Contents
What is thyroxine
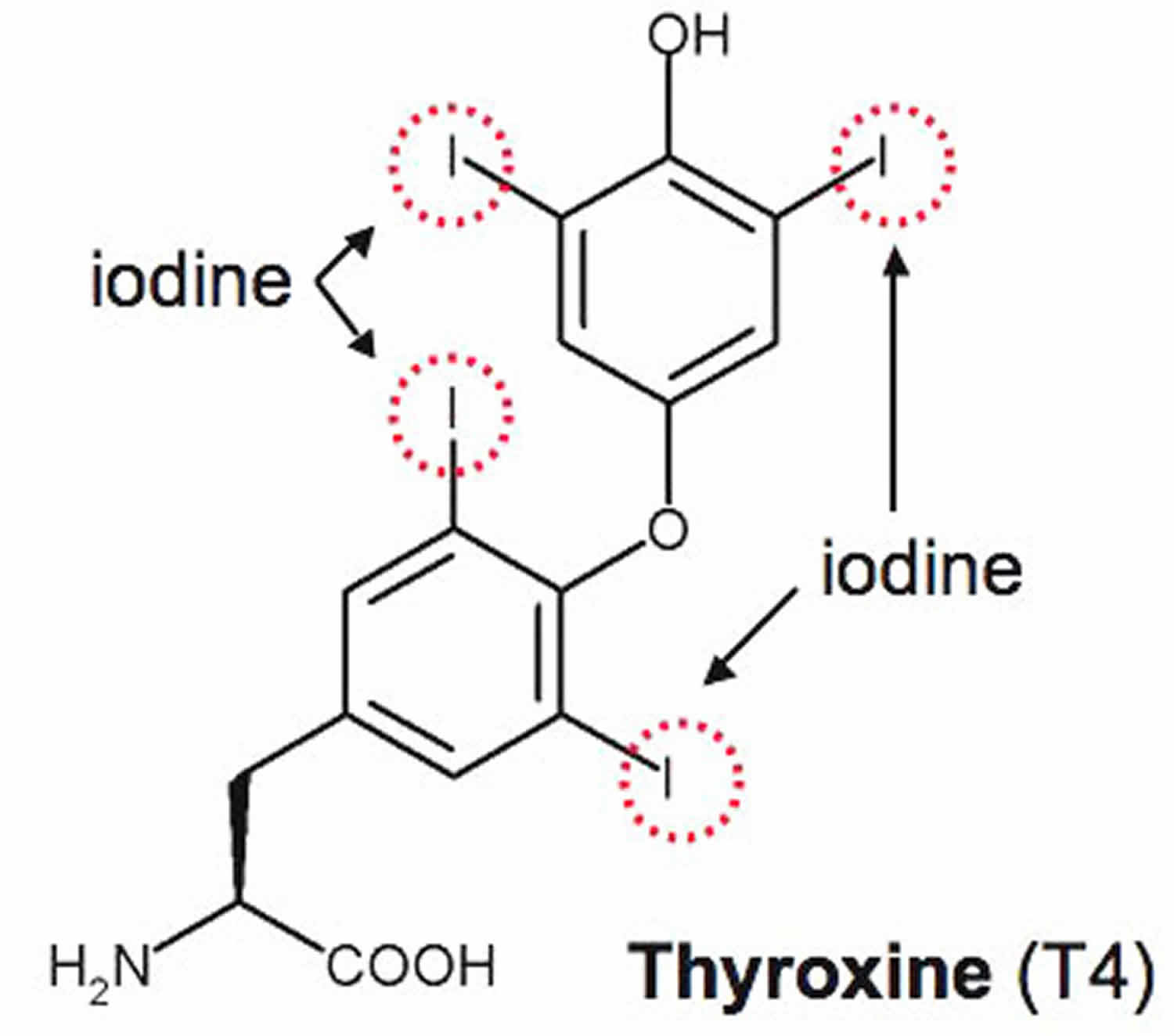
Thyroxine (T4) is one of two major hormones produced by your thyroid gland, a small butterfly-shaped organ that lies flat across the windpipe at the base of the throat. Thyroxine (T4) makes up about 90% of thyroid hormones. The other major thyroid hormone is called triiodothyronine (T3) and reverse-triiodothyronine (rT3) and together thyroxine (T4), triiodothyronine (T3) help control the rate at which your body uses energy (metabolic activity regulation) and are essential for proper brain function development in infants, as well as a wide array of effects on every organ system in your body including regulating your weight, body temperature, muscle strength, and even your mood.
Almost all of the thyroxine (T4) and triiodothyronine (T3) found in your blood is bound to protein, mainly thyroxine binding globulin (TBG). The rest is free (unbound) and is the biologically active form of the hormone (free T4 and free T3). It is the free forms of T3 and T4 that are biologically active. Free T3 is 4 to 5 times more active than free T4 in circulation. The concentration of free T4 is only about 0.1% of that of total T4. Thyroxine (T4) is converted into triiodothyronine (T3) in your liver or other tissues. Triiodothyronine (T3), like T4, is also mostly bound to protein.
When the body requires thyroid hormone, the thyroid gland releases stored thyroxine (T4) into the blood stream. Thyroxine (T4) production is regulated by a feedback system. When the level of thyroxine (T4) in the bloodstream decreases, the hypothalamus in your brain releases thyrotropin releasing hormone (TRH), which stimulates the anterior pituitary gland to produce and release thyroid-stimulating hormone (TSH). TSH (thyroid-stimulating hormone) then stimulates your thyroid gland to make and/or release more thyroxine (T4). As the blood concentration of thyroxine (T4) increases, thyroid-stimulating hormone (TSH) release is inhibited. An important mediator to thyroid hormone function is the role of iodine, which is obtained through diet. Foods rich in iodine include seafood, seaweed, and dairy products as well as iodinated salt, which is widely available throughout the United States.
If the thyroid gland does not produce sufficient thyroxine (T4), due to thyroid dysfunction or to insufficient thyroid-stimulating hormone (TSH), then the affected person experiences symptoms of hypothyroidism such as weight gain, dry skin, cold intolerance, irregular menstruation, and fatigue. Severe untreated hypothyroidism, called myxedema, can lead to heart failure, seizures, and coma. In children, hypothyroidism can stunt growth and delay sexual development.
If the thyroid gland produces too much thyroxine (T4), the rate of the person’s body functions will increase and cause symptoms associated with hyperthyroidism such as increased heart rate, anxiety, weight loss, difficulty sleeping, tremors in the hands, and puffiness around dry, irritated eyes.
The most common causes of thyroid dysfunction are related to autoimmune disorders. Graves disease causes hyperthyroidism and Hashimoto thyroiditis causes hypothyroidism. Both hyperthyroidism and hypothyroidism can also be caused by thyroiditis, thyroid cancer, and excessive or deficient production of thyroid-stimulating hormone (TSH). The effect of these conditions on thyroid hormone production can be detected and monitored by measuring the free T4.
What is reverse T3?
Reverse T3 (rT3 or REVT3) is a biologically inactive form of T3. Normally, when thyroxine (T4) is converted to triiodothyronine (T3) in your body, a certain percentage of the T3 is in the form of reverse-triiodothyronine (rT3). When the body is under stress, such as during a serious illness, thyroid hormone levels may be outside of normal ranges even though there is no thyroid disease present. Reverse T3 (rT3) may be elevated in non-thyroidal conditions, particularly the stress of illness. It is generally recommended that thyroid testing be avoided in hospitalized patients or deferred until after a person has recovered from an acute illness. Use of the reverse T3 (rT3) test remains controversial, and it is not widely requested.
Figure 1. Thyroid gland location
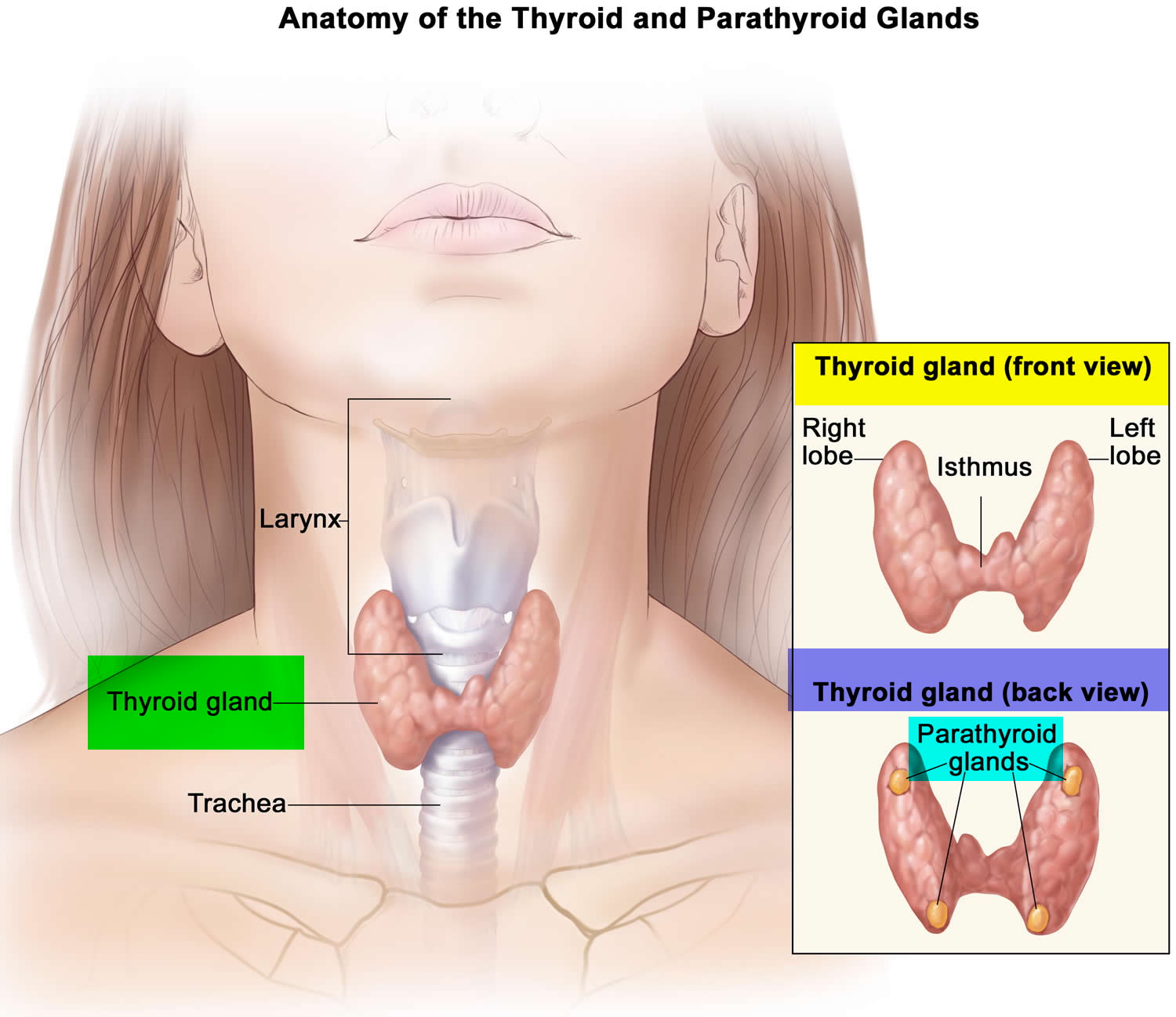
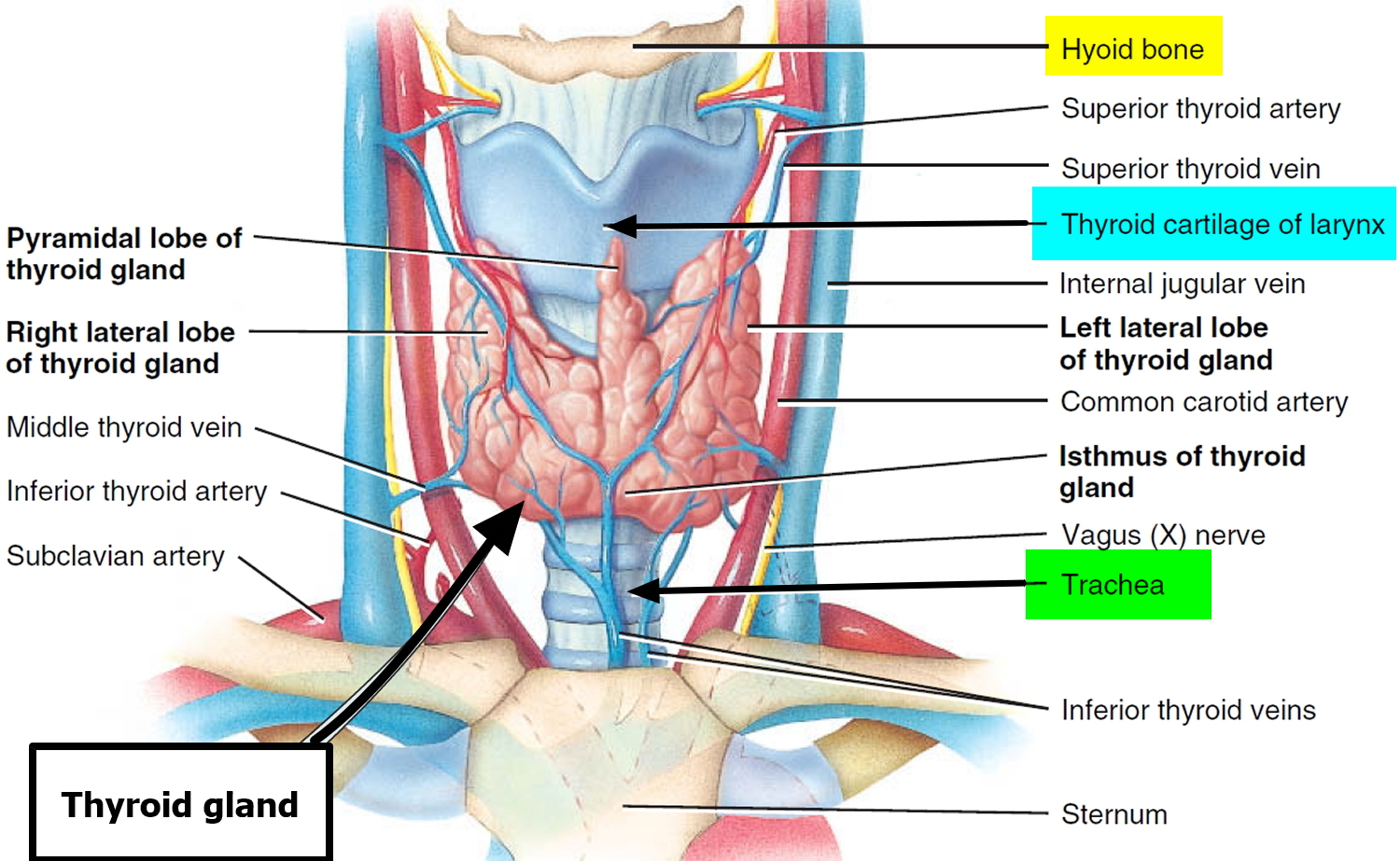
Figure 2. Thyroid gland
Control of Thyroid Hormone Secretion
Thyrotropin-releasing hormone (TRH) from the hypothalamus and thyroid-stimulating hormone (TSH) from the anterior pituitary stimulate secretion of thyroid hormones, as shown in Figure 3:
- Low blood levels of thyroxine (T4) and triiodothyronine (T3) or low metabolic rate stimulate the hypothalamus to secrete thyrotropin-releasing hormone (TRH).
- Thyrotropin-releasing hormone (TRH) enters the hypothalamic–hypophyseal portal system and flows to the anterior pituitary, where it stimulates thyrotrophs to secrete thyroid stimulating hormone (TSH).
- Thyroid stimulating hormone (TSH) stimulates virtually all aspects of thyroid follicular cell activity, including iodide trapping, hormone synthesis and secretion, and growth of the follicular cells.
- The thyroid follicular cells release thyroxine (T4) and triiodothyronine (T3) into the blood until the metabolic rate returns to normal.
- An elevated level of T3 inhibits release of TRH and TSH (negative feedback inhibition).
Conditions that increase ATP demand—a cold environment, hypoglycemia, high altitude, and pregnancy—increase the secretion of the thyroid hormones.
Figure 3. Control of Thyroid Hormone Secretion

Note: Negative Feedback Inhibition of the Anterior Pituitary Gland by the Thyroid Gland
What does thyroxine do
In your blood, thyroid hormone is predominantly transferred while bound to serum binding proteins such as thyroid-binding globulin (TBG), transthyretin, or albumin. When it reaches its target site, thyroxine (T4) and triiodothyronine (T3) can dissociate from their binding protein to enter cells either by diffusion or carrier-mediated transport. They then bind to nuclear alpha or beta receptors in the respective tissue and cause activation of certain transcription factors. This leads to the activation of certain genes in the cell type, leading to the cell-specific response thyroxine (T4) and triiodothyronine (T3) exert.
Thyroid hormones affect virtually every organ system in your body, including the heart, CNS (central nervous system), autonomic nervous system, bone, gastrointestinal tract, and metabolism. When thyroid hormone binds to its intracellular receptors in mitochondria, they cause an increase in nutrient breakdown and production of adenosine triphosphate (ATP). The generation of ATP (adenosine triphosphate) leads to an increased level of heat as a byproduct of its reactions, causing an increase in body temperature. Thyroid hormone also can act primarily on beta receptors on the heart, causing an increase in heart rate. In the gastrointestinal tract, thyroid hormone can cause an increase in gastrointestinal motility. In the brain, thyroid hormone is essential for proper neurological development; it helps in neurogenesis, neuronal migration, neuronal and glial cell differentiation, myelination, and synaptogenesis. Thyroid hormone also increases the body’s sensitivity to catecholamines, causing an increase in sympathetic tone. The effects of this hormone are magnified when there is a disease that is causing an increase or decrease in the level of the hormone.
Functions of thyroid hormones include the following:
- Increase basal metabolic rate. Thyroid hormones raise the basal metabolic rate (BMR), the rate of energy expenditure under standard or basal conditions (awake, at rest, and fasting). When basal metabolic rate increases, cellular metabolism of carbohydrates, lipids, and proteins increases. Thyroid hormones increase BMR in several ways: (1) They stimulate synthesis of additional Na+/K+ ATPases, which use large amounts of ATP to continually eject sodium ions (Na+) from cytosol into extracellular fluid and potassium ions (K+) from extracellular fluid into cytosol; (2) they increase the concentrations of enzymes involved in cellular respiration, which increases the breakdown of organic fuels and ATP production; and (3) they increase the number and activity of mitochondria in cells, which also increases ATP production. As cells produce and use more ATP, basal metabolic rate increases, more heat is given off and body temperature rises, a phenomenon called the calorigenic effect. In this way, thyroid hormones play an important role in the maintenance of normal body temperature. Normal mammals can survive in freezing temperatures, but those whose thyroid glands have been removed cannot.
- Enhance actions of catechlolamines. Thyroid hormones have permissive effects on the catecholamines (epinephrine and norepinephrine) because they up-regulate β-adrenergic receptors. Catecholamines bind to β-adrenergic receptors, promoting sympathetic responses. Therefore, symptoms of excess levels of thyroid hormone include increased heart rate, more forceful heartbeats, and increased blood pressure.
- Regulate development and growth of nervous tissue and bones. Thyroid hormones are necessary for the development of the nervous system: They promote synapse formation, myelin production, and growth of dendrites. Thyroid hormones are also required for growth of the skeletal system: They promote formation of ossification centers in developing bones, synthesis of many bone proteins, and secretion of growth hormone (GH) and insulin-like growth factors (IGFs). Deficiency of thyroid hormones during fetal development, infancy, or childhood causes severe mental retardation and stunted bone growth.
Thyroxine test
A thyroxine test helps diagnose disorders of the thyroid. The thyroid is a small, butterfly-shaped gland located near the throat. Your thyroid makes hormones that regulate the way your body uses energy. The thyroxine (T4) test measures the level of thyroxine (T4) in your blood. Too much or too little T4 can indicate thyroid disease. More commonly, the preferred initial test of choice to screen for any thyroid disorders are a TSH and free thyroxine (free T4) test. If the TSH (thyroid-stimulating hormone) level is abnormal, it will usually be followed up with a test for free T4. These determine whether the abnormality arises centrally from the thyroid gland or peripherally from the pituitary gland in your brain. If a diagnosis of hypothyroidism is suspected, TSH levels will be abnormally increased while thyroxine (T4) levels will be decreased. If a diagnosis of hyperthyroidism is suspected, TSH levels will be decreased while T4 levels will be abnormally increased.
A free T4 test may be used along with or following a TSH test and sometimes with a free T3 test to:
- Help detect too much or too little thyroid hormone (hyperthyroidism and hypothyroidism) and diagnose the cause
- Distinguish between different thyroid disorders
- Help diagnose pituitary disorders
- Aid in the diagnosis of female infertility
- Monitor the effectiveness of treatment in a person with known thyroid disorder
- Monitor people with pituitary disease, to make sure that the thyroid is still working, and to monitor thyroid hormone treatment if it is not
- Monitor individuals with thyroid cancer, in which the tumors respond to TSH. TSH and T4 levels will be regularly checked to make sure that enough thyroid hormone is being given to keep TSH low without making T4 too high.
- In the United States, newborns are commonly screened for T4 levels as well as TSH concentrations to check for congenital hypothyroidism, which can cause mental retardation if left untreated.
Free T4 along with TSH may sometimes be used to screen for thyroid disorders, but expert opinions vary on who can benefit from screening and at what age to begin.
If a health practitioner suspects that someone may have an autoimmune-related thyroid condition, then thyroid antibodies may be ordered along with a free T4 test.
Sometimes a total T3 or free T3 will also be performed. Often, the laboratory will do this follow-up testing automatically. This is known as reflex testing and it saves your healthcare practitioner time from having to wait for the results of the initial test and then requesting additional testing to confirm or clarify a diagnosis. Reflex tests are typically performed on the original sample that was submitted when the initial test was requested.
As an alternative, a thyroid panel may be requested by your health practitioner. This means that all three tests will be performed at the same time to get a more complete initial picture of thyroid function.
The thyroid panel usually includes:
- TSH (thyroid-stimulating hormone) – to test for hypothyroidism, hyperthyroidism and to monitor treatment for a thyroid disorder
- Free T4 (thyroxine) – to test for hypothyroidism and hyperthyroidism; may also be used to monitor treatment
- Free T3 or total T3 (triiodothyronine) – to test for hyperthyroidism; may also be used to monitor treatment
A test that measures both free and bound T4 is called a total T4 test. Other tests measure just free T4. A free T4 test is considered more accurate than a total T4 test for checking thyroid function.
The total thyroxine (T4) and total triiodothyronine (T3) tests have been used for many years, but they can be affected by the amount of protein available in your blood to bind to the hormone. The free T4 and free T3 tests are not affected by protein levels and are thought by many to be more accurate reflections of thyroid hormone function. In most cases, the free T4 test has replaced that of the total T4 test. However, some professional guidelines recommend the total triiodothyronine (T3) test, so either total triiodothyronine (T3) or free T3 test may be used to assess thyroid function.
Sometimes a T3 resin uptake (T3RU) test is included to calculate, along with the thyroxine (T4) value, the free thyroxine index (FTI), another method for evaluating thyroid function that corrects for changes in certain proteins that can affect total thyroxine (T4) levels. Other lab tests such as TSH receptor antibodies or antibodies to thyroid peroxidase can help aid in the diagnosis of Graves disease or Hashimoto thyroiditis respectively.
TSH is produced by the anterior pituitary gland and is part of the body’s feedback system to maintain stable amounts of the thyroid hormones thyroxine (T4) and triiodothyronine (T3) in your blood. When thyroid hormone levels decrease, the pituitary is stimulated to release TSH. TSH in turn stimulates the production and release of thyroxine (T4) and triiodothyronine (T3) by your thyroid gland. When the system is functioning normally, thyroid production turns on and off to maintain constant blood thyroid hormone levels.
When is thyroxine (T4) test ordered?
A thyroxine test may be ordered when symptoms suggest hypo- or hyperthyroidism due to a condition affecting the thyroid. Free T4 testing may be ordered along with other thyroid tests on a regular basis when a person is undergoing treatment for a thyroid disorder.
In pregnant women with thyroid disorders, the health practitioner is likely to order thyroid testing early and late in the pregnancy and for a time period following delivery to monitor the mother and baby.
Thyroid hormone screening is commonly performed on newborns in the United States as part of newborn screening programs.
Thyroid disease is much more common in women and most often occurs under the age of 40. It also tend to run in families. You may need a thyroxine test if a family member has ever had thyroid disease or if you have symptoms of having too much thyroid hormone in your blood, a condition called hyperthyroidism, or symptoms of having too little thyroid hormone, a condition called hypothyroidism.
Signs and symptoms of hypothyroidism may include:
- Weight gain
- Dry skin
- Constipation
- Cold intolerance
- Puffy skin
- Hair loss
- Fatigue
- Menstrual irregularity in women
- Enlarged thyroid gland (goiter)
Signs and symptoms of hyperthyroidism may include:
- Increased heart rate
- Anxiety
- Weight loss
- Difficulty sleeping
- Tremors in the hands
- Weakness
- Diarrhea
- Puffiness around the eyes, dryness, irritation, or bulging of the eyes
Thyroxine (T4) Normal Levels
TOTAL Thyroxine (T4)
- Adult (> or =20 years): 4.5-11.7 mcg/dL
- Pediatric:
- 0-5 days: 5.0-18.5 mcg/dL
- 6 days-2 months: 5.4-17.0 mcg/dL
- 3 -11 months: 5.7-16.0 mcg/dL
- 1 -5 years: 6.0-14.7 mcg/dL
- 6 -10 years: 6.0-13.8 mcg/dL
- 11 -19 years: 5.9-13.2 mcg/dL
FREE Thyroxine (T4)
- Adult (> or =20 years of age): 0.9-1.7 ng/dL
- Pediatric:
- 0-5 days: 0.9-2.5 ng/dL
- 6 days-2 months: 0.9-2.2 ng/dL
- 3-11 months: 0.9-2.0 ng/dL
- 1-5 years: 1.0-1.8 ng/dL
- 6-10 years: 1.0-1.7 ng/dL
- 11-19 years: 1.0-1.6 ng/dL
What do the thyroxine results mean?
Your results may come in the form of total T4, free T4, or a free T4 index.
- The free T4 index includes a formula that compares free and bound T4.
- High levels of any of these tests (total T4, free T4, or free T4 index) may indicate an overactive thyroid, also known as hyperthyroidism.
- Low levels of any of these tests (total T4, free T4, or free T4 index) may indicate an underactive thyroid, also known as hypothyroidism.
The test results alone are not diagnostic but will prompt the health practitioner to perform additional testing to investigate the cause of the excess or deficiency.
Many medications—including estrogen, certain types of birth control pills, and large doses of aspirin—can affect total T4 test results and their use should be discussed with the health practitioner prior to testing. In general, free T4 levels are not affected by these medications.
A higher than normal level of T4 may be due to conditions that involve an overactive thyroid, including:
- Graves disease
- Taking too much thyroid hormone medicine
- Thyroiditis
- Toxic goiter or toxic thyroid nodules
- Some tumors of the testes or ovaries (rare)
- Getting medical imaging tests with contrast dye that contains iodine (rare, and only if there is a problem with the thyroid)
- Eating a lot of foods that contain iodine (very rare, and only if there is a problem with the thyroid)
A lower than normal level of T4 may be due to:
- Hypothyroidism (including Hashimoto disease and other disorders involving an underactive thyroid)
- Severe acute illness
- Malnutrition or fasting
- Use of certain medicines
It is important to note that thyroid tests are a “snapshot” of what is occurring within a dynamic system. An individual person’s total T4, free T4, total T3, free T3, and/or TSH results may vary and may be affected by:
- Increases, decreases, and changes (inherited or acquired) in the proteins that bind thyroxine (T4) and triiodothyronine (T3)
- Pregnancy
- Estrogen and other drugs
- Liver disease
- Systemic illness
- Resistance to thyroid hormones
- Pituitary dysfunction
If your T4 test results are not normal, your health care provider will likely order more thyroid tests to help make a diagnosis. These may include:
- T3 thyroid hormone tests. T3 is another hormone made by the thyroid.
- A TSH (thyroid stimulating hormone) test. TSH is a hormone made by the pituitary gland. It stimulates the thyroid to produce T4 and T3 hormones.
- Tests to diagnose Graves’ disease, an autoimmune disease that causes hyperthyroidism
- Tests to diagnose Hashimoto’s thyroiditis, an autoimmune disease that causes hypothyroidism
Both decreased and increased free T4 results are associated with a variety of temporary and chronic thyroid conditions. Low free T4 results in conjunction with a low TSH level or high free T4 results along with a high TSH may indicate a pituitary gland condition.
The following table summarizes some examples of typical test results and their potential meaning.
| TSH | Free T4 | Free or total T3 | Interpretation |
|---|---|---|---|
| High | Normal | Normal | Mild (subclinical) hypothyroidism |
| High | Low | Low or normal | Hypothyroidism |
| Low | Normal | Normal | Mild (subclinical) hyperthyroidism |
| Low | High or normal | High or normal | Hyperthyroidism |
| Low | Low or normal | Low or normal | Nonthyroidal illness; pituitary (secondary) hypothyroidism |
| Normal | High | High | Thyroid hormone resistance syndrome (a mutation in the thyroid hormone receptor decreases thyroid hormone function) |
The above test results alone are not diagnostic but will prompt a health practitioner to perform additional testing to investigate the cause of the excess or deficiency and thyroid disorder. As examples, the most common cause of hyperthyroidism is Graves disease and the most common cause of hypothyroidism is Hashimoto thyroiditis.
When used for monitoring treatment for thyroid or pituitary disorders, results of thyroid tests will inform the health practitioner whether treatment is effective and/or whether an adjustment to dose is necessary. For example, in people with hyperthyroidism, free T4, free T3, and TSH are regularly checked while they are on anti-thyroid drugs to assure that the drugs are working and to decrease doses if thyroid hormone levels get too low. In people with hypothyroidism, TSH and free T4 are regularly checked to assure that the right dose of thyroid hormone is being given to make TSH normal.
Is there anything else I need to know about a thyroxine test?
Thyroid changes can happen during pregnancy. These changes are usually not significant, but some women can develop thyroid disease during pregnancy. Hyperthyroidism happens in about one in every 500 pregnancies, while hypothyroidism happens in approximately one in every 250 pregnancies. Hyperthyroidism, and less often, hypothyroidism, may remain after pregnancy. If you develop a thyroid condition during pregnancy, your health care provider will monitor your condition after your baby is born. Also, if you have a history of thyroid disease, be sure to talk with your health care provider if you are pregnant or are thinking of becoming pregnant.
Are there things that I can do to raise or lower my free T4 level?
In general, free T4 does not respond to lifestyle changes. What is important is that the thyroid gland is producing adequate amounts of free T4 and the body’s feedback mechanism is responding appropriately. For those who do not produce enough free T4, thyroid hormone replacement medication can be given.
What is Free Thyroxine Index?
Free Thyroxine Index (FTI) and it is an estimation of the free T4 concentration. It is sometimes referred to as T7. It is a calculated value determined from the total T4 test and some estimation of the level of thyroid hormone binding proteins. The original test for estimating the level of binding proteins was called the T3-uptake test and later versions were called T-uptake methods. These are rarely used now that there are methods available to measure free T4 and T3 directly.
What other tests may be ordered in addition to a thyroid panel?
Blood tests that may be performed in addition to a thyroid panel may include:
- Thyroid antibodies – to help differentiate different types of thyroiditis and identify autoimmune thyroid conditions
- Calcitonin – to help detect the presence of excessive calcitonin production as can occur with C-cell hyperplasia and medullary thyroid cancer
- Thyroglobulin – to monitor treatment of thyroid cancer
- Thyroxine-binding globulin (TBG) – to evaluate patients with abnormal T4 and T3 levels
Thyroxine medication
Levothyroxine (L-thyroxine) is a thyroid medicine that replaces thyroxine (T4) hormone normally produced by your thyroid gland to regulate the body’s energy and metabolism.
Levothyroxine is given when your thyroid does not produce enough of thyroxine (T4) hormone on its own.
Levothyroxine is used to treat hypothyroidism (low thyroid hormone). It is also used to treat or prevent goiter (enlarged thyroid gland), which can be caused by hormone imbalances, radiation treatment, surgery, or cancer.
You may not be able to take levothyroxine if you have certain medical conditions. Tell your doctor if you have an untreated or uncontrolled adrenal gland disorder, a thyroid disorder called thyrotoxicosis, or if you have any recent or current symptoms of a heart attack.
Levothyroxine should not be used to treat obesity or weight problems. Dangerous side effects or death can occur from the misuse of this medicine, especially if you are taking any other weight-loss medications or appetite suppressants.
Before taking levothyroxine
Levothyroxine should not be used to treat obesity or weight problems. Dangerous side effects or death can occur from the misuse of this medicine, especially if you are taking any other weight-loss medications or appetite suppressants.
Since thyroid hormone occurs naturally in the body, almost anyone can take levothyroxine. However, you may not be able to take this medicine if you have certain medical conditions. Tell your doctor if you have:
- an untreated or uncontrolled adrenal gland disorder;
- a thyroid disorder called thyrotoxicosis; or
- symptoms of a heart attack (chest pain or heavy feeling, pain spreading to the jaw or shoulder, nausea, sweating, general ill feeling).
Tell your doctor if you have ever had:
- a thyroid nodule;
- heart disease, a blood clot, or a blood-clotting disorder;
- diabetes (insulin or oral diabetes medication doses may need to be changed when you start taking this medicine);
- kidney disease;
- anemia (lack of red blood cells);
- osteoporosis, or low bone mineral density;
- problems with your pituitary gland; or
- any food or drug allergies.
Tell your doctor if you have recently received radiation therapy with iodine (such as Iodine-131).
If you become pregnant while taking levothyroxine, do not stop taking the medicine without your doctor’s advice. Having low thyroid hormone levels during pregnancy could harm both mother and baby. Your dose needs may be different during pregnancy.
Tell your doctor if you are breast-feeding. Your dose needs may be different while you are nursing.
Do not give this medicine to a child without medical advice. Tirosint is not approved for use by anyone younger than 6 years old.
How should I take thyroxine medication?
Take levothyroxine exactly as prescribed by your doctor. Follow all directions on your prescription label and read all medication guides or instruction sheets. Your doctor may occasionally change your dose. Use the medicine exactly as directed.
Levothyroxine works best if you take it on an empty stomach, at least 30 minutes before breakfast. Follow your doctor’s dosing instructions and try to take the medicine at the same time each day.
Swallow the tablet or capsule whole, with a full glass (8 ounces) of water. The tablet may dissolve very quickly and could swell in your throat.
Certain medicines can make levothyroxine less effective if taken at the same time. If you use any of the following drugs, avoid taking them within 4 hours before or 4 hours after you take this medicine:
- calcium carbonate (Alka-Mints, Caltrate, Os-Cal, Oyster Shell Calcium, Rolaids Soft Chew, Tums, and ot
Levothyroxine doses are based on weight in children. Your dose needs may change if you gain or lose weight.
It may take several weeks before your body starts to respond to levothyroxine. Keep using this medicine even if you feel well. You may need to use this medicine for the rest of your life.
You may need frequent medical tests. Tell any doctor, dentist, or surgeon who treats you that you are using this medicine.
Store at room temperature away from moisture and heat.
Do not share this medicine with another person, even if they have the same symptoms you have.
Thyroxine medication side effects
Get emergency medical help if you have signs of an allergic reaction to levothyroxine: hives; difficult breathing; swelling of your face, lips, tongue, or throat.
Call your doctor at once if you have:
- irregular heart rate;
- chest pain, feeling short breath;
- fever, hot flashes, sweating;
- feeling unusually cold;
- weakness, tiredness, sleep problems (insomnia);
- memory problems, feeling depressed or irritable;
- headache, leg cramps, muscle aches;
- feeling nervous or irritable;
- dryness of your skin or hair, hair loss;
- changes in your menstrual periods; or
- vomiting, diarrhea, appetite changes, weight changes.
Certain side effects may be more likely in older adults.
Common levothyroxine side effects may include:
- muscle weakness;
- headache, leg cramps;
- tremors, nervousness, trouble sleeping;
- diarrhea; or
- skin rash, mild hair loss.
Less Common
- chest pain or discomfort
- decreased urine output
- difficult or labored breathing
- difficulty with swallowing
- dilated neck veins
- extreme fatigue
- fainting
- fast, slow, irregular, pounding, or racing heartbeat or pulse
- fever
- heat intolerance
- hives or welts, skin itching, rash, or redness
- irregular breathing
- irritability
- menstrual changes
- nausea
- pain or discomfort in the arms, jaw, back, or neck
- sweating
- swelling of the eyes, face, lips, throat, or tongue
- tightness in the chest
- tremors
Rare
- blurred or double vision
- dizziness
- eye pain
- lack or slowing of normal growth in children
- limp or walk favoring one leg
- pain in the hip or knee
- seizures
- severe headache
Symptoms of thyroxine medication overdose
Get emergency help immediately if any of the following symptoms of overdose occur while taking levothyroxine:
- change in consciousness
- cold, clammy skin
- confusion
- disorientation
- fast or weak pulse
- lightheadedness
- loss of consciousness
- sudden headache
- sudden loss of coordination
- sudden slurring of speech
Common-effects:
- Nervousness
- Insomnia
- Mild elevation of temperature
- Blood pressure elevation
- Loose stools
Rare symptoms:
- Coma
- Convulsions
- Acute psychosis
- Thyroid storm
- Tachycardia, arrhythmias
Thyroxine medication treatment
- Gastric lavage (within hours of ingestion).
- Emetic agents (not advised)
- Propranolol (10-40 mg 3 times daily)
- Activated Charcoal (1g/kg p.o.)
- Dexamethasone (4 mg p.o. daily)
- Sodium ipodate, if available
- Cholestyramine (4g every 8h p.o.)
- Propylthiouracil (PTU) (May inhibit conversion of T4>T3)
- Activated charcoal hemoperfusion
- Plasmapheresis (seldom necessary)
- Hemodialysis (probably of limited value)
- Thyroid storm: demands treatment in an Intensive Care Unit.
Administration of activated charcoal is a common practice in many drug overdoses and is an agent that can prevent absorption of several drugs from the gastro-intestinal system 2. However, in many reports repeated doses of activated charcoal were ineffective in accelerating the elimination of levothyroxine, probably due to high uptake in the duodenum and jejuno-ileum.
Hemoperfusion using activated charcoal is a rather complicated procedure but has been reported to be highly effective in decreasing total serum levels. It should be reserved for adult patients with severe intoxication by very large doses of thyroxine and the same applies to plasmapheresis which has been seldom used.
Cholestyramine, an ion-exchange resin (Questran ®), can be administered in the usual dose of 4 grams every 8 hours orally. This drug binds thyroxine and enhances its elimination.
Glucocorticoids (Dexamethasone 4 mg orally) decrease the conversion of LT4 to T3, the active hormone. Sodium Ipodate (oral cholecystographic agent) has also been used for blocking the conversion of LT4 to T3, but it is no longer generally available.
Beta-blockers such as propranolol, are useful to ameliorate the metabolic effects of thyroid hormone, mostly on the cardiac system (controlling tachycardia, preventing arrhythmias). Seizures may be treated with phenytoin and phenobarbital. Propylthiouracil (PTU) might be used for blocking the conversion of T4 to T3 but may have very limited usefulness in the presence of a large load of LT4.
Hemodialysis has been used in severe cases, but it is probably of limited value since both T3 and T4 are highly protein-bound.
- Melmed S, Polonsky KS, Larsen PR, et al: Williams textbook of Endocrinology. 12th edition. Elsevier Saunders Company, 2011, pp 348-414[↩]
- Medeiros-Neto G. Thyroxine Poisoning. 2018 Jul 17. In: De Groot LJ, Chrousos G, Dungan K, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK279036[↩]





{kind=link}