Contents
- What is urinary incontinence
- What is the urinary tract?
- Types of urinary incontinence
- Urinary incontinence causes
- Risk factors for urinary incontinence
- Complications of chronic urinary incontinence
- Preventing urinary incontinence
- Urinary incontinence diagnosis
- Urinary incontinence treatment
What is urinary incontinence
Urinary incontinence is the unintentional passing of urine. It’s a common problem thought to affect millions of people.
Having urinary incontinence means you pass urine unintentionally.
When and how this happens varies depending on the type of urinary incontinence you have.
It’s a good idea to see your doctor if you have urinary incontinence. It’s a common problem, and seeing your doctor can be the first step towards finding a way to effectively manage it.
You may feel uncomfortable discussing incontinence with your doctor. But if incontinence is frequent or is affecting your quality of life, it’s important to seek medical advice because urinary incontinence may:
- Indicate a more-serious underlying condition
- Cause you to restrict your activities and limit your social interactions
- Increase the risk of falls in older adults as they rush to the toilet
What is the urinary tract?
The urinary tract is the body’s drainage system for removing wastes and extra fluid. The urinary tract includes
- two kidneys
- two ureters
- the bladder
- the urethra
The kidneys are two bean-shaped organs, each about the size of a fist. They are located just below the rib cage, one on each side of the spine. Every day, the kidneys filter about 120 to 150 quarts of blood to produce about 1 to 2 quarts of urine, composed of wastes and extra fluid. Children produce less urine than adults. The urine flows from the kidneys to the bladder through tubes called ureters. The bladder stores urine until releasing it through urination. When the bladder empties, urine flows out of the body through a tube called the urethra at the bottom of the bladder.
Figure 1. Urinary tract anatomy
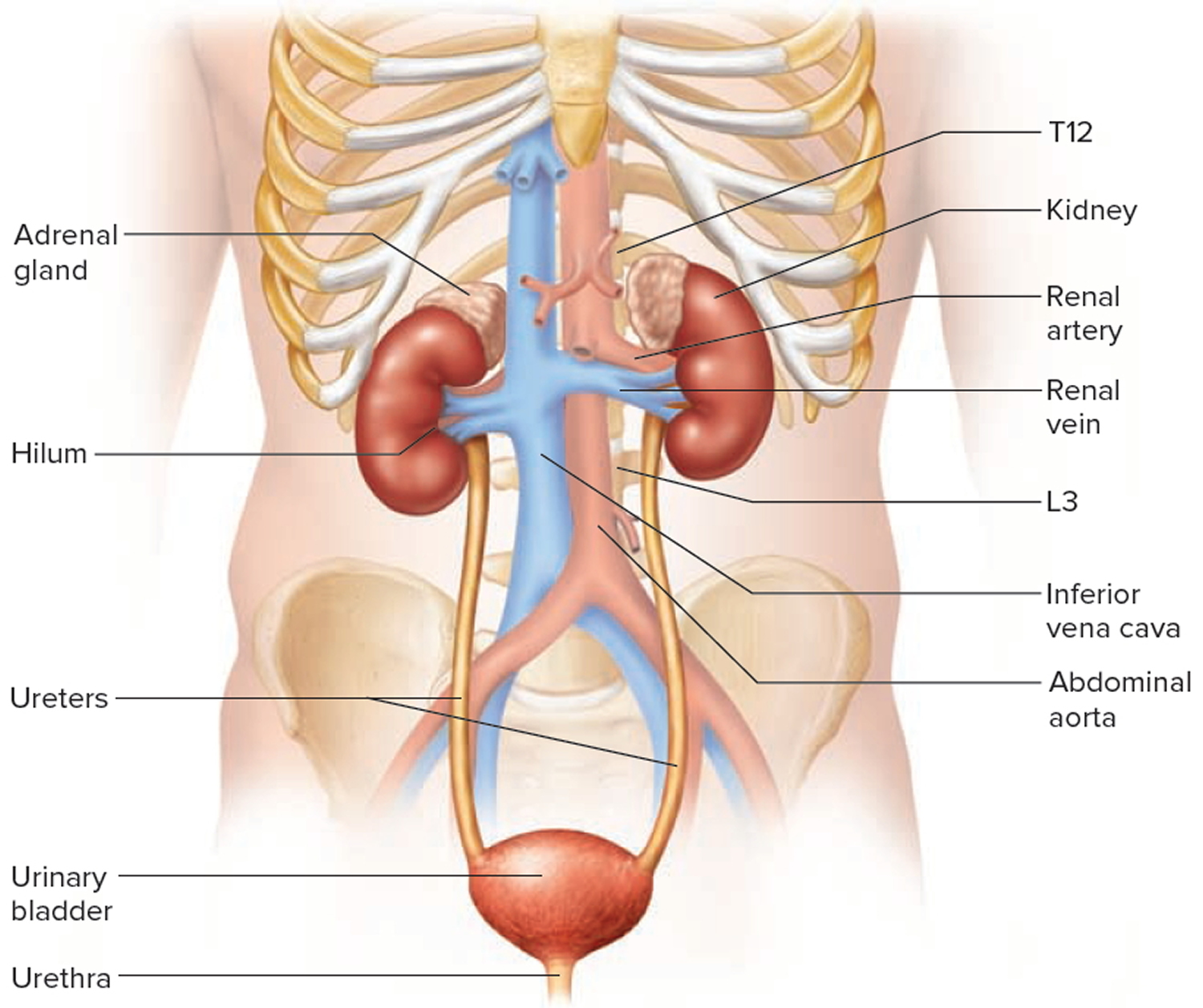
Figure 2. Urinary bladder anatomy
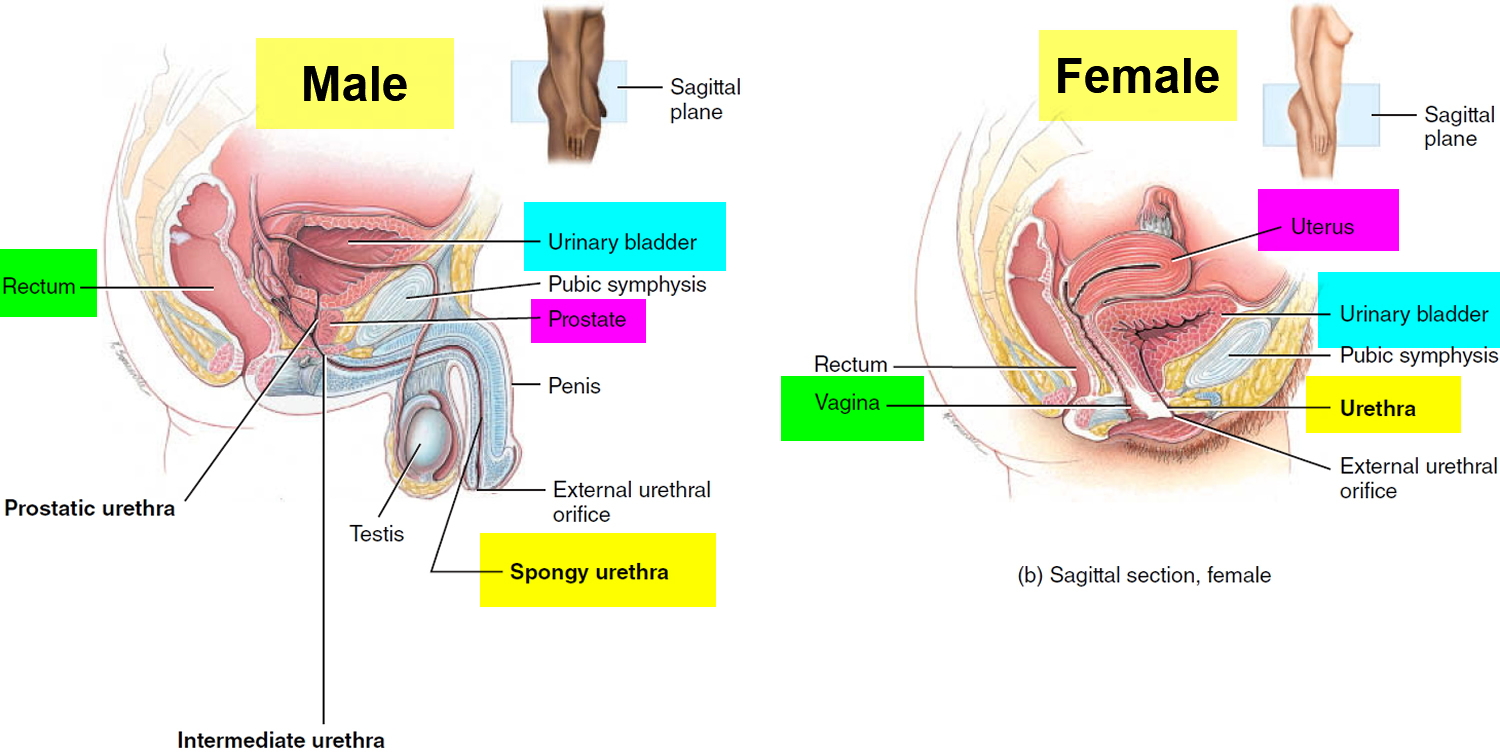
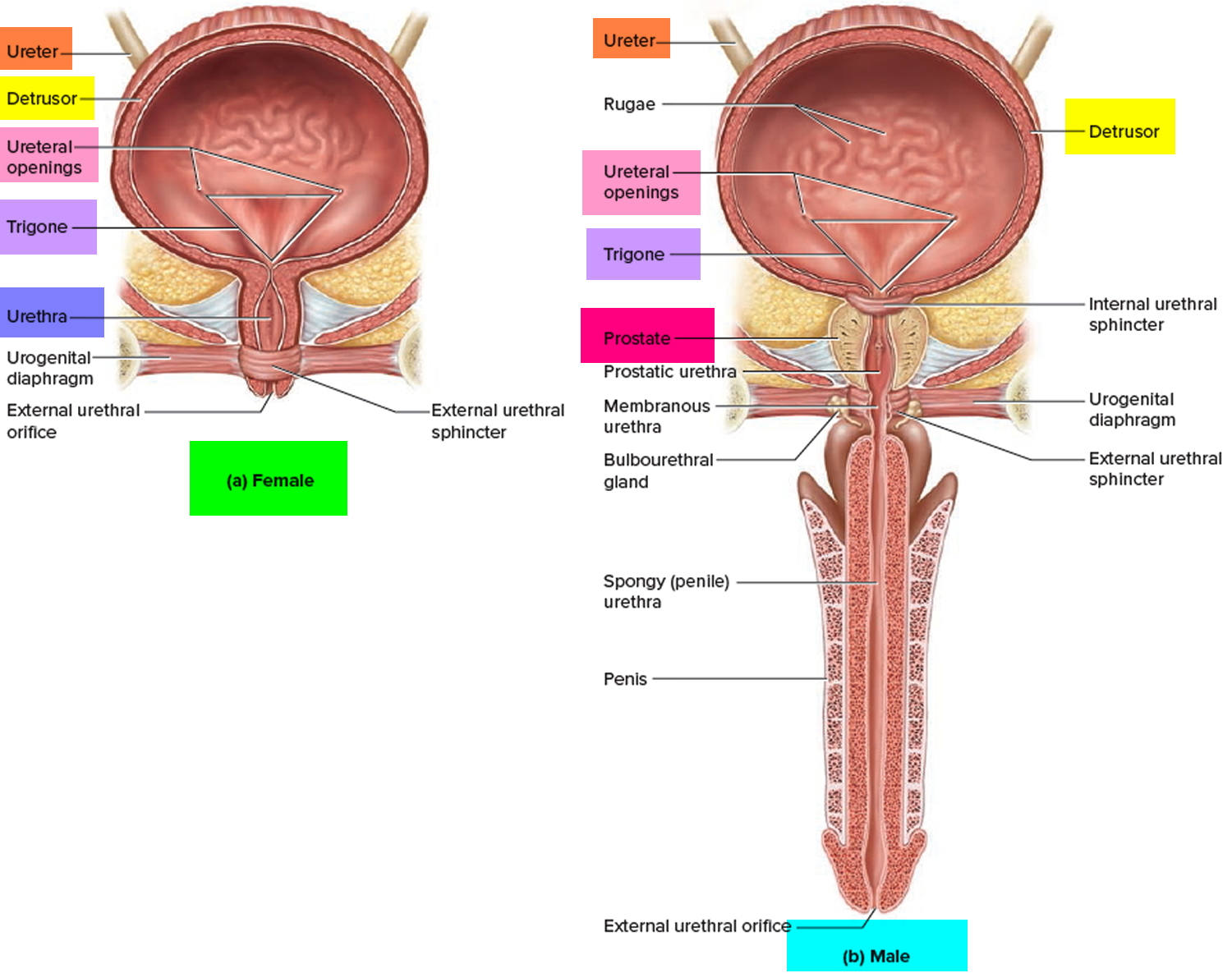
Figure 3. Urinary bladder anatomy
 What is the pelvic floor and why does it become weak in women?
What is the pelvic floor and why does it become weak in women?
The pelvic floor is a complex layer of muscles and ligaments which stretches like a hammock from the pubic bone at the front of your pelvis to the coccyx at the bottom your spine.
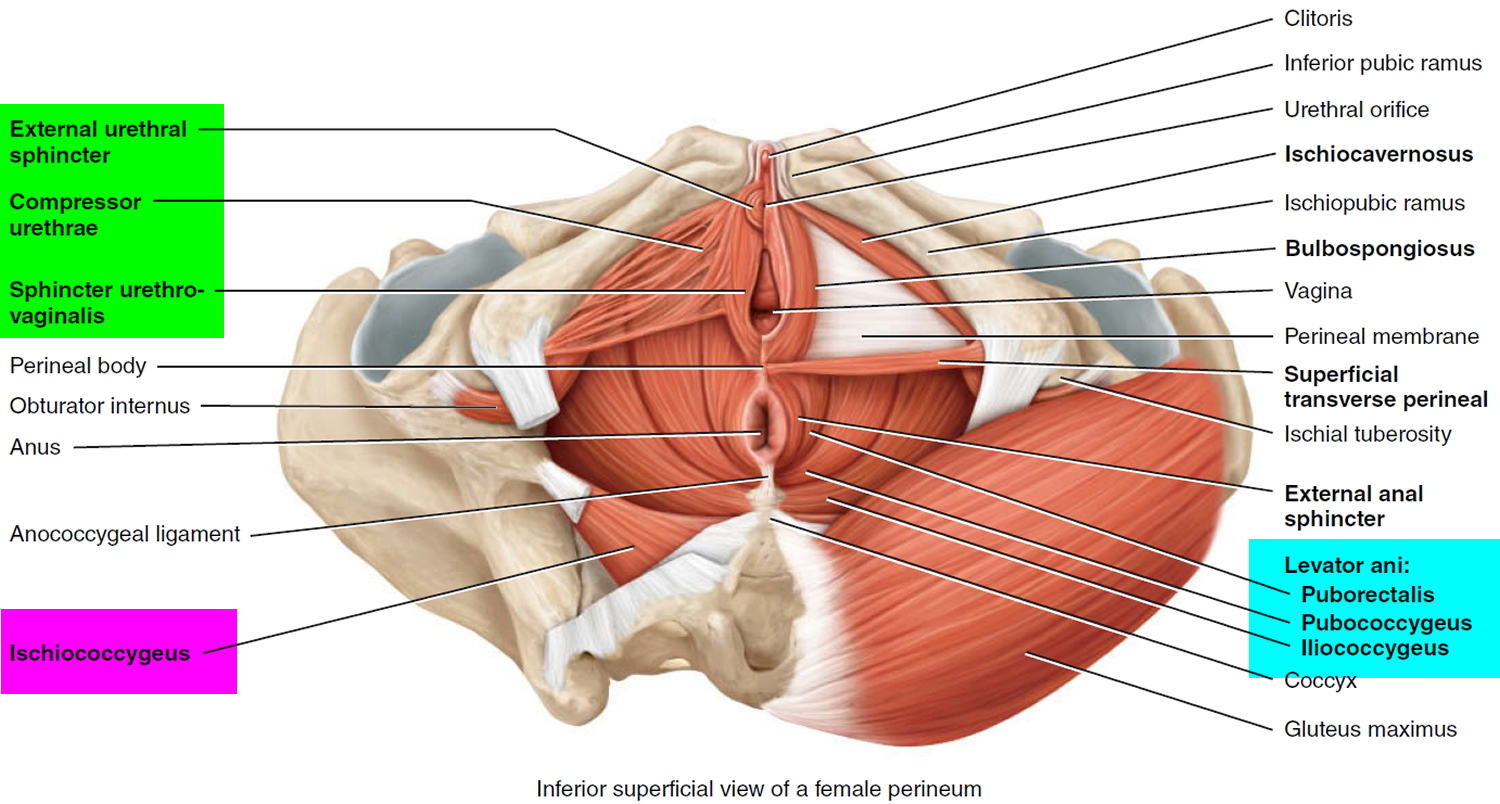
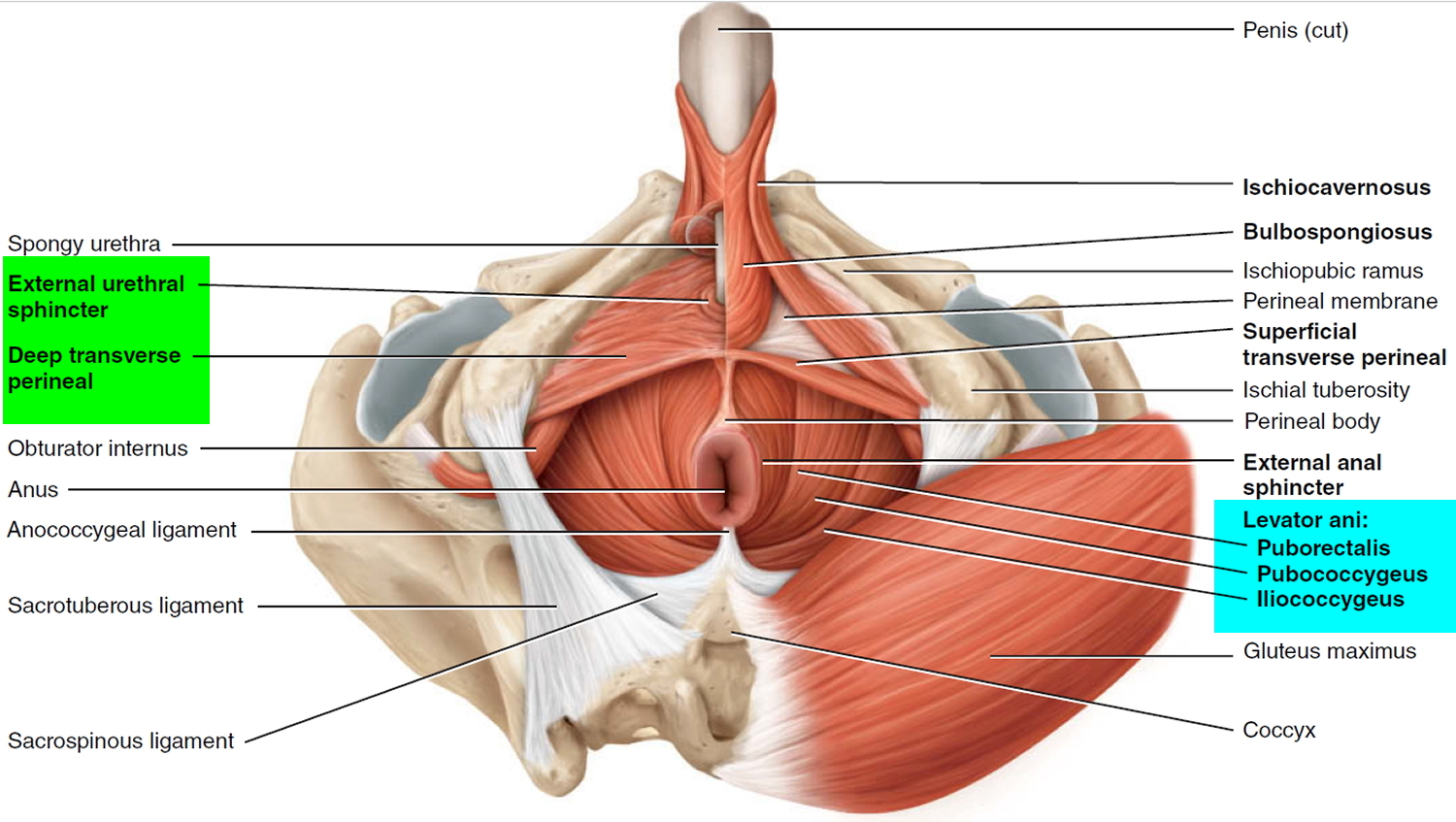
The muscles of the pelvic floor are the levator ani and ischiococcygeus. Along with the fascia covering their internal and external surfaces, these muscles are referred to as the pelvic diaphragm, which stretches from the pubis anteriorly to the coccyx posteriorly, and from one lateral wall of the pelvis to the other. This arrangement gives the pelvic diaphragm the appearance of a funnel suspended from its attachments. The pelvic diaphragm separates the pelvic cavity above from the perineum below. The anal canal and urethra pierce the pelvic diaphragm in both sexes, and the vagina also goes through it in females. The three components of the levator ani muscle are the pubococcygeus, puborectalis, and iliococcygeus. Figure 4 shows these muscles in the female and Figure 5 illustrates them in the male. The levator ani is the largest and most important muscle of the pelvic floor. It supports the pelvic viscera and resists the inferior thrust that accompanies increases in intraabdominal pressure during functions such as forced exhalation, coughing, vomiting, urination, and defecation. The muscle also functions as a sphincter at the anorectal junction, urethra, and vagina. In addition to assisting the levator ani, the ischiococcygeus pulls the coccyx anteriorly after it has been pushed posteriorly during defecation or childbirth.
Figure 4. Pelvic floor female
Why does the pelvic floor become weak in men?
The pelvic floor is a complex layer of muscles and ligaments which stretches like a hammock from the pubic bone at the front of your pelvis to the coccyx at the bottom your spine (see below). A man’s pelvic floor supports his bladder and bowel. The urethra (waterpipe) and the rectum (back passage) pass through the pelvic floor muscles.
The pelvic floor has several functions:
- it supports your pelvic and abdominal organs, especially when you are standing or straining;
- it helps your urethra stay closed when you cough, sneeze or strain; and
- it controls leakage of wind or motions from your lower bowel.
The pelvic floor muscles can be weakened by:
- operations on your prostate gland;
- operations on other organs within the pelvis (e.g. the bowel);
- damage to the nerves of your pelvic floor muscles (by disease, injury, surgery or radiotherapy);
- repeated straining to empty your bowels, usually due to constipation;
- a chronic cough such as a smoker’s cough, chronic bronchitis or asthma;
- being overweight;
- lack of general fitness; and
- ageing.
Figure 5. Pelvic floor male
The pelvic floor has several functions:
- it supports your pelvic and abdominal organs, especially when you are standing or straining
- it helps the water pipe stay closed when you cough, sneeze or strain
- it is used to control leakage of wind or motions from your lower bowel
- it helps to heighten sexual awareness by tightening during intercourse
The pelvic floor can be weakened by childbirth, prolonged straining to empty your bowels, lack of exercise and the menopause. It may also simply become weak as a result of ageing. A weak pelvic floor gives you less control so that you may leak when you exercise, lift, cough or sneeze.
Types of urinary incontinence
There are several types of urinary incontinence, including:
- Stress incontinence – when urine leaks out at times when your bladder is under pressure; for example, when you cough or laugh
- Urge incontinence – when urine leaks as you feel a sudden, intense urge to pass urine, or soon afterwards
- Overflow incontinence (chronic urinary retention) – when you’re unable to fully empty your bladder, which causes frequent leaking
- Total incontinence – when your bladder can’t store any urine at all, which causes you to pass urine constantly or have frequent leaking
It’s also possible to have a mixture of both stress and urge urinary incontinence.
Most people with urinary incontinence have either stress incontinence or urge incontinence.
Stress incontinence
Stress incontinence is when you leak urine when your bladder is put under extra sudden pressure – for example, when you cough. It’s not related to feeling stressed.
Other activities that may cause urine to leak include:
- sneezing
- laughing
- heavy lifting
- exercise
The amount of urine passed is usually small, but stress incontinence can sometimes cause you to pass larger amounts, particularly if your bladder is very full.
Urge incontinence
Urge incontinence or urgency incontinence, is when you feel a sudden and very intense need to pass urine and you’re unable to delay going to the toilet. There’s often only a few seconds between the need to urinate and the release of urine.
Your need to pass urine may be triggered by a sudden change of position, or even by the sound of running water. You may also pass urine during sex, particularly when you reach orgasm.
This type of incontinence often occurs as part of group of symptoms called overactive bladder syndrome, which is where the bladder muscle is more active than usual.
As well as sometimes causing urge incontinence, overactive bladder syndrome can also mean you need to pass urine very frequently and you may need to get up several times during the night to urinate.
Mixed incontinence
Mixed incontinence is when you have symptoms of both stress and urge incontinence. For example, you may leak urine if you cough or sneeze, and also experience very intense urges to pass urine.
Overflow incontinence
Overflow incontinence, also called chronic urinary retention, occurs when the bladder cannot completely empty when you pass urine. This causes the bladder to swell above its usual size.
If you have overflow incontinence, you may pass small trickles of urine very often. It may also feel as though your bladder is never fully empty and you cannot empty it even when you try.
Total incontinence
Urinary incontinence that’s severe and continuous is sometimes known as total incontinence.
Total incontinence may cause you to constantly pass large amounts of urine, even at night. Alternatively, you may pass large amounts of urine only occasionally and leak small amounts in between.
Lower urinary tract symptoms
The lower urinary tract comprises the bladder and the tube urine passes through out of the body (urethra).
Lower urinary tract symptoms (LUTS) are common in men and women as they get older.
They can include:
- problems with storing urine, such as an urgent or frequent need to go to the toilet, or feeling like you need to go straight after you’ve just been
- problems with passing urine, such as a slow stream of urine, straining to pass urine, or stopping and starting as you pass urine
- problems after you’ve passed urine, such as feeling that you’ve not completely emptied your bladder or passing a few drops of urine after you think you’ve finished
Experiencing LUTS can make urinary incontinence more likely.
Urinary incontinence causes
Urinary incontinence occurs when the normal process of storing and passing urine is disrupted. This can happen for a number of reasons.
Certain factors may also increase your chance of developing urinary incontinence.
Some of the possible causes lead to short-term urinary incontinence, while others may cause a long-term problem. If the cause can be treated, this may cure your incontinence.
Temporary urinary incontinence
Certain drinks, foods and medications may act as diuretics — stimulating your bladder and increasing your volume of urine. They include:
- Alcohol
- Caffeine
- Carbonated drinks and sparkling water
- Artificial sweeteners
- Chocolate
- Chili peppers
- Foods that are high in spice, sugar or acid, especially citrus fruits
- Heart and blood pressure medications, sedatives, and muscle relaxants
- Large doses of vitamin C
Urinary incontinence may also be caused by an easily treatable medical condition, such as:
- Urinary tract infection. Infections can irritate your bladder, causing you to have strong urges to urinate, and sometimes incontinence.
- Constipation. The rectum is located near the bladder and shares many of the same nerves. Hard, compacted stool in your rectum causes these nerves to be overactive and increase urinary frequency.
Persistent urinary incontinence
Urinary incontinence can also be a persistent condition caused by underlying physical problems or changes, including:
- Pregnancy. Hormonal changes and the increased weight of the fetus can lead to stress incontinence.
- Childbirth. Vaginal delivery can weaken muscles needed for bladder control and also damage bladder nerves and supportive tissue, leading to a dropped (prolapsed) pelvic floor. With prolapse, the bladder, uterus, rectum or small intestine can get pushed down from the usual position and protrude into the vagina. Such protrusions can be associated with incontinence.
- Changes with age. Aging of the bladder muscle can decrease the bladder’s capacity to store urine. Also, involuntary bladder contractions become more frequent as you get older.
- Menopause. After menopause women produce less estrogen, a hormone that helps keep the lining of the bladder and urethra healthy. Deterioration of these tissues can aggravate incontinence.
- Hysterectomy. In women, the bladder and uterus are supported by many of the same muscles and ligaments. Any surgery that involves a woman’s reproductive system, including removal of the uterus, may damage the supporting pelvic floor muscles, which can lead to incontinence.
- Enlarged prostate. Especially in older men, incontinence often stems from enlargement of the prostate gland, a condition known as benign prostatic hyperplasia.
- Prostate cancer. In men, stress incontinence or urge incontinence can be associated with untreated prostate cancer. But more often, incontinence is a side effect of treatments for prostate cancer.
- Obstruction. A tumor anywhere along your urinary tract can block the normal flow of urine, leading to overflow incontinence. Urinary stones — hard, stone-like masses that form in the bladder — sometimes cause urine leakage.
- Neurological disorders. Multiple sclerosis, Parkinson’s disease, a stroke, a brain tumor or a spinal injury can interfere with nerve signals involved in bladder control, causing urinary incontinence.
Causes of stress incontinence
Stress incontinence occurs when the pressure inside your bladder as it fills with urine becomes greater than the strength of your urethra to stay closed. The urethra is the tube urine passes through out of your body.
Any sudden extra pressure on your bladder, such as laughing or sneezing, can then cause urine to leak out of your urethra.
Your urethra may not be able to stay closed if the muscles in your pelvis (pelvic floor muscles) are weak or damaged, or your urethral sphincter – the ring of muscle that keeps the urethra closed – is damaged.
These problems may be caused by:
- damage during childbirth – particularly if the child was born vaginally, rather than by caesarean section
- increased pressure on your tummy – for example, because you are pregnant or obese
- damage to the bladder or nearby area during surgery – such as the removal of the womb (hysterectomy) in women, or removal of the prostate gland in men
- neurological conditions – that affect the brain and spinal cord, such as Parkinson’s disease or multiple sclerosis
- certain connective tissue disorders – such as Ehlers-Danlos syndrome
- certain medications
Causes of urge incontinence
The urgent and frequent need to pass urine can be caused by a problem with the detrusor muscles in the walls of the bladder.
The detrusor muscles relax to allow the bladder to fill with urine, then contract when you go to the toilet to let the urine out.
Sometimes the detrusor muscles contract too often, creating an urgent need to go to the toilet. This is known as having an overactive bladder.
The reason your detrusor muscles contract too often may not be clear, but possible causes include:
- drinking too much alcohol or caffeine
- poor fluid intake – this can cause strong, concentrated urine to collect in your bladder, which can irritate the bladder and cause symptoms of overactivity
- constipation
- conditions affecting the lower urinary tract (urethra and bladder) – such as urinary tract infections (UTIs) or tumours in the bladder
- neurological conditions
- certain medications
Causes of overflow incontinence
Overflow incontinence, also called chronic urinary retention, is often caused by a blockage or obstruction of your bladder.
Your bladder may fill up as usual, but as it’s obstructed you won’t be able to empty it completely, even when you try.
At the same time, pressure from the urine that’s still in your bladder builds up behind the obstruction, causing frequent leaks.
Your bladder can become obstructed as a result of:
- an enlarged prostate gland (in men)
- bladder stones
- constipation
Overflow incontinence may also be caused by your detrusor muscles not fully contracting, which means your bladder doesn’t completely empty when you go to the toilet. As a result, the bladder becomes stretched.
Your detrusor muscles may not fully contract if:
- there’s damage to your nerves – for example, as a result of surgery to part of your bowel or a spinal cord injury
- you’re taking certain medications
Causes of total incontinence
Total incontinence occurs when your bladder can’t store any urine at all. It can result in you either passing large amounts of urine constantly, or passing urine occasionally with frequent leaking.
Total incontinence can be caused by:
- a problem with your bladder from birth
- injury to your spinal cord – this can disrupt the nerve signals between your brain and your bladder
- a bladder fistula – a small, tunnel-like hole that can form between the bladder and a nearby area, such as the vagina, in women
Medications that may cause incontinence
Some medicines can disrupt the normal process of storing and passing urine, or increase the amount of urine you produce.
These include:
- angiotensin-converting enzyme (ACE) inhibitors
- diuretics
- some antidepressants
- hormone replacement therapy (HRT)
- sedatives
Stopping these medications, if advised to do so by a doctor, may help resolve your incontinence.
Risk factors for urinary incontinence
In addition to the causes mentioned above, some things can increase your risk of developing urinary incontinence without directly being the cause of the problem. These are known as risk factors.
Some of the main risk factors for urinary incontinence include:
- Family history – there may be a genetic link to urinary incontinence, , especially urge incontinence, so you may be more at risk if other people in your family have experienced the problem
- Increasing age – urinary incontinence becomes more common as you reach middle age, and is particularly common in people over the age of 80. As you get older, the muscles in your bladder and urethra lose some of their strength. Changes with age reduce how much your bladder can hold and increase the chances of involuntary urine release.
- Having lower urinary tract symptoms (LUTS) – a range of symptoms that affect the bladder and urethra.
- Gender. Women are more likely to have stress incontinence. Pregnancy, childbirth, menopause and normal female anatomy account for this difference. However, men with prostate gland problems are at increased risk of urge and overflow incontinence.
- Being overweight. Extra weight increases pressure on your bladder and surrounding muscles, which weakens them and allows urine to leak out when you cough or sneeze.
- Smoking. Tobacco use may increase your risk of urinary incontinence.
- Other diseases. Neurological disease or diabetes may increase your risk of incontinence.
Complications of chronic urinary incontinence
Complications of chronic urinary incontinence include:
- Skin problems. Rashes, skin infections and sores can develop from constantly wet skin.
- Urinary tract infections. Incontinence increases your risk of repeated urinary tract infections.
- Impacts on your personal life. Urinary incontinence can affect your social, work and personal relationships.
Preventing urinary incontinence
It’s not always possible to prevent urinary incontinence, but there are some steps you can take that may help reduce the chance of it developing.
These include:
- controlling your weight
- avoiding or cutting down on alcohol
- keeping fit – in particular, ensuring that your pelvic floor muscles are strong
- eat more fiber, which can prevent constipation, a cause of urinary incontinence
- don’t smoke, or seek help to quit smoking
Healthy weight
Being obese can increase your risk of developing urinary incontinence. You may therefore be able to lower your risk by maintaining a healthy weight through regular exercise and healthy eating.
Use the healthy weight calculator to see if you are a healthy weight for your height.
- Body Weight Planner. https://www.supertracker.usda.gov/bwp/index.html
To find out about how many calories you should eat to lose weight according to your weight, age, sex, height and physical activity, you can use a FREE online app Body Weight Planner 1
- ChooseMyPlate. https://www.choosemyplate.gov/
To find out about the 5 Food Groups you should have on your plate for a meal, you can use a FREE online app ChooseMyPlate 2
- SuperTracker website: https://supertracker.usda.gov
To find out What and How Much To Eat, you can use a FREE, award-winning, state-of-the-art, online diet and activity tracking tool called SuperTracker 3 from the United States Department of Agriculture Center for Nutrition Policy and Promotion 3. This free application empowers you to build a healthier diet, manage weight, and reduce your risk of chronic diet-related diseases. You can use SuperTracker 3 to determine what and how much to eat; track foods, physical activities, and weight; and personalize with goal setting, virtual coaching, and journaling.
- BMI Calculator Adults. https://www.cdc.gov/healthyweight/assessing/bmi/adult_BMI/english_bmi_calculator/bmi_calculator.html
- BMI Calculator Children. https://www.cdc.gov/healthyweight/bmi/calculator.html
To find out about your body mass index (BMI), you can use a FREE online BMI calculators from the Centers for Disease Control and Prevention (CDC) – for Adults 4 and for Children 5
Drinking habits
Depending on your particular bladder problem, your doctor can advise you about the amount of fluids you should drink.
If you have urinary incontinence, cut down on alcohol and drinks containing caffeine, such as tea, coffee and cola. These can cause your kidneys to produce more urine and irritate your bladder.
The recommended weekly limits for alcohol consumption are 14 units for men and women.
A unit of alcohol is roughly half a pint of normal-strength lager or a single measure (25ml) of spirits.
If you have to urinate frequently during the night (nocturia), try drinking less in the hours before you go to bed. However, make sure you still drink enough fluids during the day.
Pelvic floor exercises
Being pregnant and giving birth can weaken the muscles that control the flow of urine from your bladder. If you’re pregnant, strengthening your pelvic floor muscles may help prevent urinary incontinence.
Men may also benefit from strengthening their pelvic floor muscles with pelvic floor exercises.
Urinary incontinence diagnosis
If you experience urinary incontinence, see your doctor so they can determine the type of condition you have.
Try not to be embarrassed about speaking to your doctor about your incontinence. Urinary incontinence is a common problem and it’s likely your doctor has seen many people with the condition.
Your doctor will ask you questions about your symptoms and medical history, including:
- whether the urinary incontinence occurs when you cough or laugh
- whether you need the toilet frequently during the day or night
- whether you have any difficulty passing urine when you go to the toilet
- whether you’re currently taking any medication
- how much fluid, alcohol or caffeine you drink
Bladder diary
Your doctor may suggest that you keep a diary of your bladder habits for at least three days so you can give them as much information as possible about your condition.
This should include details like:
- how much fluid you drink
- the types of fluid you drink
- how often you need to pass urine
- the amount of urine you pass
- how many episodes of incontinence you experience
- how many times you experience an urgent need to go to the toilet
Tests and examinations
You may also need to have some tests and examinations so your doctor can confirm or rule out things that may be causing your incontinence. Some of these are explained below.
Physical examination
Your doctor may examine you to assess the health of your urinary system. If you’re female, your doctor will carry out a pelvic examination, which usually involves undressing from the waist down. You may be asked to cough to see if any urine leaks out.
Your doctor may also examine your vagina. In over half of women with stress incontinence, part of the bladder may bulge into the vagina.
Your doctor may place their finger inside your vagina and ask you to squeeze it with your pelvic floor muscles.
These are the muscles that surround your bladder and urethra, the tube urine passes through out of the body. Damage to your pelvic floor muscles can lead to urinary incontinence.
If you’re male, your doctor may check whether your prostate gland is enlarged. The prostate gland is located between the penis and bladder, and surrounds the urethra.
If it’s enlarged, it can cause symptoms of urinary incontinence, such as a frequent need to urinate.
You may also need a digital rectal examination to check the health of your prostate gland. This will involve your doctor inserting their finger into your bottom.
Urine Dipstick test
If your doctor thinks your symptoms may be caused by a urinary tract infection, a sample of your urine may be tested for bacteria.
A small chemically treated stick is dipped into your urine sample. It will change colour if bacteria are present. The dipstick test can also check the blood and protein levels in your urine.
Residual urine test
If your doctor thinks you may have overflow incontinence, they may suggest a test called a residual urine test to see how much urine is left in your bladder after you go for a wee.
This is usually done by carrying out an ultrasound scan of your bladder, although occasionally the amount of urine in your bladder may be measured after it’s been drained using a catheter.
A catheter is a thin, flexible tube that’s inserted into your urethra and passed through to your bladder.
Further tests
Some further tests may be necessary if the cause of your urinary incontinence isn’t clear. Your doctor will usually start treating you first and may suggest these tests if treatment isn’t effective.
Cystoscopy
A cystoscopy involves using an instrument called an endoscope to look inside your bladder and urinary system. This test can identify abnormalities that may be causing incontinence.
Urodynamic tests
These are a group of tests used to check the function of your bladder and urethra. This may include keeping a bladder diary for a few days and then attending an appointment at a hospital or clinic for tests.
Tests can include:
- measuring the pressure in your bladder by inserting a catheter into your urethra
- measuring the pressure in your tummy (abdomen) by inserting a catheter into your bottom
- asking you to urinate into a special machine that measures the amount and flow of urine.
Urinary incontinence treatment
The treatment you receive for urinary incontinence will depend on the type of incontinence you have and the severity of your symptoms.
If your incontinence is caused by an underlying condition, you may receive treatment for this alongside your incontinence treatment.
Conservative treatments, which don’t involve medication or surgery, are tried first. These include:
- lifestyle changes
- pelvic floor muscle training (Kegel exercises)
- bladder training
After this, medication or surgery may be considered.
This page is about non-surgical treatments for urinary incontinence. Find out about surgery and procedures for urinary incontinence.
Lifestyle changes
Your doctor may suggest you make simple changes to your lifestyle to improve your symptoms. These changes can help improve your condition, regardless of the type of urinary incontinence you have.
For example, your doctor may recommend:
- reducing your caffeine intake – caffeine is found in tea, coffee and cola, and can increase the amount of urine your body produces
- altering how much fluid you drink a day – drinking too much or too little can make incontinence worse
- losing weight if you are overweight or obese – use the healthy weight calculator to find out if you’re a healthy weight for your height
Pelvic floor muscle training
Your pelvic floor muscles are the muscles you use to control the flow of urine as you urinate. They surround the bladder and urethra, the tube that carries urine from the bladder outside the body.
Weak or damaged pelvic floor muscles can cause urinary incontinence, so exercising these muscles is often recommended.
Your doctor may refer you to a specialist to start a programme of pelvic floor muscle training.
Your specialist will assess whether you’re able to squeeze (contract) your pelvic floor muscles and by how much.
If you can contract your pelvic floor muscles, you’ll be given an individual exercise programme based on your assessment.
Your programme should include doing a minimum of eight muscle contractions at least three times a day and the recommended exercises for at least three months. If the exercises are helping after this time, you can keep on doing them.
How can exercising the pelvic floor muscles help?
Exercising the pelvic floor muscles can strengthen them so that they provide the support you need. This will improve your bladder control and improve, or even stop, leakage of urine. Like all other muscles in the body, the more you use and exercise them, the stronger they become and stay.
Research suggests women who complete pelvic floor muscle training experience fewer leaking episodes and report a better quality of life.
In men, some studies have shown pelvic floor muscle training can reduce urinary incontinence, particularly after surgery to remove the prostate gland.
Pelvic floor exercises for women
It is not easy to identify your pelvic floor muscles. Exercising them should not be visible from the outside.
Let your doctor, nurse, or therapist help you. Many people have trouble finding the right muscles. Your doctor, nurse, or therapist can check to make sure you are doing the exercises correctly. You can also exercise by using special weights or biofeedback. Ask your health care team about these exercise aids.
Don’t squeeze other muscles at the same time. Be careful not to tighten your stomach, legs, or other muscles. Squeezing the wrong muscles can put more pressure on your bladder control muscles. Just squeeze the pelvic muscle. Don’t hold your breath.
Here is what to do 6:
Step 1
Sit comfortably with your knees slightly apart. Imagine that you are trying to stop yourself passing wind from your bowel. To do this, you must squeeze the muscle around the back passage. Try lifting and squeezing the muscle as if you have wind. If you sense a “pulling” feeling, you are squeezing the right muscles for pelvic exercises. You should be able to feel the muscle move and your buttocks or legs should not move at all. You should notice that the skin around your back passage tightens up and creates the sensation of lifting you from your chair.
Step 2
Imagine that you are sitting on the toilet to pass urine and try to stop yourself from producing a stream of urine. You should be using the same group of muscles that you used before but you will find this a little more difficult. Do not try to stop the urinary stream when you are actually passing water because it can cause problems with bladder emptying.
Or you can lie down and put your finger inside your vagina. Squeeze as if you were trying to stop urine from coming out. If you feel tightness on your finger, you are squeezing the right pelvic muscles.
Step 3
Try to tighten the muscles around your back passage and vagina, by lifting up inside as if you are trying to stop passing wind and urine at the same time. Do not tense your abdomen, squeeze your legs together, tighten your buttocks or hold your breath. If you can master this, most of the muscle contraction should be coming from the pelvic floor.
How do you practice the exercises?
You need to develop two types of muscle activity, slow and fast.
- to practice slow contractions
- do the exercises above and try to hold the pelvic floor tight for up to ten seconds. Rest for four seconds and then repeat the contraction as many times as you can, up to a maximum of ten
- to practice quick contractions
- draw the pelvic floor rapidly upwards and hold this for one second. Repeat up to a maximum of ten times. This will protect you against sudden leakage during coughing, laughing or exercise
- Aim to do one set of slow contractions followed by one set of fast contractions up to six times a day. Do not over-do it or the muscles will get tired. The exercises can be performed standing, sitting or lying down but you may find it easier at first to do them sitting down.
Other things that help
- Get into the habit of doing your exercises regularly and linking them to everyday activities e.g. do them after emptying your bladder, while answering the telephone, standing in a queue or whenever you turn on a tap. Do your pelvic exercises at least three times a day. Every day, use three positions: lying down, sitting, and standing. You can exercise while lying on the floor, sitting at a desk, or standing in the kitchen. Using all three positions makes the muscles strongest.
- At first, find a quiet spot to practice—your bathroom or bedroom—so you can concentrate. Lie on the floor. Pull in the pelvic muscles and hold for a count of 3. Then relax for a count of 3. Work up to 10 to 15 repeats each time you exercise.
- If you are not sure you are doing the exercises correctly, insert a thumb or two fingers into the vagina and try the exercises; you should feel a gentle squeeze as the muscles contract
- Use the pelvic floor exercises to prevent leakage before you do anything which might make you leak; this way, your control will gradually improve
- Drink normally – six to eight cups (two litres) per day – avoiding caffeine and alcohol if you can
- Avoid going to the toilet “just in case”; go only when you feel that your bladder is full
- Watch your weight; extra weight puts more strain on your pelvic floor muscles and your bladder
- Avoid constipation. Straining can put excessive pressure on your bladder and bowels
- Pelvic floor exercises take three to six months to produce maximum benefit, but you should continue them for life to prevent problems recurring or worsening; you should seek help from a health professional there is little or no change in your symptoms after exercising for three months
- Other methods which help some women include weighted vaginal cones, biofeedback and electrical stimulation; consult your doctor, urologist or specialist nurse for more details
Be patient. Don’t give up. It’s just 5 minutes, three times a day. You may not feel your bladder control improve until after 3 to 6 weeks. Still, most women do notice an improvement after a few weeks.
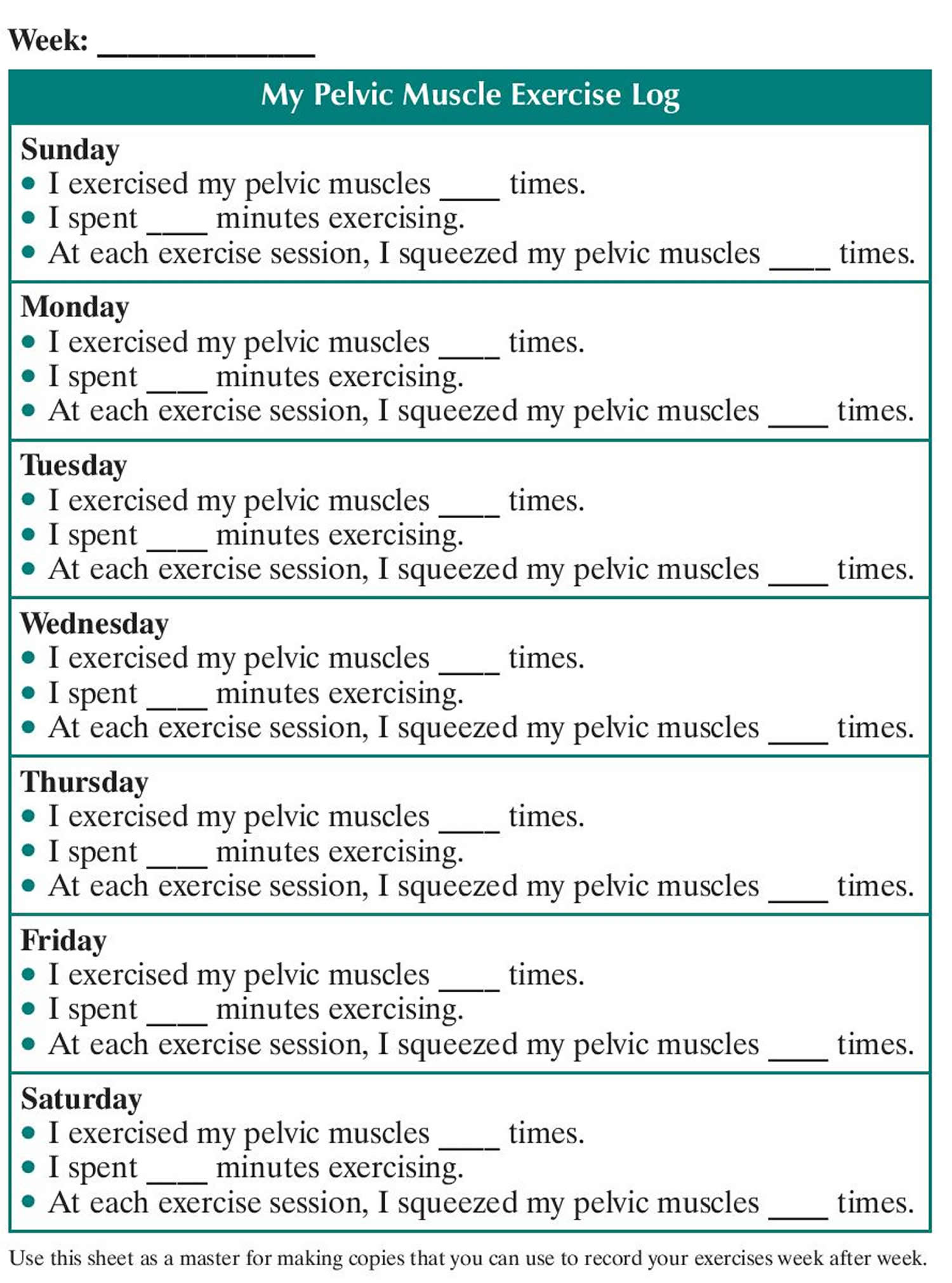
Use the Exercise Log below to keep track of your sessions.
Week: ______________
My Pelvic Muscle Exercise Log
Sunday
- I exercised my pelvic muscles ____ times.
- I spent ____ minutes exercising.
- At each exercise session, I squeezed my pelvic muscles ____ times.
Monday
- I exercised my pelvic muscles ____ times.
- I spent ____ minutes exercising.
- At each exercise session, I squeezed my pelvic muscles ____ times.
Tuesday
- I exercised my pelvic muscles ____ times.
- I spent ____ minutes exercising.
- At each exercise session, I squeezed my pelvic muscles ____ times.
Wednesday
- I exercised my pelvic muscles ____ times.
- I spent ____ minutes exercising.
- At each exercise session, I squeezed my pelvic muscles ____ times.
Thursday
- I exercised my pelvic muscles ____ times.
- I spent ____ minutes exercising.
- At each exercise session, I squeezed my pelvic muscles ____ times.
Friday
- I exercised my pelvic muscles ____ times.
- I spent ____ minutes exercising.
- At each exercise session, I squeezed my pelvic muscles ____ times.
Saturday
- I exercised my pelvic muscles ____ times.
- I spent ____ minutes exercising.
- At each exercise session, I squeezed my pelvic muscles ____ times.
Figure 6. Pelvic floor muscle exercise log – use this sheet as a master for making copies that you can use to record your exercises week after week.
Pelvic floor exercises for men
Pelvic floor exercises are an important part of preparation before surgery for removal of your prostate for cancer (radical prostatectomy) 7. They ensure that the pelvic floor muscles are in good condition and can help reduce urine leakage after the operation.
How do I contract the pelvic floor muscles?
The first thing you need to do is to identify the muscles to exercise. You can do this by sitting or lying comfortably with the muscles of your thighs, buttock and abdomen relaxed.
Step 1
Tighten the ring of muscle around the back passage as if you are trying to control diarrhea or wind. Relax the muscle again. Practice this movement several times until you are sure you are exercising the correct muscles. Try not to squeeze your buttocks, thighs or abdominal (tummy) muscles
Step 2
Imagine you are trying to pass urine, stop the flow in mid-stream and then re-start it. If your technique is correct, you will feel the base of your penis move upwards slightly towards your tummy. You can check this “for real” while passing urine, but no more than once a week, in case it interferes with normal bladder emptying
How do I do pelvic floor exercises?
Learning how to do these exercises can take a little time but, with practice, you should be able to learn the technique:
- tighten and draw in the muscles around the anus (back passage) and the urethra (water pipe) all at once. Lift them up inside you and hold this position as you count to five. Release the muscles slowly and relax for a few seconds
- repeat the contraction and relax again. Once you find it easy to hold the contraction for a count of five, try to hold it for longer (up to ten seconds)
- repeat this for a maximum of eight to ten squeezes. Try to make each contraction strong, slow and controlled
- do the same thing again but, this time, using ten short, fast contractions, pulling up rapidly and immediately letting go
- repeat this whole exercise routine at least four to five times every day. You can do it in a variety of positions – lying, sitting, standing and walking
- try to avoid holding your breath, pushing down (instead of squeezing) and tightening your abdominal muscles, buttocks or thighs
- the exercises can be performed standing, sitting or lying down but you may find it easier at first to do them sitting down
Other things that help
Once you have learnt how to do these exercises, they should be done regularly, giving each set your full attention. Find at least five regular times during the day to do them e.g. after going to the toilet, when having a drink, when lying in bed. Tightening the pelvic floor before you cough, lift anything heavy or get up from a chair will also help.
You will probably not notice an improvement for several weeks. It may take a few months before you get maximum benefit. Once you have recovered control over your bowel and bladder, continue doing the exercises twice a day for life, to keep the pelvic floor muscles strong.
Other things to do include:
- Share the lifting of heavy loads;
- Avoid constipation and straining when opening your bowels;
- Seek medical advice for hay fever, asthma or bronchitis to reduce sneezing and coughing;
- Keep your weight within the correct range for your height and age; and
- Other methods which have been shown to help some men include biofeedback and electrical stimulation.
If you would like to explore other methods or you are not sure whether you are performing the exercises correctly, ask your urologist or specialist nurse. They will be able to give you more advice or put you in touch with a continence advisor or physiotherapist.
Electrical stimulation
If you’re unable to contract your pelvic floor muscles, using a device that measures and stimulates the electrical signals in the muscles may be recommended. This is called electrical stimulation.
A small probe will be inserted into the vagina in women or the anus in men. An electrical current runs through the probe, which helps strengthen your pelvic floor muscles while you exercise them.
You may find electrical stimulation difficult or unpleasant to use, but it may be beneficial if you’re unable to complete pelvic floor muscle contractions without it.
Biofeedback
Biofeedback is a way to monitor how well you’re doing the pelvic floor exercises by giving you feedback as you do them.
There are several different methods of biofeedback:
- a small probe could be inserted into the vagina in women or the anus in men – this senses when the muscles are squeezed and sends the information to a computer screen
- electrodes could be attached to the skin of your tummy (abdomen) or around the anus – these sense when the muscles are squeezed and send the information to a computer screen
There isn’t much good evidence to suggest biofeedback offers a significant benefit to people using pelvic floor muscle training for urinary incontinence, but the feedback may help motivate some people to carry out their exercises.
Speak to your specialist if you would like to try biofeedback.
Vaginal cones
Vaginal cones may be used by women to assist with pelvic floor muscle training. These small weights are inserted into the vagina.
You hold the weights in place using your pelvic floor muscles. When you can, you progress to the next vaginal cone, which weighs more.
Some women find vaginal cones uncomfortable or unpleasant to use, but they may help with stress or mixed urinary incontinence.
Bladder training
If you’ve been diagnosed with urge incontinence, one of the first treatments you may be offered is bladder training.
Bladder training may also be combined with pelvic floor muscle training if you have mixed urinary incontinence.
It involves learning techniques to increase the length of time between feeling the need to urinate and passing urine. The course will usually last for at least six weeks.
Incontinence products
While incontinence products aren’t a treatment for urinary incontinence, you might find them useful for managing your condition while you’re waiting to be assessed or for treatment to take effect.
Incontinence products include:
- absorbent products, such as incontinence pants or pads
- handheld urinals
- a catheter, a thin tube that is inserted into your bladder to drain urine
- devices that are placed into the vagina or urethra to prevent urine leakage – for example, while you exercise
Urinary incontinence medication
Alpha blockers. In men with urge or overflow incontinence, these medications relax bladder neck muscles and muscle fibers in the prostate and make it easier to empty the bladder. Examples include tamsulosin (Flomax), alfuzosin (Uroxatral), silodosin (Rapaflo), doxazosin (Cardura) and terazosin.
Topical estrogen. For women, applying low-dose, topical estrogen in the form of a vaginal cream, ring or patch may help tone and rejuvenate tissues in the urethra and vaginal areas. Systemic estrogen — taking the hormone as a pill — isn’t recommended for urinary incontinence and may even make it worse.
Medication for stress incontinence
If stress incontinence doesn’t significantly improve, surgery for urinary incontinence will often be recommended as the next step.
However, if you’re unsuitable for surgery or want to avoid having an operation, you may benefit from a medication called duloxetine. This can help increase the muscle tone of the urethra, which should help keep it closed.
You’ll need to take duloxetine by mouth twice a day, and will be assessed after two to four weeks to see if the medicine is beneficial or causing any side effects.
Possible side effects of duloxetine can include:
- nausea
- dry mouth
- extreme tiredness (fatigue)
- constipation
Don’t suddenly stop taking duloxetine, as this can also cause unpleasant side effects. Your doctor will reduce your dose gradually.
Duloxetine isn’t suitable for everyone, however, so your doctor will discuss any other medical conditions you have to determine if you can take it.
Medication for urge incontinence
Antimuscarinics
If bladder training isn’t an effective treatment for your urge incontinence, your doctor may prescribe a type of medication called an antimuscarinic.
Antimuscarinics may also be prescribed if you have overactive bladder syndrome, which is the frequent urge to urinate that can occur with or without urinary incontinence.
A number of different antimuscarinic medications can be used to treat urge incontinence, but common ones include oxybutynin, tolterodine and darifenacin.
These are usually taken by mouth two or three times a day, although an oxybutynin patch that you place on your skin twice a week is also available.
Your doctor will usually start you at a low dose to minimise any possible side effects. The dose can then be increased until the medicine is effective.
Possible side effects of antimuscarinics include:
- dry mouth
- constipation
- blurred vision
- fatigue
In rare cases, antimuscarinic medication can also lead to a type of glaucoma, a build-up of pressure within the eye, called angle-closure glaucoma.
You’ll be assessed after four weeks to see how you’re getting on with the medication, and every 6 to 12 months thereafter if the medication continues to help.
Your doctor will discuss any other medical conditions you have to determine which antimuscarinics are suitable for you.
Mirabegron
If antimuscarinics are unsuitable for you, they haven’t helped your urge incontinence or have caused unpleasant side effects, you may be offered an alternative medication called mirabegron.
Mirabegron causes the bladder muscle to relax, which helps the bladder fill up with and store urine. It is usually taken by mouth once a day.
Side effects of mirabegron can include:
- urinary tract infections (UTIs)
- a fast or irregular heartbeat
- suddenly noticeable heartbeats (palpitations)
- a rash
- itching
Your doctor will discuss any other medical conditions you have to determine whether mirabegron is suitable for you.
Medication for nocturia
A low-dose version of a medication called desmopressin may be used to treat nocturia, which is the frequent need to get up during the night to urinate, by helping to reduce the amount of urine produced by the kidneys.
Another type of medication taken late in the afternoon, called a loop diuretic, may also prevent you getting up in the night to pass urine.
Diuretic medicine increases the production and flow of urine from your body. By removing excess fluid from your body in the afternoon, it may improve symptoms at night.
Loop diuretics are not licensed to treat nocturia. This means that the medication may not have undergone clinical trials, a type of research that tests one treatment against another, to see if it’s effective and safe in the treatment of nocturia.
However, your doctor or specialist may suggest an unlicensed medication if they think it’s likely to be effective and the benefits of treatment outweigh any associated risk.
If your doctor is considering prescribing a loop diuretic, they should tell you it’s unlicensed and discuss the possible risks and benefits with you.
Urinary incontinence surgery
If other treatments for urinary incontinence are unsuccessful or unsuitable, surgery or other procedures may be recommended.
Before making a decision, discuss the risks and benefits with a specialist, as well as any possible alternative treatments.
If you’re a woman and plan to have children, this will affect your decision – the physical strain of pregnancy and childbirth can sometimes cause surgical treatments to fail.
You may wish to wait until you no longer want to have any more children before having surgery.
The various surgical treatments for urinary incontinence are outlined below.
Surgery and procedures for stress incontinence
Tape procedures
Tape procedures can be used for women with stress incontinence. A piece of plastic tape is inserted through a cut (incision) inside the vagina and threaded behind the tube that carries urine out of the body (urethra).
The middle part of the tape supports the urethra, and the two ends are threaded through two incisions in either the:
- tops of the inner thigh – this is called a transobturator tape procedure (TOT)
- tummy (abdomen) – this is called a retropubic tape procedure or tension-free vaginal tape procedure (TVT)
By holding the urethra up in the correct position, the piece of tape can help reduce the leaking of urine associated with stress incontinence.
The effectiveness of these tape procedures is similar, with around two in every three women not experiencing any leaking afterwards.
Even those who still have some leaking after surgery often find this is less severe than it was before the operation.
However, it’s not uncommon for women to need to go to the toilet more frequently and urgently after this procedure, and some find they’re unable to completely empty their bladder when they go to the toilet.
In some cases, the tape can wear away or move over time and further surgery may be needed at a later stage to adjust it – for example, to make it looser – or remove it.
Colposuspension
Colposuspension involves making an incision in your lower abdomen, lifting up the neck of your bladder, and stitching it in this lifted position.
This can help prevent involuntary leaks in women with stress incontinence.
There are two types of colposuspension:
- open colposuspension – where surgery is carried out through a large incision
- laparoscopic (keyhole) colposuspension – where surgery is carried out through one or more small incisions using special small surgical instruments
Both types of colposuspension offer effective long-term treatment for stress incontinence, although laparoscopic colposuspension needs to be carried out by an experienced laparoscopic surgeon.
Problems that can occur after colposuspension include difficulty emptying the bladder fully when going to the toilet, recurrent urinary tract infections (UTIs), and discomfort during sex.
Sling procedures
Sling procedures involve making an incision in your lower abdomen and vagina so a sling can be placed around the neck of the bladder to support it and prevent accidental urine leaks.
The sling can be made of:
- a synthetic material
- tissue taken from another part of your body (autologous sling)
- tissue donated from another person (allograft sling)
- tissue taken from an animal (xenograft sling), such as cow or pig tissue
In many cases, an autologous sling is used and will be made using part of the layer of tissue that covers the abdominal muscles (rectus fascia). These slings are generally preferred because more is known about their long-term safety and effectiveness.
The most commonly reported problem associated with the use of slings is difficulty emptying the bladder fully when going to the toilet.
A small number of women who have the procedure also find they develop urge incontinence afterwards.
Urethral bulking agents
A urethral bulking agent is a substance that can be injected into the walls of the urethra in women with stress incontinence. This increases the size of the urethral walls and allows the urethra to stay closed with more force.
A number of different bulking agents are available, and there’s no evidence one is more beneficial than another.
This is less invasive than other surgical treatments for stress incontinence in women as it doesn’t usually require any incisions.
Instead, the substances are normally injected through a cystoscope inserted directly into the urethra.
However, this procedure is generally less effective than the other options available. The effectiveness of the bulking agents will also reduce with time and you may need repeated injections.
Many women experience a slight burning sensation or bleeding when they pass urine for a short period after the bulking agents are injected.
Artificial urinary sphincter
The urinary sphincter is a ring of muscle that stays closed to prevent urine flowing from the bladder into your urethra.
In some cases, it may be suggested that you have an artificial urinary sphincter fitted to relieve your incontinence.
This tends to be used more often as a treatment for men with stress incontinence and is only rarely used in women.
An artificial sphincter consists of three parts:
- a circular cuff that is placed around the urethra – this can be filled with fluid when necessary to compress the urethra and prevent urine passing through it
- a small pump placed in the scrotum (when used in men) that contains the mechanism for controlling the flow of fluid to and from the cuff
- a small fluid-filled reservoir in the abdomen – the fluid passes between this reservoir and the cuff as the device is activated and deactivated
The procedure to fit an artificial urinary sphincter often causes short-term bleeding and a burning sensation when you pass urine.
In the long-term, it’s not uncommon for the device to eventually stop working, in which case further surgery may be needed to remove it.
Surgery and procedures for urge incontinence
Botulinum toxin A injections
Botulinum toxin A (Botox) can be injected into the sides of your bladder to treat urge incontinence and overactive bladder syndrome.
This medication can sometimes help relieve these problems by relaxing your bladder. This effect can last for several months and the injections can be repeated if they help.
Although the symptoms of incontinence may improve after the injections, you may find it difficult to fully empty your bladder.
If this happens, you’ll need to be taught how to insert a thin, flexible tube called a catheter into your urethra to drain the urine from your bladder.
Botulinum toxin A isn’t currently licensed to treat urge incontinence or overactive bladder syndrome, so you should be made aware of any risks before deciding to have the treatment. The long-term effects of this treatment are not yet known.
Sacral nerve stimulation
The sacral nerves are located at the bottom of your back. They carry signals from your brain to some of the muscles used when you go to the toilet, such as the detrusor muscle that surrounds the bladder.
If your urge incontinence is the result of your detrusor muscles contracting too often, sacral nerve stimulation – also known as sacral neuromodulation – may be recommended.
During this operation, a device is inserted near one of your sacral nerves, usually in one of your buttocks. An electrical current is sent from this device into the sacral nerve.
This should improve the way signals are sent between your brain and your detrusor muscles, and so reduce your urges to urinate.
Sacral nerve stimulation can be painful and uncomfortable, but some people report a substantial improvement in their symptoms or the end of their incontinence completely.
Posterior tibial nerve stimulation
Your posterior tibial nerve runs down your leg to your ankle. It contains nerve fibres that start from the same place as nerves that run to your bladder and pelvic floor.
It’s thought that stimulating the tibial nerve will affect these other nerves and help control bladder symptoms, such as the urge to pass urine.
During the procedure, a very thin needle is inserted through the skin of your ankle and a mild electric current is sent through it, causing a tingling feeling and your foot to move.
You may need 12 sessions of stimulation, each lasting around half an hour, one week apart.
Some studies have shown that this treatment can offer relief from overactive bladder syndrome and urge incontinence for some people, although there isn’t enough evidence yet to recommend tibial nerve stimulation as a routine treatment.
Tibial nerve stimulation is only recommended in a few cases where urge incontinence hasn’t improved with medication and you don’t want to have botulinum toxin A injections or sacral nerve stimulation.
Augmentation cystoplasty
In rare cases, a procedure known as augmentation cystoplasty may be recommended to treat urge incontinence.
This procedure involves making your bladder bigger by adding a piece of tissue from your intestine into the bladder wall.
After the procedure, you may not be able to pass urine normally and may need to use a catheter. Because of this, augmentation cystoplasty will only be considered if you’re willing to use a catheter.
The difficulties passing urine can also mean that people who have augmentation cystoplasty can experience recurrent urinary tract infections.
Urinary diversion
Urinary diversion is a procedure where the tubes that lead from your kidneys to your bladder (ureters) are redirected to the outside of your body. The urine is then collected directly without it flowing into your bladder.
Urinary diversion should only be carried out if other treatments have been unsuccessful or are not suitable.
It can cause a number of complications, such as a bladder infection, and sometimes further surgery is needed to correct any problems that occur.
Catheterisation for overflow incontinence
Clean intermittent catheterisation
Clean intermittent catheterisation (CIC) is a technique that can be used to empty the bladder at regular intervals and so reduce overflow incontinence, also known as chronic urinary retention.
A continence adviser will teach you how to place a catheter through your urethra and into the bladder. Your urine flows out of your bladder, through the catheter and into the toilet.
Using a catheter can feel a bit painful or uncomfortable at first, but any discomfort should subside over time.
How often clean intermittent catheterisation will need to be carried out will depend on your individual circumstances. For example, you may only need clean intermittent catheterisation once a day, or you may need to use the technique several times a day.
Regular use of a catheter increases the risk of developing urinary tract infections (UTIs).
Indwelling catheterisation
If using a catheter every now and then isn’t enough to treat your overflow incontinence, you can have an indwelling catheter fitted instead.
This is a catheter inserted in the same way as for clean intermittent catheterisation, but left in place. A bag is attached to the end of the catheter to collect the urine.
Home remedies
Problems with urine leakage may require you to take extra care to prevent skin irritation:
- Use a washcloth to clean yourself
- Allow your skin to air-dry
- Avoid frequent washing and douching because these can overwhelm your body’s natural defenses against bladder infections
- Consider using a barrier cream, such as petroleum jelly or cocoa butter, to protect your skin from urine
- Ask your doctor about special cleansers made to remove urine that may be less drying than other products.
If you have urge incontinence or nighttime incontinence, make the toilet more convenient:
- Move any rugs or furniture you might trip over or collide with on the way to the toilet
- Use a night light to illuminate your path and reduce your risk of falling
If you have functional incontinence, you might:
- Keep a bedside commode in your bedroom
- Install an elevated toilet seat
- Widen an existing bathroom doorway
Alternative medicine
There are no alternative medicine therapies that have been proved to cure urinary incontinence. Early studies have shown that acupuncture can provide some short-term benefit, but more research is needed. Yoga may also provide some benefit for urinary incontinence, but more study is needed.
- Body Weight Planner. https://www.supertracker.usda.gov/bwp/index.html[↩]
- ChooseMyPlate. https://www.choosemyplate.gov/[↩]
- https://supertracker.usda.gov/[↩][↩][↩]
- BMI Calculator Adults. https://www.cdc.gov/healthyweight/assessing/bmi/adult_BMI/english_bmi_calculator/bmi_calculator.html[↩]
- BMI Calculator Children. https://www.cdc.gov/healthyweight/bmi/calculator.html[↩]
- http://www.baus.org.uk/_userfiles/pages/files/Patients/Leaflets/Pelvic%20floor%20XS%20female.pdf[↩]
- http://www.baus.org.uk/_userfiles/pages/files/Patients/Leaflets/Pelvic%20floor%20XS%20male.pdf[↩]





{kind=link}