Contents
- Human lungs
- Lung anatomy
- Lung disease
- Asthma
- Bronchitis
- Chronic obstructive pulmonary disease (COPD)
- Causes of chronic obstructive pulmonary disease (COPD)
- How to prevent chronic obstructive pulmonary disease (COPD)
- Symptoms of chronic obstructive pulmonary disease (COPD)
- Chronic obstructive pulmonary disease (COPD) diagnosis
- Treatment for chronic obstructive pulmonary disease (COPD)
- Living with chronic obstructive pulmonary disease (COPD)
- Outlook (Prognosis) of chronic obstructive pulmonary disease (COPD)
- Possible Complications of chronic obstructive pulmonary disease (COPD)
- Pulmonary embolism (PE)
- Lungs infection
- Lung nodule
Human lungs
The lungs are soft, spongy, cone-shaped organs in the thoracic (chest) cavity. The lungs consist largely of air tubes and spaces. The balance of the lung tissue, its stroma, is a framework of connective tissue containing many elastic fibers. As a result, the lungs are light, soft, spongy, elastic organs that each weigh only about 0.6 kg (1.25 pounds). The elasticity of healthy lungs helps to reduce the effort of breathing.
The left and right lungs are situated in the left and right pleural cavities inside the thoracic cavity. They are separated from each other by the heart and other structures of the mediastinum, which divides the thoracic cavity into two anatomically distinct chambers. As a result, if trauma causes one lung to collapse, the other may remain expanded. Below the lungs, a thin, dome-shaped muscle called the diaphragm separates the chest from the abdomen. When you breathe, the diaphragm moves up and down, forcing air in and out of the lungs. The thoracic cage encloses the rest of the lungs.
Each lung occupies most of the space on its side of the thoracic cavity. A bronchus and some large blood vessels suspend each lung in the cavity. These tubular structures enter the lung on its medial surface.
Parietal refers to a membrane attached to the wall of a cavity; visceral refers to a membrane that is deeper—toward the interior—and covers an internal organ, such as a lung. Within the thoracic (chest) cavity, the compartments that contain the lungs, on either side of the mediastinum, are lined with a membrane called the parietal pleura. A similar membrane, called the visceral pleura, covers each lung.
The parietal and visceral pleural membranes are separated only by a thin film of watery fluid (serous fluid), which they secrete. Although no actual space normally exists between these membranes, the potential space between them is called the pleural cavity.
A thin lining layer called the pleura surrounds the lungs. The pleura protects your lungs and helps them slide back and forth against the chest wall as they expand and contract during breathing. A layer of serous membrane, the visceral pleura, firmly attaches to each lung surface and folds back to become the parietal pleura. The parietal pleura, in turn, borders part of the mediastinum and lines the inner wall of the thoracic cavity and the superior surface of the diaphragm.
Figure 1. Lungs anatomy
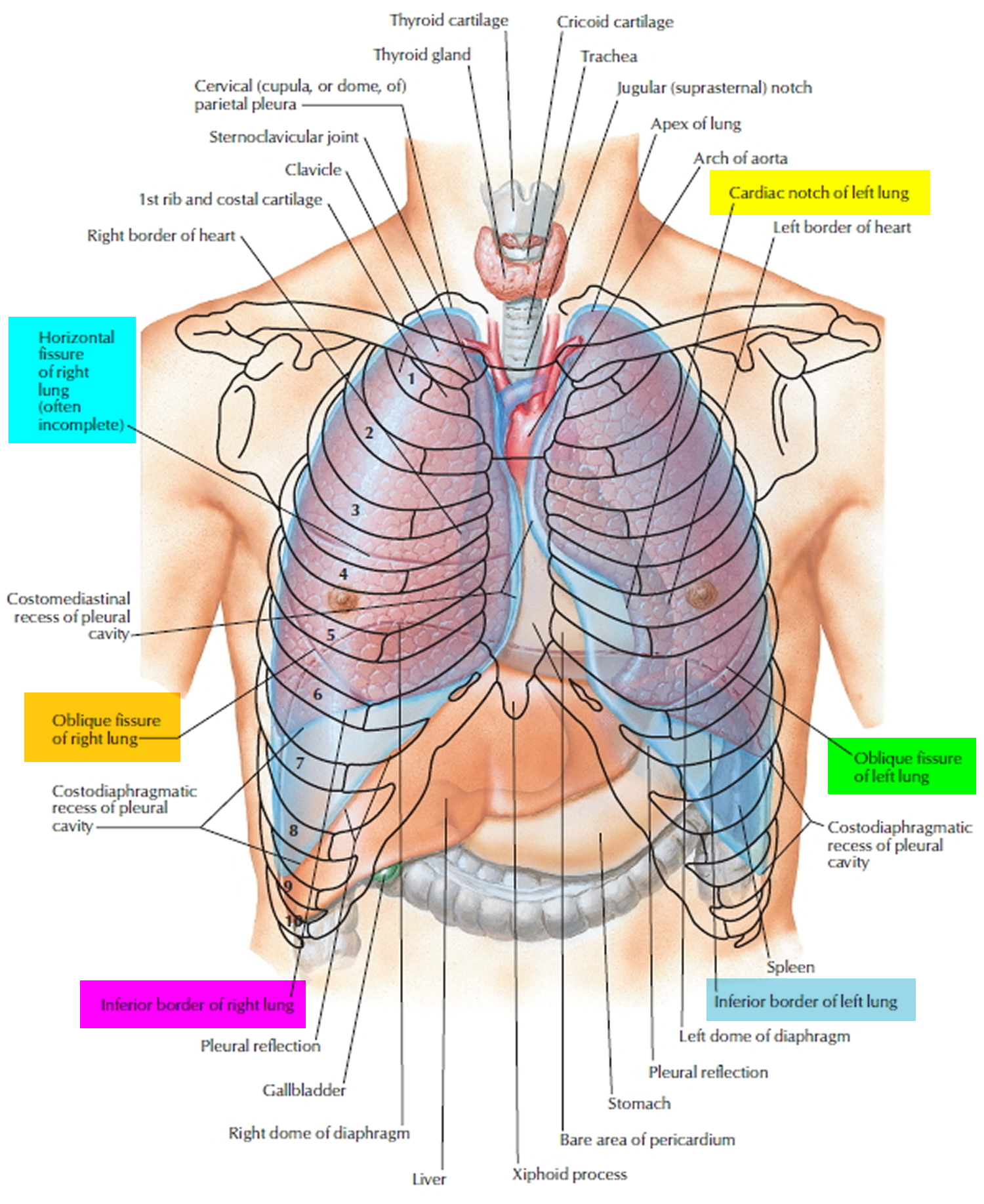
In certain conditions, the pleural cavities may fill with air (pneumothorax), blood (hemothorax), or pus. Air in the pleural cavities, most commonly introduced in a surgical opening of the chest or as a result of a stab or gunshot wound, may cause the lungs to collapse. This collapse of a part of a lung, or rarely an entire lung, is called atelectasis. The goal of treatment is the evacuation of air (or blood) from the pleural space, which allows the lung to reinflate. A small pneumothorax may resolve on its own, but it is oft en necessary to insert a chest tube to assist in evacuation.
The thoracic (chest) cavity is divided by a thick wall called the mediastinum. This is the region between the lungs, extending from the base of the neck to the diaphragm. It is occupied by the heart, the major blood vessels connected to it, the esophagus, the trachea and bronchi, and a gland called the thymus.
Each lung is a blunt cone with the tip, or apex, pointing superiorly. The apex on each side extends into the base of the neck, superior to the first rib. The broad concave inferior portion, or base, of each lung rests on the superior surface of the diaphragm.
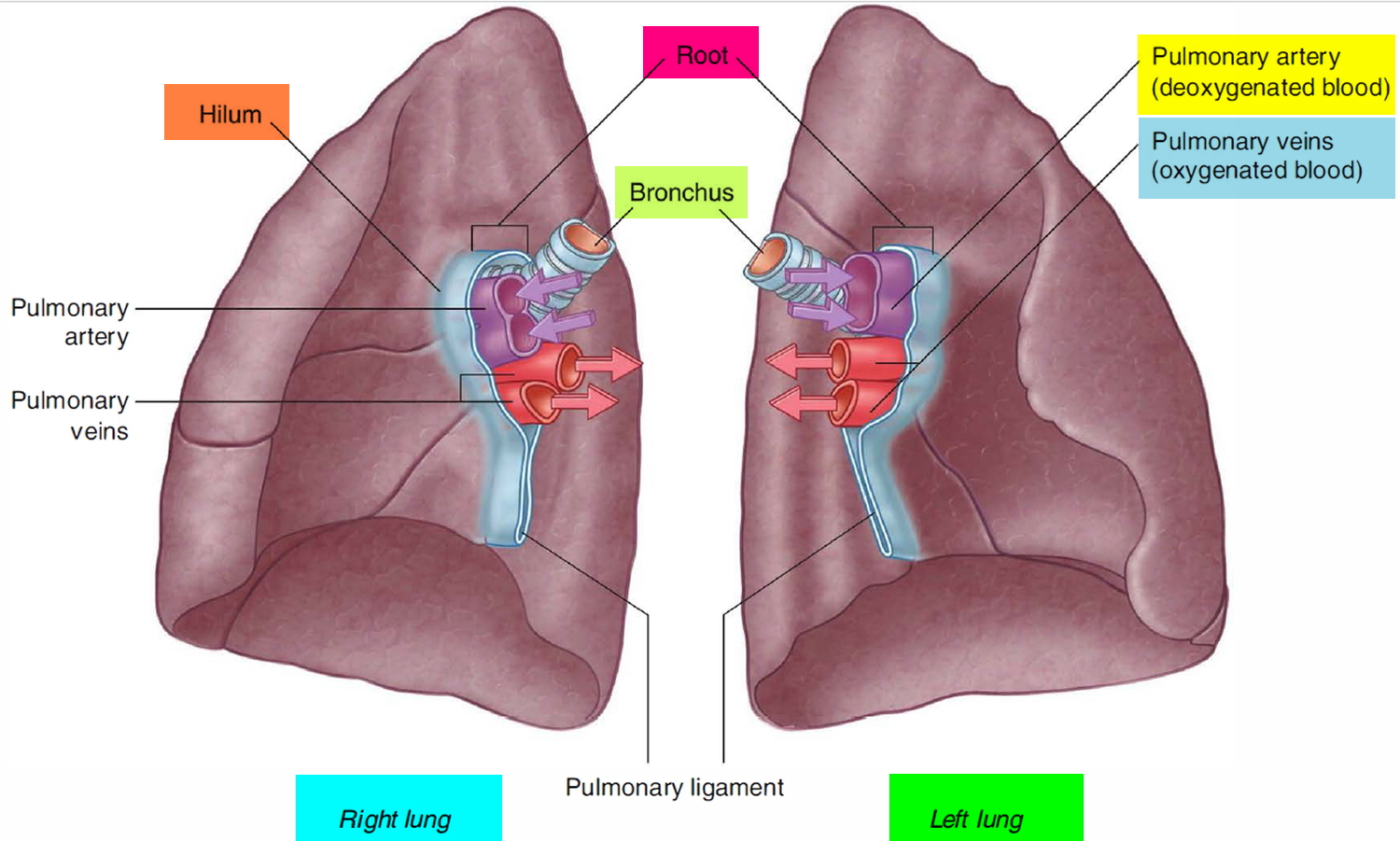
On the medial (mediastinal) surface of each lung is an indentation, the hilum, through which blood vessels, bronchi, lymphatic vessels, and nerves enter and exit the lung. Collectively, these structures attach the lung to the mediastinum and are called the root of the lung. The largest components of this root are the pulmonary artery and veins and the main (primary) bronchus. Because the heart is tilted slightly to the left of the median plane of the thorax, the left and right lungs differ slightly in shape and size.
Within each root and located in the hilum are:
- a pulmonary artery,
- two pulmonary veins,
- a main bronchus,
- bronchial vessels,
- nerves, and
- lymphatics.
Generally, the pulmonary artery is superior at the hilum, the pulmonary veins are inferior, and the bronchi are somewhat posterior in position. On the right side, the lobar bronchus to the superior lobe branches from the main bronchus in the root, unlike on the left where it branches within the lung itself, and is superior to the pulmonary artery.
Figure 2. Hilum (roots) of the lungs
Several deep fissures divide the two lungs into different patterns of lobes.
- The left lung is divided into two lobes, the superior lobe and the inferior lobe, by the oblique fissure. The left lung is somewhat smaller than the right and has a cardiac notch, a deviation in its anterior border that accommodates the heart.
- The right lung is partitioned into three lobes, the superior, middle, and inferior lobes, by the oblique and horizontal fissures.
Each lung lobe is served by a lobar (secondary) bronchus and its branches. Each of the lobes, in turn, contains a number of bronchopulmonary segments separated from one another by thin partitions of dense connective tissue. Each segment receives air from an individual segmental (tertiary) bronchus. There are approximately ten bronchopulmonary segments arranged in similar, but not identical, patterns in each of the two lungs.
The bronchopulmonary segments have clinical significance in that they limit the spread of some diseases within the lung, because infections do not easily cross the connective tissue partitions between them. Furthermore, because only small veins span these partitions, surgeons can neatly remove segments without cutting any major blood vessels.
The smallest subdivision of the lung that can be seen with the naked eye is the lobule. Appearing on the lung surface as hexagons ranging from the size of a pencil eraser to the size of a penny, each lobule is served by a bronchiole and its branches. In most city dwellers and in smokers, the connective tissue that separates the individual lobules is blackened with carbon.
Each lung has a half-cone shape, with a base, apex, two surfaces, and three borders.
- The base sits on the diaphragm.
- The apex projects above rib I and into the root of the neck.
- The two surfaces-the costal surface lies immediately adjacent to the ribs and intercostal spaces of the thoracic wall. The mediastinal surface lies against the mediastinum anteriorly and the vertebral column posteriorly and contains the comma-shaped hilum of the lung, through which structures enter and leave.
- The three borders-the inferior border of the lung is sharp and separates the base from the costal surface. The anterior and posterior borders separate the costal surface from the medial surface. Unlike the anterior and inferior borders, which are sharp, the posterior border is smooth and rounded.
Lung anatomy
Right lung
The right lung has three lobes and two fissures. Normally, the lobes are freely movable against each other because they are separated, almost to the hilum, by invaginations of visceral pleura. These invaginations form the fissures:
- The oblique fissure separates the inferior lobe (lower lobe) from the superior lobe and the middle lobe of the right lung.
- The horizontal fissure separates the superior lobe (upper lobe) from the middle lobe.
The approximate position of the oblique fissure on a patient, in quiet respiration, can be marked by a curved line on the thoracic wall that begins roughly at the spinous process of the vertebra TIV level of the spine, crosses the fifth interspace laterally, and then follows the contour of rib VI anteriorly.
The horizontal fissure follows the fourth intercostal space from the sternum until it meets the oblique fissure as it crosses rib V.
The orientations of the oblique and horizontal fissures determine where clinicians should listen for lung sounds from each lobe. The largest surface of the superior lobe is in contact with the upper part of the anterolateral wall and the apex of this lobe proj ects into the root of the neck. The surface of the middle lobe lies mainly adjacent to the lower anterior and lateral wall. The costal surface of the inferior lobe is in contact with the posterior and inferior walls.
The medial surface of the right lung lies adjacent to a number of important structures in the mediastinum and the root of the neck. These include the:
- heart,
- inferior vena cava,
- superior vena cava,
- azygos vein, and
- esophagus.
The right subclavian artery and vein arch over and are related to the superior lobe of the right lung as they pass over the dome of the cervical pleura and into the axilla.
Left lung
The left Iung is smaller than the right lung and has two lobes separated by an oblique fissure. The oblique fissure of the left lung is slightly more oblique than the corresponding fissure of the right lung. During quiet respiration, the approximate position of the left oblique fissure can be marked by a curved line on the thoracic wall that begins between the spinous processes of vertebrae T III and T IV, crosses the fifth interspace laterally, and follows the contour of rib VI anteriorly.
As with the right lung, the orientation of the oblique fissure determines where to listen for lung sounds from each lobe. The largest surface of the superior lobe is in contact with the upper part of the anterolateral wall, and the apex of this lobe proj ects into the root of the neck. The costal surface of the inferior lobe is in contact with the posterior and inferior walls.
The inferior portion o f the medial surface of the left lung, unlike the right lung, is notched because of the heart’s projection into the left pleural cavity from the middle mediastinum. From the anterior border of the lower part of the superior lobe a tongue-like extension (the lingula of the left lung) projects over the heart bulge.
The medial surface of the left lung lies adjacent to a number of important structures in the mediastinum and root of the neck. These include the:
- heart,
- aortic arch,
- thoracic aorta, and
- esophagus.
The left subclavian artery and vein arch over and are related to the superior lobe of the left lung as they pass over the dome of the cervical pleura and into the axilla.
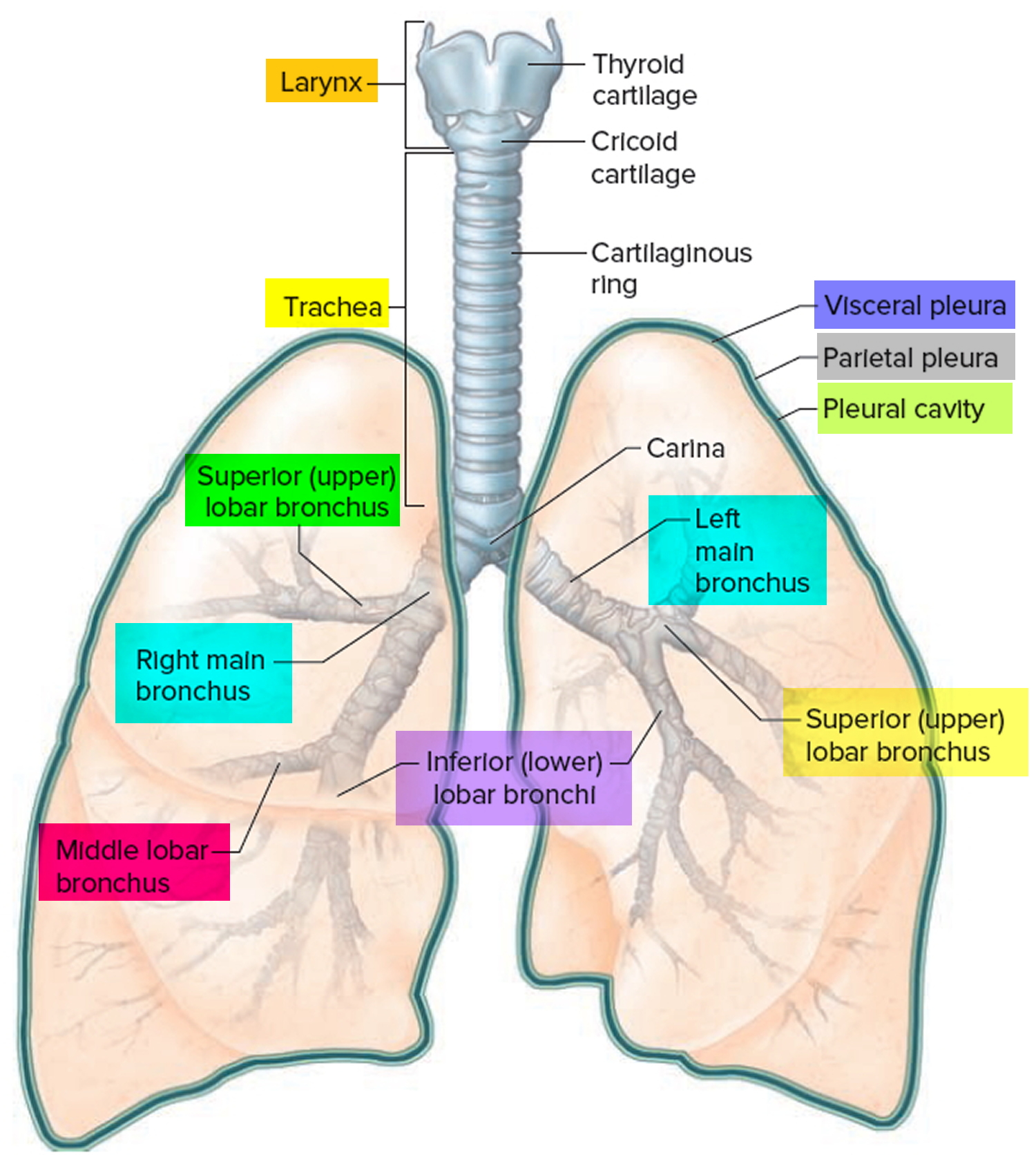
Bronchial tree
The trachea is a flexible tube that extends from cervical spine C6 (vertebral level C VI) in the lower neck to thoracic spine T4-T5 (vertebral level T4 to T5) in the mediastinum where it bifurcates into a right and a left main bronchus. The trachea is held open by C-shaped transverse cartilage rings embedded in its wall the open part of the C facing posteriorly. The lowest tracheal ring has a hook-shaped structure, the carina, that projects backwards in the midline between the origins of the two main bronchi. The posterior wall of the trachea is composed mainly of smooth muscle. Each main bronchus enters the root of a lung and passes through the hilum into the lung itself. The right main bronchus is wider and takes a more vertical course through the root and hilum than the left main bronchus. Therefore, inhaled foreign bodies tend to lodge more frequently on the right side than on the left.
The bronchial tree consists of branched airways leading from the trachea to the microscopic air sacs in the lungs. Its branches begin with the right and left main (primary) bronchi, which arise from the trachea at the level of the fifth thoracic vertebra. Each bronchus enters its respective lung. A short distance from its origin, each main bronchus divides into lobar (secondary) bronchi. The lobar bronchi branch into segmental (tertiary) bronchi, which supply bronchopulmonary segments. Within each bronchopulmonary segment, the segmental bronchi give rise to multiple generations of divisions of increasingly finer tubes and, ultimately, to bronchioles , which further subdivide to terminal bronchioles, respiratory bronchioles, and finally to very thin tubes called alveolar ducts. These ducts lead to thin-walled outpouchings called alveolar sacs. Alveolar sacs lead to smaller, microscopic air sacs called alveoli (singular, alveolus), which lie within capillary networks (Figure 6). The alveoli are the sites of gas exchange between the inhaled air and the bloodstream.
The structure of a bronchus is similar to that of the trachea, but the tubes that branch from it have less cartilage in their walls, and the bronchioles lack cartilage. As the cartilage diminishes, a layer of smooth muscle surrounding the tube becomes more prominent. This muscular layer persists even in the smallest bronchioles, but only a few muscle cells are associated with the alveolar ducts.
The absence of cartilage in the bronchioles allows their diameters to change in response to contraction of the smooth muscle in their walls, similar to what happens with arterioles of the cardiovascular system. Part of the “fight-or-flight” response, triggered by the sympathetic nervous system, is bronchodilation, in which the smooth muscle relaxes and the airways become wider and allow more airflow. The opposite, bronchoconstriction, occurs when the smooth muscle contracts and it becomes difficult to move air in and out of the lungs. Bronchoconstriction can occur with allergies. Asthma is an extreme example of bronchoconstriction.
The mucous membranes of the bronchial tree continue to filter the incoming air, and the many branches of the tree distribute the air to alveoli throughout the lungs. The alveoli, in turn, provide a large surface area of thin simple squamous epithelial cells through which gases are easily exchanged. Oxygen diffuses from the alveoli into the blood in nearby capillaries, and carbon dioxide diffuses from the blood into the alveoli.
Figure 3. Bronchial tree of the lungs
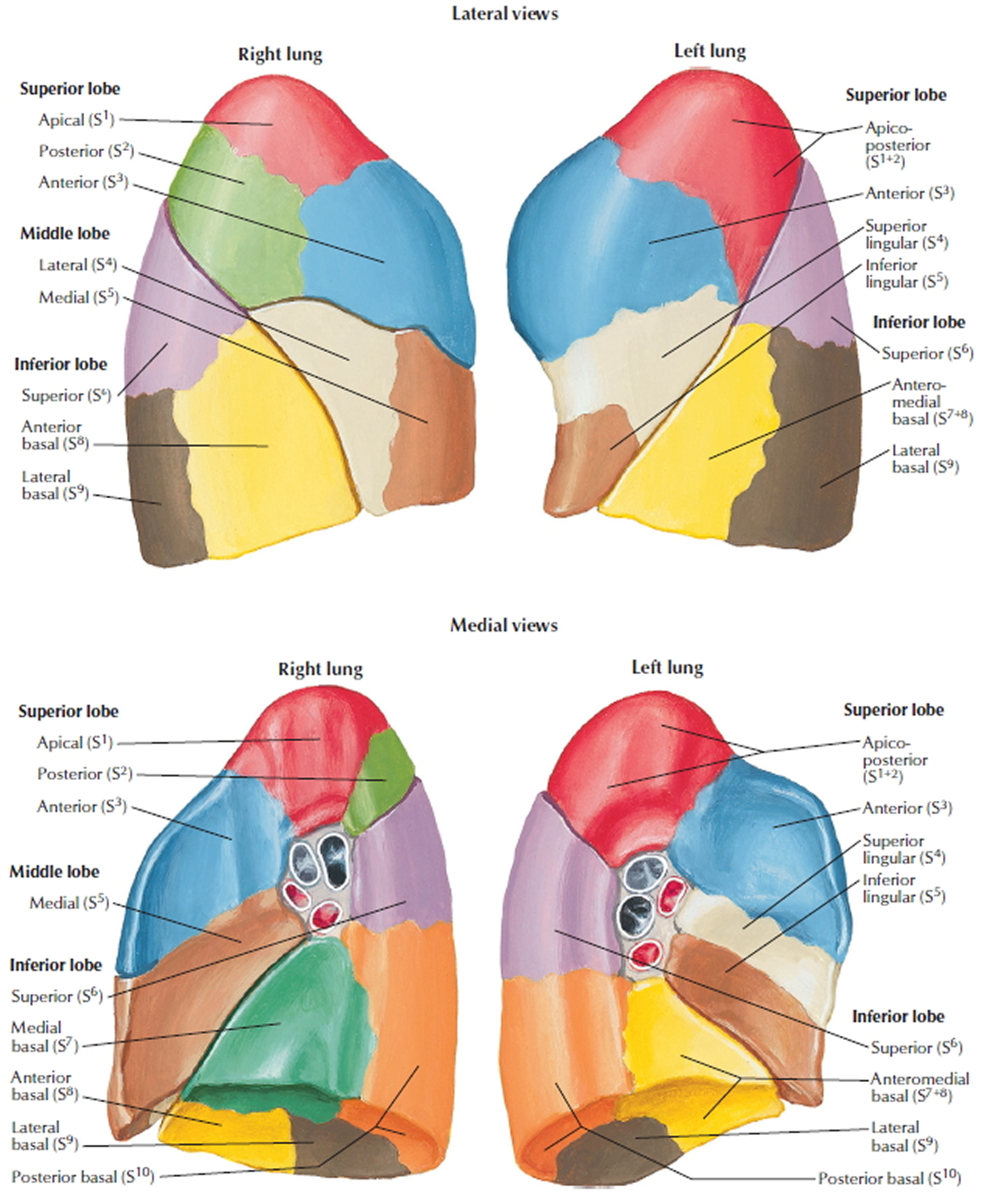
Bronchopulmonary segments
A bronchopulmonary segment is the area of lung supplied by a segmental bronchus and its accompanying pulmonary artery branch. Tributaries of the pulmonary vein tend to pass intersegmentally between and around the margins of segments. Each bronchopulmonary segment is shaped like an irregular cone, with the apex at the origin of the segmental bronchus and the base projected peripherally onto the surface of the lung.
A bronchopulmonary segment is the smallest functionally independent region of a lung and the smallest area of lung that can be isolated and removed without affecting adjacent regions.
There are ten bronchopulmonary segments in each lung; some of them fuse in the left lung.
Figure 4. Bronchopulmonary segments
Lung Alveoli
Each human lung is a spongy mass composed of 150 million little sacs, the alveoli. These provide about 70 m², per lung, of gas-exchange surface—about equal to the floor area of a handball court or a room about 8.4 m (25 ft) square.
An alveolus is a pouch about 0.2 to 0.5 mm in diameter. Thin, broad cells called squamous (type I) alveolar cells cover about 95% of the alveolar surface area. Their thinness allows for rapid gas diffusion between the air and blood. The other 5% is covered by round to cuboidal great (type II) alveolar cells. Even though they cover less surface area, these considerably outnumber the squamous alveolar cells.
Great (type II) alveolar cells have two functions:
- They repair the alveolar epithelium when the squamous cells are damaged; and
- They secrete pulmonary surfactant, a mixture of phospholipids and protein that coats the alveoli and smallest bronchioles and prevents the bronchioles from collapsing when one exhales.
The most numerous of all cells in the lung are alveolar macrophages (dust cells), which wander the lumens of the alveoli and the connective tissue between them. These cells keep the alveoli free of debris by phagocytizing dust particles that escape entrapment by mucus in the higher parts of the respiratory tract. In lungs that are infected or bleeding, the macrophages also phagocytize bacteria and loose blood cells. As many as 100 million alveolar macrophages perish each day as they ride up the mucociliary escalator to be swallowed and digested, thus ridding the lungs of their load of debris.
Each alveolus is surrounded by a web of blood capillaries supplied by small branches of the pulmonary artery. The barrier between the alveolar air and blood, called the respiratory membrane, consists only of the squamous alveolar cell, the squamous endothelial cell of the capillary, and their shared basement membrane. These have a total thickness of only 0.5 μm, just 1/15 the diameter of a single red blood cell.
It is very important to prevent fluid from accumulating in the alveoli, because gases diffuse too slowly through liquid to sufficiently aerate the blood. Except for a thin film of moisture on the alveolar wall, the alveoli are kept dry by the absorption of excess liquid by the blood capillaries. The mean blood pressure in these capillaries is only 10 mm Hg compared to 30 mm Hg at the arterial end of the average capillary elsewhere. This low blood pressure is greatly overridden by the oncotic pressure that retains fluid in the capillaries, so the osmotic uptake of water overrides filtration and keeps the alveoli free of fluid. The lungs also have a more extensive lymphatic drainage than any other organ in the body. The low capillary blood pressure also prevents rupture of the delicate respiratory membrane.
Figure 5. Lungs alveoli
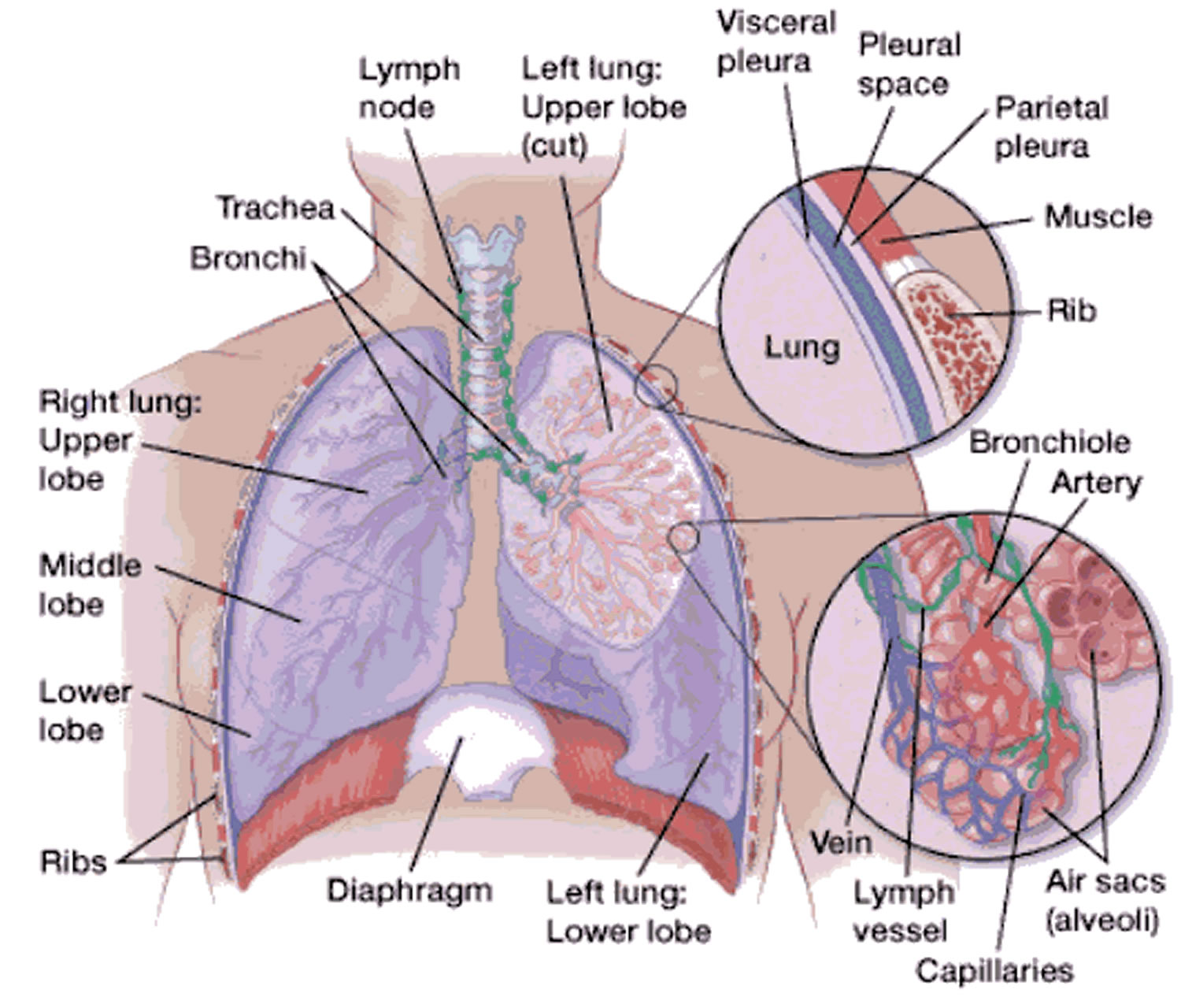 Figure 6. Pulmonary Alveoli (microscopic view)
Figure 6. Pulmonary Alveoli (microscopic view)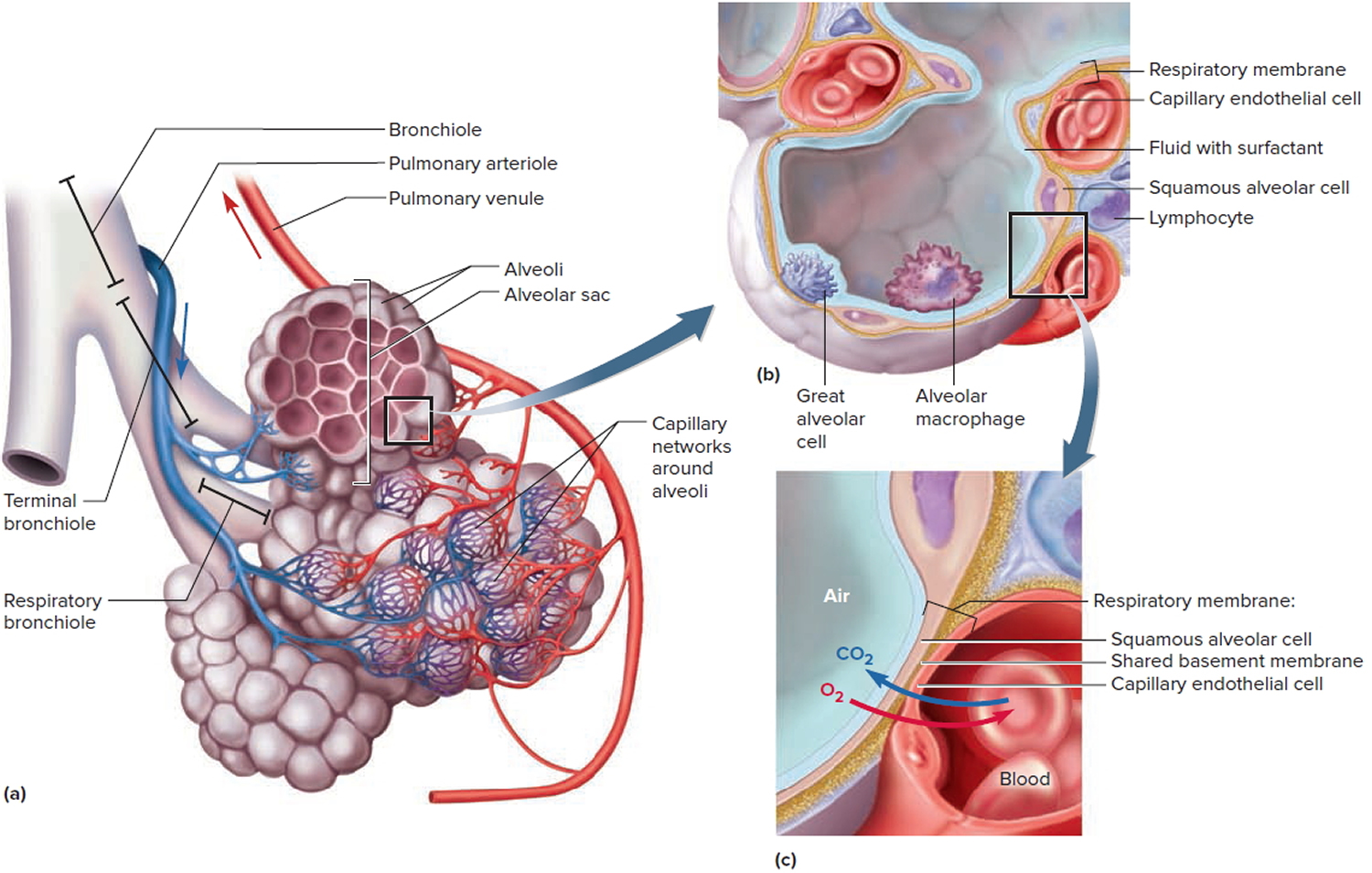
Note: (a) Clusters of alveoli and their blood supply. (b) Structure of an alveolus. (c) Structure of the respiratory membrane.
What Controls Your Breathing?
A respiratory control center at the base of your brain controls your breathing. This center sends ongoing signals down your spine and to the muscles involved in breathing.
These signals ensure your breathing muscles contract (tighten) and relax regularly. This allows your breathing to happen automatically, without you being aware of it.
To a limited degree, you can change your breathing rate, such as by breathing faster or holding your breath. Your emotions also can change your breathing. For example, being scared or angry can affect your breathing pattern.
Your breathing will change depending on how active you are and the condition of the air around you. For example, you need to breathe more often when you do physical activity. In contrast, your body needs to restrict how much air you breathe if the air contains irritants or toxins.
To adjust your breathing to changing needs, your body has many sensors in your brain, blood vessels, muscles, and lungs.
Sensors in the brain and in two major blood vessels (the carotid artery and the aorta) detect carbon dioxide or oxygen levels in your blood and change your breathing rate as needed.
Sensors in the airways detect lung irritants. The sensors can trigger sneezing or coughing. In people who have asthma, the sensors may cause the muscles around the airways in the lungs to contract. This makes the airways smaller.
Sensors in the lungs alveoli (air sacs) can detect fluid buildup in the lung tissues. These sensors are thought to trigger rapid, shallow breathing.
Sensors in your joints and muscles detect movement of your arms or legs. These sensors may play a role in increasing your breathing rate when you’re physically active.
Lung disease
Breathing is a complex process. If injury, disease, or other factors affect any part of the process, you may have trouble breathing. For example, the fine hairs (cilia) that line your upper airways may not trap all of the germs you breathe in. These germs can cause an infection in your bronchial tubes (bronchitis) or deep in your lungs (pneumonia). These infections cause a buildup of mucus or fluid that narrows the airways and limits airflow in and out of your lungs.
If you have asthma, breathing in certain substances that you’re sensitive to can trigger your airways to narrow. This makes it hard for air to flow in and out of your lungs.
Over a long period, breathing in cigarette smoke or air pollutants can damage the airways and air sacs. This can lead to a disease called COPD (chronic obstructive pulmonary disease). Chronic obstructive pulmonary disease (COPD) prevents proper airflow in and out of your lungs and can hinder gas exchange in the air sacs.
An important step to breathing is the movement of your diaphragm and other muscles in your chest, neck, and abdomen. This movement lets you inhale and exhale. Nerves that run from your brain to these muscles control their movement. Damage to these nerves in your upper spinal cord can cause breathing to stop, unless a machine is used to help you breathe. This machine is called a ventilator or a respirator.
A steady flow of blood in the small blood vessels that surround your air sacs is vital for gas exchange. Long periods of inactivity or surgery can cause a blood clot called a pulmonary embolism (PE) to block a lung artery. A pulmonary embolism (PE) can reduce or block the flow of blood in the small blood vessels and hinder gas exchange.
Asthma
Asthma is a chronic disease that affects your airways 1. Your airways are tubes that carry air in and out of your lungs. If you have asthma, the inside walls of your airways become sore and swollen. That makes them very sensitive, and they may react strongly to things that you are allergic to or find irritating. When your airways react, they get narrower and your lungs get less air.
Symptoms of asthma include
- Wheezing
- Coughing, especially early in the morning or at night
- Chest tightness
- Shortness of breath
Not all people who have asthma have these symptoms. Having these symptoms doesn’t always mean that you have asthma. Your doctor will diagnose asthma based on lung function tests, your medical history, and a physical exam. You may also have allergy tests.
When your asthma symptoms become worse than usual, it’s called an asthma attack. Severe asthma attacks may require emergency care, and they can be fatal.
Asthma is treated with two kinds of medicines: quick-relief medicines to stop asthma symptoms and long-term control medicines to prevent symptoms.
Asthma – quick-relief drugs
Asthma quick-relief medicines work fast to control asthma symptoms 2. You take them when you are coughing, wheezing, having trouble breathing, or having an asthma attack. They are also called rescue drugs. These medicines are called “bronchodilators” because they open (dilate) and help relax the muscles of your airways (bronchi) 2.
You and your doctor can make a plan for the quick-relief drugs that work for you. This plan will include when you should take them and how much you should take.
Plan ahead. Make sure you do not run out. Take enough with you when you travel.
Short-acting Beta-agonists
Short-acting beta-agonists are the most common quick-relief drugs for treating asthma attacks.
They can be used just before exercising to help prevent asthma symptoms caused by exercise. They work by relaxing the muscles of your airways, and this lets you breathe better during an attack.
Tell your doctor if you are using quick-relief medicines twice a week or more to control your asthma symptoms. Your asthma may not be under control, and your doctor may need to change your dose of daily control drugs.
Some quick-relief asthma medicines include 2:
- Albuterol (ProAir HFA, Proventil HFA, Ventolin HFA)
- Levalbuterol (Xopenex HFA)
- Metaproterenol
- Terbutaline
Quick-relief asthma medicines may cause these side effects:
- Anxiety.
- Tremor (your hand or another part of your body may shake).
- Restlessness.
- Headache.
- Fast and irregular heartbeats. Call your doctor right away if you have this side effect.
Oral Steroids
Your doctor might prescribe oral steroids when you have an asthma attack that is not going away. These are medicines that you take by mouth as pills, capsules, or liquids.
Oral steroids are not quick-relief medicines, but are often given for 7 to 14 days when your symptoms flare-up.
Oral steroids include:
- Prednisone
- Prednisolone
- Methylprednisolone.
Asthma – control drugs
Control medicines for asthma are drugs you take to control your asthma symptoms 3. You must take them every day for them to work. You and your doctor can make a plan for the medicines that work for you. This plan will include when you should take them and how much you should take.
You may need to take these medicines for at least a month before you start to feel better.
Take the medicines even when you feel OK. Take enough with you when you travel. Plan ahead. Make sure you do not run out.
Inhaled Corticosteroids
Inhaled corticosteroids prevent your airways from swelling in order to help keep your asthma symptoms away.
Inhaled steroids are used with a metered dose inhaler (MDI) and spacer. Or they may be used with a dry powder inhaler.
You should use an inhaled steroid every day, even if you do not have symptoms.
After you use it, rinse your mouth with water, gargle, and spit it out.
If your child cannot use an inhaler, your doctor will give you a drug to use with a nebulizer. This machine turns liquid medicine into a spray so your child can breathe the medicine in.
Long-acting Beta-agonist Inhalers
These medicines relax the muscles of your airways to help keep your asthma symptoms away.
Normally, you use these medicines only when you are using an inhaled steroid drug and you still have symptoms. DO NOT take these long-acting medicines alone.
Use this medicine every day, even if you do not have symptoms.
Combination Therapy
Your doctor may ask you to take both a steroid drug and a long-acting beta-agonist drug.
It may be easier to use an inhaler that has both drugs in them.
Leukotriene Modifiers
These medicines are used to prevent asthma symptoms. They come in tablet or pill form and can be used together with a steroid inhaler.
Cromolyn
Cromolyn is a medicine that may prevent asthma symptoms. It can be used in a nebulizer, so it may be easy for young children to take.
Bronchitis
Bronchitis is an inflammation of the bronchial tubes, the airways that carry air to your lungs 4. This swelling narrows the airways, which makes it harder to breathe. Other symptoms of bronchitis are a cough and coughing up mucus. It can also cause shortness of breath, wheezing, a low fever, and chest tightness. Acute means the symptoms have been present only for a short time.
There are two main types of bronchitis:
- Acute bronchitis and
- Chronic bronchitis.
Acute bronchitis
When acute bronchitis occurs, it almost always comes after having a cold or flu-like illness 5. The bronchitis infection is caused by a virus. At first, it affects your nose, sinuses, and throat. Then it spreads to the airways that lead to your lungs.
Some symptoms of acute bronchitis are:
- Chest discomfort
- Cough that produces mucus — the mucus may be clear or yellow-green
- Fatigue
- Fever — usually low-grade
- Shortness of breath that gets worse with activity
- Wheezing, in people with asthma
Even after acute bronchitis has cleared, you may have a dry, nagging cough that lasts for 1 to 4 weeks.
Sometimes it can be hard to know if you have pneumonia or bronchitis. If you have pneumonia, you are more likely to have a high fever and chills, feel sicker, or be more short of breath.
How is acute bronchitis diagnosed?
Your health care provider will listen to the breathing sounds in your lungs with a stethoscope. Your breathing may sound abnormal or rough.
Tests may include:
- Chest x-ray, if your provider suspects pneumonia
- Pulse oximetry, a painless test that helps determine the amount of oxygen in your blood by using a device placed on the end of your finger
Treatment of acute bronchitis
Most people DO NOT need antibiotics for acute bronchitis 5. The infection will almost always go away on its own within 1 week. Doing these things may help you feel better:
- Drink plenty of fluids.
- If you have asthma or another chronic lung condition, use your inhaler.
- Get plenty of rest.
- Take aspirin or acetaminophen if you have a fever. DO NOT give aspirin to children.
- Breathe moist air by using a humidifier or steaming up the bathroom.
Certain medicines that you can buy without a prescription can help break up or loosen mucus. Look for the word “guaifenesin” on the label. Ask the pharmacist for help finding it.
If your symptoms do not improve or if you are wheezing, your provider may prescribe an inhaler to open your airways.
If your provider thinks you also have bacteria in your airways, they may prescribe antibiotics. This medicine will only get rid of bacteria, not viruses.
Your provider may also prescribe corticosteroid medicine to reduce swelling in your lungs.
If you have the flu and it is caught in the first 48 hours after getting sick, your provider might also prescribe antiviral medicine.
Other tips include:
- DO NOT smoke.
- Avoid secondhand smoke and air pollution.
- Wash your hands (and your children’s hands) often to avoid spreading viruses and other germs.
Outlook (Prognosis) of acute bronchitis
Except for the cough, symptoms usually go away in 7 to 10 days if you do not have a lung disorder.
When to see a your doctor
Call your healthcare provider if you:
- Have a cough on most days, or have a cough that keeps returning
- Are coughing up blood
- Have a high fever or shaking chills
- Have a low-grade fever for 3 or more days
- Have thick, yellow-green mucus, especially if it has a bad smell
- Feel short of breath or have chest pain
- Have a chronic illness, like heart or lung disease
Chronic bronchitis
Chronic bronchitis is one type of COPD (chronic obstructive pulmonary disease). The inflamed bronchial tubes produce a lot of mucus. This leads to coughing and difficulty breathing. Cigarette smoking is the most common cause. Breathing in air pollution, fumes, or dust over a long period of time may also cause it.
To diagnose chronic bronchitis, your doctor will look at your signs and symptoms and listen to your breathing. You may also have other tests.
Chronic bronchitis is a long-term condition that keeps coming back or never goes away completely. If you smoke, it is important to quit. Treatment can help with your symptoms. It often includes medicines to open your airways and help clear away mucus. You may also need oxygen therapy. Pulmonary rehabilitation may help you manage better in daily life.
Chronic obstructive pulmonary disease (COPD)
Chronic obstructive pulmonary disease (COPD) is a common lung disease. Having COPD makes it hard to breathe.
There are two main forms of chronic obstructive pulmonary disease (COPD) 6:
- Chronic bronchitis, which involves a long-term cough with mucus
- Emphysema, which involves damage to the lungs over time
Most people with chronic obstructive pulmonary disease (COPD) have a combination of both conditions.
Causes of chronic obstructive pulmonary disease (COPD)
Smoking is the main cause of COPD. The more a person smokes, the more likely that person will develop COPD. But some people smoke for years and never get COPD.
In rare cases, nonsmokers who lack a protein called alpha-1 antitrypsin can develop emphysema.
Other risk factors for COPD are:
- Exposure to certain gases or fumes in the workplace
- Exposure to heavy amounts of secondhand smoke and pollution
- Frequent use of a cooking fire without proper ventilation.
How to prevent chronic obstructive pulmonary disease (COPD)
- Not smoking prevents most chronic obstructive pulmonary disease (COPD). Ask your provider about quit-smoking programs. Medicines are also available to help you stop smoking.
Symptoms of chronic obstructive pulmonary disease (COPD)
Symptoms may include any of the following:
- Cough, with or without mucous
- Fatigue
- Many respiratory infections
- Shortness of breath (dyspnea) that gets worse with mild activity
- Trouble catching one’s breath
- Wheezing
Because the symptoms develop slowly, some people may not know that they have COPD.
Chronic obstructive pulmonary disease (COPD) diagnosis
The best test for COPD is a lung function test called spirometry. This involves blowing out as hard as possible into a small machine that tests lung capacity. The results can be checked right away.
Using a stethoscope to listen to the lungs can also be helpful. But sometimes, the lungs sound normal, even when a person has COPD.
Imaging tests of the lungs, such as x-rays and CT scans, can be helpful. With an x-ray, the lungs may look normal, even when a person has COPD. A CT scan will usually show signs of COPD.
Sometimes, a blood test called arterial blood gas may be done to measure the amounts of oxygen and carbon dioxide in the blood.
Treatment for chronic obstructive pulmonary disease (COPD)
There is no cure for COPD. But there are many things you can do to relieve symptoms and keep the disease from getting worse.
If you smoke, now is the time to quit. This is the best way to slow lung damage.
Medicines used to treat COPD include:
- Inhalers (bronchodilators) COPD — quick-relief drugs to help open the airways
- Inhaled COPD control drugs or oral steroids to reduce lung inflammation
- Anti-inflammatory drugs to reduce swelling in the airways
- Certain long-term antibiotics
In severe cases or during flare-ups, you may need to receive:
- Steroids by mouth or through a vein (intravenously)
- Bronchodilators through a nebulizer
- Oxygen therapy
- Assistance from a machine to help breathing by using a mask, BiPAP, or through the use of an endotracheal tube
Your health care provider may prescribe antibiotics during symptom flare-ups, because an infection can make COPD worse.
You may need oxygen therapy at home if you have a low level of oxygen in your blood.
Pulmonary rehabilitation does not cure COPD. But it can teach you to breathe in a different way so you can stay active and feel better.
Living with chronic obstructive pulmonary disease (COPD)
You can do things every day to keep COPD from getting worse, protect your lungs, and stay healthy.
Walk to build up strength:
- Ask the provider or therapist how far to walk.
- Slowly increase how far you walk.
- Avoid talking if you get short of breath when you walk.
- Use pursed lip breathing when you breathe out, to empty your lungs before the next breath.
Things you can do to make it easier for yourself around the home include:
- Avoid very cold air or very hot weather
- Make sure no one smokes in your home
- Reduce air pollution by not using the fireplace and getting rid of other irritants
- Manage stress in your mood
Eat healthy foods, including fish, poultry, and lean meat, as well as fruits and vegetables. If it is hard to keep your weight up, talk to a provider or dietitian about eating foods with more calories.
Surgery may be used to treat COPD. Only a few people benefit from these surgical treatments:
Surgery to remove parts of the diseased lung, which can help less-diseased parts work better in some people with emphysema. Lung transplant for a small number of very severe cases
Outlook (Prognosis) of chronic obstructive pulmonary disease (COPD)
COPD is a long-term (chronic) illness. The disease will get worse more quickly if you do not stop smoking.
If you have severe COPD, you will be short of breath with most activities. You may be admitted to the hospital more often.
Talk with your provider about breathing machines and end-of-life care as the disease progresses.
Possible Complications of chronic obstructive pulmonary disease (COPD)
With COPD, you may have other health problems such as:
- Irregular heartbeat (arrhythmia)
- Need for breathing machine and oxygen therapy
- Right-sided heart failure or cor pulmonale (heart swelling and heart failure due to chronic lung disease)
- Pneumonia
- Pneumothorax
- Severe weight loss and malnutrition
- Thinning of the bones (osteoporosis)
- Debilitation
- Increased anxiety
Pulmonary embolism (PE)
A pulmonary embolism is a sudden blockage in a lung artery 7. The cause is usually a blood clot in the leg called a deep vein thrombosis (DVT) that breaks loose and travels through the bloodstream to the lung. Pulmonary embolism is a serious condition that can cause:
- Permanent damage to the affected lung
- Low oxygen levels in your blood
- Damage to other organs in your body from not getting enough oxygen
If a clot is large, or if there are many clots, pulmonary embolism can cause death.
Half the people who have pulmonary embolism have no symptoms. If you do have symptoms, they can include shortness of breath, chest pain or coughing up blood. Symptoms of a blood clot include warmth, swelling, pain, tenderness and redness of the leg. The goal of treatment is to break up clots and help keep other clots from forming.
Causes of pulmonary embolism
A pulmonary embolus is most often caused by a blood clot that develops in a vein outside the lungs. The most common blood clot is one in a deep vein of the thigh or in the pelvis (hip area). This type of clot is called a deep vein thrombosis. The blood clot breaks off and travels to the lungs where it lodges.
Less common causes include air bubbles, fat droplets, amniotic fluid, or clumps of parasites or tumor cells.
You are more likely to get this condition if you or your family has a history of blood clots or certain clotting disorders.
A pulmonary embolus may occur 8:
- After childbirth
- After heart attack, heart surgery, or stroke
- After severe injuries, burns, or fractures of the hips or thigh bone
- After surgery, most commonly bone, joint, or brain surgery
- During or after a long plane or car ride
- If you have cancer
- If you take birth control pills or estrogen therapy
- Long-term bed rest or staying in one position for a long time
Disorders that may lead to blood clots include 8:
- Diseases of the immune system that make it harder for the blood to clot.
- Inherited disorders that make the blood more likely to clot. One such disorder is antithrombin III deficiency.
Prevention of pulmonary embolism
Blood thinners may be prescribed to help prevent deep vein thrombosis (DVT) in people at high risk, or those who are undergoing high-risk surgery.
If you had a deep vein thrombosis, your provider will prescribe pressure stockings. Wear them as instructed. They will improve blood flow in your legs and reduce your risk of blood clots.
Moving your legs often during long plane trips, car trips, and other situations in which you are sitting or lying down for long periods can also help prevent deep vein thrombosis. People at very high risk for blood clots may need shots of a blood thinner called heparin when they take a flight that lasts longer than 4 hours.
Do not smoke. If you smoke, quit. Women who are taking estrogen must stop smoking. Smoking increases your risk of developing blood clots.
Symptoms of pulmonary embolism
Main symptoms of a pulmonary embolism include chest pain that may be any of the following:
- Under the breastbone or on one side
- Sharp or stabbing
- Burning, aching, or a dull, heavy sensation
- Often gets worse with deep breathing
- You may bend over or hold your chest in response to the pain
Other symptoms may include:
- Bluish skin (cyanosis)
- Dizziness, lightheadedness, or fainting
- Fast breathing or wheezing
- Fast heart rate
- Feeling anxious
- Leg pain, redness, or swelling
- Low blood pressure
- Sudden cough, possibly coughing up blood or bloody mucus
- Shortness of breath that starts suddenly
- Sweating, clammy skin.
How is pulmonary embolism diagnosed?
The health care provider will perform a physical exam and ask about your symptoms and medical history.
The following lab tests may be done to see how well your lungs are working:
- Arterial blood gases
- Pulse oximetry
The following imaging tests can help determine where the blood clot is located:
- Chest x-ray
- CT angiogram of the chest
- Pulmonary ventilation/perfusion scan, also called a V/Q scan
- Pulmonary angiogram
Other tests that may be done include:
- Chest CT scan
- D-dimer blood test
- Doppler ultrasound exam of the legs
- Echocardiogram (ECG)
Blood tests may be done to check if you have an increased chance of blood clotting, including:
- Antiphospholipid antibodies
- Genetic testing to look for changes that make you more likely to develop blood clots
- Lupus anticoagulant
- Protein C and protein S levels
Treatment for pulmonary embolism
A pulmonary embolus requires treatment right away. You may need to stay in the hospital:
- You will receive medicines to thin the blood and make it less likely your blood will form more clots.
- In cases of severe, life-threatening pulmonary embolism, treatment may involve dissolving the clot. This is called thrombolytic therapy. You will receive medicines to dissolve the clot.
Whether or not you need to stay in the hospital, you will likely need to take medicines at home to thin the blood:
- You may be given pills to take or you may need to give yourself injections.
- For some medicines, you will need blood tests to monitor your dosage.
- How long you need to take these medicines depends mostly on the cause and size of your blood clot.
- Your provider will talk to you about the risk of bleeding problems when you take these medicines.
If you cannot take blood thinners, your doctor may suggest surgery to place a device called an inferior vena cava filter (IVC filter). This device is placed in the main vein in your belly. It keeps large clots from traveling into the blood vessels of the lungs. Sometimes, a temporary filter can be placed and removed later.
Outlook (Prognosis) of pulmonary embolism
How well a person recovers from a pulmonary embolus can be hard to predict. It often depends on:
- What caused the problem in the first place (for example, cancer, major surgery, or an injury)
- The size of the blood clot in the lungs
- If the blood clot dissolves over time
Some people can develop long-term heart and lung problems.
Death is possible in people with a severe pulmonary embolism.
Lungs infection
Pneumonia is an infection in one or both of the lungs. Many germs, such as bacteria, viruses, and fungi, can cause pneumonia. You can also get pneumonia by inhaling a liquid or chemical. People most at risk are older than 65 or younger than 2 years of age, or already have health problems.
Symptoms of pneumonia vary from mild to severe. See your doctor promptly if you
- Have a high fever
- Have shaking chills
- Have a cough with phlegm that doesn’t improve or gets worse
- Develop shortness of breath with normal daily activities
- Have chest pain when you breathe or cough
- Feel suddenly worse after a cold or the flu
Your doctor will use your medical history, a physical exam, and lab tests to diagnose pneumonia. Treatment depends on what kind you have. If bacteria are the cause, antibiotics should help. If you have viral pneumonia, your doctor may prescribe an antiviral medicine to treat it.
Preventing pneumonia is always better than treating it. Vaccines are available to prevent pneumococcal pneumonia and the flu. Other preventive measures include washing your hands frequently and not smoking.
Lung nodule
A lung nodule is also called a spot on your lung (pulmonary nodule). It is usually round or oval in shape. They are easy to find but can be hard to diagnose. Nodules are found in 1 out of every 4 chest CT scans. Most nodules (more than 90%) are benign and not cancerous 9. Benign or non-cancerous nodules can be caused by previous infections or old surgery scars.
Nodules need to be examined and watched closely because they might be a small cancer. Finding cancers early when they are small and curable, is the goal of a screening program. Almost eighty percent of people who have a small lung cancer (1 cm in size, about ½ inch) surgically removed, live at least five years after the diagnosis and are considered cured. Unfortunately people with larger lung cancer have a lower survival rate. Early detection is the key to a better outcome.
What are the symptoms of a lung nodule?
Nearly 90% of all lung nodules are discovered by accident 9. Usually they are seen on a chest x-rays or a CT scan that was performed for other reasons. Symptoms are few if any, but may include those similar to a chest cold or a mild flu.
How is a lung nodule examined?
If a lung nodule is considered highly suspicious for lung cancer based on its size, shape and appearance on chest x-ray or CT scan as well as considering other risk factors such as your smoking history and family history of cancer, it will need to be biopsied to determine if it is cancerous. The biopsy is a simple procedure of getting a sample from the pulmonary nodule for microscopic exam. It can be done surgically, bronchoscopically and by placing a needle thru the chest wall under radiographic guidance.
The bronchoscope approach is an outpatient procedure without any cutting, sutures or sticking needles thru the chest wall. After heavy sedation and numbing of mouth and throat, the bronchoscope is inserted in your airways and is guided to the lung nodule. A sample is taken and immediately examined by a pathologist (a doctor who identifies diseases by studying cells and tissue under a microscope).
The pathologist will determine if the nodule is cancerous or benign. If it is benign or not cancerous, your doctor will ask you to come back in the future to re-examine the spot with another X-ray. Your doctor will watch the nodule for any changes and catch it early if it becomes cancerous. If the nodule is cancerous, a few more samples will be taken or other tests performed to determine if the cancer has spread. The next steps will be discussed.
How are lung nodules treated?
Benign or non-cancerous lung nodules do not need treatment.
In some cases your doctor may recommend annual chest imaging to see if a lung nodule grows or changes over time 10.
If a lung nodule is new or has changed in size, shape or appearance, your doctor may recommend further testing — such as a CT scan, positron emission tomography (PET) scan, bronchoscopy or tissue biopsy — to determine if it’s cancerous.
Lung cancer, if localized is usually removed surgically. If part of the cancer has spread to other parts of the body, you may need radiation and/or chemotherapy with or without surgery.
- Asthma. Medline Plus. https://medlineplus.gov/asthma.html[↩]
- Asthma – quick-relief drugs. Medline Plus. https://medlineplus.gov/ency/patientinstructions/000008.htm[↩][↩][↩]
- Asthma – control drugs. Medline Plus. https://medlineplus.gov/ency/patientinstructions/000005.htm[↩]
- Acute Bronchitis. Medline Plus. https://medlineplus.gov/acutebronchitis.html[↩]
- Bronchitis – acute. Medline Plus. https://medlineplus.gov/ency/article/001087.htm[↩][↩]
- Chronic obstructive pulmonary disease. Medline Plus. https://medlineplus.gov/ency/article/000091.htm[↩]
- Pulmonary Embolism. Medline Plus. https://medlineplus.gov/pulmonaryembolism.html[↩]
- Pulmonary embolus. Medline Plus. https://medlineplus.gov/ency/article/000132.htm[↩][↩]
- What is a lung nodule ? National Jewish Health. https://www.nationaljewish.org/conditions/lung-nodules[↩][↩]
- Can lung nodules be cancerous ? Mayo Clinic. http://www.mayoclinic.org/diseases-conditions/lung-cancer/expert-answers/lung-nodules/FAQ-20058445?p=1[↩]

{kind=link}