is not responding adequately to the stimulation of TSH due to some type of acute or chronic thyroid dysfunction
- A person with hypothyroidism or who has had their thyroid gland removed is receiving too little thyroid hormone replacement medication and the dose may need to be adjusted
- A person with hyperthyroidism is receiving too much anti-thyroid medication and the dose needs adjusting
- There is a problem with the pituitary gland, such as a tumor producing unregulated levels of TSH
Low TSH levels
A low TSH result may indicate:
- An overactive thyroid gland (hyperthyroidism)
- Excessive amounts of thyroid hormone medication in those who are being treated for an underactive (or removed) thyroid gland
- Insufficient anti-thyroid medication in a person being treated for hyperthyroidism; however, it may take a while for TSH production to resume after successful anti-thyroid treatment. This is why the American Thyroid Association recommends monitoring this treatment with tests for thyroid hormones (T4 and T3) as well as TSH levels.
- Damage to the pituitary gland that prevents it from producing adequate amounts of TSH
Is there anything else I should know?
It is important to note that TSH, free T4, and free T3 tests are a “snapshot” of what is occurring within a dynamic system. An individual person’s thyroid testing results may vary and may be affected by:
- Increases, decreases, and changes (inherited or acquired) in the proteins that bind T4 and T3
- Pregnancy
- Estrogen and other drugs
- Liver disease
- Systemic illness
- Resistance to thyroid hormones
Many medications — including aspirin and thyroid-hormone replacement therapy — may affect thyroid gland function test results and their use should be discussed with the health practitioner prior to testing.
Illnesses not directly related to the thyroid, “nonthyroidal illnesses,” can affect thyroid hormones levels. In particular, the level of T3 can be low in nonthyroidal illness. Typically, the thyroid hormone levels return to normal after a person recovers from the nonthyroidal illness. Historically, this condition was referred to as “euthyroid sick syndrome” but that term is controversial because there is some question as to whether those affected have a thyroid gland that is functioning normally (euthyroid).
When a health practitioner adjusts a person’s thyroid hormone replacement dosage, it is important to wait at least one to two months before checking the TSH again so that the new dose can have its full effect.
Extreme stress and acute illness may affect TSH test results. It is generally recommended that thyroid testing be avoided in hospitalized patients or deferred until after a person has recovered from an acute illness.
Results may be low during the first trimester of pregnancy.
Do healthcare practitioners test TSH during pregnancy?
Health practitioners do not generally test asymptomatic women, but those with symptoms and/or a known thyroid disorder may be tested at intervals to detect and evaluate hyperthyroidism or hypothyroidism both during pregnancy and after.
Thyroid changes can happen during pregnancy. These changes are usually not significant, but some women can develop thyroid disease during pregnancy. Hyperthyroidism happens in about one in every 500 pregnancies, while hypothyroidism happens in approximately one in every 250 pregnancies. Hyperthyroidism, and less often, hypothyroidism, may remain after pregnancy. If you develop a thyroid condition during pregnancy, your health care provider will monitor your condition after your baby is born. Also, if you have a history of thyroid disease, be sure to talk with your health care provider if you are pregnant or are thinking of becoming pregnant.
Are there things that I can do to raise or lower my TSH level?
In general, TSH does not respond to lifestyle changes. What is important is that the pituitary and thyroid glands are healthy and working together to produce appropriate amounts of thyroid hormone.
What is a 3rd generation TSH and an ultrasensitive TSH?
The original immunoassays for TSH were not sensitive enough to differentiate the very low levels seen in patients with hyperthyroidism from levels seen in normal euthyroid individuals. In the 1980s, more sensitive assays (“second generation”) were developed and these were able to identify patients with TSH levels that were suppressed due to the excess amounts of free T4 present in hyperthyroidism. In the 1990s, TSH assays were made even more sensitive and, although these were able to measure even lower levels, they were widely adopted because they performed much better than the second generation assays in the range that was important for differentiating normal from hyperthyroid. Almost all laboratories currently use so-called “third generation” or “ultrasensitive” TSH assays today.





{kind=link}