
Contents
What is vasovagal syncope
Syncope is defined by rapid onset of brief loss of consciousness and postural tone attributed to cerebral hypoperfusion with spontaneous recovery 1. Syncope is commonly called fainting or “passing out.” Vasovagal syncope occurs when you faint because your body overreacts to certain triggers, such as the sight of blood or extreme emotional distress. It may also be called neurocardiogenic syncope. Vasovagal syncope is not epilepsy, it is not a seizure and it is not concussion nor it is transient ischemic attack [TIA] 1.
If an individual is about to faint, he or she will feel dizzy, lightheaded, or nauseous and their field of vision may “white out” or “black out.” The skin may be cold and clammy. The person drops to the floor as he or she loses consciousness. After fainting, an individual may be unconscious for a minute or two, but will revive and slowly return to normal. Syncope can occur in otherwise healthy people and affects all age groups, but occurs more often in the elderly. There are several types of syncope.
The vasovagal syncope trigger causes your heart rate to slow (bradycardia) and blood pressure to drop (hypotension) suddenly, usually brought on by multiple different types of stimuli including prolonged sitting or standing, emotional stress, trauma, pain, the sight of blood, pain and anxiety, large muscle use, and exercise 2. That leads to reduced blood flow to your brain, causing you to briefly lose consciousness. The proposed mechanism of vasovagal syncope, which has not been fully understood, is thought to be associated with the imbalance between the sympathetic and the parasympathetic nervous systems, as well as the abnormal regulation of peripheral vascular tone 3. Vasovagal syncope occurs when arterial pressure decreases below that which provides adequate cerebral blood flow to maintain consciousness.
Vasovagal syncope is usually harmless and requires no treatment 4. However, vasovagal syncope can be recurrent, causing significant injury in 5% of cases, and leads to impaired quality of life 5. Your doctor may recommend tests to rule out more serious causes of fainting, such as heart disorders.
The immediate treatment for an individual who has fainted involves checking first to see if their airway is open and they are breathing. The person should remain lying down for at least 10-15 minutes, preferably in a cool and quiet space. If this isn’t possible, have the individual sit forward and lower their head below their shoulders and between their knees. Ice or cold water in a cup is refreshing. For individuals who have problems with chronic fainting spells, therapy should focus on recognizing the triggers and learning techniques to keep from fainting. At the appearance of warning signs such as lightheadedness, nausea, or cold and clammy skin, counter-pressure maneuvers that involve gripping fingers into a fist, tensing the arms, and crossing the legs or squeezing the thighs together can be used to ward off a fainting spell. If fainting spells occur often without a triggering event, syncope may be a sign of an underlying heart disease.
If you see someone having a seizure or fit, there are some simple things you can do to help. You should call an ambulance if you know it’s their first seizure or it’s lasting longer than 5 minutes.
It might be scary to witness, but don’t panic.
If you’re with someone having a seizure:
- only move them if they’re in danger – such as near a busy road or hot cooker
- cushion their head if they’re on the ground
- loosen any tight clothing around their neck – such as a collar or tie to – aid breathing
- when their convulsions stop, turn them so they’re lying on their side (the recovery position)
- stay with them and talk to them calmly until they recover
- note the time the seizure starts and finishes
If they’re in a wheelchair, put the brakes on and leave any seatbelt or harness on. Support them gently and cushion their head, but don’t try to move them.
- Don’t put anything in their mouth, including your fingers. They shouldn’t have any food or drink until they fully recover.
When to call an ambulance:
Call your local emergency number and ask for an ambulance if:
- it’s the first time someone has had a seizure
- the seizure lasts for more than 5 minutes
- the person doesn’t regain full consciousness, or has several seizures without regaining consciousness
- the person is seriously injured during the seizure
People with epilepsy don’t always need to go to hospital every time they have a seizure.
Some people with epilepsy wear a special bracelet or carry a card to let medical professionals and anyone witnessing a seizure know they have epilepsy.
Figure 1. Recovery position

Vasovagal syncope pregnancy
Vasovagal syncope patients have no greater risk of gynecological abnormalities and pregnancy complications than healthy subjects 6. Vasovagal syncope patients and healthy subjects had similar rates of pregnancy (41% vs. 38%). Among those participants who were pregnant, there were no differences in the incidence of difficulties getting pregnant or complications during pregnancy such as gestational diabetes, high blood pressure, preterm delivery, preeclampsia, miscarriages, or vaginal bleeding 6. There were no significant differences in lightheadedness during the three trimesters of pregnancy between vasovagal syncope patients and healthy subjects. Neither cohort reported a significant increase in presyncope during pregnancy compared to their non-pregnant state 6.
Fainting can be a sign of a more serious condition, such as a heart or brain disorder. You may want to consult your doctor after a fainting spell, especially if you never had one before.
Vasovagal syncope causes
Vasovagal syncope occurs when the part of your nervous system that regulates heart rate and blood pressure malfunctions in response to a trigger, such as the sight of blood.
Your heart rate slows, and the blood vessels in your legs widen (dilate.) This allows blood to pool in your legs, which lowers your blood pressure. Combined, the drop in blood pressure and slowed heart rate quickly reduce blood flow to your brain, and you faint.
Vasovagal syncope triggers
- Standing for long periods of time
- Heat exposure
- Seeing blood
- Having blood drawn
- Fear of bodily injury
- Straining, such as to have a bowel movement
Vasovagal syncope prevention
You may not always be able to avoid a vasovagal syncope episode. If you feel like you might faint, lie down and lift your legs.
This allows gravity to keep blood flowing to your brain. If you can’t lie down, sit down and put your head between your knees until you feel better.
Vasovagal syncope symptoms
Before you faint due to vasovagal syncope, you may experience some of the following:
- Pale skin
- Lightheadedness
- Tunnel vision — your field of vision narrows so that you see only what’s in front of you
- Nausea
- Feeling warm
- A cold, clammy sweat
- Yawning
- Blurred vision
During a vasovagal syncope episode, bystanders may notice:
- Jerky, abnormal movements
- A slow, weak pulse
- Dilated pupils
Recovery after a vasovagal episode generally begins in less than a minute. However, if you stand up too soon after fainting — within about 15 to 30 minutes — you’re at risk of fainting again.
Vasovagal syncope diagnosis
Diagnosing vasovagal syncope often involves ruling out other possible causes of your fainting — particularly heart-related problems. These tests may include:
- Electrocardiogram. This test records the electrical signals your heart produces. It can detect irregular heart rhythms and other cardiac problems. You may need to wear a portable monitor for at least a day or as long as a month.
- Echocardiogram. This test uses ultrasound imaging to view the heart and look for conditions, such as valve problems, that can cause fainting.
- Exercise stress test. This test studies heart rhythms during exercise. It’s usually conducted while you walk or jog on a treadmill.
- Blood tests. Your doctor may look for conditions, such as anemia, that can cause or contribute to fainting spells.
Tilt table test
If no heart problems appear to cause your fainting, your doctor may suggest you undergo a tilt table test. For a tilt table test:
- You lie flat on your back on a table.
- The table changes position, tilting you upward at various angles.
- A technician monitors your heart rhythms and blood pressure to see if the postural changes affect them.
Vasovagal syncope treatment
In most cases of vasovagal syncope, treatment is unnecessary. Your doctor may help you identify your fainting triggers and discuss ways you might avoid them.
However, if you experience vasovagal syncope often enough to interfere with your quality of life, your doctor may suggest trying one or more of the following remedies.
Table 1. Treatment of Vasovagal Syncope
| Non-pharmacologic Interventions |
| Avoid exacerbating situations (hot weather, volume depletion) |
| Increase sodium and water intake in an effort to increase blood volume |
| Discontinue potentially offending medications |
| Diuretics |
| Venodilators |
| Isometric muscle contractions / Physical countermeasures with presyncope |
| Get down (supine) at onset of prodromal symptoms |
| Outpatient “tilt training” |
| Pharmacologic Interventions |
| Fludrocortisone oral 0.1–0.2 mg once daily (especially in young patients) |
| Midodrine oral 2.5–10 mg every 4 hour x 3/day (avoid within 4–5 hour of bedtime) |
| Metoprolol oral 25 mg twice daily (would use in the elderly or hypertensive patient) |
| Selective serotonin reuptake inhibitor (SSRI) (would only use if psychosocial issues are present) |
| Other Interventions |
| Implantable Loop Recorder to document asystole with clinical syncope |
| Consider Permanent Pacemaker if asystole is present during syncopal episodes |
Many approaches have been proposed for the treatment of vasovagal syncope 8. These include physical countermeasures, pharmacological approaches, and device-based modulation of heart rate. Our local treatment plans include early education, avoiding environmental triggers, and lifestyle changes. These strategies are often quite effective. If these are not effective, then the next step is pharmacologic or invasive electrophysiological treatments, although very few of these therapies have been shown to be effective in randomized clinical trials. Unfortunately, a small but significant minority of patients do not achieve adequate symptom control using usual treatments.
Medications
A drug called fludrocortisone acetate that’s normally used to treat low blood pressure may be helpful in preventing vasovagal syncope. Selective serotonin inhibitors may also be used.
Therapies
Your doctor may recommend ways to decrease the pooling of blood in your legs. These may include foot exercises, wearing compression stockings or tensing your leg muscles when standing.
You may need to increase salt in your diet if you don’t usually have high blood pressure. Avoid prolonged standing — especially in hot, crowded places — and drink plenty of fluids.
Surgery
Very rarely, inserting an electrical pacemaker to regulate the heartbeat may help some people with vasovagal syncope who haven’t been helped by other treatments.
Figure 2. Classes of recommendations (best recommendation is class 1)
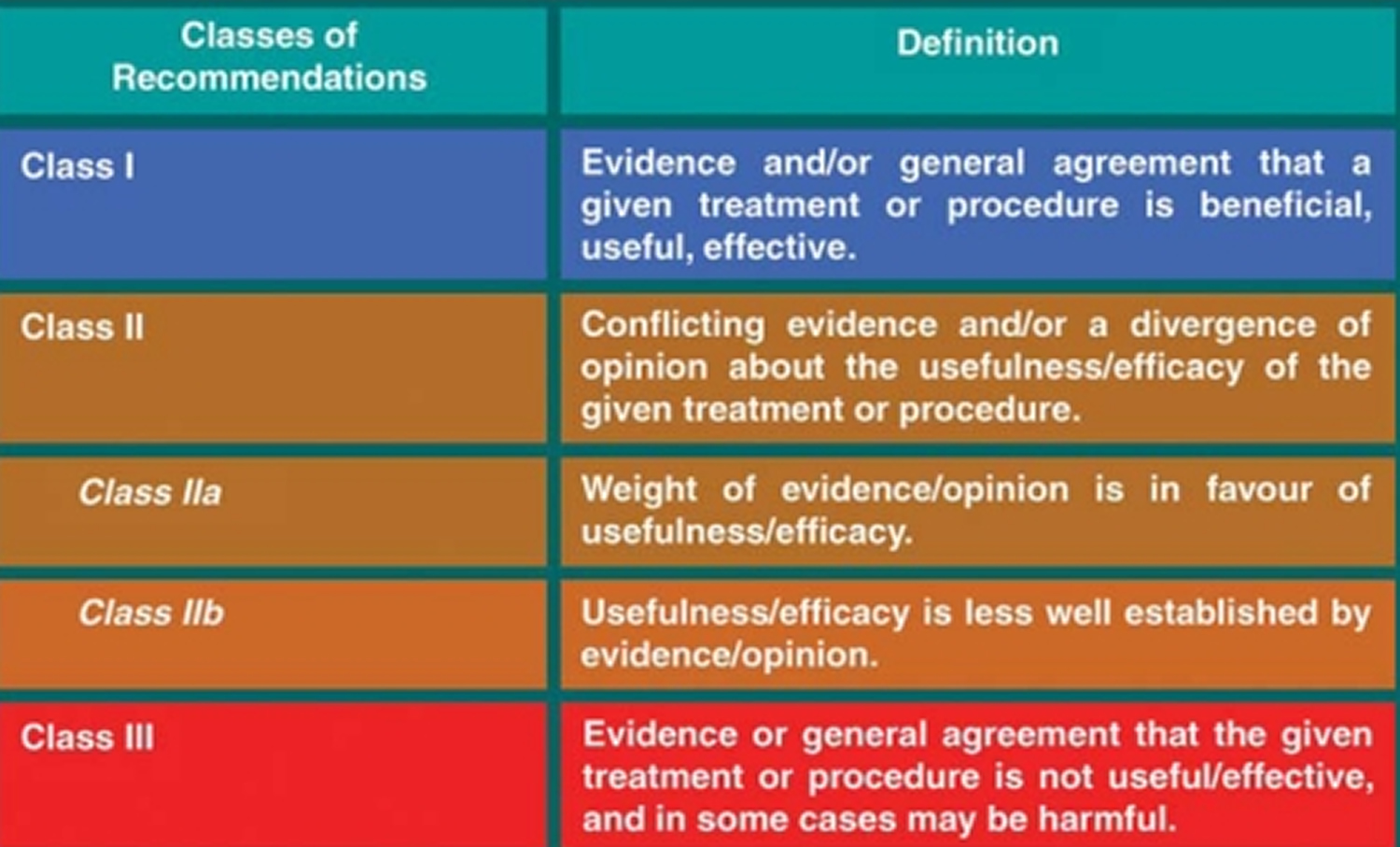
Note: Strength of recommendation and level of evidence grading used the American College of Cardiology & American Heart Association clinical practice guidelines guidance 9
Figure 3. Levels of evidence (best evidence is level A)
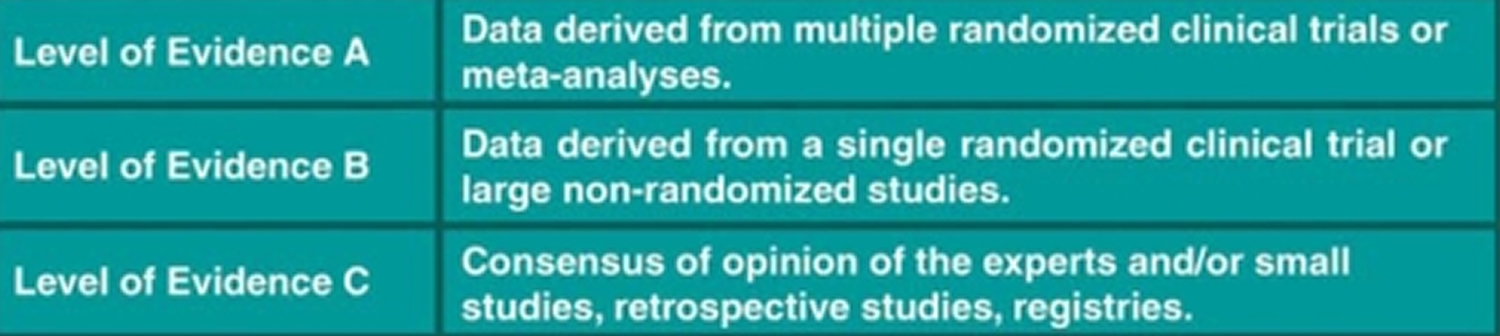
Note: Strength of recommendation and level of evidence grading used the American College of Cardiology & American Heart Association clinical practice guidelines guidance 9
Table 2. Non-pharmacologic Interventions for Vasovagal Syncope
| Treatment | Strength of Recommendation | Level of Evidence |
|---|---|---|
| Providing Early Education | Class IIa (Reasonable to Perform) | Level C |
| Explanation of disease prognosis | ||
Teaching about avoiding triggering situations
| ||
| Increasing sodium and water intake to increase intravascular volume | Class IIa (Reasonable to Perform) | Level B |
| Daily sodium intake of 10 grams for recurrent symptoms | ||
| Daily water intake of at least 2 liters | ||
| Discontinuing potentially offending medications | Class IIa (Reasonable to Perform) | Level C |
| Diuretics, vasodilators, venodilators | ||
| Physical counter-maneuvers | Class IIa (Reasonable to Perform) | Level B |
| Rapid supine positioning | ||
| Abdominal binders and elastic stockings | ||
| Squatting | ||
| Leg crossing and large muscle contraction | ||
| Physical exercise | Class IIb (May Be Considered) | Level C |
| Tilt training | ||
| Inpatient tilt training | Class IIb (May Be Considered) | Level B |
| Outpatient tilt training | Class III (No Benefit) | Level B |
Non-Pharmacological Treatment of vasovagal syncope
Education
A wide range of non-pharmacologic approaches are beneficial for the treatment of vasovagal syncope (Table 2). Education, in particular, is a quite helpful and necessary initial strategy 10. It is common for patients to fear that they are at an increased risk of having a myocardial infarction (heart attack) of even dying when suffering from vasovagal syncope. An initial priority is to make sure the patient is aware that vasovagal syncope is not a fatal illness 11. Especially in younger patients, vasovagal syncope almost always follows a benign course. An observational study noted that mortality in non-cardiovascular syncope patients age 60 years or older was 5 times higher than for patients younger than age 60 years, likely explained by comorbid disease 12. Along with reassurance, doctors recommend patient education focused on cause, management, natural history, maintaining appropriate hydration, and avoiding potential triggers. There are a wide range of stimuli that can trigger vasovagal episodes. Physical triggers, including prolonged standing or upright sitting, exposure to high temperatures, dehydration, coughing, and physical pain can be causative. Likewise, emotional triggers such as watching medical procedures, seeing or thinking about blood, and the sudden onset of extreme emotions, can be effective triggers.
Medical alert bracelets can also be useful. Depending on the frequency of vasovagal syncope episodes, patients may have repeatedly been taken to the Emergency Department (ED) and have been subjected to expensive and unnecessary testing for other causes of syncope. With the simple addition of a bracelet, patients may be able to avoid recurring and unnecessary Emergency Department visits.
Fluid and Salt Intake
The initial treatment approach for vasovagal syncope is to increase dietary intake of salt and water. Venous pooling reduces ventricular preload during a vasovagal syncope episode. A small, double-blinded, placebo-controlled study showed that intake of salt and water expands intravascular volume 13, potentially increasing venous return during an episode. This recommendation, along with general education, is thought to result in significant improvement in the vast majority of patients with vasovagal syncope. Despite almost universal use of this strategy, there is limited evidence in support of increased water and salt intake. Increased hydration improved orthostatic symptoms for short periods of time in a prospective randomized open study, but did not improve intolerance overall 14. This strategy can also be significantly limited by co-existing hypertension, heart failure, or renal failure 13. If not medically contraindicated, we recommend hydration with at least 2 liters of fluid a day. Augmented salt intake can be achieved through an increase in dietary salt intake or the use of NaCl (salt) tablets in patients who do not like the taste of salt.
A recent large observational study showed a significant decrease in syncope burden and traumatic syncope burden with a standardized education protocol 15. Patients were first informed about the benign nature of the condition, received information about the pathophysiology and probable triggers for the condition, were taught how to avoid potentially triggering situations, and were given motivation to drink at least 2 liters of water per day and to start regular physical activities. They were also taught to use isometric counter-pressure maneuvers and to adopt supine positions with lightheadedness or other symptoms. Education significantly reduced traumatic injuries and syncope recurrences in vasovagal syncope patients.
Removing Offending Agents
Any medications that could potentially worsen symptoms should be removed if possible. Common agents that could worsen symptoms include diuretics (decreased preload), venodilators (decreased preload), and vasodilators (decreased afterload). Removing these medications can be extremely helpful in reducing episodes.
Psychological and Emotional Distress
Emotional distress is common in vasovagal syncope and can be an extremely debilitating symptom for patients. Repeated episodes of syncope can lead to anxiety over possible injury, negative social consequences, or even dying. This can be quite distressing. Anxiety and psychosocial issues commonly related to recurrent vasovagal syncope predicted non-response to other therapies for vasovagal syncope in a prospective cohort study 16. Emotional distress can result from vasovagal syncope and also be a trigger for vasovagal syncope. In patients that suffer from significant anxiety or negative emotional states around their syncope, this should also be a target of therapy. This could involve a selective serotonin reuptake inhibitor, psychotherapy, or both.
Exercise Training
Once education and initial attempts to increase intravascular volume have been attempted, there are a wide range of physical treatment strategies and maneuvers that can help to improve vasovagal syncope treatment. Exercise training was initially widely used after it was shown to increase blood volume and improve baroreceptor function in 2 observational studies on vasovagal syncope patients 17. Patients in exercise studies would do both aerobic exercises as well as core strengthening exercises. Despite the physiologic findings, there are only weak data for this exercise strategy actually preventing syncope 17. Despite the lack of clear evidence of efficacy, exercise is often recommended in the treatment of vasovagal syncope.
Physical Countermeasures
Doctors recommend that their patients with vasovagal syncope lie down as quickly as possible after the onset of the vasovagal syncope prodrome. Despite the lack of trial data, clinical experience has shown this strategy highly effective at preventing injury from syncope and preventing an episode leading to frank syncope.
Isometric muscle contractions have been shown to increase cardiac output and arterial blood pressure (BP) while decreasing syncope occurrence in both non-randomized and randomized trials 18. The most effective maneuver combines leg crossing and buttocks clenching, but improvement can also occur with arm contractions (arm contractions may be preferred by patients for use due to ease and to avoid embarrassment in public situations). It is important to educate patients to avoid performing a simultaneous Valsalva maneuver, which could accelerate syncope by decreasing venous return. One way for the patient to avoid performing an accidental Valsalva maneuver is for them to ensure that they can talk while performing the muscle-tensing maneuver. These maneuvers are easy to learn, free of cost and significant side effects, and have a well-understood physiologic basis that both patients and physicians can easily understand. A limitation of muscle contraction strategies is that an adequate prodrome is required in order to allow a conscious patient to actually perform the maneuvers.
The Physical Counterpressure Manoeuvres Trial 18 addressed the use of these maneuvers in a multicenter, prospective, randomized controlled trial of the addition of these maneuvers to conventional therapy in affected patients. The study randomized 223 patients with recurrent vasovagal syncope, and treatment arm patients were taught several counterpressure techniques and advised to hold a chosen maneuver for the maximum tolerated time or until symptoms disappeared. There was a 36% relative risk reduction for syncope (among the largest seen in any randomized controlled trial for any type of vasovagal syncope therapy) over an average of 14 months of follow-up. A limitation was that 35% of patients did not have a prodrome that was long enough to see a significant benefit.
Tilt Training
“Tilt training”, or recurrent exposure to tilt testing maneuvers, was developed after the observation that repeated tilt testing was associated with a decrease in positive results of later tilt testing. This led to the hypothesis that repeated tilt testing could increase peripheral sympathetic function. One trial repeated daily tilt tests with patients remaining in the hospital until the patient could tolerate the entire duration of the tilt table test, which could take several days 19. Prolonged inpatient hospital stays are increasingly hard to justify, so multiple studies have evaluated outpatient training (standing against a wall for 30 minutes [or until presyncopal symptoms began] x1–2 times per day), which have shown mixed results. While a randomized Chinese trial did suggest a benefit with outpatient tilt training, the majority of trials reported no significant effect 20. A recent observational registry trial suggested modest benefit, but only recommended outpatient tilt training in young patients with refractory vasovagal syncope 21. The efficacy of home training may be limited by poor compliance. In a randomized, controlled trial, Foglia-Manzillo et al. 22 found that only 34% of patients performed all of the prescribed sessions, even with a short follow-up period. Given the concerns about modest efficacy and poor compliance, doctors do not routinely advise self-administered tilt training in their practice, and reserve it only for the most motivated vasovagal syncope patients.
Pharmacological Treatment of vasovagal syncope
Pharmacological therapy for vasovagal syncope should be considered in patients in whom non-pharmacologic measures, including education, fluid intake, and physical countermeasures, have failed. Many pharmacological treatments exist for vasovagal syncope, but none has shown significant effectiveness in large, randomized, controlled trials. In spite of this, clinical management of refractory and recurrent vasovagal syncope in well-chosen patients can result in decreased symptom burden.
Beta-blockers
Animal studies have shown beta-receptor involvement in ventricular baroreceptor reflexes, resultant hypotension and bradycardia during isoproterenol-influenced tilt testing 23 and the ability of beta-blockers to block the downstream effects of isoproterenol 24. Based on this data, beta-blockers were widely tested in the treatment of vasovagal syncope. Multiple small non-randomized and prospective randomized trials of mainly beta-1 selective blockers showed mixed results 25. The Prevention of Syncope Trial 26 was a large, randomized, placebo-controlled, double-blinded trial that determined the effectiveness of metoprolol in vasovagal syncope over a 1 year treatment period. Metoprolol provided no overall benefit in “freedom from syncope” over the year when compared to placebo. The hazard ratio for metoprolol in patients ≥42 years of age was 0.53, but in patients <42 years of age, the hazard ratio was 1.62. When combined with a pooled cohort study, these results became more convincing with a hazard ratio of 0.52 in patients ≥42 years of age compared with a ratio of 1.58 for patients <42 years of age 27. These results suggest an age-dependent effect on syncope. This, in combination with beta-blocker therapy’s status as one of the very few pharmacologic treatments that does not increase blood pressure, make beta-blockers a reasonable choice for older vasovagal syncope patients with co-morbid hypertension. The Prevention of Syncope Trial 5 is a current randomized, placebo-controlled, double-blinded study powered to assess whether metoprolol is beneficial in older vasovagal syncope patients (≥40 years).
Another small randomized, double-blinded, tilt-based crossover study by Eldadah et al. 28 suggested that propranolol may be the optimal beta-blocker to use in the treatment of vasovagal syncope. The beta-2 adrenergic blockade might counter the adrenaline-mediated vasodilation at the time of syncope.
Mineralocorticoids
Fludrocortisone is a corticosteroid that has been fluorinated, increasing its selectivity in activating mineralocorticoid receptors. This leads to acute sodium and water retention along with potassium excretion into the urine. The hypothetical mechanism of benefit in vasovagal syncope would be to increase intravascular volume and perhaps decrease the autonomic outflow brought on by triggering situations. Fludrocortisone is considered an addition to dietary salt and water expansion rather than mono-therapy for vasovagal syncope. An early open-label, uncontrolled study showed that children had significantly fewer syncopal and presyncopal episodes while taking fludrocortisone 29. However, a randomized, double-blinded, controlled study actually found more symptoms in children randomized to fludrocortisone than those in the placebo arm 30. The Second Prevention of Syncope Trial 31 examined fludrocortisone in the treatment of adults with vasovagal syncope. The Second Prevention of Syncope Trial 32 was the first randomized, double-blinded, placebo-controlled clinical trial using fludrocortisone. 211 patients were randomized to either placebo or fludrocortisone for 1 year. There was a trend toward benefit with a relative risk reduction of 26%. Likely due to blood pressure constraints, the average age of the subjects skewed toward the young, with a mean age of 30 years and a maximum age of 46 years. Given this trend toward significance, doctors continue to utilize fludrocortisone in younger vasovagal syncope patients. Hypertension can limit the use of fludrocortisone, especially in older vasovagal syncope patients.
Selective Serotonin Reuptake Inhibitors
Serotonin is a neurotransmitter that is known to affect BP and heart rate via modulation of the central nervous system. Selective serotonin reuptake inhibitors (SSRIs) are known to cause postsynaptic serotonin receptor down-regulation in the brain stem. This down-regulation in receptor density could potentially blunt a sympathetic withdrawal response to rapid increases in serotonin levels. Several studies have attempted to use SSRIs in the treatment of vasovagal syncope. A randomized, double-blinded, placebo-controlled study of paroxetine in patients with recurrent vasovagal syncope showed a reduction in syncope recurrence over 2 years from 53% with placebo to 18% with paroxetine 33. In contrast, Theodorakis et al. performed a randomized, placebo-controlled, double-blinded trial of fluoxetine (a different SSRI) and found that it was no more effective than placebo for the prevention of vasovagal syncope 25. Overall, the literature does not convincingly show selective serotonin reuptake inhibitors (SSRIs) to be effective in preventing vasovagal syncope symptoms.
Alpha-1 Agonists
Midodrine has been used to affect peripheral alpha-1 adrenergic activity via its active metabolite, which is an agonist at alpha-1 receptors. It is known to cause arteriolar constriction as well as venoconstriction, which increases peripheral vascular resistance and cardiac output. Trial data has shown that in the majority of patients with vasovagal syncope, a moderate fall in cardiac output with coincident vasodilatation occurs during a syncopal event 34. A number of clinical studies have reported promising evidence for using midodrine to prevent vasovagal syncope 35, but they are not conclusive and are accompanied by a negative study 36. The ongoing Prevention of Syncope Trial IV 37, a randomized, placebo-controlled, double-blinded study, is assessing midodrine vs. placebo in patients with frequent syncopal episodes, with results expected in 2017. Midodrine is generally well-tolerated at low doses, and remains a reasonable option in patients without significant hypertension. At higher doses, there are a number of potential side effects including supine hypertension, nausea, piloerection, urinary retention, rash, and scalp paresthesias that generally resolve with dose decrease. The frequency of dosing and compliance challenges, the necessity to avoid bedtime dosing, and the side effect profile may limit midodrine’s utility in older vasovagal syncope patients. In addition, midodrine is not available over much of Europe, and a trial on etilefrine (similar to midodrine) was negative 38.
Norepinephrine Transporter Inhibitors
Norepinephrine transporter 39 inhibitors block reuptake of norepinephrine at sympathetic neuronal pre-synaptic terminals. This can lead to an increase in sympathetic tone in situations where norepinephrine is released, such as during orthostatic stress. This could block the triggering of the vasovagal reflex, as well as prevent the subsequent loss of sympathetic tone. Sheldon et al. recently performed a proof of concept test using sibutramine in a prospective dose-ranging study in the most extremely symptomatic and treatment-refractory patients. Out of 7 patients, 5 had significantly decreased syncopal spell frequency 40. While more research is needed, norepinephrine transporter inhibitors may represent a promising treatment for treatment-refractory vasovagal syncope patients.
Other Medications
There are several other medications that have been reported to have been used in the management of vasovagal syncope, but are not used in our practice. Disopyramide is a sodium channel blocker with prominent anticholinergic effects on the heart. This could potentially modify the cardioinhibitory reflex seen in a vasovagal reaction and reduce vasovagal syncope symptoms. Unfortunately, 2 studies of disopyramide have shown no significant benefit over placebo, and extracardiac anticholinergic side-effects (including dry mouth, constipation, urinary retention, or even agranulocytosis) can often limit the use of disopyramide. In occasional patients, disopyramide can have life-threatening proarrhythmic effects.
Yohimbine is an alpha-2 receptor antagonist (the opposite of clonidine). By blocking the negative feedback alpha-2 receptor, yohimbine can increase sympathoneural tone. Yohimbine has been shown to be effective at preventing tilt-test-induced syncope in a prospective proof of concept study 41, but clinical syncope data is lacking. Tolerance of yohimbine can be limited due to its symptomatic sympathetic activation, and it is no longer manufactured, so it is available only through compounding pharmacies.
- Moya A, Sutton R, Ammirati F, Blanc JJ, Brignole M, Dahm JB, Deharo JC, Gajek J, Gjesdal K, Krahn A, Massin M, Pepi M, Pezawas T, Ruiz Granell R, Sarasin F, Ungar A, van Dijk JG, Walma EP, Wieling W. Guidelines for the diagnosis and management of syncope (version 2009). Eur Heart J. 2009;30:2631–2671 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3295536/[↩][↩]
- Management of vasovagal syncope: 2004. Sheldon R, Morillo C, Krahn A. Expert Rev Cardiovasc Ther. 2004 Nov; 2(6):915-23. https://www.ncbi.nlm.nih.gov/pubmed/15500436/[↩]
- Cardiac output and vasodilation in the vasovagal response: An analysis of the classic papers. Wieling W, Jardine DL, de Lange FJ, Brignole M, Nielsen HB, Stewart J, Sutton R. Heart Rhythm. 2016 Mar; 13(3):798-805. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5234327/[↩]
- Incidence and prognosis of syncope. Soteriades ES, Evans JC, Larson MG, Chen MH, Chen L, Benjamin EJ, Levy D. N Engl J Med. 2002 Sep 19; 347(12):878-85. http://www.nejm.org/doi/10.1056/NEJMoa012407[↩]
- Physical injuries caused by a transient loss of consciousness: main clinical characteristics of patients and diagnostic contribution of carotid sinus massage. Bartoletti A, Fabiani P, Bagnoli L, Cappelletti C, Cappellini M, Nappini G, Gianni R, Lavacchi A, Santoro GM. Eur Heart J. 2008 Mar; 29(5):618-24. https://www.ncbi.nlm.nih.gov/pubmed/18086659/[↩]
- Muppa P, Sheldon RS, McRae M, et al. Gynecological and Menstrual Disorders in Women with Vasovagal Syncope. Clinical autonomic research : official journal of the Clinical Autonomic Research Society. 2013;23(3):117-122. doi:10.1007/s10286-013-0190-1. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3681885/[↩][↩][↩]
- Raj SR, Coffin ST. Medical Therapy and Physical Maneuvers in the Treatment of the Vasovagal Syncope and Orthostatic Hypotension. Progress in cardiovascular diseases. 2013;55(4):425-433. doi:10.1016/j.pcad.2012.11.004. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3594734/[↩]
- Medical therapy and physical maneuvers in the treatment of the vasovagal syncope and orthostatic hypotension. Raj SR, Coffin ST. Prog Cardiovasc Dis. 2013 Jan-Feb; 55(4):425-33. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3594734/[↩]
- Gibbons RJ, Smith S, Antman E. American College of Cardiology/American Heart Association clinical practice guidelines: Part I: where do they come from? Circulation. 2003;107:2979–2986. http://circ.ahajournals.org/content/107/23/2979.long[↩][↩]
- White WD, Sheldon RS, Ritchie DA. Learning needs of patients with vasovagal syncope. Can J Cardiovasc Nurs. 2003;13:26–30. https://www.ncbi.nlm.nih.gov/pubmed/12703103[↩]
- Soteriades ES, Evans JC, Larson MG, Chen MH, Chen L, Benjamin EJ, et al. Incidence and prognosis of syncope. N Engl J Med. 2002;347:878–885 http://www.nejm.org/doi/10.1056/NEJMoa012407[↩]
- Kapoor W, Snustad D, Peterson J, Wieand HS, Cha R, Karpf M. Syncope in the elderly. Am J Med. 1986;80:419–428. https://www.ncbi.nlm.nih.gov/pubmed/3953619[↩]
- El-Sayed H, Hainsworth R. Salt supplement increases plasma volume and orthostatic tolerance in patients with unexplained syncope. Heart. 1996;75:134–140 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC484248/[↩][↩]
- Bellard E, Fortrat JO, Custaud MA, Victor J, Greenleaf J, Leftheriotis G. Increased hydration alone does not improve orthostatic tolerance in patients with neurocardiogenic syncope. Clin Auton Res. 2007;17:99–105 https://www.ncbi.nlm.nih.gov/pubmed/17464552[↩]
- Aydin MA, Mortensen K, Salukhe TV, Wilke I, Ortak M, Drewitz I, et al. A standardized education protocol significantly reduces traumatic injuries and syncope recurrence: an observational study in 316 patients with vasovagal syncope. Europace. 2012;14:410–415 https://www.ncbi.nlm.nih.gov/pubmed/22048993[↩]
- Flint B, Baker C, Freeston M, Newton JL. Level of psychosocial impairment predicts early response to treatment in vasovagal syncope. Europace. 2009;11:231–236. https://www.ncbi.nlm.nih.gov/pubmed/19059994[↩]
- Gardenghi G, Rondon MU, Braga AM, Scanavacca MI, Negrao CE, Sosa E, et al. The effects of exercise training on arterial baroreflex sensitivity in neurally mediated syncope patients. Eur Heart J. 2007;28:2749–2755. https://www.ncbi.nlm.nih.gov/pubmed/17561494[↩][↩]
- van Dijk N, Quartieri F, Blanc JJ, Garcia-Civera R, Brignole M, Moya A, et al. Effectiveness of physical counterpressure maneuvers in preventing vasovagal syncope: the Physical Counterpressure Manoeuvres Trial (PC-Trial) J Am Coll Cardiol. 2006;48:1652–1657 https://www.ncbi.nlm.nih.gov/pubmed/17045903[↩][↩]
- Ector H, Willems R, Heidbuchel H, Reybrouck T. Repeated tilt testing in patients with tilt-positive neurally mediated syncope. Europace. 2005;7:628–633 https://www.ncbi.nlm.nih.gov/pubmed/16216768[↩]
- Tan MP, Newton JL, Chadwick TJ, Gray JC, Nath S, Parry SW. Home orthostatic training in vasovagal syncope modifies autonomic tone: results of a randomized, placebo-controlled pilot study. Europace. 2010;12:240–246. https://www.ncbi.nlm.nih.gov/pubmed/19919966[↩]
- Jang WJ, Yim HR, Lee SH, Park SJ, Kim JS, On YK. Prognosis after tilt training in patients with recurrent vasovagal syncope. Int J Cardiol. 2013;168:4264–4265 https://www.ncbi.nlm.nih.gov/pubmed/23642601[↩]
- Foglia-Manzillo G, Giada F, Gaggioli G, Bartoletti A, Lolli G, Dinelli M, et al. Efficacy of tilt training in the treatment of neurally mediated syncope. A randomized study. Europace. 2004;6:199–204. https://www.ncbi.nlm.nih.gov/pubmed/15121070[↩]
- Sheldon R, Killam S. Methodology of isoproterenol-tilt table testing in patients with syncope. J Am Coll Cardiol. 1992;19:773–779. https://www.ncbi.nlm.nih.gov/pubmed/1545073[↩]
- Sra JS, Murthy VS, Jazayeri MR, Shen YH, Troup PJ, Avitall B, et al. Use of intravenous esmolol to predict efficacy of oral beta-adrenergic blocker therapy in patients with neurocardiogenic syncope. J Am Coll Cardiol. 1992;19:402–408 https://www.ncbi.nlm.nih.gov/pubmed/1346266[↩]
- Theodorakis GN, Leftheriotis D, Livanis EG, Flevari P, Karabela G, Aggelopoulou N, et al. Fluoxetine vs. propranolol in the treatment of vasovagal syncope: a prospective, randomized, placebo-controlled study. Europace. 2006;(8):193–198 https://www.ncbi.nlm.nih.gov/pubmed/16627439[↩][↩]
- Sheldon R, Connolly S, Rose S, Klingenheben T, Krahn A, Morillo C, et al. Prevention of Syncope Trial (POST): a randomized, placebo-controlled study of metoprolol in the prevention of vasovagal syncope. Circulation. 2006;113:1164–1170 http://circ.ahajournals.org/content/113/9/1164.long[↩]
- Sheldon RS, Morillo CA, Klingenheben T, Krahn AD, Sheldon A, Rose MS. Age-dependent effect of beta-blockers in preventing vasovagal syncope. Circ Arrhythm Electrophysiol. 2012;5:920–926. http://circep.ahajournals.org/content/5/5/920.long[↩]
- Eldadah BA, Pechnik SL, Holmes CS, Moak JP, Saleem AM, Goldstein DS. Failure of propranolol to prevent tilt-evoked systemic vasodilatation, adrenaline release and neurocardiogenic syncope. Clin Sci (Lond) 2006;111:209–216. https://www.ncbi.nlm.nih.gov/pubmed/16634720[↩]
- Scott WA, Pongiglione G, Bromberg BI, Schaffer MS, Deal BJ, Fish FA, et al. Randomized comparison of atenolol and fludrocortisone acetate in the treatment of pediatric neurally mediated syncope. Am J Cardiol. 1995;76:400–402. https://www.ncbi.nlm.nih.gov/pubmed/7639169[↩]
- Salim MA, Di Sessa TG. Effectiveness of fludrocortisone and salt in preventing syncope recurrence in children: a double-blind, placebo-controlled, randomized trial. J Am Coll Cardiol. 2005;45:484–488 https://www.ncbi.nlm.nih.gov/pubmed/15708690[↩]
- Raj SR, Rose S, Ritchie D, Sheldon RS. The Second Prevention of Syncope Trial (POST II)–a randomized clinical trial of fludrocortisone for the prevention of neurally mediated syncope: rationale and study design. Am Heart J. 2006;151:1186–1187 https://www.ncbi.nlm.nih.gov/pubmed/16781217[↩]
- Sheldon R, Morillo C, Krahn A, Medina E, Talajic M, Kus T, et al. A randomized clinical trial of fludrocortisone for the prevention of vasovagal syncope (POST2) Can J Cardiol. 2011;27(5):S335–S336.[↩]
- Di Girolamo E, Di IC, Sabatini P, Leonzio L, Barbone C, Barsotti A. Effects of paroxetine hydrochloride, a selective serotonin reuptake inhibitor, on refractory vasovagal syncope: a randomized, double-blind, placebo-controlled study. J Am Coll Cardiol. 1999;33:1227–1230. https://www.ncbi.nlm.nih.gov/pubmed/10193720[↩]
- Fu Q, Verheyden B, Wieling W, Levine BD. Cardiac output and sympathetic vasoconstrictor responses during upright tilt to presyncope in healthy humans. J Physiol. 2012;590:1839–1848. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3573307/[↩]
- Qingyou Z, Junbao D, Chaoshu T. The efficacy of midodrine hydrochloride in the treatment of children with vasovagal syncope. J Pediatr. 2006;149:777–780 https://www.ncbi.nlm.nih.gov/pubmed/17137891[↩]
- Romme JJ, van DN, Go-Schon IK, Reitsma JB, Wieling W. Effectiveness of midodrine treatment in patients with recurrent vasovagal syncope not responding to non-pharmacological treatment (STAND-trial) Europace. 2011;13:1639–1647. https://www.ncbi.nlm.nih.gov/pubmed/21752826[↩]
- Raj SR, Faris PD, McRae M, Sheldon RS. Rationale for the prevention of syncope trial IV: assessment of midodrine. Clin Auton Res. 2012;22:275–280 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3439533/[↩]
- Raviele A, Brignole M, Sutton R, Alboni P, Giani P, Menozzi C, et al. Effect of etilefrine in preventing syncopal recurrence in patients with vasovagal syncope: a double-blind, randomized, placebo-controlled trial. The Vasovagal Syncope International Study. Circulation. 1999;99:1452–1457 http://circ.ahajournals.org/content/99/11/1452.long[↩]
- Lechin F, van der Dijs B, Hernandez G, Orozco B, Rodriguez S, Baez S. Neurochemical, neuroautonomic and neuropharmacological acute effects of sibutramine in healthy subjects. Neurotoxicology. 2006;27:184–191 https://www.ncbi.nlm.nih.gov/pubmed/16269176[↩]
- Sheldon RS, Ritchie D, McRae M, Raj S. Norepinephrine transport inhibition for treatment of vasovagal syncope. J Cardiovasc Electrophysiol. 2013;24:799–803 https://www.ncbi.nlm.nih.gov/pubmed/23444896[↩]
- Mosqueda-Garcia R, Fernandez-Violante R, Tank J, Snell M, Cunningham G, Furlan R. Yohimbine in neurally mediated syncope. Pathophysiological implications. J Clin Invest. 1998;102:1824–1830. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC509132/[↩]





{kind=link}