

Contents
- What is flaxseed
- Flax seed nutrition facts
- Flaxseed fiber
- Flaxseed Oil
- Table 2. Other sources of Omega-3 Alpha-linolenic acid (ALA) and content of ALA in selected novel sources of omega-3 polyunsaturated fatty acids
- What are omega-3 fatty acids ?
- Non-fish oil based Omega-3 Polyunsaturated Fatty Acids
- Figure 1. Omega-3 fatty acids and Omega-6 fatty acids structure
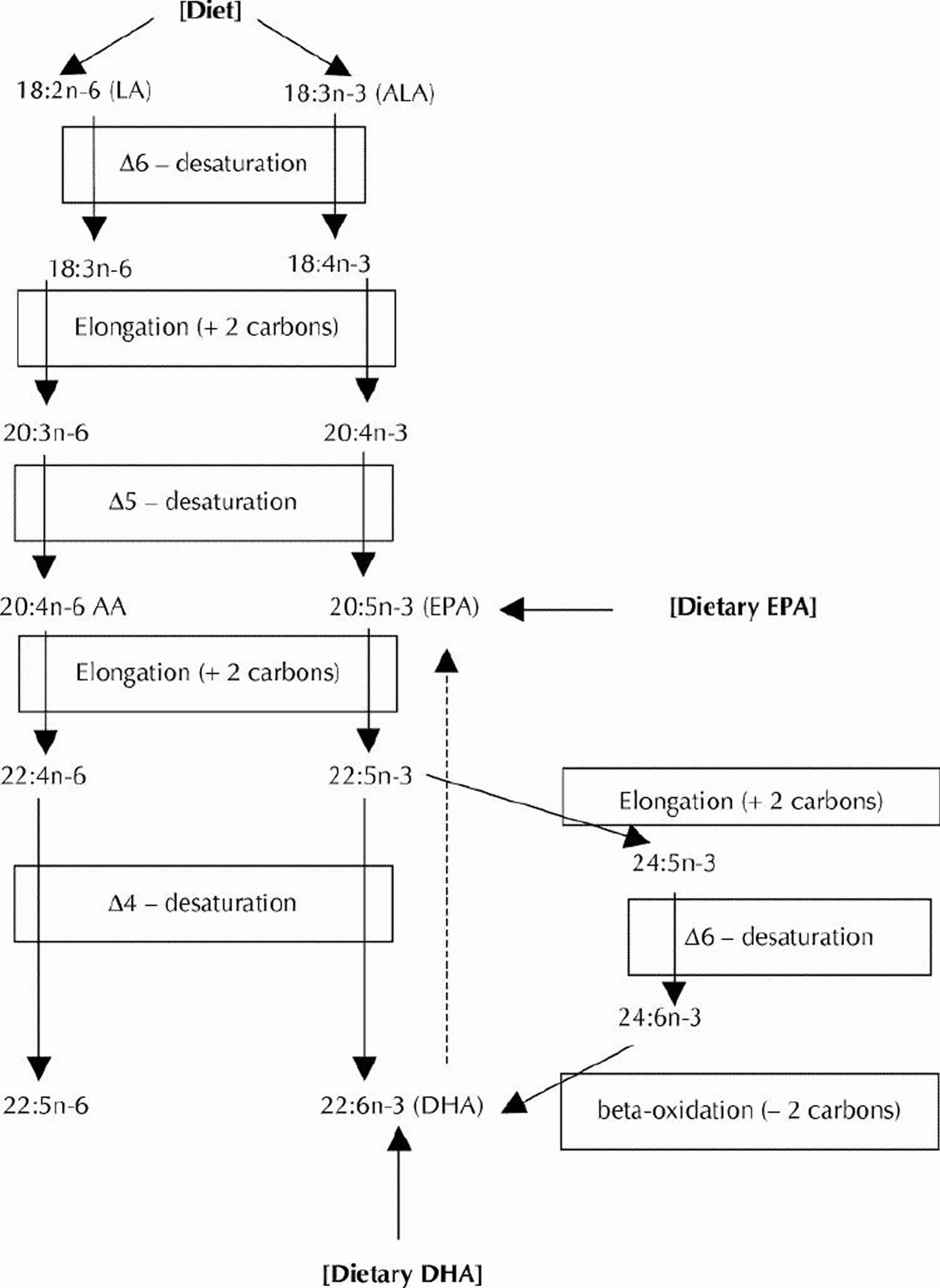
- Figure 2. Conversion of dietary ALA to EPA and DHA via Desaturation, elongation and retroconversion of polyunsaturated fatty acids.
- Flaxseed phytoestrogen
- Flax seed benefits
- Flaxseed side effects and toxicity
What is flaxseed
Flaxseed (Linum usitatissimum) is also known as linseed or flax 1. In North America, flaxseed is the preferred term for flax used in human consumption, whereas Europeans use the term “linseed” for edible flax. In addition to oil content, fatty acid distribution in flaxseed can be affected by environmental conditions. Growing conditions and variety can influence the unsaturated fatty acid content in flaxseed. In contrast, the environment may also have an undesired impact on flaxseed composition. Early and late frosts, heat damage, and drought can have detrimental effects on flaxseed quality 2. Flaxseed has been cultivated over thousands of years and around 500 B.C., Hippocrates wrote about flaxseed being a laxative, and pioneers in North America made flaxseed dressings for cuts and burns 1. Flaxseed is an annual plant that is cultivated in temperate and tropical areas. Fiber from the flaxseed plant is made into linen, and oil from the seed is used in paints, among other products.
The flax seeds, as well as the oil from the seed, are the main components of the plant that are considered to have physiologic properties 3.
Flaxseed can now be made into tablets, extracts, powder, and flour. The oil is also put in capsules. Today, flaxseed and flaxseed oil are used as dietary supplements for constipation, diabetes, cholesterol, cancer, and other conditions.
Flax seed nutrition facts
Table 1. Flax Seed Nutrition Content
Nutrient | Unit | 24 g | Value per 100 g | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Approximates | |||||||||||||||||||
| Energy | kcal | 130 | 542 | ||||||||||||||||
| Protein | g | 4.00 | 16.67 | ||||||||||||||||
| Total lipid (fat) | g | 10.00 | 41.67 | ||||||||||||||||
| Carbohydrate, by difference | g | 7.00 | 29.17 | ||||||||||||||||
| Fiber, total dietary | g | 7.0 | 29.2 | ||||||||||||||||
| Sugars, total | g | 0.00 | 0.00 | ||||||||||||||||
| Minerals | |||||||||||||||||||
| Calcium, Ca | mg | 60 | 250 | ||||||||||||||||
| Iron, Fe | mg | 1.44 | 6.00 | ||||||||||||||||
| Sodium, Na | mg | 5 | 21 | ||||||||||||||||
| Vitamins | |||||||||||||||||||
| Vitamin C, total ascorbic acid | mg | 0.0 | 0.0 | ||||||||||||||||
| Vitamin A, IU | IU | 0 | 0 | ||||||||||||||||
| Lipids | |||||||||||||||||||
| Fatty acids, total saturated | g | 1.001 | 4.170 | ||||||||||||||||
| Fatty acids, total monounsaturated | g | 1.999 | 8.330 | ||||||||||||||||
| Fatty acids, total polyunsaturated | g | 7.001 | 29.170 | ||||||||||||||||
| Fatty acids, total trans | g | 0.000 | 0.000 | ||||||||||||||||
| Cholesterol | mg | 0 | 0 | ||||||||||||||||
Flaxseed fiber
Flaxseed contains a large amount of fiber (28% by weight), and 25% of the fiber is in the soluble form 5, 6, 7. Dietary soluble fiber has been proven to have cholesterol-lowering effects, causing significant decreases in total and LDL cholesterol (−0.045 and −0.057 mmol/L per gram, respectively) 8.
Flaxseed Oil
Major flaxseed oil component – Alpha-linolenic acid (ALA) is one of the most common omega-3 essential fatty acids. In addition to flaxseed being the richest plant source of α-linolenic acid (ALA; 50–62% of flaxseed oil, or ≈22% of whole flaxseed) and lignans (range: 0.2–13.3 mg/g flaxseed), flaxseed is also a good source of dietary fiber (28% by weight), of which 25% is in the soluble form 9, 10, 2. The human body can make most of the types of fats it needs from other fats or raw materials. That isn’t the case for omega-3 fatty acids (also called omega-3 fats and n-3 fats). These are essential fats—the body can’t make them from scratch but must get them from food. Foods high in Omega-3 include fish, vegetable oils, nuts (especially walnuts), flax seeds, flaxseed oil, and leafy vegetables.
Current dietary recommendations for adults suggest a daily intake of 2.22 g of Alpha-linolenic acid (ALA) based on a 2000 kcal diet 11. Ingesting flaxseed can provide ALA to the circulation and tissues of the body. ALA levels are increased as early as two weeks after the initiation of flaxseed supplementation 12. The bioavailability of ALA is dependent on the type of flax ingested – ALA has greater bioavailability in oil than in milled seed, and has greater bioavailability in milled seed than in whole seed 13. Crushing and milling of flaxseed substantially improve the bio-availability of enterolignans 14, likely due to the improved accessibility of the colon bacteria to crushed and ground flaxseed, the dose of flaxseed ingested 15 and the fat composition of the diet. For example, concurrent administration of LA in the diet will reduce ALA accumulation 15 because there is a competition among the enzymes involved in the elongation and desaturation of LA and ALA (Figure 2). A ratio of LA to ALA of 4:1 or lower has been shown to be optimal for the elongation of 11 g ALA to 1 g long-chain ω-3 PUFA 16. The age of the subject does not appear to influence ALA bio-availability or its conversion to DHA 17. The relative bioavailability of enterolignans from flaxseed does not differ in men versus women 14. Approximately 4 g of ALA appears to have biological effects similar to those of 0.3 g of long-chain ω-3 PUFA. Comparatively, EPA and DHA are more rapidly incorporated into plasma and membrane lipids, and produce more rapid effects than ALA. Therefore, the role of ALA in human nutrition may be more important in terms of long-term dietary intake 11.
Table 2. Other sources of Omega-3 Alpha-linolenic acid (ALA) and content of ALA in selected novel sources of omega-3 polyunsaturated fatty acids
| Source of ALA | ALA content, g |
|---|---|
| Pumpkin seeds (1 tbsp) | 0.051 |
| Olive oil (1 tbsp) | 0.103 |
| Walnuts, black (1 tbsp) | 0.156 |
| Soybean oil (1 tbsp) | 1.231 |
| Rapeseed oil (1 tbsp) | 1.302 |
| Walnut oil (1 tbsp) | 1.414 |
| Flaxseeds (1 tbsp) | 2.350 |
| Walnuts, English (1 tbsp) | 2.574 |
| Flaxseed oil (1 tbsp) | 7.249 |
| Almonds (100 g) | 0.4 |
| Peanuts (100 g) | 0.003 |
| Beans, navy, sprouted (100 g) | 0.3 |
| Broccoli, raw (100 g) | 0.1 |
| Lettuce, red leaf (100 g) | 0.1 |
| Mustard (100 g) | 0.1 |
| Purslane (100 g) | 0.4 |
| Spinach (100 g) | 0.1 |
| Seaweed, spirulina, dried (100 g) | 0.8 |
| Beans, common, dry (100 g) | 0.6 |
| Chickpeas, dry (100 g) | 0.1 |
| Soybeans, dry (100 g) | 1.6 |
| Oats, germ (100 g) | 1.4 |
| Rice, bran (100 g) | 0.2 |
| Wheat, germ (100 g) | 0.7 |
| Avocados, California, raw (100 g) | 0.1 |
| Raspberries, raw (100 g) | 0.1 |
| Strawberries, raw (100 g) | 0.1 |
| Novel sources of ALA | ALA content, g |
| Breads and pasta (100 g) | 0.1–1.6 |
| Cereals (and granola bars) (55 g) | 1.0–4.9 |
| Eggs (50 g or 1 egg) | 0.1–0.6 |
| Processed meats (100 g) | 0.5 |
| Salad dressing (14 g – 31 g) | 2.0–4.0 |
| Margarine spreads (10 g – 100 g) | 0.3–1.0 |
| Nutrition bars (50 g) | 0.1–2.2 |
Note: 1 tablespoon (tbsp) oil = 13.6 g; 1 tbsp seeds or nuts = 12.35 g.
This meta-analysis found that flaxseed oil treatment did not significantly reduce total and LDL “bad” cholesterol concentrations compared with the control regimens 19. Such results are consistent with a recent meta-analysis that reported neutral effects of Alpha-linolenic acid (ALA) on total and LDL cholesterol compared with the control arms 20. One of the plausible explanations for the null findings is that the effects of flaxseed oil may have been masked by the use of monounsaturated fatty acid (MUFA) or Omega-6 (polyunsaturated fatty acid) PUFA–enriched oils as the control regimen in these studies. Previous studies have indeed shown that dietary replacement of MUFAs or n−6 PUFAs for saturated fatty acids also has a cholesterol-lowering effect 21, 22. It was noticed that flaxseed oil treatment induced a modest but nonsignificant decrease in total and LDL cholesterol compared with baseline values (data not shown). Prospective epidemiologic studies also reported a reduced relative risk of coronary heart disease when saturated or trans fatty acids were replaced with Omega-3 Alpha-linolenic acid 23. Taken together and those of others 24 indicate that the effect of Omega-3 Alpha-linolenic acid (ALA) on blood lipids is similar to that of MUFAs or n−6 PUFAs, and whether replacement of Omega-3 Alpha-linolenic acid (ALA) for saturated or trans fatty acids could lower blood lipids remains to be elucidated. Nevertheless, flaxseed oil has consistently been found to induce a significant increase in the proportion of Omega-3 fatty acids in the plasma or erythrocyte membranes and a decrease in the ratio of Omega-6 to Omega-3 fatty acid, which may have other benefits for cardiovascular disease 25. However, the long-term consequences of such an effect remain unclear.
What are omega-3 fatty acids ?
Omega-3 fatty acids are long-chain polyunsaturated fatty acids (18–22 carbon atoms in chain length) with the first of many double bonds beginning with the third carbon atom (when counting from the methyl end of the fatty acid molecule). The three principal omega-3 fatty acids are:
- Alpha-linolenic acid (ALA) (18:3ω-3),
- Eicosapentaenoic acid (EPA) (20:5ω-3),
- Docosahexaenoic acid (DHA) (22:6ω-3).
Non-fish oil based Omega-3 Polyunsaturated Fatty Acids
The main sources of alpha-linolenic acid (ALA) in the U.S. diet are vegetable oils, particularly canola and soybean oils; flaxseed oil is richer in alpha-linolenic acid (ALA) than soybean and canola oils but is not commonly consumed. The typical North American diet provides approximately 1.4 g of ALA per day, and 0.1 g to 0.2 g of EPA and DHA 26. Alpha-linolenic acid (ALA) can be converted, usually in small amounts, into (Eicosapentaenoic acid) EPA and (Docosahexaenoic acid) DHA in the body. EPA and DHA are found in seafood, including fatty fish (e.g., salmon, tuna, and trout) and shellfish (e.g., crab, mussels, and oysters). Note the differences between the Omega-3 fatty acids found in flaxseed, soybean, vegetable oils (alpha-linolenic acid (ALA)) from those in fish and seafoods (Eicosapentaenoic acid (EPA) and Docosahexaenoic acid (DHA)).
For those who do not consume fish, the omega-3 fatty acid known as alpha-linolenic acid (ALA) can be a dietary source of some metabolically derived Eicosapentaenoic acid (EPA) and Docosahexaenoic acid (DHA). The desaturation plus elongation reactions in the liver and elsewhere in the body that provide for the conversion of dietary ALA to EPA and DHA are depicted in Figure 2. The conversion of ALA to EPA and DHA occurs to a low extent (about 10%–15% efficiency) in the adult human body 27. Nonetheless, there is evidence that the benefits of the Mediterranean-type diet after myocardial infarction may be partly caused by the higher intake of ALA (commonly found in nonhydrogenated canola oil, ground flaxseed and other selected ALA-enriched foods) 28. A prospective cohort study (Nurses Health Study) revealed an inverse relation between ALA intakes and the risk of fatal ischemic heart disease among women 29. However, the Zutphen Elderly Study did not observe a beneficial effect of dietary ALA on the 10-year risk of coronary artery disease 30. The metabolic conversion of ALA to the longer chain omega-3 fatty acids (EPA and DHA) is thought to mediate any possible cardioprotective effects of dietary ALA. In contrast to the well-recognized serum triglyceride-lowering effect of EPA and DHA, most human intervention studies with ALA (e.g., using flaxseed oil) have not exhibited any lipid-lowering effects. Whereas ALA (from flaxseed oil) at a relatively high dose has been found to improve arterial compliance 31, considerably lower supplementation levels of EPA and DHA improved arterial and endothelial functioning in subjects with hypercholesterolemia 32 and subjects with type 2 diabetes mellitus 33.
Figure 1. Omega-3 fatty acids and Omega-6 fatty acids structure
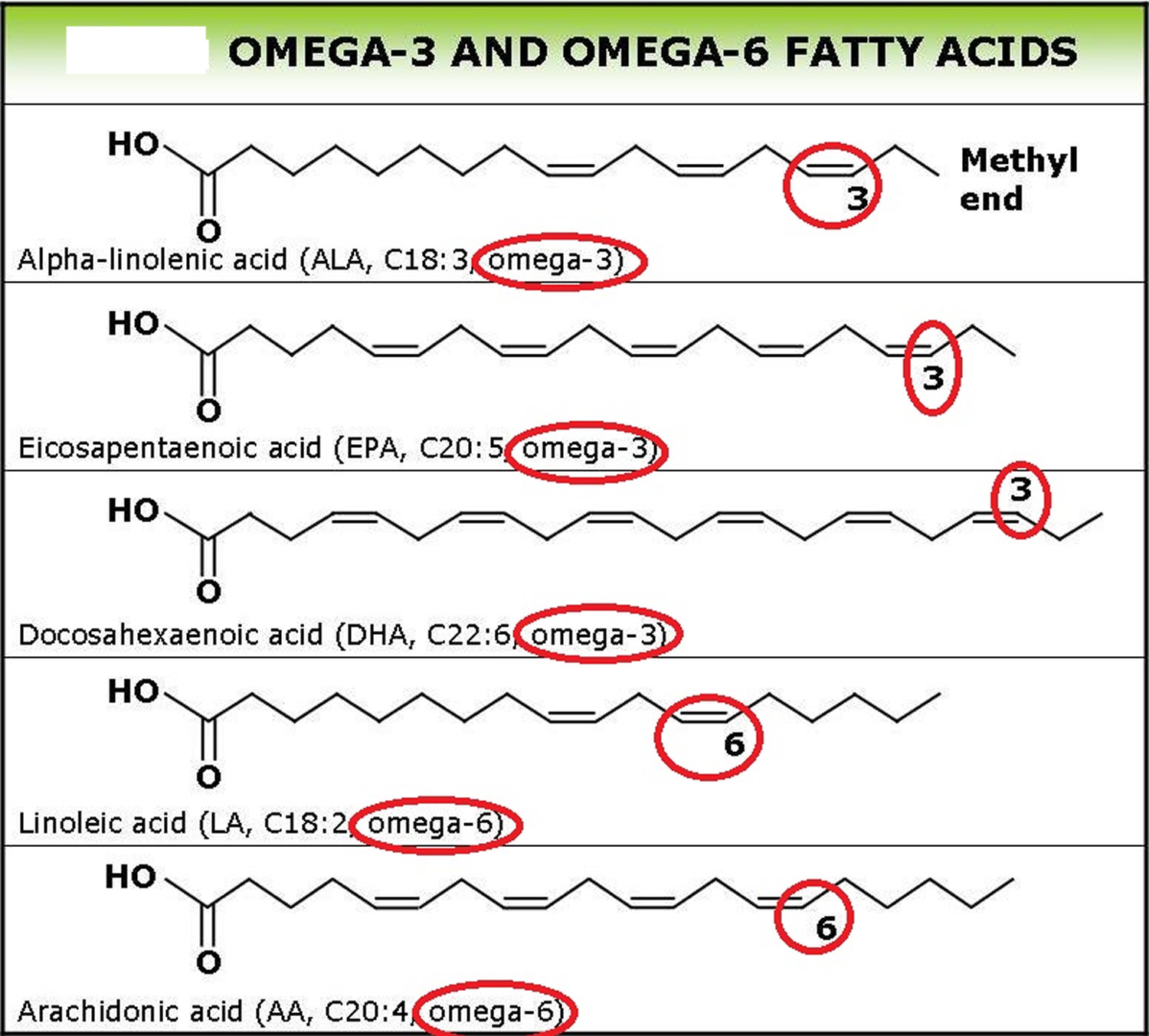
Figure 2. Conversion of dietary ALA to EPA and DHA via Desaturation, elongation and retroconversion of polyunsaturated fatty acids.
Flaxseed phytoestrogen
Phytoestrogens are naturally occurring compounds that are found in plants and in most foods of plant origin. Phytoestrogens consist mainly of isoflavones, which are found in high concentrations in soy and legumes, and lignans, which are found in a variety of fruits, vegetables, and cereal products. Because phytoestrogens have a chemical structure that is similar to that of 17 β-estradiol, they may compete with estrogens for binding to estrogen receptors and in so doing, may act as weak estrogen agonists or antagonists 35. Therefore, phytoestrogens have been hypothesized to behave like selective estrogen receptor modulators and to play a role in the chemoprevention of breast cancer 35. However, despite 15 years of epidemiologic research, the possible association between dietary intake of phytoestrogens and the risk of breast cancer remains unclear. Initially, results from international comparisons and studies of migrant populations gave rise to the hypothesis that higher intakes of soy, a primary source of isoflavones, might be associated with a decreased risk of breast cancer 36, 37. Subsequent case–control and cohort studies 38 conducted in Asia generally confirmed that a high consumption of soy-based foods and isoflavones is associated with a lower risk of premenopausal breast cancer, especially if exposure occurs early in life, for instance, during adolescence. However, studies conducted in North America and Europe have been less conclusive than the Asian studies 38.
Flaxseed is the richest source of lignans, which is one of three major classes of phytoestrogens. The lignans associated with flaxseed are primarily secoisolariciresinol, the essential fatty acid alpha-linolenic acid (ALA), (which is a biologic precursor to omega 3 fatty acids), as well as fiber. Lignans are thought to have estrogen agonist and antagonist effects as well as antioxidant properties. Flaxseed and its lignans may have potent anti-estrogenic effects on estrogen receptor-positive breast cancer and may have benefits in breast cancer prevention efforts 39, 40. Lignans are converted by colonic bacteria to enterodiol and enterolactone which are metabolites believed to have important physiologic properties such as decreased cell proliferation and inhibition of aromatase, 5 alpha reductase and 17 beta hydroxysteroid activity.
Flax seed benefits
Flaxseed and constipation
Flaxseed contains fiber, which generally helps with constipation. However, there’s little research on the effectiveness of flaxseed for constipation 41.
Flaxseed and Diabetes
Djoussé et al 42 studied 3993 nondiabetic subjects and found that a higher consumption of ALA was associated with higher plasma insulin, but not glucose levels. The authors suggested that plant-based ω-3 fatty acids might influence insulin secretion in vivo, and improve glucose use and efficiency. Studies in animal models of diabetes mellitus have shown that SDG from flaxseed can prevent the development of type 1 diabetes by approximately 71% and type 2 diabetes by 80%. Pan et al 43 reported more modest but statistically significant improvements in glycemic control in type 2 diabetic patients treated for 12 weeks with 360 mg/day of flaxseed-derived lignan supplement. Das 44 has proposed that a defect in the activity of delta-6 and delta-5 desaturases may be a factor that predisposes individuals to the development of insulin resistance syndrome because long-chain PUFAs can increase cell membrane fluidity, enhance the number of insulin receptors and the affinity of insulin to its receptors; suppress TNF-α, IL-6, macrophage migration inhibitory factor and leptin synthesis; increase the number of glucose transporter type 4 receptors; serve as endogenous ligands of peroxisome proliferator-activated receptors; modify lipolysis; and regulate the balance between pro- and antioxidants.
Ingestion of flaxseed or ALA may help in preventing or treating a variety of diabetic complications. For example, in 1062 adults older than 40 years of age with self-reported diagnosed diabetes, Tao et al 45 found that dietary intake of ALA (greater than 2.11 g/day) was positively associated with lower odds of peripheral neuropathy. In an animal model, Velasquez et al 46 reported that flaxseed meals reduced proteinuria and ameliorated nephropathy in type 2 diabetes mellitus. In type 2 diabetic patients, 5 g/day of flaxseed oil consumption has been associated with a significant reduction of plasmin alpha-2-plasmin inhibitor complex level, plasminogen activator inhibitor-1 activity and thrombin antithrombin III complex level after two weeks of intervention 47. Because diabetic patients are more likely to develop thrombotic events, these findings have important clinical implications.
Flaxseed and flaxseed oil and Cholesterol
Studies of flaxseed and flaxseed oil to lower cholesterol levels have had mixed results. A 2009 research review found that flaxseed lowered cholesterol only in people with relatively high initial cholesterol levels 48.
Human studies have shown that flaxseed can modestly reduce serum total and low-density lipoprotein cholesterol concentrations, reduce postprandial glucose absorption, decrease some markers of inflammation, and raise serum levels of the omega-3 fatty acids, ALA and eicosapentaenoic acid 9. Data on the antiplatelet, antioxidant, and hypotensive effects of flaxseed, however, are inconclusive. More research is needed to define the role of this functional food in reducing cardiovascular risk.
Recently, Patade et al 49 found that mild to moderate hypercholesterolemic Native American postmenopausal women who consumed flaxseed (30 g/day) for three months exhibited a reduction of total cholesterol by 7% and LDL cholesterol by 10% without changes in HDL cholesterol or triglyceride concentrations. Zhang et al 50 also found significant reductions in total cholesterol (22%) and LDL cholesterol levels (24%) in hypercholesterolemic subjects after an eight-week dietary supplementation with 600 mg/day of secoisolariciresinol diglucoside, a lignan derived from flaxseed. These results suggest that specific subgroups of patients could obtain more beneficial hypolipemic effects from flaxseed or its components. In general, flaxseed-enriched diets have been reported to induce anywhere from 0% to 18% decreases in LDL and 0% to 11% decreases in total cholesterol 6. With only one exception that reported a 16% decrease in HDL concentrations in men 51, most studies reported no changes in HDL levels in response to dietary flax-seed 52, 53, 54.
This study showed whole flaxseed supplementation was associated with a decrease in blood total and LDL “bad” cholesterol concentrations, but did not substantially affect HDL “good” cholesterol and triglycerides. These changes varied substantially depending on the treatment form of flaxseed, quality of the study, sex, and initial lipid profile of the subjects 19. The results showed that whole flaxseed interventions were associated with significant reductions in total and LDL cholesterol, whereas flaxseed oil interventions were not 19. The daily doses used in the flaxseed interventions included in this study ranged from 20.0 to 50.0 g/d (median dose: 38.0 g). Therefore, estimates of the effect of the soluble fiber on total and LDL cholesterol were calculated as −0.12 and −0.15 mmol/L, respectively. Additionally, flaxseed is one of the richest sources of dietary lignans (range: 0.2–13.3 mg/g) and purified lignans also have been shown to reduce total and LDL cholesterol in animal studies 55, 56. Human data, however, are still limited; only 5 studies have used lignan supplements and they all show no effects of flaxseed lignan on lipids but significant improvements in glycemic control in type 2 diabetic patients without apparently affecting fasting glucose, lipid profiles and insulin sensitivity 57, 58, 59, 60, 61. Moreover, the results were largely determined by one of the studies 61 that showed plasma concentrations of secoisolariciresinol, enterodiol and enterolactone were all significantly raised in the groups supplemented with flaxseed lignan. The observed cholesterol-lowering values were correlated with the concentrations of plasma secoisolariciresinol and enterodiol . In conclusion that study showed dietary flaxseed lignan extract decreased plasma cholesterol and glucose concentrations in a dose-dependent manner 61.
Flaxseed and Hot Flushes in post-menopausal women
Flaxseed doesn’t decrease hot flashes, studies from 2010 and 2012 suggest 62, 63, 64.
Flaxseed and obesity.
Because of its high fat content, it is possible that flaxseed supplementation will induce weight gain. However, dietary flaxseed intervention studies 65, 66 have not found any evidence of weight gain or changes in body mass index after supplementation.
Flaxseed and High Blood Pressure
In the National NHLBI Family Heart Study 67, Djoussé et al found that dietary ALA was associated with a lower prevalence of hypertension and lower systolic blood pressure in 4594 subjects. Others 68, 69 have confirmed that dietary ALA is associated with lower blood pressure values. ALA may lower blood pressure by acting as a precursor for eicosanoids, which can generate the production of prostaglandins and leukotrienes that may reduce vascular tone 70.
In a study, people who added 30 grams of milled flaxseed to their diet every day for six months saw their systolic blood pressure (the top number in a blood pressure reading) drop an average 15 mm Hg and their diastolic blood pressure (the bottom number) an average 8 mm Hg. By comparison, people who got a “dummy” supplement called a placebo had slightly increased systolic blood pressure while diastolic pressure remained steady. The researchers said the level of blood pressure decrease from adding flaxseed could result in 50 percent less strokes and 30 percent less heart attacks 71.
Studies on high blood pressure using flaxseed as a source of ALA are inconclusive. Paschos et al 72 have reported that 12 weeks of dietary flaxseed supplementation (8 g/day of ALA) resulted in a significant decrease in systolic and diastolic blood pressure in dyslipidemic patients. Conversely, Stuglin and Prasad 73 found no changes in blood pressure in a shorter four-week intervention using 32.7 g/day of total flaxseed. However, their study examined healthy men and may indicate that pathological conditions are required to detect significant changes in high blood pressure.
The mechanism for any change in blood pressure is unclear. However, shorter studies using healthy individuals, obese subjects or dyslipidemic patients may provide some insight. Administration of 8 g of ALA/day to dyslipidemic men or 20 g/day of flax oil containing ALA to obese adults with markers of insulin resistance has resulted in significant decreases in systolic, diastolic and mean arterial blood pressure 72, 74. Systemic arterial compliance was also improved significantly 74. This would agree well with experimental work in which Dupasquier et al 75 found that a flaxseed-supplemented, ALA-rich diet (12.5 g of flaxseed/day; ALA comprises 70% of total fatty acids) preserved vascular relaxation from the deleterious effects that an atherogenic, high-cholesterol diet can induce. These results would suggest that ALA may directly induce beneficial vascular effects.
- The US National Center for Complementary and Integrative Health is funding preliminary research on the potential role of substances in flaxseed for ovarian cancer, cardiovascular disease, metabolic syndrome, diabetes, asthma, and inflammation 1.
Flaxseed side effects and toxicity
- Don’t eat raw or unripe flaxseeds, which may contain potentially toxic compounds.
- Flaxseed and flaxseed oil supplements seem to be well tolerated in limited amounts. Few side effects have been reported. Common side effects were for whole flaxseed and flaxseed oil preparations which induced adverse gastrointestinal effects within 4 weeks 13. Moreover. milled flaxseed has been shown to be free of any adverse reactions 13.
- Avoid flaxseed and flaxseed oil during pregnancy as they may have mild hormonal effects. There’s little reliable information on whether it’s safe to use flaxseed when nursing.
- Flaxseed, like any fiber supplement, should be taken with plenty of water, as it could worsen constipation or, in rare cases, cause an intestinal blockage.
- Both flaxseed and flaxseed oil can cause diarrhea.
- U.S. Department of Health & Human Services. National Center for Complementary and Integrative Health. Flaxseed and Flaxseed Oil. https://nccih.nih.gov/health/flaxseed/ataglance.htm[↩][↩][↩]
- Hall C, III, Tulbek MC, Xu Y. Flaxseed. Adv Food Nutr Res 2006;51:1–97. https://www.ncbi.nlm.nih.gov/pubmed/17011474[↩][↩]
- Flax and flaxseed oil (Linum usitatissimum): a review by the Natural Standard Research Collaboration. Basch E, Bent S, Collins J, Dacey C, Hammerness P, Harrison M, Smith M, Szapary P, Ulbricht C, Vora M, Weissner W, Natural Standard Resource Collaboration. J Soc Integr Oncol. 2007 Summer; 5(3):92-105. https://www.ncbi.nlm.nih.gov/pubmed/17761128/[↩]
- United States Department of Agriculture, Agriculture Research Service. USDA Food Composition Databases. https://ndb.nal.usda.gov/ndb/[↩]
- Thompson LU, Cunnane SC. Flaxseed in human nutrition. 2nd ed. Champaign, IL: AOCS Publishing, 2003.[↩]
- Flaxseed and cardiovascular risk. Bloedon LT, Szapary PO. Nutr Rev. 2004 Jan; 62(1):18-27. https://www.ncbi.nlm.nih.gov/pubmed/14995053/[↩][↩]
- Flaxseed. Hall C 3rd, Tulbek MC, Xu Y. Adv Food Nutr Res. 2006; 51():1-97. https://www.ncbi.nlm.nih.gov/pubmed/17011474/[↩]
- Cholesterol-lowering effects of dietary fiber: a meta-analysis. Brown L, Rosner B, Willett WW, Sacks FM. Am J Clin Nutr. 1999 Jan; 69(1):30-42. http://ajcn.nutrition.org/content/69/1/30.long[↩]
- Bloedon LT, Szapary PO. Flaxseed and cardiovascular risk. Nutr Rev 2004;62:18–27. https://www.ncbi.nlm.nih.gov/pubmed/14995053[↩][↩]
- Muir AD. Flax lignans—analytical methods and how they influence our understanding of biological activity. J AOAC Int 2006;89:1147–57. https://www.ncbi.nlm.nih.gov/pubmed/16915858[↩]
- Human requirement for N-3 polyunsaturated fatty acids. Simopoulos AP. Poult Sci. 2000 Jul; 79(7):961-70. https://www.ncbi.nlm.nih.gov/pubmed/10901194/[↩][↩]
- Supplementing lactating women with flaxseed oil does not increase docosahexaenoic acid in their milk. Francois CA, Connor SL, Bolewicz LC, Connor WE. Am J Clin Nutr. 2003 Jan; 77(1):226-33. http://ajcn.nutrition.org/content/77/1/226.long[↩]
- Bioavailability of alpha-linolenic acid in subjects after ingestion of three different forms of flaxseed. Austria JA, Richard MN, Chahine MN, Edel AL, Malcolmson LJ, Dupasquier CM, Pierce GN. J Am Coll Nutr. 2008 Apr; 27(2):214-21. https://www.ncbi.nlm.nih.gov/pubmed/18689552/[↩][↩][↩]
- The relative bioavailability of enterolignans in humans is enhanced by milling and crushing of flaxseed. Kuijsten A, Arts IC, van’t Veer P, Hollman PC. J Nutr. 2005 Dec; 135(12):2812-6. https://www.ncbi.nlm.nih.gov/pubmed/16317125/[↩][↩]
- Distribution, interconversion, and dose response of n-3 fatty acids in humans. Arterburn LM, Hall EB, Oken H. Am J Clin Nutr. 2006 Jun; 83(6 Suppl):1467S-1476S. https://www.ncbi.nlm.nih.gov/pubmed/16841856/[↩][↩]
- Indu M, Ghafoorunissa N-3 fatty acids in Indian diets – comparison of the effects of precursor (alpha-linolenic acid) vs product (long chain n-3 polyunsaturated fatty acids) Nutr Res. 1992;12:569–82.[↩]
- Bioavailability of alpha-linolenic acid from flaxseed diets as a function of the age of the subject. Patenaude A, Rodriguez-Leyva D, Edel AL, Dibrov E, Dupasquier CM, Austria JA, Richard MN, Chahine MN, Malcolmson LJ, Pierce GN. Eur J Clin Nutr. 2009 Sep; 63(9):1123-9. https://www.ncbi.nlm.nih.gov/pubmed/19584895/[↩]
- Rodriguez-Leyva D, Bassett CM, McCullough R, Pierce GN. The cardiovascular effects of flaxseed and its omega-3 fatty acid, alpha-linolenic acid. The Canadian Journal of Cardiology. 2010;26(9):489-496. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2989356/[↩]
- Pan A, Yu D, Demark-Wahnefried W, Franco OH, Lin X. Meta-analysis of the effects of flaxseed interventions on blood lipids. The American Journal of Clinical Nutrition. 2009;90(2):288-297. doi:10.3945/ajcn.2009.27469. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3361740/[↩][↩][↩]
- Wendland E, Farmer A, Glasziou P, Neil A. Effect of α linolenic acid on cardiovascular risk markers: a systematic review. Heart 2006;92:166–9. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1860766/[↩]
- Fernandez ML, West KL. Mechanisms by which dietary fatty acids modulate plasma lipids. J Nutr 2005;135:2075–8. http://jn.nutrition.org/content/135/9/2075.long[↩]
- Harris WS. n−3 fatty acids and serum lipoproteins: human studies. Am J Clin Nutr 1997;65:1645S–54S. https://www.ncbi.nlm.nih.gov/pubmed/9129504[↩]
- Hu FB, Stampfer MJ, Manson JE, et al. Dietary fat intake and the risk of coronary heart disease in women. N Engl J Med 1997;337:1491–9. http://www.nejm.org/doi/full/10.1056/NEJM199711203372102[↩]
- Wendland E, Farmer A, Glasziou P, Neil A. Effect of α linolenic acid on cardiovascular risk markers: a systematic review. Heart. 2006;92(2):166-169. doi:10.1136/hrt.2004.053538. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1860766/[↩]
- Simopoulos AP. The importance of the omega-6/omega-3 fatty acid ratio in cardiovascular disease and other chronic diseases. Exp Biol Med (Maywood) 2008;233:674–88. https://www.ncbi.nlm.nih.gov/pubmed/18408140[↩]
- Dietary intakes of omega-6 and omega-3 polyunsaturated fatty acids and the risk of breast cancer. Thiébaut AC, Chajès V, Gerber M, Boutron-Ruault MC, Joulin V, Lenoir G, Berrino F, Riboli E, Bénichou J, Clavel-Chapelon F. Int J Cancer. 2009 Feb 15; 124(4):924-31. https://www.ncbi.nlm.nih.gov/pubmed/19035453/[↩]
- Dietary linoleic acid influences desaturation and acylation of deuterium-labeled linoleic and linolenic acids in young adult males. Emken EA, Adlof RO, Gulley RM. Biochim Biophys Acta. 1994 Aug 4; 1213(3):277-88. https://www.ncbi.nlm.nih.gov/pubmed/7914092/[↩]
- Mediterranean diet, traditional risk factors, and the rate of cardiovascular complications after myocardial infarction: final report of the Lyon Diet Heart Study. de Lorgeril M, Salen P, Martin JL, Monjaud I, Delaye J, Mamelle N. Circulation. 1999 Feb 16; 99(6):779-85. https://www.ncbi.nlm.nih.gov/pubmed/9989963/[↩]
- Dietary intake of alpha-linolenic acid and risk of fatal ischemic heart disease among women. Hu FB, Stampfer MJ, Manson JE, Rimm EB, Wolk A, Colditz GA, Hennekens CH, Willett WC. Am J Clin Nutr. 1999 May; 69(5):890-7. http://ajcn.nutrition.org/content/69/5/890.long[↩]
- alpha-Linolenic acid intake is not beneficially associated with 10-y risk of coronary artery disease incidence: the Zutphen Elderly Study. Oomen CM, Ocké MC, Feskens EJ, Kok FJ, Kromhout D. Am J Clin Nutr. 2001 Oct; 74(4):457-63. http://ajcn.nutrition.org/content/74/4/457.long[↩]
- Arterial compliance in obese subjects is improved with dietary plant n-3 fatty acid from flaxseed oil despite increased LDL oxidizability. Nestel PJ, Pomeroy SE, Sasahara T, Yamashita T, Liang YL, Dart AM, Jennings GL, Abbey M, Cameron JD. Arterioscler Thromb Vasc Biol. 1997 Jun; 17(6):1163-70. http://atvb.ahajournals.org/content/17/6/1163.long[↩]
- Dietary supplementation with marine omega-3 fatty acids improve systemic large artery endothelial function in subjects with hypercholesterolemia. Goodfellow J, Bellamy MF, Ramsey MW, Jones CJ, Lewis MJ. J Am Coll Cardiol. 2000 Feb; 35(2):265-70. https://www.ncbi.nlm.nih.gov/pubmed/10676668/[↩]
- Fish oil improves arterial compliance in non-insulin-dependent diabetes mellitus. McVeigh GE, Brennan GM, Cohn JN, Finkelstein SM, Hayes RJ, Johnston GD. Arterioscler Thromb. 1994 Sep; 14(9):1425-9. http://atvb.ahajournals.org/content/14/9/1425.long[↩]
- Holub BJ. Clinical nutrition: 4. Omega-3 fatty acids in cardiovascular care. Hoffer LJ, Jones PJ, eds. CMAJ: Canadian Medical Association Journal. 2002;166(5):608-615. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC99405/[↩]
- Clinical review 97: Potential health benefits of dietary phytoestrogens: a review of the clinical, epidemiological, and mechanistic evidence. Tham DM, Gardner CD, Haskell WL. J Clin Endocrinol Metab. 1998 Jul; 83(7):2223-35. https://www.ncbi.nlm.nih.gov/pubmed/9661587/[↩][↩]
- Rapidly rising breast cancer incidence rates among Asian-American women. Deapen D, Liu L, Perkins C, Bernstein L, Ross RK. Int J Cancer. 2002 Jun 10; 99(5):747-50. https://www.ncbi.nlm.nih.gov/pubmed/12115511/[↩]
- Migration patterns and breast cancer risk in Asian-American women. Ziegler RG, Hoover RN, Pike MC, Hildesheim A, Nomura AM, West DW, Wu-Williams AH, Kolonel LN, Horn-Ross PL, Rosenthal JF, Hyer MB. J Natl Cancer Inst. 1993 Nov 17; 85(22):1819-27. https://www.ncbi.nlm.nih.gov/pubmed/8230262/[↩]
- Meta-analysis of soy intake and breast cancer risk. Trock BJ, Hilakivi-Clarke L, Clarke R. J Natl Cancer Inst. 2006 Apr 5; 98(7):459-71. https://www.ncbi.nlm.nih.gov/pubmed/16595782/[↩][↩]
- Flaxseed and its lignans inhibit estradiol-induced growth, angiogenesis, and secretion of vascular endothelial growth factor in human breast cancer xenografts in vivo. Bergman Jungeström M, Thompson LU, Dabrosin C. Clin Cancer Res. 2007 Feb 1; 13(3):1061-7. http://clincancerres.aacrjournals.org/content/13/3/1061.long[↩]
- Touillaud MS, Thiébaut ACM, Fournier A, Niravong M, Boutron-Ruault M-C, Clavel-Chapelon F. Dietary lignan intake and postmenopausal breast cancer risk by estrogen and progesterone receptor status. Journal of the National Cancer Institute. 2007;99(6):475-486. doi:10.1093/jnci/djk096. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2292813/[↩]
- Thompson LU, Mason JK. Flaxseed. In: Coates PM, Betz JM, Blackman MR, et al., eds. Encyclopedia of Dietary Supplements, 2nd ed. New York, NY: Informa Healthcare; 2010:274-287.[↩]
- Dietary linolenic acid and fasting glucose and insulin: the National Heart, Lung, and Blood Institute Family Heart Study. Djoussé L, Hunt SC, Tang W, Eckfeldt JH, Province MA, Ellison RC. Obesity (Silver Spring). 2006 Feb; 14(2):295-300. https://www.ncbi.nlm.nih.gov/pubmed/16571856/[↩]
- Effects of a flaxseed-derived lignan supplement in type 2 diabetic patients: a randomized, double-blind, cross-over trial. Pan A, Sun J, Chen Y, Ye X, Li H, Yu Z, Wang Y, Gu W, Zhang X, Chen X, Demark-Wahnefried W, Liu Y, Lin X. PLoS One. 2007 Nov 7; 2(11):e1148. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2048577/[↩]
- A defect in the activity of Delta6 and Delta5 desaturases may be a factor predisposing to the development of insulin resistance syndrome. Das UN. Prostaglandins Leukot Essent Fatty Acids. 2005 May; 72(5):343-50. https://www.ncbi.nlm.nih.gov/pubmed/15850715/[↩]
- Relationship of polyunsaturated fatty acid intake to peripheral neuropathy among adults with diabetes in the National Health and Nutrition Examination Survey (NHANES) 1999 2004. Tao M, McDowell MA, Saydah SH, Eberhardt MS. Diabetes Care. 2008 Jan; 31(1):93-5. https://www.ncbi.nlm.nih.gov/pubmed/17914029/[↩]
- Dietary flaxseed meal reduces proteinuria and ameliorates nephropathy in an animal model of type II diabetes mellitus. Velasquez MT, Bhathena SJ, Ranich T, Schwartz AM, Kardon DE, Ali AA, Haudenschild CC, Hansen CT. Kidney Int. 2003 Dec; 64(6):2100-7. https://www.ncbi.nlm.nih.gov/pubmed/14633132/[↩]
- Effect of alpha-linolenic acid-containing linseed oil on coagulation in type 2 diabetes. Tohgi N. Diabetes Care. 2004 Oct; 27(10):2563-4. https://www.ncbi.nlm.nih.gov/pubmed/15451940/[↩]
- Pan A, Yu D, Demark-Wahnefried W, et al. Meta-analysis of the effects of flaxseed interventions on blood lipids. American Journal of Clinical Nutrition. 2009;90(2):288-297. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3361740/[↩]
- Flaxseed reduces total and LDL cholesterol concentrations in Native American postmenopausal women. Patade A, Devareddy L, Lucas EA, Korlagunta K, Daggy BP, Arjmandi BH. J Womens Health (Larchmt). 2008 Apr; 17(3):355-66. https://www.ncbi.nlm.nih.gov/pubmed/18328014/[↩]
- Dietary flaxseed lignan extract lowers plasma cholesterol and glucose concentrations in hypercholesterolaemic subjects. Zhang W, Wang X, Liu Y, Tian H, Flickinger B, Empie MW, Sun SZ. Br J Nutr. 2008 Jun; 99(6):1301-9. https://www.ncbi.nlm.nih.gov/pubmed/18053310/[↩]
- Flaxseed and cardiovascular risk factors: results from a double blind, randomized, controlled clinical trial. Bloedon LT, Balikai S, Chittams J, Cunnane SC, Berlin JA, Rader DJ, Szapary PO. J Am Coll Nutr. 2008 Feb; 27(1):65-74. https://www.ncbi.nlm.nih.gov/pubmed/18460483/[↩]
- Arjmandi BH, Khan DA, Juma S. Whole flaxseed consumption lowers serum LDL-cholesterol and lipoprotein(a) concentrations in postmenopausal women. Nutr Res. 1998;18:1203–14.[↩]
- Flaxseed improves lipid profile without altering biomarkers of bone metabolism in postmenopausal women. Lucas EA, Wild RD, Hammond LJ, Khalil DA, Juma S, Daggy BP, Stoecker BJ, Arjmandi BH. J Clin Endocrinol Metab. 2002 Apr; 87(4):1527-32. https://www.ncbi.nlm.nih.gov/pubmed/11932276/[↩]
- Flaxseed dietary supplement versus hormone replacement therapy in hypercholesterolemic menopausal women. Lemay A, Dodin S, Kadri N, Jacques H, Forest JC. Obstet Gynecol. 2002 Sep; 100(3):495-504. https://www.ncbi.nlm.nih.gov/pubmed/12220769/[↩]
- Regression of hypercholesterolemic atherosclerosis in rabbits by secoisolariciresinol diglucoside isolated from flaxseed. Prasad K. Atherosclerosis. 2008 Mar; 197(1):34-42. https://www.ncbi.nlm.nih.gov/pubmed/17904562/[↩]
- Reduction of serum cholesterol and hypercholesterolemic atherosclerosis in rabbits by secoisolariciresinol diglucoside isolated from flaxseed. Prasad K. Circulation. 1999 Mar 16; 99(10):1355-62. https://www.ncbi.nlm.nih.gov/pubmed/10077521/[↩]
- Cornish SM, Chilibeck PD, Paus-Jennsen L, et al. A randomized controlled trial of the effects of flaxseed lignan complex on metabolic syndrome composite score and bone mineral in older adults. Appl Physiol Nutr Metab 2009;34:89–98. http://www.nrcresearchpress.com/doi/full/10.1139/H08-142[↩]
- Hallund J, Ravn-Haren G, Bugel S, Tholstrup T, Tetens I. A lignan complex isolated from flaxseed does not affect plasma lipid concentrations or antioxidant capacity in healthy postmenopausal women. J Nutr 2006;136:112–6. http://jn.nutrition.org/content/136/1/112.long[↩]
- Marblestone B. The effects of flaxseed SDG on perimenopausal women with mild hyperlipidemia. San Diego, CA: University of San Diego, 2008[↩]
- Pan A, Sun J, Chen Y, et al. Effects of a flaxseed-derived lignan supplement in type 2 diabetic patients: a randomized, double-blind, cross-over trial. PLoS One 2007;2:e1148. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2048577/[↩]
- Zhang W, Wang X, Liu Y, et al. Dietary flaxseed lignan extract lowers plasma cholesterol and glucose concentrations in hypercholesterolaemic subjects. Br J Nutr 2008;99:1301–9. https://www.ncbi.nlm.nih.gov/pubmed/18053310[↩][↩][↩]
- Colli MC, Bracht A, Soares AA, et al. Evaluation of the efficacy of flaxseed meal and flaxseed extract in reducing menopausal symptoms. Journal of Medicinal Food. 2012;15(9):840-845. https://www.ncbi.nlm.nih.gov/pubmed/22925074[↩]
- Pruthi S, Qin R, Terstreip SA, et al. A phase III, randomized, placebo-controlled, double-blind trial of flaxseed for the treatment of hot flashes: North Central Cancer Treatment Group N08C7. Menopause. 2012;19(1):48-53. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3246070/[↩]
- Simbalista RL, Sauerbronn AV, Aldrighi JM, et al. Consumption of a flaxseed-rich food is not more effective than a placebo in alleviating the climacteric symptoms of postmenopausal women. Journal of Nutrition. 2010;140(2):293-297. http://jn.nutrition.org/content/140/2/293.long[↩]
- Inflammatory markers are not altered by an eight week dietary alpha-linolenic acid intervention in healthy abdominally obese adult males and females. Nelson TL, Stevens JR, Hickey MS. Cytokine. 2007 May; 38(2):101-6. https://www.ncbi.nlm.nih.gov/pubmed/17613244/[↩]
- Systemic inflammation in morbidly obese subjects: response to oral supplementation with alpha-linolenic acid. Faintuch J, Horie LM, Barbeiro HV, Barbeiro DF, Soriano FG, Ishida RK, Cecconello I. Obes Surg. 2007 Mar; 17(3):341-7. https://www.ncbi.nlm.nih.gov/pubmed/17546842/[↩]
- Dietary linolenic acid is associated with a lower prevalence of hypertension in the NHLBI Family Heart Study. Djoussé L, Arnett DK, Pankow JS, Hopkins PN, Province MA, Ellison RC. Hypertension. 2005 Mar; 45(3):368-73. https://www.ncbi.nlm.nih.gov/pubmed/15655119/[↩]
- Associations of alpha-linolenic acid and linoleic acid with risk factors for coronary heart disease. Bemelmans WJ, Muskiet FA, Feskens EJ, de Vries JH, Broer J, May JF, Jong BM. Eur J Clin Nutr. 2000 Dec; 54(12):865-71. https://www.ncbi.nlm.nih.gov/pubmed/11114683/[↩]
- Antihypertensive effect and safety of dietary alpha-linolenic acid in subjects with high-normal blood pressure and mild hypertension. Takeuchi H, Sakurai C, Noda R, Sekine S, Murano Y, Wanaka K, Kasai M, Watanabe S, Aoyama T, Kondo K. J Oleo Sci. 2007; 56(7):347-60. https://www.ncbi.nlm.nih.gov/pubmed/17898501/[↩]
- Blood pressure, dietary fats, and antioxidants. Salonen JT, Salonen R, Ihanainen M, Parviainen M, Seppänen R, Kantola M, Seppänen K, Rauramaa R. Am J Clin Nutr. 1988 Nov; 48(5):1226-32. https://www.ncbi.nlm.nih.gov/pubmed/3189209/[↩]
- American Heart Association. Eating flaxseed may lower blood pressure. http://www.heart.org/HEARTORG/News/NewsReleases/Eating-flaxseed-may-lower-blood-pressure_UCM_446258_Article.jsp [↩]
- Dietary supplementation with flaxseed oil lowers blood pressure in dyslipidaemic patients. Paschos GK, Magkos F, Panagiotakos DB, Votteas V, Zampelas A. Eur J Clin Nutr. 2007 Oct; 61(10):1201-6. https://www.ncbi.nlm.nih.gov/pubmed/17268413/[↩][↩]
- Effect of flaxseed consumption on blood pressure, serum lipids, hemopoietic system and liver and kidney enzymes in healthy humans. Stuglin C, Prasad K. J Cardiovasc Pharmacol Ther. 2005 Mar; 10(1):23-7. https://www.ncbi.nlm.nih.gov/pubmed/15821835/[↩]
- Arterial compliance in obese subjects is improved with dietary plant n-3 fatty acid from flaxseed oil despite increased LDL oxidizability. Nestel PJ, Pomeroy SE, Sasahara T, Yamashita T, Liang YL, Dart AM, Jennings GL, Abbey M, Cameron JD. Arterioscler Thromb Vasc Biol. 1997 Jun; 17(6):1163-70. https://www.ncbi.nlm.nih.gov/pubmed/9194769/[↩][↩]
- Dupasquier CM, Weber AM, Ander BP, et al. Effects of dietary flaxseed on vascular contractile function and atherosclerosis during prolonged hypercholesterolemia in rabbits. Am J Physiol Heart Circ Physiol. 2006;291:H2987–96. https://www.ncbi.nlm.nih.gov/pubmed/16844912[↩]





{kind=link}