
Contents
What is West Nile virus
West Nile is a virus most commonly spread to people by mosquito bites in many countries. West Nile virus has occurred in Africa, Asia, Europe and the Middle East. It appeared in the United States in the summer of 1999, and since then has been reported in every state except Hawaii and Alaska, as well as in Canada. In North America, cases of West Nile virus occur during mosquito season, which starts in the summer and continues through autumn. West Nile virus cases have been reported in all of the continental United States. There are no vaccines to prevent or medications to treat West Nile virus. Fortunately, most people infected with West Nile virus do not have symptoms. About 1 in 5 people who are infected develop a fever and other symptoms. About 1 out of 150 infected people develop a serious, sometimes fatal, illness. You can reduce your risk of West Nile virus by using insect repellent and wearing long-sleeved shirts and long pants to prevent mosquito bites.
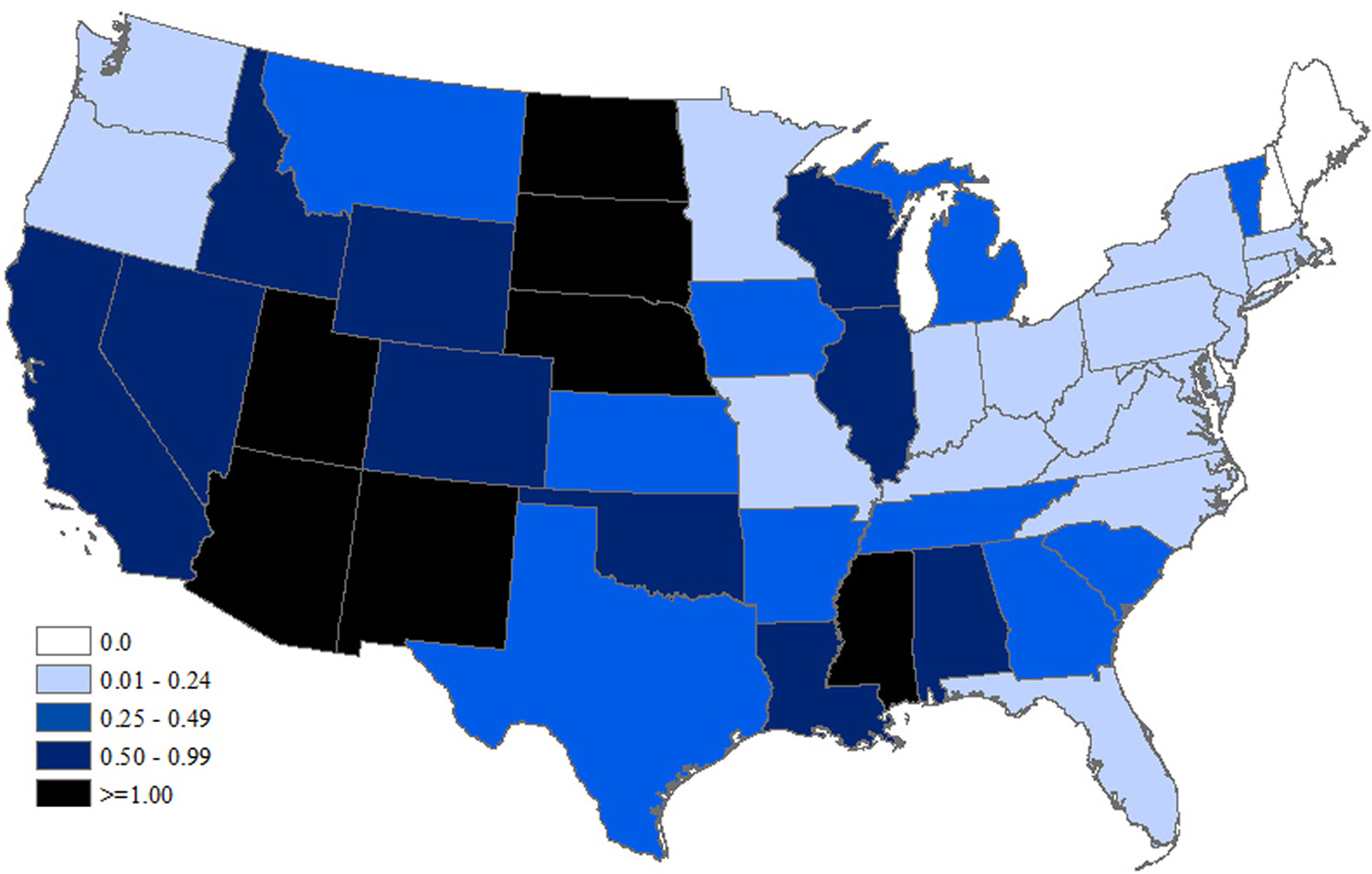
Most cases of West Nile virus in the United States occur June through September. Cases have been reported in all 48 lower states.
As of January 9, 2018, a total of 47 states and the District of Columbia have reported West Nile virus infections in people, birds, or mosquitoes in 2017 1. Overall, 2,002 cases of West Nile virus disease in people have been reported to CDC. Of these, 1,339 (67%) were classified as neuroinvasive disease (such as meningitis or encephalitis) and 663 (33%) were classified as non-neuroinvasive disease. For live map go here: https://wwwn.cdc.gov/arbonet/maps/ADB_Diseases_Map/index.html
In majority of West Nile virus infection there are usually no symptoms and people gets better without treatment. Some people develop mild flu-like symptoms, nausea and skin rash. But severe signs and symptoms — such as a severe headache, fever, disorientation or sudden weakness — require immediate medical attention.
Risk of serious West Nile virus infection
Even if you’re infected, your risk of developing a serious West Nile virus-related illness is extremely small — less than 1 percent of people who are infected become severely ill. And most people who do become sick recover fully. You’re more likely to develop a severe or fatal infection based on:
- Age. Being older puts you at higher risk.
- Certain medical conditions. Certain diseases, such as cancer, diabetes, hypertension and kidney disease, increase your risk. So does receiving an organ transplant.
Furthermore, there is no specific treatment for West Nile virus disease; clinical management is supportive. Patients with severe meningeal symptoms often require pain control for headaches and antiemetic therapy and rehydration for associated nausea and vomiting. Patients with encephalitis require close monitoring for the development of elevated intracranial pressure and seizures. Patients with encephalitis or poliomyelitis should be monitored in hospital for to protect their airway. Acute neuromuscular respiratory failure may develop rapidly and prolonged ventilatory support may be required.
Various drugs have been evaluated or empirically used for West Nile virus disease. However, none have shown specific benefit to date. The National Institutes of Health maintains a registry of federally and privately supported clinical trials conducted in the United States and around the world.
Figure 1. West Nile Virus Neuroinvasive Disease Incidence by State – United States
West Nile virus transmission
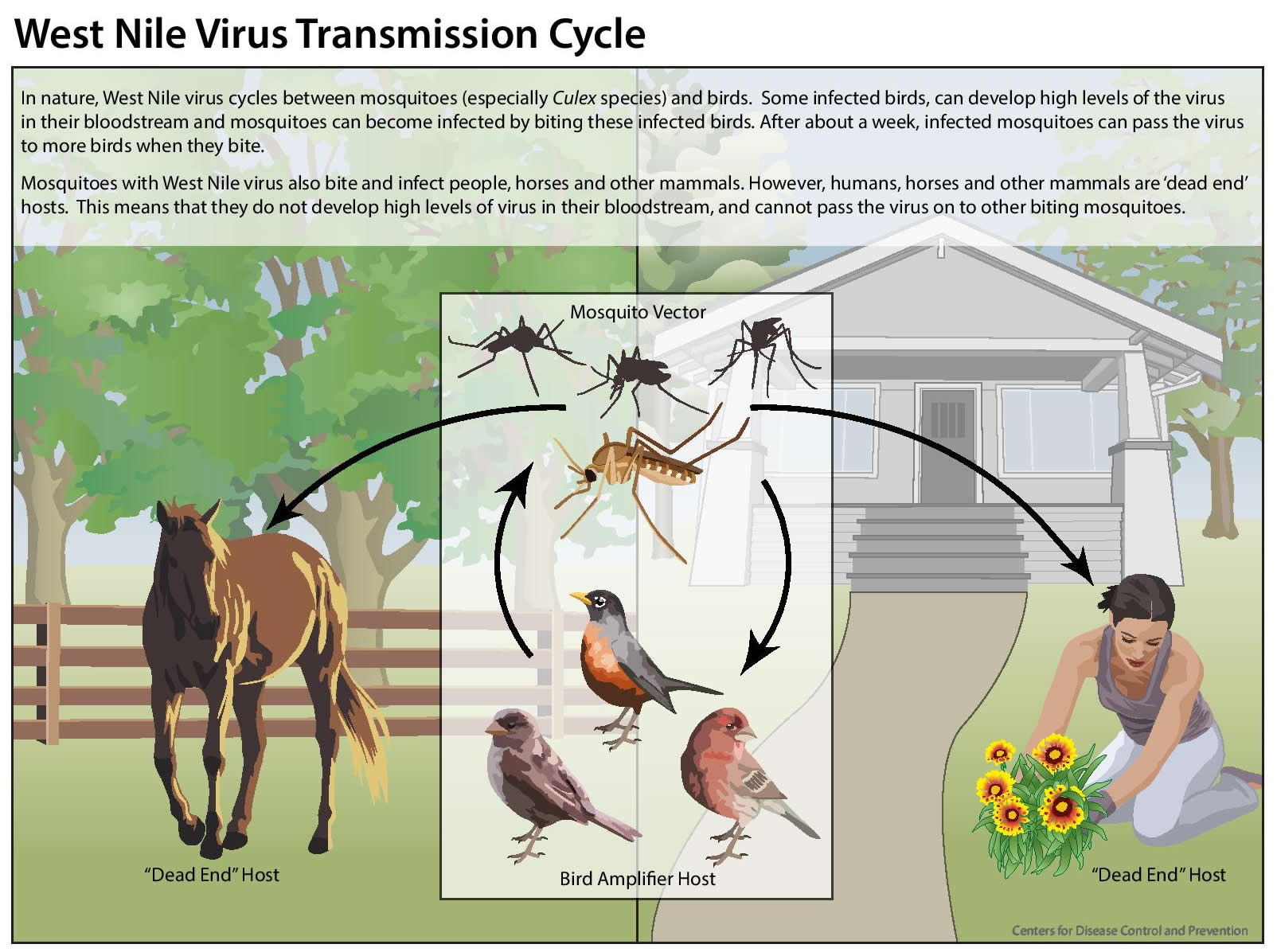
West Nile virus is most commonly spread to people by the bite of an infected mosquito.
Mosquitoes become infected when they feed on infected birds. Infected mosquitoes then spread West Nile virus to people and other animals by biting them.
In a very small number of cases, West Nile virus has been spread through:
- Exposure in a laboratory setting
- Blood transfusion and organ donation
- Mother to baby, during pregnancy, delivery, or breast feeding
I am pregnant. Am I at higher risk for getting infected with West Nile virus?
No. Pregnant women are not at higher risk for West Nile virus infection.
I am pregnant and was just diagnosed with West Nile virus infection. Is my baby at risk of infection?
The risk appears to be very low that a woman who is infected with West Nile virus during pregnancy will transmit the virus to her fetus or newborn. Only a few cases of West Nile virus in newborns have been reported. Pregnant women should take precautions to reduce their risk for West Nile virus infection by avoiding mosquitoes, wearing protective clothing, and using insect repellent.
If I am pregnant or breastfeeding, should I use insect repellents?
Yes. Protecting yourself from mosquito bites is the only way to prevent infection with West Nile virus. In addition to wearing protective clothing such as long-sleeve shirts and long pants, use insect repellents. Repellents containing active ingredients which have been registered with the EPA are considered safe for pregnant and breastfeeding women. Find the insect repellent that’s right for you by using EPA’s search tool (https://www.epa.gov/insect-repellents/find-repellent-right-you).
Can West Nile virus be transmitted through breast milk?
Possibly. It appears that West Nile virus may be transmitted through breast milk.
In 2002, a woman developed encephalitis due to West Nile virus from a blood transfusion she received shortly after giving birth. Laboratory analysis showed evidence of West Nile virus in breast milk collected from the mother soon after she became ill. She had been breastfeeding her infant and about 3 weeks after birth the infant tested positive for West Nile virus. Because of the infant’s minimal outdoor exposure, it is unlikely that infection was acquired from a mosquito. The infant had no symptoms of West Nile virus infection and remained healthy.
Should I continue breastfeeding if I have West Nile virus disease?
Yes. The risk for West Nile virus transmission through breastfeeding is unknown. However, the health benefits of breastfeeding are well established. Therefore, there are no recommendations for a woman to stop breastfeeding because of West Nile virus illness.
Is West Nile virus contagious?
No. West Nile virus is not contagious. You only get it from being bitten by an infected mosquito.
West Nile virus is NOT spread:
- Through coughing, sneezing, or touching
- By touching live animals
- From handling live or dead infected birds. Avoid bare-handed contact when handling any dead animal. If you are disposing of a dead bird, use gloves or double plastic bags to place the carcass in a garbage can.
- Through eating infected birds or animals. Always follow instructions for fully cooking meat from either birds or mammals.
Figure 2. West Nile virus transmission
West Nile virus prevention
Your best bet for preventing West Nile virus and other mosquito-borne illnesses is to prevent mosquito bites and to avoid exposure to mosquitoes and eliminate standing water, where mosquitoes breed. Be aware of the West Nile virus activity in your area and take action to protect yourself and your family.
- Unclog roof gutters.
- Empty unused swimming pools or empty standing water on pool covers.
- Change water in birdbaths and pet bowls regularly.
- Remove old tires or unused containers that might hold water and serve as a breeding place for mosquitoes.
- Install or repair screens on windows and doors.
To reduce your exposure to mosquitoes:
- Avoid unnecessary outdoor activity when mosquitoes are most prevalent, such as at dawn, dusk and early evening.
- Wear long-sleeved shirts and long pants when outdoors.
- Apply mosquito repellent containing an Environmental Protection Agency-registered insect repellent to your skin and clothing. Choose the concentration based on the hours of protection you need — the higher the percentage (concentration) of the active ingredient, the longer the repellent will work. Follow the directions on the package, paying special attention to recommendations for use on children.
- When outside, cover your infant’s stroller or playpen with mosquito netting.
Prevent Mosquito Bites
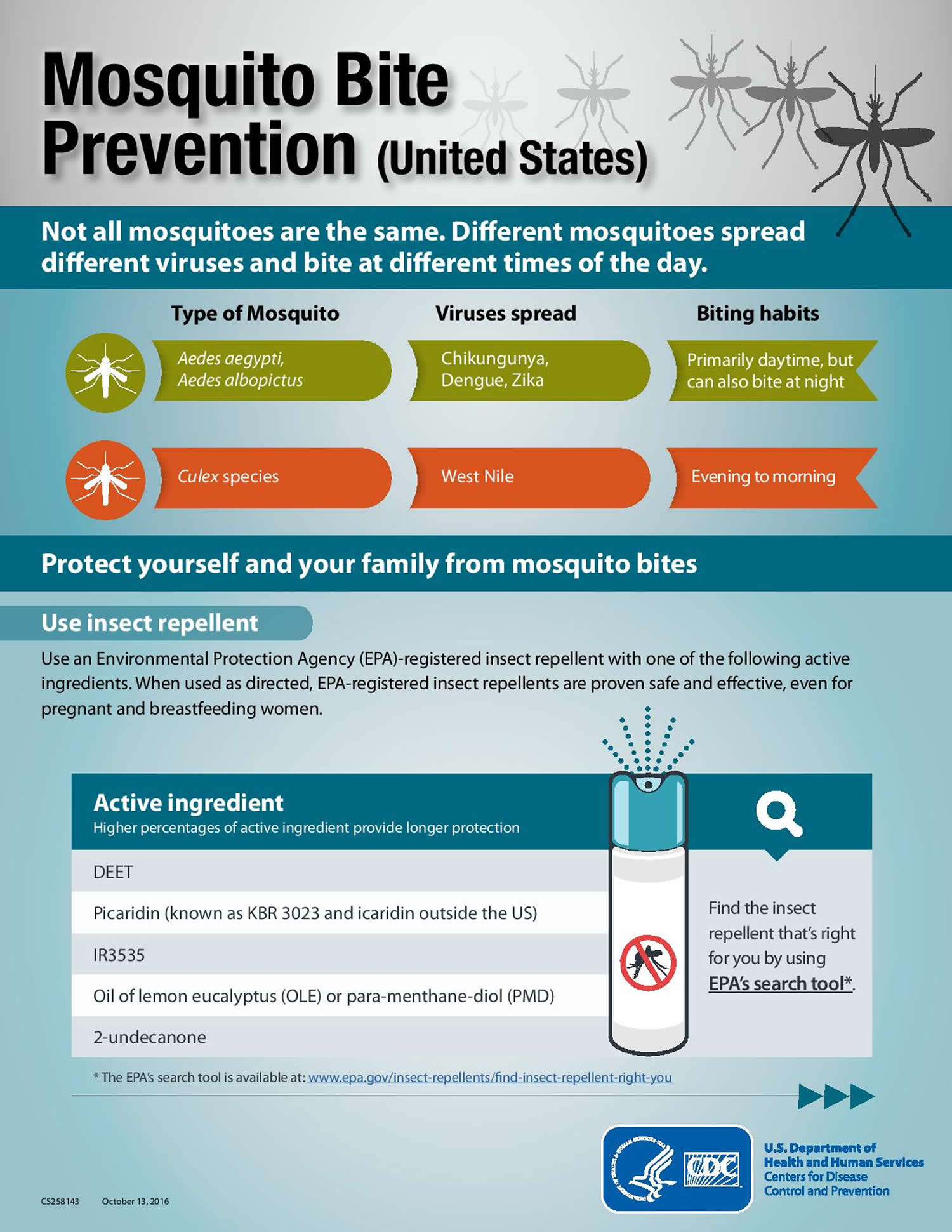
Use Insect Repellent
Use Environmental Protection Agency (EPA)-registered insect repellents with one of the active ingredients below 3. When used as directed, EPA-registered insect repellents are proven safe and effective, even for pregnant and breastfeeding women.
- DEET
- Picaridin (known as KBR 3023 and icaridin outside the US)
- IR3535
- Oil of lemon eucalyptus (OLE) or para-menthane-diol (PMD)
- 2-undecanone
Find the insect repellent that’s right for you by using EPA’s search tool (https://www.epa.gov/insect-repellents/find-repellent-right-you).
Tips for Everyone
- Always follow the product label instructions.
- Reapply insect repellent as directed.
- Do not spray repellent on the skin under clothing.
- If you are also using sunscreen, apply sunscreen first and insect repellent second.
Tips for Babies & Children
- Always follow instructions when applying insect repellent to children.
- Do NOT use insect repellent on babies younger than 2 months old.
- Do NOT apply insect repellent onto a child’s hands, eyes, mouth, and cut or irritated skin.
- Adults: Spray insect repellent onto your hands and then apply to a child’s face.
- Do NOT use products containing oil of lemon eucalyptus (OLE) or para-menthane-diol (PMD) on children under 3 years old.
Natural insect repellents (repellents not registered with EPA)
- Scientists do not know the effectiveness of non-EPA registered insect repellents, including some natural repellents.
- To protect yourself against diseases spread by mosquitoes, CDC and EPA recommend using an EPA-registered insect repellent.
- Choosing an EPA-registered repellent ensures the EPA has evaluated the product for effectiveness.
Protect your baby or child
- Dress your child in clothing that covers arms and legs.
- Cover crib, stroller, and baby carrier with mosquito netting.
Wear long-sleeved shirts and long pants
- Treat items, such as boots, pants, socks, and tents, with permethrin* or buy permethrin-treated clothing and gear.
- Permethrin-treated clothing will protect you after multiple washings. See product information to find out how long the protection will last.
- If treating items yourself, follow the product instructions.
- Do NOT use permethrin products directly on skin.
*In some places, such as Puerto Rico, where permethrin products have been used for years in mosquito control efforts, mosquitoes have become resistant to it. In areas with high levels of resistance, use of permethrin is not likely to be effective.
Take steps to control mosquitoes inside and outside your home
- Use screens on windows and doors. Repair holes in screens to keep mosquitoes outside.
- Use air conditioning when available.
- Sleep under a mosquito bed net if air conditioned or screened rooms are not available or if sleeping outdoors.
- Once a week, empty and scrub, turn over, cover, or throw out items that hold water, such as tires, buckets, planters, toys, pools, birdbaths, flowerpots, or trash containers. Check inside and outside your home. Mosquitoes lay eggs near water.
Figure 3. West Nile virus prevention

West Nile virus signs and symptoms
The incubation period for West Nile virus disease is typically 2 to 6 days but ranges from 2 to 14 days and can be several weeks in immunocompromised people.
An estimated 70-80% of human West Nile virus infections are subclinical or asymptomatic. Most symptomatic persons experience an acute systemic febrile illness that often includes headache, weakness, myalgia, or arthralgia; gastrointestinal symptoms and a transient maculopapular rash also are commonly reported.
Most women known to have been infected with West Nile virus during pregnancy have delivered infants without evidence of infection or clinical abnormalities. In the best-documented, confirmed congenital West Nile virus infection, the mother developed neuroinvasive West Nile virus disease during the twenty-seventh week of gestation, and her neonate was born with cystic lesions in brain tissue and chorioretinitis. One infant who apparently acquired West Nile virus infection through breastfeeding remained asymptomatic.
Figure 4. West Nile virus rash (diffuse maculopapular rash associated with West Nile virus infection)

West Nile virus symptoms in humans
- No symptoms in most people. Most people (8 out of 10) infected with West Nile virus do not develop any symptoms.
- Febrile illness (fever) in some people. About 20 percent of (1 in 5) people develop a mild infection called West Nile fever. Common signs and symptoms include:
- Fever with other symptoms such as:
- Headache,
- Body aches,
- Joint pains,
- Vomiting,
- Diarrhea, or
- Rash, which tends to be morbilliform, maculopapular and non-pruritic and predominates over the torso and extremities, sparing the palms and soles (Figure 4) 5. The rash may be transient, lasting less than 24 hours in some persons. Interestingly, this rash appears to be more frequently seen in West Nile fever than in more severe illness manifestations (West Nile meningitis or West Nile encephalitis) 5. In addition, rash is more frequently observed among younger persons than among older persons 5. These findings raise the question as to whether the presence of a rash correlates with host immune or cytokine response to infection.
- Signs and symptoms of West Nile fever usually last a few days.
- Most people with this type of West Nile virus disease recover completely, but fatigue and weakness can last for weeks or months.
- Fever with other symptoms such as:
- Serious symptoms in a few people. About 1 in 150 people who are infected develop a severe illness affecting the central nervous system (Neuroinvasive West Nile disease) such as West Nile encephalitis (inflammation of the brain), West Nile meningitis (inflammation of the membranes that surround the brain and spinal cord) and West Nile poliomyelitis (an acute poliomyelitis-like syndrome) 6. West Nile meningitis involves infection of the meninges (the outer covering of the brain and spinal cord) and makes up the largest percentage of neuroinvasive disease cases in younger age groups. West Nile encephalitis involves viral infection of the brain parenchyma itself and is more typically manifested in older persons or individuals with compromised immune systems. West Nile poliomyelitis results from viral infection of the anterior horn cells of the spinal cord, leading to acute flaccid limb weakness.
- Symptoms of severe neurological infections (Neuroinvasive West Nile virus infections) include:
- high fever,
- headache,
- neck stiffness,
- stupor,
- disorientation,
- coma,
- tremors,
- convulsions,
- muscle weakness,
- vision loss,
- numbness and
- paralysis.
- When discussing the various manifestations of West Nile virus infection, it is important to keep in mind that the clinical picture may not always be as clear-cut as delineated above, and sometimes, the clinical features of West Nile fever, West Nile meningitis and West Nile encephalitis may overlap. For example, patients may develop an altered mental status, due to severe systemic illness, without true histopathologic or radiologic evidence of cerebral inflammation or “encephalitis” in the pathophysiologic sense. Similarly, patients presenting with fever, headache and “neck stiffness” may not undergo lumbar puncture to demonstrate pleocytosis, and consequently, a diagnosis of WN “meningitis” may not be reported.
- Severe illness can occur in people of any age; however, people over 60 years of age are at greater risk. People with certain medical conditions, such as cancer, diabetes, hypertension, kidney disease, and people who have received organ transplants, are also at greater risk.
- Signs and symptoms of encephalitis or meningitis can linger for weeks or months.
- Recovery from severe illness might take several weeks or months. Some effects to the central nervous system might be permanent, such as muscle weakness, can be permanent.
- About 1 out of 10 people who develop severe illness affecting the central nervous system die.
- Symptoms of severe neurological infections (Neuroinvasive West Nile virus infections) include:
Very young and elderly people, and people with conditions like diabetes are more at risk of developing severe infection.
Signs of a severe West Nile virus infection can include flu-like symptoms and also:
- muscle weakness
- confusion
- fits (seizures)
Severe West Nile virus infections are treated in hospital. In rare cases it can lead to meningitis.
Less than 1% of infected persons develop neuroinvasive disease, which typically manifests as meningitis, encephalitis, or acute flaccid paralysis.
- West Nile virus meningitis is clinically indistinguishable from viral meningitis due to other etiologies and typically presents with fever, headache, and nuchal rigidity.
- West Nile virus encephalitis is a more severe clinical syndrome that usually manifests with fever and altered mental status, seizures, focal neurologic deficits, or movement disorders such as tremor or parkinsonism.
- West Nile virus acute flaccid paralysis is usually clinically and pathologically identical to poliovirus-associated poliomyelitis, with damage of anterior horn cells, and may progress to respiratory paralysis requiring mechanical ventilation. West Nile virus poliomyelitis often presents as isolated limb paresis or paralysis and can occur without fever or apparent viral prodrome. West Nile virus-associated Guillain-Barré syndrome and radiculopathy have also been reported and can be distinguished from West Nile virus poliomyelitis by clinical manifestations and electrophysiologic testing.
Rarely, cardiac dysrhythmias, myocarditis, rhabdomyolysis, optic neuritis, uveitis, chorioretinitis, orchitis, pancreatitis, and hepatitis have been described in patients with West Nile virus disease.
West Nile virus diagnosis
Besides conducting a physical exam, your doctor can confirm the presence of West Nile virus or a West Nile-related illness, such as meningitis or encephalitis, by performing one of the following tests:
- Laboratory tests. If you’re infected, a blood test may show a rising level of antibodies to the West Nile virus. Antibodies are immune system proteins that attack foreign substances, such as viruses.
- Lumbar puncture (spinal tap). The most common way to diagnose meningitis is to analyze the cerebrospinal fluid surrounding your brain and spinal cord. A needle inserted between the lower vertebrae of your spine is used to extract a sample of fluid for laboratory analysis. The fluid sample may show an elevated white cell count — a signal that your immune system is fighting an infection — and antibodies to the West Nile virus.
- Brain tests. In some cases, an electroencephalography (EEG) — a procedure that measures your brain’s activity — or an MRI scan can help detect brain inflammation.
West Nile virus Antibody Testing
Laboratory diagnosis is generally accomplished by testing of serum or cerebrospinal fluid (CSF) to detect West Nile virus-specific IgM antibodies. Immunoassays for West Nile virus-specific IgM are available commercially and through state public health laboratories.
West Nile virus-specific IgM antibodies are usually detectable 3 to 8 days after onset of illness and persist for 30 to 90 days, but longer persistence has been documented. Therefore, positive IgM antibodies occasionally may reflect a past infection. If serum is collected within 8 days of illness onset, the absence of detectable virus-specific IgM does not rule out the diagnosis of West Nile virus infection, and the test may need to be repeated on a later sample.
The presence of West Nile virus-specific IgM in blood or cerebrospinal fluid (CSF) provides good evidence of recent infection but may also result from cross-reactive antibodies after infection with other flaviviruses or from non-specific reactivity. According to product inserts for commercially available West Nile virus IgM assays, all positive results obtained with these assays should be confirmed by neutralizing antibody testing of acute- and convalescent-phase serum specimens at a state public health laboratory or CDC.
West Nile virus IgG antibodies generally are detected shortly after IgM antibodies and persist for many years following a symptomatic or asymptomatic infection. Therefore, the presence of IgG antibodies alone is only evidence of previous infection and clinically compatible cases with the presence of IgG, but not IgM, should be evaluated for other etiologic agents.
Plaque-reduction neutralization tests (PRNTs) performed in reference laboratories, including some state public health laboratories and CDC, can help determine the specific infecting flavivirus. Plaque-reduction neutralization tests (PRNTs) can also confirm acute infection by demonstrating a fourfold or greater change in West Nile virus-specific neutralizing antibody titer between acute- and convalescent-phase serum samples collected 2 to 3 weeks apart.
Other testing for West Nile virus disease
Viral cultures and tests to detect viral RNA (e.g., reverse transcriptase-polymerase chain reaction) can be performed on serum, cerebrospinal fluid (CSF), and tissue specimens that are collected early in the course of illness and, if results are positive, can confirm an infection. Immunohistochemistry can detect West Nile virus antigen in formalin-fixed tissue. Negative results of these tests do not rule out West Nile virus infection. Viral culture, reverse transcriptase-polymerase chain reaction and immunohistochemistry can be requested through state public health laboratories or CDC.
West Nile virus treatment
Most people recover from West Nile virus without treatment. Most severe cases require supportive therapy in a hospital with intravenous fluids and pain medication.
- No vaccine or specific antiviral treatments for West Nile virus infection are available.
- Over-the-counter pain relievers can be used to reduce fever and relieve some symptoms
- In severe cases, patients often need to be hospitalized to receive supportive treatment, such as intravenous fluids, pain medication, and nursing care.
- Scientists are investigating interferon therapy — a type of immune cell therapy — as a treatment for encephalitis caused by West Nile virus. Some research shows that people who receive interferon recover better than those who don’t receive the drug, but more study is needed.
- If you think you or a family member might have West Nile virus disease, talk with your health care provider.
Most patients with non-neuroinvasive West Nile virus disease or West Nile virus meningitis recover completely, but fatigue, malaise, and weakness can linger for weeks or months. Patients who recover from West Nile virus encephalitis or poliomyelitis often have residual neurologic deficits. Among patients with neuroinvasive disease, the overall case-fatality ratio is approximately 10%, but it is significantly higher for patients with West Nile virus encephalitis and poliomyelitis than West Nile virus meningitis.
Recent studies have raised questions about the possible persistence of West Nile virus infection and subsequent renal disease.
- https://www.cdc.gov/westnile/statsmaps/preliminarymapsdata2017/incidencestate.html[↩]
- West Nile Virus Neuroinvasive Disease Incidence by State – United States, 2017 (as of January 9, 2018). https://www.cdc.gov/westnile/statsmaps/preliminarymapsdata2017/incidencestate.html[↩]
- Repellents: Protection against Mosquitoes, Ticks and Other Arthropods. https://www.epa.gov/insect-repellents[↩]
- Sejvar JJ. Clinical Manifestations and Outcomes of West Nile Virus Infection. Viruses. 2014;6(2):606-623. doi:10.3390/v6020606. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3939474/[↩]
- Characteristics of the rash associated with West Nile virus fever. Ferguson DD, Gershman K, LeBailly A, Petersen LR. Clin Infect Dis. 2005 Oct 15; 41(8):1204-7. https://www.ncbi.nlm.nih.gov/pubmed/16163642/[↩][↩][↩]
- West Nile virus. Campbell GL, Marfin AA, Lanciotti RS, Gubler DJ. Lancet Infect Dis. 2002 Sep; 2(9):519-29. https://www.ncbi.nlm.nih.gov/pubmed/12206968/[↩]





{kind=link}