Contents
What is vaginal cancer
Vaginal cancer is cancer that affects the vagina.
Vaginal cancer is rare, especially in women under 40.
Only about 1 of every 1,100 women will develop vaginal cancer in her lifetime. The American Cancer Society’s estimates for vaginal cancer in the United States for 2018 are 1:
- About 5,170 new cases of vaginal cancer will be diagnosed.
- About 1,330 women will die of vaginal cancer.
Symptoms of vaginal cancer include:
- vaginal bleeding after the menopause
- bleeding after sex or pain during sex
- smelly or bloodstained vaginal discharge
- bleeding between periods
- a lump or itch in your vagina that won’t go away
- pain when peeing, or needing to pee a lot.
The vagina
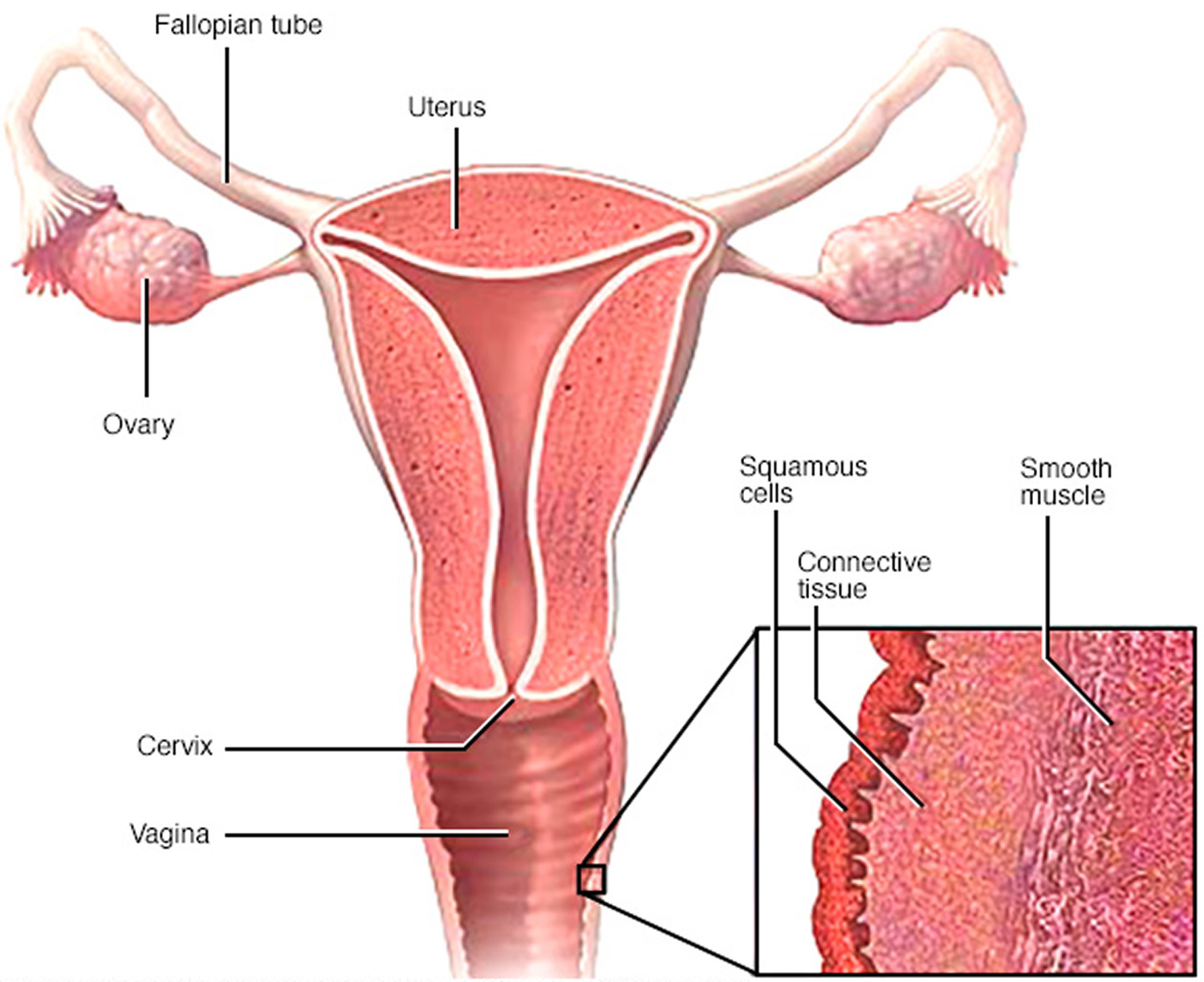
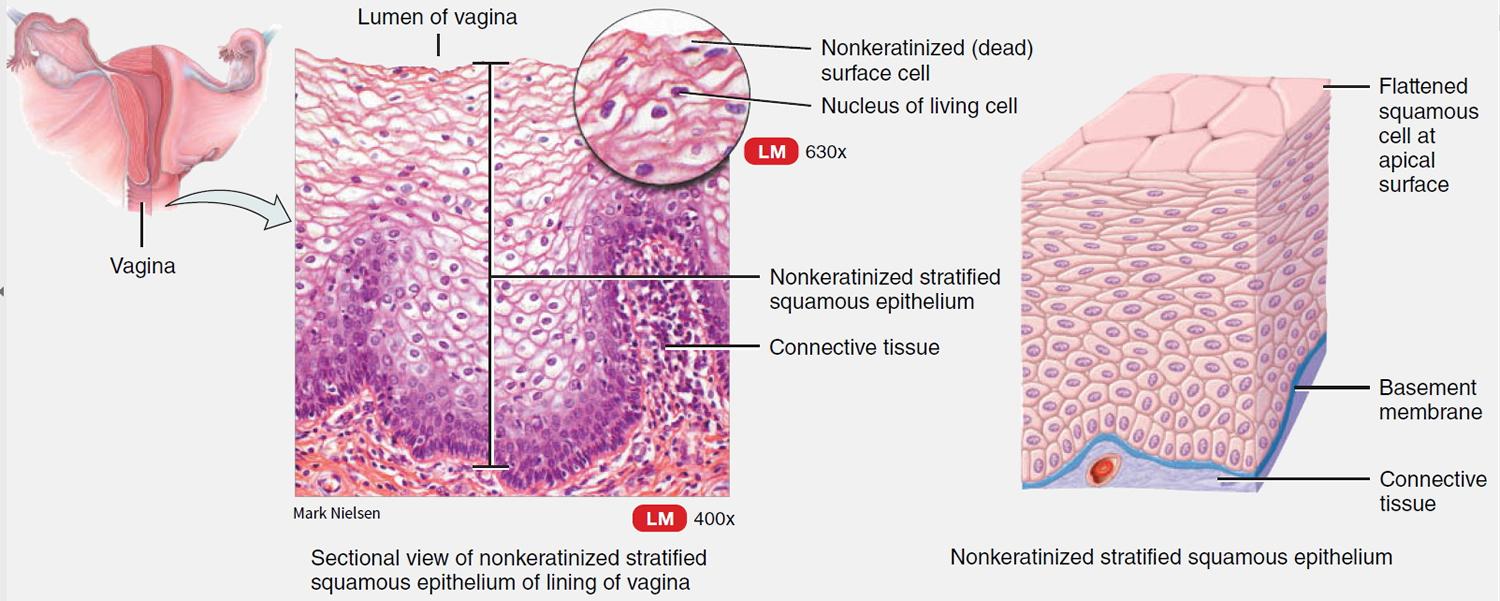
The vagina is a 3- to 4-inch (7½- to 10-cm) tube (see Figure 1). It’s sometimes called the birth canal. The vagina goes from the cervix (the lower part of the uterus) to open up at the vulva (the external female genitals). The vagina is lined by a layer of flat cells called squamous cells (see Figure 2). This layer of cells is also called epithelium (or epithelial lining) because it is formed by epithelial cells.
The vaginal wall underneath the epithelium is made up of connective tissue, muscle tissue, lymph vessels, and nerves. The vagina is usually collapsed with its walls touching each other. The vaginal walls have many folds that help the vagina open and expand during sexual intercourse or the birth of a baby. Glands near the opening of the vagina secrete mucus to keep the vaginal lining moist.
Figure 1. Female reproductive system
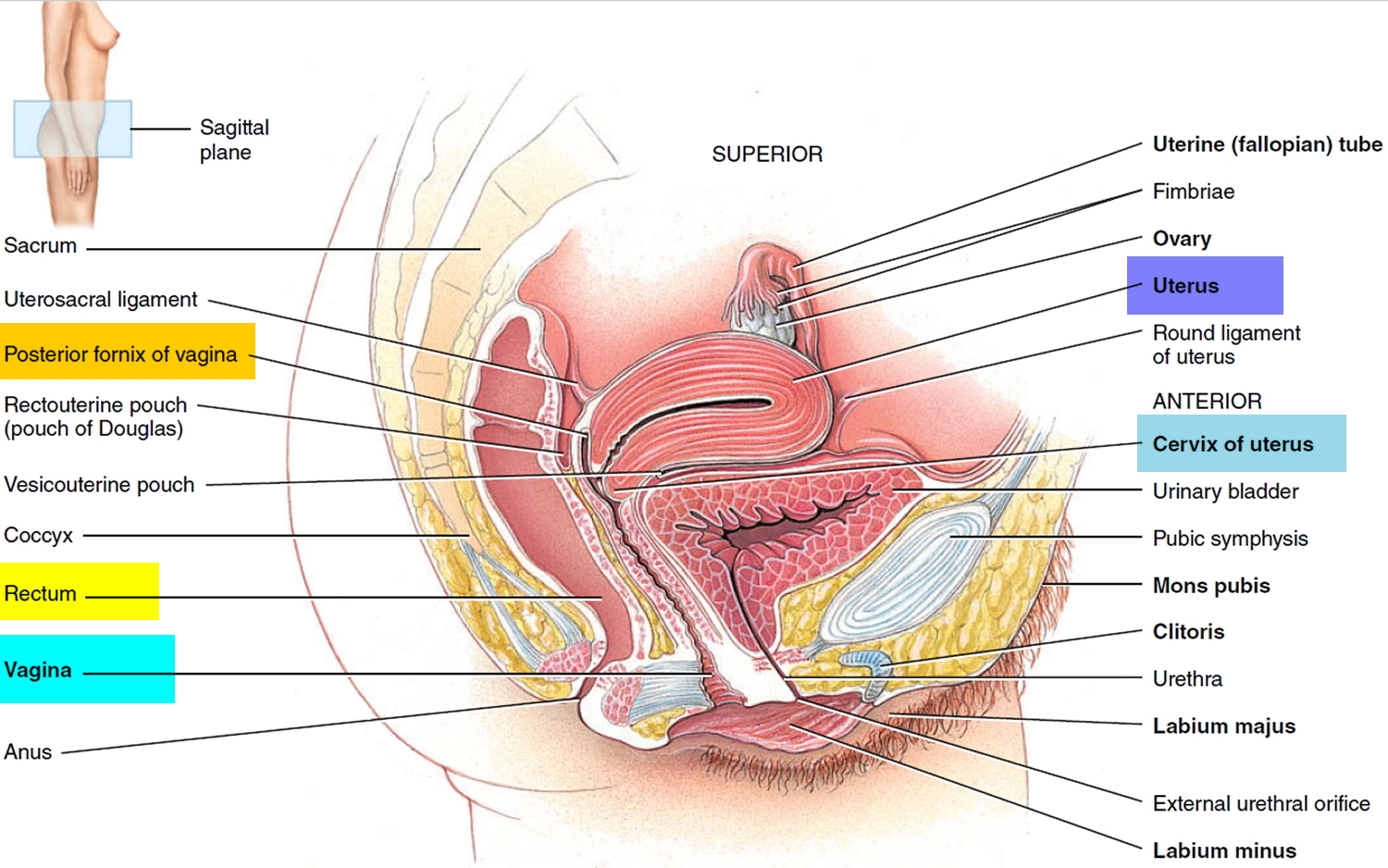
Figure 2. Cells of the vagina
Types of vaginal cancer
There are several types of vaginal cancer.
The most common type of vaginal cancer starts in the squamous cells (see Figures 2 and 3 above). It is called squamous cell carcinoma. A rarer type starts in the gland cells in the lining of the vagina. This is called adenocarcinoma.
Cancers that starts in the connective tissue of the vagina are extremely rare. They are called sarcomas.
Squamous cell carcinoma
About 70 of every 100 cases of vaginal cancer are squamous cell carcinomas. These cancers begin in the squamous cells that make up the epithelial lining of the vagina. Squamous cells are the flat, skin like cells that cover the surface of the vagina. The tumours look like small lumps (nodules) or sores (ulcers). These cancers are more common in the upper area of the vagina near the cervix. Squamous cell cancers of the vagina often develop slowly. First, some of the normal cells of the vagina get pre-cancerous changes. Then some of the pre-cancer cells turn into cancer cells. This process can take many years.
Before squamous cell cancer develops, there may be pre cancerous changes to the cells. These cell changes are called vaginal intraepithelial neoplasia (VAIN). The medical term most often used for this pre-cancerous condition is vaginal intraepithelial neoplasia (VAIN). “Intraepithelial” means that the abnormal cells are only found in the surface layer of the vaginal skin (epithelium). There are 3 types of vaginal intraepithelial neoplasia (VAIN): VAIN1, VAIN2, and VAIN3.
VAIN is graded 1, 2 or 3:
- VAIN 1 means the abnormal cells are in one third of the thickness of the vagina lining
- VAIN 2 means the abnormal cells are in two thirds of the thickness of the vagina lining
- VAIN 3 means the full thickness of the lining of the vagina has abnormal cells
Women who have VAIN 1 do not usually need any treatment. The cancerous cells often disappear after a while. Your doctor will arrange regular check ups to make sure this has happened.
Your doctor might recommend treating the abnormal cells if you have VAIN 2 or 3. This aim is to prevent vaginal cancer from developing.
VAIN 3 also indicates furthest progression toward a true cancer. Vaginal intraepithelial neoplasia (VAIN) is more common in women who have had their uterus removed (hysterectomy) and in those who were previously treated for cervical cancer or pre-cancer.
In the past, the term dysplasia was used instead of vaginal intraepithelial neoplasia (VAIN). This term is used much less now. When talking about dysplasia, there is also a range of increasing progress toward cancer – first, mild dysplasia; next, moderate dysplasia; and then severe dysplasia.
Verrucous carcinoma is a rare type of squamous cell vaginal cancer. It looks like a large wart and is a slow growing tumour that rarely spreads to other parts of the body. It is usually curable with surgery.
Treatment for VAIN 2 and 3
There are a number of treatment options for VAIN 2 or 3.
- Laser treatment
A laser is a very strong, hot beam of light that burns away the abnormal cells. Your doctor will use local anaesthetic to numb the area.
You might have some samples of tissue (biopsies) taken before the laser treatment. Your doctor sends the samples to the laboratory so that the cells can be examined.
- Surgery
You might have surgery, especially if the abnormal cells have come back or you have had a hysterectomy in the past.
You surgeon removes the abnormal cells and some surrounding healthy tissue. This is called a wide local excision. The doctor sends the tissue to the laboratory and the pathologist looks at the cells under a microscope.
Sometimes, a surgeon might remove the area of abnormal cells with a small loop of wire that has an electric current. This is called loop diarthermy or LEEP. They remove a surrounding area of healthy tissue to lower the risk of the abnormal cells coming back.
- Creams
Creams are not standard treatment for VAIN and are usually used as part of clinical trials. Imiquimod cream (Aldara) is a newer cream being tested for VAIN. It is an antiviral drug that boosts the immune system to destroy the abnormal cells.
Some women might have treatment with a chemotherapy cream called fluorouracil. This needs to be applied often and can irritate the delicate skin of the vagina. So it is not commonly used.
- Radiotherapy
Radiotherapy is not often used to treat VAIN. But you might have it if the pre-cancerous cells have come back after treatment or you have abnormal cells in several areas of your vagina.
You usually have internal radiotherapy (brachytherapy) to treat VAIN. You have a radioactive source or implant placed inside the vagina. This means a radioactive object called a source is placed inside your vagina to treat the local area. You may have this treatment over several hours or a few days.
Adenocarcinoma
Cancers that begin in gland cells are called adenocarcinomas. About 15 of every 100 cases of vaginal cancer are adenocarcinomas. The usual type of vaginal adenocarcinoma typically develops in women older than 50. One type, called clear cell adenocarcinoma, occurs more often in young women who were exposed to diethylstilbestrol (DES) in utero (when they were in their mother’s womb).
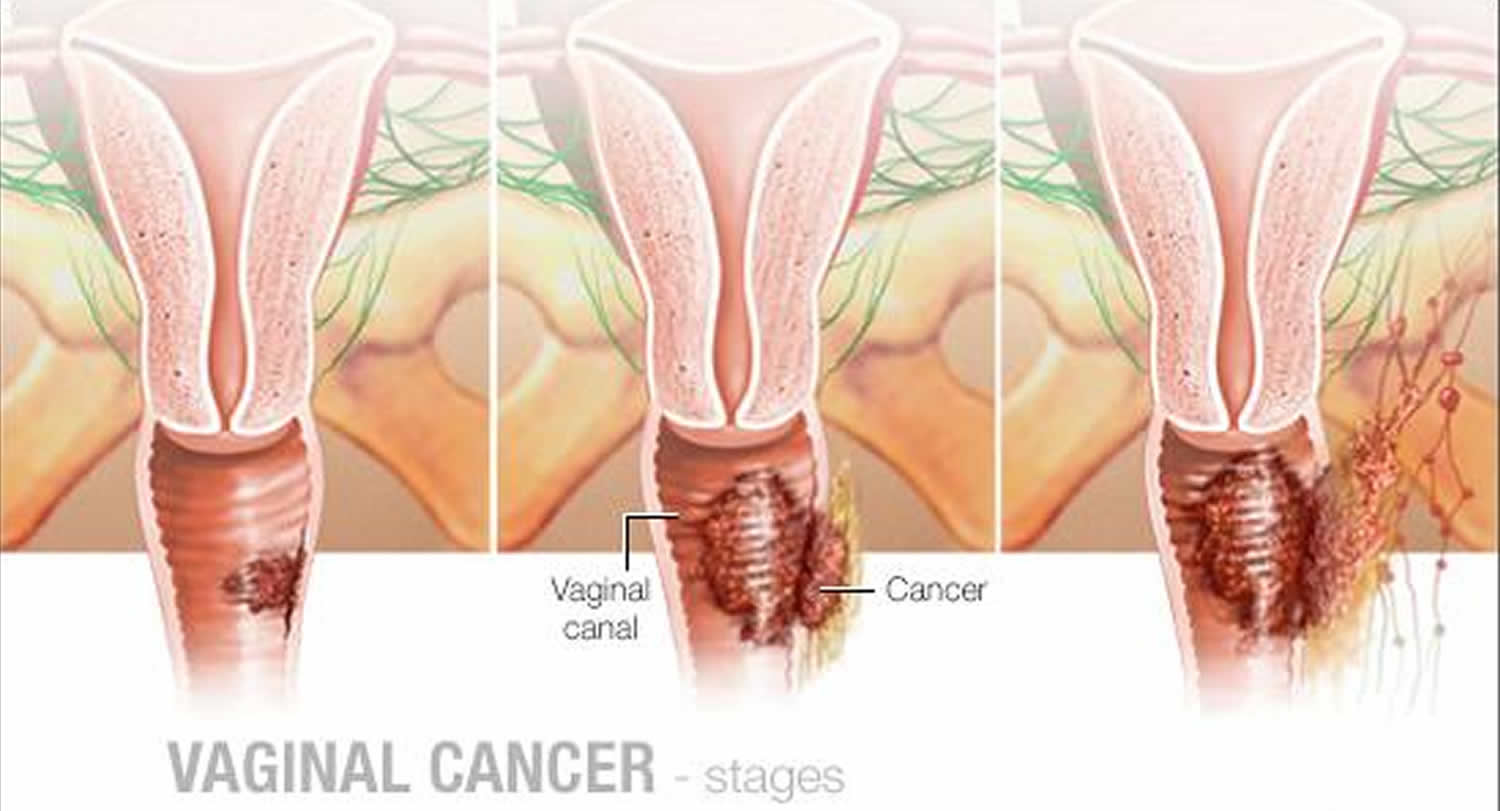
This type of cancer can be harder to diagnose than squamous cell cancer. The cancer is more likely to be hidden inside the vaginal canal. It’s sometimes difficult for doctors to tell whether this type of cancer started in the vagina, or in a nearby organ and then spread into the vagina.
There are 4 main types of adenocarcinoma of the vagina.
- Clear cell adenocarcinoma
Clear cell vaginal cancer:
- is a rare type
- only occurs in young women whose mothers took the diethylstilbestrol (DES) drug when they were pregnant
Up until 1971, DES was sometimes given to women to stop them having a miscarriage.
Clear cell cancers of the vagina usually develop in women in their teens or twenties, but there are reports of women being diagnosed in their early forties. As it’s now more than 40 years since DES was used in pregnancy, these cancers are becoming even rarer.
- Papillary adenocarcinoma
Papillary cancers can grow throughout the connective tissues that surround the vagina and hold it in place. They are less likely than other types of vaginal cancer to spread into nearby lymph nodes.
- Mucinous adenocarcinoma
Mucinous adenocarcinomas get their name from the pools of mucus that you can see around the cancer cells when you look at them under a microscope.
- Adenosquamous carcinoma
Adenosquamous cancers of the vagina are made up of a combination of squamous cells and gland cells. They are also called mixed epithelial tumors. They are very rare. Only between 1 and 2 out of every 100 women (1 to 2%) with vaginal cancer have this type. They are often quickly growing tumors.
Melanoma
Melanomas develop from pigment-producing cells that give skin its color. These cancers usually are found on sun-exposed areas of the skin but can form in the vagina or other internal organs. About 9 of every 100 cases of vaginal cancer are melanomas. Melanoma tends to affect the lower or outer portion of the vagina. The tumors vary greatly in size, color, and growth pattern.
Sarcoma
Sarcomas are cancers that begins in the cells of bones, muscles, or connective tissue. Up to 4 of every 100 cases of vaginal cancer are sarcomas. These cancers form deep in the wall of the vagina, not on its surface. There are several types of vaginal sarcomas. Rhabdomyosarcoma is the most common type of vaginal sarcoma. It’s most often found in children and is rare in adults. A sarcoma called leiomyosarcoma is seen more often in adults. It tends to occur in women older than 50.
Other cancers
Cancers that start in the vagina are much less common than cancers that start in other organs (such as the cervix, uterus, rectum, or bladder) and then spread to the vagina. These cancers are named after the place where they started. Also, a cancer that involves both the cervix and vagina is considered a cervical cancer. Likewise, if the cancer involves both the vulva and the vagina, it’s considered a vulvar cancer.
Grading of vaginal cancer
Grading is a way of dividing cancer cells into groups depending on how much the cells look like normal cells. This gives your doctor an idea of how quickly or slowly the cancer might grow and whether it is likely to spread.
Grade 1
The cells look very like normal cells. They are also called low grade or well differentiated. They tend to be slow growing and are less likely to spread than higher grade cancer cells.
Grade 2
The cells look more abnormal and are more likely to spread. This grade is also called moderately differentiated or moderate grade.
Grade 3
The cells look very abnormal and not like normal cells. They tend to grow quickly and are more likely to spread. They are called poorly differentiated or high grade.
Vaginal cancer causes
The exact cause of most vaginal cancers is not known. But scientists have found that it is associated with a number of other known risk factors and conditions.
Research has shown that normal cells make substances called tumor suppressor gene products to keep from growing too rapidly and becoming cancers. High-risk HPV (human papillomavirus) types (like 16 and 18) produce 2 proteins (E6 and E7) that can interfere with the functioning of known tumor suppressor gene products.
As mentioned in the section on risk factors, women exposed to diethylstilbestrol (DES) as a fetus (that is, their mothers took DES during pregnancy) are at increased risk for developing clear cell carcinoma. DES also increases the likelihood of vaginal adenosis (gland-type cells in the vaginal lining rather than the usual squamous cells). Most women with vaginal adenosis never develop vaginal clear cell carcinoma. However, those with a rare type of adenosis (called atypical tuboendometrial adenosis) do have an increased risk of developing this cancer.
Risk factors for vaginal cancer
A risk factor is anything that affects your chance of getting a disease such as cancer. Different cancers have different risk factors. For example, exposing skin to strong sunlight is a risk factor for skin cancer. Smoking is a risk factor for many cancers.
There are different kinds of risk factors. Some, such as your age or race, can’t be changed. Others may be related to personal choices such as smoking, drinking, or diet. Some factors influence risk more than others. But risk factors don’t tell us everything. Having a risk factor, or even several, does not mean that a person will get the disease. Also, not having any risk factors doesn’t mean that you won’t get it, either.
Scientists have found that certain risk factors make a woman more likely to develop vaginal cancer. But many women with vaginal cancer don’t have any apparent risk factors. And even if a woman with vaginal cancer has one or more risk factors, it’s impossible to know for sure how much that risk factor contributed to causing the cancer.
Age
Squamous cell cancer of the vagina occurs mainly in older women. Only 15% of cases are found in women younger than 40. Almost half of cases occur in women who are 70 years old or older.
Diethylstilbestrol (DES)
DES (diethylstilbestrol) is a man-made (synthetic) form of estrogen (a female hormone) that was given to some women to prevent miscarriage between 1938 and 1971. Women whose mothers took DES (diethylstilbestrol) (when pregnant with them) develop clear-cell adenocarcinoma of the vagina or cervix more often than would normally be expected. There is about 1 case of this type of cancer in every 1,000 daughters of women who took DES during their pregnancy. This means that about 99.9% of DES (diethylstilbestrol) daughters do not develop this cancer.
Many women do not know if they got DES (diethylstilbestrol) while they were pregnant. Any woman who was pregnant between 1938 and 1971 and had problems during the current or a previous pregnancy may have been given DES (diethylstilbestrol) or another estrogen-like drug. Women who did not have problems are less likely to have been given DES. Women who were not under a doctor’s care while pregnant most likely did not take DES (diethylstilbestrol) either, because you could only get it with a doctor’s prescription. DES (diethylstilbestrol) was given in pills, injections, and vaginal suppositories (sometimes called pessaries).
The Centers for Disease Control and Prevention (CDC) has a list of DES brand names on their website (www.cdc.gov/des/hcp/brand/index.html). Two of the most commonly used names were stilbestrol and DESPlex, but there are dozens more.
DES-related clear cell adenocarcinoma is more common in the vagina than the cervix. The risk appears to be greatest in those whose mothers took the drug during their first 16 weeks of pregnancy. Their average age when they are diagnosed is 19 years. Since the use of DES during pregnancy was stopped by the FDA in 1971, even the youngest DES daughters are older than 35 – past the age of highest risk. But a woman is not safe from a DES-related cancer at any age. Doctors do not know exactly how long women remain at risk.
DES (diethylstilbestrol) daughters have an increased risk of developing clear cell carcinomas, but women don’t have to be exposed to DES for clear cell carcinoma to develop. In fact, women were diagnosed with this type of cancer before DES was invented.
DES (diethylstilbestrol) daughters are also more likely to have high grade cervical dysplasia (CIN 3) and vaginal dysplasia (VAIN 3) when compared to women who were never exposed.
Getting recommended screening exams and tests
DES-exposed daughters should get regular gynecologic exams throughout their lifetimes. Discuss with your doctor which tests are appropriate for you and when you should have them.
Many doctors recommend these women have regular, thorough exams every year. These exams may include the following:
Pelvic exam
This is a physical exam of the reproductive organs. As part of a pelvic exam, the doctor feels the vagina, uterus, cervix, and ovaries for any lumps. This is also known as a bimanual exam. An exam of the rectal area may be included as well. Sometimes, feeling for lumps is the only way to find an abnormal growth.
Pap test
A routine Pap test is not enough for DES-exposed daughters. The cervical Pap test must be done along with a special Pap test of the vagina called a four-quadrant Pap test, in which cell samples are taken from all sides of the vagina.
Iodine staining of the cervix and vagina
An iodine solution is used to briefly stain the linings of the cervix and vagina. This helps the doctor find adenosis (an abnormal growth of glandular tissue that is not cancer) or other abnormal tissue.
Colposcopy
For this exam, the doctor uses a magnifier to look closely for abnormal tissue in the vagina and cervix. Some doctors do not do this for everyone, but this is commonly done if the Pap test result is not normal.
Biopsy
Small samples of any parts of the cervix or vagina that look abnormal on other tests are removed and looked at under a microscope to see if cancer cells are present.
Breast exams and screening tests
DES-exposed daughters should follow current breast cancer screening recommendations. Women should report any new breast lumps or other breast changes to a doctor right away.
Reducing risks during pregnancy
Because of the problems that may show up during pregnancy, DES-exposed daughters need to tell their doctors about their DES exposure. It’s best if they do this before they become pregnant. This way they can work with their doctors to watch for signs of problems and deal with them as soon as possible. Their pregnancies will probably be treated as high-risk, meaning these women will be closely watched by their doctors throughout the pregnancy.
Again, it’s important to note that most DES-exposed daughters do not have problems getting pregnant or carrying a baby to full term. All women should have good prenatal care, but it’s even more important for DES-exposed daughters.
Is it safe to use oral contraceptives (birth control pills) or hormone replacement therapy?
Each woman should talk about this with her doctor. Studies have not shown that birth control pills or hormone replacement therapy is unsafe for DES-exposed daughters, but some doctors believe DES-exposed daughters should avoid them because of the estrogen in them. Structural changes in the vagina or cervix do not usually cause problems with the use of other forms of contraception, such as diaphragms, female condoms, or spermicides.
Vaginal adenosis
Normally, the vagina is lined by flat cells called squamous cells. In about 40% of women who have already started having periods, the vagina may have one or more areas lined instead by glandular cells. These cells look like those found in the glands of the cervix, the lining of the body of the uterus (endometrium), and the lining of the fallopian tubes. These areas of gland cells are called adenosis. It occurs in nearly all women who were exposed to DES during their mothers’ pregnancy. Having adenosis increases the risk of developing clear cell carcinoma, but this cancer is still very rare. The risk of clear cell carcinoma in a woman who has adenosis that is not related to DES is very, very small. Still, many doctors feel that any woman with adenosis should have very careful screening and follow-up.
Human papillomavirus
HPV is short for human papilloma virus. HPVs are a large group of related viruses. Each virus in the group is given a number, which is called an HPV type.
Different HPV types can cause different types of warts in different parts of the body. Some types cause common warts on the hands and feet. Other types tend to cause warts on the lips or tongue.
Certain HPV types can infect the outer female and male genital organs and the anal area, causing raised, bumpy warts. These warts may barely be visible or they may be several inches across. The medical term for genital warts is condyloma acuminatum. These 2 types are seldom linked to cancer, and so are called low-risk types of HPV.
Other HPV types have been linked with cancers of the cervix and vulva in women, cancer of the penis in men, and cancers of the anus and throat (in men and women). These are known as high-risk types of HPV and include HPV 16 and HPV 18, as well as others. Infection with a high-risk HPV may produce no visible signs until pre-cancerous changes or cancer develops.
HPV can be passed from one person to another during skin-to-skin contact. One way HPV is spread is through sexual activity, including vaginal and anal intercourse and even oral sex.
Vaccines have been developed to help prevent infection with some types of HPV.
Cervical cancer
Having cervical cancer or pre-cancer (cervical intraepithelial neoplasia or cervical dysplasia) increases a woman’s risk of vaginal squamous cell cancer. This is most likely because cervical and vaginal cancers have similar risk factors, such as HPV infection and smoking.
Some studies suggest that treating cervical cancer with radiation therapy may increase the risk of vaginal cancer, but this was not seen in other studies, and the issue remains unresolved.
Smoking
Smoking cigarettes more than doubles a woman’s risk of getting vaginal cancer.
Alcohol
Drinking alcohol might affect the risk of vaginal cancer. A study of alcoholic women found more cases of vaginal cancer than expected. But this study was flawed because it didn’t look at other factors that can alter risk, such as smoking and HPV infection. A more recent study that did take these other risk factors into account found a decreased risk of vaginal cancer in women who do not drink alcohol at all.
Human immunodeficiency virus
Infection with HIV (human immunodeficiency virus), the virus that causes AIDS, also increases the risk of vaginal cancer.
Vaginal irritation
In some women, stretched pelvic ligaments may let the uterus sag into the vagina or even extend outside the vagina. This condition is called uterine prolapse and can be treated by surgery or by wearing a pessary, a device to keep the uterus in place. Some studies suggest that long-term (chronic) irritation of the vagina in women using a pessary may slightly increase the risk of squamous cell vaginal cancer. But this association is extremely rare, and no studies have conclusively proven that pessaries actually cause vaginal cancer.
Other risk factors that have been linked to an increased risk of vaginal cancer include:
- Multiple sexual partners
- Early age at first intercourse
Vaginal Cancer Prevention
The best way to reduce the risk of vaginal cancer is to avoid known risk factors and to find and treat any vaginal pre-cancers. But since many women with vaginal cancer have no known risk factors, it is not possible to completely prevent this disease.
HPV infection
Infection with human papillomavirus (HPV) is a risk factor for vaginal cancer. HPV infections occur mainly in younger women and are less common in women over 30. The reason for this is not clear.
HPV is passed from one person to another during skin-to-skin contact with an infected area of the body. HPV can be spread during sexual activity – including vaginal intercourse, anal intercourse, and oral sex – but sex doesn’t have to occur for the infection to spread. All that is needed is skin-to-skin contact with an area of the body infected with HPV. The virus can be spread through genital-to-genital contact. It’s even possible for a genital infection to spread through hand-to-genital contact.
An HPV infection also seems to be able to be spread from one part of the body to another. This means that an infection may start in the cervix and then spread to the vagina and vulva.
It can be very hard to avoid being exposed to HPV. If you are sexually active, limiting the number of sex partners and avoiding sex with people who have had many other sex partners can help lower your risk of exposure to HPV. But again, HPV is very common, so having sex with even one other person can put you at risk.
Infection with HPV is common, and in most cases the body is able to clear the infection on its own. But in some cases the infection does not go away and becomes chronic. Chronic infection, especially with high-risk HPV types, can eventually cause certain cancers, including vaginal cancer and pre-cancer.
A person can be infected with HPV for years without any symptoms, so the absence of visible warts cannot be used to tell if someone has HPV. Even when someone doesn’t have warts (or any other symptom), he (or she) can still be infected with HPV and pass the virus to somebody else.
Condom use
Condoms (“rubbers”) provide some protection against HPV. Condoms cannot protect completely because they don’t cover every possible HPV-infected area of the body, such as skin on the genital or anal area. Still, condoms do provide some protection against HPV, and they also protect against HIV and some other sexually transmitted diseases.
Get vaccinated
Vaccines are available that protect against certain HPV infections. All of them protect against infection with HPV subtypes 16 and 18. Some can also protect against infections with other HPV subtypes, including some types that cause anal and genital warts.
These vaccines can only be used to prevent HPV infection – they do not help treat an existing infection. To be most effective, the vaccines should be given before a person is exposed to HPV (such as through sexual activity).
These vaccines are approved to help prevent vaginal cancers and pre-cancers. They are also approved to help prevent others cancers, as well as anal and genital warts.
More HPV vaccines are being developed and tested.
Don’t smoke
Not smoking is another way to lower vaginal cancer risk. Women who don’t smoke are also less likely to develop a number of other cancers, such as those of the lungs, mouth, throat, bladder, kidneys, and several other organs.
Find and treat pre-cancerous conditions
Most vaginal squamous cell cancers are believed to start out as pre-cancerous changes, called vaginal intraepithelial neoplasia (VAIN). Vaginal intraepithelial neoplasia (VAIN) may be present for years before turning into a true (invasive) cancer. Screening for cervical cancer (such as with a Pap test or HPV test) can sometimes pick up these pre-cancers. If a pre-cancer is found, it can be treated, stopping cancer before it really starts.
Still, since vaginal cancer and VAIN are rare, doctors do not often do other tests to look for these conditions in women who do not have symptoms or a history of pre-cancer or cancer of the cervix, vagina, or vulva.
How Pap tests and pelvic examinations are done
First, the skin of the outer vaginal lips (labia majora) and inner lips (labia minora) is examined for any visible abnormalities. The health care professional first places a speculum inside the vagina. A speculum is a metal or plastic instrument that keeps the vagina open so that the cervix can be seen clearly. Next, using a small spatula, a sample of cells and mucus is lightly scraped from the exocervix (the surface of the cervix that is closest to the vagina). A small brush or a cotton-tipped swab is then inserted into the cervical opening to take a sample from the endocervix (the inside part of the cervix that is closest to the body of the uterus). Then, the speculum is removed.
The doctor then checks the organs of the pelvis by inserting 1 or 2 gloved fingers of one hand into the vagina while feeling (palpating) the lower abdomen, just above the pubic bone, with the other. The doctor may do a rectal exam at this time also. It’s very important to know that a Pap test is not always done when a pelvic exam is done, so if you are uncertain you should ask if one was done.
Vaginal intraepithelial neoplasia (VAIN; pre-cancer of the vagina) may not be visible during a routine exam of the vagina. But it may be found with a Pap test. Because cervical cancer is much more common than vaginal cancer, Pap test samples are scraped or brushed from the cervix. However, some cells of the vaginal lining are usually also picked up at the same time. That allows cases of VAIN to be found in women whose vaginal lining is not intentionally scraped. Still, the main goal of a Pap test is to find cervical pre-cancers and early cervical cancers, not vaginal cancer or VAIN. That’s why women who have had a total hysterectomy (removal of the uterus and cervix) stop getting Pap tests, unless the hysterectomy was done as a treatment for cervical pre-cancer (or cancer).
In women whose cervix has been removed by surgery to treat cervical cancer or pre-cancer, Pap test samples may be taken from the lining of the upper vagina to look for cervical cancer (that has come back), and to look for early vaginal cancer or VAIN. Vaginal cancer and VAIN are more common in women who have had cervical cancer or pre-cancer.
Many women with VAIN may also have a pre-cancer of the cervix (known as cervical intraepithelial neoplasia or CIN). If abnormal cells are seen on a Pap test, the next step is a procedure called colposcopy, in which the cervix, the vagina, and at times the vulva are examined with a special instrument called a colposcope.
Can Vaginal Cancer Be Found Early?
Some cases of vaginal cancer can be found early. They may produce symptoms that cause patients to seek medical attention, but many vaginal cancers do not cause symptoms until after they have reached an advanced stage. Pre-cancerous areas of vaginal intraepithelial neoplasia (VAIN) do not usually produce any symptoms. Still, well-woman exams and cervical cancer screening can sometimes find cases of VAIN and early invasive vaginal cancer.
Vaginal cancer signs and symptoms
More than 8 out of 10 women with invasive vaginal cancer have one or more symptoms, such as:
- Abnormal vaginal bleeding (often after intercourse)
- Abnormal vaginal discharge
- A mass that can be felt
- Pain during intercourse
Symptoms of advanced vaginal cancer may be painful urination, constipation, and continuous pain in the pelvis.
Having these symptoms does not always mean that you have cancer. In fact, these symptoms are more likely to be caused by something besides cancer, like an infection. The only way to know for sure what’s causing these problems is to see a health care professional. If you have any of these symptoms, discuss them with a doctor right away. Remember, the sooner the problem is correctly diagnosed, the sooner you can start treatment, and the more effective your treatment will be.
Vaginal cancer diagnosis
If a woman has any of the signs or symptoms of vaginal cancer, she should see a doctor. If the Pap test detects abnormal cells, or if the pelvic exam results are not normal, more tests will be needed. This may mean referral to a gynecologist (specialist in problems of the female genital system).
Medical history and physical exam
The first step is for the doctor to take a complete medical history to check for risk factors and symptoms. Then your doctor will physically examine you, including a pelvic exam and possibly a Pap test and a vaginal biopsy.
Colposcopy
If certain symptoms suggest cancer or if the Pap test shows abnormal cells, you will need to have a test called colposcopy. In this procedure you will lie on the exam table as you do for a pelvic exam. A speculum is placed in the vagina. The doctor will use the colposcope to examine the cervix and vagina. The colposcope stays outside the body and has magnifying lenses (like binoculars). When the doctor looks through the colposcope, he or she can see the vaginal walls and the surface of the cervix closely and clearly. Sometimes a weak solution of acetic acid (similar to vinegar) or iodine is applied to make any abnormal areas easier to see. Using a colposcope to look at the vagina is called vaginoscopy.
Colposcopy itself is no more painful than a speculum exam and can be done safely even if you are pregnant. If an abnormal area is seen on the cervix or vagina, a biopsy will be done. The biopsy can be slightly painful and may some cause pelvic cramping.
Biopsy
Certain signs and symptoms may strongly suggest vaginal cancer, but many of them can be caused by conditions that aren’t cancer. The only way to be certain that cancer is present is to do a biopsy. In this procedure, a small piece of tissue from the suspicious area is removed. A doctor specializing in diagnosing diseases by laboratory tests (a pathologist) will look at the tissue sample under a microscope to see if cancer or a pre-cancerous condition is present and, if so, what type it is.
Nearby lymph nodes
There are lymph nodes around the vagina (also called lymph glands). They’re small bean shaped glands that are part of the lymphatic system. They drain fluid from the tissues around the vagina and help to control infection by trapping and killing bacteria and viruses. The nearest lymph nodes are usually the first place that cancer cells reach when they break away from a tumor.
Your specialist may remove some of the lymph nodes during surgery. These will be closely looked at under a microscope to see if they contain cancer cells. This helps your specialist stage the cancer, so they can decide on the most suitable treatment for you.
Imaging tests
Chest x-ray
If vaginal cancer is diagnosed, a plain x-ray of your chest may be done to see if your cancer has spread to your lungs. This is very unlikely unless your cancer is far advanced. This x-ray can be done in any outpatient setting.
Computed tomography (CT)
The computed tomography (CT) scan is an x-ray test that produces detailed cross-sectional images of your body. Instead of taking one picture, like a standard x-ray, a CT scanner takes many pictures as it rotates around you. A computer then combines these pictures into an image of a slice of your body. A CT scan can provide information about the size, shape, and position of a tumor, and can be helpful to see if the cancer has spread to other organs. It can also help find enlarged lymph nodes that might have cancer cells.
A CT scanner has been described as a large donut, with a narrow table in the middle opening. You will need to lie still on the table while the scan is being done. CT scans take longer than regular x-rays, and you might feel a bit confined by the ring while the pictures are being taken.
Before the test, you may be asked to drink 1 to 2 pints of a liquid called oral contrast. This helps outline the intestine so that certain areas are not mistaken for tumors. You may also receive an IV line through which a different kind of contrast dye (IV contrast) is injected. This helps better outline structures such as blood vessels in your body.
The injection can cause some flushing (redness and warm feeling). A few people are allergic to the dye and get hives, or rarely, have more serious reactions like trouble breathing and low blood pressure. Be sure to tell the doctor if you have ever had a reaction to any contrast material used for x-rays.
CT-guided needle biopsy: CT scans can also be used to guide a biopsy needle precisely into a suspected tumor. For this procedure, the patient remains on the CT scanning table, while a doctor moves a biopsy needle through the skin and toward the tumor. CT scans are repeated until the needle is within the mass. A fine-needle biopsy sample or a core needle biopsy sample is removed and looked at under a microscope. This is not used to biopsy vaginal tumors, but it may be used to biopsy possible metastases.
Magnetic resonance imaging (MRI)
Magnetic resonance imaging (MRI) scans use radio waves and strong magnets instead of x-rays to make images of the body. The energy from the radio waves is absorbed by the body and then released in a specific pattern formed by the type of tissue and by certain diseases. A computer translates the pattern into a detailed image of parts of the body. Like a CT scanner, this produce cross-sectional slices of the body. An MRI can also produce slices that are parallel with the length of your body. As with a CT scan, a contrast material might be used, but it is not needed as often.
MRI scans are more uncomfortable than CT scans. They take longer – often up to an hour. You have to be placed inside tube-like equipment. This is confining and can upset people with claustrophobia (a fear of close spaces). If you have trouble with close spaces, let your doctor know before the MRI scan. Sometimes medicine can be given just before the scan to reduce anxiety. Another option is to use a special “open” MRI machine that is less confining and more comfortable for such people, the drawback being that the images from these machines are not as good. The machine also makes a buzzing or clanging noise that some people find disturbing. Some places will provide headphones with music to block this noise.
MRI images are particularly useful in examining pelvic tumors. They may show enlarged lymph nodes in the groin. They are also helpful in finding cancer that has spread to the brain or spinal cord. This rarely occurs in vaginal cancer.
Positron emission tomography
Positron emission tomography (PET) uses glucose (a form of sugar) that contains a low-level radioactive atom. Because cancer cells use glucose at a higher rate than normal cells, they absorb more of the radioactive sugar. The areas of radioactivity are detected with this test.
You will be injected with the special glucose, and then about an hour later you will be moved onto a table in the PET scanner. You lie on the table for about 30 minutes while a special camera creates a picture of areas of radioactivity in the body. The picture is not finely detailed like a CT or MRI scan, but it provides helpful information about your body.
This test can be helpful for spotting collections of cancer cells, and seeing if the cancer has spread to lymph nodes. PET scans are also useful when your doctor thinks the cancer has spread, but doesn’t know where (although they aren’t useful for finding cancer spread in the brain). PET scans can be used instead of several different x-rays because they scan your whole body. Often, a machine that combines a PET scanner and a CT scanner (called a PET/CT) is used, which gives more information about areas of cancer and cancer spread.
PET scans are not often used in patients with early vaginal cancer, but they may be helpful in finding areas of cancer spread.
Proctosigmoidoscopy
Proctosigmoidoscopy is a procedure that looks at the rectum and part of the colon. It’s done to check for spread of vaginal cancer to the rectum or colon. In this procedure a slender, flexible, hollow, lighted tube is placed into the rectum. Any areas that look suspicious will be biopsied. This test may be somewhat uncomfortable, but it should not be painful. Proctosigmoidoscopy may be recommended for patients whose vaginal cancers are large and/or located in the part of the vagina next to the rectum and colon.
Cystoscopy
Cystoscopy is a procedure that looks at the inside of the bladder. It’s done to check for spread of vaginal cancer to the bladder. This procedure can be done in the doctor’s office or clinic. You may be given an intravenous drug to make you drowsy. A thin tube with a lens and light is inserted into the bladder through the urethra. If suspicious areas or growths are seen, a biopsy will be done. Cystoscopy may be recommended if a vaginal cancer is large and/or located in the front wall of the vagina, near the bladder.
Vaginal cancer staging
After a woman is diagnosed with vaginal cancer, doctors will try to figure out if it has spread, and if so, how far. This process is called staging. The stage of a cancer describes how much cancer is in the body. It helps determine how serious the cancer is and how best to treat it. Doctors also use a cancer’s stage when talking about survival statistics.
Vaginal cancer stages range from stage I (1) through IV (4). As a rule, the lower the number, the less the cancer has spread. A higher number, such as stage IV, means cancer has spread more. Although each person’s cancer experience is unique, cancers with similar stages tend to have a similar outlook and are often treated in much the same way.
How is the stage determined?
The 2 systems used for staging vaginal cancer, the FIGO (International Federation of Gynecology and Obstetrics) system and the AJCC (American Joint Committee on Cancer TNM staging system) are basically the same.
They both use 3 key pieces of information to stage (classify) this cancer :
- The extent (size) of the tumor (T): How large is the cancer and has it grown into the vaginal wall? Has the cancer reached nearby structures like the wall of the pelvis? (The pelvis is the internal cavity that contains the internal female reproductive organs, rectum, bladder, and parts of the large intestine.)
- The spread to nearby lymph nodes (N): Has the cancer spread to the lymph nodes in the pelvis or groin (inguinal) area?
- The spread (metastasis) to distant sites (M): Has the cancer spread to distant lymph nodes or distant organs?
Numbers or letters after T, N, and M provide more details about each of these factors. Higher numbers mean the cancer is more advanced. Once a person’s T, N, and M categories have been determined, this information is combined in a process called stage grouping to assign an overall stage.
The staging system in the table primarily uses the clinical stage. This is based on the results of a physical exam, biopsy, and imaging tests done before surgery. Surgical staging is determined by examining tissue removed during an operation.
The system described below is the most recent AJCC system, effective as of January 2018.
These systems are not used to stage vaginal melanoma, which is staged like melanoma of the skin.
Vaginal cancer staging can be complex, so ask your doctor to explain it to you in a way you understand.
Table 1. Vaginal cancer staging
| AJCC Stage | Stage grouping | FIGO Stage | Stage description* |
| IA | T1a N0 M0 | I | The cancer is only in the vagina and is no larger than 2.0 cm (4/5 inch) (T1a). It has not spread to nearby lymph nodes (N0) or to distant sites (M0). |
| IB | T1b N0 M0
| I | The cancer is only in the vagina and is larger than 2.0 cm (4/5 inch) (T1b). It has not spread to nearby lymph nodes (N0) or to distant sites (M0). |
| IIA
| T2a N0 M0 | II | The cancer has grown through the vaginal wall, but not as far as the pelvic wall and is no larger than 2.0 cm (4/5 inch) (T2a). It has not spread to nearby lymph nodes (N0) or to distant sites (M0). |
| IIB | T2b N0 M0 | II | The cancer has grown through the vaginal wall, but not as far as the pelvic wall and is larger than 2.0 cm (4/5 inch) (T2b). It has not spread to nearby lymph nodes (N0) or to distant sites (M0). |
| III
| T1 to T3 N1 M0 | III | The cancer can be any size and might be growing into the pelvic wall, and/or growing into the lower 1/3 of the vagina and/or has blocked the flow of urine (hydronephrosis) which is causing the kidneys to not work. (T1 to T3). It has also spread to nearby lymph nodes in the pelvis or groin (inguinal) area (N1) but not distant sites (M0). |
| OR | |||
| T3 N0 M0 | III | The cancer is growing into the pelvic wall, and/or growing into the lower 1/3 of the vagina and/or has blocked the flow of urine (hydronephrosis) which is causing the kidneys to not work. (T3). It has not spread to nearby lymph nodes (N0) or to distant sites (M0). | |
| IVA | T4 Any N M0 | IVA | The cancer is growing into the bladder or rectum or is growing out of the pelvis (T4). It might or might not have spread to lymph nodes in the pelvis or groin (inguinal area) (Any N). It has not spread to distant sites (M0). |
| IVB | Any T Any N M1 | IVB | The cancer has spread to distant organs such as the lungs or bones. (M1). It can be any size and might or might not have grown into nearby structures or organs (Any T). It might or might not have spread to nearby lymph nodes (Any N). |
* The T categories are described in the table above, except for: TX: Main tumor cannot be assessed due to lack of information. T0: No evidence of a primary tumor. The N categories are described in the table above, except for: NX: Regional lymph nodes cannot be assessed due to lack of information.
Vaginal cancer survival rates
The 5-year survival rate refers to the percentage of patients who live at least 5 years after their cancer is diagnosed. Of course, many people live much longer than 5 years (and many are cured).
Five-year disease-specific survival rates assume that some people will die of other causes and only count the deaths from the cancer itself. This is a more accurate way to describe the prognosis for patients with a particular type and stage of cancer.
Survival rates are often based on previous outcomes of large numbers of people who had the disease, but they cannot predict what will happen to any person specifically. Many other factors can affect a person’s outlook, such as their overall health, the treatment they receive, and how well the cancer responds to treatment. Your doctor can tell you how the numbers below may apply to you, as he or she is familiar with the aspects of your situation.
The numbers below come from the National Cancer Institute’s SEER database, and are based on women with vaginal cancer (any type) who were diagnosed between 1990 and 2004.
Table 2. Survival rates for vaginal cancer, by stage
| AJCC Stage | 5-Year Disease Specific Survival Rate |
| I | 84% |
| II | 75% |
| III and IV | 57% |
Survival rates also vary based on the type of vaginal cancer. The following statistics for vaginal cancer come from the SEER database, and are based on women who were diagnosed with vaginal cancer between 1988 and 2001. These are relative survival rates. Relative survival rates compare the observed survival with that expected for people without vaginal cancer. This is another way to describe the prognosis for patients with a particular type and stage of cancer.
- For all cases of vaginal cancer combined, the relative 5-year survival is about 50%.
- For squamous cell carcinoma of the vagina, the relative 5-year survival is 54%.
- For adenocarcinoma of the vagina it is almost 60%.
- For vaginal melanoma, the 5-year relative survival is only 13%.
Vaginal cancer treatment
After the diagnostic tests are done, your cancer care team will recommend a treatment plan. Don’t feel rushed about considering your options. If there’s anything you do not understand, ask to have it explained again. The choice of treatment depends on the type of cancer and stage of the disease when it is diagnosed.
Other factors might play a part in choosing the best treatment plan. These could include your age, your overall state of health, whether you plan to have children, and other personal considerations. Vaginal cancer can affect your sex life and your ability to have children. These concerns should also be considered as you make treatment decisions.
Be sure you understand all the risks and side effects of the various therapies before making a decision about treatment.
You might want to get a second opinion. This can provide more information and help you feel confident about the treatment plan you choose. Some insurance companies require a second opinion before they will pay for treatments.
Some treatments are only used to treat pre-cancers of the vagina (vaginal intraepithelial neoplasia, VAIN), such as:
- Laser surgery (vaporization)
- Topical treatments
For invasive vaginal cancer, there are 3 main treatments:
- Radiation therapy
- Surgery
- Chemotherapy
Invasive vaginal cancer is treated mainly with radiation therapy and surgery. Chemotherapy in combination with radiation might be used to treat advanced disease.
Surgery
Types of surgery that may be used to treat vaginal cancer include:
- Removal of small tumors or lesions. Cancer limited to the surface of your vagina may be cut away, along with a small margin of surrounding healthy tissue to ensure that all of the cancer cells have been removed.
- Removal of the vagina (vaginectomy). Removing part of your vagina (partial vaginectomy) or your entire vagina (radical vaginectomy) may be necessary to remove all of the cancer. Depending on the extent of your cancer, your surgeon may recommend surgery to remove your uterus and ovaries (hysterectomy) and nearby lymph nodes (lymphadenectomy) at the same time as your vaginectomy.
- Removal of the majority of the pelvic organs (pelvic exenteration). This extensive surgery may be an option if cancer has spread throughout your pelvic area or if your vaginal cancer has recurred. During pelvic exenteration, the surgeon may remove many of the organs in your pelvic area, including your bladder, ovaries, uterus, vagina, rectum and the lower portion of your colon. Openings are created in your abdomen to allow urine (urostomy) and waste (colostomy) to exit your body and collect in ostomy bags.
If your vagina is completely removed, you may choose to undergo surgery to construct a new vagina. Surgeons use pieces of skin, sections of intestine or flaps of muscle from other areas of your body to form a new vagina.
With some adjustments, a reconstructed vagina allows you to have vaginal intercourse. However, a reconstructed vagina isn’t the same as your own vagina. For instance, a reconstructed vagina lacks natural lubrication and creates a different sensation when touched due to changes in surrounding nerves.
Radiation therapy
Radiotherapy is the main treatment for vaginal cancer.
Radiation therapy uses high-powered energy beams, such as X-rays, to kill cancer cells. Radiation can be delivered two ways:
- External radiation. External beam radiation is directed at your entire abdomen or just your pelvis, depending on the extent of your cancer. During external beam radiation, you’re positioned on a table and a large radiation machine is maneuvered around you in order to target the treatment area. Most women with vaginal cancer receive external beam radiation.
- Internal radiation. During internal radiation (brachytherapy), radioactive devices — seeds, wires, cylinders or other materials — are placed in your vagina or the surrounding tissue. After a set amount of time, the devices may be removed. Those with very early-stage vaginal cancer may receive internal radiation only. Others may receive internal radiation after undergoing external radiation.
Radiation therapy kills quickly growing cancer cells, but it may also damage nearby healthy cells, causing side effects. Side effects of radiation depend on the radiation’s intensity and where it’s aimed.
Other options
If surgery and radiation can’t control your cancer, you may be offered other treatments, including:
- Chemotherapy. Chemotherapy uses chemicals to kill cancer cells. It isn’t clear whether chemotherapy is useful for treating vaginal cancer. For this reason, chemotherapy generally isn’t used on its own to treat vaginal cancer. Chemotherapy may be used during radiation therapy to enhance the effectiveness of radiation.
- Clinical trials. Clinical trials are experiments to test new treatment methods. While a clinical trial gives you a chance to try the latest treatment advances, a cure isn’t guaranteed. Discuss available clinical trials with your doctor to better understand your options, or contact the National Cancer Institute or the American Cancer Society to find out what clinical trials might be available to you.
Supportive (palliative) care
Palliative care is specialized medical care that focuses on providing relief from pain and other symptoms of a serious illness. Palliative care specialists work with you, your family and your other doctors to provide an extra layer of support that complements your ongoing care.
When palliative care is used along with all of the other appropriate treatments, people with cancer may feel better and live longer.
Palliative care is provided by a team of doctors, nurses and other specially trained professionals. Palliative care teams aim to improve the quality of life for people with cancer and their families. This form of care is offered alongside curative or other treatments you may be receiving.
Coping and support
How you respond to your cancer diagnosis is unique. You might want to surround yourself with friends and family, or you may ask for time alone to sort through your feelings. The shock and confusion of your diagnosis may leave you feeling lost and unsure of yourself. To help you cope, try to:
- Learn enough about your cancer to make decisions about your care. Write down the questions to ask at your next doctor appointment. Get a friend or family member to come to appointments with you to take notes. Ask your health care team for further sources of information. The National Cancer Institute 2 and the American Cancer Society 3 are good places to start. The more you know about your condition, the more comfortable you may feel when it comes time to make decisions about your treatment.
- Maintain intimacy with your partner. Vaginal cancer treatments are likely to cause side effects that make sexual intimacy more difficult for you and your partner. If treatment makes sex painful or temporarily impossible, try to find new ways of maintaining intimacy. Spending quality time together and having meaningful conversations are ways to build your emotional intimacy. When you’re ready for physical intimacy, take it slowly. If sexual side effects of your cancer treatment are hurting your relationship with your partner, talk to your doctor. He or she may offer ways to cope with sexual side effects and may refer you to a specialist.
- Create a support network. Having friends and family supporting you can be valuable. You may find it helps to talk with someone about your emotions. Other sources of support include social workers and psychologists — ask your doctor for a referral if you feel like you need someone to talk to. Talk with your pastor, rabbi or other spiritual leader. Other people with cancer can offer a unique perspective and may better understand what you’re going through, so consider joining a support group — whether it’s in your community or online. Contact the American Cancer Society for more information on support groups.





{kind=link}