Contents
What is Turner syndrome
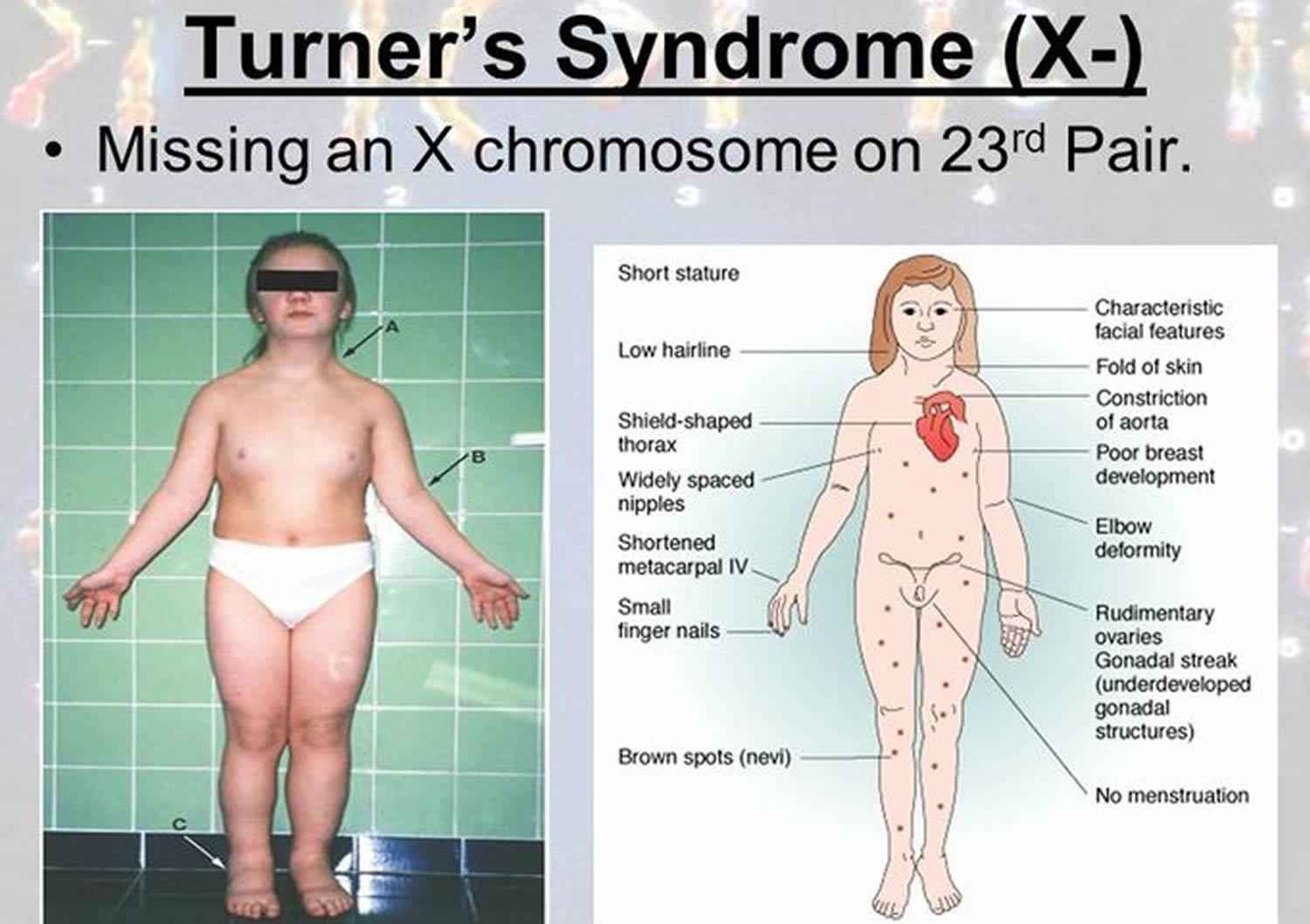
Turner syndrome is a genetic disorder affecting some women and girls. A girl with Turner syndrome only has one normal X sex chromosome, rather than the usual two (XX) – this is also known as monosomy X. This chromosome variation happens randomly when the baby is conceived in the womb. It is not linked to the mother’s age. Turner syndrome is sometimes called Bonnevie-Ullrich syndrome or Ullrich-Turner syndrome. It can affect development before and after birth. Turner syndrome might cause problems with hearing, vision and infertility, but usually not with intellectual ability. Hormones can help deal with some of problems.
First described in 1938 by Dr. Henry Turner, Turner syndrome is a condition that occurs in 1 out of every 2,000-4,000 females in America. Turner syndrome occurs in about 1 in 2,500 newborn girls worldwide, but it is much more common among pregnancies that do not survive to term (miscarriages and stillbirths). As many as 15% of spontaneous abortions have a 45 X karyotype. Turner syndrome does not affect men or boys.
The most common feature of Turner syndrome is short stature, which becomes evident by about age 5. An early loss of ovarian function (ovarian hypofunction or premature ovarian failure) is also very common. The ovaries develop normally at first, but egg cells (oocytes) usually die prematurely and most ovarian tissue degenerates before birth. Many affected girls do not undergo puberty unless they receive hormone therapy, and most are unable to conceive (infertile). A small percentage of females with Turner syndrome retain normal ovarian function through young adulthood.
About 30 percent of females with Turner syndrome have extra folds of skin on the neck (webbed neck), a low hairline at the back of the neck, puffiness or swelling (lymphedema) of the hands and feet, skeletal abnormalities, or kidney problems. One third to one half of individuals with Turner syndrome are born with a heart defect, such as a narrowing of the large artery leaving the heart (coarctation of the aorta) or abnormalities of the valve that connects the aorta with the heart (the aortic valve). Complications associated with these heart defects can be life-threatening.
Almost all girls with Turner syndrome:
- are shorter than average (final adult height of 136–147 cm)
- have underdeveloped ovaries (female reproductive organs), resulting in a lack of monthly periods and infertility
As height and sexual development are the two main characteristics, Turner syndrome may not be diagnosed until a girl fails to show sexual development associated with puberty, usually between the ages of 8 and 14 years.
Other characteristics of Turner syndrome can vary significantly between individuals.
They might have some or all of the following problems:
- short stature and slow growth achieving an average adult height of only 4’7″ (143 cm). Adult women with Turner syndrome are on average 20 cm shorter than other adult women.
- difficulty feeding in infancy
- problems with hearing or eyesight
- problems with coordination
- puffiness of the hands and feet
- slower sexual development
- problems with the heart, arteries or kidneys.
Because girls with Turner syndrome do not have proper ovarian development, they may fail to develop secondary sexual characteristics during adolescence and may be infertile as adults.
Most girls and women with Turner syndrome have normal intelligence and a normal lifespan. Developmental delays, nonverbal learning disabilities, and behavioral problems are possible, although these characteristics vary among affected individuals.
Girls who have been diagnosed with Turner syndrome will need to have medical checks to make sure they are staying healthy and will need hormones to replace those that normally come from the ovaries.
If a woman with Turner syndrome wants to have children, she will probably need some help with her fertility.
Turner syndrome increases the risk of some other medical conditions such as:
- Celiac disease or gluten intolerance
- Bowel diseases
- Diabetes
- Low thyroid hormone (hypothyroidism)
- Osteoporosis.
Doctors may want to check for these conditions.
Turner syndrome life expectancy
There is no cure for Turner syndrome, but many of the associated symptoms can be treated.
Girls and women with Turner syndrome need ongoing medical care from a variety of specialists.
Girls and women with Turner syndrome will need to have regular health checks of their heart, kidneys and reproductive system throughout their lives. However, it is usually possible to lead a relatively normal and healthy life.
Life expectancy is slightly reduced, but it can be improved with regular health checks to identify and treat potential problems at an early stage.
Figure 1. Normal female karyotype
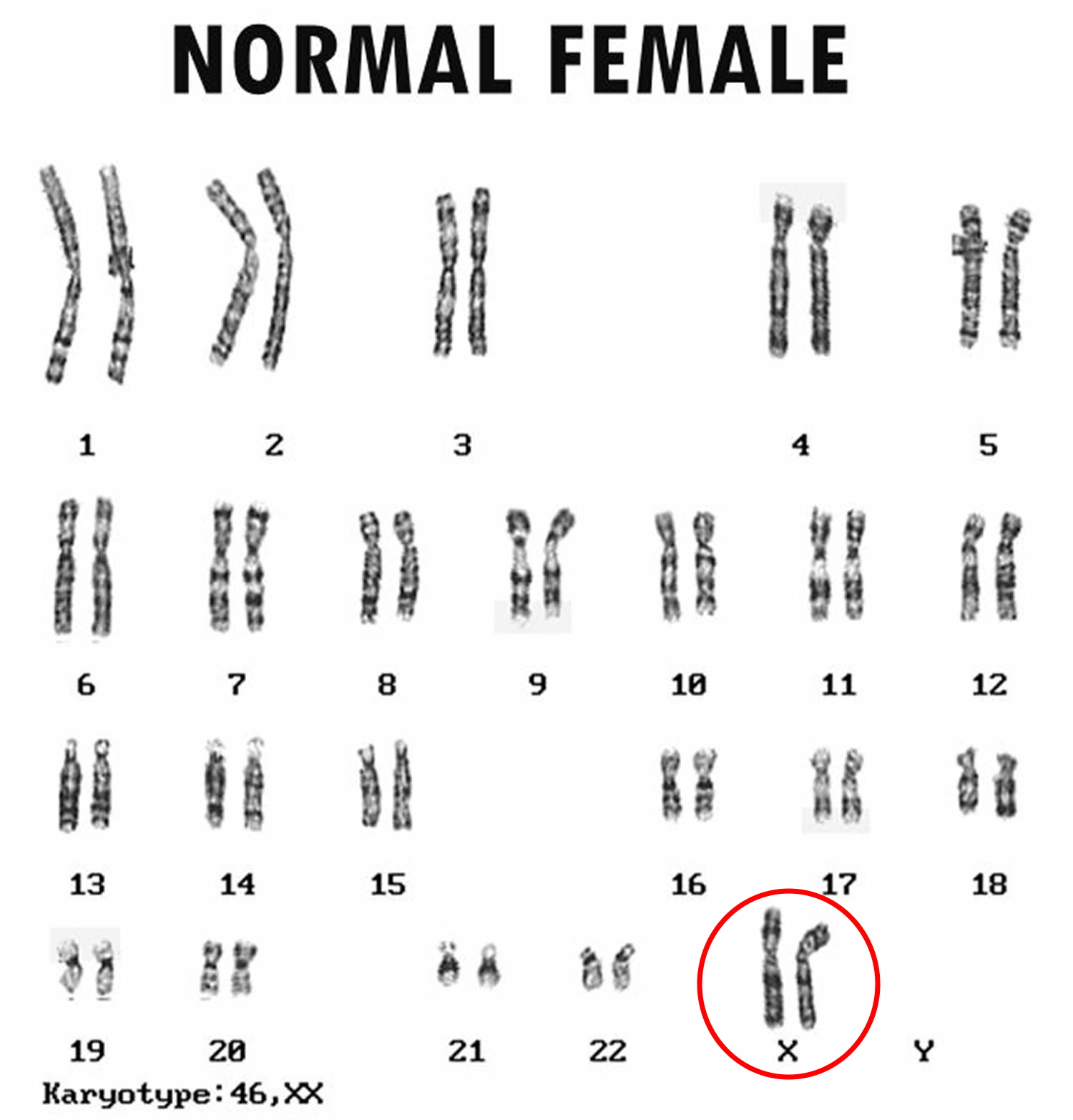
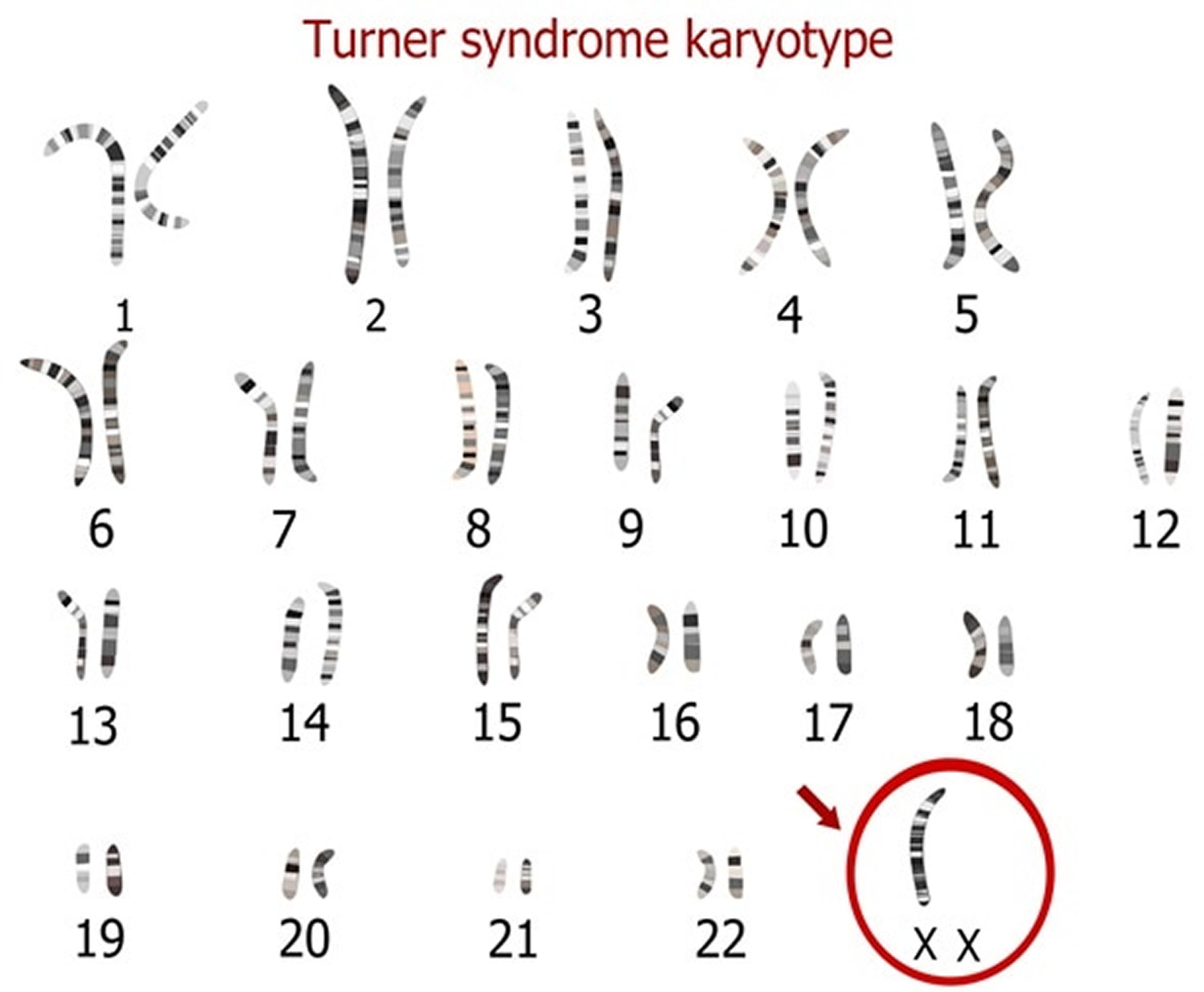
Figure 2. Turner syndrome karyotype
Turner syndrome prognosis
Those affected require special medical surveillance throughout life. Although infertility cannot be altered, pregnancy may be possible through in vitro fertilization (IVF).
Turner syndrome complications
Turner syndrome can affect the proper development of several body systems, but varies greatly among individuals with the syndrome. Complications that can occur include:
- Heart problems. Many infants with Turner syndrome are born with heart defects or even slight abnormalities in heart structure that increase their risk of serious complications. Heart defects often include problems with the aorta, the large blood vessel that branches off the heart and delivers oxygen-rich blood to the body.
- High blood pressure. Women with Turner syndrome have an increased risk of high blood pressure — a condition that increases the risk of developing diseases of the heart and blood vessels.
- Hearing loss. Hearing loss is common with Turner syndrome. In some cases, this is due to the gradual loss of nerve function. An increased risk of frequent middle ear infections can also result in hearing loss.
- Vision problems. Girls with Turner syndrome have an increased risk of weak muscle control of eye movements (strabismus), nearsightedness and other vision problems.
- Kidney problems. Girls with Turner syndrome may have some malformation of the kidneys. Although these abnormalities generally don’t cause medical problems, they may increase the risk of high blood pressure and urinary tract infections.
- Autoimmune disorders. Girls and women with Turner syndrome have an increased risk of an underactive thyroid (hypothyroidism) due to the autoimmune disorder Hashimoto’s thyroiditis. They also have an increased risk of diabetes. Some women with Turner syndrome have gluten intolerance (celiac disease) or inflammatory bowel disease.
- Skeletal problems. Problems with the growth and development of bones increase the risk of abnormal curvature of the spine (scoliosis) and forward rounding of the upper back (kyphosis). Women with Turner syndrome are also at increased risk of developing weak, brittle bones (osteoporosis).
- Learning disabilities. Girls and women with Turner syndrome usually have normal intelligence. However, there is increased risk of learning disabilities, particularly with learning that involves spatial concepts, math, memory and attention.
- Mental health issues. Girls and women with Turner syndrome may have difficulties functioning well in social situations and have an increased risk of attention-deficit/hyperactivity disorder (ADHD).
- Infertility. Most women with Turner syndrome are infertile. However, a very small number of women may become pregnant spontaneously, and some can become pregnant with fertility treatment.
- Pregnancy complications. Because women with Turner syndrome are at increased risk of complications during pregnancy, such as high blood pressure and aortic dissection, they should be evaluated by a cardiologist before pregnancy.
Turner syndrome causes
A girl with Turner syndrome only has one normal X sex chromosome, rather than the usual two (XX).
Everyone is born with 23 pairs of chromosomes. One pair of chromosomes – the sex chromosomes – determines the baby’s gender.
One sex chromosome comes from the father and the other comes from the mother. The mother’s contribution is always an X chromosome. The father’s contribution can either be an X or a Y chromosome.
A baby girl usually has two X chromosomes (XX), and boys have an X and a Y chromosome (XY). The Y chromosome determines “maleness”, so if it is missing – as in Turner syndrome – the sex of the child will invariably be female.
A female with Turner syndrome is missing part or all of one sex chromosome. This means she has just one complete X chromosome and the other sex chromosome is missing or structurally altered. The missing genetic material affects development before and after birth.
About half of individuals with Turner syndrome have monosomy X, which means each cell in the individual’s body has only one copy of the X chromosome instead of the usual two sex chromosomes. Turner syndrome can also occur if one of the sex chromosomes is partially missing or rearranged rather than completely absent. Some women with Turner syndrome have a chromosomal change in only some of their cells, which is known as mosaicism. Women with Turner syndrome caused by X chromosome mosaicism are said to have mosaic Turner syndrome.
Researchers have not determined which genes on the X chromosome are associated with most of the features of Turner syndrome. They have, however, identified one gene called SHOX that is important for bone development and growth. The loss of one copy of this gene likely causes short stature and skeletal abnormalities in women with Turner syndrome.
Most cases of Turner syndrome are not inherited. When this condition results from monosomy X, the chromosomal abnormality occurs as a random event during the formation of reproductive cells (eggs and sperm) in the affected person’s parent. An error in cell division called nondisjunction can result in reproductive cells with an abnormal number of chromosomes. For example, an egg or sperm cell may lose a sex chromosome as a result of nondisjunction. If one of these atypical reproductive cells contributes to the genetic makeup of a child, the child will have a single X chromosome in each cell and will be missing the other sex chromosome.
Mosaic Turner syndrome is also not inherited. In an affected individual, mosaic Turner syndrome occurs as a random event during cell division in early fetal development. As a result, some of an affected person’s cells have the usual two sex chromosomes, and other cells have only one copy of the X chromosome. Other sex chromosome abnormalities are also possible in females with X chromosome mosaicism.
Rarely, Turner syndrome caused by a partial deletion of the X chromosome can be passed from one generation to the next.
The genetic alterations of Turner syndrome may be one of the following:
- Monosomy. The complete absence of an X chromosome generally occurs because of an error in the father’s sperm or in the mother’s egg. This results in every cell in the body having only one X chromosome.
- Mosaicism. In some cases, an error occurs in cell division during early stages of fetal development. This results in some cells in the body having two complete copies of the X chromosome. Other cells have only one copy of the X chromosome.
- X chromosome abnormalities. Abnormal or missing parts of one of the X chromosomes can occur. Cells have one complete and one altered copy. This error can occur in the sperm or egg with all cells having one complete and one altered copy. Or the error can occur in cell division in early fetal development so that only some cells contain the abnormal or missing parts of one of the X chromosomes (mosaicism).
- Y chromosome material. In a small percentage of Turner syndrome cases, some cells have one copy of the X chromosome and other cells have one copy of the X chromosome and some Y chromosome material. These individuals develop biologically as female, but the presence of Y chromosome material increases the risk of developing a type of cancer called gonadoblastoma.
Mosaicism in Turner Syndrome
There are different types of mosaicism. A few of these are:
- 45,X/46,XX – This can be harder to diagnose because they can, but not always, have fewer features related to Turner syndrome, because fewer cells are missing an X.
- 45,X/46,XY – This occurs in a small percentage of girls with Turner syndrome. There are small fragments of Y chromosome in their cells, which can increase the risk of developing tumors, called gonadoblastomas, in their gonads (internal sex organs). These tumors are benign, but can lead to cancerous tumors, so it is usually recommended that the ovaries be surgically removed. It is important to remember that having Y chromosome material will not make a girl with Turner syndrome have male features.
- 45,X/47XXX – This is a rare type of mosaicism in which there are 45,X cells and another cell type that has an extra X. These girls are typically taller. About 20% of those with Turner syndrome will have two X chromosomes, but one will be incomplete or have a different structure.
- Ring chromosome – There are two X chromosomes, but one is shaped like a circle with the ends joined.
- Isochromosome – The X chromosome has two long arms instead of a long and short arm.
- Deletion – This occurs when the X chromosome is missing some of its genetic material.
Turner syndrome symptoms
Girls and women who have Turner syndrome are affected in different ways.
Almost all girls with Turner syndrome will grow up to be shorter than average, with underdeveloped ovaries.
Girls with Turner syndrome will also have distinctive features and associated health conditions, some of which may be apparent from birth.
They may be born with swollen hands and feet, caused by a build-up of excess fluid in the surrounding tissues. This is known as lymphedema, and it usually clears soon after birth.
Other features that may have developed in the womb include:
- thick neck tissue
- swelling of the neck (cystic hygroma)
- being a small baby
- heart conditions
- kidney abnormalities
Growth
Babies with Turner syndrome may grow at a normal rate until three years of age. After this age, their growth slows down.
At puberty (usually at age 8 to 14), a girl with Turner syndrome will not have the normal growth spurt, even with female oestrogen hormone replacement (HRT).
Girls with Turner syndrome are typically short in relation to the height of their parents. On average, adult women with untreated Turner syndrome are 20cm (8 inches) shorter than adult women without the syndrome. Treatment with additional high-dose growth hormone reduces this difference by about 5cm (about 2 inches) on average.
Ovaries
Ovaries are the pair of female reproductive organs that produce eggs and sex hormones. During puberty, a girl’s ovaries usually begin to produce the sex hormones estrogen and, once fully mature, progesterone. These trigger periods to begin.
Around 90% of girls with Turner syndrome will not produce enough of these sex hormones, which means:
- they may not begin sexual development or fully develop breasts without female hormone replacement therapy (HRT)
- they may begin sexual development but not complete it
- they may not start their monthly periods naturally
- it’s likely they will be infertile (unable to have a baby) without assistance
Even though many women with Turner syndrome have undeveloped ovaries and are infertile, their vagina and womb develop normally. This means they are able to have a normal sex life following treatment with female hormones.
Most girls need hormone replacement therapy (HRT) with oestrogen from around 10 to 12 years of age to begin breast development, and about three years later with added progesterone to bring on monthly periods.
A minority (10%) of girls with Turner syndrome experience some physical changes naturally during puberty, but only a very small number (1%) become spontaneously pregnant.
Other symptoms
There are many other symptoms or characteristics that can affect girls and women with Turner syndrome. Some of these are listed below.
General features
- a particularly short, wide neck (webbed neck)
- a broad chest and widely spaced nipples
- arms that turn out slightly at the elbows
- a low hairline
- mouth abnormalities, which can cause problems with the teeth
- a large number of moles
- small, spoon-shaped nails
- a short fourth finger or toe
Eyes
- eyes that slant downwards
- droopy eyelids (ptosis)
- a squint (strabismus)
- lazy eye (amblyopia)
- cataracts – cloudy patches in the lens at the front of the eye
- short-sightedness (myopia)
Ears
- low-set ears
- recurring middle ear infections (otitis media) and glue ear during early childhood
- hearing loss – this can occur in later life, but is often more severe and develops earlier than the normal age-related decline in hearing
Associated conditions
Turner syndrome is often associated with a number of other health conditions. Some of these include:
- heart murmur – where the heart makes a whooshing or swishing noise between beats; this is sometimes linked to a narrowing of the main blood vessel in the heart (the aorta) and high blood pressure
- kidney and urinary tract problems – this can increase the risk of developing urinary tract infections (UTIs) and high blood pressure
- underactive thyroid gland (hypothyroidism) – this occurs in around 10-30% of women with Turner syndrome; regular blood tests are needed to detect it early before it causes symptoms
- high blood pressure (hypertension)
- osteoporosis (brittle bones) – in adult life, this may develop if oestrogen isn’t adequately replaced by HRT
- scoliosis (abnormal curvature of the spine) – this should be screened for
- diabetes – a lifelong condition that causes a person’s blood sugar level to become too high
- obesity – this increases the risk of type 2 diabetes and stroke, and can be reversed by following a healthy diet with regular exercise
- lymphedema – this can occur at any age, not just in newborn babies
- bleeding in the digestive system – caused by abnormalities in the blood vessels in the intestines
- other digestive conditions – conditions such as Crohn’s disease and ulcerative colitis are more common in females with Turner syndrome, but are still rare
Learning difficulties
Most girls with Turner syndrome have good language and reading skills. However, some have behavioral, social and specific learning difficulties.
Social intelligence
About a third of girls with Turner syndrome have problems understanding social relationships because of the way their brain develops.
This can make it difficult to sustain friendships and leads to relationship problems in later life, both at home and at work.
Spatial awareness and numeracy
Spatial awareness is the ability to understand where you are in relation to objects or other people.
More than 8 out of 10 females with Turner syndrome have difficulty understanding spatial relationships. This may cause problems when learning to drive or following directions on a map.
A similar number have some degree of difficulty learning or understanding maths. This is known as dyscalculia.
Attention and hyperactivity problems
Typically, girls with Turner syndrome will go through a phase in childhood that involves:
- physical overactivity, such as constant fidgeting and restlessness
- acting impulsively, such as breaking rules or having no sense of danger
- having a short attention span and being easily distracted
Attention and hyperactivity problems usually begin when the girl is a toddler, but may not be a serious problem until the girl starts school at four or five years of age. Girls with Turner syndrome may have difficulty settling in class.
Medicines usually given to treat symptoms of attention deficit hyperactivity disorder (ADHD) may not be as effective in cases of Turner syndrome.
The physical hyperactivity usually reduces around the time the girl starts secondary school at 11 years of age, although problems with inattention can last longer, into the teens.
Signs of Turner syndrome
Signs of Turner syndrome at birth or during infancy may include:
- Wide or weblike neck
- Low-set ears
- Broad chest with widely spaced nipples
- High, narrow roof of the mouth (palate)
- Arms that turn outward at the elbows
- Fingernails and toenails that are narrow and turned upward
- Swelling of the hands and feet, especially at birth
- Slightly smaller than average height at birth
- Slowed growth
- Cardiac defects
- Low hairline at the back of the head
- Receding or small lower jaw
- Short fingers and toes
Infants with Turner syndrome often have swelling of the hands and feet, probably reflecting changes in drainage in the lymphatic system.
In childhood, teens and adulthood
The most common signs in almost all girls, teenagers and young women with Turner syndrome are short stature and ovarian insufficiency due to ovarian failure that may have occurred by birth or gradually during childhood, the teen years or young adulthood. Signs and symptoms of these include:
- Slowed growth
- No growth spurts at expected times in childhood
- Adult height significantly less than might be expected for a female member of the family
- Failure to begin sexual changes expected during puberty
- Sexual development that “stalls” during teenage years
- Early end to menstrual cycles not due to pregnancy
- For most women with Turner syndrome, inability to conceive a child without fertility treatment
Turner syndrome diagnosis
Turner syndrome might be suspected due to symptoms, but the diagnosis needs to be confirmed by genetic testing. It is possible to test for Turner syndrome before a baby is born if the ultrasound or other prenatal tests (e.g. amniocentesis) show signs of Turner syndrome.
Sometimes a girl can have Turner syndrome and not have the condition diagnosed until childhood or puberty.
Prenatal diagnosis
A diagnosis is sometimes made during fetal development. Certain features on an ultrasound image may raise suspicion that your baby has Turner syndrome or another genetic condition affecting development in the womb.
Prenatal screening tests that evaluate the baby’s DNA in the mother’s blood (prenatal cell-free DNA screening or noninvasive prenatal screening) may also indicate an increased risk of Turner syndrome. However, doing a karyotype during pregnancy or after delivery is recommended to confirm the diagnosis.
Your pregnancy and childbirth specialist (obstetrician) may ask if you’re interested in additional tests to make a diagnosis before your baby’s birth. One of two procedures can be performed to test prenatally for Turner syndrome:
- Chorionic villus sampling. This involves taking a small piece of tissue from the developing placenta. The placenta contains the same genetic material as the baby. The chorionic villus cells can be sent to the genetics laboratory for chromosome studies.
- Amniocentesis. In this test, a sample of the amniotic fluid is taken from the uterus. The baby sheds cells into the amniotic fluid. The fluid can be sent to the genetics laboratory for study of the baby’s chromosomes in these cells.
Discuss the benefits and risks of prenatal testing with your doctor.
Pregnancy and birth
Turner syndrome may be suspected in pregnancy during a routine ultrasound scan if, for example, heart or kidney abnormalities are detected.
Lymphedema, a condition that causes swelling in the body’s tissues, can affect unborn babies with Turner syndrome, and may be visible on an ultrasound scan.
Sometimes Turner syndrome is diagnosed at birth as the result of heart problems, kidney problems or lymphedema.
Childhood
If a girl has the typical characteristics and symptoms of Turner syndrome, such as short stature, a webbed neck, a broad chest and widely spaced nipples, the syndrome may be suspected.
It is often identified during early childhood, when a slow growth rate and other common features become noticeable.
In some cases, a diagnosis is not made until puberty (sexual maturity) when breasts don’t develop or monthly periods don’t start.
Girls with Turner syndrome are typically short in relation to the height of their parents. But an affected girl who has two tall parents may be taller than some of her peers, and is less likely to be identified based on her poor growth.
Karyotypying
Karyotyping is a test that involves analyzing the 23 pairs of chromosomes (strands of genes present in all human cells).
It is often used where Turner syndrome is suspected. The test can either be carried out while the baby is inside the womb by taking a sample of amniotic fluid (amniocentesis), or after birth by taking a sample of the baby’s blood.
Tests
- Karyotyping shows 45 chromosomes with a pattern 45 X,0 (i.e., a missing sex chromosome).
- Ultrasound may reveal small or underdeveloped female reproductive organs.
- A kidney ultrasound can evaluate kidney abnormalities.
- A gynecologic exam may reveal dry vaginal lining.
- Serum luteinizing hormone (LH) is elevated.
- Serum follicle stimulating hormone (FSH) is elevated.
- Echocardiogram (heart ultrasound) and MRI of the chest are frequently performed after the diagnosis is made to evaluate possible cardiac defects.
Turner syndrome may also alter the results of the following tests:
- estriol – urine
- estriol – serum
- estradiol
Turner syndrome treatment
There is no cure for Turner syndrome, but many of the associated symptoms can be treated.
Studies indicate that much of the growth deficit in children with Turner’s Syndrome can be restored by injections of human growth hormone before growth is completed. Orally-administered replacement sex hormones at the appropriate age will promote pubertal development. Although infertility cannot be altered, pregnancy may be possible through in vitro fertilization (IVF).
Replacement with thyroid hormone is important for growth and health in patients who need it.
The primary treatments for nearly all girls and women with Turner syndrome include hormone therapies:
- Growth hormone. For most girls, growth hormone therapy — usually given daily as injections of recombinant human growth hormone — is recommended to increase height as much as possible at appropriate times during early childhood until the early teen years. Starting treatment early can improve height and bone growth. In girls with very short stature, the doctor may recommend oxandrolone in addition to the growth hormone. Oxandrolone is a hormone that helps to increase height by increasing the body’s production of protein and improving bone mineral density.
- Estrogen therapy. Most girls with Turner syndrome need to start estrogen and related hormone therapy in order to begin puberty. Often, estrogen therapy is started around age 11 or 12 years. Estrogen helps to promote breast development and improve the size (volume) of the uterus. Estrogen helps with bone mineralization, and when used with growth hormone, may also help with height. Estrogen replacement therapy usually continues throughout life, until the average age of menopause is reached.
Other treatments are tailored to address your child’s particular problems as needed. Regular checkups have shown substantial improvements in the health and quality of life for girls and women with Turner syndrome.
It’s important to help your child prepare for the transition from care with your pediatrician to adult medical and mental health care. A primary care doctor can help to continue coordination of care among a number of specialists throughout life.
Health checks
Regular health checks and preventative care and treatment are important for girls and women with Turner syndrome. This is because of the risk of complications.
Some hospitals have dedicated Turner syndrome clinics with a number of specialists, including:
- a pediatric endocrinologist – a specialist in conditions that affect the hormones of children and teenagers
- a psychologist – a specialist in managing emotional, behavioral and educational problems
- a gynecologist – a specialist in treating conditions that affect the female reproductive system
- a geneticist – a specialist in genetic and inherited conditions
- a nephrologist – a specialist in kidney conditions who helps manage high blood pressure
- an ear, nose and throat (ENT) specialist – who monitors ear conditions and hearing alongside an audiologist
- an adult endocrinologist
- a cardiologist – a heart specialist
- an obstetrician – a specialist in pregnancy and birth
If a girl or woman is diagnosed with Turner syndrome, the following areas may be monitored throughout her life.
Hearing and ears
During childhood, middle ear infections (otitis media) are more likely to develop and need to be treated quickly. About half of all women with Turner syndrome lose their hearing at a faster rate compared with normal age-related decline. This can reduce their ability to interact socially.
Blood pressure
High blood pressure (hypertension) is quite common in women with Turner syndrome, so it’s important that blood pressure is regularly checked and treated, if necessary. This may be related to underlying heart or kidney problems.
Thyroid gland
Thyroid function tests can be used to assess how well the thyroid gland is working, as girls with Turner syndrome are at a slightly greater risk of having an underactive thyroid (hypothyroidism).
Glucose levels
The glucose levels in your blood or urine may be checked to screen for diabetes, a lifelong condition that causes your blood sugar level to become too high.
Bone mineral density
Women with Turner syndrome have an increased risk of developing osteoporosis (brittle bones) in late adulthood. Bone mineral density can be measured at regular intervals using a dual energy X-ray scan (DEXA scan) to assess any change with time.
Growth hormone therapy
An endocrinologist (specialist in hormone-related conditions) will be able to carry out tests and checks on a regular basis. They will also be able to recommend appropriate treatment, such as growth hormone therapy.
Girls with Turner syndrome are entitled to receive high-dose growth hormone therapy as soon as it becomes apparent that they’re not growing normally. It will help reduce short height in adulthood.
Growth hormone therapy is a daily injection started at around five or six years of age or later. It is usually continued until the age of 15 or 16, helping them gain on average around 5cm (about 2 inches) in height.
Somatropin
The National Institute for Health and Care Excellence 1 has produced guidance about somatropin, the growth hormone sometimes used to treat Turner syndrome. Studies reviewed by the National Institute for Health and Care Excellence found somatropin increased height by around 5-9cm (2-3.5in).
There are a number of different types of somatropin available. The type used will be based on the needs of the individual following a discussion between the specialist and the girl and her parents, including any advantages and disadvantages of the treatment.
Treatment with somatropin should be stopped if:
- there is not enough growth in the first year of treatment
- the girl is near to her final height and has grown less than 2cm (0.8 inches) in a year
- the girl is unable to continue taking the medicine because of side effects or because she refuses to take it
- the girl reaches her final height
Somatropin is usually given daily as a single injection. Parents can perform the injection or the girl can be taught to do it herself. The dose will depend on the girl’s size.
Estrogen and progesterone replacement therapy
Estrogen and progesterone replacement therapy may also be recommended. Estrogen and progesterone are the female hormones responsible for sexual development. Estrogen is also important in preventing osteoporosis (brittle bones).
In girls with Turner syndrome, the ovaries (female reproductive organs) don’t work properly. As a result, the girl may not go through puberty and is likely to be unable to have a baby without help (be infertile).
Women with Turner syndrome will usually need regular sex hormone treatment until they’re about 50. After this time, the body usually stops producing Estrogen and monthly periods stop. This is known as the menopause.
Estrogen
Estrogen replacement therapy is usually started around the time of normal puberty. In girls, this is around 11 years old. It may be recommended that Estrogen replacement is started earlier in gradually increasing doses. Treatment will be tailored to the specific needs of each girl.
Estrogen triggers the changes that usually happen during puberty, such as breast development. It’s important for the health of the womb and bones (protecting against osteoporosis).
It can be given as a gel, tablet or patch. Low doses are used to start with, and gradually increased to adult levels with time and age to mimic normal puberty.
Progesterone
Progesterone replacement therapy is usually started after Estrogen therapy and will cause monthly periods to start. It also may be given alone or combined in a tablet or patch with Estrogen.
Fertility
Most women with Turner syndrome are infertile (unable to have children). A minority will be able to conceive naturally, so girls and women with Turner syndrome should have access to sexual health and contraception advice.
Assisted conception techniques, such as egg donation and in vitro fertilization (IVF), may be recommended for women with Turner syndrome who want to have children.
If a woman has Turner syndrome and becomes pregnant, she will need regular heart checks because the heart and blood vessels will be put under extra strain during pregnancy. It’s vital that her womb is healthy and has developed fully during puberty for the pregnancy to be successful.
Psychological therapy
Some girls and women with Turner syndrome may develop psychological problems, such as low self-esteem or depression.
Doctors sometimes attribute these problems to physical appearance or infertility, but they are more commonly related to difficulties understanding other people’s social behavior and how to respond appropriately. Associated problems commonly arise at home, in school and in the workplace.
Psychological therapy, such as counseling or cognitive behavioral therapy (CBT), may be recommended.
Learning difficulties
Most girls with Turner syndrome have a normal level of intelligence, but some may have specific learning difficulties and require extra support.
It’s important to seek help if your daughter is affected. Not all aspects of ability are affected equally, so an experienced psychologist should be asked to give an opinion.
You can speak to your doctor or health visitor, or the teacher at your child’s school or nursery. The school or nursery should follow guidelines about how to assess and meet your child’s special educational needs to ensure she gets the appropriate support.
Coping and support
The Turner Syndrome Society of the United States 2 and other organizations provide educational materials, resources for families and information about support groups. Groups for parents provide an opportunity to exchange ideas, develop coping strategies and locate resources.
Peer groups for girls with Turner syndrome can help reinforce self-esteem and provide a social network of people who understand how to live with Turner syndrome.





{kind=link}