Contents
The Larynx
The larynx is the upper end of the lower airway. It is continuous with the trachea below and the pharynx posterosuperiorly.
The larynx is a cartilaginous chamber about 4 cm (1.5 in.) long. Its primary function is to keep food and drink out of the airway, but it evolved the additional role of sound production (phonation) in many animals; hence, we colloquially think of it as the “voice box.”
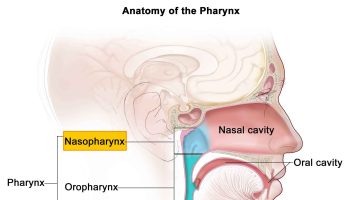
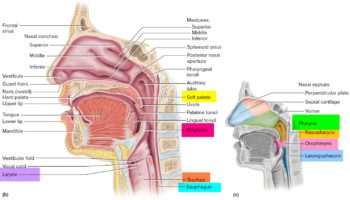
Figure 1. Larynx and pharynx anatomy
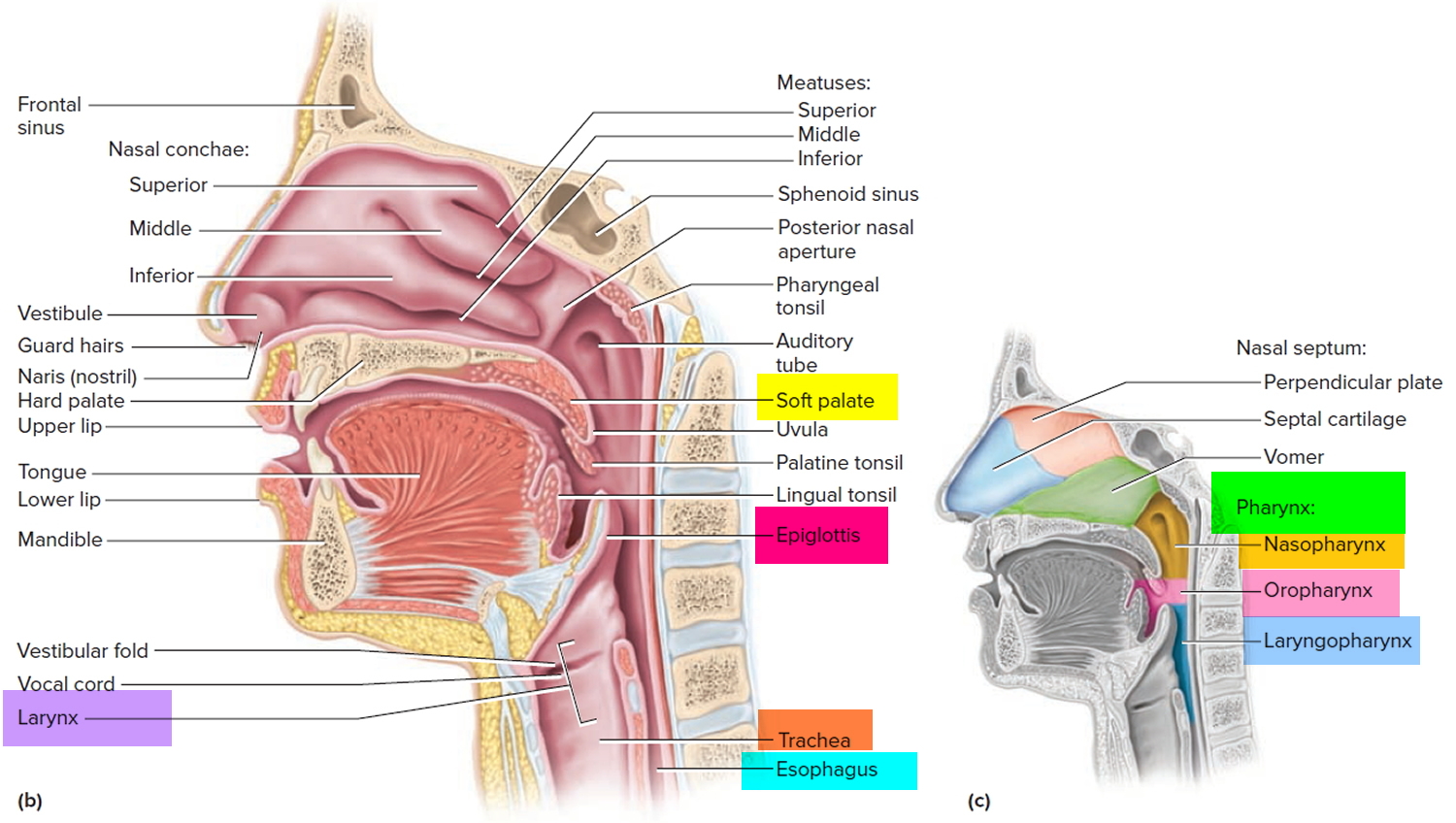
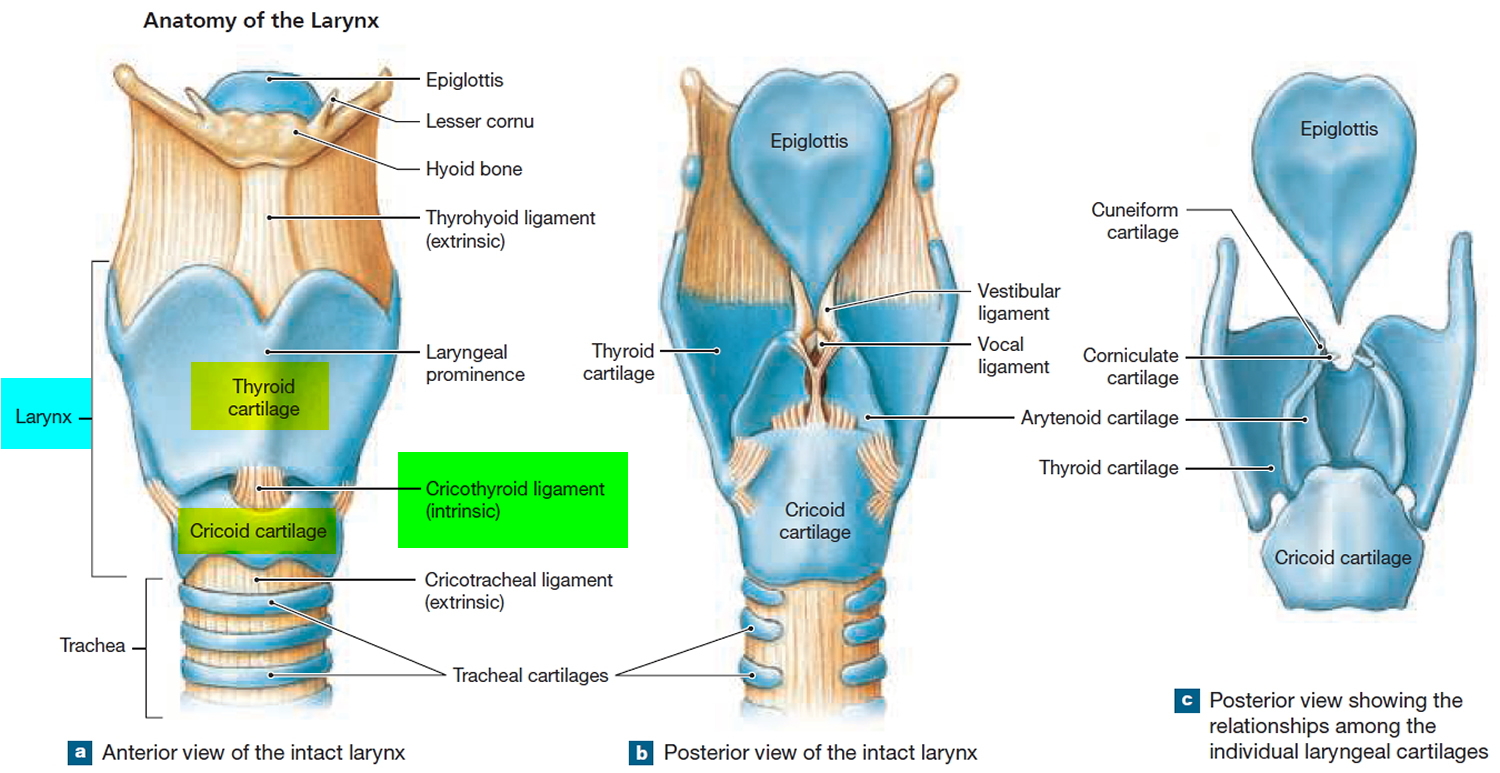
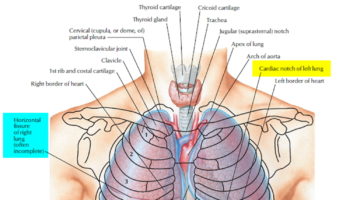
Figure 2. Larynx anatomy
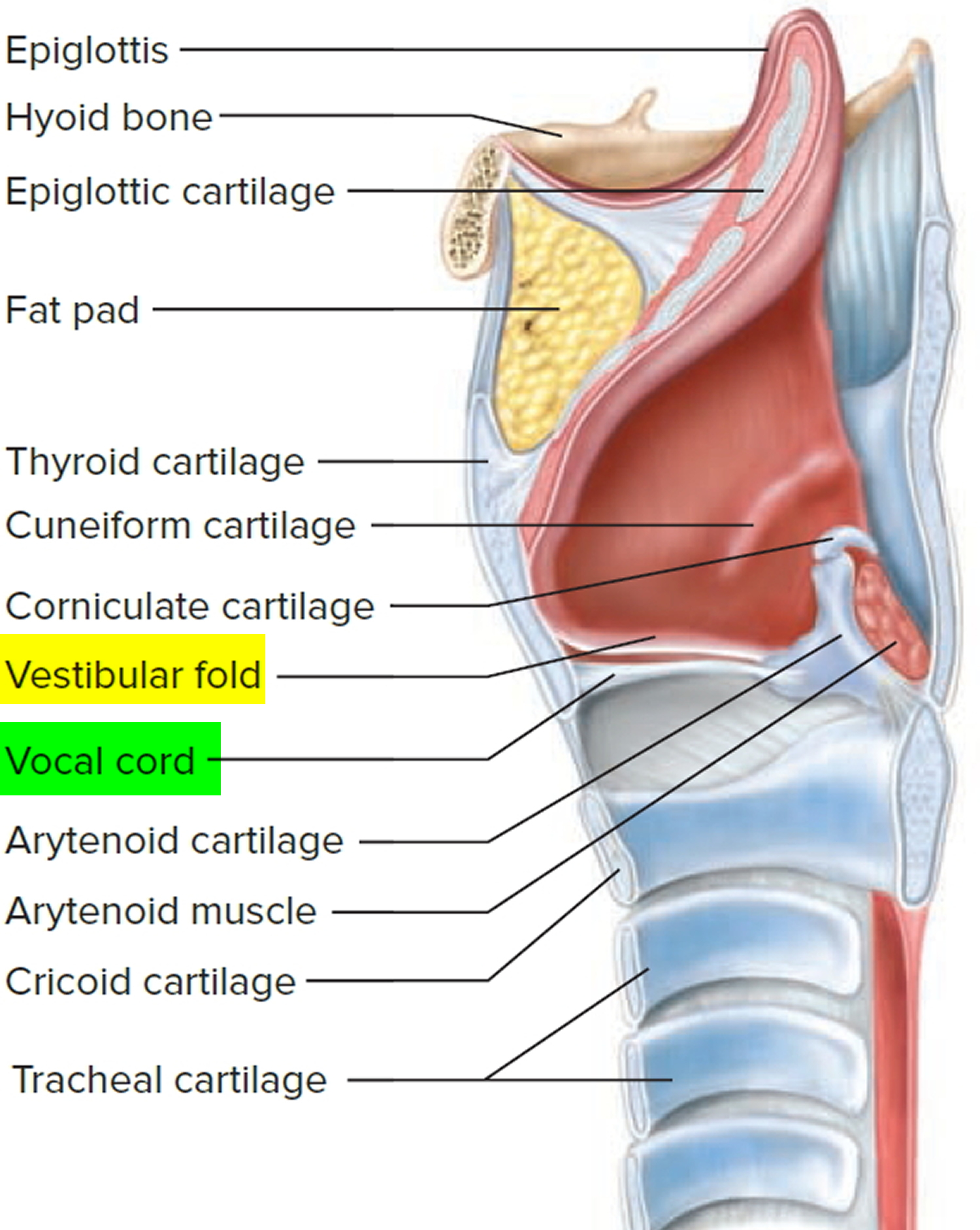
The superior opening of the larynx is guarded by a flap of tissue called the epiglottis. At rest, the epiglottis stands almost vertically. During swallowing, however, extrinsic muscles of the larynx pull the larynx upward toward the epiglottis, the tongue pushes the epiglottis downward to meet it, and the epiglottis closes the airway and directs food and drink into the esophagus behind it. The vestibular folds of the larynx, play a greater role in keeping food and drink out of the airway, however.
The framework of the larynx consists of nine cartilages. The first three are solitary and relatively large. The most superior one, the epiglottic cartilage, is a spoon-shaped supportive plate in the epiglottis. The largest, the thyroid cartilage, is named for its shieldlike shape. It broadly covers the anterior and lateral aspects of the larynx. The “Adam’s apple” is an anterior peak of the thyroid cartilage called the laryngeal prominence. Testosterone stimulates the growth of this prominence, which is therefore larger in males than in females. Inferior to the thyroid cartilage is a ringlike cricoid cartilage. The thyroid and cricoid cartilages essentially constitute the “box” of the voice box.
The remaining cartilages are smaller and occur in three pairs. Posterior to the thyroid cartilage are the two arytenoid cartilages and attached to their upper ends is a pair of little horns, the corniculate cartilages. The arytenoid and corniculate cartilages function in speech, as explained shortly. A pair of cuneiform cartilages supports the soft tissues between the arytenoids and the epiglottis.
A group of fibrous ligaments binds the cartilages of the larynx together and forms a suspension system for the upper airway. A broad sheet called the thyrohyoid ligament suspends the larynx from the hyoid bone above, and below, the cricotracheal ligament suspends the trachea from the cricoid cartilage. These are collectively called the extrinsic ligaments because they link the larynx to other organs. The intrinsic ligaments are contained entirely within the larynx and link its nine cartilages to each other; they include ligaments of the vocal cords and vestibular folds.
Figure 3. Cricothyroid ligament (cricovocal membrane, cricothyroid membrane)
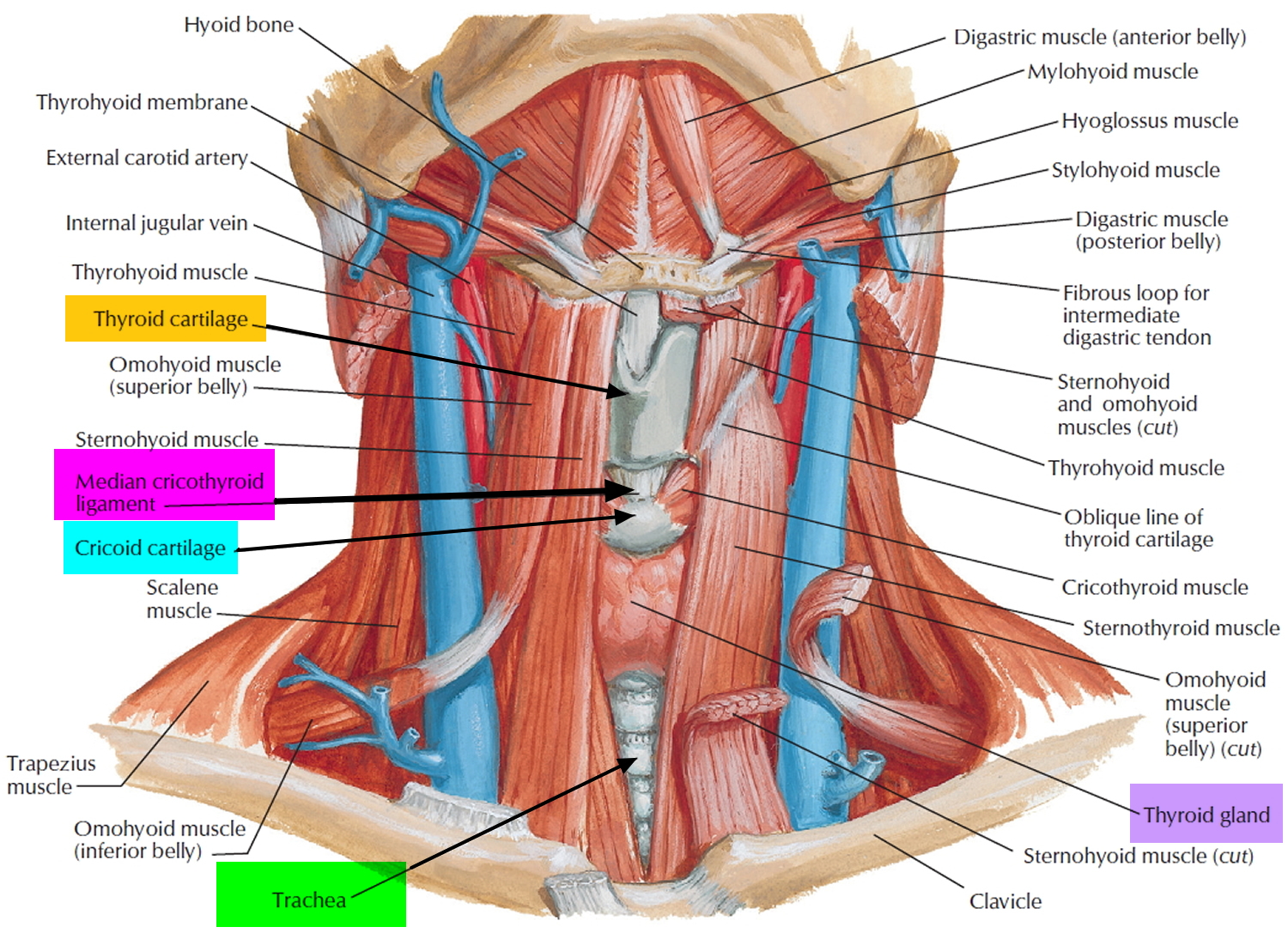
The cricothyroid ligament (cricothyroid membrane) is attached to the arch of cricoid cartilage and extends superiorly to end in a free upper margin within the space enclosed by the thyroid cartilage.
On each side, this upper free margin attaches :
- anteriorly to the thyroid cartilage, and
- posteriorly to the vocal processes of the arytenoid cartilages.
The free margin between these two points of attachment is thickened to form the vocal ligament, which is under the vocal fold (true vocal cord) of the larynx. The cricothyroid ligament is also thickened anteriorly in the midline to form a distinct median cricothyroid ligament, which spans the distance between the arch of cricoid cartilage and the inferior thyroid notch and adjacent deep surface of the thyroid cartilage up to the attachment of the vocal ligaments.
- In emergency situations, when the airway is blocked above the level of the vocal folds, the median cricothyroid ligament can be perforated to establish an airway. Except for small vessels and the occasional presence of a pyramidal lobe of the thyroid gland, normally there are few structures between the median cricothyroid ligament and skin.
In infants, the larynx is relatively high in the throat and the epiglottis touches the soft palate. This creates a more or less continuous airway from the nasal cavity to the larynx and allows an infant to breathe continually while swallowing. The epiglottis deflects milk away from the airstream, like rain running off a tent while it remains dry inside. By age 2, the root of the tongue becomes more muscular and forces the larynx to descend to a lower position. It then becomes impossible to breathe and swallow at the same time without choking.
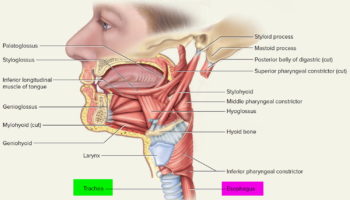
The walls of the larynx are quite muscular. The superficial extrinsic muscles connect the larynx to the hyoid bone and elevate the larynx during swallowing. Also called the infrahyoid group. The deeper intrinsic muscles control the vocal cords by pulling on the corniculate and arytenoid cartilages, causing the cartilages to pivot. Depending on their direction of rotation, the arytenoid cartilages abduct or adduct the vocal cords.
The interior wall of the larynx has two folds on each side that stretch from the thyroid cartilage in front to the arytenoid cartilages in back. The superior vestibular folds play no role in speech but close the larynx during swallowing. They are supported by the vestibular ligaments. The inferior vocal cords (vocal folds) produce sound when air passes between them. They contain the vocal ligaments and are covered with stratified squamous epithelium, best suited to endure vibration and contact between the cords. The vocal cords and the opening between them are collectively called the glottis.
Sound Production
Air passing through the glottis vibrates the vocal folds and produces sound waves. Air forced between the adducted vocal cords vibrates them, producing a high-pitched sound when the cords are relatively taut and a lower pitched sound when they are more slack. Children have slender, short vocal folds, so their voices are high-pitched. At puberty the larynx of a male enlarges more than that of a female. In adult males, the vocal cords are usually longer and thicker, vibrate more slowly, and produce lower-pitched sounds than in females. Loudness is determined by the force of the air passing between the vocal cords.
Although the vocal cords alone produce sound, they do not produce intelligible speech; some anatomists have likened their sound to a hunter’s duck call. Amplification and echoing of the sound occur within the pharynx, oral cavity, nasal cavity, and paranasal sinuses. The crude sounds from the larynx are formed into words by actions of the pharynx, oral cavity, voluntary movements of the tongue, and lips.
The Pharynx
The pharynx, is a common passageway shared by both the digestive and respiratory systems. The pharynx connects the nose, mouth, and throat. The digestive and respiratory systems share the pharynx. It extends between the posterior nasal apertures and the entrances to the trachea and esophagus. The curving superior and posterior walls are attached to the axial skeleton, but the lateral walls are flexible and muscular. The pharynx is a muscular funnel extending about 13 cm (5 in.) from the posterior nasal apertures to the larynx. The pharynx is attached above to the base of the skull and is continuous below, approximately at the level of vertebra CVI (cervical vertebrum C6), with the top of the esophagus. The walls of the pharynx are attached anteriorly to the margins of the nasal cavities, oral cavity, and larynx. Muscles of the pharynx play necessary roles in swallowing and speech.
The pharynx is subdivided into three regions (Figure 1):
- the Nasopharynx,
- the Oropharynx, and
- the Laryngopharynx.
The Nasopharynx
The posterior apertures (choanae) of the nasal cavities open into the nasopharynx above the soft palate. The nasopharynx receives the auditory (eustachian) tubes from the middle ears and houses the pharyngeal tonsil. The nasopharynx passes only air and is lined by pseudostratified columnar epithelium. Inhaled air turns 90° downward as it passes through the nasopharynx. Relatively large particles (>10 μm) generally cannot make the turn because of their inertia. They collide with the wall of the nasopharynx and stick to the mucosa near the tonsil, which is well positioned to respond to airborne pathogens.
The Oropharynx
The oropharynx extends between the soft palate and the base of the tongue at the level of the hyoid bone. Like the posterior and inferior portions of the nasopharynx, the posterior portion of the oral cavity communicates directly with the oropharynx. The epithelium changes from a pseudostratified ciliated columnar epithelium to a nonkeratinized (mucosal type) stratified squamous epithelium at the boundary between the nasopharynx and oropharynx. The posterior margin of the soft palate supports the dangling uvula and two pairs of muscular pharyngeal arches, the posterior arch and the anterior arch.
The Laryngopharynx
The narrow laryngopharynx includes the region of the pharynx lying between the hyoid bone and the entrance to the esophagus. Like the oropharynx, the laryngopharynx is lined with a stratified squamous epithelium that resists abrasion, chemicals, and pathogens.
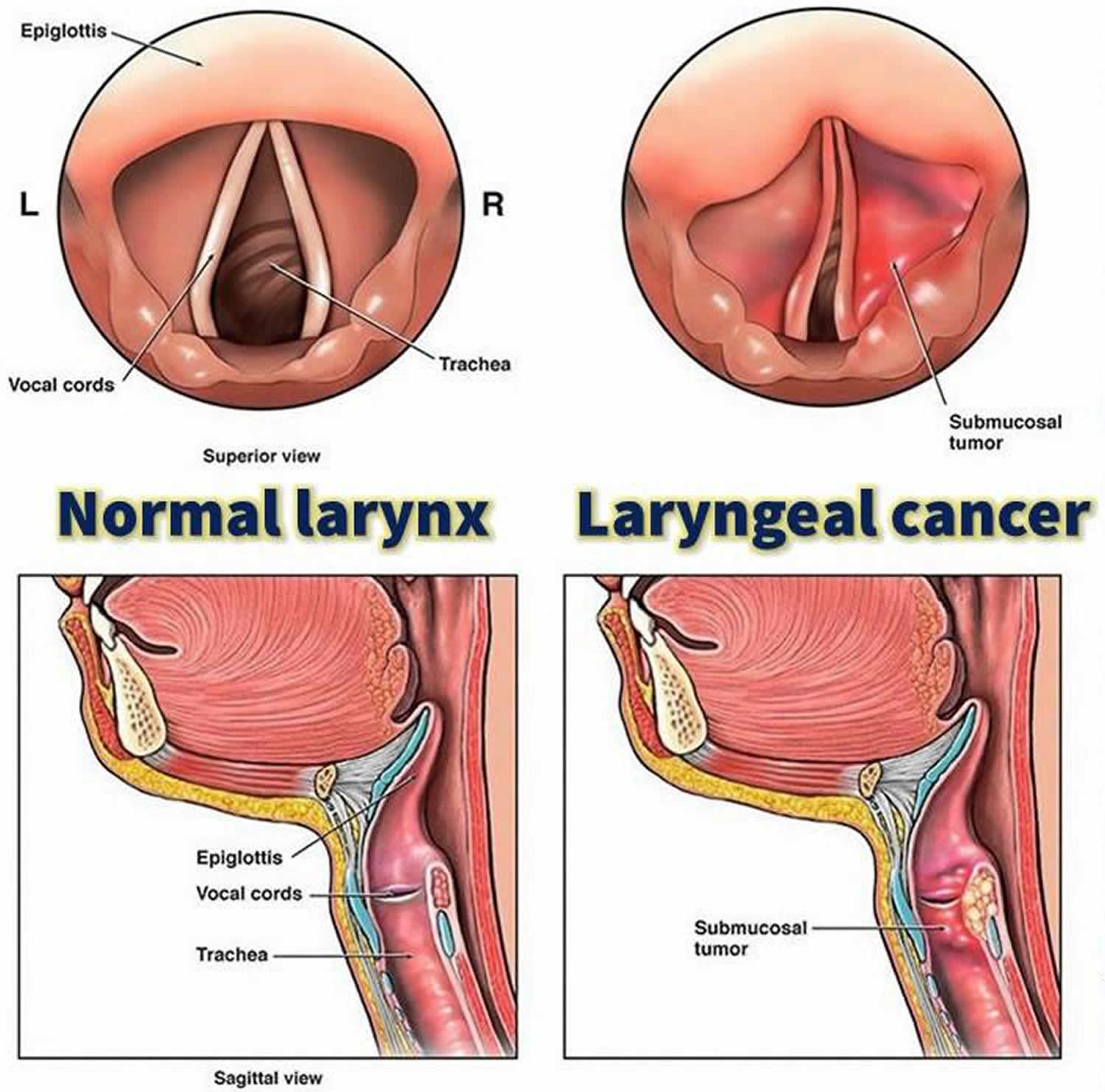
Larynx cancer
Larynx or throat cancer is cancer of the vocal cords, larynx (voice box), or other areas of the throat 1.
Alternative Names:
- Vocal cord cancer;
- Throat cancer;
- Laryngeal cancer;
- Cancer of the glottis;
- Cancer of oropharynx or hypopharynx.
Causes of larynx cancer
People who smoke or use tobacco are at risk of developing throat cancer. Drinking too much alcohol over a long time also increases risk. Smoking and drinking alcohol combined lead to an increased risk for throat cancer.
Most throat cancers develop in adults older than 50. Men are more likely than women to develop throat cancer.
Prevention of larynx cancer
Do not smoke or use other tobacco. Limit or avoid alcohol use.
Figure 3. Larynx cancer
Symptoms of larynx cancer
Symptoms of throat cancer include any of the following 1:
- Abnormal (high-pitched) breathing sounds
- Cough
- Coughing up blood
- Difficulty swallowing
- Hoarseness that does not get better in 3 to 4 weeks
- Neck or ear pain
- Sore throat that does not get better in 2 to 3 weeks, even with antibiotics
- Swelling or lumps in the neck
- Weight loss not due to dieting
Exams and Tests for larynx cancer
The health care provider will perform a physical exam. This may show a lump on the outside of the neck.
The provider may look in your throat or nose using a flexible tube with a small camera at the end.
Other tests that may be ordered include:
- Biopsy of suspected tumor
- Chest x-ray
- CT scan of chest
- CT scan of head and neck
- MRI of the head or neck
- PET (positron emission tomography) scan: PET scan is an imaging test that allows your doctor to check for diseases in your body. The scan uses a special dye that has radioactive tracers. These tracers are injected into a vein in your arm. Your organs and tissues then absorb the tracer.
Treatment for larynx cancer
The goal of treatment is to completely remove the cancer and prevent it from spreading to other parts of the body.
When the tumor is small, either surgery or radiation therapy alone can be used to remove the tumor.
When the tumor is larger or has spread to lymph nodes in the neck, a combination of radiation and chemotherapy is often used to save the voice box (vocal cords). If this is not possible, the voice box is removed. This surgery is called laryngectomy.
Outlook (Prognosis) for larynx cancer
Throat cancers may be cured when detected early. If the cancer has spread (metastasized) to surrounding tissues or lymph nodes in the neck, about half of patients can be cured. If the cancer has spread to parts of the body outside the head and neck, the cancer is not curable. Treatment is aimed at prolonging and improving quality of life.
After treatment, therapy is needed to help with speech and swallowing. If the person is not able to swallow, a feeding tube will be needed.
Possible Complications of larynx cancer
Complications of this type of cancer may include:
- Airway obstruction
- Difficulty swallowing
- Disfigurement of the neck or face
- Hardening of the skin of the neck
- Loss of voice and speaking ability
- Spread of the cancer to other body areas (metastasis).
{kind=link}