Contents
- Stomach cancer
- Stomach anatomy
- Types of stomach cancers
- Stomach cancer causes
- Stomach Cancer Risk Factors
- Stomach cancer prevention
- Stomach cancer symptoms
- Stomach cancer diagnosis
- Stomach Cancer Stages
- Stomach cancer treatment
- Stomach Cancer Treatment Based on Stage
- Stomach cancer prognosis
- Stomach cancer survival rate
Stomach cancer
Stomach cancer also called gastric cancer, occurs when cells in your stomach grow abnormally and develop into tumors, which could become harmful if left untreated 1. Stomach cancer is common worldwide but rare in the U.S. Common stomach cancer symptoms like unexplained weight loss and stomach pain often don’t appear in the early stages.
The stomach is a J-shaped pouch like organ in the left upper abdomen. It is part of the digestive system, which processes nutrients (vitamins, minerals, carbohydrates, fats, proteins, and water) in foods that are eaten and helps pass waste material out of the body. Food moves from the throat to the stomach through a hollow, muscular tube called the esophagus. The esophagus joins the stomach at the gastroesophageal junction, which is just beneath the diaphragm (the thin sheet of breathing muscle under the lungs). After leaving the stomach, partly-digested food passes into the small intestine and then into the large intestine.
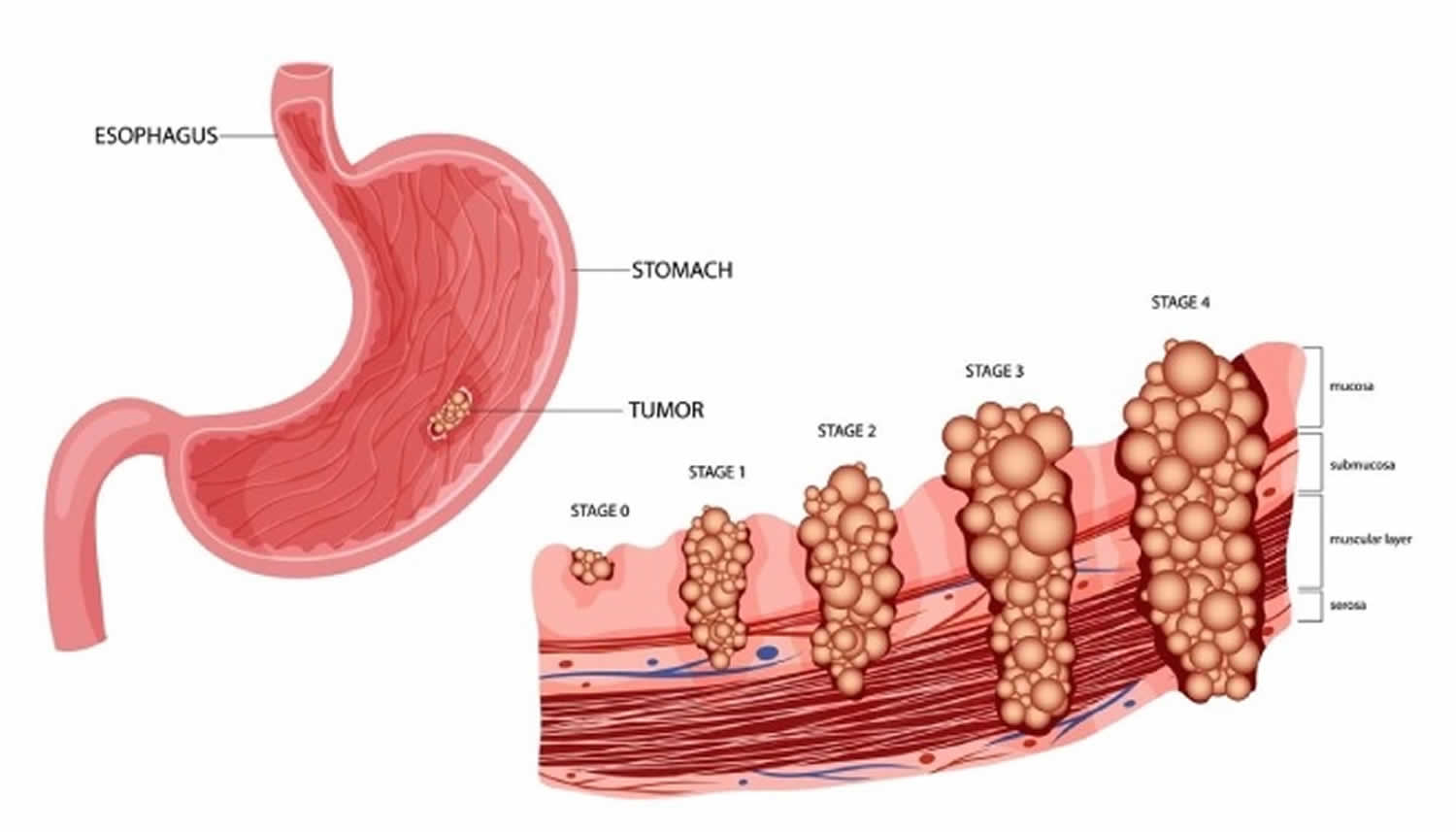
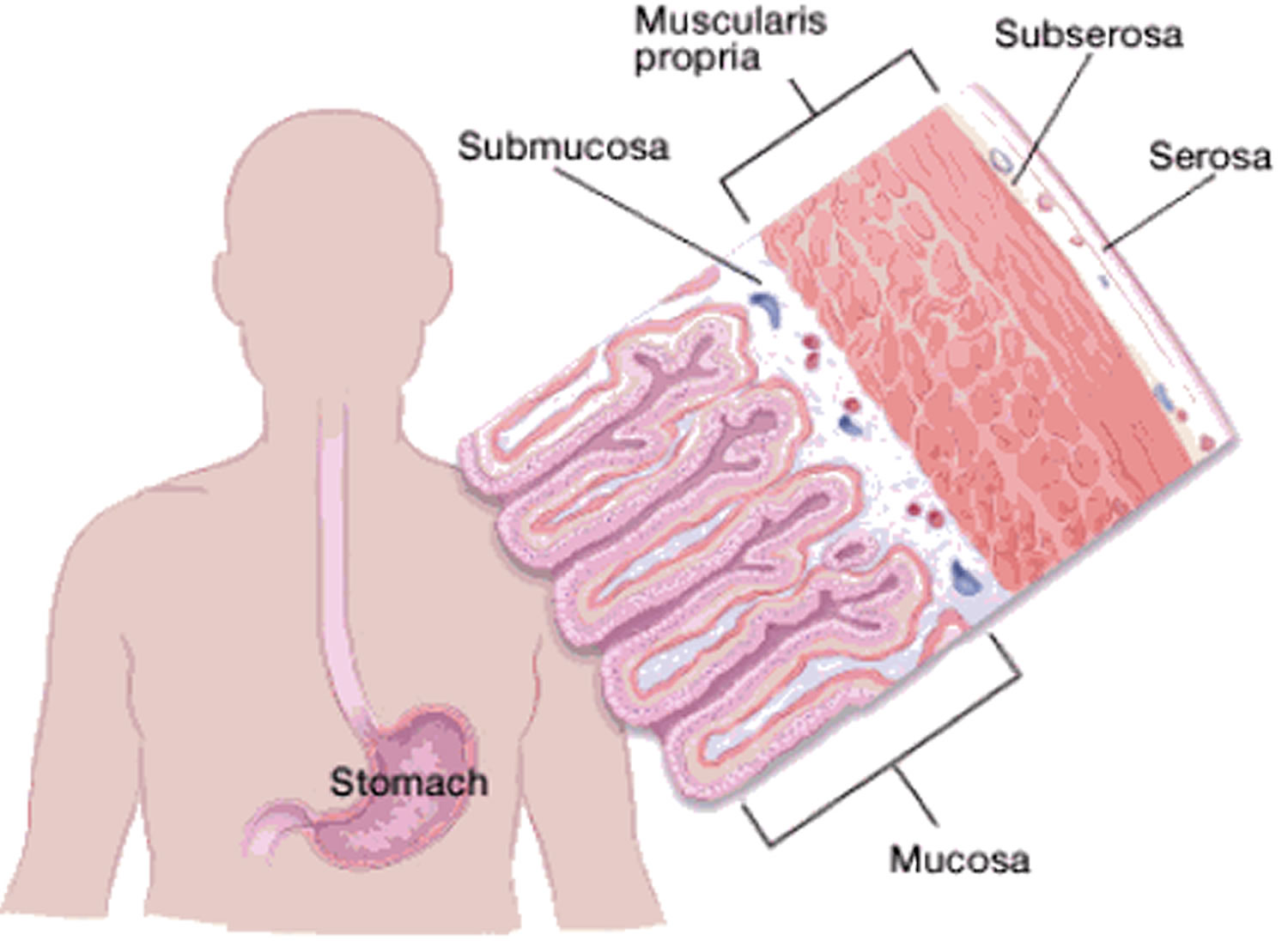
The stomach wall has 5 layers:
The stomach wall is made up of several layers of mucous membrane, connective tissue with blood vessels and nerves, and muscle fibers (see Figure 4).
- The innermost layer is the mucosa. This is where stomach acid and digestive enzymes are made. Most stomach cancers start in this layer.
- Next is a supporting layer called the submucosa.
- Outside of this is the muscularis propria, a thick layer of muscle that moves and mixes the stomach contents.
- The outer 2 layers, the subserosa and the outermost serosa, wrap the stomach.
The layers are important in determining the stage (extent) of the cancer and in helping to determine a person’s prognosis (outlook). Stomach cancer cells usually begin in the inner lining (the mucosa) of your stomach. They then grow deeper into your stomach walls as the cancer develops. As a cancer grows from the mucosa into deeper layers, the stage becomes more advanced and the prognosis is not as good.
Stomach cancer should not be confused with other cancers that can occur in the abdomen, like cancer of the colon (large intestine), liver, pancreas, or small intestine because these cancers may have different symptoms, different outlooks, and different treatments.
The National Cancer Institute and the American Cancer Society estimate for stomach cancer in the United States for 2025 are 2, 3:
- About 30,300 new cases of stomach cancer. 17,720 in men and 12,580 in women.
- About 10,780 deaths from stomach cancer. 6,400 men and 4,380 women.
- The rate of new cases of stomach cancer was 7.3 per 100,000 men and women per year. The death rate was 2.7 per 100,000 men and women per year. These rates are age-adjusted and based on 2018–2022 cases and 2019–2023 deaths.
- 5-Year Relative Survival: 37.9%. Relative survival is an estimate of the percentage of patients who would be expected to survive the effects of their cancer. It excludes the risk of dying from other causes. Because survival statistics are based on large groups of people, they cannot be used to predict exactly what will happen to an individual patient. No two patients are entirely alike, and treatment and responses to treatment can vary greatly.
- Percentage of All Cancer Deaths: 1.7%.
- In 2022, there were an estimated 140,524 people living with stomach cancer in the United States.
Stomach cancer represents 1.5% of all new cancer cases diagnosed in the US each year. In 2025, it is estimated that there will be 30,300 new cases of stomach cancer and an estimated 10,780 people will die of this disease 4. Approximately 0.8 percent of men and women will be diagnosed with stomach cancer at some point during their lifetime, based on 2018–2021 data. For stomach cancer, death rates increase with age. Stomach cancer is the fifteenth leading cause of cancer death in the United States. The number of deaths was 2.7 per 100,000 men and women per year based on 2019-2023 deaths. Stomach cancer is more common in men than women and among other races and ethnicities than non-Hispanic whites. Stomach cancer is most frequently diagnosed among people aged 65-74. The average age of people when they are diagnosed is 68. About 6 of every 10 people diagnosed with stomach cancer each year are 65 or older. Age, diet and stomach disease, including infection with Helicobacter pylori (H. pylori) bacteria can affect your risk of developing stomach cancer. The number of new cases of stomach cancer was 7.3 per 100,000 men and women per year based on 2018-2022 cases. The lifetime risk of developing stomach cancer is higher in men (about 1 in 101) than in women (about 1 in 155) 3. But each person’s risk can be affected by many other factors.
In the US, the number of new cases of stomach cancer has been dropping by about 1.5% each year over the last 10 years 3.
For much of the early 20th century, stomach cancer was the leading cause of cancer death in the United States, but today it is well down on this list. The reasons for this aren’t completely clear, but two main factors are thought to have been important:
- The increased use of refrigeration for food storage, which has led to people eating fewer salted and smoked foods (known risk factors for stomach cancer).
- The decline in the number of people infected with the Helicobacter pylori (H. pylori) bacteria, which is thought to be a major cause of stomach cancer.
The incidence and mortality of gastric cancer have fallen dramatically in US and elsewhere over the past 70 years 5. Nonetheless, gastric cancer remains a major public health issue as the fourth most common cancer and the second leading cause of cancer death worldwide, particularly in East Asia 6. In 2000, about 880 000 people were diagnosed with gastric cancer and approximately 650 000 died of the disease 7. In Japan, gastric cancer remains the most common type of cancer among both men and women. Age-standardized incidence rates in Japan are 69.2 per 100 000 in men and 28.6 per 100 000 in women 8. In contrast to the increasing incidence of proximal tumors in the West, distal tumors continue to predominate in Japan. However, even in Japan, the proportion of proximal stomach cancers has increased among men 9.
The wall of the stomach is made up of 3 layers of tissue: the mucosal (innermost) layer, the muscularis (middle) layer, and the serosal (outermost) layer. Stomach cancer begins in the cells lining the mucosal layer and spreads through the outer layers as it grows. Almost all stomach cancers are adenocarcinomas (cancers that begin in cells that make and release mucus and other fluids) 10. Other types of gastric cancer are gastrointestinal carcinoid tumors, gastrointestinal stromal tumors, and lymphomas 10.
Infection with bacteria called Helicobacter pylori is a common cause of gastric cancer.
Stomach cancer can happen in any part of your stomach. In the United States, stomach cancer is more likely to start by the gastroesophageal junction. This is the part where the long tube that carries food you swallow meets the stomach. The muscular tube that carries food to the stomach is called the esophagus. However, in most of the world, stomach cancers happen in the main part of the stomach. This part is called the stomach body.
The two main tumor sites of gastric adenocarcinoma are proximal (cardia) and distal (noncardia). Despite a decline in distal gastric cancers, proximal tumors have been increasing in incidence since the 1970s, especially among males in the Western countries 11, 12. These gastric tumor types predominate in populations from different geographic locations, racial and socio-economic groups. They may also differ in genetic susceptibility, pathologic profile, clinical presentation, and prognosis. The observed differences between gastric cancers by anatomic site suggest that they are distinct diseases with different etiologies.
- Gastric cancer is often diagnosed at an advanced stage because there are no early signs or symptoms.
- Since symptoms of stomach cancer often do not appear until the disease is advanced, only about 1 in 5 stomach cancers in the United States is found at an early stage, before it has spread to other areas of the body.
Stomach cancer mostly affects older people – two-thirds of people who have it are over age 65. Your risk of getting it is also higher if you:
- Have had a Helicobacter pylori infection 13, 14, which is a type of bacteria that lives in and affects the mucous lining of the stomach
- Have chronic gastritis, a long-term inflammation of the stomach
- Are a man
- Eat lots of salted, smoked, or pickled foods
- Smoke cigarettes
- Have a family history of stomach cancer
- A diet low in fruits and vegetables
- Pernicious anaemia 15, a decrease in red blood cells when the intestines cannot properly absorb vitamin B12
It is hard to diagnose stomach cancer in its early stages 1.
Indigestion and stomach discomfort can be symptoms of early cancer, but other problems can cause the same symptoms. In advanced cases, there may be blood in your stool, vomiting, unexplained weight loss, jaundice, or trouble swallowing. Doctors diagnose stomach cancer with a physical exam, blood and imaging tests, an endoscopy, and a biopsy.
Because it is often found late, it can be hard to treat stomach cancer. Treatment options include surgery, chemotherapy, radiation or a combination.
Figure 1. Stomach
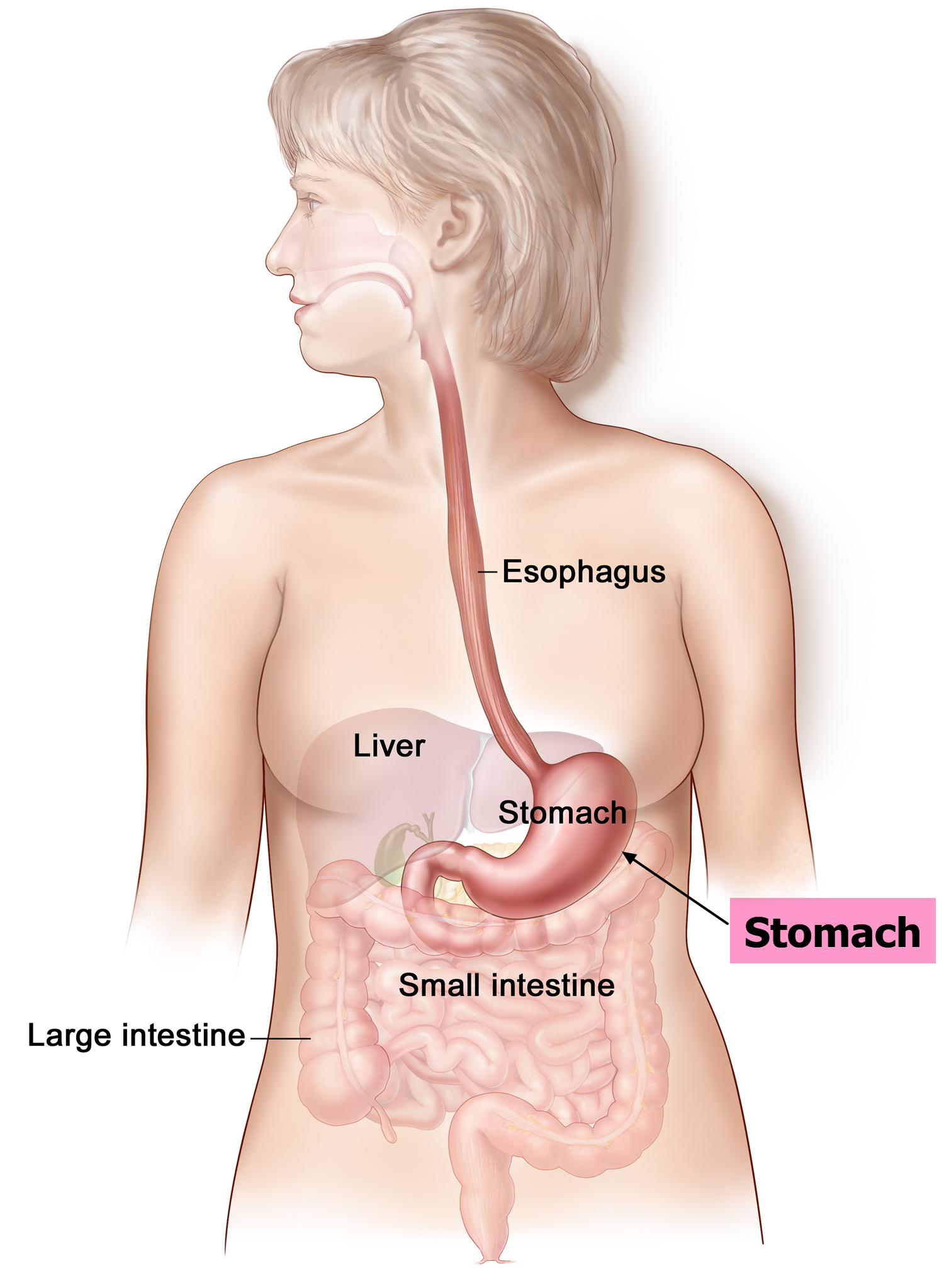
Figure 2. Parts of the stomach
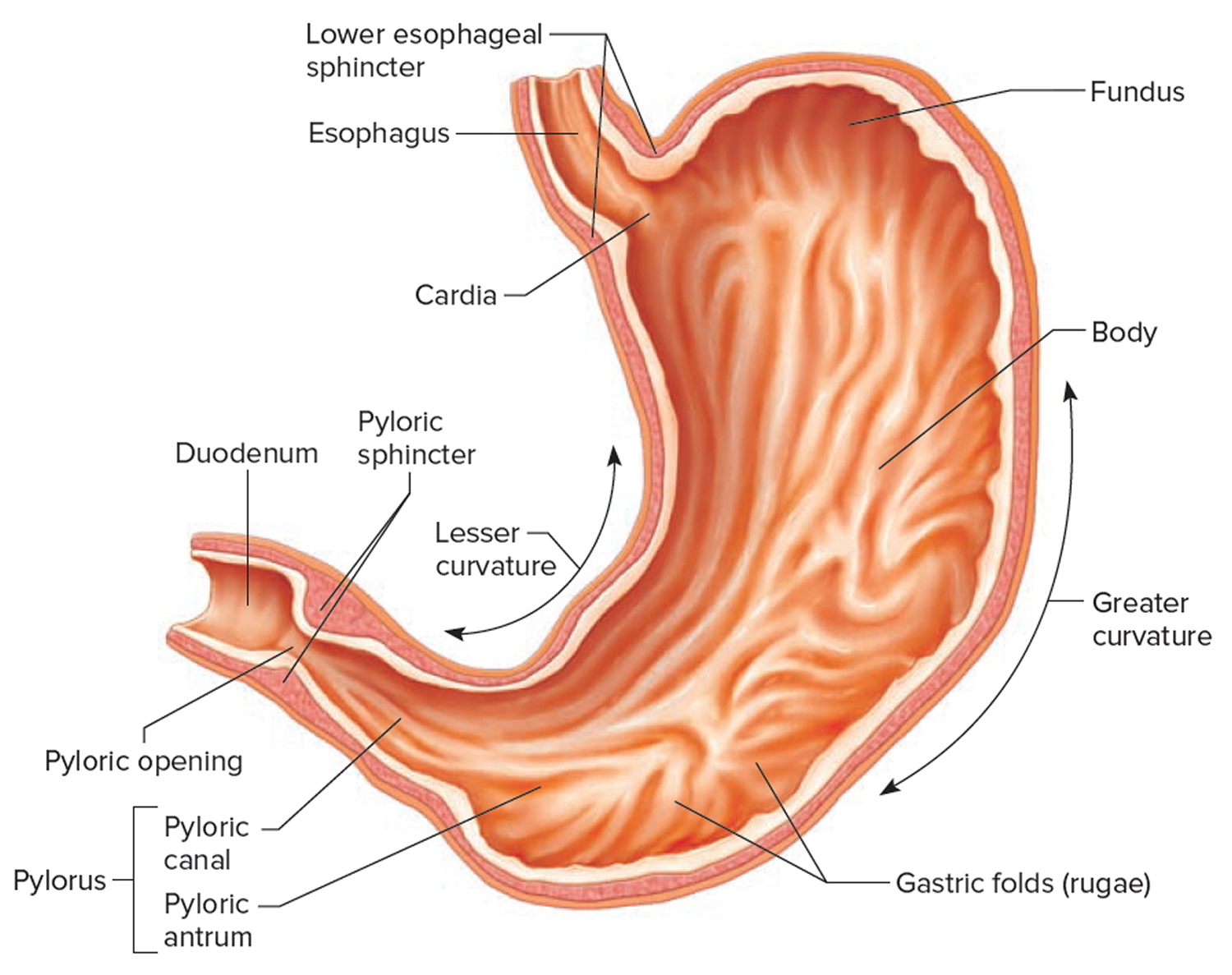
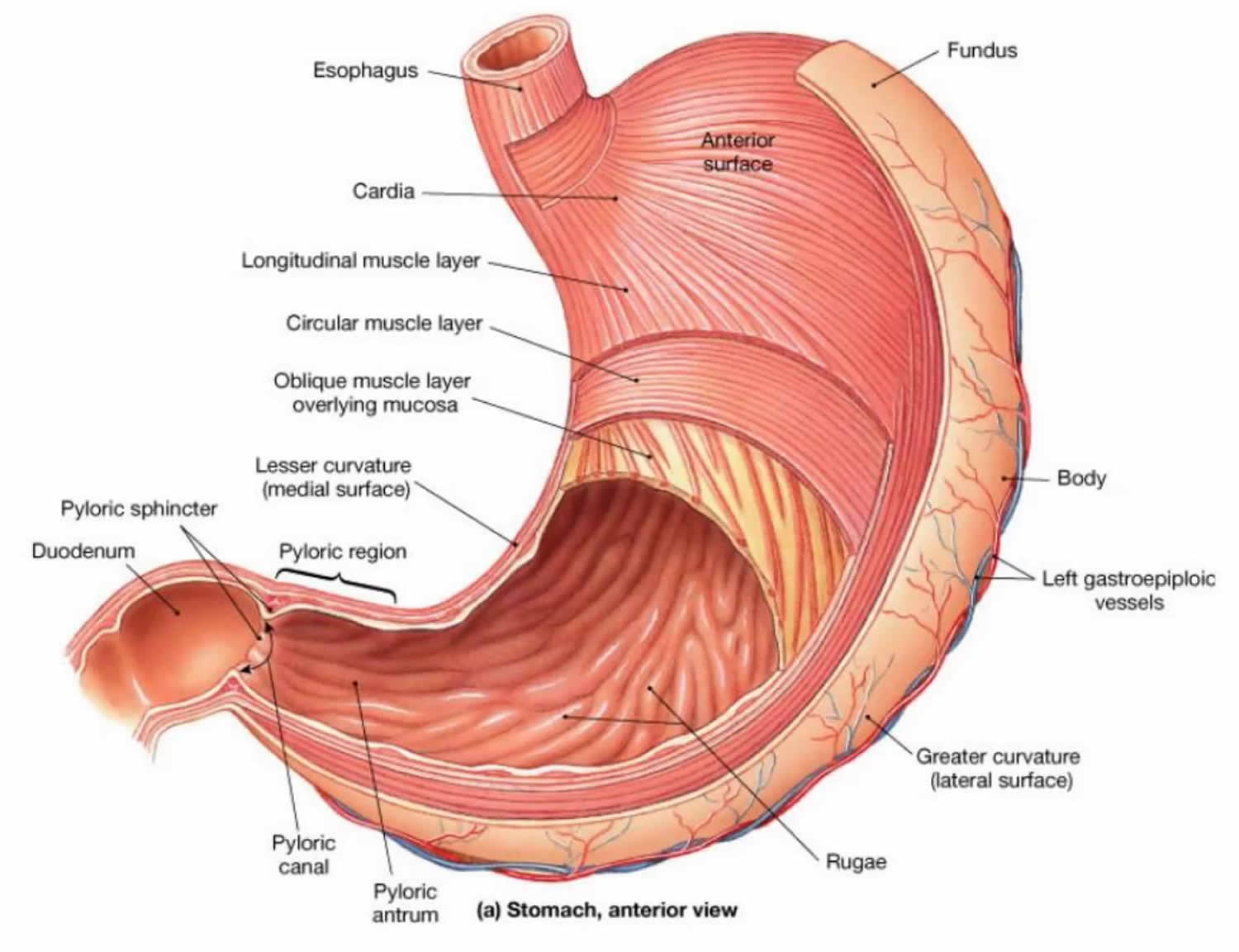
Figure 3. Stomach mucus and gastric acid secreting cells
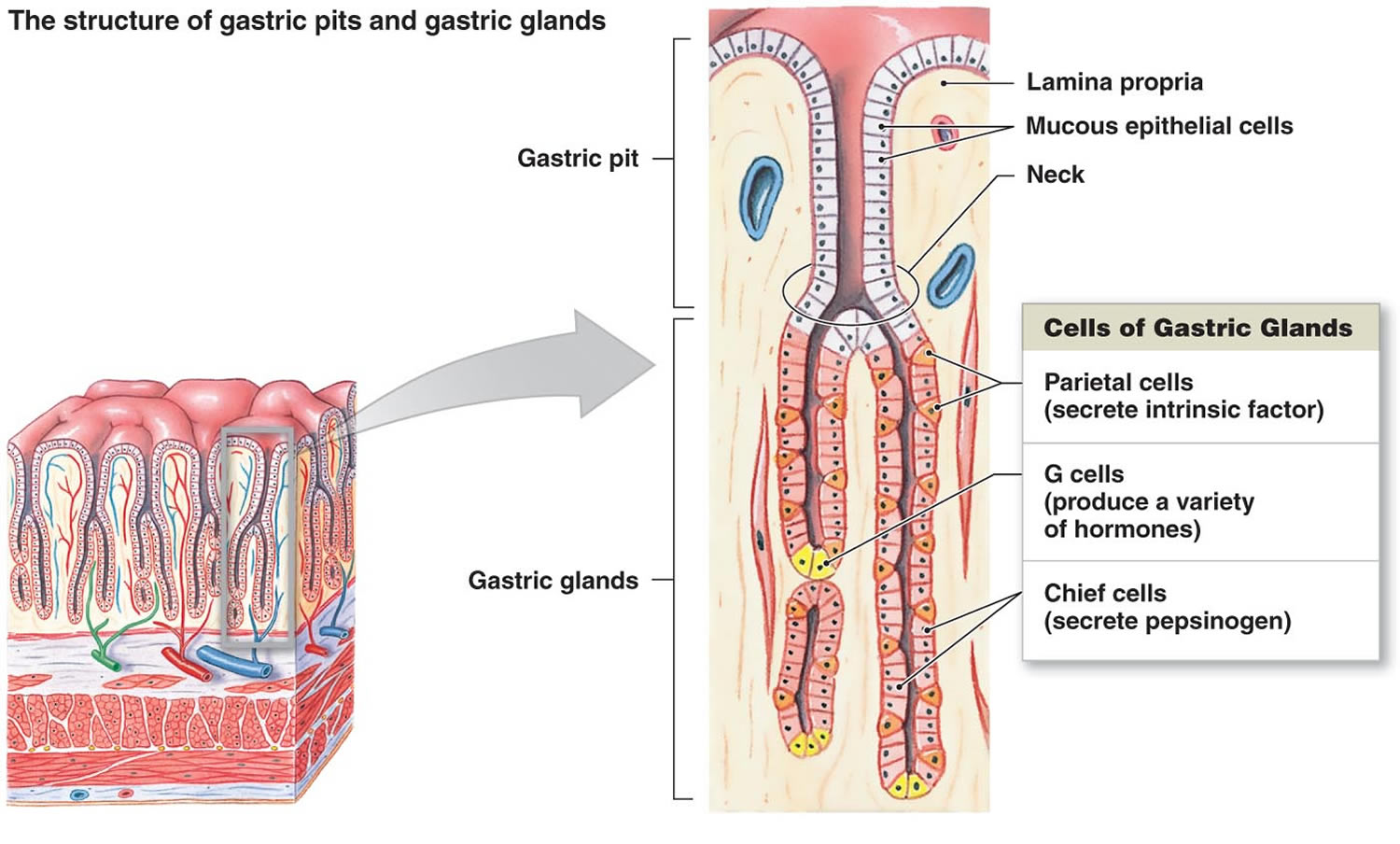
Figure 4. Layers of the stomach
Can stomach cancer be found early?
Screening is testing for a disease, such as cancer, in people without symptoms. In countries such as Japan, where stomach cancer is very common, mass screening of the population has helped find many cases at an early, curable stage. Mass screening of the population has helped find many stomach cancers at an early, possibly more curable stage. However, it’s not clear if this has led to a lower number of stomach cancer deaths.
Studies in the United States have not found that routine screening in people at average risk for stomach cancer is useful, because stomach cancer is not that common. On the other hand, people with certain stomach cancer risk factors may benefit from screening.
- Hereditary diffuse gastric cancer (HDGC) is a rare inherited condition in which people have a greatly increased risk of stomach cancer, which often develops at a fairly early age. Hereditary diffuse gastric cancer (HDGC) is most often caused by an inherited mutation in the CDH1 gene. It’s very important to recognize people and families with this inherited syndrome, because most people who have it will develop stomach cancer. Families with hereditary diffuse gastric cancer (HDGC) typically have two or more close relatives who develop stomach cancer (usually the diffuse type), and/or at least one person who is diagnosed before age 50. Some family members might also develop invasive lobular breast cancer. Doctors often refer people who might have hereditary diffuse gastric cancer (HDGC) to a genetics professional, so they can discuss possibly getting genetic testing. If testing is done and shows a person has a mutation (abnormal change) in the CDH1 gene, doctors often recommend they consider having their stomach removed (typically between the ages of 20 and 30) before cancer develops. However, this operation called a total gastrectomy can lead to long-term changes in the way a person eats.
- Some other hereditary cancer syndromes are also linked with an increased risk for stomach cancer, including Lynch syndrome, familial adenomatous polyposis (FAP), Li-Fraumeni syndrome, and Peutz-Jeghers syndrome. The risk of stomach cancer with these syndromes is not nearly as high as it is with hereditary diffuse gastric cancer (HDGC), so removal of the stomach (total gastrectomy) is not typically recommended for people who have these syndromes. However, doctors might recommend getting regular tests to try to find stomach cancer early in some of these people.
If you have any questions about your stomach cancer risk or about the benefits of screening, please ask your doctor.
The benefits of screening might outweigh the risks in some people who are at increased risk for stomach cancer because they have certain risk factors. For example, certain potentially pre-cancerous stomach conditions or inherited conditions such as Lynch syndrome or familial adenomatous polyposis (FAP). For example, upper endoscopy might be recommended at regular intervals in these people.
If you have risk factors that might increase your risk of stomach cancer, talk to your doctor about the possible pros and cons of stomach cancer screening for you.
Screening isn’t usually recommended for people in families with hereditary diffuse gastric cancer (HDGC). Instead, doctors often recommend that people who have changes in the CDH1 gene that causes this syndrome consider having their stomach removed (total gastrectomy), because their risk of stomach cancer is very high.
Some of the tests that could be used for screening, such as upper endoscopy, are described in Stomach Cancer Diagnosis.
Because routine screening for stomach cancer is not done in the United States, most people are not diagnosed with stomach cancer until they have certain signs and symptoms that point to the need for medical tests.
Stomach anatomy
To understand stomach cancer, it helps to know about the normal structure and function of your stomach. Your stomach is a sac-like organ that’s an important part of your digestive system. After food is chewed and swallowed, it enters your esophagus, a muscular tube that carries food through from your throat and chest to your stomach. Your esophagus joins your stomach at the gastroesophageal (GE) junction, which is just beneath the diaphragm (the thin sheet of breathing muscle under the lungs). Your stomach then starts to digest the food you eat by secreting gastric juice. The food and gastric juice are mixed and then emptied into the first part of the small intestine called the duodenum.
Some people use the word ‘stomach’ to refer to the belly area. The medical term for this area is the abdomen. For instance, some people with pain in this area would say they have a ‘stomach ache’, when in fact the pain could be coming from some other organ in the area. Doctors would call this symptom ‘abdominal pain’, because the stomach is only one of many organs in the abdomen.
Stomach cancer is different from other cancers that can occur in the abdomen, like cancer of the colon or rectum (large intestine), liver, pancreas, or small intestine. These cancers can have different symptoms, different outlooks, and different treatments.
Your stomach is a muscular bag that is divided into several anatomical parts: the cardia, fundus, body, antrum and pylorus. :
- Cardia: The cardia is the area where the esophagus connects to the stomach
- Fundus: The fundus is the dome-shaped of the stomach above the cardia, often containing gas and food.
- Body (Corpus): The body is the largest and main part of the stomach, extending from the fundus to the antrum.
- Antrum: The lower part of the stomach, located below the body, connecting to the pylorus.
- Pylorus: The narrowest part of the stomach, connecting to the duodenum (the first part of the small intestine). It’s divided into the pyloric antrum, pyloric canal, and pyloric sphincter, which controls the release of partially digested food into the small intestine
At each end of your stomach there is a muscular valve called a sphincter. These muscular valves control the movement of food through your digestive system.
The sphincters or muscular valves are the:
- Cardiac sphincter also called lower esophageal sphincter (LES) or gastroesophageal sphincter, is a ring of muscle at the bottom of the esophagus that prevents stomach contents from flowing back up into the esophagus. It acts like a one-way valve, opening to allow food to enter the stomach and then closing to prevent reflux.
- Pyloric sphincter is a ring of muscle located at the bottom of your stomach, serving as a valve between the stomach and the duodenum, the first part of the small intestine. Its primary function is to regulate the passage of partially digested food and stomach juices from the stomach into the small intestine. It opens and closes to control the flow of chyme, allowing it to enter the duodenum at appropriate intervals.
Your stomach has 5 layers.
- The innermost layer is the mucosa. This is where stomach acid and digestive enzymes are made. Most stomach cancers start in this layer.
- Next is a supporting layer called the submucosa.
- Outside of this is the muscularis propria, a thick layer of muscle that helps move and mix the stomach contents.
- The outer 2 layers, the subserosa and the outermost serosa, wrap the stomach.
The layers of your stomach are important in determining the stage (extent) of the cancer, which can affect a person’s treatment options and prognosis (outlook). Gastric cancer begins in the cells lining the mucosal layer and spreads through the outer layers as it grows. As a cancer grows from the mucosa into deeper layers, the stage becomes more advanced and treatment might need to be more extensive.
Note that stromal tumors of the stomach begin in supporting connective tissue and are treated differently from stomach cancer.
Your stomach’s purpose is to digest food and send it to your small intestine. It has three functions:
- Temporarily store food.
- Contract and relax to mix and break down food.
- Produce enzymes, acid and other specialized cells to digest food.
How does the stomach work?
Food passes from your esophagus into your stomach. The stomach then stores the food and breaks it down (digests it) so your body can absorb it. It does this by producing gastric juice which mixes with the food, so it is easy to digest.
Glands in the inner lining of your stomach make gastric juice. It contains stomach acid, water and a protein called pepsin. It begins to flow as soon as you smell something. The stomach muscle contracts, churning the food with the juice, which changes it to a thick liquid. It takes a couple of hours for this to happen. Then the liquid moves into the bowel (small and large intestines) where the body absorbs it.
The stomach continues to produce gastric juice and hormones, even when it’s empty. It also produces a thick mucus to protect the lining of the stomach from the acid and pepsin.
Types of stomach cancers
Different types of stomach cancer include 16:
Adenocarcinoma
About 90% to 95% of cancers of the stomach are adenocarcinomas 16. When the term stomach cancer or gastric cancer is used, it almost always refers to an adenocarcinoma. Most stomach cancers start in the gland cells in the innermost lining of the stomach (the mucosa).
There are 2 main types of stomach adenocarcinomas 16:
- The intestinal type tends to have a slightly better prognosis (outlook). The cancer cells are more likely to have certain gene changes that might allow for treatment with targeted drug therapy.
- The diffuse type tends to grow spread more quickly. It is less common than the intestinal type, and it tends to be harder to treat.
Lymphoma
These cancers start in immune system cells called lymphocytes. Lymphomas usually start in other parts of the body, but some can start in the wall of the stomach. The treatment and outlook for these cancers depend on the type of lymphoma and other factors. For more information, see Non-Hodgkin Lymphoma.
Gastrointestinal stromal tumor (GIST)
These are rare tumors that start in very early forms of cells in the wall of the stomach called interstitial cells of Cajal. Some of these tumors are much more likely than others to grow into other areas or spread to other parts of the body. Although GISTs can start anywhere in the digestive tract, most start in the stomach.
Neuroendocrine tumors (including carcinoids)
Neuroendocrine tumors (NETs) start in cells in the stomach or other parts of the digestive tract that act like nerve cells in some ways and like hormone-making (endocrine) cells in others. Most neuroendocrine tumors (NETs) tend to grow slowly and do not spread to other organs, but some can grow and spread quickly. About 3% of stomach cancers are carcinoid tumors. These are tumors that start in hormone-making cells of the stomach. Most of these tumors do not spread to other organs.
Other cancers
Other types of cancer, such as squamous cell carcinomas, small cell carcinomas, and leiomyosarcomas, can also start in the stomach, but these cancers are very rare.
Stomach cancer causes
Researchers don’t know what causes stomach cancer 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39. Experts believe most stomach cancers is a multifactorial disease that includes both lifestyle and environmental risk factors such as Helicobacter pylori (H. pylori) infection, low socioeconomic status, dietary factors, such as high intake of salty and smoked food and low consumption of fruits and vegetables, fiber intake, in addition to tobacco smoking, alcohol use, low physical activity, obesity, radiation, gastroesophageal reflux disease (GERD), positive family history and inherited predisposition 40, 41, 42, 43. Though, not everyone with these risk factors gets stomach cancer. So more research is needed to find out exactly what causes it.
Stomach cancer begins when something hurts cells in the inner lining of the stomach. It causes the cells to develop changes (mutations) in their DNA. A cell’s DNA holds the instructions that tell a cell what to do. The changes tell the cells to multiply quickly. The cells can go on living when healthy cells would die as part of their natural lifecycle. This causes a lot of extra cells in the stomach. The cells can form a mass called a tumor.
Cancer cells in the stomach can invade and destroy healthy body tissue. They might start to grow deeper into the wall of the stomach. In time, cancer cells can break away and spread to other parts of the body. When cancer cells spread to another part of the body it’s called metastasis.
Pre-cancerous changes in the stomach
Several changes thought to be pre-cancerous can occur in the inner lining of the stomach.
In atrophic gastritis, the normal gland cells of the stomach are either fewer or absent. There is also some degree of inflammation (in which the stomach cells are damaged by cells of the immune system). Atrophic gastritis is often caused by infection with H. pylori bacteria. It can also be caused by an autoimmune reaction, in which a person’s immune system attacks the cells lining the stomach. Some people with this condition go on to develop pernicious anemia or other stomach problems, including cancer.
Another possible pre-cancerous change is intestinal metaplasia. In this condition, the cells that normally line the stomach are replaced by cells that look like the cells that usually line the intestine. People with this condition often have chronic atrophic gastritis as well. This might also be related to H. pylori infection.
Both atrophic gastritis and intestinal metaplasia can lead to having too few gland cells, which would normally secrete substances that help protect the cells in the stomach’s inner lining. Damage to the DNA inside these cells can sometimes lead to dysplasia, in which the cells become larger and very abnormal looking more like cancer cells. In some cases, dysplasia can then progress to stomach cancer.
Changes in genes (DNA) in stomach cancer cells
Recent research has provided clues on how some stomach cancers form. For instance, H. pylori bacteria, particularly certain subtypes, can convert substances in some foods into chemicals that cause mutations (changes) in the DNA of the cells in the stomach lining. This may help explain why certain foods such as preserved meats increase a person’s risk for stomach cancer. On the other hand, some of the foods that might lower stomach cancer risk, such as fruits and vegetables, contain antioxidants like vitamin A and vitamin C that can block substances that damage a cell’s DNA.
Stomach cancers, like other cancers, are caused by changes in the DNA inside cells. DNA is the chemical that carries your genes, which control how our cells function. You look like your parents because they are the source of your DNA. But DNA affects more than how you look.
Some genes control when cells grow, divide into new cells, and die:
- Genes that normally help cells grow, divide, and stay alive can sometimes change to become oncogenes. An oncogene is a mutated gene that has the potential to cause cancer 44. Before an oncogene becomes mutated, it is called a proto-oncogene, and it plays a role in regulating normal cell division. Cancer can arise when a proto-oncogene is mutated, changing it into an oncogene and causing the cell to divide and multiply uncontrollably. Some oncogenes work like an accelerator pedal in a car, pushing a cell to divide again and again. Others work like a faulty brake in a car parked on a hill, also causing the cell to divide unchecked.
- Genes that help keep cell division under control, repair mistakes in DNA, or cause cells to die at the right time are called tumor suppressor genes. A tumor suppressor gene is a normal gene that helps regulate cell division and replication, preventing cells from growing out of control 45. When these genes are mutated, they can lose or reduce their function, which can contribute to cancer development.
Cancers can be caused by DNA changes that keep oncogenes turned on, or that turn off tumor suppressor genes.
Inherited versus acquired gene mutations
Inherited mutations in some genes can increase a person’s stomach cancer risk. But these are thought to cause only a small percentage of stomach cancers.
Most of the gene changes that lead to stomach cancer occur after birth. Some of these acquired mutations might be caused by risk factors such as H pylori infection or tobacco use. But other gene changes may just be random events that sometimes happen inside cells, without having an outside cause.
Development of stomach cancer
Stomach cancers tend to develop slowly over many years. Before a true cancer develops, pre-cancerous changes often occur in the inner lining (mucosa) of the stomach. These early changes rarely cause symptoms and therefore often go undetected.
Cancers starting in different sections of the stomach may cause different symptoms and tend to have different outcomes. The cancer’s location can also affect the treatment options. For example, cancers that start at the gastroesophageal (GE) junction are staged and treated the same as cancers of the esophagus. A cancer that starts in the cardia of the stomach but then grows into the gastroesophageal junction is also staged and treated like a cancer of the esophagus.
Stomach cancers can spread (metastasize) in different ways. They can grow through the wall of the stomach and invade nearby organs. They can also spread to the lymph vessels and nearby lymph nodes. Lymph nodes are bean-sized structures that help fight infections. The stomach has a very rich network of lymph vessels and nodes. As the stomach cancer becomes more advanced, it can travel through the bloodstream and spread to organs such as the liver, lungs, and bones. If cancer has spread to the lymph nodes or to other organs, the patient’s outlook is not as good.
Stomach Cancer Risk Factors
Anything that increases your risk of getting a disease is called a risk factor. Having a risk factor does not mean that you will get cancer; not having risk factors doesn’t mean that you will not get cancer. Talk with your doctor if you think you may be at risk.
Risk factors for gastric cancer include the following:
- Ongoing problems with stomach acid backing up into the esophagus, which is called gastroesophageal reflux disease (GERD)
- A diet high in salty and smoked foods. Stomach cancer risk is increased in people whose diets include large amounts of foods preserved by salting, such as salted fish and meat and pickled vegetables. Eating processed, grilled, or charcoaled meats regularly appears to increase risk of non-cardia stomach cancers.
- A diet low in fruits and vegetables. Eating few or no fruits likely increases the risk of stomach cancer. On the other hand, eating lots of fresh fruits (especially citrus fruits) and raw vegetables appears to lower the risk of stomach cancer.
- Eating foods that have not been prepared or stored properly.
- Infection in the stomach caused by bacteria called Helicobacter pylori (H. pylori) seems to be a major cause of stomach cancer, especially cancers in the lower (distal) part of the stomach. Long-term infection of the stomach with Helicobacter pylori (H. pylori) bacteria may lead to atrophic gastritis and other pre-cancerous changes of the inner lining of the stomach. People with stomach cancer have a higher rate of H. pylori infection than people without this cancer. Helicobacter pylori (H. pylori) infection is also linked to some types of lymphoma of the stomach. Even so, most people who carry this germ in their stomach never develop cancer.
- Epstein-Barr virus (EBV) infection. Epstein-Barr virus (EBV) causes infectious mononucleosis also called mono. Most people are infected with Epstein-Barr virus (EBV) at some time in their lives, usually as children or teens. Epstein-Barr virus (EBV) has been linked to nasopharyngeal cancer and to some forms of lymphoma. It is also found in the cancer cells of about 5% to 10% of people with stomach cancer, although it isn’t yet clear if the virus actually causes stomach cancer. Stomach cancers linked to Epstein-Barr virus (EBV) tend to be slower growing and have less of a tendency to spread.
- Swelling and irritation of the inside of the stomach, which is called gastritis
- Pernicious anemia. Pernicious anemia is an autoimmune condition where the body can’t absorb enough vitamin B12, leading to a deficiency and reduced red blood cell production. This occurs because the body doesn’t produce enough intrinsic factor (IF), a protein needed to absorb vitamin B12 from foods. People without enough intrinsic factor (IF) may end up with a vitamin B12 deficiency, which affects the body’s ability to make new red blood cells and can cause other problems as well. This condition, called pernicious anemia, can be caused by certain autoimmune conditions, as well as by some types of stomach surgery. Along with anemia (having too few red blood cells), people with this disease have an increased risk of stomach cancer. Symptoms can include fatigue, weakness, pale skin, and in severe cases, neurological problems.
- Certain cells in the stomach lining normally make a substance called intrinsic factor (IF) that the body needs to absorb vitamin B12 .
- Smoking. Smoking increases stomach cancer risk, particularly for cancers of the upper part of the stomach near the esophagus. The rate of stomach cancer is about doubled in people who smoke.
- Alcohol use. Alcohol use probably increases the risk of stomach cancer. The evidence for this link is strongest for people who have 3 or more drinks per day.
- Being overweight or obese. Being overweight or obese is linked with an increased risk of cancers of the cardia (the upper part of the stomach near the esophagus).
- Certain occupations. Workers in the coal, metal, and rubber industries seem to have a higher risk of getting stomach cancer.
- Growths of noncancerous cells in the stomach, called polyps. Polyps are non-cancerous growths on the lining of the stomach. Most types of polyps such as hyperplastic polyps or inflammatory polyps do not seem to increase a person’s risk of stomach cancer much, if at all. But adenomatous polyps also called adenomas can sometimes develop into cancer.
- Intestinal metaplasia (a condition in which the normal stomach lining is replaced with the cells that line the intestines).
- Previous stomach surgery. Stomach cancers are more likely to develop in people who have had part of their stomach removed to treat non-cancerous diseases such as ulcers. This might be because the stomach makes less acid, which allows more harmful bacteria to be present. Reflux (backup) of bile from the small intestine into the stomach after surgery might also add to the increased risk. These cancers typically develop many years after the surgery.
- Menetrier disease (hypertrophic gastropathy). In Menetrier disease (hypertrophic gastropathy) excess growth of the stomach’s inner lining causes large folds in the lining and leads to low levels of stomach acid. Because this disease is very rare, it is not known exactly how much this increases the risk of stomach cancer.
- Common variable immune deficiency (CVID). Common Variable Immunodeficiency (CVID) is a primary immunodeficiency disorder characterized by low levels of antibodies, increasing the risk of infections and as well as other problems, including atrophic gastritis and pernicious anemia. People with Common Variable Immunodeficiency (CVID) are more likely to get gastric lymphoma and stomach cancer. It affects both men and women, and symptoms can appear in childhood or adulthood
- Family history of stomach cancer. People with first-degree relatives (parents, siblings, or children) who have had stomach cancer are more likely to develop this disease, even without one of the inherited cancer syndromes described above. Still, most people who get stomach cancer do not have a family history of it.
- Family history of genetic syndromes that increase the risk of stomach cancer and other cancers. Some people inherit gene mutations (changes) from their parents that lead to conditions that can raise their risk of stomach cancer. These inherited syndromes account for only a small percentage of stomach cancers worldwide:
- Hereditary diffuse gastric cancer (HDGC) is a rare, inherited cancer syndrome characterized by a significantly increased risk of developing diffuse-type stomach cancer and, in women, lobular breast cancer. Hereditary diffuse gastric cancer (HDGC) is caused by mutations in the CDH1 gene, which is responsible for the cell adhesion protein E-cadherin. Hereditary diffuse gastric cancer (HDGC) is rare, but the lifetime stomach cancer risk among affected people is up to 70%. Women with this syndrome also have an increased risk of invasive lobular breast cancer.
- Lynch syndrome also known as hereditary non-polyposis colorectal cancer (HNPCC), is an inherited condition that significantly increases the risk of developing certain types of cancer, particularly colorectal and endometrial cancers. It’s caused by a gene mutation affecting DNA mismatch repair, which normally corrects errors in DNA replication.
- Juvenile polyposis syndrome is a genetic condition leading to multiple, non-cancerous growths (juvenile polyps) in the gastrointestinal tract. These polyps, which are hamartomas (abnormal tissue development), can occur in the stomach, small intestine, colon, and rectum. While most juvenile polyps are benign, there is an increased risk of developing gastrointestinal cancers, particularly colorectal cancer, in individuals with juvenile polyposis syndrome.
- Peutz-Jeghers syndrome is a rare inherited disorder characterized by distinctive freckle-like spots (hyperpigmented macules) on the skin and in the mouth, along with hamartomatous polyps in the gastrointestinal tract. The polyps in the stomach and intestines are called hamartomas. They can cause problems like bleeding or blockage of the intestines. These polyps, while benign, increase the risk of developing certain cancers including those of the stomach, small and large intestines, pancreas, breast, and ovary. Peutz-Jeghers syndrome is caused by mutations in the STK11 gene, which is a tumor suppressor gene. These mutations disrupt the normal function of the STK11 protein, leading to uncontrolled cell growth and the development of polyps and cancer.
- Familial Adenomatous Polyposis (FAP) is a rare inherited condition where many polyps (usually more than 100) form in the large intestine (colon and rectum), significantly increasing the risk of bowel cancer. People with Familial Adenomatous Polyposis (FAP) have a very high risk of getting colorectal cancer and a slightly increased risk of getting stomach cancer. It’s caused by a mutation in the APC gene.
- Gastric Adenocarcinoma and Proximal Polyposis of the Stomach (GAPPS) is a rare, inherited condition characterized by the development of numerous polyps in the proximal (upper) part of the stomach, significantly increasing the risk of gastric adenocarcinoma (a type of stomach cancer). These polyps, known as fundic gland polyps, are typically small and benign but can undergo dysplasia or transform into cancer. Gastric Adenocarcinoma and Proximal Polyposis of the Stomach (GAPPS) is caused by a mutation in the APC gene, which also causes familial adenomatous polyposis (FAP).
- Li-Fraumeni syndrome is a rare, inherited cancer predisposition syndrome caused by mutations in the TP53 gene, which is a tumor suppressor gene. People with Li-Fraumeni syndrome have a significantly higher lifetime risk of developing multiple cancers, including soft tissue sarcomas, osteosarcomas, breast cancer, brain tumors, adrenocortical carcinomas, and leukemia
- Being older. Stomach cancer can occur in younger people, but the risk goes up as a person gets older. Most people diagnosed with stomach cancer are in their 60s, 70s, or 80s.
- Male. Stomach cancer is more common in men than in women.
- Ethnicity. In the United States, stomach cancer is more common in Hispanic Americans, African Americans, Native Americans, Asian Americans, and Pacific Islanders than it is in non-Hispanic White people.
- Type A blood. Blood type groups refer to certain substances that are normally present on the surface of red blood cells and some other types of cells. These groups are important in matching blood for transfusions. For unknown reasons, people with type A blood have a higher risk of getting stomach cancer.
- Geography. Worldwide, stomach cancer is more common in East Asia, Eastern Europe, and South and Central America. Stomach cancer is less common in Africa and North America.
Having a mother, father, sister, or brother who has had stomach cancer. Only a small percentage of stomach cancers are caused by hereditary diffuse gastric cancer syndrome. But it is very important to recognize it, because most people who inherit this condition eventually get stomach cancer. A personal history of invasive lobular breast cancer before age 50 as well as having close family members who have had stomach cancer suggests that they might be at risk for having this syndrome. These people can talk to a genetics professional about getting genetic testing. If the testing shows the person has a mutation (abnormal change) in the CDH1 gene, many doctors will recommend they have their stomach removed before the cancer develops.
People at elevated risk for gastric cancer include elderly patients with atrophic gastritis or pernicious anemia, patients with sporadic gastric adenomas 15, familial adenomatous polyposis 46, or hereditary nonpolyposis colon cancer 47 and immigrant ethnic populations from countries with high rates of gastric carcinoma 48, 49. Workers in the rubber and coal industries are also at increased risk 50.
Risk factors for gastric cancer include the presence of precursor conditions such as chronic atrophic gastritis and intestinal metaplasia, pernicious anemia, and gastric adenomatous polyps. Genetic factors include a family history of gastric cancer, Li Fraumeni syndrome, and Type A blood type 50. Environmental factors include low consumption of fruits and vegetables; consumption of salted, smoked, or poorly preserved foods; cigarette smoking; and radiation exposure 51, 52, 50.
There is consistent evidence that Helicobacter pylori infection, also known as H. pylori infection, of the stomach is strongly associated with both the initiation and promotion of carcinoma of the gastric body and antrum and of gastric lymphoma 53, 13, 14. The International Agency for Research on Cancer classifies Helicobacter pylori infection as a cause of noncardia gastric carcinoma and gastric low-grade B-cell mucosa-associated lymphoid tissue or MALT lymphoma (i.e., a Group 1 human carcinogen) 54, 55.
Compared with the general population, people with duodenal ulcer disease may have a lower risk of gastric cancer 56.
Stomach cancer prevention
Cancer prevention is action taken to lower the chance of getting cancer. By preventing cancer, the number of new cases of cancer in a group or population is lowered. Hopefully, this will lower the number of deaths caused by cancer.
To prevent new cancers from starting, scientists look at risk factors and protective factors. Anything that increases your chance of developing cancer is called a cancer risk factor; anything that decreases your chance of developing cancer is called a cancer protective factor.
Some risk factors for cancer can be avoided, but many cannot. For example, both smoking and inheriting certain genes are risk factors for some types of cancer, but only smoking can be avoided. Regular exercise and a healthy diet may be protective factors for some types of cancer. Avoiding risk factors and increasing protective factors may lower your risk but it does not mean that you will not get cancer.
Different ways to prevent cancer are being studied, including:
- Changing lifestyle or eating habits.
- Avoiding things known to cause cancer.
- Taking medicines to treat a precancerous condition or to keep cancer from starting.
To lower your risk of stomach cancer, you can:
- Eat plenty of fruits and vegetables. Try to include fruits and vegetables in your diet each day. Choose a variety of colorful fruits and vegetables.
- Reduce the amount of salty and smoked foods you eat. Protect your stomach by limiting these foods.
- Stop smoking. If you smoke, quit. If you don’t smoke, don’t start. Smoking increases your risk of stomach cancer and many other types of cancer. Quitting smoking can be very hard, so ask your doctor for help.
- Tell your doctor if stomach cancer runs in your family. People with a strong family history of stomach cancer might have stomach cancer screening. Screening tests can detect stomach cancer before it causes symptoms.
- Hereditary diffuse gastric cancer (HDGC) is a rare inherited condition in which people have a greatly increased risk of stomach cancer, which often develops at a fairly early age. Hereditary diffuse gastric cancer (HDGC) is most often caused by an inherited mutation in the CDH1 gene. It’s very important to recognize people and families with this inherited syndrome, because most people who have it will develop stomach cancer. Families with hereditary diffuse gastric cancer (HDGC) typically have two or more close relatives who develop stomach cancer (usually the diffuse type), and/or at least one person who is diagnosed before age 50. Some family members might also develop invasive lobular breast cancer. Doctors often refer people who might have hereditary diffuse gastric cancer (HDGC) to a genetics professional, so they can discuss possibly getting genetic testing. If testing is done and shows a person has a mutation (abnormal change) in the CDH1 gene, doctors often recommend they consider having their stomach removed (typically between the ages of 20 and 30) before cancer develops. However, this operation called a total gastrectomy can lead to long-term changes in the way a person eats.
- Some other hereditary cancer syndromes are also linked with an increased risk for stomach cancer, including Lynch syndrome, familial adenomatous polyposis (FAP), Li-Fraumeni syndrome, and Peutz-Jeghers syndrome. The risk of stomach cancer with these syndromes is not nearly as high as it is with hereditary diffuse gastric cancer (HDGC), so removal of the stomach (total gastrectomy) is not typically recommended for people who have these syndromes. However, doctors might recommend getting regular tests to try to find stomach cancer early in some of these people.
Smoking cessation
Based on solid evidence, smoking is associated with an increased risk of stomach cancer 57, 58, 59. Tobacco use can increase the risk of cancers of the proximal stomach, the portion of the stomach closest to the esophagus 60. Tobacco use also increases the risk for many other types of cancer and is responsible for about one-third of all cancer deaths in the United States.
The 2004 Surgeon General’s report identifies cigarette smoking as a cause of stomach cancer, with an average relative risk (RR) in former smokers of 1.2 and in current smokers of 1.6 61. Compared with persistent smokers, the risk of stomach cancer decreases among former smokers with time since cessation. This pattern of observations makes it reasonable to infer that cigarette smoking prevention or cessation would result in a decreased risk of gastric cancer.
Magnitude of Effect: A systematic review and meta-analysis showed a 60% increase in gastric cancer in male smokers and a 20% increase in gastric cancer in female smokers compared with nonsmokers 57.
H. Pylori infection eradication
Based on solid evidence, H. pylori infection is associated with an increased risk of gastric cancer. A meta-analysis of seven randomized studies, all conducted in areas of high-risk gastric cancer and all but one conducted in Asia, suggests that treatment of H. pylori may reduce stomach cancer risk (from 1.7% to 1.1% a 65% reduction in cancer rsik) 62. Only two studies assessed gastric cancer incidence as the primary study outcome, and two different studies were double blinded. It is unclear how generalizable the results may be to the North American population.
In the initial report from a clinical trial, 3,365 randomized subjects were followed in an intention-to-treat analysis; it was shown that short-term treatment with amoxicillin and omeprazole reduced the incidence of gastric cancer by 39% during a period of 15 years following randomization, with similar but not statistically significant reductions for gastric cancer mortality 63.
Magnitude of Effect: Risk of cancer may be reduced; effect on cancer mortality is not known.
If your doctor thinks you might have H. pylori infection, there are several ways to test for this:
- The simplest way is a blood test that looks for antibodies to H. pylori. Antibodies are proteins the body’s immune system makes in response to an infection. A positive H pylori antibody test result can mean either that you are infected with H pylori or that you had an infection in the past that is now cleared.
- Another approach is to have an endoscopy procedure to take a biopsy sample of the stomach lining. This sample can be used for chemical tests for this kind of bacteria. Doctors can also identify H. pylori in biopsy samples viewed under a microscope. The biopsy sample can also be cultured (placed in a substance that promotes bacterial growth) to see if H. pylori grows out of the sample.
- There is also a special breath test for the bacteria. For this test, you drink a liquid containing urea. If H. pylori is present, it will chemically change the urea. A sample of your breath is then tested for these chemical changes.
Interventions With Inadequate Evidence as to Whether They Reduce the Risk of Stomach Cancer
Diet
The dramatic decline of stomach cancer in the past several decades is thought to be a result of people reducing many of the known dietary risk factors. This includes greater use of refrigeration for food storage rather than preserving foods by salting, pickling, and smoking. To help reduce your risk, avoid a diet that is high in smoked and pickled foods and salted meats and fish.
A diet high in fresh fruits and vegetables can also lower stomach cancer risk. Citrus fruits (such as oranges, lemons, and grapefruit) may be especially helpful, but grapefruit and grapefruit juice can change the blood levels of certain drugs you take, so it’s important to discuss this with your health care team before adding grapefruit to your diet.
Although some small studies suggested that drinking tea, particularly green tea, may help protect against stomach cancer, most large studies have not found such a link.
Being overweight or obese may add to the risk of stomach cancer. On the other hand, being physically active may help lower your risk.
Based on fair evidence, excessive salt intake and deficient dietary consumption of fresh fruits and vegetables are associated with an increased risk of gastric cancer. Dietary intake of vitamin C contained in vegetables, fruits, and other foods of plant origin is associated with a reduced risk of gastric cancer. Diets high in whole-grain cereals, carotenoids, allium compounds, and green tea are also associated with a reduced risk of this cancer. However, it is uncertain if changing one’s diet to include more vegetables, fruits, and whole grains would reduce the risk of gastric cancer.
Epidemiologic evidence from case-control and cohort studies suggests that increased intake of fresh fruits and vegetables is associated with decreased gastric cancer rates 64, 50.
The American Cancer Society 65 recommends that people eat a healthy diet, with an emphasis on plant foods. This includes eating at least 2½ cups of vegetables and fruits every day. Choosing whole-grain breads, pastas, and cereals instead of refined grains, and eating fish, poultry, or beans instead of processed meat and red meat may also help lower your risk of cancer. However, no randomized clinical trials have been done to establish a causal association.
Dietary supplements
Because of the evidence for an inverse association between gastric cancer and dietary intake of fruits and vegetables, especially those rich in antioxidants, there has been interest in dietary supplementation with antioxidants.
Dietary indices of micronutrient intake have been calculated and indicate possible protective effects of beta carotene, vitamin A, vitamin E, selenium, vitamin C or foods that contain these compounds. A chemoprevention trial in China reported a statistically significant reduction in the gastric cancer mortality rate after supplementation with beta carotene, vitamin E, and selenium 66. The population studied, however, may have been nutritionally deficient, raising questions of generalizability to other populations such as that of the United States. In addition, the experimental design did not permit assessment of the relative effects of beta carotene, vitamin E, and selenium.
Likewise, there was a randomized placebo-controlled trial of 200 mg of oral allitridium (a component of garlic) every day combined with 100 mcg of oral selenium every other day for 1 month of each year over a 3-year period in Qixia County (Shandong Province, China), an area with low intake of garlic and low selenium content in their garlic compared with other areas of China 67. Although designed as a double-blinded trial, allitridium causes a distinctive odor of garlic. A total of 5,033 people, who met at least one of the following criteria: (1) medical history of stomach disorder, (2) family history of tumor, (3) history of smoking, or (4) history of alcohol consumption, were randomly assigned. The study, published in a Chinese medical journal, was not well described. After a follow-up for as many as 11 years, there were a total of 23 gastric cancer cases in the allitridium/selenium group and 30 cases in the placebo group. Only 60% of the gastric cancers were diagnosed by histopathology. There was a qualitative difference in outcome by sex: relative risk men = 0.36; relative risk women = 1.14. Given the problems with design and reporting of the study, the evidence of benefit (including men) is weak and may not be generalizable to Western countries.
In a randomized, double-blind, chemoprevention trial in Venezuela among a population at increased risk for gastric cancer, a combination of antioxidant vitamins (vitamins C, E, and beta carotene) failed to modify progression or regression of precancerous gastric lesions 68. Another potential explanation for the lack of benefit of vitamin supplementation in this trial was the high prevalence of advanced premalignant lesions and the high H. pylori infection rate 69.
A secondary analysis of the Alpha-Tocopherol Beta Carotene trial conducted on male smokers in Finland evaluated the effect of supplementation on gastric cancer incidence 70. No protective effects for these supplements against gastric cancer were observed. Six-year follow-up results of a study of 976 Colombian patients have been reported. Patients were randomly assigned to receive eight different treatments that included vitamin supplements and anti-Helicobacter therapy either alone or in combination versus placebo. Among the 79 patients who received anti-Helicobacter therapy, a borderline statistically significant regression of intestinal metaplasia when compared with a placebo was noted. However, the combinations of antibiotics and vitamins did not confer additional benefits. More importantly, the progression rate of intestinal metaplasia was comparable irrespective of the treatments received. The progression rate was 23% in the placebo group and 17% in antibiotic recipients 71.
A 2008 Cochrane review examined randomized trials of antioxidant dietary supplements for the prevention of gastrointestinal cancers, including gastric cancer 72. Twenty trials were identified that assessed the preventive effects of antioxidant supplements or vitamin C on gastrointestinal cancer. With regard to gastric cancer, there were 12 comparisons of one or more micronutrients with placebo: beta-carotene alone (4 trials); vitamin C alone (1 trial); vitamin E alone (1 trial); vitamin A plus beta-carotene (1 trial); beta-carotene plus vitamin C (1 trial); beta-carotene plus vitamin E (1 trial); beta-carotene plus vitamins C and E (1 trial); selenium plus vitamins C and E (1 trial); and beta-carotene, vitamins C and E, and selenium (1 trial). None of the comparisons showed a statistically significant effect on the incidence of gastric cancer. The overall summary estimate across all trials of antioxidants showed no statistically significant effect. Approximately 0.51% of participants in the combined antioxidant groups developed gastric cancer versus 0.38% in the placebo groups after treatment of 2.1 to 12 years and follow-up for as many as 14.1 years. In the combined analysis of all 20 trials of antioxidants for the prevention of gastrointestinal cancers, a fixed effects model showed an increase in overall mortality of antioxidants compared with a placebo, but not in a random effects model 73.
Stomach cancer symptoms
Stomach cancer has few or no symptoms in the early stages, making early detection difficult. When they happen, symptoms might include indigestion and pain in the upper part of the belly. Symptoms might not happen until the cancer is advanced. Later stages of stomach cancer might cause symptoms such as feeling very tired, losing weight without trying, vomiting blood and having black stools.
These and other signs and symptoms may be caused by gastric cancer or by other conditions.
In the early stages of gastric cancer, the following symptoms may occur:
- Indigestion and stomach discomfort.
- A bloated feeling after eating.
- Mild nausea.
- Loss of appetite.
- Heartburn or Dyspepsia (pain or discomfort in the upper abdomen).
However, these are also symptoms of common conditions affecting the stomach like acid gatroesophageal reflux (GERD) or gastritis. They may also occur with other types of cancer.
In more advanced stages of gastric cancer, the following signs and symptoms may occur:
- Blood in the stool.
- Low red blood cell count (anemia).
- Vomiting.
- Weight loss for no known reason.
- Stomach pain.
- A sense of fullness in the upper abdomen after eating a small meal.
- Jaundice (yellowing of eyes and skin).
- Ascites (build-up of fluid in the abdomen).
- Trouble swallowing.
Check with your doctor if you have any of these problems.
Stomach cancer that spreads to other parts of the body is called metastatic stomach cancer. It causes symptoms specific to where it spreads. For example, when cancer spreads to the lymph nodes it might cause lumps you can feel through the skin. Cancer that spreads to the liver might cause yellowing of the skin and whites of the eyes. If cancer spreads within the belly, it might cause fluid to fill the belly. The belly might look swollen.
The main reason why stomach cancer is often discovered late is because many, even doctors, may not immediately suspect stomach cancer. Less common symptoms of stomach cancer, which tend to present in the more advanced stages, include black stools (a sign of bleeding in stomach).
If you have signs and symptoms that worry you, make an appointment with your doctor. Many conditions can cause symptoms that are like the ones caused by stomach cancer. Your doctor might test for those other causes first before testing for stomach cancer.
Stomach cancer diagnosis
Your doctor will review your medical history, ask about your symptoms and perform a physical exam that may involve feeling for a mass in your stomach. Your doctor may order several tests to examine your stomach and esophagus to detect (find), diagnose and stage gastric cancer.
The following tests and procedures may be used:
- Physical exam and history : An exam of the body to check general signs of health, including checking for signs of disease, such as lumps or anything else that seems unusual. A history of the patient’s health habits and past illnesses and treatments will also be taken.
- Blood chemistry studies : A procedure in which a blood sample is checked to measure the amounts of certain substances released into the blood by organs and tissues in the body. An unusual (higher or lower than normal) amount of a substance can be a sign of disease.
- CEA (carcinoembryonic antigen) assay: Tests that measure the level of CEA in the blood. This substance is released into the bloodstream from both cancer cells and normal cells. When found in higher than normal amounts, it can be a sign of gastric cancer or other conditions.
- Complete blood count (CBC): A procedure in which a sample of blood is drawn and checked for the following:
- The number of red blood cells, white blood cells, and platelets.
- The amount of hemoglobin (the protein that carries oxygen) in the red blood cells.
- The portion of the sample made up of red blood cells.
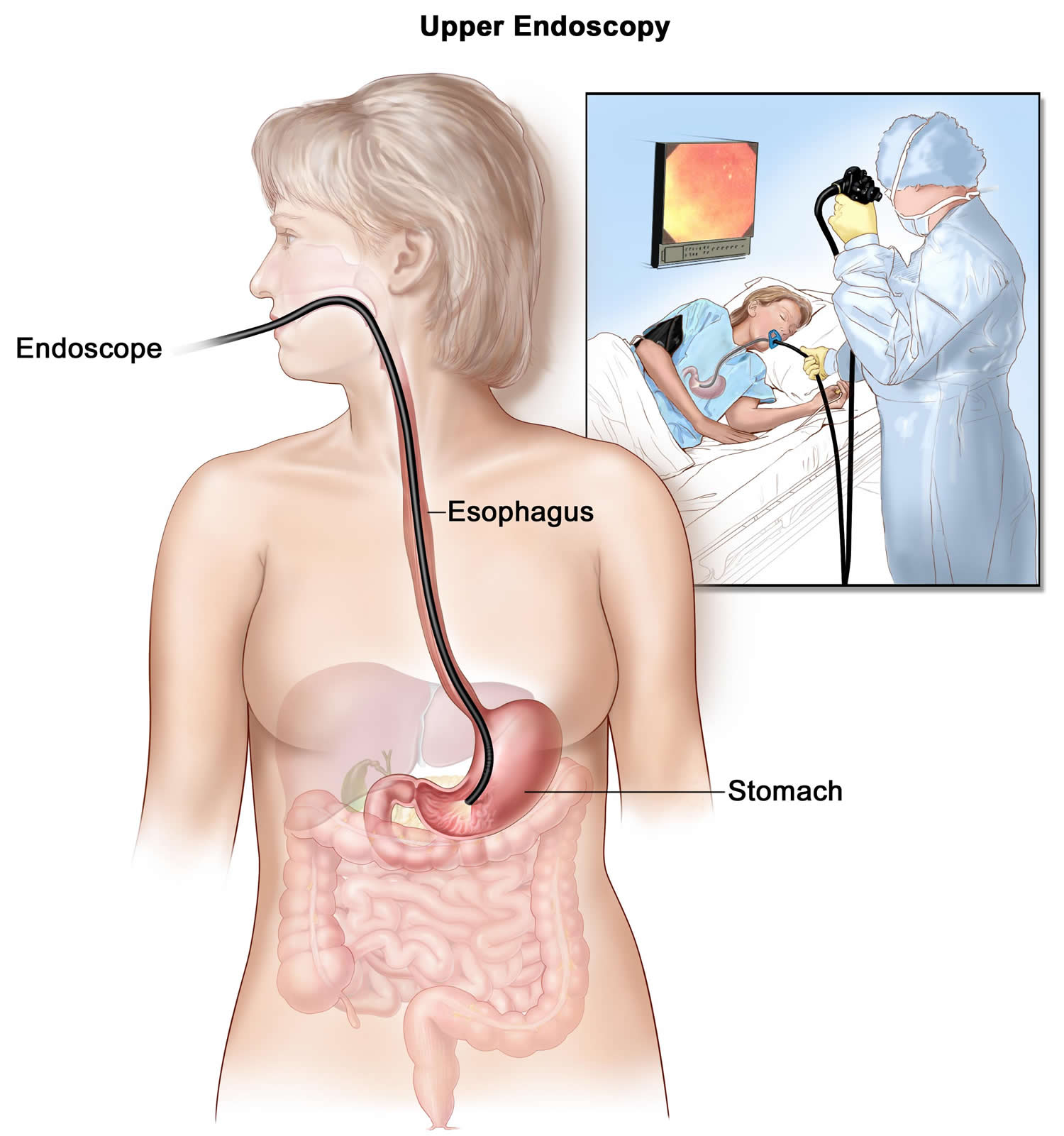
- Upper endoscopy : A procedure to look inside the esophagus, stomach, and duodenum (first part of the small intestine) to check for abnormal areas. An endoscope (a thin, lighted tube) is passed through the mouth and down the throat into the esophagus, stomach, and first part of the small intestine.
- Endoscopic ultrasound (EUS): A procedure in which an endoscope is inserted into the body, usually through the mouth or rectum. An endoscope is a thin, tube-like instrument with a light and a lens for viewing. A probe at the end of the endoscope is used to bounce high-energy sound waves (ultrasound) off internal tissues or organs and make echoes. The echoes form a picture of body tissues called a sonogram. This procedure is also called endosonography.
- Barium swallow : A series of x-rays of the esophagus and stomach. The patient drinks a liquid that contains barium (a silver-white metallic compound). The liquid coats the esophagus and stomach, and x-rays are taken. This procedure is also called an upper GI series.
- CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
- PET scan (positron emission tomography scan): A procedure to find malignant tumor cells in the body. A small amount of radioactive glucose (sugar) is injected into a vein. The PET scanner rotates around the body and makes a picture of where glucose is being used in the body. Malignant tumor cells show up brighter in the picture because they are more active and take up more glucose than normal cells do. A PET scan and CT scan may be done at the same time. This is called a PET-CT.
- Biopsy : The removal of cells or tissues so they can be viewed under a microscope to check for signs of cancer. A biopsy of the stomach is usually done during the endoscopy. The sample of tissue may be checked to measure how many human epidermal growth factor receptor 2 (HER2) genes there are and how much human epidermal growth factor receptor 2 (HER2) protein is being made. If there are more human epidermal growth factor receptor 2 (HER2) genes or higher levels of human epidermal growth factor receptor 2 (HER2) protein than normal, the cancer is called human epidermal growth factor receptor 2 (HER2) positive. human epidermal growth factor receptor 2 (HER2)-positive gastric cancer may be treated with a monoclonal antibody that targets the human epidermal growth factor receptor 2 (HER2) protein.
Upper endoscopy
Upper endoscopy also called esophagogastroduodenoscopy (EGD) is the test most often done if the doctor thinks you might have stomach cancer. During upper endoscopy, your doctor passes an endoscope, which is a thin, flexible, lighted tube with a small video camera on the end, down your throat. This lets your doctor see the inner lining of your esophagus, stomach, and first part of the small intestine. If abnormal areas are seen, biopsy samples can be removed using instruments passed through the endoscope. The tissue samples are sent to a lab, where they are looked at with a microscope to see if they contain cancer.
Unfortunately, some types of stomach cancers can be hard to see during an endoscopy.
Endoscopy can also be used as part of a special imaging test known as endoscopic ultrasound (EUS).
In some situations, endoscopy can be used to help remove very early stage cancers. It can also be used to help prevent or relieve symptoms or other complications from stomach cancer, without the need for more extensive surgery.
You will most likely be given medicine to make you sleepy (sedation) before the endoscopy.
Figure 5. Upper endoscopy
Endoscopic ultrasound
Endoscopic ultrasound (EUS) is often used to see how far a cancer might have spread into the wall of the stomach, or into nearby areas or nearby lymph nodes. For this test, a small ultrasound probe is placed on the tip of an endoscope. While you are sedated, the endoscope is passed down your throat and into the stomach. The probe is put up against the wall of the stomach where the cancer is. It gives off sound waves and detects the echoes as they bounce back, which are then converted into images. Doctors can use these images to look at the layers of the stomach wall, as well as the nearby lymph nodes and other structures just outside the stomach.
Endoscopic ultrasound (EUS) can also be used to help guide a needle into a suspicious area to get a biopsy sample known as an EUS-guided needle biopsy.
Biopsy
Your doctor may suspect cancer if an abnormal-looking area is seen on endoscopy or an imaging test, but the only way to tell for sure if it’s cancer is by doing a biopsy. During a biopsy, the doctor removes small pieces (samples) of the abnormal area. Biopsies to check for stomach cancer are most often done during an upper endoscopy. If the doctor sees any abnormal areas in the stomach lining during the endoscopy, instruments can be passed down the endoscope to biopsy them.
Some stomach cancers can start deep within the stomach wall, which can make them hard to biopsy with standard endoscopy. If the doctor suspects cancer might be deeper in the stomach wall, endoscopic ultrasound (EUS) can be used to guide a thin, hollow needle into the wall of the stomach to get a biopsy sample.
Biopsies may also be taken from areas of possible cancer spread, such as nearby lymph nodes or suspicious areas in other parts of the body.
Testing biopsy samples
Biopsy samples are sent to a lab to be looked at under a microscope. The samples are checked to see if they contain cancer, and if they do, what kind it is. For example, intestinal or diffuse adenocarcinoma, carcinoid tumor, gastrointestinal stromal tumor (GIST), or lymphoma.
If stomach cancer is found, more lab tests may be done on the biopsy samples to learn more about the cancer cells. This might affect how the cancer is treated.
HER2 testing: The cancer cells may be tested to see if they have too much of a growth-promoting protein called HER2. Cancers with increased levels of HER2 are called HER2-positive. These cancers can be treated with drugs that target the HER2 protein.
The biopsy sample is usually tested for HER2 using either immunohistochemistry (IHC) or fluorescent in situ hybridization (FISH). Often the IHC test is used first, which gives results on a scale from 0 to 3+.
- If the results are 0 or 1+, the cancer is HER2-negative, so drugs targeting HER2 aren’t likely to be helpful.
- If the test comes back 3+, the cancer is HER2-positive, so treatment with drugs targeting HER2 could be an option.
- When the result is 2+, the HER2 status of the cancer is not clear, so it needs to be tested with FISH to clarify the result.
Testing for other gene or protein changes: The cancer cells may also be tested for other gene or protein changes that might affect treatment. For example:
- If the cells have a certain amount of an immune checkpoint protein called PD-L1, treatment with an immune checkpoint inhibitor such as pembrolizumab (Keytruda) might be an option.
- If the cells have high levels of microsatellite instability (MSI-H) or a defect in a mismatch repair gene (dMMR), treatment with an immune checkpoint inhibitor might be an option.
- If the cells have a high tumor mutational burden (TMB-H), meaning they have many gene mutations, treatment with an immune checkpoint inhibitor might be an option.
- If the cells have changes in one of the NTRK genes, certain targeted drugs might be an option for treatment.
Imaging tests
Imaging tests use x-rays, magnetic fields, sound waves, or radioactive substances to create pictures of the inside of your body. Imaging tests may be done for a number of reasons, including:
- To help find out if a suspicious area might be cancer
- To learn how far cancer may have spread
- To help determine if treatment has been effective
Upper gastrointestinal (GI) series
Upper gastrointestinal (GI) series is an x-ray test to look at the inner lining of the esophagus, stomach, and first part of the small intestine. Upper gastrointestinal (GI) series is used less often than upper endoscopy to look for stomach cancer or other stomach problems, as it can miss some abnormal areas, and it doesn’t allow the doctor to take biopsy samples. But it is less invasive than endoscopy, and it might be useful in some situations.
For upper gastrointestinal (GI) series, you drink a white chalky solution containing a substance called barium. The barium coats the inner lining of the esophagus, stomach, and small intestine. Air might be pumped into the stomach through a thin tube at this time as well. Several x-ray pictures are then taken. Because x-rays can’t pass through the coating of barium, this outline any abnormal areas in the lining of these organs.
Computed tomography (CT or CAT) scan
A CT scan uses x-rays to make detailed, cross-sectional images of the soft tissues in the body.
CT scans can show the stomach fairly clearly and often can confirm the location of a cancer. CT scans can also show other parts of the body to which stomach cancer might have spread, such as the liver and nearby lymph nodes. This can help determine the extent (stage) of the cancer and if surgery may be a good treatment option.
CT-guided needle biopsy: CT scans can also be used to guide a biopsy needle into a suspected area of cancer spread. For this test, you will lie on the CT scanning table while the doctor moves a biopsy needle through the skin toward the mass. CT scans are repeated until the needle is within the mass. A biopsy sample is then removed and sent to a lab for testing.
Positron emission tomography (PET) scan
A positron emission tomography (PET) scan can be useful to help determine the extent of the cancer in the body. For this test, you are injected with a slightly radioactive form of sugar, which collects mainly in cancer cells. A special camera is then used to create a picture of areas of radioactivity in the body. The picture is not detailed like a CT or MRI scan, but a PET scan can look for possible areas of cancer spread in all areas of the body at once.
Many newer machines can do both a PET and CT scan at the same time (PET/CT scan). This lets the doctor see areas that “light up” on the PET scan in more detail.
Although PET scans can be useful for finding areas of cancer spread, they aren’t always helpful in certain kinds of stomach cancer because some types don’t take up much of the radioactive sugar.
Magnetic resonance imaging (MRI)
Like a CT scan, an MRI can show detailed images of soft tissues in the body. But MRIs use radio waves and strong magnets instead of x-rays.
This test is not used as often as CT scans to look for stomach cancer, but it may be helpful in certain situations, such as when looking for tumors in the liver.
Chest x-ray
Chest x-ray can help show if the cancer has spread to the lungs. It might also be used to help determine if a person has any serious lung or heart diseases, which might affect whether surgery would be a treatment option. A chest x-ray isn’t needed if a CT scan of the chest has been done.
Laparoscopy
If stomach cancer has already been found, and imaging tests such as CT or PET scans have not shown it has spread to other parts of the body, doctors might do a laparoscopy before any other surgery. This can help confirm the cancer is still only in the stomach, which means surgery to remove it might still be an option.
This procedure is done in an operating room while you are under general anesthesia (in a deep sleep). A laparoscope (a thin, flexible tube with a small video camera on the end) is inserted through a small cut in the belly. This lets the doctor look closely at the surfaces of the organs and nearby lymph nodes inside the abdomen, or even remove small samples of tissue, which can then be tested for cancer.
If it doesn’t look like the cancer has spread, sometimes the doctor will “wash” the abdomen with saline (saltwater). This is called peritoneal washing. The fluid is then collected and checked for cancer cells.
Sometimes laparoscopy is combined with ultrasound to give a better picture of the cancer.
Tests of organ function
If cancer is found, the doctor might recommend certain lab tests, especially if surgery might be an option. For instance, blood tests will be done to make sure your liver and kidneys are working normally and that your blood clots normally.
If surgery is planned or you are going to get medicines that can affect the heart, you may also have an electrocardiogram (ECG) and/or an echocardiogram (an ultrasound of the heart) to make sure your heart is functioning well.
Stomach Cancer Stages
The stage of a cancer is a description of how far the cancer has spread. Cancer stage at diagnosis, which refers to extent of a cancer in the body, determines treatment options and has a strong influence on the length of survival. In general, if the cancer is found only in the part of the body where it started it is localized (sometimes referred to as stage 1). If it has spread to a different part of the body, the stage is regional or distant. The earlier stomach cancer is caught, the better chance a person has of surviving five years after being diagnosed. For stomach cancer, 31% are diagnosed at the local stage 4. The 5-year survival for localized stomach cancer is 76.5% 4.
There are actually 2 types of stages for stomach cancer:
- The clinical stage of the cancer is the doctor’s best estimate of the extent of the cancer, based on the results of physical exams, endoscopy, biopsies, and any imaging tests (such as CT scans) that have been done.
- If surgery is done, the pathologic stage can be determined using the same test results used for the clinical stage, plus what is found from tissues removed during surgery.
The clinical stage is used to help plan treatment. Sometimes, though, the cancer has spread further than the clinical stage estimates. Because the pathologic stage is based on what was found at surgery, it can more accurately predict the patient’s outlook. The staging described here is the pathologic stage.
There are three ways that cancer spreads in the body
Cancer can spread through tissue, the lymph system, and the blood:
- Tissue. The cancer spreads from where it began by growing into nearby areas.
- Lymph system. The cancer spreads from where it began by getting into the lymph system. The cancer travels through the lymph vessels to other parts of the body.
- Blood. The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body.
Cancer may spread from where it began to other parts of the body.
When cancer spreads to another part of the body, it is called metastasis. Cancer cells break away from where they began (the primary tumor) and travel through the lymph system or blood.
- Lymph system. The cancer gets into the lymph system, travels through the lymph vessels, and forms a tumor (metastatic tumor) in another part of the body.
- Blood. The cancer gets into the blood, travels through the blood vessels, and forms a tumor (metastatic tumor) in another part of the body.
The metastatic tumor is the same type of cancer as the primary tumor.
For example, if gastric cancer spreads to the liver, the cancer cells in the liver are actually gastric cancer cells. The disease is metastatic gastric cancer, not liver cancer.
A staging system is a way for members of the cancer care team to describe the extent of a cancer’s spread. The system most often used to stage stomach cancer in the United States is the American Joint Commission on Cancer (AJCC) TNM classification system 74. The TNM classification system for staging contains 3 key pieces of information:
- T describes the size of the original (primary) tumor and whether it has invaded nearby tissue (how far it has grown into the wall of the stomach and into nearby organs). The 5 layers of the stomach wall include:
- Mucosa: the innermost layer, where nearly all stomach cancers start. The mucosa has 3 parts: epithelial cells, a layer of connective tissue (the lamina propria), and a thin layer of muscle (the muscularis mucosa).
- Submucosa: a supporting layer under the mucosa
- Muscularis propria: a thick layer of muscle that moves and mixes the stomach contents
- Subserosa
- Serosa: the outer, wrapping layer of the stomach
- N describes the spread to nearby (regional) lymph nodes.
- M indicates whether the cancer has metastasized (spread) to distant parts of the body. The most common sites of distant spread of stomach cancer are the liver, the peritoneum (the lining of the space around the digestive organs), and distant lymph nodes. Less common sites of spread include the lungs and brain.
Numbers or letters appear after T, N, and M to provide more details about each of these factors:
- The numbers 0 through 4 indicate increasing severity.
- The letter X means “cannot be assessed” because the information is not available.
- The letters “is” refer to carcinoma in situ, which means the tumor is only in the top layer of mucosa cells and has not yet invaded deeper layers of tissue.
Once a person’s T, N, and M categories have been determined, this information is combined in a process called stage grouping to assign an overall stage. The earliest stage stomach cancers are called stage 0 (carcinoma in situ), and then range from stages I (1) through IV (4). The lower the number, the less the cancer has spread. See the table below for more details about the stage grouping for stomach cancer.
The American Joint Commission on Cancer (AJCC) TNM classification system is for staging all stomach cancers except those starting in either the gastroesophageal junction (where the stomach and the esophagus meet) or in the cardia (the first part of the stomach) and growing into the gastroesophageal junction. Those cancers are staged (and often treated) like cancers of the esophagus.
The AJCC staging system provides a detailed summary of how far a stomach cancer has spread. But for treatment purposes, doctors are often more concerned about whether the tumor can be removed (resected) with surgery.
- Resectable cancers are those the doctor believes can be completely removed during surgery.
- Unresectable cancers can’t be removed completely. This might be because the tumor has grown too far into nearby organs or lymph nodes, it has grown too close to major blood vessels, it has spread to distant parts of the body, or the person is not healthy enough for surgery.
There is no distinct dividing line between resectable and unresectable in terms of the TNM stage of the cancer, but earlier stage cancers are more likely to be resectable.
Stomach cancer staging can be complex, so ask your doctor to explain it to you in a way you understand.
Figure 6. Stomach cancer stages
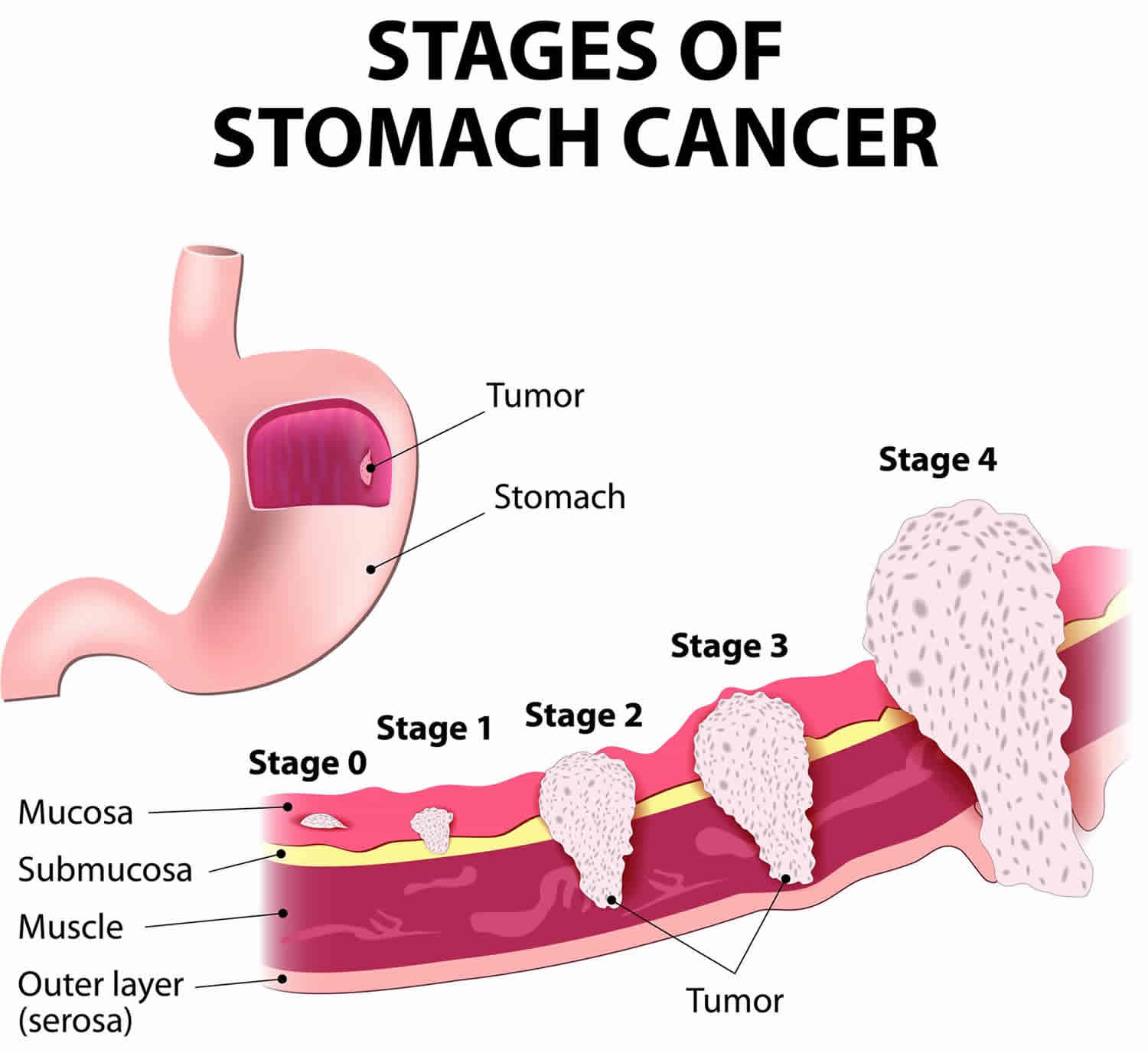
Table 1. Stomach Cancer TNM stage
| AJCC Stage | Stage grouping | Stage description* |
|---|---|---|
| 0 | Tis N0 M0 | There is high grade dysplasia (very abnormal looking cells) in the stomach lining, OR there are cancer cells only in the top layer of cells of the mucosa (innermost layer of the stomach) that have not grown into deeper layers of tissue such as the lamina propria (Tis). The cancer has not spread to nearby lymph nodes (N0) or distant parts of the body (M0). This stage is also known as carcinoma in situ. |
| 1A | T1 N0 M0 | The main tumor has grown from the top layer of cells of the mucosa into the next layers below such as the lamina propria, the muscularis mucosa, or submucosa (T1). The cancer has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0). |
| 1B | T1 N1 M0 | The main tumor has grown from the top layer of cells of the mucosa into the next layers below such as the lamina propria, the muscularis mucosa, or submucosa (T1), AND the cancer has spread to 1 to 2 nearby lymph nodes (N1). The cancer has not spread to distant parts of the body (M0). |
| OR | ||
| T2 N0 M0 | The main tumor is growing into the muscularis propria layer (T2). The cancer has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0). | |
| 2A | T1 N2 M0 | The main tumor has grown from the top layer of cells of the mucosa into the next layers below such as the lamina propria, the muscularis mucosa, or submucosa (T1), AND the cancer has spread to 3 to 6 nearby lymph nodes (N2). The cancer has not spread to distant parts of the body (M0). |
| OR | ||
| T2 N1 M0 | The main tumor is growing into the muscularis propria layer (T2), AND the cancer has spread to 1 to 2 nearby lymph nodes (N1). The cancer has not spread to distant parts of the body (M0). | |
| OR | ||
| T3 N0 M0 | The main tumor is growing into the subserosa layer (T3). The cancer has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0). | |
| 2B | T1 N3a M0 | The main tumor has grown from the top layer of cells of the mucosa into the next layers below such as the lamina propria, the muscularis mucosa, or submucosa (T1), AND the cancer has spread to 7 to 15 nearby lymph nodes (N3a). The cancer has not spread to distant parts of the body (M0). |
| OR | ||
| T2 N2 M0 | The main tumor is growing into the muscularis propria layer (T2), AND the cancer has spread to 3 to 6 nearby lymph nodes (N2). The cancer has not spread to distant parts of the body (M0). | |
| T3 N1 M0 | The main tumor is growing into the subserosa layer (T3), AND the cancer has spread to 1 to 2 nearby lymph nodes (N1). The cancer has not spread to distant parts of the body (M0). | |
| OR | ||
| T4a N0 M0 | The main tumor has grown through the stomach wall into the serosa, but it hasn’t grown into any of the nearby organs or structures (T4a). The cancer has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0). | |
| 3A | T2 N3a M0 | The main tumor is growing into the muscularis propria layer (T2), AND the cancer has spread to 7 to 15 nearby lymph nodes (N3a). The cancer has not spread to distant parts of the body (M0). |
| OR | ||
| T3 N2 M0 | The main tumor is growing into the subserosa layer (T3), AND the cancer has spread to 3 to 6 nearby lymph nodes (N2). The cancer has not spread to distant parts of the body (M0). | |
| OR | ||
| T4a N1 M0 | The main tumor has grown through the stomach wall into the serosa, but it has not grown into any of the nearby organs or structures (T4a). The cancer has spread to 1 to 2 nearby lymph nodes (N1). The cancer has not spread to distant parts of the body (M0). | |
| OR | ||
| T4a N2 M0 | The main tumor has grown through the stomach wall into the serosa, but it has not grown into any of the nearby organs or structures (T4a). The cancer has spread to 3 to 6 nearby lymph nodes (N1). The cancer has not spread to distant parts of the body (M0). | |
| OR | ||
| T4b N0 M0 | The main tumor has grown through the stomach wall and into nearby organs or structures (T4b). The cancer has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0). | |
| 3B | T1 N3b M0 | The main tumor has grown from the top layer of cells of the mucosa into the next layers below such as the lamina propria, the muscularis mucosa, or submucosa (T1), AND the cancer has spread to 16 or more nearby lymph nodes (N3b). The cancer has not spread to distant parts of the body (M0). |
| OR | ||
| T2 N3b M0 | The main tumor is growing into the muscularis propria layer (T2), AND the cancer has spread to 16 or more nearby lymph nodes (N3b). The cancer has not spread to distant parts of the body (M0). | |
| OR | ||
| T3 N3a M0 | The main tumor is growing into the subserosa layer (T3), AND the cancer has spread to 7 to 15 nearby lymph nodes (N3a). The cancer has not spread to distant parts of the body (M0). | |
| OR | ||
| T4a N3a M0 | The main tumor has grown through the stomach wall into the serosa, but it has not grown into any of the nearby organs or structures (T4a), AND the cancer has spread to 7 to 15 nearby lymph nodes (N3a). The cancer has not spread to distant parts of the body (M0). | |
| OR | ||
| T4b N1 M0 | The main tumor has grown through the stomach wall and into nearby organs or structures (T4b). The cancer has spread to 1 to 2 nearby lymph nodes (N1). The cancer has not spread to distant parts of the body (M0). | |
| OR | ||
| T4b N2 M0 | The main tumor has grown through the stomach wall and into nearby organs or structures (T4b). The cancer has spread to 3 to 6 nearby lymph nodes (N1). The cancer has not spread to distant parts of the body (M0). | |
| 3C | T3 N3b M0 | The main tumor is growing into the subserosa layer (T3), AND the cancer has spread to 16 or more nearby lymph nodes (N3b). The cancer has not spread to distant parts of the body (M0). |
| OR | ||
| T4a N3b M0 | The main tumor has grown through the stomach wall into the serosa, but it has not grown into any of the nearby organs or structures (T4a), AND the cancer has spread to 16 or more nearby lymph nodes (N3b). The cancer has not spread to distant parts of the body (M0). | |
| OR | ||
| T4b N3a M0 | The main tumor has grown through the stomach wall and into nearby organs or structures (T4b), AND the cancer has spread to 7 to 15 nearby lymph nodes (N3a). The cancer has not spread to distant parts of the body (M0). | |
| OR | ||
| T4b N3b M0 | The main tumor has grown through the stomach wall and into nearby organs or structures (T4b), AND the cancer has spread to 16 or more nearby lymph nodes (N3b). The cancer has not spread to distant parts of the body (M0). | |
| 4 | Any T Any N M1 | The cancer might or might not have grown into any of the layers of the stomach wall (Any T), and it might or might not have spread to nearby lymph nodes (Any N). The cancer has spread to distant organs such as the liver, lungs, brain, or the peritoneum (the lining of the space around the digestive organs) (M1). |
Footnotes: *The following additional categories are not listed in the table above:
- TX: Main tumor cannot be assessed due to lack of information.
- T0: No evidence of a primary tumor.
- NX: Regional lymph nodes cannot be assessed due to lack of information.
Tumor (T) category of stomach cancer
Nearly all stomach cancers start in the innermost layer of the stomach wall (the mucosa). The Tumor (T) category describes how far through the stomach’s 5 layers the cancer has invaded.
There are 4 main stages of tumor size in stomach cancer 74:
- TX: Primary tumor cannot be assessed.
- T0: No evidence of primary tumor.
- Tis Carcinoma in situ: intraepithelial tumor without invasion of the lamina propria.
- T1 means the tumor has started to grow into the wall of the stomach (lamina propria, muscularis mucosae, or submucosa). It’s divided into T1a and T1b:
- T1a means the tumor is within the inner layers of the stomach (lamina propria or muscularis mucosae)
- T1b means the tumor has grown through the mucosa and into a layer of supportive tissue called the submucosa
- T2 means the tumor has grown into the muscle layer of the stomach (muscularis propria)
- T3 means the tumor has grown into the outer lining of the stomach. Tumor penetrates subserosal connective tissue without invasion of visceral peritoneum or adjacent structures.
- T4 means that the tumor has grown through the outer lining of the stomach. It’s divided into T4a and T4b:
- T4a means the tumor has broken through the outer lining of the stomach wall invading the serosa (visceral peritoneum)
- T4b means the tumor has grown through the stomach wall and into other organs or body structures nearby such as the liver, food pipe (esophagus) or abdominal wall.
Layers of the stomach
- The innermost layer is the mucosa. The mucosa has 3 parts: epithelial cells, which lie on top of a layer of connective tissue (the lamina propria), which is on top of a thin layer of muscle (the muscularis mucosa).
- Under the mucosa is a supporting layer called the submucosa.
- Below this is the muscularis propria, a thick layer of muscle that moves and mixes the stomach contents.
- The next 2 layers, the subserosa and the outermost serosa, act as wrapping layers for the stomach.
Figure 7. T stage stomach cancer
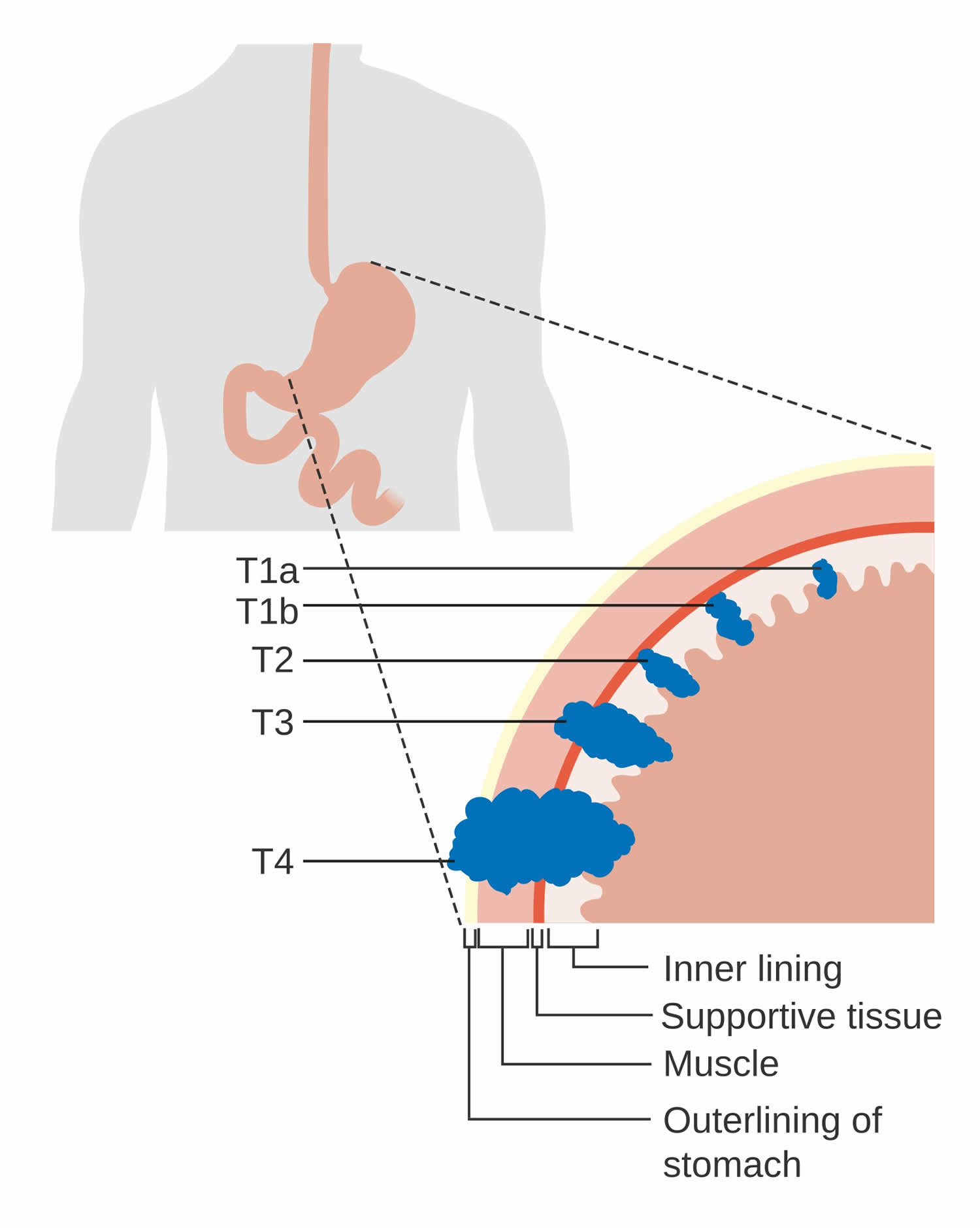
Node (N) category of stomach cancer
Node (N) describes whether the cancer has spread to the lymph nodes. Lymph nodes are a network of glands throughout the body, for example in your armpits, neck and groins. They drain away waste fluid, waste products and damaged cells, and contain cells that fight infection.
There are 4 possible stages describing whether cancer cells are in the lymph nodes – N0, N1, N2 and N3 74:
- NX Regional lymph node(s) cannot be assessed.
- N0 means there are no lymph nodes containing cancer cells
- N1 means there are cancer cells in 1 to 2 lymph nodes near to the stomach.
- N2 means there are cancer cells in 3 to 6 nearby lymph nodes.
- N3 means there are cancer cells in ≥7 regional lymph nodes. N3 is split into N3a and N3b:
- N3a means there are cancer cells in 7 to 15 nearby lymph nodes
- N3b means there are cancer cells in 16 or more nearby lymph nodes
Metastasis (M) category of stomach cancer
Metastasis describes whether the cancer has spread to a different part of the body.
There are 2 stages of metastasis 74:
- M0 means the cancer has not spread to other organs (no distant metastasis)
- M1 means the cancer has spread to other parts of the body (distant metastasis)
Metastases that have spread from the stomach are also called secondary stomach cancer.
The following stages are used for stomach cancer
Once the T, N, and M categories have been determined, this information is combined and expressed as a stage, using the number 0 (zero) and the Roman numerals I (1) through IV (4). This is known as stage grouping. Some stages are split into substages, indicated by letters.
Stage 0 (Carcinoma in Situ): Tis, N0, M0
In stage 0, abnormal cells are found in the inside lining of the mucosa (innermost layer) of the stomach wall. These abnormal cells may become cancer and spread into nearby normal tissue. Stage 0 is also called carcinoma in situ.
Stage 1 Stomach cancer
In stage 1 (I), cancer has formed in the inside lining of the mucosa (innermost layer) of the stomach wall. Stage I is divided into stage IA and stage IB, depending on where the cancer has spread.
- Stage 1A: Cancer may have spread into the submucosa (layer of tissue next to the mucosa) of the stomach wall.
- Stage 1B: Cancer: may have spread into the submucosa (layer of tissue next to the mucosa) of the stomach wall and is found in 1 or 2 lymph nodes near the tumor; or has spread to the muscle layer of the stomach wall.
Stage 2 Stomach cancer
Stage 2 (II) gastric cancer is divided into stage IIA and stage IIB, depending on where the cancer has spread.
Stage 2A: Cancer:
- has spread to the subserosa (layer of tissue next to the serosa) of the stomach wall; or
- has spread to the muscle layer of the stomach wall and is found in 1 or 2 lymph nodes near the tumor; or
- may have spread to the submucosa (layer of tissue next to the mucosa) of the stomach wall and is found in 3 to 6 lymph nodes near the tumor.
Stage 2B: Cancer:
- has spread to the serosa (outermost layer) of the stomach wall; or
- has spread to the subserosa (layer of tissue next to the serosa) of the stomach wall and is found in 1 or 2 lymph nodes near the tumor; or
- has spread to the muscle layer of the stomach wall and is found in 3 to 6 lymph nodes near the tumor; or
- may have spread to the submucosa (layer of tissue next to the mucosa) of the stomach wall and is found in 7 or more lymph nodes near the tumor.
Stage 3 Stomach cancer
Stage 3 (III) gastric cancer is divided into stage IIIA, stage IIIB, and stage IIIC, depending on where the cancer has spread.
Stage 3A: Cancer has spread to:
- the serosa (outermost) layer of the stomach wall and is found in 1 or 2 lymph nodes near the tumor; or
- the subserosa (layer of tissue next to the serosa) of the stomach wall and is found in 3 to 6 lymph nodes near the tumor; or
- the muscle layer of the stomach wall and is found in 7 or more lymph nodes near the tumor.
Stage 3B: Cancer has spread to:
- nearby organs such as the spleen, transverse colon, liver, diaphragm, pancreas, kidney, adrenal gland, or small intestine, and may be found in 1 or 2 lymph nodes near the tumor; or
- the serosa (outermost layer) of the stomach wall and is found in 3 to 6 lymph nodes near the tumor; or
- the subserosa (layer of tissue next to the serosa) of the stomach wall and is found in 7 or more lymph nodes near the tumor.
Stage 3C: Cancer has spread to:
- nearby organs such as the spleen, transverse colon, liver, diaphragm, pancreas, kidney, adrenal gland, or small intestine, and may be found in 3 or more lymph nodes near the tumor; or
- the serosa (outermost layer) of the stomach wall and is found in 7 or more lymph nodes near the tumor.
Stage 4 Stomach cancer
In stage 4 (IV), cancer has spread to distant parts of the body.
There are 2 stages of metastasis 74:
- M0 means the cancer has not spread to other organs (no distant metastasis)
- M1 means the cancer has spread to other parts of the body (distant metastasis)
Recurrent Gastric Cancer
Recurrent gastric cancer is cancer that has recurred (come back) after it has been treated. The cancer may come back in the stomach or in other parts of the body such as the liver or lymph nodes.
Stomach cancer treatment
Treatment options for stomach cancer depend on the cancer’s location within your stomach and its stage (extent of spread). Your doctor also thinks about your overall health and your preferences when making a treatment plan. Stomach cancer treatments include surgery, chemotherapy, radiation therapy, targeted therapy, immunotherapy and palliative care. Often the best approach uses 2 or more types of treatment. In choosing your treatment plan, you and your cancer care team will also take your age, overall health, and personal preferences into account.
Stomach cancer is often treated by a team of doctors with different specialties. Most likely, your treatment team will include:
- Gastroenterologist: a doctor who specializes in treating diseases of the digestive system
- Surgical oncologist: a doctor who treats cancer with surgery
- Medical oncologist: a doctor who treats cancer with medicines such as chemotherapy, targeted therapy, and immunotherapy
- Radiation oncologist: a doctor who treats cancer with radiation therapy
Surgery
Surgery is a common treatment of all stages of stomach cancer (gastric cancer).
Surgery can be done for two main reasons:
- Surgery to remove the cancer: Surgery may be done to remove the cancer and part or all of the stomach, as well as some nearby lymph nodes and other structures, depending on the location and stage (extent) of the cancer. The surgeon will try to leave behind as much normal stomach as possible. Sometimes other organs will need to be removed as well.
- Palliative surgery: If the cancer is too widespread to be removed completely, surgery might still be done to help prevent bleeding from the tumor or prevent the stomach from being blocked by tumor growth. This type of surgery can prevent or relieve symptoms, but it is not expected to cure the cancer.
If the cancer hasn’t spread to other parts of the body, surgery (often along with other treatments) offers the best chance to try to cure the cancer.
The following types of surgery may be used:
- Endoscopic resection. Endoscopic mucosal resection (EMR) and endoscopic submucosal dissection (ESD) are procedures that can be used to treat some very early-stage stomach cancers, when the tumor is not thought to have grown deeply into the stomach wall and the chance of spread outside the stomach is very low. Endoscopic mucosal resection (EMR) goes deeper into the stomach wall than endoscopic submucosal dissection (ESD). These procedures do not require a cut (incision) in the skin. Instead, the surgeon passes an endoscope (a long, flexible tube with a small video camera on the end) down the throat and into the stomach. Surgical tools can be passed through the endoscope to remove the tumor and some layers of the normal stomach wall below and around it. These operations are not done as often in the United States as they are in some East Asian countries like Japan where stomach cancer is more common and more often found at an early stage due to screening. If you are going to have this kind of surgery, it should be done at a center that has experience with this technique.
- Subtotal (partial) gastrectomy: In subtotal (partial) gastrectomy only part of the stomach is removed. This is often recommended if the cancer is only in the lower part of the stomach in which case it is known as a distal gastrectomy. It might also be used for cancers that are only in the upper part of the stomach in which case it is known as a proximal gastrectomy. Part of the stomach is removed, sometimes along with part of the esophagus (in a proximal gastrectomy) or the first part of the small intestine (in a distal gastrectomy). The remaining section of stomach is then reattached. Some of the omentum (an apron-like layer of fatty tissue that covers the stomach and intestines) is removed as well, along with nearby lymph nodes. If the cancer has reached the spleen or parts of other nearby organs, these are removed as well. Eating is much easier after surgery if only part of the stomach is removed instead of the entire stomach.
- The spleen may be removed. The spleen is an organ in the upper abdomen that filters the blood and removes old blood cells.
- Total gastrectomy: Total gastrectomy is done if the cancer has spread widely in the stomach. Total gastrectomy is also often advised if the cancer is in the upper part of the stomach, near the esophagus. The surgeon removes the entire stomach, nearby lymph nodes, and the omentum, and may remove the spleen and parts of the esophagus, intestines, pancreas, or other nearby organs if the cancer has reached them. The end of the esophagus is then attached to part of the small intestine so the patient can continue to eat and swallow. This allows food to move down the intestinal tract. But people who have had their stomach removed can only eat a small amount of food at a time. Because of this, they will need to eat more often.
- Lymph node removal (lymphadenectomy). In either a subtotal or total gastrectomy, the nearby lymph nodes are removed. This is known as a lymph node dissection or lymphadenectomy, and it’s a very important part of the operation. Many doctors feel that the success of the surgery is directly related to how many lymph nodes the surgeon removes.
- In the United States, it is recommended that at least 16 lymph nodes be removed called a D1 lymphadenectomy when a gastrectomy is done. Surgeons in some East Asian countries such as Japan and South Korea have had very high success rates by removing even more lymph nodes near the cancer called a D2 lymphadenectomy.
- Surgeons in Europe and the United States have not been able to equal the results of the East Asian surgeons. It is not clear if this is because East Asian surgeons are more experienced because stomach cancer is much more common in these countries or their patients tend to have earlier stage disease because they screen for stomach cancer and are healthier, or if other factors play a role. In any event, it takes a skilled surgeon who is experienced in stomach cancer surgery to remove as many lymph nodes as possible. Ask your surgeon about their experience in operating on stomach cancer. Studies have shown that the results are better when both the surgeon and the hospital have had extensive experience in treating patients with stomach cancer.
Before your surgery, talk to your surgeon about how much of the stomach will need to be removed. Some surgeons try to leave behind as much of the stomach as they can, which might allow patients to eat more normally afterward. However, the main goal of surgery is to be sure all the cancer has been removed. The surgeon will try to achieve negative surgical margins, meaning that no cancer cells are seen at the edges of the removed part of the stomach, even when looking at it under a microscope.
Most subtotal and total gastrectomies are done through a large incision (cut) in the skin of the abdomen (belly). This is sometimes referred to as an open surgical approach.
In some centers, these operations are done as a laparoscopic gastrectomy, in which long, thin surgical instruments including one with a small video camera on the end are inserted into the abdomen through several small cuts. Some surgeons do these operations using robotic-assisted laparoscopic surgery sometimes just called robotic surgery. In this technique, the surgeon sits at a control panel and moves robotic arms that have laparoscopic instruments on the ends
Although the laparoscopic approach including robotic surgery might result in a shorter hospital stay, less pain after the operation, and a shorter recovery time because of the smaller incisions, many doctors feel that this technique needs to be studied further before it can be considered a standard treatment for stomach cancer.
No matter which approach is used, it’s important that your surgeon is skilled and experienced with the technique.
For people with stomach cancer that can’t be removed completely, surgery can often still be used to help control the cancer or to help prevent or relieve symptoms or complications. If the tumor is blocking the stomach but the cancer cannot be completely removed by standard surgery, the following procedures may be used:
- Endoluminal stent placement: A procedure to insert a stent (a hollow metal tube) in order to keep a passage open and allows food to pass through it. For tumors blocking the passage into or out of the stomach, an endoscope (a long, flexible tube passed down the throat) may be done to place a stent from the esophagus to the stomach or from the stomach to the small intestine to allow the patient to eat normally. For tumors in the upper (proximal) stomach, the stent is placed where the esophagus and stomach meet. For tumors in the lower (distal) part of the stomach, the stent is placed at the junction of the stomach and the small intestine.
- Endoluminal laser therapy: A procedure in which an endoscope (a thin, lighted tube) with a laser attached is inserted into the body. A laser is an intense beam of light that can be used as a knife. This can be done to stop bleeding or help relieve a blockage without surgery.
- Gastric bypass (gastrojejunostomy): Tumors in the lower part of the stomach may eventually grow large enough to block food from leaving the stomach. For people healthy enough for surgery, one option to help prevent or treat this is to bypass the lower part of the stomach. Surgery to remove the part of the stomach with cancer that is blocking the opening into the small intestine. The stomach is connected to the jejunum (a part of the small intestine) to allow food and medicine to pass from the stomach into the small intestine.
- Subtotal gastrectomy. For some people who are healthy enough for surgery, removing the part of the stomach with the tumor can help treat problems such as bleeding, pain, or the tumor blocking the passage of food through the stomach, even if the surgery does not cure the cancer. Because the goal is not to cure the cancer, nearby lymph nodes and parts of other organs usually do not need to be removed.
- Feeding tube placement. Some people with stomach cancer aren’t able to eat or drink enough to get adequate nutrition. A minor operation can be done to place a feeding tube through the skin of the abdomen and into the lower part of the stomach known as a gastrostomy tube or G tube or into the small intestine (jejunostomy tube or J tube). Liquid nutrition can then be put directly into the tube.
Chemotherapy
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy). When chemotherapy is placed directly into the cerebrospinal fluid, an organ, or a body cavity such as the abdomen, the drugs mainly affect cancer cells in those areas (regional chemotherapy). The way the chemotherapy is given depends on the type and stage of the cancer being treated.
Many different chemo drugs can be used to treat stomach cancer, including:
- 5-FU (fluorouracil), often given along with leucovorin (folinic acid)
- Capecitabine
- Carboplatin
- Cisplatin
- Docetaxel
- Epirubicin
- Irinotecan
- Oxaliplatin
- Paclitaxel
- Trifluridine and tipiracil (Lonsurf), a combination drug in pill form
Most often, 2 or 3 of these drugs are combined (sometimes along with a targeted drug or immunotherapy drug as well). But this depends on factors such as the stage of the cancer, the person’s overall health, and whether chemo is combined with radiation therapy. Three-drug combinations can have more side effects, so they are usually reserved for people who are in very good health and who can be followed closely by their doctor.
For earlier stage cancers, some common drug combinations used before and/or after surgery include:
- Oxaliplatin plus 5-FU/leucovorin (FOLFOX), or oxaliplatin plus capecitabine (CAPOX)
- FLOT (5-FU/leucovorin, oxaliplatin, and docetaxel)
- Docetaxel or paclitaxel plus either 5-FU or capecitabine
- Cisplatin plus either 5-FU or capecitabine
- Paclitaxel and carboplatin
When chemo is given with radiation after surgery, a single drug such as 5-FU or capecitabine may be used.
For advanced stomach cancer, many of the same combinations of drugs can be used, although doctors often prefer combinations of 2 drugs rather than 3 to try to reduce side effects. Some of the most commonly used combinations include:
- Oxaliplatin plus 5-FU/leucovorin (FOLFOX), or oxaliplatin plus capecitabine (CAPOX)
- Cisplatin plus either 5-FU or capecitabine
- Irinotecan plus 5-FU/leucovorin (FOLFIRI)
- Paclitaxel plus either cisplatin or carboplatin
- Docetaxel plus cisplatin
- Epirubicin, either cisplatin or oxaliplatin, and either 5-FU or capecitabine
- Docetaxel, 5-FU, and either cisplatin, carboplatin, or oxaliplatin
If a person isn’t healthy enough to get a combination of chemo drugs, a single drug, such as 5-FU, capecitabine, docetaxel, or paclitaxel, might be used instead.
If one of these combinations or a single drug is no longer helpful, another drug or combination of drugs might be tried.
Chemo might be used at different times to help treat stomach cancer:
- Chemo can be given before surgery for stomach cancer also known as neoadjuvant treatment. Sometimes chemo is given along with radiation therapy, which is known as chemoradiation. Neoadjuvant treatment can often shrink the tumor and possibly make surgery easier. It may also help keep the cancer from coming back and help patients live longer. For some stages of stomach cancer, neoadjuvant chemo is one of the standard treatment options. Often, chemo is then given again after surgery.
- Chemo may be given after surgery has been done to remove the cancer also known as adjuvant treatment. The goal of adjuvant chemo is to kill any areas of cancer that may have been left behind but are too small to see. This can help keep the cancer from coming back. Often, for stomach cancer, chemo is given with radiation therapy after surgery. This may be especially helpful for cancers that could not be removed completely by surgery.
- Chemo may be given as the primary (main) treatment if the cancer has spread (metastasized) to distant parts of the body, or if it can’t be removed for some other reason. Chemo may help shrink the cancer or slow its growth, which can relieve symptoms and help people live longer.
Doctors give chemo in cycles, with each period of treatment followed by a rest period to allow the body time to recover. Each cycle typically lasts for a few weeks.
Chemo side effects
Chemo drugs attack cells in the body that are dividing quickly, which can lead to side effects. These depend on the type and dose of drugs, and the length of treatment. Side effects from chemo can include:
- Nausea and vomiting
- Loss of appetite
- Hair loss
- Diarrhea or constipation
- Mouth sores
- Increased chance of infection (from a shortage of white blood cells)
- Easy bleeding or bruising (from a shortage of platelets)
- Fatigue and shortness of breath (from a shortage of red blood cells)
These side effects usually go away once treatment is finished. For example, hair will usually grow back after treatment ends. Be sure to tell your cancer care team about any side effects you have because there are often ways to help with them. For example, you can be given drugs to prevent or reduce nausea and vomiting.
Some chemo drugs have specific side effects. Your treatment team can help you know which of these you might need to look out for.
- Nerve damage (neuropathy): Cisplatin, oxaliplatin, docetaxel, and paclitaxel can damage nerves. This can sometimes lead to symptoms (mainly in the hands and feet) such as pain, burning or tingling sensations, sensitivity to cold or heat, or weakness. In most cases this goes away once treatment is stopped, but it may be long-lasting in some people. Oxaliplatin can also affect nerves in the throat, causing throat pain that is worse when trying to eat or drink cold liquids or foods.
- Heart damage: Epirubicin and some other drugs can damage the heart if used for a long time or in high doses. For this reason, doctors carefully control the doses and use heart tests such as echocardiograms or MUGA scans to monitor heart function. Treatment with these drugs is stopped at the first sign of heart damage.
- Hand-foot syndrome can occur during treatment with capecitabine or 5-FU (when given as an infusion). This starts out as redness in the hands and feet, which can then progress to pain and sensitivity in the palms and soles. If it worsens, blistering, calluses, or skin peeling can occur, sometimes leading to painful sores. The best way to prevent severe hand-foot syndrome is to tell your doctor if you have early symptoms, such as redness or sensitivity, so that steps can be taken to keep things from getting worse.
- Diarrhea is a common side effect with many chemo drugs, but it can be particularly bad with irinotecan. It needs to be treated right away — at the first sign of loose stools — to prevent severe dehydration. If you are getting a chemo drug that is likely to cause diarrhea, your doctor will give you instructions on what drugs to take and how often to take them to control this symptom.
Some chemo drugs can cause other side effects. Talk with your cancer treatment team about what types of side effects you should watch for.
Radiation therapy
Radiation therapy is a cancer treatment that uses high-energy X-rays or other types of radiation to kill cancer cells or keep them from growing. There are two types of radiation therapy:
- External radiation therapy uses a machine outside the body to send radiation toward the cancer.
- Internal radiation therapy uses a radioactive substance sealed in needles, seeds, wires, or catheters that are placed directly into or near the cancer.
Radiation therapy can be used in different ways to help treat stomach cancer (gastric cancer):
- For some earlier stage cancers, radiation can be used along with chemotherapy (chemo) before surgery to try to shrink the cancer and make it easier to remove. This combination is known as chemoradiation.
- After surgery, radiation therapy can be used along with chemo to try to kill any cancer cells that weren’t removed during the surgery. This may help delay or prevent recurrence of the cancer.
For cancers that can’t be removed by surgery, radiation therapy can sometimes be used to help slow the growth of the cancer and ease symptoms, such as pain, bleeding, or eating problems.
The way the radiation therapy is given depends on the type and stage of the cancer being treated. External radiation therapy is used to treat gastric cancer.
When radiation therapy is used to treat stomach cancer, the radiation is focused on the cancer from a machine outside the body. Often, special types of radiation therapy, such three-dimensional conformal radiation therapy (3D-CRT) or intensity modulated radiation therapy (IMRT) are used. These approaches use computers to aim the radiation at the cancer from several angles (as well as other special techniques). This can help focus the radiation on the cancer and limit the damage to nearby normal tissues.
Before your treatments start, your radiation team will take careful measurements to determine the correct angles for aiming the radiation beams and the proper dose of radiation. This planning session, called simulation, usually includes getting imaging tests such as CT or MRI scans.
Radiation therapy is much like getting an X-ray, but the radiation is much stronger. The treatment itself is painless. Each treatment lasts only a few minutes, although the setup time — getting you into place for treatment — usually takes longer. Treatments are usually given 5 days a week over at least several weeks, but the length of treatment depends on the reason it’s being given.
Side effects from radiation therapy for stomach cancer can include:
- Skin problems, ranging from redness to blistering and peeling, in areas the radiation passed through
- Nausea and vomiting
- Diarrhea
- Fatigue
- Low blood cell counts
These usually go away within a few weeks after the treatment is finished.
When radiation is given with chemotherapy, side effects are often worse.
Some people may have problems eating and getting enough fluids during and after treatment. Some might need to have fluids given into a vein (IV) or have a feeding tube placed to get nutrition during treatment. If the tube is only needed for a short time, one can be passed down the nose and throat and into the stomach or intestine. If the tube is needed for a longer time, it can be placed through the skin in the abdomen and into the intestine during a surgical procedure. This is known as a jejunostomy tube or J-tube. Liquid nutrition can then be put directly into the tube.
Be sure to tell your doctor about any side effects you have, because there are often ways to relieve them.
Radiation might also damage nearby organs. This could lead to problems such as heart or lung damage, or even an increased risk of another cancer later on. Doctors do their best to prevent this by using only the needed dose of radiation, carefully controlling where the beams are aimed, and shielding certain parts of the body from the radiation during treatment.
Chemoradiation
Chemoradiation therapy combines chemotherapy and radiation therapy to increase the effects of both. Chemoradiation given after surgery, to lower the risk that the cancer will come back, is called adjuvant therapy. Chemoradiation given before surgery, to shrink the tumor (neoadjuvant therapy), is being studied.
Targeted therapy
Targeted therapy is a type of treatment that uses drugs or other substances to identify and attack specific cancer cells without harming normal cells. Monoclonal antibody therapy is a type of targeted therapy used in the treatment of gastric cancer.
Monoclonal antibody therapy uses antibodies made in the laboratory from a single type of immune system cell. These antibodies can identify substances on cancer cells or normal substances that may help cancer cells grow. The antibodies attach to the substances and kill the cancer cells, block their growth, or keep them from spreading. Monoclonal antibodies are given by infusion. They may be used alone or to carry drugs, toxins, or radioactive material directly to cancer cells. For stage 4 gastric cancer and gastric cancer that has recurred, monoclonal antibodies, such as trastuzumab or ramucirumab, may be given. Trastuzumab blocks the effect of the growth factor protein HER2, which sends growth signals to gastric cancer cells. Ramucirumab blocks the effect of the protein VEGF and may prevent the growth of new blood vessels that tumors need to grow.
Drugs that target HER2
In some people with stomach cancer, the cancer cells have too much of a growth-promoting protein called HER2 on their surface. Cancers with increased levels of HER2 are called HER2-positive. Drugs that target the HER2 protein can often be helpful in treating these cancers.
Trastuzumab (Herceptin, others)
Trastuzumab is a monoclonal antibody, a man-made version of an immune system protein, which targets HER2. Adding trastuzumab to chemo can help some people with advanced, HER2-positive stomach cancer live longer than just chemo alone.
Trastuzumab only works if the cancer cells have too much HER2, so samples of the cancer must be tested for HER2 before starting treatment.
Trastuzumab is infused into a vein through an intravenous (IV) line or central venous catheter. For stomach cancer, it is typically given once every 2 or 3 weeks along with chemo.
Herceptin was the original brand name for trastuzumab, but several similar versions called biosimilars are now available as well, including Ogivri, Herzuma, Ontruzant, Trazimera, and Kanjinti.
Side effects of trastuzumab
The side effects of trastuzumab tend to be relatively mild. They can include fever and chills, weakness, nausea, vomiting, cough, diarrhea, and headache. These side effects occur less often after the first dose.
This drug can also rarely cause heart damage. The risk is higher if trastuzumab is given with certain chemo drugs called anthracyclines, such as epirubicin. Before starting treatment with this drug, your doctor may test your heart function with an echocardiogram or a multigated acquisition (MUGA) scan – an imaging test to see how your heart pumps blood.
Fam-trastuzumab deruxtecan (Enhertu)
This is an antibody-drug conjugate (ADC), which is a monoclonal antibody linked to a chemotherapy drug. In this case, the anti-HER2 antibody acts like a homing signal by attaching to the HER2 protein on cancer cells, bringing the chemo directly to them.
This ADC can be used by itself to treat advanced HER2-positive stomach cancer, typically after treatment with trastuzumab has been tried.
This drug is infused into a vein (through an IV line or central venous catheter). For stomach cancer, it is typically given once every 3 weeks.
Side effects of fam-trastuzumab deruxtecan
Fam-trastuzumab deruxtecan (Enhertu) can cause low blood cell counts, which can increase a person’s risk of infections and bleeding. Other common side effects of this drug can include nausea, vomiting, diarrhea or constipation, loss of appetite, fever, feeling tired, and hair loss.
Fam-trastuzumab deruxtecan (Enhertu) can cause serious lung disease in some people, which might even be life threatening. It’s very important to let your doctor or nurse know right away if you’re having symptoms such as coughing, wheezing, trouble breathing, or fever.
Fam-trastuzumab deruxtecan (Enhertu) can also rarely cause heart damage. Before starting treatment with this drug, your doctor may test your heart function with an echocardiogram or a MUGA scan.
Drugs that target VEGF
For tumors to grow, they need to make new blood vessels to get blood and nutrients. One of the proteins that tells cells in the body to make new blood vessels is called VEGF. The VEGF protein does this by attaching to cell surface proteins called VEGF receptors.
Ramucirumab (Cyramza)
Ramucirumab (Cyramza) is a monoclonal antibody that binds to a VEGF receptor. This keeps VEGF from binding to cells and telling them to make more blood vessels. This can help slow or stop the growth of some cancers.
Ramucirumab is used to treat advanced stomach cancer, most often after at least one chemo drug (or combination) stops working.
Ramucirumab is given as infusion into a vein (IV), typically once every 2 weeks. It can be given by itself or along with chemo.
Side effects of ramucirumab
The most common side effects of this drug are high blood pressure, headache, and diarrhea.
Less common but possibly serious side effects can include blood clots, severe bleeding, holes forming in the stomach or intestines (perforations), and problems with wound healing. If a hole forms in the stomach or intestine, it can lead to severe infection and may require surgery to correct.
TRK inhibitors
A very small number of stomach cancers have changes in one of the NTRK genes. This causes them to make abnormal TRK proteins, which can lead to abnormal cell growth and cancer.
Larotrectinib (Vitrakvi) and entrectinib (Rozlytrek) are drugs that target the TRK proteins. These drugs can be used to treat advanced cancers with NTRK gene changes that are still growing despite other treatments.
Larotrectinib (Vitrakvi) and entrectinib (Rozlytrek) are taken as pills, once or twice daily.
Side effects of TRK inhibitors
Common side effects of these drugs can include dizziness, fatigue, nausea, vomiting, constipation, weight gain, and diarrhea.
Less common but serious side effects can include abnormal liver tests, heart problems, and confusion.
Drug that target CLDN18.2
Claudin 18.2 (CLDN18.2) is a protein that plays an important role in keeping healthy epithelial cells bound together. Epithelial cells are cells that are commonly found along the gastrointestinal tract. When an epithelial cell turns into a cancer cell, however, CLDN18.2 may move to the surface of the cancer cell. As a result, CLDN18.2 can serve as a target for therapy.
Zolbetuximab (Vyloy)
Zolbetuximab is a monoclonal antibody that targets CLDN18.2. It is used to treat advanced stomach cancer that is HER2-negative and found to express high amounts of CLDN18.2 on their cell surface. For this type of stomach cancer, zolbetuximab can be given with chemo as the initial therapy.
Zolbetuximab is given into a vein (IV), typically once every 2 or 3 weeks, along with chemo.
Side effects of zolbetuximab
Common side effects are nausea, vomiting, diarrhea, fatigue, decreased appetite, stomach pain, weight loss, constipation, and decreased sensation in fingertips/toes (also called sensory neuropathy).
Less common but serious side effects can include low blood cell counts, which can increase a person’s risk of infections and bleeding; abnormal liver tests; and changes in electrolyte levels, such as sodium, phosphate, potassium, and magnesium.
Immunotherapy
Immunotherapy is the use of medicines to help a person’s own immune system find and destroy cancer cells more effectively. It can be used to treat some people with stomach cancer.
Immune checkpoint inhibitors
An important part of the immune system is its ability to prevent itself from attacking normal cells in the body. To do this, it uses “checkpoint” proteins on immune cells, which act like switches that need to be turned on (or off) to start an immune response. Cancer cells sometimes use these checkpoints to avoid being attacked by the immune system.
Drugs that target these checkpoints called immune checkpoint inhibitors can be used to treat some people with stomach cancer (gastric cancer).
PD-1 inhibitors
Nivolumab (Opdivo), pembrolizumab (Keytruda), and tislelizumab (Tevimbra) are drugs that target PD-1, a protein on immune system cells called T cells. The PD-1 protein normally helps keep T cells from attacking other cells in the body. By blocking PD-1, these drugs boost the immune response against cancer cells. This can shrink some tumors or slow their growth.
Nivolumab (Opdivo) can be used in people with advanced stomach cancer, typically along with chemotherapy. Nivolumab is given as an intravenous (IV) infusion, usually once every 2 or 3 weeks.
Pembrolizumab (Keytruda) can be used as part of the first treatment for people with advanced stomach cancer, either:
- Along with chemotherapy if the cancer cells test negative for HER2, or
- Along with chemotherapy and the targeted drug trastuzumab, if the cancer cells test positive for both HER2 and for the PD-L1 protein
Pembrolizumab can also be used after other treatments including chemotherapy have been tried, and if the cancer cells test positive for any of the following:
- A high level of microsatellite instability (MSI-H) or a defect in a mismatch repair gene (dMMR)
- A high tumor mutational burden (TMB-H), meaning they have many gene mutations
Pembrolizumab is given as an intravenous (IV) infusion, typically once every 3 or 6 weeks.
Tislelizumab (Tevimbra) can be used along with chemotherapy as a first treatment in people with advanced stomach cancer, if the cancer cells test negative for the HER2 protein and positive for the PD-L1 protein.T islelizumab is given as an intravenous (IV) infusion, usually once every 3 weeks.
Possible side effects of immune checkpoint inhibitors can include:
- Feeling tired or weak
- Fever
- Cough
- Nausea
- Itching
- Skin rash
- Loss of appetite
- Muscle or joint pain
- Shortness of breath
- Constipation or diarrhea
Other, more serious side effects occur less often. These can include:
- Infusion reactions: Some people might have an infusion reaction while getting one of these drugs. This is like an allergic reaction, and can include fever, chills, flushing of the face, rash, itchy skin, feeling dizzy, wheezing, and trouble breathing. It’s important to tell your doctor or nurse right away if you have any of these symptoms while getting one of these drugs.
- Autoimmune reactions: These drugs work by basically removing one of the safeguards on the body’s immune system. Sometimes this causes the immune system to attack other parts of the body, which can lead to serious or even life-threatening problems in the lungs, intestines, liver, hormone-making glands, kidneys, skin, or other organs.
It’s very important to report any new side effects to your cancer treatment team right away. If serious side effects do occur, treatment may need to be stopped and you may get high doses of corticosteroids to suppress your immune system.
Stomach Cancer Treatment Based on Stage
Treatment of stomach cancer (gastric cancer) depends largely on where the cancer is in the stomach and how far it has spread. But other factors, such as a person’s age, overall health, and preferences, can be important as well.
Stomach cancer typically starts in the inner lining of the stomach. From there, it can grow and spread in different ways. It can grow through the wall of the stomach and into nearby organs. It might also spread to the nearby lymph nodes. As the cancer becomes more advanced, it can travel through the bloodstream or lymph system and spread (metastasize) to organs such as the liver, lungs, and bones, which can make it harder to treat.
Surgery to remove the cancer is typically part of treatment if it can be done, as it offers the best chance for long-term survival. But surgery might not be a good option if the cancer has spread widely or if a person isn’t healthy enough for it. Other treatments such as chemotherapy and radiation therapy are often part of treatment as well, either along with or instead of surgery. Newer treatments such as targeted drugs and immunotherapy might be helpful in some situations as well.
Because most people will get different types of treatment for their cancer, it’s important that a team of doctors review and discuss the best options for treatment. Stomach cancer isn’t common in the United States, and it can be challenging to treat, so it’s important that your cancer care team is experienced in treating stomach cancer.
While the AJCC TNM stage of the cancer can be important when deciding on treatment, doctors often divide stomach cancers into larger groups when determining the best treatment options. These include:
- Very early stage cancers. These cancers have not grown deeply into the wall of the stomach or spread outside the stomach. These cancers make up only a small portion of stomach cancers in the United States.
- Potentially resectable cancers. These cancers have grown deeper into the stomach wall and may have grown into nearby areas or lymph nodes. But these cancers aren’t thought to have spread to distant parts of the body, so surgery might still be an option to try to remove (resect) them completely. Depending on the location and extent of the cancer, some people might get surgery as their first treatment, with either subtotal gastrectomy (removal of part of the stomach) or total gastrectomy (removal of the entire stomach). Nearby lymph nodes (and possibly parts of nearby organs) are removed as well. Other people might get chemotherapy alone or chemo plus radiation therapy (known as chemoradiation) first to try to shrink the cancer and make the surgery easier. After surgery, chemo (or chemoradiation, if it wasn’t used before surgery) might be given to try to kill any remaining cancer cells. This is especially true if it’s not clear that all of the cancer was removed, or if too few lymph nodes were removed during surgery. Another option if not all of the cancer was removed might be a more extensive operation.
- Unresectable local or regional cancers. These cancers have also grown deeper into the stomach wall and may have grown into nearby areas or lymph nodes. While the cancer hasn’t yet spread to distant parts of the body, it’s unlikely it can all be removed with surgery. For example, the cancer might be too close to vital areas, or the person might not be healthy enough for major surgery.
- Metastatic cancers. These cancers have spread to distant parts of the body.
Stage 0 Gastric Cancer
Standard treatment options:
- Surgery. Very early stage cancers can typically be treated by surgery, with either subtotal gastrectomy (removal of part of the stomach) or total gastrectomy (removal of the entire stomach). Nearby lymph nodes are removed as well.
Stage 0 is gastric cancer confined to mucosa. Some small stage 0 cancers can be treated by endoscopic resection. In this procedure the cancer and some layers of the stomach wall are removed through an endoscope passed down the throat. This procedure is done more often in countries like Japan, where stomach cancer is often detected early during screening. It is rare to find stomach cancer so early in the United States, so this treatment has not been used as often here. If it is done, it should be at a cancer center that has experience with this technique.
Experience in Japan, where stage 0 is diagnosed frequently, indicates that more than 90% of patients treated by gastrectomy with lymphadenectomy will survive beyond 5 years. An American series has confirmed these results 76.
If the results of surgery (or endoscopic resection) show that all of the cancer has been removed, the person can usually be followed closely, without needing any further treatment. If it’s not clear that all of the cancer has been removed, chemotherapy and radiation are likely to be recommended. Another option might be a more extensive surgery to remove the cancer.
Stage 1 Gastric Cancer
Standard treatment options:
One of the following surgical procedures:
- Distal subtotal gastrectomy (if the lesion is not in the fundus or at the cardioesophageal junction).
- Proximal subtotal gastrectomy or total gastrectomy, both with distal esophagectomy (if the lesion involves the cardia). These tumors often involve the submucosal lymphatics of the esophagus.
- Total gastrectomy (if the tumor involves the stomach diffusely or arises in the body of the stomach and extends to within 6 cm of the cardia or distal antrum).
Regional lymphadenectomy is recommended with all of the above procedures. Splenectomy is not routinely performed 77.
Postoperative chemoradiation therapy for patients with node-positive (T1 N1) and muscle-invasive (T2 N0) disease 78.
Surgical resection including regional lymphadenectomy is the treatment of choice for patients with stage I gastric cancer 77. If the lesion is not in the cardioesophageal junction and does not diffusely involve the stomach, subtotal gastrectomy is the procedure of choice, since it has been demonstrated to provide equivalent survival when compared with total gastrectomy and is associated with decreased morbidity 79. When the lesion involves the cardia, proximal subtotal gastrectomy or total gastrectomy (including a sufficient length of esophagus) may be performed with curative intent. If the lesion diffusely involves the stomach, total gastrectomy is required. At a minimum, surgical resection should include greater and lesser curvature perigastric regional lymph nodes. Note that in patients with stage I gastric cancer, perigastric lymph nodes may contain cancer.
In patients with node-positive (T1 N1) and muscle-invasive (T2 N0) disease, postoperative chemoradiation therapy may be considered. A prospective multi-institution phase III trial evaluated postoperative combined chemoradiation therapy versus surgery alone in 556 patients with completely resected stage IB to stage IV (M0) adenocarcinoma of the stomach and gastroesophageal junction and reported a significant survival benefit with adjuvant combined modality therapy 78. With a median follow-up of 5 years, median survival was 36 months for the adjuvant chemoradiation therapy group and 27 months for the surgery-alone arm. Three-year overall survival rates were 50%, and relapse-free survival rates were 48% with adjuvant chemoradiation therapy versus 3-year overall survival rates of 41% and relapse-free survival rates of 31% for surgery alone. However, only 36 patients in the trial had stage IB tumors (18 patients in each arm) 80. Since the prognosis is relatively favorable for patients with completely resected stage IB disease, the effectiveness of adjuvant chemoradiation therapy for this group is less clear.
Stage 2 Gastric Cancer
Standard treatment options:
- One of the following surgical procedures:
- Distal subtotal gastrectomy (if the lesion is not in the fundus or at the cardioesophageal junction).
- Proximal subtotal gastrectomy or total gastrectomy (if the lesion involves the cardia).
- Total gastrectomy (if the tumor involves the stomach diffusely or arises in the body of the stomach and extends to within 6 cm of the cardia).
- Regional lymphadenectomy is recommended with all of the above procedures. Splenectomy is not routinely performed 77.
- Postoperative chemoradiation therapy 78.
- Perioperative chemotherapy 81.
- Postoperative chemotherapy.
Surgical resection with regional lymphadenectomy is the treatment of choice for patients with stage II gastric cancer 77. If the lesion is not in the cardioesophageal junction and does not diffusely involve the stomach, subtotal gastrectomy is the procedure of choice. When the lesion involves the cardia, proximal subtotal gastrectomy or total gastrectomy may be performed with curative intent. If the lesion diffusely involves the stomach, total gastrectomy and appropriate lymph node resection may be required. The role of extended lymph node (D2) dissection is uncertain 82 and in some series is associated with increased morbidity 83.
Postoperative chemoradiation therapy may be considered for patients with stage II gastric cancer. A prospective multi-institution phase III trial evaluated postoperative combined chemoradiation therapy versus surgery alone in 556 patients with completely resected stage IB to stage IV (M0) adenocarcinoma of the stomach and gastroesophageal junction and reported a significant survival benefit with adjuvant combined modality therapy 78. With a median follow-up of 5 years, median survival was 36 months for the adjuvant chemoradiation therapy group and 27 months for the surgery-alone arm. Three-year overall survival rates were 50%, and relapse-free survival rates were 48% with adjuvant chemoradiation therapy versus 3-year overall survival rates of 41% and relapse-free survival rates of 31% for surgery alone.The rate of distant metastases was 32% for the surgery-alone arm and 40% for the chemoradiation therapy arm.
Investigators in Europe evaluated the role of preoperative and postoperative chemotherapy without radiation therapy 81. In the randomized phase III trial, patients with stage II or higher adenocarcinoma of the stomach or of the lower third of the esophagus were assigned to receive three cycles of epirubicin, cisplatin, and continuous infusion fluorouracil (ECF) before and after surgery or to receive surgery alone. Compared with the surgery group, the perioperative chemotherapy group had a significantly higher likelihood of progression-free survival (hazard ratio for progression, 0.66) and of overall survival (hazard ratio for death, 0.75). Five-year overall survival was 36.3%, 29 to 43 for the perioperative chemotherapy group and 23%, 16.6 to 29.4 for the surgery group 81.
Japanese investigators randomly assigned 1,059 patients with stage II or III gastric cancer who had undergone a D2 gastrectomy to receive either 1 year of S-1, an oral fluoropyrimidine not available in the United States, or follow-up after surgery alone 84. Patients were randomly assigned in a 1:1 fashion. The 3-year overall survival rate was 80.1% in the S-1 group and 70.1% in the surgery-only group. The hazard ratio for death in the S-1 group, as compared with the surgery-only group, was 0.68 84.
Subsequently, investigators in Asia evaluated the role of capecitabine/oxaliplatin as adjuvant therapy after gastric cancer resection. In the CLASSIC trial, 37 centers in South Korea, China, and Taiwan randomly assigned 1,035 patients with stage IIA, IIB, IIIA, or IIIB gastric cancer who had undergone a curative D2 gastrectomy to receive adjuvant chemotherapy (eight 3-week cycles of capecitabine plus oxaliplatin) or follow-up post-surgery alone 85. The 3-year disease-free survival rate was 74% in the chemotherapy group and 59% in the surgery-alone group (hazard ratio, 0.56). The 3-year overall survival was 83% in the chemotherapy group and 78% in the surgery-alone group (hazard ratio, 0.72) 85.
Stage 3 Gastric Cancer
Standard treatment options:
- Radical surgery. Curative resection procedures are confined to patients who do not have extensive nodal involvement at the time of surgical exploration.
- Postoperative chemoradiation therapy 78.
- Perioperative chemotherapy 81.
- Postoperative chemotherapy.
All patients with tumors that can be resected should undergo surgery. As many as 15% of selected stage III patients can be cured by surgery alone, particularly if lymph node involvement is minimal (<7 lymph nodes).
Postoperative chemoradiation therapy may be considered for patients with stage III gastric cancer. A prospective multi-institution phase III trial evaluating postoperative combined chemoradiation therapy versus surgery alone in 556 patients with completely resected stage IB to stage IV (M0) adenocarcinoma of the stomach and gastroesophageal junction reported a significant survival benefit with adjuvant combined modality therapy 78. With a median follow-up of 5 years, median survival was 36 months for the adjuvant chemoradiation therapy group and 27 months for the surgery-alone arm. Three-year overall survival rates were 50%, and relapse-free survival rates were 48% with adjuvant chemoradiation therapy versus 3-year overall survival rates of 41% and relapse-free survival rates of 31% for surgery alone.
Investigators in Europe evaluated the role of preoperative and postoperative chemotherapy without radiation therapy 81. In the randomized phase III trial, patients with stage II or higher adenocarcinoma of the stomach or of the lower third of the esophagus were assigned to receive three cycles of epirubicin, cisplatin, and continuous infusion 5-fluorouracil (ECF) before and after surgery or to receive surgery alone. Compared with the surgery group, the perioperative chemotherapy group had a significantly higher likelihood of progression-free survival (hazard ratio for progression, 0.66) and of overall survival (hazard ratio for death, 0.75). Five-year overall survival was 36.3%, 29 to 43 for the perioperative chemotherapy group and 23%, 16.6 to 29.4 for the surgery group 81.
Japanese investigators randomly assigned 1,059 patients with stage II or III gastric cancer who had undergone a D2 gastrectomy to receive either 1 year of S-1, an oral fluoropyrimidine not available in the United States, or follow-up after surgery alone 84. Patients were randomized in a 1:1 fashion. The 3-year overall survival rate was 80.1% in the S-1 group and 70.1% in the surgery-only group. The hazard ratio for death in the S-1 group, as compared with the surgery-only group, was 0.68 84.
Subsequently, investigators in Asia evaluated the role of capecitabine/oxaliplatin as adjuvant therapy after gastric cancer resection. In the CLASSIC trial , 37 centers in South Korea, China, and Taiwan randomly assigned 1,035 patients with stage IIA, IIB, IIIA, or IIIB gastric cancer who had undergone a curative D2 gastrectomy to receive adjuvant chemotherapy (eight 3-week cycles of capecitabine plus oxaliplatin) or follow-up post-surgery alone 85. The 3-year disease-free survival rate was 74% in the chemotherapy group and 59% in the surgery-alone group. The 3-year overall survival was 83% in the chemotherapy group and 78% in the surgery-alone group 85.
Stage 4 and Recurrent Gastric Cancer
Metastatic cancers have spread to distant parts of the body, and they are very hard to cure. Cancer that comes back after initial treatment is known as recurrent cancer.
Standard treatment options:
- Palliative chemotherapy with:
- Trastuzumab, cisplatin, and either 5-FU or capecitabine in patients with HER2-positive tumors (3+ on immunohistochemistry [IHC] or fluorescence in situ hybridization [FISH]-positive).
- Endoluminal laser therapy, endoluminal stent placement, or gastrojejunostomy, may be helpful to patients with gastric obstruction 92.
- Palliative radiation therapy may alleviate bleeding, pain, and obstruction.
- Palliative resection should be reserved for patients with continued bleeding or obstruction.
Standard chemotherapy versus best supportive care for patients with metastatic gastric cancer has been tested in several clinical trials, and there is general agreement that patients who receive chemotherapy live for several months longer on average than patients who receive supportive care 93, 94, 95. During the last 20 years, multiple randomized studies evaluating different treatment regimens (monotherapy vs. combination chemotherapy) have been performed in patients with metastatic gastric cancer with no clear consensus emerging as to the best management approach. A meta-analysis of these studies demonstrated an hazard ratio of 0.83 for overall survival in favor of combination chemotherapy 96.
Of all the combination regimens, Epirubicin, Cisplatin, and 5-FU (ECF) is often considered the reference standard in the United States and Europe. In one European trial, 274 patients with metastatic esophagogastric cancer were randomly assigned to receive either ECF or 5-FU, doxorubicin, and methotrexate (FAMTX) 97. The group who received ECF had a significantly longer median survival (8.9 vs. 5.7 months) than the FAMTX group 97. In a second trial that compared ECF with mitomycin, cisplatin, and 5-FU (MCF), there was no statistically significant difference in median survival (9.4 vs. 8.7 months) 87.
Oxaliplatin and capecitabine are often substituted for cisplatin and 5-FU within the ECF regimen as a result of data from the REAL-2 trial 88. This randomized trial of 1,002 patients with advanced esophageal, gastroesophageal junction, or gastric cancer utilized a 2 × 2 design to demonstrate noninferior median overall survival in patients treated with capecitabine rather than 5-FU (hazard ratio death = 0.86) and in patients treated with oxaliplatin in place of cisplatin (hazard ratio death = 0.92).
An international collaboration of investigators randomly assigned 445 patients with metastatic gastric cancer to receive docetaxel, cisplatin, and 5-FU (DCF) or Cisplatin, and 5-FU 98. Time-to-treatment progression was the primary endpoint. Patients who received DCF experienced a significantly longer time-to-treatment progression (5.6 months vs. 3.7 months). The median overall survival was significantly longer for patients who received DCF versus patients who received CF (9.2 months vs. 8.6 months) 98. There were high toxicity rates in both arms. Febrile neutropenia was more common in patients who received DCF (29% vs. 12%), and the death rate on the study was 10.4% for patients on the DCF arm and 9.4% for patients on the CF arm 99.
Whether the CF regimen should be considered as an index regimen for the treatment of patients with metastatic gastric cancer is the subject of debate 99. The results of a study that randomly assigned 245 patients with metastatic gastric cancer to receive CF, FAMTX, or ELF demonstrated no significant difference in response rate, progression-free survival, or overall survival between the arms 89. Grades 3 and 4 neutropenia occurred in 35% to 43% of patients on all arms, but severe nausea and vomiting was more common in patients in the CF arm and occurred in 26% of those patients 89.
Trastuzumab
In an open-label, international phase III trial, patients with HER2-positive metastatic, inoperable locally advanced, or recurrent gastric or GE junction cancer were randomly assigned to chemotherapy with or without the anti-HER2 monoclonal antibody trastuzumab.[18] HER2 positivity was defined as either 3+ staining by IHC or a HER2 to CEP17 ratio of two or more using FISH. Tumors from 3,665 patients were HER2 tested; of the patients, 810 were positive (22%) and 594 met eligibility criteria for randomization. Chemotherapy consisted of cisplatin plus 5-FU or capecitabine chosen at the investigator’s discretion. The study treatment was administered every 3 weeks for six cycles, and trastuzumab was continued every 3 weeks until disease progression, unacceptable toxicity, or withdrawal of consent. Crossover to trastuzumab at disease progression was not permitted. Median overall survival was 13.8 months in patients assigned to trastuzumab and 11.1 months in patients assigned to chemotherapy alone 100. There was no significant difference in rates of any adverse event, and cardiotoxic effects were equally rare in both arms.
Second-line Chemotherapy
When patients develop progression of disease after first-line chemotherapy, there is no standard treatment option. Investigators in Korea randomly assigned patients with advanced gastric cancer who had received one or two prior chemotherapy regimens involving both a fluoropyrimidine and a platinum agent to either salvage chemotherapy or best supportive care in a 2:1 fashion 101. Salvage chemotherapy consisted of either docetaxel (60 mg/m2 every 3 weeks) or irinotecan (150 mg/m2 every 2 weeks) and was left to the discretion of the treating physicians. Of the 202 patients enrolled, 133 received salvage chemotherapy and 69 received best supportive care. Median overall survival was 5.3 months in the group that received salvage chemotherapy and 3.8 months in the group that received best supportive care. There was no difference in median OS between docetaxel and irinotecan (5.2 months vs. 6.5 months 101.
Ramucirumab
Ramucirumab is a fully humanized monoclonal antibody directed against the vascular endothelial growth factor receptor-2. In the international, phase III, placebo-controlled, REGARD trial, 355 patients with stage IV gastric or gastroesophageal junction cancer who had progressed on a first-line fluorouracil- or platinum-containing regimen were randomly assigned in a 2:1 fashion to ramucirumab or placebo 102. Patients who were assigned to ramucirumab had a significantly improved median overall survival of 5.2 months compared with patients assigned to the placebo who had a median overall survival of 3.8 months. Rates of hypertension were higher in the ramucirumab group than in the placebo group. Ramucirumab is an acceptable treatment in cisplatin or 5-fluorouracil refractory, stage IV, gastric cancer 102.
In the international, double-blinded, phase III RAINBOW trial, 665 patients were randomly assigned to receive paclitaxel (80 mg/m2) on days 1, 8, and 15 every 28 days with ramucirumab (8 mg/kg) added on days 1 and 15 or a placebo added on days 1 and 15 103. Patients assigned to ramucirumab had a significant improvement in median overall survival of 9.6 months compared with patients assigned to a placebo who had a median overall survival of 7.4 months. Grade 3 or higher neutropenia, fatigue, hypertension, and abdominal pain were more common in the ramucirumab group. The combination of paclitaxel and ramucirumab is an acceptable second-line-chemotherapy regimen in patients with stage IV gastric or gastroesophageal junction cancer 103.
Treatment options under clinical evaluation:
Palliative chemotherapy with:
- Irinotecan and cisplatin.
- Folic acid, 5-FU, and irinotecan (FOLFIRI).
- Leucovorin, 5-FU, and oxaliplatin (FOLFOX).
Phase II studies evaluating irinotecan-based or oxaliplatin-based regimens demonstrate similar response rates and time-to-treatment progression to those found with ECF or CF, but the former may be less toxic 104, 105, 106, 107, 108, 109. There are conflicting data regarding relative efficacy of any one regimen for another. Ongoing studies are evaluating these newer regimens.
Stomach cancer prognosis
The prognosis of patients with gastric cancer is related to tumor extent and includes both nodal involvement and direct tumor extension beyond the gastric wall 110, 111. Tumor grade may also provide some prognostic information 112.
In localized distal gastric cancer, more than 50% of patients can be cured. However, early-stage disease accounts for only 10% to 20% of all cases diagnosed in the United States. The remaining patients present with metastatic disease in either regional or distant sites. The overall survival rate in these patients at 5 years ranges from almost no survival for patients with disseminated disease to almost 50% survival for patients with localized distal gastric cancers confined to resectable regional disease. Even with apparent localized disease, the 5-year survival rate of patients with proximal gastric cancer is only 10% to 15%. Although the treatment of patients with disseminated gastric cancer may result in palliation of symptoms and some prolongation of survival, long remissions are uncommon.
Speak with your doctor for a more accurate assessment of your prognosis. The type of cancer you have, its spread, your health and how your cancer responds to treatment all shape your prognosis.
Incidence and mortality of stomach cancer
The age-adjusted incidence rate for gastric cancer in the United States for the years 2004 to 2008 was 7.7 persons per 100,000 population. Incidence among men is twice as high as among women 113. Mortality rates for gastric cancer have been declining worldwide in recent decades, most prominently in the United States 114. Mortality rates for white males in the United States were approximately 40 deaths per 100,000 population in 1930, compared with 4.6 deaths per 100,000 population for the years 2003 to 2007. The death rate from gastric cancer for black males was 2.3 times higher than for whites for the years 2003 to 2007 115. The annual number of new cases seems to be steady in recent years; in 2017, it is estimated that 28,000 Americans will be diagnosed with gastric cancer and 10,960 persons will die of it 116. Gastric cancer is the fourth most common cancer in the world 117. Worldwide, the estimated number of cases per year in 2008 was 988,000, and the estimated number of deaths was 736,000. Age-standardized annual incidence rates vary widely across the world: from 3.9 to 42.4 cases per 100,000 in men, and from 2.2 to 18.3 cases per 100,000 in women. More than 70% of cases occur in developing countries, and 50% of the cases occur in Eastern Asia 117.
Most cancers in the United States are advanced at diagnosis, which is reflected in an overall 5-year survival rate of 29.9% from 2005 to 2011 118. Carcinomas localized to the mucosa or submucosa (“early” cancers) have a much better prognosis; the 5-year survival rate is more than 95% in Japan and more than 65% in the United States. In high-risk populations, secondary prevention measures linked to screening programs have been instituted 119. In Japan, endoscopic resection techniques have been refined and could possibly be responsible for drastic reductions in mortality rates in the presence of steady incidence rates. This hypothesis, however, has not been tested in clinical trials.
Stomach cancer survival rate
Survival rates can give you an idea of what percentage of people with the same type and stage of stomach cancer are still alive a certain amount of time usually 5 years after they were diagnosed. Survival rates can’t tell you how long you will live, but they may help give you a better understanding of how likely it is that your treatment will be successful.
Keep in mind that survival rates are estimates and are often based on previous outcomes of large numbers of people who had a specific cancer, but they can’t predict what will happen in any particular person’s case. These statistics can be confusing and may lead you to have more questions. Ask your doctor how these numbers might apply to you.
A relative survival rate compares people with the same type and stage of cancer to people in the overall population. For example, if the 5-year relative survival rate for a specific stage of stomach cancer is 37.9%, it means that people who have that cancer are, on average, about 37.9% as likely as people who don’t have that cancer to live for at least 5 years after being diagnosed.
The National Cancer Institute and American Cancer Society relies on information from the Surveillance, Epidemiology, and End Results (SEER) database, maintained by the National Cancer Institute, to provide survival statistics for different types of cancer 2.
The SEER (Surveillance, Epidemiology, and End Results) database tracks 5-year relative survival rates for stomach cancer (gastric cancer) in the United States, based on how far the cancer has spread. The SEER database, however, does not group cancers by AJCC TNM stages (stage 1, stage 2, stage 3, etc.). Instead, it groups cancers into localized, regional, and distant stages:
- Localized: There is no sign that the cancer has spread outside of the stomach.
- Regional: The cancer has spread outside the stomach to nearby structures or lymph nodes.
- Distant: The cancer has spread to distant parts of the body, such as the liver.
Table 2. stomach cancer 5-year relative survival rates
| SEER (Surveillance, Epidemiology, and End Results) stage | 5-year relative survival rate |
|---|---|
| Localized | 75% |
| Regional | 36% |
| Distant | 7% |
Footnotes:
- These numbers are based on people diagnosed with stomach cancer between 2014 and 2020.
- These numbers apply only to the stage of the cancer when it is first diagnosed. They do not apply later on if the cancer grows, spreads, or comes back after treatment.
- These numbers don’t take everything into account. Survival rates are grouped based on how far the cancer has spread, but your age and overall health, how well the cancer responds to treatment, and other factors can also affect your outlook.
- People now being diagnosed with stomach cancer may have a better outlook than these numbers show. Treatments improve over time, and these numbers are based on people who were diagnosed and treated at least five years earlier.
Stomach Cancer Survival Rates by Stage
Survival rates are often used by doctors as a standard way of discussing a person’s prognosis (outlook).
The 5-year survival rate refers to the percentage of patients who live at least 5 years after their cancer is diagnosed. Of course, many of these people live much longer than 5 years (and many are cured).
To get 5-year survival rates, doctors have to look at people who were treated at least 5 years ago. Improvements in treatment since then may result in a better outlook for people now being diagnosed with stomach cancer.
Survival rates are often based on previous outcomes of large numbers of people who had the disease, but they cannot predict what will happen in any particular person’s case. Many other factors may affect a person’s outlook, such as their general health, the location of the cancer in the stomach, the treatment received, and how well the cancer responds to treatment. Your doctor can tell you how these survival rates may apply to you.
The survival rates that follow come from the National Cancer Institute’s Surveillance, Epidemiology and End Results Program (SEER) database. They are based on people diagnosed with stomach cancer and treated with surgery between 1991 and 2000. Survival rates for patients not treated with surgery are likely to be lower. It is also important to note that these are observed survival rates. People with cancer can die of other things and these rates do not take that into account.
The rates below are based on the stage of the cancer at the time of diagnosis. When looking at survival rates, it’s important to understand that the stage of a cancer does not change over time, even if the cancer progresses. A cancer that comes back or spreads is still referred to by the stage it was given when it was first found and diagnosed, but more information is added to explain the current extent of the cancer.
The overall 5-year relative survival rate of all people with stomach cancer in the United States is about 29%. The 5-year relative survival rate compares the observed survival of people with stomach cancer to that expected for people without stomach cancer. Since some people may die from other causes, this is a better way to see the impact of cancer on survival.
This survival rate has improved gradually over the last 30 years. One reason the overall survival rate is poor in the United States is that most stomach cancers are diagnosed at an advanced rather than an early stage. The stage of the cancer has a major effect on a patient’s prognosis (outlook for survival).
Figure 8. New Stomach Cancer Cases, Deaths and 5-Year Relative Survival
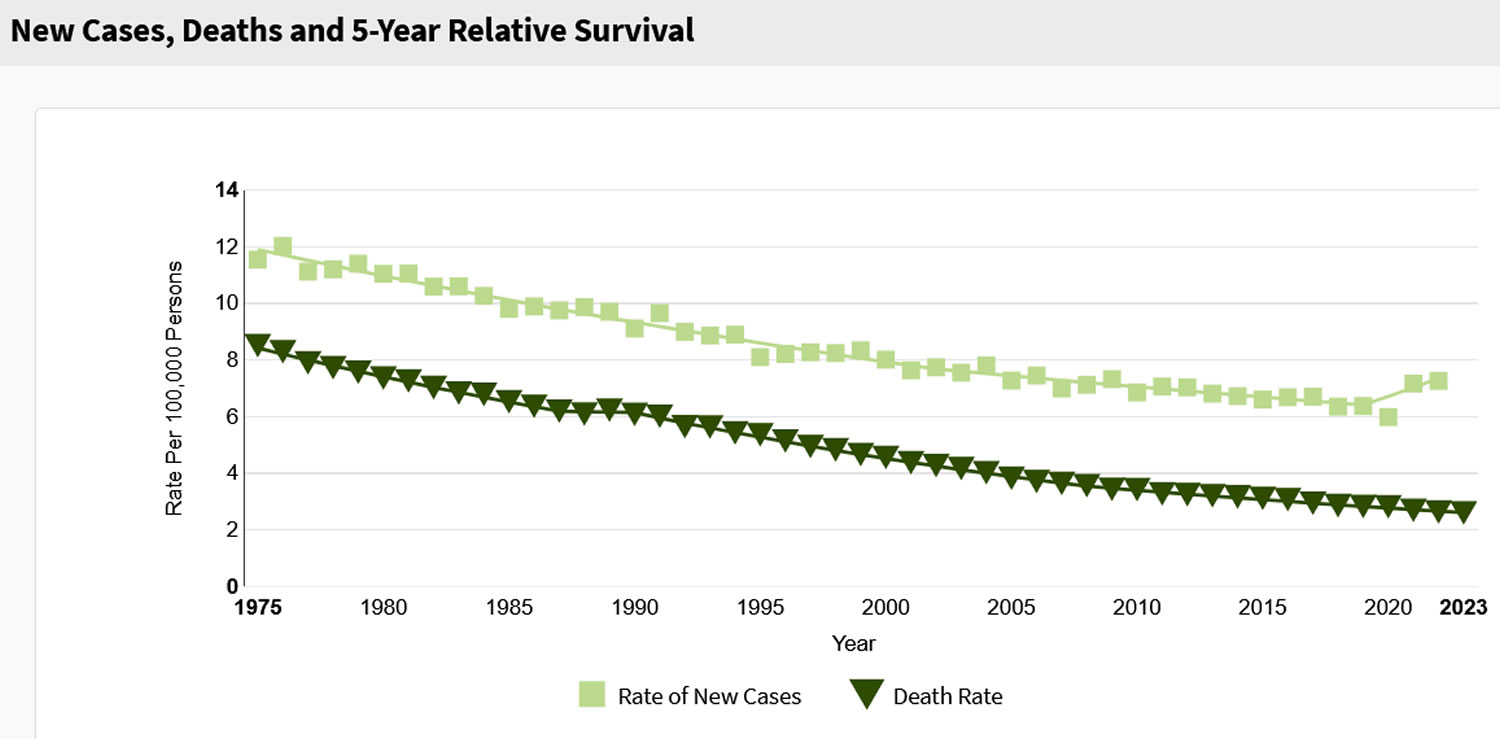
Figure 9. 5 Year Relative Survival Rate by Stomach Cancer Stage at Diagnosis
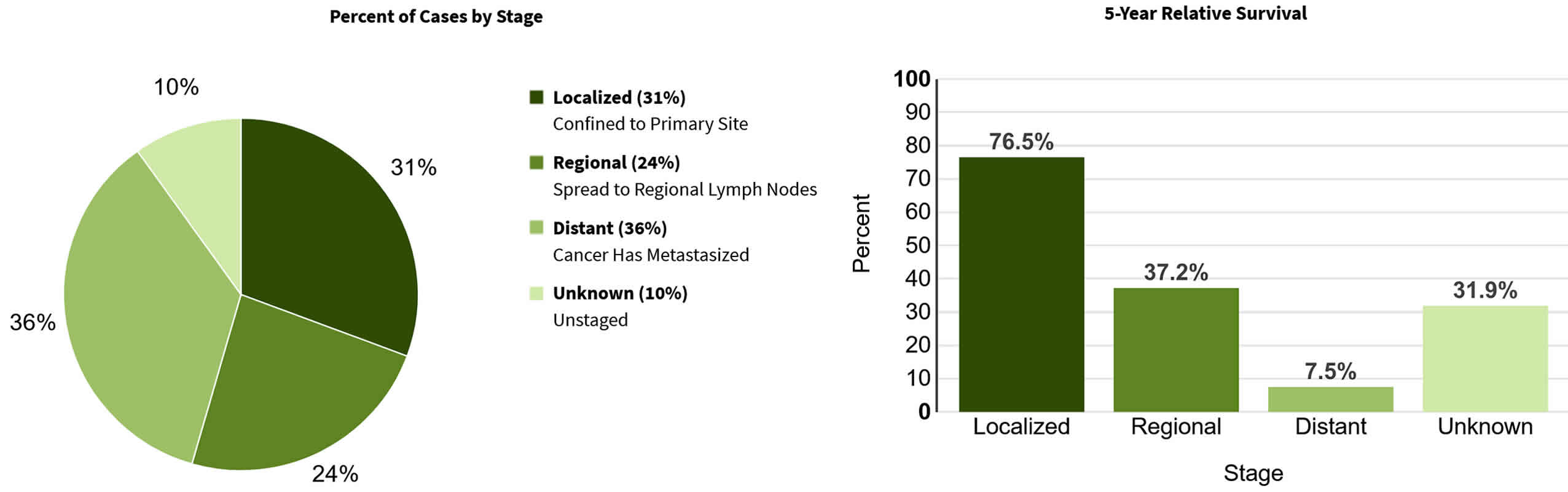
- Stomach Cancer. Medline Plus. https://medlineplus.gov/stomachcancer.html[↩][↩]
- Stomach Cancer — Cancer Stat Facts. https://seer.cancer.gov/statfacts/html/stomach.html[↩][↩]
- Key Statistics About Stomach Cancer. https://www.cancer.org/cancer/types/stomach-cancer/about/key-statistics.html[↩][↩][↩]
- Cancer of the Stomach. Surveillance Research Program, Cancer Control and Population Sciences. https://seer.cancer.gov/statfacts/html/stomach.html[↩][↩][↩][↩][↩]
- Estimates of the worldwide incidence of eighteen major cancers in 1985. Parkin DM, Pisani P, Ferlay J. Int J Cancer. 1993 Jun 19; 54(4):594-606. https://www.ncbi.nlm.nih.gov/pubmed/8514451/[↩]
- Crew KD, Neugut AI. Epidemiology of gastric cancer. World Journal of Gastroenterology : WJG. 2006;12(3):354-362. doi:10.3748/wjg.v12.i3.354. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4066052/[↩]
- Stewart BW, Kleihues P. World Cancer Report. Lyon: IARC Press; 2003.[↩]
- International variation. Parkin DM. Oncogene. 2004 Aug 23; 23(38):6329-40. https://www.ncbi.nlm.nih.gov/pubmed/15322508/[↩]
- Trends in reported incidences of gastric cancer by tumour location, from 1975 to 1989 in Japan. Liu Y, Kaneko S, Sobue T. Int J Epidemiol. 2004 Aug; 33(4):808-15. https://www.ncbi.nlm.nih.gov/pubmed/15020567/[↩]
- Stomach cancer. National Cancer Institute at the National Institutes of Health. https://www.cancer.gov/types/stomach[↩][↩]
- Blot WJ, Devesa SS, Kneller RW, Fraumeni JF. Rising incidence of adenocarcinoma of the esophagus and gastric cardia. JAMA. 1991;265:1287–1289. https://www.ncbi.nlm.nih.gov/pubmed/1995976[↩]
- Brown LM, Devesa SS. Epidemiologic trends in esophageal and gastric cancer in the United States. Surg Oncol Clin N Am. 2002;11:235–256. https://www.ncbi.nlm.nih.gov/pubmed/12424848[↩]
- Ando T, Goto Y, Maeda O, et al.: Causal role of Helicobacter pylori infection in gastric cancer. World J Gastroenterol 12 (2): 181-6, 2006. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4066024/[↩][↩]
- Aromaa A, Kosunen TU, Knekt P, et al.: Circulating anti-Helicobacter pylori immunoglobulin A antibodies and low serum pepsinogen I level are associated with increased risk of gastric cancer. Am J Epidemiol 144 (2): 142-9, 1996. https://www.ncbi.nlm.nih.gov/pubmed/8678045[↩][↩]
- MING SC, GOLDMAN H: Gastric polyps: a histogenetic classification and its relation to carcinoma. Cancer 18: 721-6, 1965. https://www.ncbi.nlm.nih.gov/pubmed/14297468[↩][↩]
- What Is Stomach Cancer? https://www.cancer.org/cancer/types/stomach-cancer/about/what-is-stomach-cancer.html[↩][↩][↩]
- Menon G, El-Nakeep S, Babiker HM. Gastric Cancer. [Updated 2024 Oct 28]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459142[↩]
- PDQ Adult Treatment Editorial Board. Gastric Cancer Treatment (PDQ®): Health Professional Version. 2025 Feb 21. In: PDQ Cancer Information Summaries [Internet]. Bethesda (MD): National Cancer Institute (US); 2002-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK65766[↩]
- Ilic M, Ilic I. Epidemiology of stomach cancer. World J Gastroenterol. 2022 Mar 28;28(12):1187-1203. doi: 10.3748/wjg.v28.i12.1187[↩]
- Vanhoefer U, Rougier P, Wilke H, Ducreux MP, Lacave AJ, Van Cutsem E, Planker M, Santos JG, Piedbois P, Paillot B, Bodenstein H, Schmoll HJ, Bleiberg H, Nordlinger B, Couvreur ML, Baron B, Wils JA. Final results of a randomized phase III trial of sequential high-dose methotrexate, fluorouracil, and doxorubicin versus etoposide, leucovorin, and fluorouracil versus infusional fluorouracil and cisplatin in advanced gastric cancer: A trial of the European Organization for Research and Treatment of Cancer Gastrointestinal Tract Cancer Cooperative Group. J Clin Oncol. 2000 Jul;18(14):2648-57. doi: 10.1200/JCO.2000.18.14.2648[↩]
- Van Cutsem E, Moiseyenko VM, Tjulandin S, Majlis A, Constenla M, Boni C, Rodrigues A, Fodor M, Chao Y, Voznyi E, Risse ML, Ajani JA; V325 Study Group. Phase III study of docetaxel and cisplatin plus fluorouracil compared with cisplatin and fluorouracil as first-line therapy for advanced gastric cancer: a report of the V325 Study Group. J Clin Oncol. 2006 Nov 1;24(31):4991-7. doi: 10.1200/JCO.2006.06.8429[↩]
- Al-Batran SE, Homann N, Pauligk C, et al. FLOT4-AIO Investigators. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): a randomised, phase 2/3 trial. Lancet. 2019 May 11;393(10184):1948-1957. doi: 10.1016/S0140-6736(18)32557-1[↩]
- Ajani JA, Ota DM, Jackson DE. Current strategies in the management of locoregional and metastatic gastric carcinoma. Cancer. 1991 Jan 1;67(1 Suppl):260-5. doi: 10.1002/1097-0142(19910101)67:1+<260::aid-cncr2820671309>3.0.co;2-2[↩]
- Yan X, Lei L, Li H, Cao M, Yang F, He S, Zhang S, Teng Y, Li Q, Xia C, Chen W. Stomach cancer burden in China: Epidemiology and prevention. Chin J Cancer Res. 2023 Apr 30;35(2):81-91. doi: 10.21147/j.issn.1000-9604.2023.02.01[↩]
- Zhu W, Dong W, Liu Y, Bai R. Stomach cancer epidemic in Chinese mainland: Current trends and future predictions. Chin Med J (Engl). 2025 Jan 20;138(2):205-212. doi: 10.1097/CM9.0000000000002993[↩]
- Ye JB, Wen JJ, Wu DL, Hu BX, Luo MQ, Lin YQ, Ning YS, Li Y. Elevated DLL3 in stomach cancer by tumor-associated macrophages enhances cancer-cell proliferation and cytokine secretion of macrophages. Gastroenterol Rep (Oxf). 2021 Nov 25;10:goab052. doi: 10.1093/gastro/goab052[↩]
- Zhan Z, Chen B, Zeng Y, Huang R, Yu J, Guo Z, Lin X. Long-term trends and projections of stomach cancer burden in China: Insights from the GBD 2021 study. PLoS One. 2025 Apr 8;20(4):e0320751. doi: 10.1371/journal.pone.0320751[↩]
- Qin Y, Tong X, Fan J, Liu Z, Zhao R, Zhang T, Suo C, Chen X, Zhao G. Global Burden and Trends in Incidence, Mortality, and Disability of Stomach Cancer From 1990 to 2017. Clin Transl Gastroenterol. 2021 Oct 5;12(10):e00406. doi: 10.14309/ctg.0000000000000406[↩]
- Zhang Z, Wang J, Song N, Shi L, Du J. The global, regional, and national burden of stomach cancer among adolescents and young adults in 204 countries and territories, 1990-2019: A population-based study. Front Public Health. 2023 Feb 24;11:1079248. doi: 10.3389/fpubh.2023.1079248[↩]
- Song Y, Liu X, Cheng W, Li H, Zhang D. The global, regional and national burden of stomach cancer and its attributable risk factors from 1990 to 2019. Sci Rep. 2022 Jul 7;12(1):11542. doi: 10.1038/s41598-022-15839-7[↩]
- Li D, Zhang D, Wang M, Hao J, Shi Y, Chu D. Pro-Inflammatory Diet as a Risk Factor for Stomach Cancer: Findings from a Multicenter Study in Central and Western China. J Multidiscip Healthc. 2024 Mar 2;17:901-912. doi: 10.2147/JMDH.S451350[↩]
- Xie X, Su J, Wang W, Wei H, Zhou Q, Su Y, Zhang L. Trends in Stomach Cancer Burden in China: A Joinpoint and APC Analysis Based on GBD 2021. J Gastroenterol Hepatol. 2025 Jun;40(6):1500-1514. doi: 10.1111/jgh.16956[↩]
- Al-Janaby T, Nahi N, Seddon A, Bagwan I, Khelwatty S, Modjtahedi H. The Combination of Afatinib With Dasatinib or Miransertib Results in Synergistic Growth Inhibition of Stomach Cancer Cells. World J Oncol. 2024 Apr;15(2):192-208. doi: 10.14740/wjon1769[↩]
- Tamura T, Wakai K, Lin Y, Tamakoshi A, Utada M, Ozasa K, Sugawara Y, Tsuji I, Ono A, Sawada N, Tsugane S, Ito H, Nagata C, Kitamura T, Naito M, Tanaka K, Shimazu T, Mizoue T, Matsuo K, Inoue M; Research Group for the Development and Evaluation of Cancer Prevention Strategies in Japan. Alcohol intake and stomach cancer risk in Japan: A pooled analysis of six cohort studies. Cancer Sci. 2022 Jan;113(1):261-276. doi: 10.1111/cas.15172[↩]
- GBD US Health Disparities Collaborators. The burden of stomach cancer mortality by county, race, and ethnicity in the USA, 2000-2019: a systematic analysis of health disparities. Lancet Reg Health Am. 2023 Aug 4;24:100547. doi: 10.1016/j.lana.2023.100547[↩]
- Aminde LN, Cobiac LJ, Phung D, Phung HN, Veerman JL. Avoidable burden of stomach cancer and potential gains in healthy life years from gradual reductions in salt consumption in Vietnam, 2019-2030: a modelling study. Public Health Nutr. 2023 Mar;26(3):586-597. doi: 10.1017/S136898002200177X[↩]
- Hemade A, Hallit S. The risk and distribution of second primary cancers according to subsite of primary stomach cancer: a retrospective cohort population-based study. Ann Med Surg (Lond). 2024 Oct 24;86(12):6944-6950. doi: 10.1097/MS9.0000000000002695[↩]
- Liu D, Liu H, Wu Y, Wang W. Time trends in stomach cancer mortality across the BRICS: an age-period-cohort analysis for the GBD 2021. Front Public Health. 2025 Feb 28;13:1506925. doi: 10.3389/fpubh.2025.1506925[↩]
- Stojanovic MM, Rancic NK, Andjelkovic Apostolovic MR, Ignjatovic AM, Ilic MV. Trends of Stomach Cancer in Central Serbia. Medicina (Kaunas). 2021 Jun 28;57(7):665. doi: 10.3390/medicina57070665[↩]
- Collatuzzo G, Pelucchi C, Negri E, López-Carrillo L, Tsugane S, Hidaka A, Shigueaki Hamada G, Hernández-Ramírez RU, López-Cervantes M, Malekzadeh R, Pourfarzi F, Mu L, Zhang ZF, Lunet N, La Vecchia C, Boffetta P. Exploring the interactions between Helicobacter pylori (Hp) infection and other risk factors of gastric cancer: A pooled analysis in the Stomach cancer Pooling (StoP) Project. Int J Cancer . 2021;149:1228–1238. doi: 10.1002/ijc.33678[↩]
- Karimi P, Islami F, Anandasabapathy S, Freedman ND, Kamangar F. Gastric cancer: descriptive epidemiology, risk factors, screening, and prevention. Cancer Epidemiol Biomarkers Prev . 2014;23:700–713. doi: 10.1158/1055-9965.EPI-13-1057[↩]
- Sitarz R, Skierucha M, Mielko J, Offerhaus GJA, Maciejewski R, Polkowski WP. Gastric cancer: epidemiology, prevention, classification, and treatment. Cancer Manag Res . 2018;10:239–248. doi: 10.2147/CMAR.S149619[↩]
- Deng W, Jin L, Zhuo H, Vasiliou V, Zhang Y. Alcohol consumption and risk of stomach cancer: A meta-analysis. Chem Biol Interact . 2021;336:109365. doi: 10.1016/j.cbi.2021.109365[↩]
- Oncogene. https://www.genome.gov/genetics-glossary/Oncogene[↩]
- Cooper GM. The Cell: A Molecular Approach. 2nd edition. Sunderland (MA): Sinauer Associates; 2000. Tumor Suppressor Genes. Available from: https://www.ncbi.nlm.nih.gov/books/NBK9894[↩]
- Utsunomiya J, Maki T, Iwama T, et al.: Gastric lesion of familial polyposis coli. Cancer 34 (3): 745-54, 1974. https://www.ncbi.nlm.nih.gov/pubmed/4852134[↩]
- Aarnio M, Salovaara R, Aaltonen LA, et al.: Features of gastric cancer in hereditary non-polyposis colorectal cancer syndrome. Int J Cancer 74 (5): 551-5, 1997. https://www.ncbi.nlm.nih.gov/pubmed/9355980[↩]
- Kurtz RC, Sherlock P: The diagnosis of gastric cancer. Semin Oncol 12 (1): 11-8, 1985. https://www.ncbi.nlm.nih.gov/pubmed/3975641[↩]
- Boeing H: Epidemiological research in stomach cancer: progress over the last ten years. J Cancer Res Clin Oncol 117 (2): 133-43, 1991. https://www.ncbi.nlm.nih.gov/pubmed/2036128[↩]
- Pisters PWT, Kelsen DP, Tepper JE: Cancer of the stomach. In: DeVita VT Jr, Hellman S, Rosenberg SA, eds.: Cancer: Principles and Practice of Oncology. Vols. 1 & 2. 8th ed. Philadelphia, Pa: Lippincott Williams & Wilkins, 2008, pp 1043-1079.[↩][↩][↩][↩]
- [↩]
- Crew KD, Neugut AI: Epidemiology of gastric cancer. World J Gastroenterol 12 (3): 354-62, 2006. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4066052/[↩]
- Parsonnet J, Hansen S, Rodriguez L, et al.: Helicobacter pylori infection and gastric lymphoma. N Engl J Med 330 (18): 1267-71, 1994. https://www.ncbi.nlm.nih.gov/pubmed/8145781[↩]
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans: A review of human carcinogens–Part B: biological agents. Volume 100. Lyon, France: IARC Press, 2011.[↩]
- Bouvard V, Baan R, Straif K, et al.: A review of human carcinogens–Part B: biological agents. Lancet Oncol 10 (4): 321-2, 2009. https://www.ncbi.nlm.nih.gov/pubmed/19350698[↩]
- Hansson LE, Nyrén O, Hsing AW, et al.: The risk of stomach cancer in patients with gastric or duodenal ulcer disease. N Engl J Med 335 (4): 242-9, 1996. http://www.nejm.org/doi/full/10.1056/NEJM199607253350404[↩]
- Ladeiras-Lopes R, Pereira AK, Nogueira A, et al.: Smoking and gastric cancer: systematic review and meta-analysis of cohort studies. Cancer Causes Control 19 (7): 689-701, 2008. https://www.ncbi.nlm.nih.gov/pubmed/18293090[↩][↩]
- González CA, Pera G, Agudo A, et al.: Smoking and the risk of gastric cancer in the European Prospective Investigation Into Cancer and Nutrition (EPIC). Int J Cancer 107 (4): 629-34, 2003. https://www.ncbi.nlm.nih.gov/pubmed/14520702[↩]
- La Torre G, Chiaradia G, Gianfagna F, et al.: Smoking status and gastric cancer risk: an updated meta-analysis of case-control studies published in the past ten years. Tumori 95 (1): 13-22, 2009 Jan-Feb. https://www.ncbi.nlm.nih.gov/pubmed/19366050[↩]
- Can Stomach Cancer Be Prevented ? American Cancer Society. https://www.cancer.org/cancer/stomach-cancer/causes-risks-prevention/prevention.html[↩]
- The Health Consequences of Smoking: A Report of the Surgeon General. Atlanta, Ga: U.S. Department of Health and Human Services, CDC, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2004. https://www.cdc.gov/tobacco/data_statistics/sgr/2004/index.htm[↩]
- Fuccio L, Zagari RM, Eusebi LH, et al.: Meta-analysis: can Helicobacter pylori eradication treatment reduce the risk for gastric cancer? Ann Intern Med 151 (2): 121-8, 2009. https://www.ncbi.nlm.nih.gov/pubmed/19620164[↩]
- Ma JL, Zhang L, Brown LM, et al.: Fifteen-year effects of Helicobacter pylori, garlic, and vitamin treatments on gastric cancer incidence and mortality. J Natl Cancer Inst 104 (6): 488-92, 2012. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3309129/[↩]
- Buiatti E, Palli D, Decarli A, et al.: A case-control study of gastric cancer and diet in Italy: II. Association with nutrients. Int J Cancer 45 (5): 896-901, 1990. https://www.ncbi.nlm.nih.gov/pubmed/2335393[↩]
- ACS Guidelines on Nutrition and Physical Activity for Cancer Prevention. The American Cancer Society. https://www.cancer.org/healthy/eat-healthy-get-active/acs-guidelines-nutrition-physical-activity-cancer-prevention.html[↩]
- Blot WJ, Li JY, Taylor PR, et al.: Nutrition intervention trials in Linxian, China: supplementation with specific vitamin/mineral combinations, cancer incidence, and disease-specific mortality in the general population. J Natl Cancer Inst 85 (18): 1483-92, 1993. https://www.ncbi.nlm.nih.gov/pubmed/8360931[↩]
- Li H, Li HQ, Wang Y, et al.: An intervention study to prevent gastric cancer by micro-selenium and large dose of allitridum. Chin Med J (Engl) 117 (8): 1155-60, 2004. https://www.ncbi.nlm.nih.gov/pubmed/15361287[↩]
- Plummer M, Vivas J, Lopez G, et al.: Chemoprevention of precancerous gastric lesions with antioxidant vitamin supplementation: a randomized trial in a high-risk population. J Natl Cancer Inst 99 (2): 137-46, 2007. https://www.ncbi.nlm.nih.gov/pubmed/17227997[↩]
- Taylor PR: Prevention of gastric cancer: a miss. J Natl Cancer Inst 99 (2): 101-3, 2007. https://www.ncbi.nlm.nih.gov/pubmed/17227989[↩]
- Malila N, Taylor PR, Virtanen MJ, et al.: Effects of alpha-tocopherol and beta-carotene supplementation on gastric cancer incidence in male smokers (ATBC Study, Finland). Cancer Causes Control 13 (7): 617-23, 2002. https://www.ncbi.nlm.nih.gov/pubmed/12296509[↩]
- Correa P, Fontham ET, Bravo JC, et al.: Chemoprevention of gastric dysplasia: randomized trial of antioxidant supplements and anti-helicobacter pylori therapy. J Natl Cancer Inst 92 (23): 1881-8, 2000. https://www.ncbi.nlm.nih.gov/pubmed/11106679[↩]
- Bjelakovic G, Nikolova D, Simonetti RG, et al.: Antioxidant supplements for preventing gastrointestinal cancers. Cochrane Database Syst Rev (3): CD004183, 2008. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD004183.pub3/full[↩]
- Bjelakovic G, Nikolova D, Simonetti RG, Gluud C. Antioxidant supplements for preventing gastrointestinal cancers. Cochrane Database of Systematic Reviews 2008, Issue 3. Art. No.: CD004183. DOI: 10.1002/14651858.CD004183.pub3. http://onlinelibrary.wiley.com/enhanced/exportCitation/doi/10.1002/14651858.CD004183.pub3[↩]
- Stomach. In: Edge SB, Byrd DR, Compton CC, et al., eds.: AJCC Cancer Staging Manual. 7th ed. New York, NY: Springer, 2010, p 120.[↩][↩][↩][↩][↩]
- Stomach Cancer Stages. https://www.cancer.org/cancer/types/stomach-cancer/detection-diagnosis-staging/staging.html[↩]
- Green PH, O’Toole KM, Slonim D, et al.: Increasing incidence and excellent survival of patients with early gastric cancer: experience in a United States medical center. Am J Med 85 (5): 658-61, 1988. https://www.ncbi.nlm.nih.gov/pubmed/3189369[↩]
- Brennan MF, Karpeh MS Jr: Surgery for gastric cancer: the American view. Semin Oncol 23 (3): 352-9, 1996. https://www.ncbi.nlm.nih.gov/pubmed/8658219[↩][↩][↩][↩]
- Macdonald JS, Smalley SR, Benedetti J, et al.: Chemoradiotherapy after surgery compared with surgery alone for adenocarcinoma of the stomach or gastroesophageal junction. N Engl J Med 345 (10): 725-30, 2001. http://www.nejm.org/doi/full/10.1056/NEJMoa010187[↩][↩][↩][↩][↩][↩]
- Bozzetti F, Marubini E, Bonfanti G, et al.: Subtotal versus total gastrectomy for gastric cancer: five-year survival rates in a multicenter randomized Italian trial. Italian Gastrointestinal Tumor Study Group. Ann Surg 230 (2): 170-8, 1999. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1420871/[↩]
- Kelsen DP: Postoperative adjuvant chemoradiation therapy for patients with resected gastric cancer: intergroup 116. J Clin Oncol 18 (21 Suppl): 32S-4S, 2000. https://www.ncbi.nlm.nih.gov/pubmed/11060322[↩]
- Cunningham D, Allum WH, Stenning SP, et al.: Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med 355 (1): 11-20, 2006. http://www.nejm.org/doi/full/10.1056/NEJMoa055531[↩][↩][↩][↩][↩][↩]
- Kitamura K, Yamaguchi T, Sawai K, et al.: Chronologic changes in the clinicopathologic findings and survival of gastric cancer patients. J Clin Oncol 15 (12): 3471-80, 1997. https://www.ncbi.nlm.nih.gov/pubmed/9396400[↩]
- Cuschieri A, Fayers P, Fielding J, et al.: Postoperative morbidity and mortality after D1 and D2 resections for gastric cancer: preliminary results of the MRC randomised controlled surgical trial.The Surgical Cooperative Group. Lancet 347 (9007): 995-9, 1996. https://www.ncbi.nlm.nih.gov/pubmed/8606613[↩]
- Sakuramoto S, Sasako M, Yamaguchi T, et al.: Adjuvant chemotherapy for gastric cancer with S-1, an oral fluoropyrimidine. N Engl J Med 357 (18): 1810-20, 2007. http://www.nejm.org/doi/full/10.1056/NEJMoa072252[↩][↩][↩][↩]
- Bang YJ, Kim YW, Yang HK, et al.: Adjuvant capecitabine and oxaliplatin for gastric cancer after D2 gastrectomy (CLASSIC): a phase 3 open-label, randomised controlled trial. Lancet 379 (9813): 315-21, 2012. https://www.ncbi.nlm.nih.gov/pubmed/22226517[↩][↩][↩][↩]
- Ohtsu A, Shimada Y, Shirao K, et al.: Randomized phase III trial of fluorouracil alone versus fluorouracil plus cisplatin versus uracil and tegafur plus mitomycin in patients with unresectable, advanced gastric cancer: The Japan Clinical Oncology Group Study (JCOG9205). J Clin Oncol 21 (1): 54-9, 2003. https://www.ncbi.nlm.nih.gov/pubmed/12506170[↩]
- Ross P, Nicolson M, Cunningham D, et al.: Prospective randomized trial comparing mitomycin, cisplatin, and protracted venous-infusion fluorouracil (PVI 5-FU) With epirubicin, cisplatin, and PVI 5-FU in advanced esophagogastric cancer. J Clin Oncol 20 (8): 1996-2004, 2002. https://www.ncbi.nlm.nih.gov/pubmed/11956258[↩][↩]
- Cunningham D, Starling N, Rao S, et al.: Capecitabine and oxaliplatin for advanced esophagogastric cancer. N Engl J Med 358 (1): 36-46, 2008. http://www.nejm.org/doi/full/10.1056/NEJMoa073149[↩][↩]
- Vanhoefer U, Rougier P, Wilke H, et al.: Final results of a randomized phase III trial of sequential high-dose methotrexate, fluorouracil, and doxorubicin versus etoposide, leucovorin, and fluorouracil versus infusional fluorouracil and cisplatin in advanced gastric cancer: A trial of the European Organization for Research and Treatment of Cancer Gastrointestinal Tract Cancer Cooperative Group. J Clin Oncol 18 (14): 2648-57, 2000. https://www.ncbi.nlm.nih.gov/pubmed/10894863[↩][↩][↩][↩]
- Van Cutsem E, Moiseyenko VM, Tjulandin S, et al.: Phase III study of docetaxel and cisplatin plus fluorouracil compared with cisplatin and fluorouracil as first-line therapy for advanced gastric cancer: a report of the V325 Study Group. J Clin Oncol 24 (31): 4991-7, 2006. https://www.ncbi.nlm.nih.gov/pubmed/17075117[↩]
- Ajani JA, Ota DM, Jackson DE: Current strategies in the management of locoregional and metastatic gastric carcinoma. Cancer 67 (1 Suppl): 260-5, 1991. https://www.ncbi.nlm.nih.gov/pubmed/1984825[↩]
- Ell C, Hochberger J, May A, et al.: Coated and uncoated self-expanding metal stents for malignant stenosis in the upper GI tract: preliminary clinical experiences with Wallstents. Am J Gastroenterol 89 (9): 1496-500, 1994. https://www.ncbi.nlm.nih.gov/pubmed/7521573[↩]
- Murad AM, Santiago FF, Petroianu A, et al.: Modified therapy with 5-fluorouracil, doxorubicin, and methotrexate in advanced gastric cancer. Cancer 72 (1): 37-41, 1993. https://www.ncbi.nlm.nih.gov/pubmed/8508427[↩]
- Pyrhönen S, Kuitunen T, Nyandoto P, et al.: Randomised comparison of fluorouracil, epidoxorubicin and methotrexate (FEMTX) plus supportive care with supportive care alone in patients with non-resectable gastric cancer. Br J Cancer 71 (3): 587-91, 1995. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2033628/ [↩]
- Glimelius B, Ekström K, Hoffman K, et al.: Randomized comparison between chemotherapy plus best supportive care with best supportive care in advanced gastric cancer. Ann Oncol 8 (2): 163-8, 1997. https://www.ncbi.nlm.nih.gov/pubmed/9093725[↩]
- Wagner AD, Grothe W, Haerting J, et al.: Chemotherapy in advanced gastric cancer: a systematic review and meta-analysis based on aggregate data. J Clin Oncol 24 (18): 2903-9, 2006. https://www.ncbi.nlm.nih.gov/pubmed/16782930[↩]
- Webb A, Cunningham D, Scarffe JH, et al.: Randomized trial comparing epirubicin, cisplatin, and fluorouracil versus fluorouracil, doxorubicin, and methotrexate in advanced esophagogastric cancer. J Clin Oncol 15 (1): 261-7, 1997. https://www.ncbi.nlm.nih.gov/pubmed/8996151[↩][↩]
- Ajani JA, Moiseyenko VM, Tjulandin S, et al.: Clinical benefit with docetaxel plus fluorouracil and cisplatin compared with cisplatin and fluorouracil in a phase III trial of advanced gastric or gastroesophageal cancer adenocarcinoma: the V-325 Study Group. J Clin Oncol 25 (22): 3205-9, 2007. https://www.ncbi.nlm.nih.gov/pubmed/17664467[↩][↩]
- Ilson DH: Docetaxel, cisplatin, and fluorouracil in gastric cancer: does the punishment fit the crime? J Clin Oncol 25 (22): 3188-90, 2007. https://www.ncbi.nlm.nih.gov/pubmed/17664464[↩][↩]
- Bang YJ, Van Cutsem E, Feyereislova A, et al.: Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial. Lancet 376 (9742): 687-97, 2010. https://www.ncbi.nlm.nih.gov/pubmed/20728210[↩]
- Kang JH, Lee SI, Lim do H, et al.: Salvage chemotherapy for pretreated gastric cancer: a randomized phase III trial comparing chemotherapy plus best supportive care with best supportive care alone. J Clin Oncol 30 (13): 1513-8, 2012. https://www.ncbi.nlm.nih.gov/pubmed/22412140[↩][↩]
- Fuchs CS, Tomasek J, Yong CJ, et al.: Ramucirumab monotherapy for previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (REGARD): an international, randomised, multicentre, placebo-controlled, phase 3 trial. Lancet 383 (9911): 31-9, 2014. https://www.ncbi.nlm.nih.gov/pubmed/24094768[↩][↩]
- Wilke H, Muro K, Van Cutsem E, et al.: Ramucirumab plus paclitaxel versus placebo plus paclitaxel in patients with previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (RAINBOW): a double-blind, randomised phase 3 trial. Lancet Oncol 15 (11): 1224-35, 2014. https://www.ncbi.nlm.nih.gov/pubmed/25240821[↩][↩]
- Ilson DH, Saltz L, Enzinger P, et al.: Phase II trial of weekly irinotecan plus cisplatin in advanced esophageal cancer. J Clin Oncol 17 (10): 3270-5, 1999. https://www.ncbi.nlm.nih.gov/pubmed/10506629[↩]
- Beretta E, Di Bartolomeo M, Buzzoni R, et al.: Irinotecan, fluorouracil and folinic acid (FOLFIRI) as effective treatment combination for patients with advanced gastric cancer in poor clinical condition. Tumori 92 (5): 379-83, 2006 Sep-Oct. https://www.ncbi.nlm.nih.gov/pubmed/17168428[↩]
- Pozzo C, Barone C, Szanto J, et al.: Irinotecan in combination with 5-fluorouracil and folinic acid or with cisplatin in patients with advanced gastric or esophageal-gastric junction adenocarcinoma: results of a randomized phase II study. Ann Oncol 15 (12): 1773-81, 2004. https://www.ncbi.nlm.nih.gov/pubmed/15550582[↩]
- Bouché O, Raoul JL, Bonnetain F, et al.: Randomized multicenter phase II trial of a biweekly regimen of fluorouracil and leucovorin (LV5FU2), LV5FU2 plus cisplatin, or LV5FU2 plus irinotecan in patients with previously untreated metastatic gastric cancer: a Federation Francophone de Cancerologie Digestive Group Study–FFCD 9803. J Clin Oncol 22 (21): 4319-28, 2004. https://www.ncbi.nlm.nih.gov/pubmed/15514373[↩]
- Ajani JA, Baker J, Pisters PW, et al.: CPT-11 plus cisplatin in patients with advanced, untreated gastric or gastroesophageal junction carcinoma: results of a phase II study. Cancer 94 (3): 641-6, 2002. https://www.ncbi.nlm.nih.gov/pubmed/11857295[↩]
- Cavanna L, Artioli F, Codignola C, et al.: Oxaliplatin in combination with 5-fluorouracil (5-FU) and leucovorin (LV) in patients with metastatic gastric cancer (MGC). Am J Clin Oncol 29 (4): 371-5, 2006. https://www.ncbi.nlm.nih.gov/pubmed/16891864[↩]
- Siewert JR, Böttcher K, Stein HJ, et al.: Relevant prognostic factors in gastric cancer: ten-year results of the German Gastric Cancer Study. Ann Surg 228 (4): 449-61, 1998. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1191515/[↩]
- Nakamura K, Ueyama T, Yao T, et al.: Pathology and prognosis of gastric carcinoma. Findings in 10,000 patients who underwent primary gastrectomy. Cancer 70 (5): 1030-7, 1992. https://www.ncbi.nlm.nih.gov/pubmed/1515980[↩]
- Adachi Y, Yasuda K, Inomata M, et al.: Pathology and prognosis of gastric carcinoma: well versus poorly differentiated type. Cancer 89 (7): 1418-24, 2000. https://www.ncbi.nlm.nih.gov/pubmed/11013353[↩]
- Howlader N, Noone AM, Krapcho M, et al., eds.: SEER Cancer Statistics Review, 1975-2008. Bethesda, Md: National Cancer Institute, 2011. https://seer.cancer.gov/archive/csr/1975_2008/index.html[↩]
- Qiu D, Tanaka S: International comparisons of cumulative risk of stomach cancer, from Cancer Incidence in Five Continents Vol. VIII. Jpn J Clin Oncol 36 (2): 123-4, 2006. https://www.ncbi.nlm.nih.gov/pubmed/16517837[↩]
- Altekruse SF, Kosary CL, Krapcho M, et al.: SEER Cancer Statistics Review, 1975-2007. Bethesda, Md: National Cancer Institute, 2010. https://seer.cancer.gov/archive/csr/1975_2007/[↩]
- American Cancer Society: Cancer Facts and Figures 2017. Atlanta, Ga: American Cancer Society, 2017. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2017/cancer-facts-and-figures-2017.pdf[↩]
- Ferlay J, Shin HR, Bray F, et al.: GLOBOCAN 2008: Cancer Incidence and Mortality Worldwide in 2008. Lyon, France: IARC CancerBase No. 10. http://globocan.iarc.fr/Default.aspx[↩][↩]
- Howlader N, Noone AM, Krapcho M, et al., eds.: SEER Cancer Statistics Review, 1975-2012. Bethesda, Md: National Cancer Institute, 2015. https://seer.cancer.gov/archive/csr/1975_2012/[↩]
- Tan YK, Fielding JW: Early diagnosis of early gastric cancer. Eur J Gastroenterol Hepatol 18 (8): 821-9, 2006. https://www.ncbi.nlm.nih.gov/pubmed/16825897[↩]
- Stomach Cancer Survival Rates. https://www.cancer.org/cancer/types/stomach-cancer/detection-diagnosis-staging/survival-rates.html[↩]




{kind=link}