
What are voice disorders
A voice disorder occurs when voice quality, pitch, and loudness differ or are inappropriate for an individual’s age, gender, cultural background, or geographic location 1. A voice disorder is present when an individual expresses concern about having an abnormal voice that does not meet daily needs—even if others do not perceive it as different or deviant 2.
Voice disorders occur with a change in the voice, often described as hoarseness, roughness, or a raspy quality. People with voice disorders often complain about or notice changes in pitch, loss of voice, loss of endurance, and sometimes a sharp or dull pain associated with voice use. Other voice disorders may accompany a change in singing ability that is most notable in the upper singing range. A more serious problem is indicated by spitting up blood or when blood is present in the mucus. These require prompt attention by an otolaryngologist (ear, nose and throat specialist).
Signs that your voice isn’t healthy include:
- Your voice has become hoarse or raspy
- You’ve lost the ability to hit some high notes when singing
- Your voice suddenly sounds deeper
- Your throat often feels raw, achy, or strained
- It’s become an effort to talk
Ask yourself the following questions to determine if you have an unhealthy voice:
- Has your voice become hoarse or raspy?
- Does your throat often feel raw, achy, or strained?
- Does talking require more effort?
- Do you find yourself repeatedly clearing your throat?
- Do people regularly ask you if you have a cold when in fact you do not?
- Have you lost your ability to hit some high notes when singing?
Voice changes sometimes follow an upper respiratory infection lasting up to two weeks. Typically the upper respiratory infection or cold causes swelling of the vocal cords and changes their vibration resulting in an abnormal voice. Reduced voice use (voice rest) typically improves the voice after an upper respiratory infection, cold, or bronchitis. If voice does not return to its normal characteristics and capabilities within two to four weeks after a cold, a medical evaluation by an ear, nose, and throat specialist is recommended. A throat examination after a change in the voice lasting longer than one month is especially important for smokers. (Note: A change in voice is one of the first and most important symptoms of throat cancer. Early detection significantly increases the effectiveness of treatment.)
Voice disorders have been estimated to be present in between 3% and 9% of the U.S. population 3. However, information from a large U.S. claims database 4 indicates the point prevalence (i.e., the number of individuals with the condition in the database at the time that data were retrieved) of voice disorders is 0.98% in a treatment-seeking population. This likely suggests that a large number of those individuals with voice disorders do not seek treatment.
The prevalence of voice disorders among treatment-seeking individuals has been shown to be affected by gender, age, and occupation 4.
Gender
- Prevalence is higher in adult females than in adult males, with a reported ratio of 1.5:1.0 5.
- In children, voice disorders are significantly more prevalent in males than in females 5.
Age
- Prevalence has been reported to be higher in elderly adults 4, with estimates ranging from 4.8% to 29.1% in population-based studies (de Araújo Pernambuco, Espelt, Balata, & de Lima, 2014).
- In the pediatric population, the reported prevalence of a voice disorder has ranged from 1.4% to 6.0% 6.
Occupation
- Occupational groups that appear to be most at risk for developing a voice disorder include teachers, manufacturing/factory workers, salespersons, and singers 4.
- The estimated prevalence of reporting a current voice problem was higher in teachers (11.0%) than in nonteachers (6.2%) 7.
- Reported prevalence for teachers at a single point in time ranged from 9% to 37% 8. Reported lifetime prevalence (i.e., the percentage of teachers who experienced a voice disorder at some point in their lifetime) was between 50% and 80% 8.
Sound Production
Voice is the sound made by vibration of the vocal cords caused by air passing out through the larynx bringing the cords closer together. Air forced between the adducted vocal cords vibrates them, producing a high-pitched sound when the cords are relatively taut and a lower pitched sound when they are more slack. Children have slender, short vocal folds, so their voices are high-pitched. At puberty the larynx of a male enlarges more than that of a female. In adult males, the vocal cords are usually longer and thicker, vibrate more slowly, and produce lower-pitched sounds than in females. Loudness is determined by the force of the air passing between the vocal cords.
Although the vocal cords alone produce sound, they do not produce intelligible speech; some anatomists have likened their sound to a hunter’s duck call. Amplification and echoing of the sound occur within the pharynx, oral cavity, nasal cavity, and paranasal sinuses. The crude sounds from the larynx are formed into words by actions of the pharynx, oral cavity, voluntary movements of the tongue, and lips.
Figure 1. Larynx and pharynx anatomy
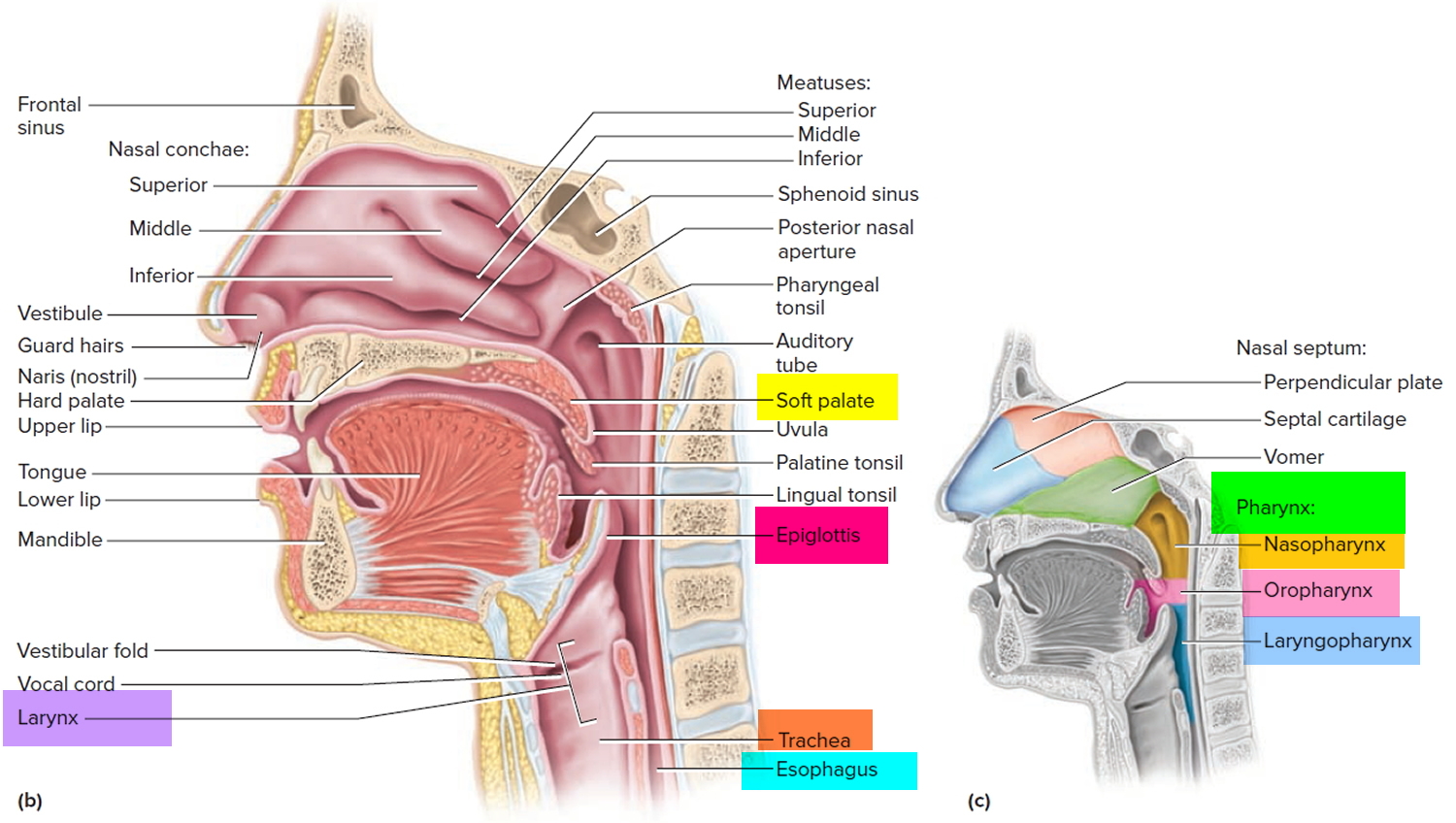
Figure 2. Larynx anatomy
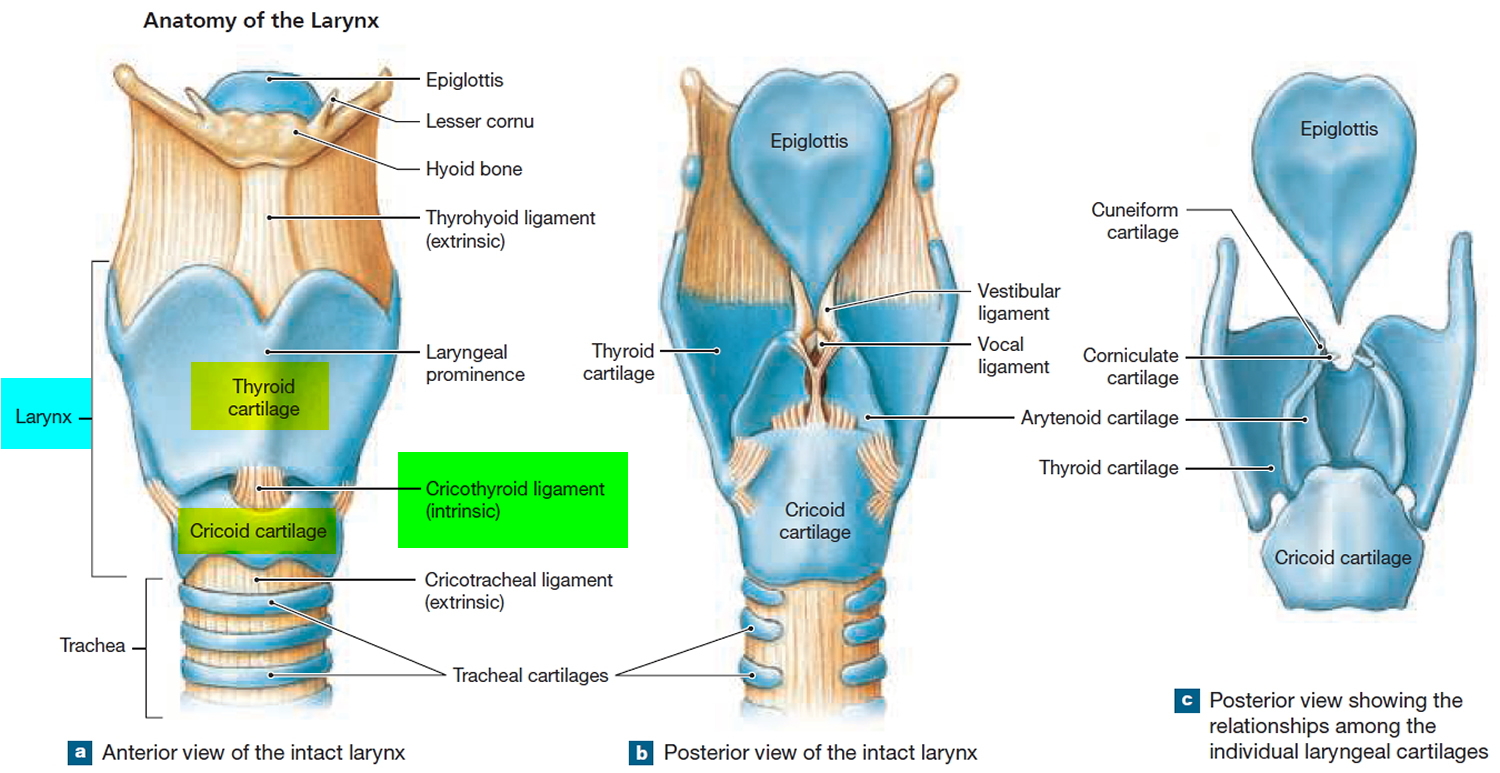
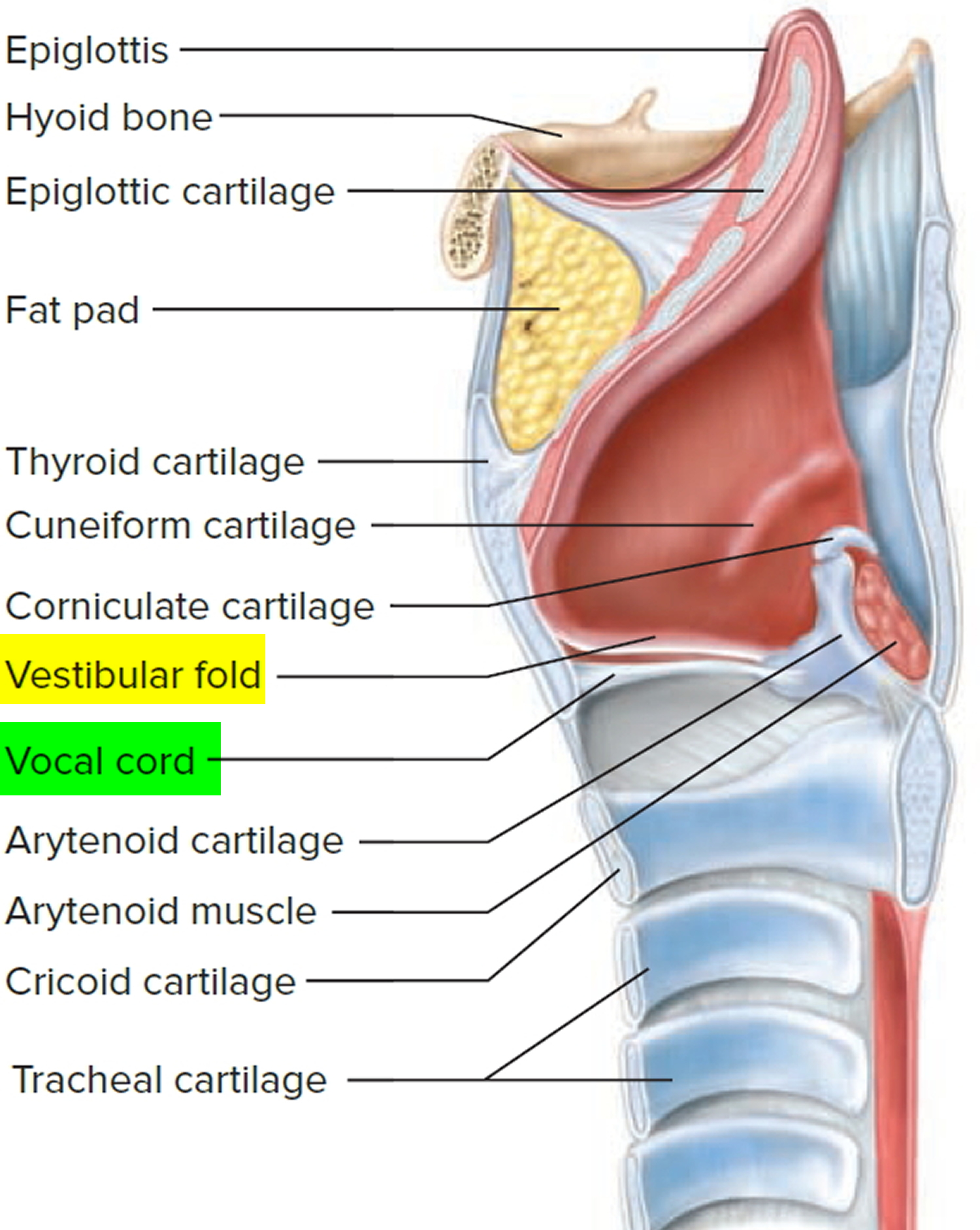
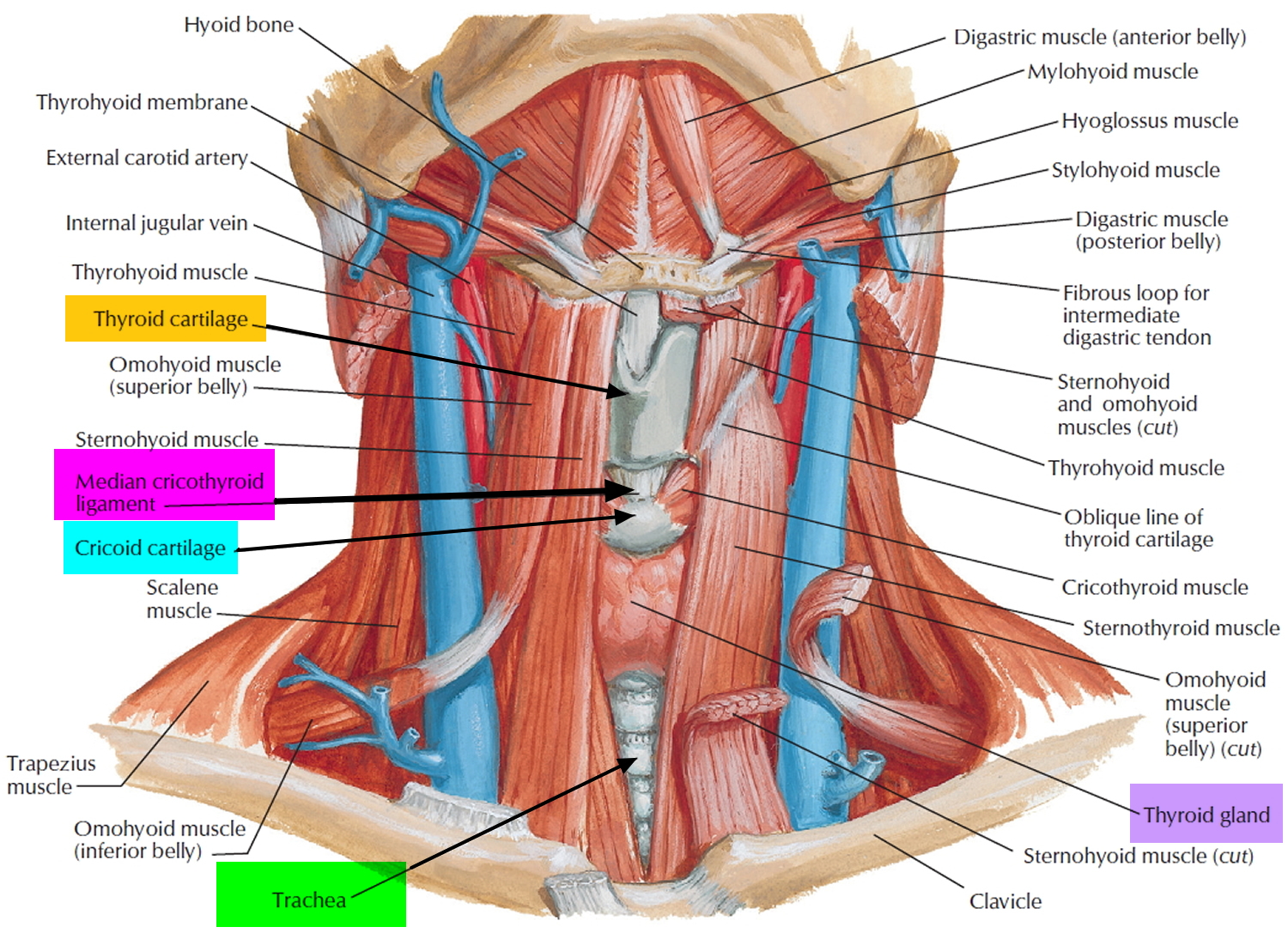
Figure 3. Cricothyroid ligament (cricovocal membrane, cricothyroid membrane)
Types of voice disorders
A number of different systems are used for classifying voice disorders. Voice disorders are categorized by ASHA 9 as follows:
- Organic voice disorders that are physiological in nature and result from alterations in respiratory, laryngeal, or vocal tract mechanisms
- Structural — organic voice disorders that result from physical changes in the voice mechanism (e.g., alterations in vocal fold tissues such as edema or vocal nodules; structural changes in the larynx due to aging)
- Neurogenic — organic voice disorders that result from problems with the central or peripheral nervous system innervation to the larynx that affect functioning of the vocal mechanism (e.g., vocal tremor, spasmodic dysphonia, or paralysis of vocal folds)
- Functional voice disorders that result from improper or inefficient use of the vocal mechanism when the physical structure is normal (e.g., vocal fatigue; muscle tension dysphonia or aphonia; diplophonia; ventricular phonation)
Voice quality can also be affected when psychological stressors lead to habitual, maladaptive aphonia (inability to speak) or dysphonia (altered vocal quality, pitch, loudness, or vocal effort). The resulting voice disorders are referred to as psychogenic voice disorders or psychogenic conversion aphonia/dysphonia 2. These voice disorders are rare. Speech-Language pathologists refer individuals suspected of having a psychogenic voice disorder to other appropriate professionals (e.g., psychologist or psychiatrist) for diagnosis and may collaborate in subsequent treatment.
Voice disorders are not mutually exclusive, and overlap is common. For example, the cause of nodules is functional, as they result from behavioral voice misuse. The voice misuse results in repeated trauma to the vocal folds, which may then lead to structural (organic) changes to the vocal fold tissue.
Speech-language pathologists may also be involved in the assessment and treatment of disorders that affect the voice mechanism (i.e., the aerodigestive tract) but are not classified as voice disorders. An example is paradoxical vocal fold movement, a condition in which there is intermittent adduction of the vocal folds that interferes with breathing. When paradoxical vocal fold movement is suspected, speech-language pathologists are often consulted to help identify abnormal laryngeal and respiratory function and to teach various techniques (e.g., vocal exercises, relaxation techniques, quick-release breathing techniques, and proper breath management) to improve laryngeal and respiratory control 10.
Voice disorders causes
Normal voice production depends on power and airflow supplied by the respiratory system; laryngeal muscle strength, balance, coordination, and stamina; and coordination among these and the supraglottic resonatory structures (pharynx, oral cavity, nasal cavity).
Your voice box (larynx) is made of cartilage, muscle and mucous membranes located at the top of your windpipe (trachea) and the base of your tongue. Sound is created when your vocal cords vibrate.
This vibration comes from air moving through the larynx, bringing your vocal cords closer together. Your vocal cords also help close your voice box when you swallow, preventing you from inhaling food or liquid.
If your vocal cords become inflamed, develop growths or become paralyzed, they can’t work properly, and you may develop a voice disorder.
A disturbance in one of the three subsystems of voice production (i.e., respiratory, laryngeal, and subglottal vocal tract) or in the physiological balance among the systems may lead to a voice disturbance. Disruptions can be due to organic, functional, and/or psychogenic causes.
Some common voice disorders include:
- Laryngitis
- Neurological voice disorders (spasmodic dysphonia)
- Polyps, nodules or cysts on the vocal cords (noncancerous lesions)
- Precancerous and cancerous lesions
- Vocal cord paralysis or weakness
- White patches (leukoplakia)
Organic voice disorders causes
- Structural
- Vocal fold abnormalities (e.g., vocal nodules, edema, glottal stenosis, recurrent respiratory papilloma, sarcopenia [muscle atrophy associated with aging])
- Inflammation of the larynx (e.g., arthritis of the cricoarytenoid or cricothyroid, laryngitis, laryngopharyngeal reflux)
- Trauma to the larynx (e.g., from intubation, chemical exposure, or external trauma)
- Neurologic
- Recurrent laryngeal nerve paralysis
- Adductor/abductor spasmodic dysphonia
- Parkinson’s disease
- Multiple sclerosis
Functional voice disorders causes
- Phonotrauma (e.g., yelling, screaming, excessive throat-clearing)
- Muscle tension dysphonia
- Ventricular phonation
- Vocal fatigue (e.g., due to effort or overuse)
Psychogenic voice disorders causes
- Chronic stress disorders
- Anxiety
- Depression
- Conversion reaction (e.g., conversion aphonia and dysphonia)
The complementary relationships among these organic, functional, and psychogenic influences ensure that many voice disorders will have contributions from more than one etiologic factor 11.
Recognizing associations among these factors, along with patient history, may help in identifying the possible causes of the voice disorder. Even when an obvious cause is identified and treated, the voice problem may persist. For example, an upper respiratory infection could be the cause of the dysphonia, but poor or inefficient compensatory techniques may cause dysphonia to persist, even when the infection has been successfully treated.
The relative proportion of these causes is also affected by gender, age, and occupation 5.
Gender
Although adult females more frequently received diagnoses of dysphonia with no specific cause noted, adult males were more frequently diagnosed with chronic laryngitis 4. Also, after the age of 40 years, males had higher prevalence rates of laryngeal cancer than did females 4.
Age
- Among adults (aged between 19 and 60 years) with a voice disorder, the most frequent diagnoses included functional dysphonia (20.5%), acid laryngitis (12.5%), and vocal polyps (12%) 5.
- Of individuals over the age of 60 years who had been evaluated for vocal problems, voice disorders were most commonly associated with presbyphonia (changes associated with aging voice), reflux/inflammation, functional dysphonia, vocal fold paralysis/paresis, Reinke’s edema, or laryngeal cancer 5.
- Vocal fold nodules were the most frequently diagnosed voice disorder in the pediatric population 5. The prevalence of vocal fold nodules may be as high as 16.9% in school-age children and is approximately twice as high for males than for females 12.
Occupation
In a Dutch treatment-seeking population, the three main pathologies associated with professional voice users (i.e., teachers, performers, telemarketers, broadcasters, salesmen, and tour guides) included functional voice disorders (41%), vocal fold nodules/hypertrophy (15%), and reflux/laryngitis/inflammation (11%) 13.
Many factors can contribute to a voice disorder, including:
- Aging
- Alcohol use
- Allergies
- Gastroesophageal reflux disease (GERD)
- Illnesses, such as colds or upper respiratory infections
- Improper throat clearing over a long time
- Neurological disorders
- Psychological stress
- Scarring from neck surgery or from trauma to the front of the neck
- Screaming
- Smoking
- Throat cancer
- Throat dehydration
- Thyroid problems
- Voice misuse or overuse.
Common Problems That Can Affect Your Voice
The most common causes of hoarseness and vocal difficulties are outlined below. If you become hoarse frequently or notice voice change for an extended period of time, please see your Otolaryngologist (Ear, Nose, and Throat doctor) for an evaluation.
Acute Laryngitis
Acute laryngitis is the most common cause of hoarseness and voice loss that starts suddenly. Most cases of acute laryngitis are caused by a viral infection that leads to swelling of the vocal cords. When the vocal cords swell, they vibrate differently, leading to hoarseness. The best treatment for this condition is to stay well hydrated and to rest or reduce your voice use. Serious injury to the vocal cords can result from strenuous voice use during an episode of acute laryngitis. Since most acute laryngitis is caused by a virus, antibiotics are not effective. Bacterial infections of the larynx are much rarer and often are associated with difficulty breathing. Any problems breathing during an illness warrants emergency evaluation.
Chronic Laryngitis
Chronic laryngitis is a non-specific term and an underlying cause should be identified. Chronic laryngitis can be caused by acid reflux disease, by exposure to irritating substances such as smoke, and by low grade infections such as yeast infections of the vocal cords in people using inhalers for asthma. Chemotherapy patients or others whose immune system is not working well can get these infections too.
Laryngopharyngeal Reflux Disease
Reflux of stomach juice into the throat can cause a variety of symptoms in the esophagus (swallowing tube) as well as in the throat. Hoarseness (chronic or intermittent), swallowing problems, a lump in the throat sensation, or throat pain are common symptoms of stomach acid irritation of the throat. Please be aware that Laryngopharyngeal Reflux Disease can occur without any symptoms of frank heartburn and regurgitation that traditionally accompany gastro esophageal reflux disease (GERD).
Voice Misuse and Overuse
Speaking is a physical task that requires coordination of breathing with the use of several muscle groups. It should come as no surprise that, just like in any other physical task, there are efficient and inefficient ways of using your voice. Excessively loud, prolonged, and/or inefficient voice use can lead to vocal difficulties, just like improper lifting can lead to back injuries. Excessive tensionin the neck and laryngeal muscles, along with poor breathing technique during speech leads to vocal fatigue, increased vocal effort, and hoarseness. Voice misuse and overuse puts you at risk for developing benign vocal cord lesions (see below) or a vocal cord hemorrhage.
Common situations that are associated with voice misuse:
- Speaking in noisy situations
- Excessive cellular phone use
- Telephone use with the handset cradled to the shoulder
- Using inappropriate pitch (too high or too low) when speaking
- Not using amplification when publicly speaking
Benign Vocal Cord Lesions
Benign non-cancerous growths on the vocal cords are most often caused by voice misuse or overuse, which causes trauma to the vocal cords. These lesions (or bumps) on the vocal cord(s) alter vocal cord vibration and lead to hoarseness. The most common vocal cord lesions are nodules, polyps, and cysts. Vocal nodules (also known as nodes or singers nodes) are similar to calluses of the vocal cords. They occur on both vocal cords opposite each other at the point of maximal wear and tear, and are usually treated with voice therapy to eliminate the vocal trauma that is causing them. Contrary to common myth, vocal nodules are highly treatable and intervention leads to improvement in most cases. Vocal cord polyps and cysts are the other common benign lesions. These are sometimes related to voice misuse or overuse, but can also occur in people who dont use their voice improperly. These types of problems typically require microsurgical treatment for cure, with voice therapy employed in a combined treatment approach in some cases.
Vocal Cord Hemorrhage
If you experience sudden loss of voice following yelling, shouting, or other strenuous vocal tasks, you may have developed a vocal cord hemorrhage. Vocal cord hemorrhage results when one of the blood vessels on the surface of the vocal cord ruptures and the soft tissues of the vocal cord fill with blood. It is considered a vocal emergency and is treated with absolute voice rest until the hemorrhage resolves. If you lose your voice after strenuous voice use, see your Otolaryngologist as soon as possible.
Vocal Cord Paralysis and Paresis
Hoarseness and other problems can occur related to problems between the nerves and muscles within the voice box or larynx. The most common neurological condition that affects the larynx is a paralysis or weakness of one or both vocal cords. Involvement of both vocal cords is rareand is usually manifested by noisy breathing or difficulty getting enough air while breathing or talking. When one vocal cord is paralyzed or weak, voice is usually the problem rather than breathing. One vocal cord can become paralyzed or weakened (paresis) from a viral infection of the throat, after surgery in the neck or chest, from a tumor or growth along the laryngeal nerves, or for unknown reasons. Vocal cord paralysis typically presents with a soft and breathy voice. Many cases of vocal cord paralysis will recover within several months. In some cases however, the paralysis will be permanent, and may require active treatment to improve the voice. Treatment choice depends on the nature of the vocal cord paralysis, the degree of vocal impairment, and the patients vocal needs. While we are not able to make paralyzed vocal cords move again, there are good treatment options for improving the voice. One option includes surgery for unilateral vocal cord paralysis that repositions the vocal cord to improve contact and vibration of the paralyzed vocal cord with the non-paralyzed vocal cord. There are a variety of surgical techniques used to accomplish this. Voice therapy may be used before or after surgical treatment of the paralyzed vocal cords, or it can also be used as the sole treatment.
Laryngeal Cancer
Throat cancer is a very serious condition requiring immediate medical attention. Chronic hoarseness warrants evaluation by an otolaryngologist to rule out laryngeal cancer. It is important to remember that prompt attention to changes in the voice facilitate early diagnosis. Remember to listen to your voice because it might be telling you something. Laryngeal cancer is highly curable if diagnosed in its early stages.
Voice disorders signs and symptoms
The generic term dysphonia encompasses the auditory-perceptual symptoms of voice disorders. Dysphonia is characterized by altered vocal quality, pitch, loudness, or vocal effort.
Signs and symptoms of dysphonia include:
- roughness (perception of aberrant vocal fold vibration);
- breathiness (perception of audible air escape in the sound signal or bursts of breathiness);
- strained quality (perception of increased effort; tense or harsh as if talking and lifting at the same time);
- strangled quality (as if talking with breath held);
- abnormal pitch (too high, too low, pitch breaks, decreased pitch range);
- abnormal loudness/volume (too high, too low, decreased range, unsteady volume);
- abnormal resonance (hypernasal, hyponasal, cul de sac resonance);
- aphonia (loss of voice);
- phonation breaks;
- asthenia (weak voice);
- gurgly/wet sounding voice;
- hoarse voice (raspy, audible aperiodicity in sound);
- pulsed voice (fry register, audible creaks or pulses in sound);
- shrill voice (high, piercing sound, as if stifling a scream); and
- tremulous voice (shaky voice; rhythmic pitch and loudness undulations).
Other signs and symptoms include:
- increased vocal effort associated with speaking;
- decreased vocal endurance or onset of fatigue with prolonged voice use;
- variable vocal quality throughout the day or during speaking;
- running out of breath quickly;
- frequent coughing or throat clearing (may worsen with increased voice use); and
- excessive throat or laryngeal tension/pain/tenderness.
Signs and symptoms can occur in isolation or in combination. As treatment progresses, some may dissipate, and others may emerge as compensatory strategies are eliminated.
Auditory-perceptual quality of voice in individuals with voice disorders can vary depending on the type and severity of disorder, the size and site of lesion (if present), and the individual’s compensatory responses. The severity of the voice disorder cannot always be determined by auditory-perceptual voice quality alone.
Voice disorders diagnosis
Your doctor and/or a speech-language pathologist will ask you detailed questions about your voice problems and examine you thoroughly. A topical anesthetic may be applied to numb your tissues before your doctor uses one of the following tools to examine your vocal cords:
- Mirror. Similar to a dental mirror, a long, rigid instrument with an angled mirror is inserted into your mouth.
- Flexible laryngoscope. A flexible tube containing a light and camera is inserted through your nose.
- Rigid laryngoscope. A rigid viewing tube is inserted through your mouth.
- Videostroboscope. A camera is combined with a flashing light to provide a slow-motion view of your vocal cords as they move.
Additional tests are sometimes used:
- Sound (acoustic) analysis. Using computer analysis, your doctor can measure irregularities in the sound produced by the vocal cords.
- Laryngeal electromyography. Small needles are inserted through the skin to measure the electric currents in your voice box muscles.
- Auditory-Perceptual Assessment. Subjective assessment based on clinical impressions of the speech-language pathologistVoice Quality
- Consensus features assessed during production of sustained vowels, sentences, and running speech
- Roughness—perceived irregularity in voicing source
- Breathiness—audible air escape in voice
- Strain—perception of excessive vocal effort
- Pitch (perceptual correlate of fundamental frequency)—deviations from normal relative to age, gender, and referent culture
- Loudness (perceptual correlate of sound intensity)—deviations from normal relative to age, gender, and referent culture
- Overall severity—global, integrated impression of voice deviance
- Additional perceptual features
- Diplophonia, aphonia, pitch instability, tremor, vocal fry, falsetto, wet/gurgly
- Consensus features assessed during production of sustained vowels, sentences, and running speech
Assessment may result in
- diagnosis of a voice disorder;
- clinical description of the characteristics and severity of the disorder;
- statement of prognosis and recommendations for intervention;
- identification of appropriate treatment or management options; and
- referral to other professionals, as needed.
Voice disorders treatment
Depending on your diagnosis, your doctor will recommend one or more treatments:
- Rest, liquids and voice therapy. Like any other part of the body, the vocal cords need regular rest and fluids. Speech pathology specialists can teach you how to use your voice more efficiently through voice therapy, how to properly clear your throat and how much liquid to drink.
- Allergy treatments. If an allergy is creating too much mucus in your throat, your doctor or an allergy specialist can identify the allergy’s cause and provide treatment.
- Smoking cessation. If your voice problem is the result of smoking, quitting smoking can help improve your voice along with many other areas of your health, such as boosting your heart health and lowering your cancer risk.
- Medications. Several medications are available for treating voice disorders. Depending on the cause of your voice disorder, you may need medication to reduce inflammation, treat gastroesophageal reflux or prevent blood vessel regrowth. Medications can be taken orally, injected into the vocal cords or applied topically during surgery.
Procedures
- Removal of lesions. Noncancerous lesions (polyps, nodules and cysts) on the vocal cords may need to be surgically removed. Your doctor can remove noncancerous, precancerous and cancerous lesions — including recurrent respiratory papillomatosis and white patches (leukoplakia) — using microsurgery, carbon-dioxide laser surgery, and when appropriate, the newest laser treatments, including potassium titanyl phosphate (KTP) laser treatment.KTP laser treatment is a state-of-the-art therapy that treats lesions on the vocal cords by cutting off the blood supply to the lesion, allowing the lesion to be removed while preserving the maximum amount of underlying tissue.
- Botox injections. Injections of tiny amounts of purified botulinum toxin into your neck skin can decrease muscle spasms or abnormal movements if you have a neurological movement disorder that affects the vocal muscles of the larynx (spasmodic dysphonia).
Sometimes one vocal cord may stop moving (become paralyzed). If you have one paralyzed vocal cord, you might often complain of hoarseness. You might also complain of choking when you drink liquids, but rarely have trouble swallowing solid foods. Sometimes the problem goes away with time.
If not, one of two procedures can be used to push the paralyzed vocal cord closer to the middle of the windpipe so that the vocal cords can meet and vibrate closer together. This improves the voice and allows the larynx to close when you swallow. Treatments include:
- Fat or collagen injection. Body fat or synthetic collagen is injected, either through your mouth or the skin on your neck, to add bulk to the paralyzed vocal cord or to treat vocal cord weakness. The material fills the space next to your vocal cord and pushes it closer to your other vocal cord, allowing them to vibrate more closely together.
- Thyroplasty. A small opening is created in the cartilage from the outside of your voice box. The doctor inserts an implant through the opening and pushes it against the paralyzed vocal cord, moving it closer to your other vocal cord.
Symptomatic Voice Therapy
The focus of symptomatic voice therapy is on the modification of the deviant vocal symptoms or perceptual voice components. Deviant symptoms may include pitch that is too high or low, voice that is too soft or loud, breathy phonation, or the use of hard glottal attacks or glottal fry. Symptomatic voice therapy assumes voice improvement through direct symptom modification using a variety of voice facilitating techniques 1 that are either direct or indirect.
Amplification
Amplification devices such as microphones can be used to amplify the voice in any situation that requires increased volume (e.g., when speaking to large groups, or during conversation when the individual’s voice is weak). As such, voice amplification can function as a supportive tool or as a means of augmentative communication. It can help prevent vocal hyperfunction as a result of talking at increased volume or for extended periods of time.
Auditory Masking
Auditory masking is used in cases of functional aphonia/dysphonia and often results in changed or normal phonation. Individuals are instructed to talk or read passages aloud while wearing headphones with masking noise input. Using a loud noise background, the individual often produces voice at increased volume (Lombard effect) that can be recorded and used later in treatment as a comparison 14.
Biofeedback
The basis of biofeedback is that self-control of physiologic functions is possible with continuous, immediate information about internal bodily state. Biofeedback provides clear and reliable feedback in response to alterations in voice production, thus facilitating improvements in pitch, loudness, quality, and effort. It can be kinesthetic, auditory, or visual. Using biofeedback, individuals are trained to become aware of physical sensations with respect to respiration, body position, and vibratory sensation. Awareness helps the individual understand his or her physiological processes when generating voice. Auditory feedback, such as real-time amplification auditory modeling is an effective way to achieve voice improvement.
Chant Speech
Chant speech is characterized by a rhythmic, prosodic pattern that serves as a template for spoken utterances. It is used in therapy to help reduce phonatory effort that results in vocal fatigue and decrease in phonatory capabilities. Chant speech requires pitch fluctuations and coordination among respiratory, phonatory, and resonance subsystems. Speakers habituate to these more efficient vocal patterns. The increased lung pressure required for these tasks may also decrease reliance on laryngeal resistance and reduce fatigue 15.
Confidential Voice
Confidential voice is designed to reduce laryngeal tension/hyperfunction and increase air flow 16. The individual begins with an easy and breathy vocal quality and builds to normal voicing without decreasing airflow. This technique is intended to address excessive vocal tension and to facilitate relaxation in the muscles of the larynx.
Glottal Fry
Glottal fry is useful for patients with vocal nodules and other problems associated with hyperfunction (e.g., polyps, functional dysphonia, spasmodic dysphonia, vocal fold thickening, and ventricular phonation). Because the vocal folds must be relaxed in order to produce glottal fry, this technique can be a useful index of vocal fold relaxation 1. Although glottal fry is a powerful facilitative technique to offload tension in the larynx, it is not a long-term speech quality target.
Inhalation Phonation
Inhalation phonation is a technique used to facilitate true vocal vibration in the presence of habitual ventricular fold phonation, functional aphonia, and muscle tension dysphonia. Individuals produce a high-pitched voice on inhalation. Upon inhalation voicing, the true vocal folds are in a stretched position, suddenly adducted and in vibration. Upon exhalation, patients try to achieve a nearly matched voice. This approach eases the way to gaining true vocal fold vibration.
Semi-Occluded Vocal Tract Exercises
Semi-occluded vocal tract exercises in voice therapy involve narrowing at any supraglottic point along the vocal tract in order to maximize interaction between vocal fold vibration (sound production) and the vocal tract (the sound filter) and to produce resonant voice.
Straw Phonation
Straw phonation is one of the most frequently used methods to create semi-occlusion in the vocal tract 17. Narrowing the vocal tract increases air pressure above the vocal folds, keeping them slightly separated during phonation and reducing the impact collision force. To accomplish this, the individual semi-occludes the vocal tract by phonating through a straw or tube. Resistance can be manipulated by varying the length and diameter of the straw. Individuals practice sustaining vowels, performing pitch glides, humming songs, and transitioning to the intonation and stress patterns of speech. Eventually, use of the straw is reduced and eliminated.
Lip Trill
Semi-occlusion at the level of the lips is accomplished via lip trills. This technique involves a smooth movement of air through the oral cavity and over the lips, causing a vibration (lip buzz), similar to blowing bubbles underwater. Often, the trills are paired with phonation and pitch changes. The focus is to improve breath support and produce voicing without tension.
Posture
The patient is instructed in the technique of sitting with upright posture and with the shoulders in a low, relaxed position to facilitate voice production with less effort. Collaboration with a physical therapist or occupational therapist may be necessary with some patients.
Relaxation
In cases of vocal hyperfunction, a variety of relaxation techniques may be useful as a tool to reduce both whole-body and laryngeal area tension. The goal of these techniques is to reduce effortful phonation. Frequently used techniques include progressive muscle relaxation (slowly tensing and then relaxing successive muscle groups), visualization (forming mental images of a peaceful, calming place or situation), and deep breathing exercises.
Twang Therapy
Twang therapy is used for individuals with hypophonic voice. It involves the narrowing of the aryepiglottic sphincter using a “twang” voice to create a high-intensity voice quality while maintaining low vocal effort 18. The desired outcome is decreasing phonatory effort and increasing vocal efficiency.
Yawn-Sigh
This facilitating technique uses the natural functions of yawning and sighing to overcome symptoms of vocal hyperfunction (e.g., elevated larynx and vocal constriction). The technique is intended to lower the position of the larynx and subsequently widen the supraglottal space in order to produce a more relaxed voice and encourage a more natural pitch.
- Boone, D. R., McFarlane, S. C., Von Berg, S. L., & Zraick, R. I. (2010). The voice and voice therapy. Boston, MA: Allyn & Bacon.[↩][↩][↩]
- Stemple, J. C., Glaze, L. E., & Klaben, B. G. (2010). Clinical voice pathology: Theory and management. San Diego, CA: Plural.[↩][↩]
- Roy, N., Merrill, R. M., Gray, S. D., & Smith, E. M. (2005). Voice disorders in the general population: Prevalence, risk factors, and occupational impact. The Laryngoscope, 115, 1988–1995[↩]
- Cohen, S. M., Kim, J., Roy, N., Asche, C., & Courey, M. (2012). Prevalence and causes of dysphonia in a large treatment-seeking population. The Laryngoscope, 122, 343–348.[↩][↩][↩][↩][↩][↩]
- Martins, R. H., do Amaral, H. A., Tavares, E. L., Martins, M. G., Gonҫalves, T. M., & Dias, N. H. (2015). Voice disorders: Etiology and diagnosis. Journal of Voice. Advance online publication. doi:10.1016/j.jvoice.2015.09.017[↩][↩][↩][↩][↩][↩]
- Black, L. I., Vahratian, A., & Hoffman, H. J. (2015). Communication disorders and use of intervention services among children aged 3–17 years: United States, 2012 (NCHS Data Brief, No. 205). Hyattsville, MD: National Center for Health Statistics.[↩]
- Roy, N., Merrill, R. M., Thibeault, S., Parsa, R. A., Gray, S. D., & Smith, E. M. (2004). Prevalence of voice disorders in teachers and the general population. Journal of Speech, Language, and Hearing Research, 47, 281–293.[↩]
- Cantor Cutiva, L. C., Vogel, I., & Burdorf, A. (2013). Voice disorders in teachers and their associations with work-related factors: A systematic review. Journal of Communication Disorders, 46, 143–155.[↩][↩]
- American Speech-Language-Hearing Association. http://www.asha.org/Practice-Portal/Clinical-Topics/Voice-Disorders/[↩]
- Traister, R. S., Fajt, M. L., & Petrov, A. A. (2016). The morbidity and cost of vocal cord dysfunction misdiagnosed as asthma. Allergy and Asthma Proceedings, 37, e25–e31.[↩]
- Stemple, J. C., Roy, N., & Klaben, B. G. (2014). Clinical voice pathology: Theory and management. San Diego, CA: Plural. [↩]
- Kiliҫ, M. A., Okur, E., Yildirim, I., & Güzelsoy, S. (2004). The prevalence of vocal fold nodules in school age children. International Journal of Pediatric Otorhinolaryngology, 68, 409–412.[↩]
- Van Houtte, E., Van Lierde, K., D’Haeseleer, E., & Claeys, D. (2009). The prevalence of laryngeal pathology in a treatment-seeking population with dysphonia. The Laryngoscope, 120, 306–312.[↩]
- Brumm, H., & Zollinger, S. A. (2011). The evolution of the Lombard effect: 100 years of psychoacoustic research. Behaviour, 148, 1173–1198.[↩]
- McCabe, D. J., & Titze, I. R. (2002). Chant therapy for treating vocal fatigue among public school teachers: A preliminary study. American Journal of Speech-Language Pathology, 11, 356–369.[↩]
- Casper, J. (2000). Confidential voice. In J. C. Stemple (Ed.), Voice therapy: Clinical studies (pp. 128–139). San Diego, CA: Singular.[↩]
- Titze, I. R. (2006). Voice training and therapy with a semi-occluded vocal tract: Rationale and scientific underpinnings. Journal of Speech, Language, and Hearing Research, 49, 448–459.[↩]
- Lombard, L. E., & Steinhauer, K. M. (2007). A novel treatment for hypophonic voice: Twang therapy. Journal of Voice, 21, 294–299.[↩]





{kind=link}