Contents
- What is Liver cancer
- Prevention of liver cancer
- Benign liver tumors
- Types of Primary Liver Cancer
- Causes of liver cancer
- Liver Cancer Risk Factors
- Gender
- Race/ethnicity
- Being infected with certain types of the hepatitis virus can cause hepatitis and increase the risk of liver cancer.
- Chronic viral hepatitis (Hepatitis B or Hepatitis C)
- Cirrhosis
- Non-alcoholic fatty liver disease
- Primary biliary cirrhosis
- Inherited metabolic diseases
- Heavy alcohol use
- Obesity
- Type 2 diabetes
- Metabolic syndrome
- Hemochromatosis
- Certain rare diseases
- Aflatoxins B1
- Vinyl chloride and thorium dioxide (Thorotrast)
- Anabolic steroids
- Arsenic
- Infection with parasites
- Tobacco use
- Factors with unclear effects on liver cancer risk
- Liver Cancer Risk Factors
- Liver cancer symptoms and signs
- Liver cancer diagnosis
- Liver Cancer Stages
- Liver cancer treatment
- Liver Cancer Treatment by Stage
- Liver Cancer Prognosis
- Liver cancer survival rates
What is Liver cancer
Cancer that starts in your liver is called liver cancer or primary liver cancer 1. Most primary liver cancer is cancer in your liver and cancer in the bile ducts in your liver. On the other hand, secondary liver cancer also called metastatic cancer is cancer that spreads to your liver from another part of your body such as from your colon cancer, lung cancer or breast cancer. Cancer that spreads to your liver is more common than cancer that begins in the liver cells (primary liver cancer).
Your liver is the largest organ inside your body. You cannot live without your liver because your liver helps your body digest food, store energy, and remove poisons.
The main functions of your liver include the following:
- To make bile to help digest fat that comes from food. Bile is a substance that helps the digestion and absorption of food. Bile is stored in a small sack below your liver called the gallbladder. The bile passes into the duodenum (first part of your small intestine) through the common bile duct. The bile duct is a tube that goes from your liver to the first part of the small intestine (duodenum).
- To store glycogen (sugar) and fat, which your body uses for energy.
- To make proteins. Your liver makes proteins including albumin. Albumin is a protein found in your blood. Albumin helps to keep the right balance of fluid between your body’s tissues and the bloodstream.
- Make blood clotting proteins (clotting factors) to clot your blood. Your liver makes substances that help your blood to clot. These substances help to control bleeding when you cut yourself.
- Makes substances your body needs. Your liver makes substances that are essential for healthy bones and tissues. It also makes cholesterol, which is an important part of cell walls.
- Breaks down harmful substances. Your liver filters and breaks down harmful substances so that your body can get rid of them in your urine or poop (feces). This includes alcohol, many drugs, and waste products from normal body processes. If your liver is not working properly, harmful substances can build up and cause problems.
Your liver lie under your right ribs just beneath your right lung. It is divided into lobes. A large right lobe and a smaller left lobe and two minor lobes, the quadrate lobe and the caudate lobe (Figure 2). Each lobe is separated into many tiny hepatic lobules, the liver’s functional units (Figure 3).
Your liver is made up mainly of cells called hepatocytes. It also is made up of other types of cells, including cells that line its blood vessels and cells that line small tubes in the liver called bile ducts. The bile ducts extend out of the liver and carry bile from the liver to the gallbladder or directly to the intestines.
These different types of cells in your liver can form several types of malignant (cancerous) and benign (non-cancerous) tumors. These tumors have different causes, are treated differently, and have a different prognosis (outlook).
The National Cancer Institute and the American Cancer Society estimate for liver cancer in the United States for 2025 are 2, 3:
- About 42,240 new cases of liver cancer. 28,220 in men and 14,020 in women.
- About 30,090 deaths from liver cancer. 19,250 men and 10,840 women.
- The rate of new cases of liver and intrahepatic bile duct cancer was 9.4 per 100,000 men and women per year. The death rate was 6.6 per 100,000 men and women per year. These rates are age-adjusted and based on 2018–2022 cases and 2019–2023 deaths.
- 5-Year Relative Survival: 22%. Relative survival is an estimate of the percentage of patients who would be expected to survive the effects of their cancer. It excludes the risk of dying from other causes. Because survival statistics are based on large groups of people, they cannot be used to predict exactly what will happen to an individual patient. No two patients are entirely alike, and treatment and responses to treatment can vary greatly.
- Percentage of All Cancer Deaths: 4.9%.
- In 2022, there were an estimated 113,557 people living with liver and intrahepatic bile duct cancer in the United States.
Approximately 1.1 percent of men and women will be diagnosed with liver and intrahepatic bile duct cancer at some point during their lifetime, based on 2018–2021 data.
Liver cancer is much more common in countries in sub-Saharan Africa and Southeast Asia than in the United States. In many of these countries liver cancer is the most common type of cancer. More than 800,000 people are diagnosed with liver cancer each year throughout the world. Worldwide, liver cancer is the sixth most common cancer and the third leading cause of cancer death, accounting for more than 700,000 deaths each year. In the United States, rates are highest in American Indian or Alaska Native individuals. Liver cancer is the sixth leading cause of cancer deaths in the United States.
Liver cancer happens when your liver cells develop changes (mutations) in their DNA. A cell’s DNA is the material that provides instructions for every chemical process in your body. DNA mutations cause changes in these instructions. One result is that cells may begin to grow out of control and eventually form a tumor — a mass of cancerous cells. Sometimes the cause of liver cancer is known, such as with chronic virus hepatitis (hepatitis B or hepatitis C infection). But sometimes liver cancer happens in people with no underlying diseases and it’s not clear what causes it.
Risk factors that increase your risk of primary liver cancer include:
- Having hepatitis B or hepatitis C. Chronic infection with the hepatitis B virus (HBV) or hepatitis C virus (HCV) increases your risk of liver cancer.
- Hepatitis B virus (HBV) infection: Hepatitis B virus (HBV) can be transmitted in blood, semen, or other body fluids. The infection can be passed from mother to child during childbirth, through sexual contact, or by sharing needles that are used to inject drugs. It can cause inflammation (swelling) of the liver that leads to cancer. Routine hepatitis B virus (HBV) vaccination in infancy is reducing the incidence of hepatitis B virus (HBV) infection. Chronic hepatitis B virus (HBV) infection is the leading cause of liver cancer in Asia and Africa.
- Hepatitis C virus (HCV) infection: Hepatitis C virus (HCV) can be transmitted in the blood. The infection can be spread by sharing needles that are used to inject drugs or, less often, through sexual contact. In the past, it was also spread during blood transfusions or organ transplants. Today, blood banks test all donated blood for hepatitis C virus (HCV), which greatly lowers the risk of getting the virus from blood transfusions. It can cause cirrhosis that may lead to liver cancer. Chronic hepatitis C virus (HCV) infection is the leading cause of liver cancer in North America, Europe, and Japan.
- Heavy alcohol use. Consuming more than a moderate amount of alcohol daily over many years can lead to irreversible liver damage and increase your risk of liver cancer. Liver cancer can also occur in heavy alcohol users who do not have cirrhosis or scarring of the liver. Heavy alcohol users who have cirrhosis are ten times more likely to develop liver cancer, compared with heavy alcohol users who do not have cirrhosis. Studies have also shown there is also an increased risk of liver cancer in people with hepatitis B virus (HBV) or hepatitis C virus (HCV) infection who use alcohol heavily.
- Cigarette smoking. Cigarette smoking has been linked to a higher risk of liver cancer. The risk increases with the number of cigarettes smoked per day and the number of years the person has smoked.
- Having cirrhosis, or scarring of the liver. This progressive and irreversible condition causes scar tissue to form in your liver and increases your chances of developing liver cancer. The scar tissue blocks the flow of blood through the liver and keeps it from working as it should. Chronic alcoholism and chronic hepatitis infections are common causes of cirrhosis. People with hepatitis C virus (HCV) related cirrhosis have a higher risk of developing liver cancer than people with cirrhosis related to hepatitis B virus (HBV) or alcohol use.
- Having hemochromatosis, an iron storage disease. Liver diseases that can increase the risk of liver cancer include hemochromatosis and Wilson’s disease (a genetic disorder caused by mutations in the ATP7B gene where the body accumulates too much copper, primarily affecting the liver and brain).
- Obesity and diabetes. People with this blood sugar disorder have a greater risk of liver cancer than those who don’t have diabetes.
- Nonalcoholic fatty liver disease (NAFLD) also known as metabolic dysfunction-associated steatotic liver disease (MASLD) is a common condition in which fat builds up in your liver. This is more common in people with excess body weight (obesity). An accumulation of fat in the liver increases the risk of liver cancer. Some people with a subtype of nonalcoholic fatty liver disease (NAFLD), known as metabolic dysfunction-associated steatohepatitis (MASH) or non-alcoholic steatohepatitis (NASH), might go on to develop cirrhosis.
- Nonalcoholic steatohepatitis (NASH): Nonalcoholic steatohepatitis (NASH) is a condition that can cause cirrhosis that may lead to liver cancer. It is the most severe form of nonalcoholic fatty liver disease (NAFLD), where there is an abnormal amount of fat in the liver. In some people, this can cause inflammation and injury to the cells of the liver. Having nonalcoholic steatohepatitis (NASH)-related cirrhosis increases the risk of developing liver cancer. Liver cancer has also been found in people with nonalcoholic steatohepatitis (NASH) who do not have cirrhosis.
- Exposure to aflatoxins. Aflatoxins are poisons produced by molds that grow on crops that are stored poorly (that have been stored in hot, humid places). Crops, such as grains and nuts, can become contaminated with aflatoxins, which can end up in foods made of these products. It is most common in sub-Saharan Africa, Southeast Asia, and China.
- Certain rare medical and genetic conditions may increase the risk of liver cancer. These conditions include the following:
- Primary biliary cirrhosis also called primary biliary cholangitis. In primary biliary cirrhosis (PBC) or primary biliary cholangitis is a chronic, autoimmune disease where the body’s immune system mistakenly attacks the small bile ducts in the liver, which can lead to cirrhosis. People with advanced primary biliary cholangitis have a high risk of liver cancer.
- Hereditary hemochromatosis. People with hereditary hemochromatosis absorb too much iron from their food. The iron settles in tissues throughout the body, including the liver. If enough iron builds up in the liver, it can lead to cirrhosis and liver cancer.
- Alpha-1 antitrypsin deficiency
- Glycogen storage disease
- Acute intermittent porphyria (AIP). Acute intermittent porphyria is a rare genetic disorder that affects the production of heme, a component of hemoglobin. It’s characterized by attacks of severe abdominal pain, neurological and psychological symptoms, and potential complications like muscle weakness, paralysis, and seizures
- Porphyria cutanea tarda
- Wilson disease
There are 3 types of primary liver cancer:
- Hepatocellular carcinoma (HCC) also called hepatocellular cancer. This is the most common type of liver cancer, about 90 percent of liver cancers in adults 4. Hepatocellular carcinoma (HCC) type of liver cancer is the third leading cause of cancer-related deaths worldwide.
- Intrahepatic cancer (IHC) also called bile duct cancer. This is bile duct cancer (cholangiocarcinoma) in your liver. It represents about 10% to 20% of all primary liver cancer cases.
- Hepatic angiosarcoma and hemangiosarcoma. This type is very rare. It represents about 1% of all primary liver cancer cases. This cancer begins in the lining of blood cells in your liver. Angiosarcoma may also affect other organs.
The 3 types of primary liver cancer cause similar symptoms. Liver cancer symptoms may include:
- Dark-colored pee or grey or pale poop
- Unexplained bruising
- Fatigue
- Fever
- Hard bump or lump on the right side of your body just below your rib cage
- Itchy skin
- Loss of appetite or unexplained weight loss
- Nausea and vomiting
- Upper abdominal pain on the right side of your body or swollen abdomen
- Yellowing of your skin and the whites of your eyes from jaundice
Unfortunately, you can have very early liver cancer without any symptoms.
To diagnose liver cancer, your doctor will ask about your symptoms and perform a physical examination. Your doctor may do the following tests:
- Angiogram. This test helps your doctor examine your liver’s blood vessels.
- Blood tests. Your doctor may do blood tests for cancer. Your doctor will also do liver function tests.
- CT scan. This test takes detailed images of your liver. It gives providers information about liver tumor size and location.
- ERCP test. Your doctor may do this test to diagnose bile cancer in your liver.
- Liver ultrasound. This test takes pictures of the inside of your liver.
- MRI scan. This test uses a large magnet, radio waves and a computer. It produces very clear images of your liver’s insides.
Your doctor may do a liver biopsy if your blood and other tests detect cancer in your liver. Liver biopsies are the most reliable way to confirm a liver cancer diagnosis.
Your treatment for liver cancer depends on the stage of your cancer and how well your liver is working. The most common treatments are surgery, heat treatment, chemotherapy, radiotherapy or liver transplantation. You might have one or more treatments. Successful liver transplants can cure liver cancer. But not everyone who needs a liver transplant can receive one. For example, they may not be healthy enough to go through a liver transplant. And it can be difficult to find a donated liver that’s a match. Note that treatment for liver cancer in children is different than treatment for adults 5.
Figure 1. Normal liver
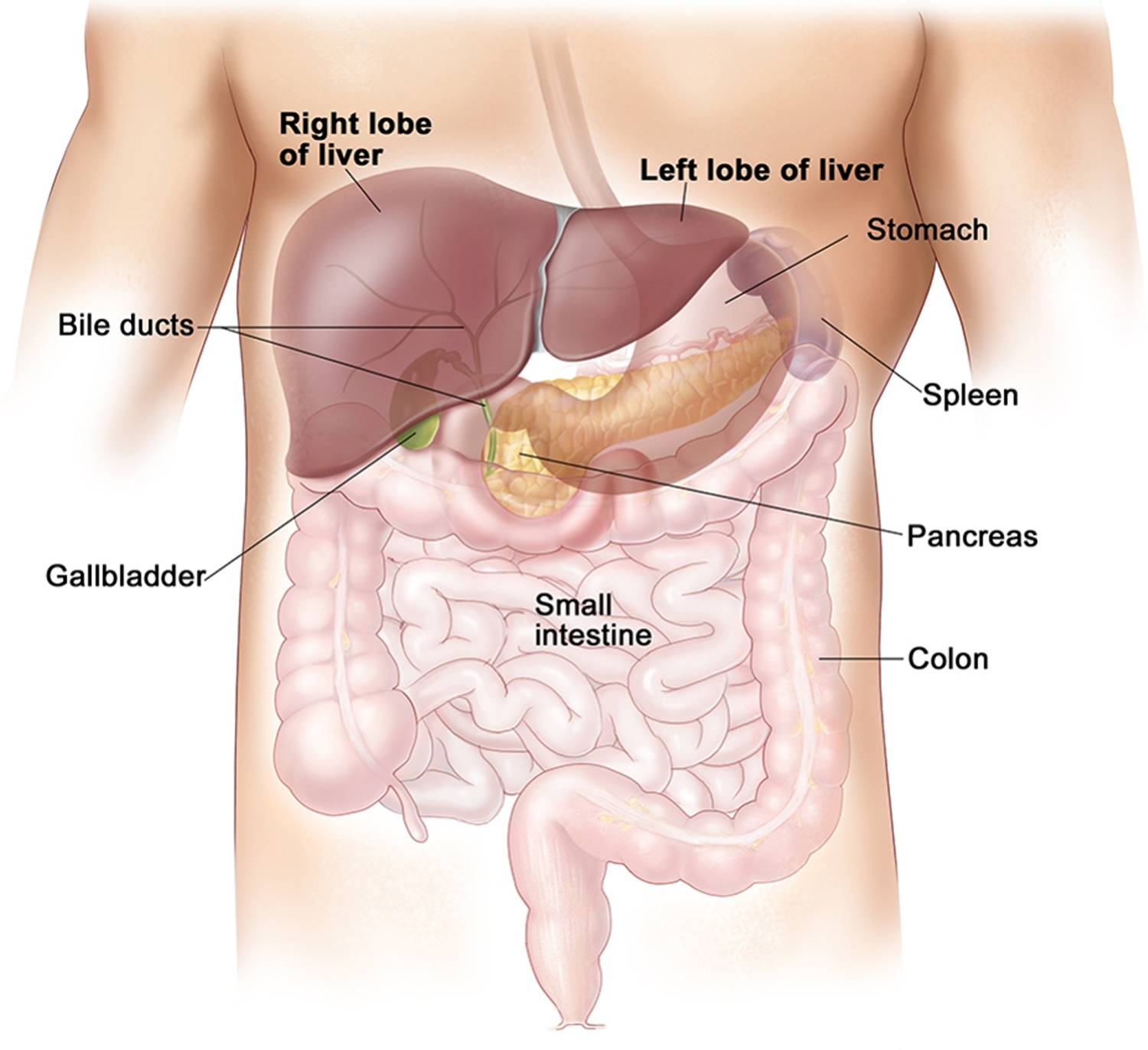
Figure 2. Liver anatomy
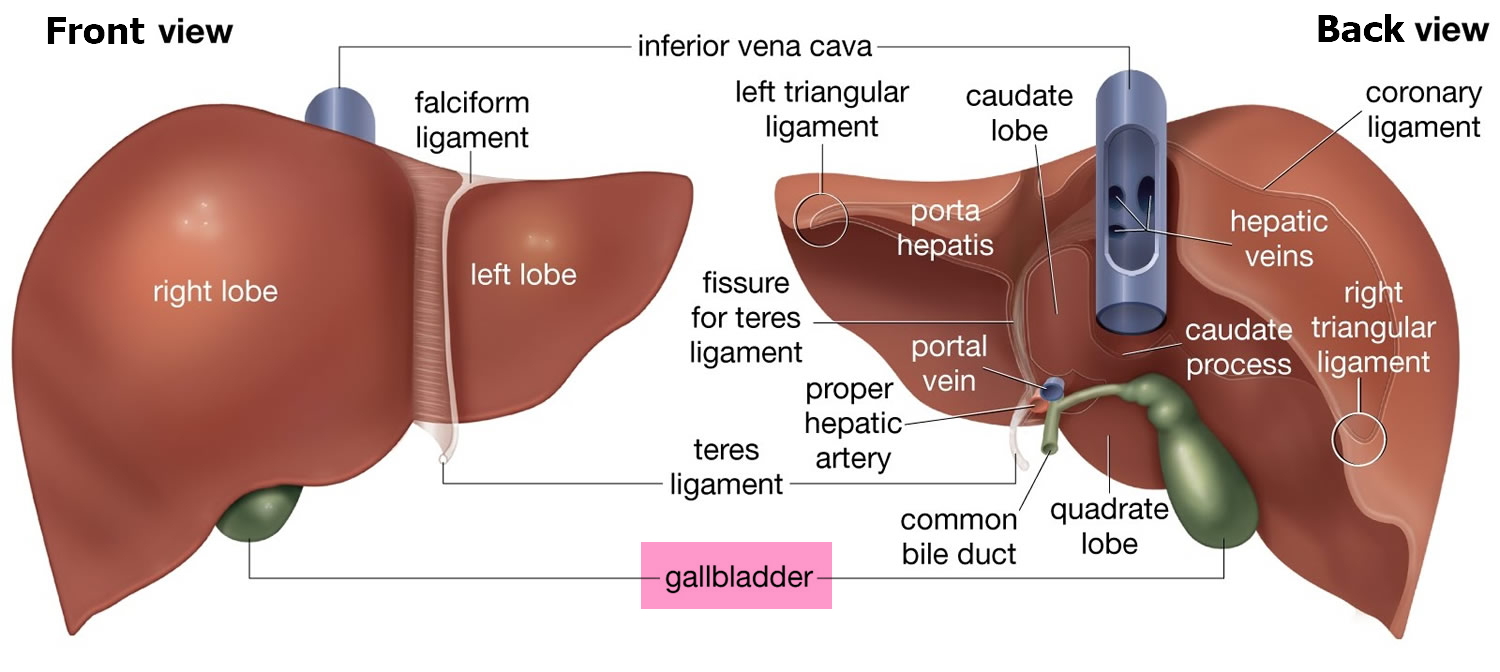
Figure 3. Liver lobule
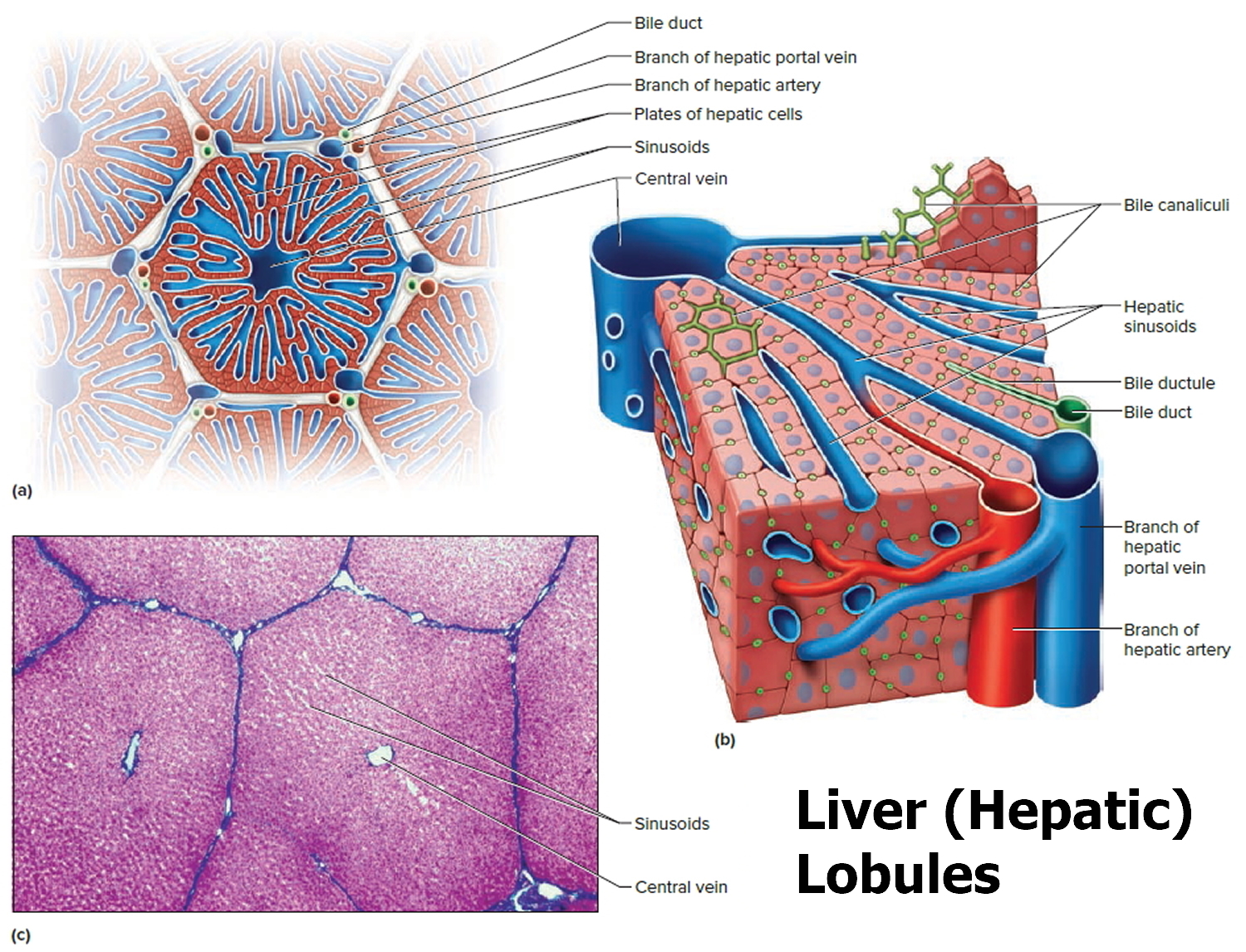
Note: (a) Cross section of a hepatic lobule. (b) Enlarged longitudinal section of a hepatic lobule. (c) Light micrograph of hepatic lobules in cross section.
Figure 4. Bile duct anatomy
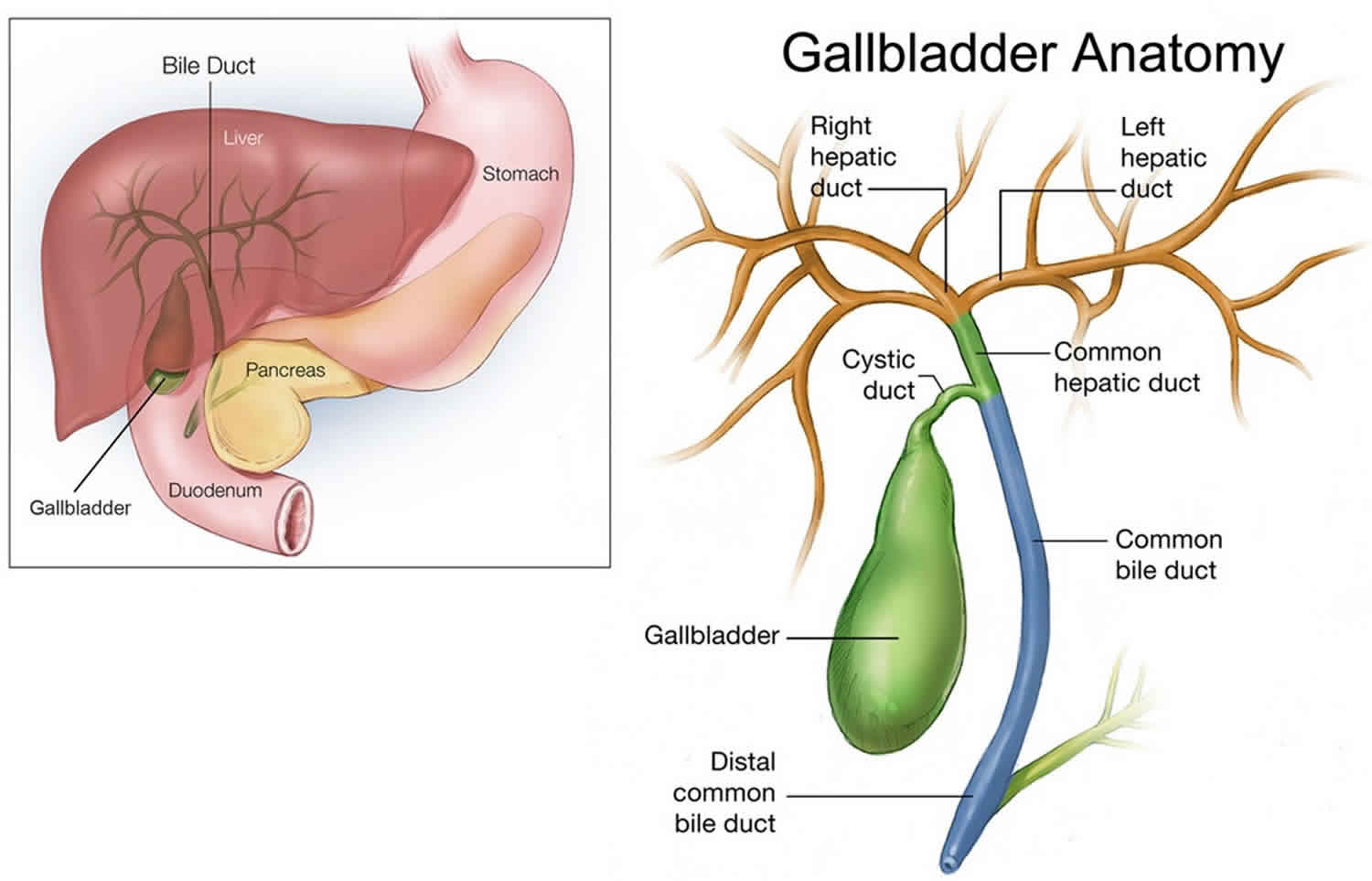
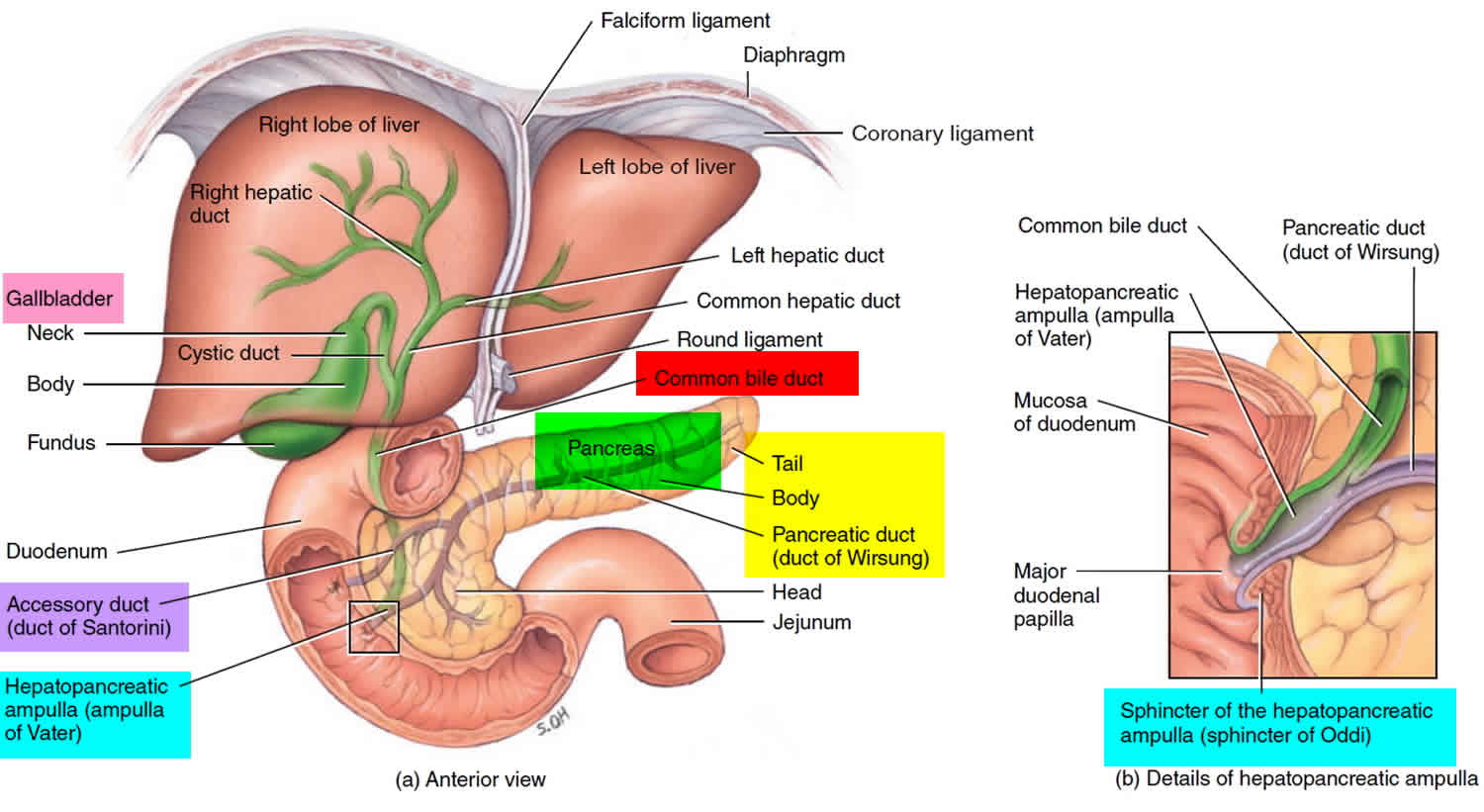
Figure 5. Relationship of the duodenum to the liver and gallbladder
How common is liver cancer?
The National Cancer Institute and the American Cancer Society estimate for liver cancer in the United States for 2025 are 2, 3:
- About 42,240 new cases of liver cancer. 28,220 in men and 14,020 in women.
- About 30,090 deaths from liver cancer. 19,250 men and 10,840 women.
- The rate of new cases of liver and intrahepatic bile duct cancer was 9.4 per 100,000 men and women per year. The death rate was 6.6 per 100,000 men and women per year. These rates are age-adjusted and based on 2018–2022 cases and 2019–2023 deaths.
- 5-Year Relative Survival: 22%. Relative survival is an estimate of the percentage of patients who would be expected to survive the effects of their cancer. It excludes the risk of dying from other causes. Because survival statistics are based on large groups of people, they cannot be used to predict exactly what will happen to an individual patient. No two patients are entirely alike, and treatment and responses to treatment can vary greatly.
- Percentage of All Cancer Deaths: 4.9%.
- In 2022, there were an estimated 113,557 people living with liver and intrahepatic bile duct cancer in the United States.
Liver cancer incidence has more than tripled since 1980. However, rates in young adults have recently begun to decline. Liver cancer death rates have increased by almost 3% per year since 2000. Liver cancer is seen more often in men than in women.
Approximately 1.1 percent of men and women will be diagnosed with liver and intrahepatic bile duct cancer at some point during their lifetime, based on 2018–2021 data.
Liver cancer is much more common in countries in sub-Saharan Africa and Southeast Asia than in the United States. In many of these countries liver cancer is the most common type of cancer. More than 800,000 people are diagnosed with liver cancer each year throughout the world. Worldwide, liver cancer is the sixth most common cancer and the third leading cause of cancer death, accounting for more than 700,000 deaths each year. In the United States, rates are highest in American Indian or Alaska Native individuals. Liver cancer is the sixth leading cause of cancer deaths in the United States.
Where is liver cancer more common?
Liver cancer is much more common in countries in sub-Saharan Africa and Southeast Asia than in the US 6. In many of these countries it is the most common type of cancer. More than 700,000 people are diagnosed with this cancer each year throughout the world. Liver cancer is also a leading cause of cancer deaths worldwide, accounting for more than 700,000 deaths each year.
Prevention of liver cancer
The most effective way to reduce the worldwide burden of liver cancer is to prevent it from happening in the first place. Some scientists believe that vaccinations and improved treatments for hepatitis could prevent about half of liver cancer cases worldwide. Researchers are studying ways to prevent or treat hepatitis infections before they cause liver cancers. Research into developing a vaccine to prevent hepatitis C is ongoing. Progress is also being made in treating chronic hepatitis.
Avoiding and treating hepatitis infections
Worldwide, the most significant risk factor for liver cancer is chronic infection with hepatitis B virus (HBV) and hepatitis C virus (HCV). These viruses can spread from person to person through sharing contaminated needles (such as in drug use) and through unprotected sex, so some of these cancers may be prevented by not sharing needles and by using safer sex practices (such as consistent use of condoms).
A vaccine to help prevent hepatitis B virus infection has been available since the early 1980s. The US Centers for Disease Control and Prevention (CDC) recommends that all children, as well as adults at risk get this vaccine to reduce the risk of hepatitis and liver cancer.
There is no vaccine for hepatitis C virus. Preventing hepatitis C virus infection, as well as hepatitis B virus infection in people who have not been immunized, is based on understanding how these infections occur. These viruses can be spread through sharing contaminated needles (such as in drug use), unprotected sex, and through childbirth.
Blood transfusions were once a major source of hepatitis infection as well. But because blood banks in the United States test donated blood to look for these viruses, the risk of getting a hepatitis infection from a blood transfusion is extremely low.
People at high risk for hepatitis B virus (HBV) or hepatitis C virus (HCV) should be tested for these infections so they can be watched for liver disease and treated if needed.
According to the CDC, you are at risk of having hepatitis B if you:
- Have sex with someone who is infected
- Have multiple sex partners
- Have a sexually transmitted disease
- Are a man who has sex with other men
- Inject drugs
- Live with a person who has chronic hepatitis B virus
- Travel to countries where many people have hepatitis B virus
- Are exposed to blood on the job
- Get long-term hemodialysis
A baby born to a mother that is infected with hepatitis B virus is also at risk for being infected.
The CDC recommends that you get tested for hepatitis C virus if any of the following are true:
- You were born from 1945 through 1965 (this is because most of the people in the US that are infected with hepatitis C virus were born in these years)
- You ever injected drugs (even just once or a long time ago)
- You needed medicine for a blood clotting problem before 1987
- You received a blood transfusion or organ transplant before July 1992 (when blood and organs started being screened for HCV)
- You are on long-term hemodialysis
- You are infected with HIV
Treatment of chronic hepatitis C virus infection can eliminate the virus in many people.
A number of drugs are used to treat chronic hepatitis B virus infection. These drugs reduce the number of viruses in the blood and lessen liver damage. Although they do not cure the disease, they lower the risk of cirrhosis and might lower the risk of liver cancer, as well.
Limiting alcohol and tobacco use
Drinking alcohol can lead to cirrhosis, which in turn, can lead to liver cancer. Not drinking alcohol or drinking in moderation could help prevent liver cancer.
Since smoking also increases the risk of liver cancer, not smoking will also prevent some of these cancers. If you smoke, quitting will help lower your risk of this cancer, as well as many other cancers and life-threatening diseases.
Getting to and staying at a healthy weight
Avoiding obesity might be another way to help protect against liver cancer. People who are obese are more likely to have fatty liver disease and diabetes, both of which have been linked to liver cancer.
Limiting exposure to cancer-causing chemicals
Changing the way certain grains are stored in tropical and subtropical countries could reduce exposure to cancer-causing substances such as aflatoxins. Many developed countries already have regulations to prevent and monitor grain contamination.
Most developed countries also have regulations to protect consumers and workers from certain chemicals known to cause liver cancer. For example, the US Environmental Protection Agency (EPA) limits the allowable level of arsenic in drinking water in the United States. But this may continue to be a problem in areas of the world where naturally occurring arsenic commonly gets into drinking water.
Treating diseases that increase liver cancer risk
Certain inherited diseases can cause cirrhosis of the liver, increasing a person’s risk for liver cancer. Finding and treating these diseases early in life could lower this risk. For example, all children in families with hemochromatosis should be screened for the disease and treated if they have it. Treatment regularly removes small amounts of blood to lower the amount of excess iron in the body.
Benign liver tumors
Benign tumors sometimes grow large enough to cause problems, but they do not grow into nearby tissues or spread to distant parts of the body. If they need to be treated, the patient can usually be cured with surgery.
Hemangioma
The most common type of benign liver tumor, hemangiomas, start in blood vessels. Most hemangiomas of the liver cause no symptoms and do not need treatment. But some may bleed and need to be removed surgically.
Hepatic adenoma
Hepatic adenoma is a benign tumor that starts from hepatocytes (the main type of liver cell). Most cause no symptoms and do not need treatment. But some eventually cause symptoms, such as pain or a mass in the abdomen (stomach area) or blood loss. Because there is a risk that the tumor could rupture (leading to severe blood loss) and a small risk that it could eventually develop into liver cancer, most experts will usually advise surgery to remove the tumor if possible.
Using certain drugs may increase the risk of getting these tumors. Women have a higher chance of having one of these tumors if they take birth control pills, although this is rare. Men who use anabolic steroids may also develop these tumors. Adenomas may shrink when the drugs are stopped.
Focal nodular hyperplasia
Focal nodular hyperplasia is a tumor-like growth made up of several cell types (hepatocytes, bile duct cells, and connective tissue cells). Although focal nodular hyperplasia tumors are benign, it can be hard to tell them apart from true liver cancers, and doctors sometimes remove them when the diagnosis is unclear. If you have symptoms from an focal nodular hyperplasia tumor, it can be removed with surgery.
Both hepatic adenomas and focal nodular hyperplasia tumors are more common in women than in men.
Types of Primary Liver Cancer
A cancer that starts in the liver is called primary liver cancer. There is more than one kind of primary liver cancer.
Hepatocellular carcinoma (hepatocellular cancer)
This is the most common form of liver cancer in adults about 90 percent of liver cancers 4.
Hepatocellular cancer can have different growth patterns:
- Some begin as a single tumor that grows larger. Only late in the disease does it spread to other parts of the liver.
- A second type seems to start as many small cancer nodules throughout the liver, not just a single tumor. This is seen most often in people with cirrhosis (chronic liver damage) and is the most common pattern seen in the United States.
Using a microscope, doctors can distinguish several subtypes of hepatocellular cancer. Most often these subtypes do not affect treatment or prognosis (outlook). But one of these subtypes, fibrolamellar, is important to recognize. This type is rare, making up less than 1% of hepatocellular cancers 7. This type is most often seen in women younger than age 35, and often the rest of the liver is not diseased 8. This subtype generally has a better outlook than other forms of hepatocellular cancer 8.
Intrahepatic cholangiocarcinoma (bile duct cancer)
About 10% to 20% of cancers that start in the liver are intrahepatic cholangiocarcinomas 7. These cancers start in the cells that line the small bile ducts (tubes that carry bile to the gallbladder) within the liver. (Most cholangiocarcinomas actually start in the bile ducts outside the liver.)
Although the rest of this article deals mainly with hepatocellular cancers, cholangiocarcinomas are often treated the same way.
Fibrolamellar carcinoma
Fibrolamellar carcinoma (FLC) was once considered a subtype of hepatocellular carcinoma (HCC), but it’s now thought of as a separate type of liver cancer. Fibrolamellar carcinoma (FLC) is rare, and it most often develops in women younger than age 35, although it can also occur in older people. Often the rest of the liver is not diseased.
Fibrolamellar carcinoma (FLC) is more likely to be removable by surgery than hepatocellular carcinoma (HCC).
Angiosarcoma and hemangiosarcoma
These are rare cancers that begin in cells lining the blood vessels of the liver. People who have been exposed to vinyl chloride or to thorium dioxide (Thorotrast) are more likely to develop these cancers 7. Some other cases are thought to be caused by exposure to arsenic or radium, or to an inherited condition known as hereditary hemochromatosis. In about half of all cases, no likely cause can be identified.
These tumors grow quickly and are usually too widespread to be removed surgically by the time they are found. Chemotherapy and radiation therapy may help slow the disease, but these cancers are usually very hard to treat. These cancers are treated like other sarcomas.
Hepatoblastoma
This is a very rare kind of cancer that develops in children, usually affects children younger than 3 years of age 7, 9.
In hepatoblastoma, the histology (how the cancer cells look under a microscope) affects the way the cancer is treated. The histology for hepatoblastoma includes:
- Well-differentiated fetal (pure fetal) histology
- Small cell undifferentiated histology hepatoblastoma and rhabdoid tumors of the liver
- Mixed epithelial and fetal histology (non–well-differentiated fetal histology, non-small cell undifferentiated histology)
About 2 out of 3 children with hepatoblastoma are treated successfully with surgery and chemotherapy, although the tumors are harder to treat if they have spread outside the liver.
Secondary liver cancer (metastatic liver cancer)
Most of the time when cancer is found in the liver it did not start there but has spread (metastasized) from somewhere else in the body, such as the pancreas, colon, stomach, breast, or lung. Because this cancer has spread from its original (primary) site, it is a secondary liver cancer. These tumors are named and treated based on their primary site (where they started). For example, cancer that started in the lung and spread to the liver is called lung cancer with spread to the liver, not liver cancer, and it is treated as lung cancer.
In the United States and Europe, secondary (metastatic) liver tumors are more common than primary liver cancer 7. The opposite is true for many areas of Asia and Africa 7.
Most of the remaining content refers only to hepatocellular carcinoma.
Causes of liver cancer
Although several risk factors for hepatocellular cancer are known (see Liver Cancer Risk Factors below), exactly how these may lead normal liver cells to become cancerous is only partially understood.
Cancers develop when a cell’s DNA is damaged. DNA is the chemical in each of our cells that makes up our genes – the instructions for how our cells function. Some genes have instructions for controlling when cells grow, divide into new cells, and die.
- Some genes that tell cells to grow and divide are called oncogenes.
- Genes that slow down cell division or cause cells to die at the right time are called tumor suppressor genes.
Cancers can be caused by DNA changes that turn on oncogenes or turn off tumor suppressor genes. Several different genes usually need to have changes for a cell to become cancerous.
Certain chemicals that cause liver cancer, such as aflatoxins, are known to damage the DNA in liver cells. For example, studies have shown that aflatoxins can damage the TP53 tumor suppressor gene, which normally works to prevent cells from growing too much. Damage to the TP53 gene can lead to increased growth of abnormal cells and formation of cancers.
Infection of liver cells with hepatitis viruses can also damage DNA. These viruses have their own DNA, which carries instructions on how to infect cells and produce more viruses. In some patients, this viral DNA can insert itself into a liver cell’s DNA, where it may affect the cell’s genes. But scientists still don’t know exactly how this might lead to cancer.
The most common type of liver cancer in adults, hepatocellular carcinoma (HCC), typically develops in people with chronic (long-lasting) liver disease caused by hepatitis virus infection or cirrhosis. Men are more likely to develop hepatocellular carcinoma (HCC) than women. People with multiple risk factors have an even higher risk.
Liver cancer clearly has many different causes, and there are undoubtedly many different genes involved in its development. It is hoped that a more complete understanding of how liver cancers develop will help doctors find ways to better prevent and treat them.
Liver Cancer Risk Factors
A risk factor is anything that affects your chance of getting a disease, such as cancer. Different cancers have different risk factors. Some risk factors, like smoking, can be changed. Others, like a person’s age or family history, can’t be changed.
But risk factors don’t tell us everything. Having a risk factor, or even several risk factors, does not mean that you will get the disease. And some people who get the disease may have few or no known risk factors.
Scientists have found several risk factors that make a person more likely to develop hepatocellular carcinoma.
Gender
Hepatocellular carcinoma is much more common in males than in females. Much of this is probably because of behaviors affecting some of the risk factors described below. The fibrolamellar subtype of hepatocellular carcinoma is more common in women.
Race/ethnicity
In the United States, Asian Americans and Pacific Islanders have the highest rates of liver cancer, followed by American Indians/Alaska Natives and Hispanics/Latinos, African Americans, and whites.
Being infected with certain types of the hepatitis virus can cause hepatitis and increase the risk of liver cancer.
- Hepatitis A
- Hepatitis B
- Hepatitis C
- Hepatitis D
- Hepatitis E
- Hepatitis G
Hepatitis is most commonly caused by the hepatitis virus. Hepatitis is a disease that causes inflammation (swelling) of the liver. Damage to the liver from hepatitis that lasts a long time can increase the risk of liver cancer.
There are six types of the hepatitis virus 10. Hepatitis A (HAV), hepatitis B (HBV), and hepatitis C (HCV) are the three most common types. These three viruses cause similar symptoms, but the ways they spread and affect the liver are different. People infected with hepatitis A virus and hepatitis E virus do not develop chronic hepatitis or cirrhosis and do not have an increased risk of liver cancer.
The Hepatitis A vaccine and the hepatitis B vaccine prevent infection with hepatitis A and hepatitis B. There is no vaccine to prevent infection with hepatitis C. If a person has had one type of hepatitis in the past, it is still possible to get the other types.
Hepatitis viruses include:
- Hepatitis A
Hepatitis A is caused by eating food or drinking water infected with hepatitis A virus. It does not lead to chronic disease. People with hepatitis A usually get better without treatment.
- Hepatitis B
Hepatitis B is caused by contact with the blood, semen, or other body fluid of a person infected with hepatitis B virus (HBV). Hepatitis B is more likely to cause symptoms, such as a flu-like illness and jaundice (a yellowing of the whites of the eyes and skin). Hepatitis B is a serious infection that may become chronic and cause scarring of the liver (cirrhosis). This may lead to liver cancer. But most people recover completely from hepatitis B virus (HBV) infection within a few months. Only a very small percentage of adults become chronic carriers and have a higher risk for liver cancer. Infants and young children who become infected have a higher risk of becoming chronic carriers. Blood banks test all donated blood for hepatitis B virus (HBV), which greatly lowers the risk of getting the virus from blood transfusions.
- Hepatitis C
Hepatitis C is caused by contact with the blood of a person infected with hepatitis C virus (HCV). Hepatitis C may range from a mild illness that lasts a few weeks to a serious, lifelong illness. Most people who have hepatitis C develop a chronic infection that may cause scarring of the liver (cirrhosis). This may lead to liver cancer. Blood banks test all donated blood for hepatitis C virus (HCV), which greatly lowers the risk of getting the virus from blood transfusions.
- Hepatitis D
Hepatitis D develops in people already infected with hepatitis B. It is caused by hepatitis D virus (HDV) and is spread through contact with infected blood or dirty needles, or by having unprotected sex with a person infected with HDV. Hepatitis D causes acute hepatitis.
- Hepatitis E
Hepatitis E is caused by hepatitis E virus (HEV). Hepatitis E can be spread through oral- anal contact or by drinking infected water. Hepatitis E is rare in the United States.
- Hepatitis G
Being infected with hepatitis G virus (HGV) has not been shown to cause liver cancer.
Worldwide, the most common risk factor for liver cancer is chronic (long-term) infection with hepatitis B virus (HBV) or hepatitis C virus (HCV). These infections lead to cirrhosis of the liver and are responsible for making liver cancer the most common cancer in many parts of the world.
In the United States, Europe and Japan infection with hepatitis C is the more common cause of hepatocellular carcinoma 11, while in Asia and Africa, hepatitis B is more common 12. People infected with both viruses have a high risk of developing chronic hepatitis, cirrhosis, and liver cancer. The risk is even higher if they are heavy drinkers (at least 6 standard drinks a day).
The annual incidence of hepatocellular carcinoma in hepatitis B virus carriers is 0.5% to 1% per year in patients without cirrhosis and 2.5% per year in patients with cirrhosis. The relative risk of hepatocellular carcinoma is 100 (i.e., carriers of hepatitis B virus are 100 times more likely to develop hepatocellular carcinoma than uninfected persons) 13, 14.
In a single, prospective, population-based study that included 12,008 patients, the presence of anti-HCV positivity conferred a twentyfold increased risk of hepatocellular carcinoma compared with persons who were anti-HCV negative 15. Hepatocellular carcinoma may occur in hepatitis C virus-infected patients with bridging fibrosis, even in the absence of overt cirrhosis 16. However, the risk is highest among patients with hepatitis C virus-related established cirrhosis, which has an incidence rate of hepatocellular carcinoma of 2% to 8% per year 17.
Hepatitis B virus (HBV) and hepatitis C virus (HCV) can spread from person to person through sharing contaminated needles (such as in drug use), unprotected sex, or childbirth. They can also be passed on through blood transfusions, although this is very rare in the United States since the start of blood product testing for these viruses. In developing countries, children sometimes contract hepatitis B infection from prolonged contact with family members who are infected.
Hepatitis B virus is more likely to cause symptoms, such as a flu-like illness and a yellowing of the eyes and skin (jaundice). But most people recover completely from hepatitis B virus infection within a few months. Only a very small percentage of adults become chronic carriers (and have a higher risk for liver cancer). Infants and small children who become infected have a higher risk of becoming chronic carriers.
Hepatitis C virus, on the other hand, is less likely to cause symptoms. But most people with hepatitis C virus develop chronic infections, which are more likely to lead to liver damage or even cancer.
Other viruses, such as the hepatitis A virus and hepatitis E virus, can also cause hepatitis. But people infected with these viruses do not develop chronic hepatitis or cirrhosis, and do not have an increased risk of liver cancer.
Cirrhosis
Cirrhosis is a disease in which liver cells become damaged and are replaced by scar tissue. People with cirrhosis have an increased risk of liver cancer. Most (but not all) people who develop liver cancer already have some evidence of cirrhosis.
There are several possible causes of cirrhosis. Most cases in the United States occur in people who abuse alcohol or have chronic hepatitis B virus (HBV) or hepatitis C virus (HCV) infections.
Non-alcoholic fatty liver disease
Non-alcoholic fatty liver disease, a condition in which people who consume little or no alcohol develop a fatty liver, is common in obese people. People with a type of this disease known as non-alcoholic steatohepatitis (NASH) might go on to develop cirrhosis.
Primary biliary cirrhosis
Some types of autoimmune diseases that affect the liver can also cause cirrhosis. For example, there is also a disease called primary biliary cirrhosis or primary biliary cholangitis. In primary biliary cirrhosis or primary biliary cholangitis, the bile ducts in the liver are damaged and even destroyed which can lead to cirrhosis. People with advanced primary biliary cirrhosis or primary biliary cholangitis have a high risk of liver cancer 18.
Inherited metabolic diseases
Certain inherited metabolic diseases can lead to cirrhosis.
People with hereditary hemochromatosis absorb too much iron from their food. The iron settles in tissues throughout the body, including the liver. If enough iron builds up in the liver, it can lead to cirrhosis and liver cancer.
Heavy alcohol use
Alcohol abuse is a leading cause of cirrhosis in the United States, which in turn is linked with an increased risk of liver cancer. However, the true incidence of hepatocellular carcinoma in alcoholic cirrhosis is unknown because most epidemiology reports on this subject were published before the identification of hepatitis C virus (HCV) infections 19.
Obesity
Being obese (very overweight) increases the risk of developing liver cancer. This is probably because it can result in fatty liver disease and cirrhosis.
Type 2 diabetes
Type 2 diabetes has been linked with an increased risk of liver cancer, usually in patients who also have other risk factors such as heavy alcohol use and/or chronic viral hepatitis. This risk may be increased because people with type 2 diabetes tend to be overweight or obese, which in turn can cause liver problems.
Metabolic syndrome
The risk factors associated with metabolic syndrome, including insulin resistance, hypertension, dyslipidemia, and obesity, have been recognized as potential causes of nonalcoholic hepatosteatosis, cirrhosis, and hepatocellular carcinoma. However, no study to date has followed a sufficiently large group of these patients for long enough to describe the incidence of hepatocellular carcinoma caused by metabolic syndrome 20.
Hemochromatosis
Hemochromatosis is a significant risk factor for hepatocellular carcinoma and has an increased relative risk twenty times that of the normal population 21.
Certain rare diseases
Diseases that increase the risk of liver cancer include:
- Tyrosinemia
- Alpha1-antitrypsin deficiency
- Porphyria cutanea tarda
- Glycogen storage diseases
- Wilson disease
Aflatoxins B1
Aflatoxin B1 is produced by fungi of the Aspergillus species and is a common contaminant of peanuts, wheat, soybeans, ground nuts, corn, and rice and vegetables in some parts of Asia and Africa. Storage in a moist, warm environment can lead to the growth of this fungus. Although this can occur almost anywhere in the world, it is more common in warmer and tropical countries. Developed countries such as the United States and those in Europe regulate the content of aflatoxins B1 in foods through testing.
Long-term exposure to these substances is a major risk factor for liver cancer. The risk is increased by three fold in people with hepatitis B or C infections 22.
Vinyl chloride and thorium dioxide (Thorotrast)
Exposure to these chemicals raises the risk of angiosarcoma of the liver. It also increases the risk of developing cholangiocarcinoma and hepatocellular cancer, but to a far lesser degree. Vinyl chloride is a chemical used in making some kinds of plastics. Thorotrast is a chemical that in the past was injected into some patients as part of certain x-ray tests. When the cancer-causing properties of these chemicals were recognized, steps were taken to eliminate them or minimize exposure to them. Thorotrast is no longer used, and exposure of workers to vinyl chloride is strictly regulated.
Anabolic steroids
Anabolic steroids are male hormones used by some athletes to increase their strength and muscle mass. Long-term anabolic steroid use can slightly increase the risk of hepatocellular cancer. Cortisone-like steroids, such as hydrocortisone, prednisone, and dexamethasone, do not carry this same risk.
Arsenic
Drinking water contaminated with naturally occurring arsenic, such as that from some wells, over a long period of time increases the risk of some types of liver cancer. This is more common in parts of East Asia, but it might also be a concern in some areas of the United States.
Infection with parasites
Infection with the parasite that causes schistosomiasis can cause liver damage and is linked to liver cancer. This parasite is not found in the US, but infection can occur in Asia, Africa, and South America.
Tobacco use
Smoking increases the risk of liver cancer. Former smokers have a lower risk than current smokers, but both groups have a higher risk than those who never smoked.
Factors with unclear effects on liver cancer risk
Birth control pills
In rare cases, birth control pills, also known as oral contraceptives, can cause benign tumors called hepatic adenomas. But it is not known if they increase the risk of hepatocellular cancer. Some of the studies that have looked at this issue have suggested there may be a link, but most of the studies were not of high quality and looked at types of pills that are no longer used. Current birth control pills use different types of estrogens, different estrogen doses, and different combinations of estrogens with other hormones. It is not known if the newer pills increase liver cancer risk.
Liver cancer symptoms and signs
Signs and symptoms of liver cancer often do not show up until the later stages of the cancer, but sometimes they may show up sooner. If you go to your doctor when you first notice symptoms, your cancer might be diagnosed earlier, when treatment is most likely to be helpful.
Some of the most common symptoms of liver cancer are 23:
- Weight loss (without trying)
- Loss of appetite
- Feeling very full after a small meal
- Nausea or vomiting
- An enlarged liver, felt as a mass under the ribs on the right side
- An enlarged spleen, felt as a mass under the ribs on the left side
- Pain in the abdomen or near the right shoulder blade
- Swelling or fluid build-up in the abdomen
- Itching
- Yellowing of the skin and eyes (jaundice)
Some other symptoms can include fever, enlarged veins on the belly that can be seen through the skin, and abnormal bruising or bleeding.
People who have chronic hepatitis or cirrhosis may feel worse than usual or just have changes in lab test results, such as alpha-fetoprotein (AFP) levels.
Some liver tumors make hormones that act on organs other than the liver. These hormones may cause:
- High blood calcium levels (hypercalcemia), which can cause nausea, confusion, constipation, weakness, or muscle problems
- Low blood sugar levels (hypoglycemia), which can cause fatigue or fainting
- Breast enlargement (gynecomastia) and/or shrinkage of the testicles in men
- High counts of red blood cells (erythrocytosis) which can cause someone to look red and flushed
- High cholesterol levels
Many of the signs and symptoms of liver cancer can also be caused by other conditions, including other liver problems. Still, if you have any of these problems, it’s important to see your doctor right away so the cause can be found and treated, if needed.
Can Liver Cancer Be Found Early?
It is often hard to find liver cancer early because signs and symptoms often do not appear until it is in its later stages. Small liver tumors are hard to detect on a physical exam because most of the liver is covered by the right rib cage. By the time a tumor can be felt, it might already be quite large.
There are no widely recommended screening tests for liver cancer in people who are not at increased risk. (Screening is testing for cancer in people without any symptoms.) But testing might be recommended for some people at higher risk.
Many patients who develop liver cancer have long-standing cirrhosis (scar tissue formation from liver cell damage). Doctors may do tests to look for liver cancer if a patient with cirrhosis gets worse for no apparent reason.
For people at higher risk of liver cancer due to cirrhosis (from any cause) or chronic hepatitis B infection (even without cirrhosis), some experts recommend screening for liver cancer with alpha-fetoprotein (AFP) blood tests and ultrasound exams every 6 to 12 months. In some studies, screening was linked to improved survival from liver cancer.
Ultrasound uses sound waves to take pictures of internal organs.
Alpha-fetoprotein is a protein that can be present at increased levels in patients with liver cancer. But looking at alpha-fetoprotein levels isn’t a perfect test for liver cancer. Many patients with early liver cancer have normal alpha-fetoprotein levels. Also, alpha-fetoprotein levels can be increased from other kinds of cancer as well as some non-cancerous liver conditions.
The American Cancer Society does not have recommendations for liver cancer screening 24.
Liver cancer diagnosis
If you have some of the signs and symptoms of liver cancer, your doctor will try to find if they are caused by liver cancer or something else.
Medical history and physical exam
Your doctor will ask about your medical history to check for risk factors and learn more about your symptoms. Your doctor will also examine you for signs of liver cancer and other health problems, probably paying special attention to your abdomen and checking your skin and the whites of your eyes looking for jaundice (a yellowish color).
If symptoms and/or the results of the physical exam suggest you might have liver cancer, other tests will probably be done. These might include imaging tests, lab tests, and other procedures.
Imaging tests
Imaging tests use x-rays, magnetic fields, or sound waves to create pictures of the inside of your body. Imaging tests are done for a number of reasons, including:
- To help find suspicious areas that might be cancerous
- To help diagnose liver cancer
- To help a doctor guide a biopsy needle into a suspicious area to take a sample
- To learn how far cancer might have spread
- To help guide certain treatments in the liver
- To help determine if treatment has been effective
- To look for a possible recurrence of the cancer
People who have (or may have) liver cancer may get one or more of the following tests.
Ultrasound
Ultrasound is often the first test used to look at the liver.
Ultrasound (ultrasonography) is the use of sound waves to create an image on a video screen. This test can show masses (tumors) growing in the liver, which then can be tested for cancer, if needed.
Computed tomography (CT)
The CT scan is an x-ray test that produces detailed cross-sectional images of your body. A CT scan of the abdomen can help identify many types of liver tumors. It can provide precise information about the size, shape, and position of any tumors in the liver or elsewhere in the abdomen, as well as nearby blood vessels. CT scans can also be used to guide a biopsy needle precisely into a suspected tumor (called a CT-guided needle biopsy). If you are found to have liver cancer, a CT of your chest may also be done to look for possible spread to the lungs.
Magnetic resonance imaging (MRI)
Like CT scans, MRI scans provide detailed images of soft tissues in the body. But MRI scans use radio waves and strong magnets instead of x-rays. The energy from the radio waves is absorbed and then released in a pattern formed by the type of body tissue and by certain diseases. A computer translates the pattern into a very detailed image of parts of the body.
MRI scans can be very helpful in looking at liver tumors. Sometimes they can tell a benign tumor from a malignant one. They can also be used to look at blood vessels in and around the liver, and can help show if liver cancer has spread to other parts of the body.
Angiography
An angiogram is an x-ray test that looks at blood vessels. Contrast medium, or dye, is injected into an artery to outline blood vessels while x-ray images are taken.
Angiography can be used to show the arteries that supply blood to a liver cancer, which can help doctors decide if a cancer can be removed and to help plan the operation. It can also be used to help guide some types of non-surgical treatment, such as embolization (see the section Embolization Therapy for Liver Cancer).
Angiography can be uncomfortable because a small catheter (a flexible hollow tube) must be put into the artery leading to the liver to inject the dye. Usually the catheter is put into an artery in your groin and threaded up into the liver artery. You have to stay very still while the catheter is in place. A local anesthetic is often used to numb the area before inserting the catheter. Then the dye is injected quickly to outline all the vessels while the x-rays are being taken.
Angiography may also be done with a CT scanner (CT angiography) or an MRI scanner (MR angiography). These techniques are often used instead of x-ray angiography because they can give information about the blood vessels in the liver without the need for a catheter in the artery. You will still need an IV line so that a contrast dye can be injected into the bloodstream during the imaging.
Bone scan
A bone scan can help look for cancer that has spread (metastasized) to bones. Doctors don’t usually order this test for people with liver cancer unless you have symptoms such as bone pain, or if there’s a chance you may be eligible for a liver transplant to treat your cancer. .
Other tests and procedures
Other types of tests may be done if your doctor thinks you might have liver cancer but the imaging test results aren’t conclusive.
Laparoscopy
Laparoscopy can be used for liver cancer:
- To help doctors confirm a diagnosis of cancer through biopsy
- To confirm the stage or (extent) of the cancer
- To help plan surgery or other treatments
Laparoscopy is usually done at an outpatient surgery center. In this procedure, a doctor inserts a thin, lighted tube with a small video camera on the end through a small incision (cut) in the front of the abdomen to look at the liver and other internal organs. (Sometimes more than one cut is made.) This procedure is done in the operating room. Usually you are under general anesthesia (in a deep sleep), although sometimes the person may just be sedated (made sleepy) and the area of the incision will be numbed.
Because the surgeon only makes a small incision to insert the tubes, you should not have much pain after surgery. You should be able to go home after you recover from the anesthesia.
Biopsy
A biopsy is the removal of a sample of tissue to see if it is cancer. Sometimes, the only way to be certain that liver cancer is present is to take a biopsy and look at it under a microscope.
But in some cases, doctors can be fairly certain that a person has liver cancer based on the results of imaging tests such as CT and MRI scans. In these cases, a biopsy may not be needed. Doctors are often concerned that sticking a needle into the tumor or otherwise disturbing it without completely removing it might help cancer cells spread to other areas. This is a major concern if a liver transplant might be an option to try to cure the cancer, as any spread of the cancer might make the person ineligible for a transplant. That is why some experts recommend that patients who could be transplant candidates only have biopsies done at the center where the transplant will be done.
If a biopsy is needed, it can be done in several ways.
- Needle biopsy: A hollow needle is placed through the skin in the abdomen and into the liver. The skin is first numbed with local anesthesia before the needle is placed. Different-sized needles may be used.
- Laparoscopic biopsy: Biopsy specimens can also be taken during laparoscopy. This lets the doctor see the surface of the liver and take samples of abnormal-appearing areas.
- Surgical biopsy: An incisional biopsy (removing a piece of the tumor) or an excisional biopsy (removing the entire tumor and some surrounding normal liver tissue) can be done during an operation.
Lab tests
Your doctor could order lab tests for a number of reasons:
- To help diagnose liver cancer
- To help determine what might have caused your liver cancer
- To learn how well your liver is working, which can affect what types of treatments you can have
- To get an idea of your general health and how well your other organs are working, which also could affect what types of treatments you can have
- To see how well treatment is working
- To look for signs that the cancer has come back after treatment
Alpha-fetoprotein (AFP) blood test
If AFP levels are very high in someone with a liver tumor, it can be a sign that liver cancer is present. But because liver cancer isn’t the only reason for high AFP levels and many patients with early liver cancer have normal levels of AFP, it isn’t very helpful in determining if a liver mass might be cancer.
This test is sometimes useful in people already diagnosed with liver cancer. The AFP level can help determine what treatment might be an option. During treatment, the test can be used to help give an idea of how well it is working, as the AFP level should go down if treatment is effective. The test can be used after treatment as well, to look for possible signs that the cancer has come back (recurred).
Other blood tests
Liver function tests (LFTs): Because liver cancer often develops in livers already damaged by hepatitis and/or cirrhosis, doctors need to know the condition of your liver before starting your treatment. A series of blood tests can measure levels of certain substances in your blood that show how well your liver is working.
If the part of your liver not affected by cancer isn’t working well, you might not be able to have surgery to try to cure the cancer, as the surgery might require removal of a large part of your liver. This is a common problem in people with liver cancer.
Blood clotting tests: The liver also makes proteins that help blood clot when you bleed. A damaged liver might not make enough of these clotting factors, which could increase your risk of bleeding. Your doctor may order blood tests such as a prothrombin time (PT) to help assess this risk.
Tests for viral hepatitis: Your doctor might order blood tests to check for hepatitis B and C.
Kidney function tests: Tests of blood urea nitrogen (BUN) and creatinine levels are often done to assess how well your kidneys are working.
Complete blood count (CBC): This test measures levels of red blood cells (which carry oxygen throughout your body), white blood cells (which fight infections), and platelets (which help the blood clot). It gives an idea of how well the bone marrow (where new blood cells are made) is functioning.
Blood chemistry tests and other tests: Blood chemistry tests check the levels of a number of substances in the blood, some of which might be affected by liver cancer. For example, liver cancer can raise blood levels of calcium, while blood glucose levels may fall. Liver cancer can also sometimes raise cholesterol levels, so this may be checked as well.
Liver Cancer Stages
After someone is diagnosed with liver cancer, doctors will try to figure out if it has spread, and if so, how far. This process is called staging. The stage of a cancer describes how much cancer is in the body. It helps determine how serious the cancer is and the best way to treat it. Doctors also use a cancer’s stage when talking about survival statistics.
Liver cancer is staged based on the results of the physical exam, imaging tests (ultrasound, CT or MRI scan, etc.) and other tests, as well as by the results of surgery if it has been done.
There are several staging systems for liver cancer, and not all doctors use the same system.
Liver cancer stages range from stage I (1) through IV (4). As a rule, the lower the number, the less the cancer has spread. A higher number, such as stage IV (stage 4), means cancer has spread more. Although each person’s cancer experience is unique, cancers with similar stages tend to have a similar outlook and are often treated in much the same way.
The American Joint Committee on Cancer (AJCC) TNM system
A staging system is a standard way for the cancer care team to sum up information about how far a cancer has spread. Doctors use staging systems to get an idea about a patient’s prognosis (outlook) and to help determine the most appropriate treatment.
The American Joint Committee on Cancer (AJCC) TNM system for staging liver cancer contains 3 key pieces of information:
- T describes the number and size of the primary tumor(s), measured in centimeters (cm), and whether the cancer has grown into nearby blood vessels or organs.
- N describes the extent of spread to nearby (regional) lymph nodes, which are bean-sized collections of immune system cells to which cancers often spread first.
- M indicates whether the cancer has metastasized (spread) to distant parts of the body.
Numbers or letters that appear after T, N, and M provide more details about each of these factors:
- The numbers 0 through 4 indicate increasing severity.
- The letter X means “cannot be assessed” because the information is not available.
Liver cancer can be staged in 2 ways:
- The clinical stage is based on the results of the physical exam, biopsies (if done), and imaging tests (ultrasound, CT or MRI scan, etc.). The clinical stage can be used, along with other factors, to help determine the best treatment options.
- If surgery is done, the pathological stage also called the surgical stage can be determined by examining tissue removed during an operation. Sometimes the pathological stage might be more advanced than the clinical stage, for example, if surgery finds cancer in places that didn’t show up on imaging tests.
T groups
- TX: Primary tumor cannot be assessed
- T0: No evidence of primary tumor
- T1: A single tumor (any size) that hasn’t grown into blood vessels
- T2: Either a single tumor (any size) that has grown into blood vessels, OR more than one tumor but no tumor is larger than 5 cm (about 2 inches) across
- T3a: More than one tumor, with at least one tumor larger than 5 cm across
- T3b: At least one tumor (any size) that has grown into a major branch of a large vein of the liver (the portal or hepatic vein)
- T4: The tumor (any size) has grown into a nearby organ (other than the gallbladder), OR the tumor is growing into the thin layer of tissue covering the liver (called the visceral peritoneum)
N groups
- NX: Regional (nearby) lymph nodes cannot be assessed.
- N0: The cancer has not spread to the regional lymph nodes.
- N1: The cancer has spread to the regional lymph nodes.
M groups
- M0: The cancer has not spread to distant lymph nodes or other organs.
- M1: The cancer has spread to distant lymph nodes or other organs. Liver cancer most often spreads to the lining of the belly (peritoneum), the lungs, and to bones.
Once the T, N, and M groups have been determined, they are then combined to give an overall stage, using Roman numerals I to IV (1 to 4).
Table 1. Stages of liver cancer (TNM classification)
| American Joint Committee on Cancer (AJCC) Stage | Stage grouping | Stage description* |
|---|---|---|
| 1A | T1a N0 M0 | A single tumor 2 cm (4/5 inch) or smaller (T1a). The cancer has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0). |
| 1B | T1b N0 M0 | A single tumor larger than 2cm (4/5 inch) that hasn’t grown into blood vessels (T1b). The cancer has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0). |
| 2 | T2 N0 M0 | Either a single tumor larger than 2 cm (4/5 inch) that has grown into blood vessels, OR more than one tumor but none larger than 5 cm (about 2 inches) across (T2). The cancer has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0). |
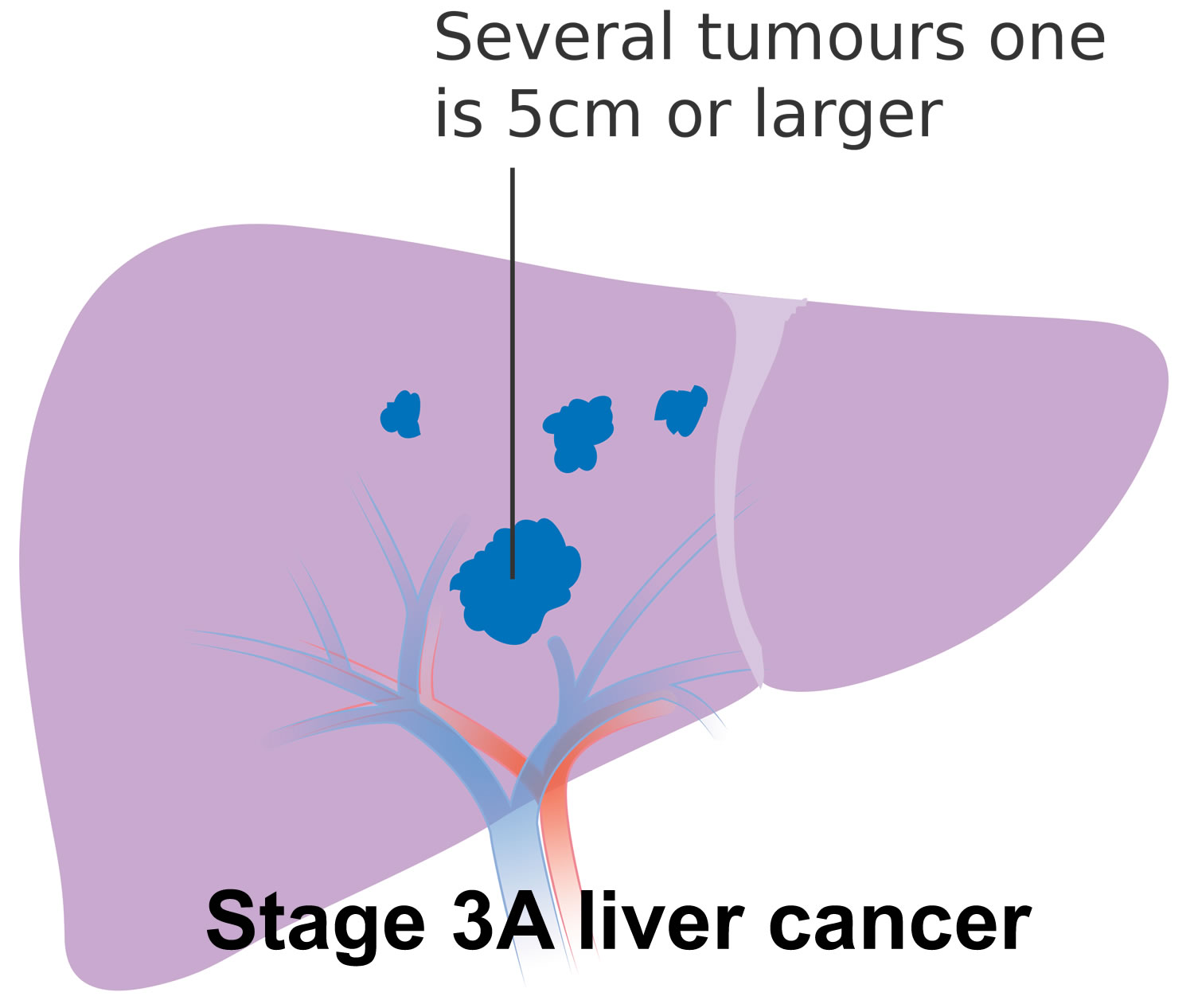
| 3A | T3 N0 M0 | More than one tumor, with at least one tumor larger than 5 cm across (T3). The cancer has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0). |
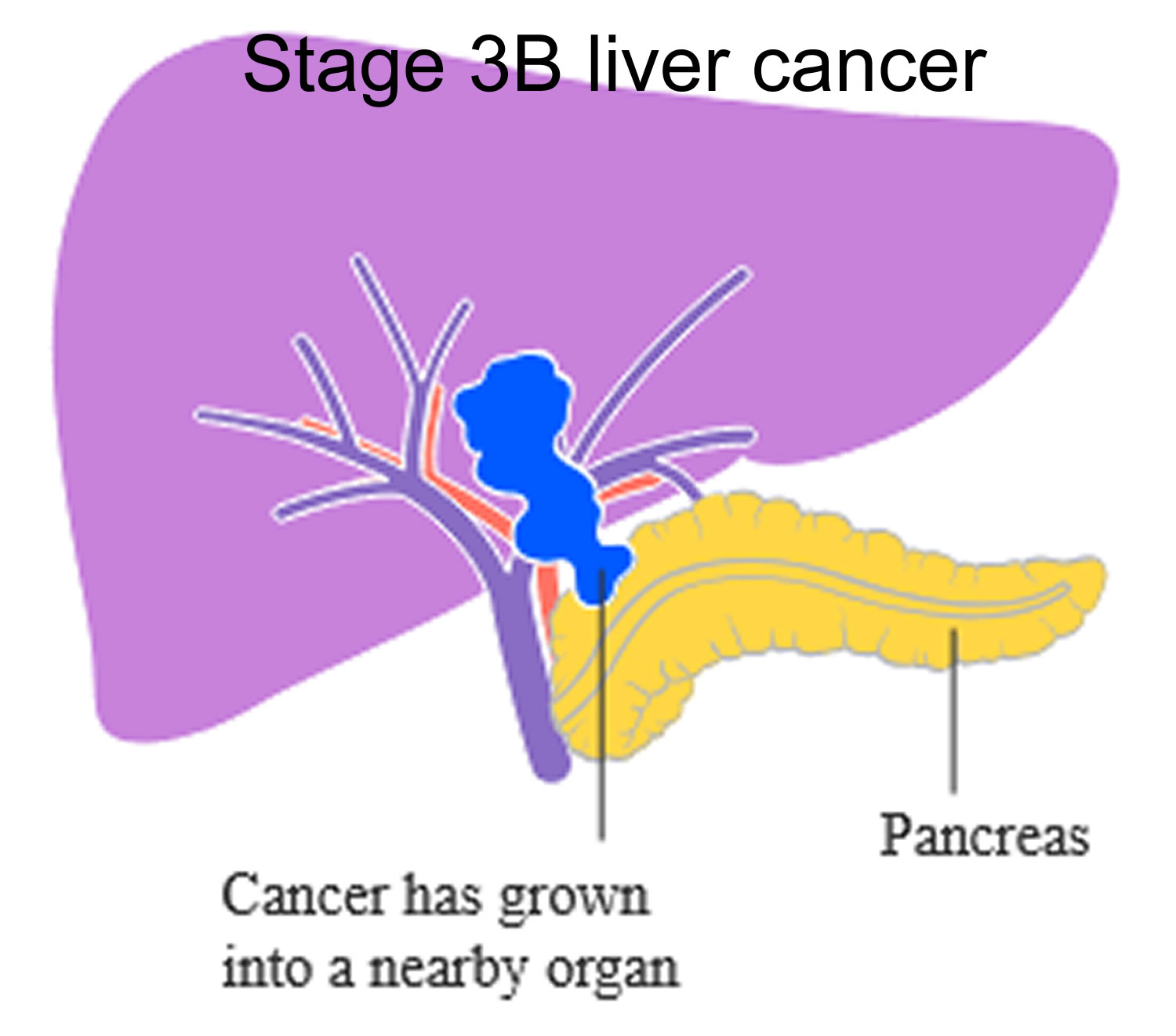
| 3B | T4 N0 M0 | At least one tumor (any size) that has grown into a major branch of a large vein of the liver (the portal or hepatic vein), or that has grown directly into a nearby organ (other than the gallbladder) (T4). The cancer has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0). |
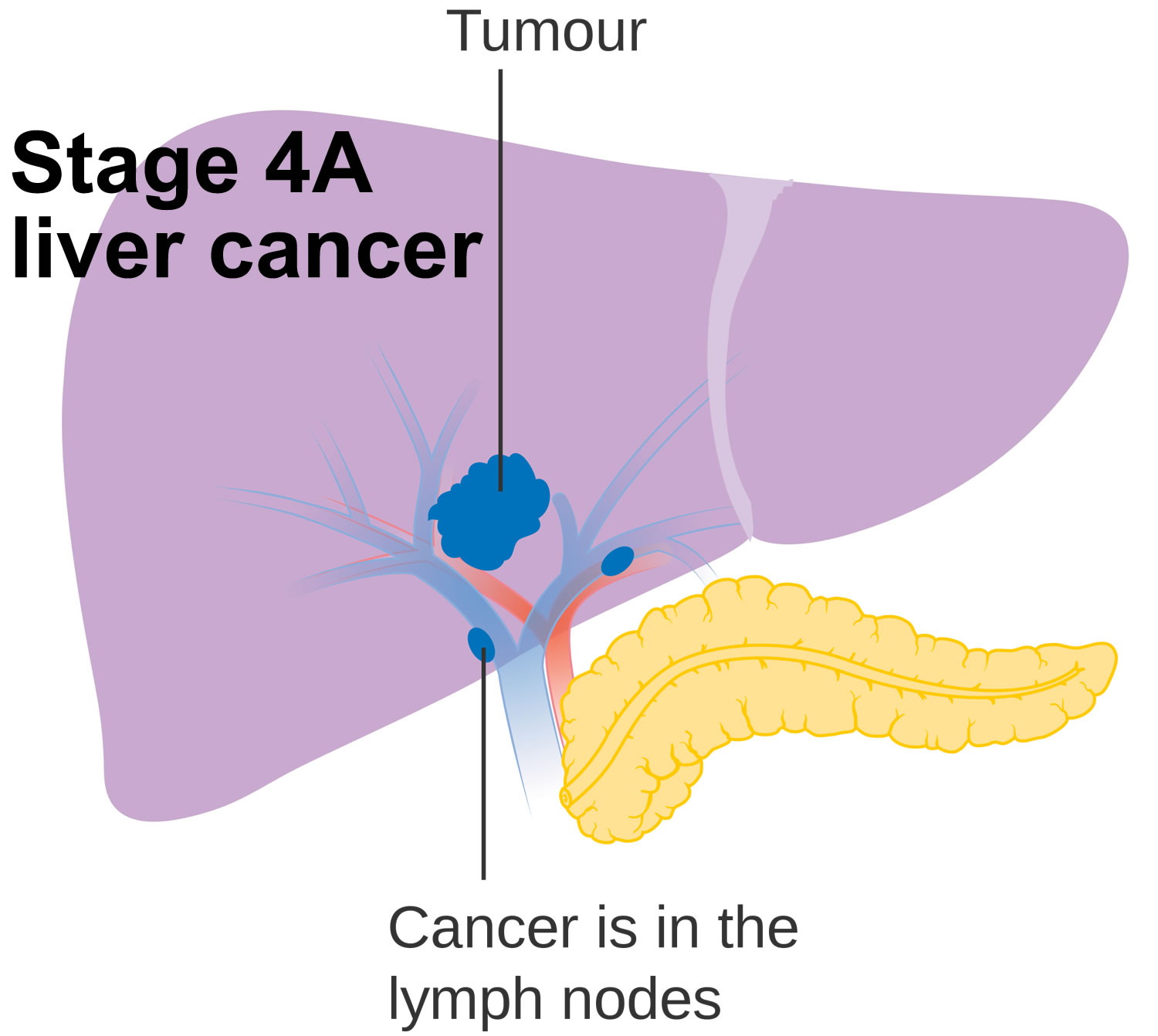
| 4A | Any T N1 M0 | A single tumor or multiple tumors of any size (Any T). The cancer has spread to nearby lymph nodes (N1) but not to distant parts of the body (M0). |
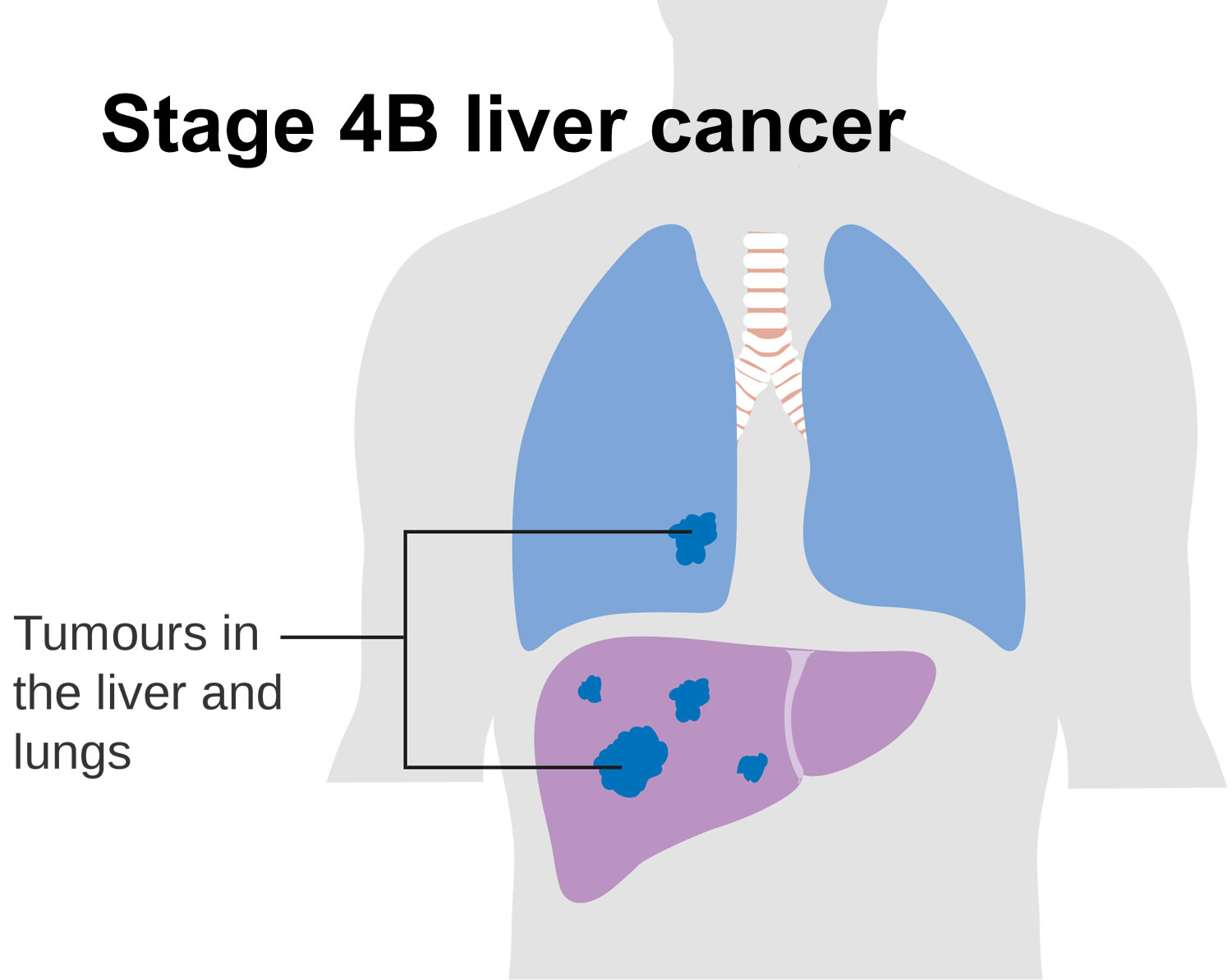
| 4B | Any T Any N M1 | A single tumor or multiple tumors of any size (any T). The cancer might or might not have spread to nearby lymph nodes (any N). The cancer has spread to distant organs such as the bones or lungs (M1). |
Footnotes: * The following additional categories are not listed on the table above:
- TX: Main tumor cannot be assessed due to lack of information.
- T0: No evidence of a primary tumor.
- NX: Regional lymph nodes cannot be assessed due to lack of information.
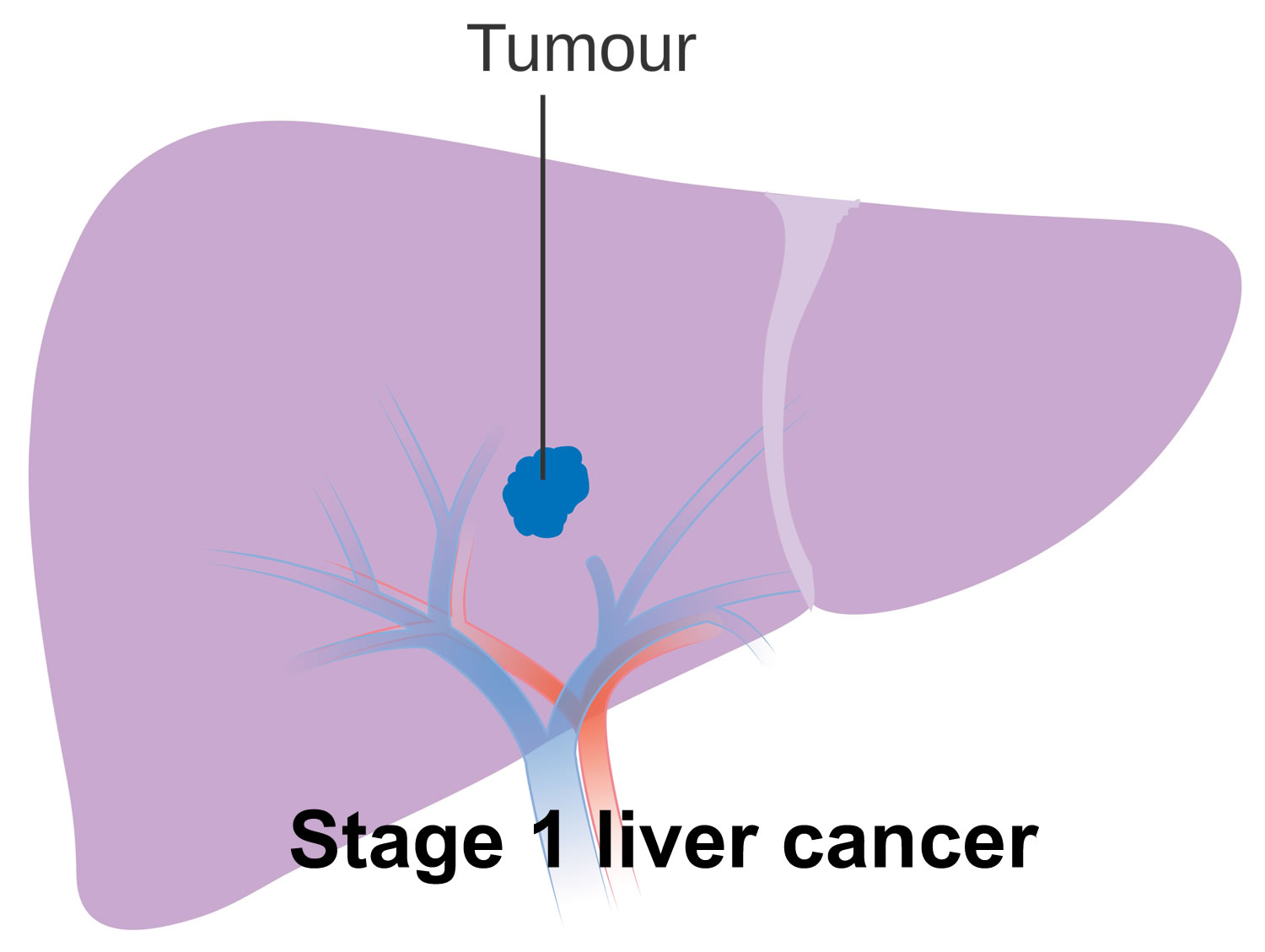
Stage 1 liver cancer
Stage 1 liver cancer has not spread to the lymph nodes or anywhere else in the body. It is divided into stage 1A and stage 1B.
- Stage 1A liver cancer means there is a single tumor in the liver that is 2cm or less, and it has not grown into the blood vessels. This is the same as T1a, N0, M0 in the TNM staging system.
- Stage 1B liver cancer means there is a single tumor that is more than 2cm, and it has not grown into the blood vessels. This is the same as T1b, N0, M0 in the TNM staging system.
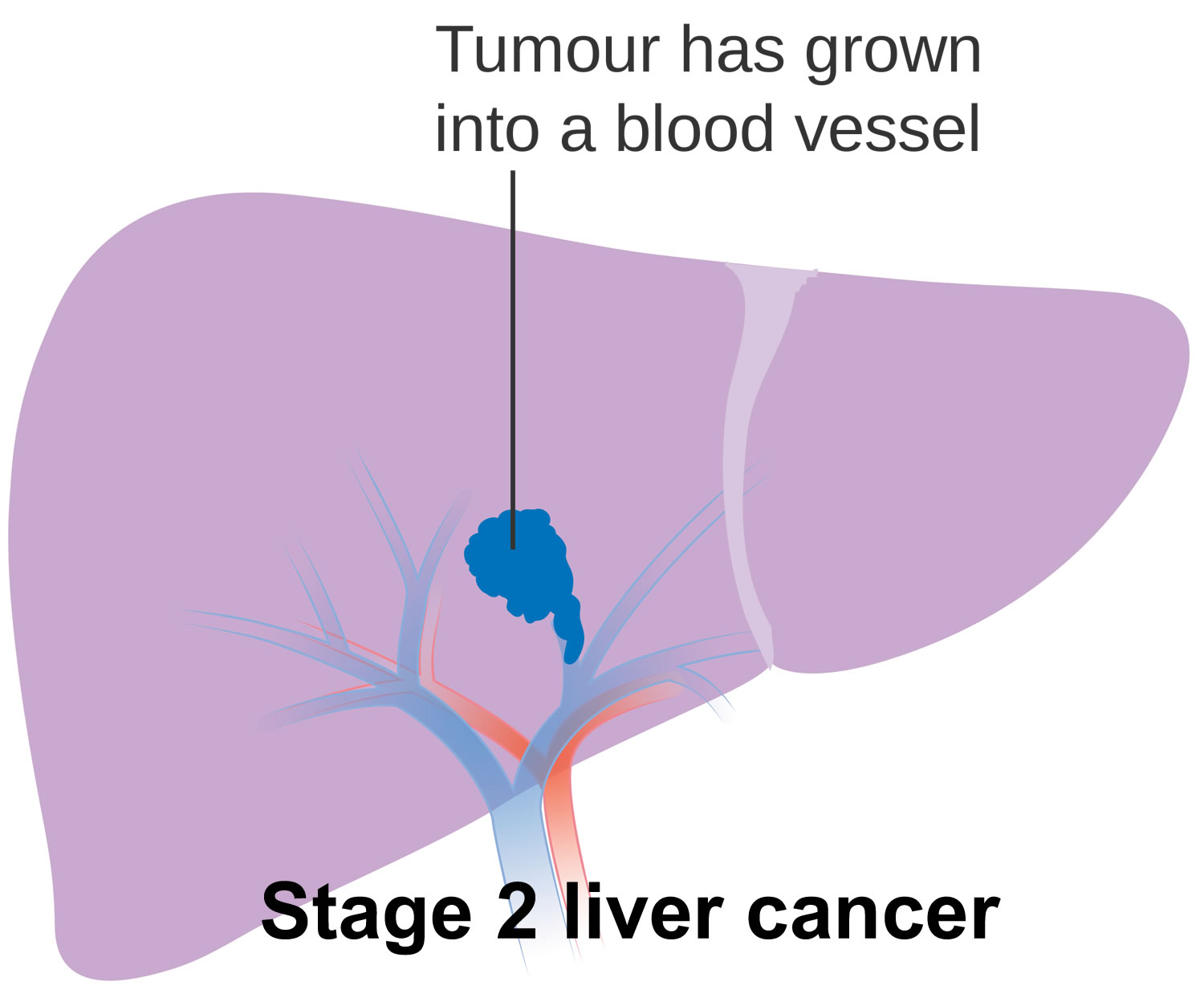
Stage 2 liver cancer
Stage 2 liver cancer has not spread to the lymph nodes or other areas of the body. In TNM staging, stage 2 liver cancer is the same as T2, N0, M0.
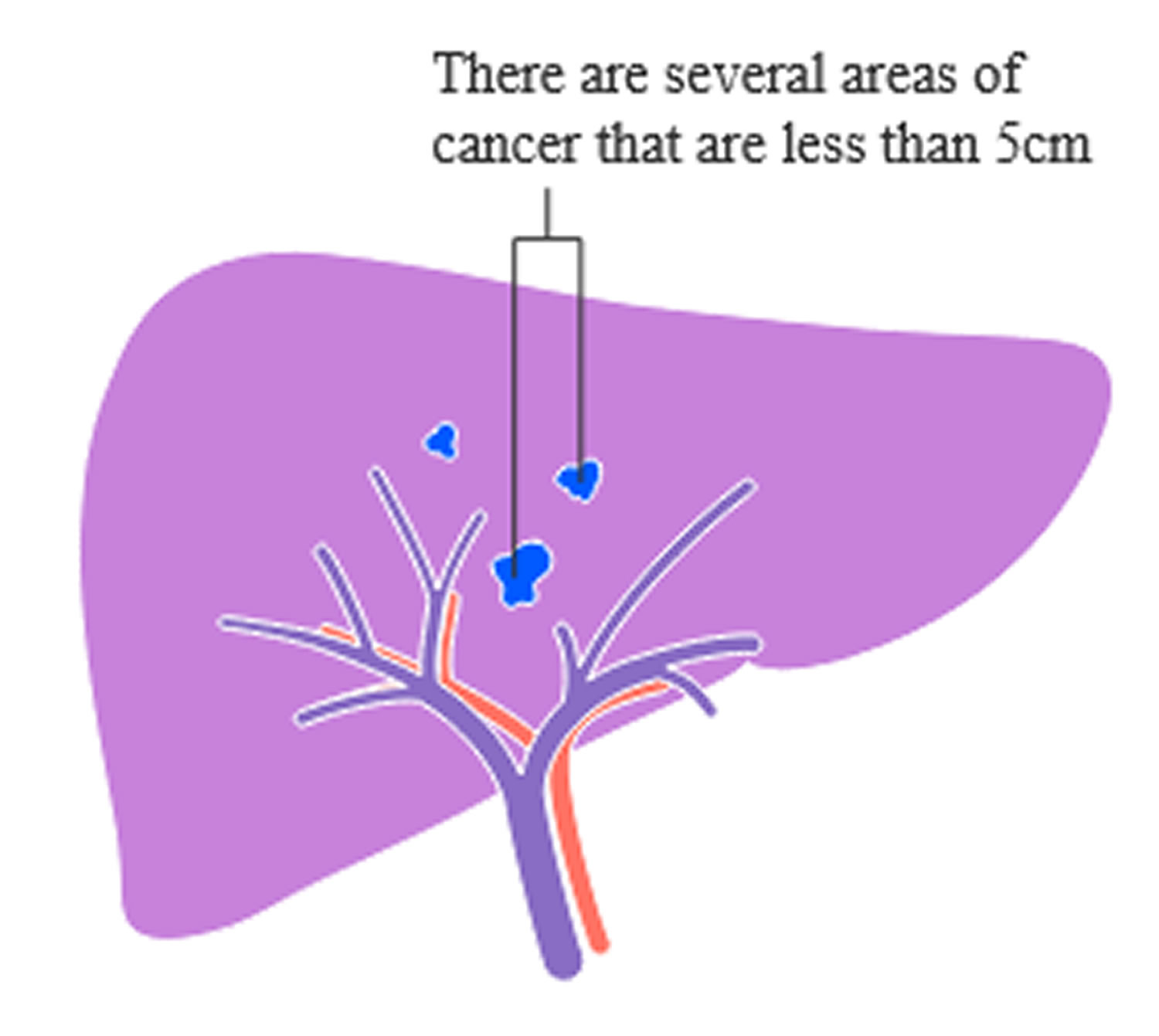
Stage 2 liver cancer means that there is a single tumor that is more than 2 cm, and it has grown into blood vessels of the liver. Or it means that there are two or more tumors in the liver and they are all less than 5cm.
Stage 3 liver cancer
Stage 3 liver cancer hasn’t spread to the lymph nodes or any distant body parts. It is divided into stage 3A and stage 3B.
- Stage 3A liver cancer means there are two or more tumors. At least one of them is larger than 5cm. Stage 3A liver cancer is the same as T3, N0, M0 in the TNM staging system.
- Stage 3B liver cancer means the cancer has grown into one of the main blood vessels of the liver (the portal vein or hepatic vein). Or it has spread into organs close to the liver (not including the gallbladder), or through the lining that wraps around the internal organs of the abdomen (the visceral peritoneum). Stage 3B liver cancer is the same as T4, N0, M0 in the TNM staging system.

Stage 4 liver cancer
Stage 4 liver cancer is divided into 2 further stages – stage 4A and 4B.
- Stage 4A liver cancer means the cancer is any size and there may be more than one tumor. It may have grown into blood vessels or the organs around the liver. It has spread to lymph nodes but not to distant parts of the body. In TNM staging, stage 4A liver cancer is the same as Any T, N1, M0.
- Stage 4B liver cancer means the cancer is any size and there may be more than one tumour. It may have grown into blood vessels or the organs around the liver. It may or may not have spread into lymph nodes. It has spread to another part of the body such as the lungs or bones. In TNM staging, stage 4B liver cancer is the same as Any T, Any N, M1.
Other liver cancer staging systems
The staging systems for most types of cancer depend only on the extent of the cancer, but liver cancer is complicated by the fact that most patients have damage to the rest of their liver along with the cancer. This also affects treatment options and prognosis.
Although the TNM system defines the extent of liver cancer in some detail, it does not take liver function into account. Several other staging systems have been developed that include both of these factors:
- The Barcelona Clinic Liver Cancer (BCLC) system
- The Cancer of the Liver Italian Program (CLIP) system
- The Okuda system
These staging systems have not been compared against each other. Some are used more than others in different parts of the world, but at this time there is no single staging system that all doctors use. If you have questions about the stage of your cancer or which system your doctor uses, be sure to ask.
Child-Pugh score (cirrhosis staging system)
The Child-Pugh score is a measure of liver function, especially in people with cirrhosis. Many people with liver cancer also have cirrhosis, and in order to treat the cancer, doctors need to know how well the liver is working. The Child-Pugh score system looks at 5 factors, the first 3 of which are results of blood tests:
- Blood levels of bilirubin (the substance that can cause yellowing of the skin and eyes)
- Blood levels of albumin (a major protein normally made by the liver)
- The prothrombin time (measures how well the liver is making blood clotting factors)
- Whether there is fluid in the abdomen (ascites)
- Whether the liver disease is affecting brain function (hepatic encephalopathy)
Based on these factors, liver function is divided into 3 classes.
- If all these factors are normal, then liver function is called class A.
- Mild abnormalities are class B.
- Severe abnormalities are class C.
People with liver cancer and class C cirrhosis are often too sick for surgery or other major cancer treatments.
The Child-Pugh score is actually part of the Barcelona Clinic Liver Cancer (BCLC) system and Cancer of the Liver Italian Program (CLIP) staging systems mentioned previously.
Liver cancer classification
Formal staging systems (such as those described before) can often help doctors determine a patient’s prognosis (outlook). But for treatment purposes, doctors often classify liver cancers more simply, based on whether or not they can be entirely cut out (resected). Resectable is the medical term meaning “able to be removed by surgery”.
Potentially resectable or transplantable cancers
These cancers can be completely removed by surgery or treated with a liver transplant and the patient is healthy enough for surgery. This would include most stage 1 and some stage 2 cancers in the TNM system, in patients who do not have cirrhosis or other serious medical problems. Only a small portion of people with liver cancer have resectable tumors.
Unresectable liver cancers
Cancers that have not spread to the lymph nodes or distant organs but cannot be completely removed by surgery are classified as unresectable. This includes cancers that have spread throughout the liver or can’t be removed safely because they are close to the area where the liver meets the main arteries, veins, and bile ducts.
Inoperable (unresectable) with only local disease
The liver cancer is small enough and in the right place to be removed but you aren’t healthy enough for surgery. Often this is because the non-cancerous part of your liver is not healthy (because of cirrhosis, for example), and if the cancer is removed, there might not be enough liver tissue left for it to function properly. It could also mean that you have serious medical problems that make surgery unsafe.
Advanced (metastatic) liver cancers
Cancers that have spread to lymph nodes or other organs are classified as advanced. These would include stages 4A and 4B cancers in the TNM system. Most advanced liver cancers cannot be treated with surgery.
Liver cancer treatment
After your liver cancer is diagnosed and staged, your cancer care team will discuss your treatment options with you.
In creating your treatment plan, important factors to consider include the stage (extent) of the cancer and the health of the rest of your liver. But you and your cancer care team will also want to take into account the possible side effects of treatment, your overall health, and the chances of curing the disease, extending life, or relieving symptoms. Based on these factors, your treatment options may include:
- Surgery (partial hepatectomy or liver transplant)
- Tumor ablation
- Tumor embolization
- Radiation therapy
- Targeted therapy
- Chemotherapy
Which doctors treat liver cancer?
Depending on your situation, you may have different types of doctors on your treatment team. These doctors may include:
- A surgeon: a doctor who treats diseases with surgery.
- A radiation oncologist: a doctor who treats cancer with radiation therapy.
- A medical oncologist: a doctor who treats cancer with medicines such as chemotherapy.
- A gastroenterologist: a doctor who specializes in treating diseases of the digestive system, including the liver.
Many other specialists may be involved in your care as well, including nurse practitioners, nurses, nutrition specialists, social workers, and other health professionals.
Making treatment decisions
It is important to discuss all of your treatment options, including their goals and possible side effects, with your doctors to help make the decision that best fits your needs. Some important things to consider include:
- Your age and expected life span
- Any other serious health conditions you have
- The stage (extent) of your cancer
- Whether or not surgery can remove (resect) the cancer
- The likelihood that treatment will cure the cancer (or help in some other way)
- Your feelings about the possible side effects from treatment
You may feel that you must make a decision quickly, but it’s important to give yourself time to absorb the information you have just learned. It’s also very important to ask questions if there is anything you’re not sure about.
Getting a second opinion
If time allows, you may also want to get a second opinion from another doctor or medical team. This can give you more information and help you feel more certain about the treatment plan you choose. If you aren’t sure where to go for a second opinion, ask your doctor for help.
Thinking about taking part in a clinical trial
Clinical trials are carefully controlled research studies that are done to get a closer look at promising new treatments or procedures. Clinical trials are one way to get state-of-the art cancer treatment. Sometimes they may be the only way to get access to newer treatments. They are also the best way for doctors to learn better methods to treat cancer. Still, they are not right for everyone.
If you would like to learn more about clinical trials that might be right for you, start by asking your doctor if your clinic or hospital conducts clinical trials.
Surgery
You might have tests to see if surgery is an option for you. There are 2 types of surgery for primary liver cancer:
- An operation to remove part of the liver (liver resection or partial hepatectomy)
- A liver transplant
Surgery may not be possible if the tumor is large and takes up too much of the liver, the liver is too damaged, the cancer has spread outside of the liver, or if you have other serious illnesses.
Partial hepatectomy
Partial hepatectomy is surgery to remove part of the liver. To have this surgery, people generally need to have a good liver function, good overall health, and have a single tumor that has not grown into blood vessels.
Imaging tests such as CT or MRI are done first to see if the cancer is resectable – that is, if it can be removed completely. Still, sometimes during surgery the cancer is found to be too large or has spread too far to be removed, and the surgery that was planned cannot be done.
For some people who have unresectable liver cancer, using other treatments first might shrink the tumor enough so that surgery could then be an option.
In the United States, most people with liver cancer also have cirrhosis. For someone with severe cirrhosis, removing even a small amount of normal liver tissue at the edges of a cancer might not leave enough healthy liver behind to perform important functions.
People with cirrhosis might still be eligible for surgery if there is only one tumor (that has not grown into blood vessels) and they will still have a reasonable amount of liver function left once the tumor is removed. Doctors often assess this function by assigning a Child-Pugh score (see above), which is a measure of cirrhosis based on certain lab tests and symptoms.
People in Child-Pugh class A are most likely to have enough liver function to have surgery. People in class B are less likely to be able to have surgery. Surgery is not typically an option for people in class C.
After surgery, the remaining section of liver takes over the functions of the entire liver. A healthy liver may grow back to its normal size over time.
Possible risks and side effects of surgery
Liver resection is a major, serious operation that should only be done by skilled and experienced surgeons. People with liver cancer usually have other liver problems besides the cancer. In this case, surgeons have to remove enough of the liver to get all of the cancer, but also leave enough behind for the liver to function.
- Bleeding: A lot of blood passes through the liver, and bleeding after surgery is a major concern. Also, the liver normally makes substances that help with blood clotting. Damage to the liver (both before the surgery and during the surgery) can add to potential bleeding problems.
- Infection
- Complications from anesthesia
- Blood clots
- Pneumonia
- New liver cancer: Because the remaining liver still has the underlying disease that led to the cancer, sometimes a new liver cancer can develop afterward.
Liver transplant
When it is available, a liver transplant may be the best option for some people with liver cancer. Liver transplants can be an option for those with tumors that cannot be removed with surgery, either because of the location of the tumor(s) or because the liver has too much disease for the person to tolerate removing it all.
People who have cirrhosis usually can’t have a liver resection because the rest of the liver isn’t healthy enough. In some situations, your surgeon may suggest a liver transplant if you have cirrhosis of the liver and you have:
- a single tumor no more than 5cm across
- a single tumor that is 5 to 7 cm across and has not grown for at least 6 months
- no more than 5 small tumors, each no larger than 3 cm across
- a level of alpha fetoprotein (AFP) less than 1000
In general, a liver transplant might be an option to treat people with small tumors that have not grown into nearby blood vessels. Rarely, a liver transplant can also be an option for people with cancers that can be removed completely. Possible advantages of a transplant in this setting are that the risk of getting a new liver cancer is much lower, and the new liver will function normally. But this has to be weighed against the complexity and possible long-term side effects of a liver transplant.
Unfortunately, there are only a limited number of donor livers available for transplant each year, and most of these are used for people with diseases other than liver cancer.
Most livers used for transplants come from people who have just died. But some people can get part of a liver from a living donor usually a close relative for a transplant. The liver can regenerate some of its lost function over time if part of it is removed. Still, the surgery does carry some risks for the donor.
People needing a liver transplant must wait until a liver becomes available, which often can take too long for some people with liver cancer. In many cases a person may get other treatments, such as embolization or ablation, while waiting for a liver transplant. Or doctors may suggest surgery or other treatments first and then a transplant if the cancer comes back.
Liver transplant possible risks and side effects
Like partial hepatectomy, a liver transplant is a major operation with serious risks and should only be done by skilled and experienced surgeons. Possible risks include:
- Bleeding
- Blood clots
- Complications from anesthesia
- Problems from a weakened or suppressed immune system: People who get a liver transplant need to take medicines to prevent their bodies from rejecting the new organ. These drugs have their own risks and side effects, especially the risk of getting serious infections. Suppressing the immune system might also allow any liver cancer that had spread outside of the liver to grow even faster than before. Some of the drugs used to prevent rejection can also cause high blood pressure, high cholesterol, and diabetes; can damage the bones and kidneys; and can increase the risk of getting a new cancer.
- Rejection of the new liver: After a liver transplant, regular blood tests are done to check for signs of the body rejecting the new liver. Sometimes liver biopsies are also taken to see if the new liver is being rejected and if changes are needed in the drugs that can prevent it.
Ablation Treatments
Ablation is treatment that destroys (ablates) liver tumors without having surgery to remove them. Types of ablation for liver cancer include histotripsy, radiofrequency ablation, microwave ablation, cryotherapy, and ethanol injections.
Ablation for liver tumors can often be done without surgery, so people getting this type of treatment typically do not need to stay in a hospital. Ablation might be done using an ultrasound machine or CT scan to help guide where the treatment needs to be given. Sometimes, though, to be sure the treatment is aimed at the right place, ablation is done in the operating room with either laparoscopy or a surgical incision (cut) in the skin over the belly, while the person is under general anesthesia (in a deep sleep).
Ablation techniques can be used for people with a few small liver tumors, especially when surgery is not a good option because of poor health or reduced liver function. Ablation is best used for tumors no larger than 3 cm across (a little over an inch). For slightly larger tumors (1 to 2 inches, or 3 to 5 cm across), it may be used along with embolization.
Ablation is less likely to cure liver cancer than surgery, but it can still be very helpful for some people.
Ablation treatments are also sometimes used in people waiting for a liver transplant.
Because certain types of ablation often destroy some of the normal liver tissue around the tumor, they might not be a good choice for treating tumors near major blood vessels, the diaphragm, or major bile ducts.
Heat treatment (thermal ablation)
There are different types of thermal ablation for liver cancer. You might have:
- Radiofrequency ablation (RFA)
- Microwave ablation (MWA)
These treatments use heat to destroy cancer cells. You might have thermal ablation if your cancer is very small, or if you can’t have surgery. Or you may have it to help control the cancer while you are waiting for a liver transplant.
Preparing for treatment
You may have an appointment at the pre assessment clinic about a week before your treatment. This is to prepare you for the treatment and check you are well enough to have it. You might need tests such as blood tests and an ECG to check your heart.
Tell your doctor if you’re having medicine that changes how your blood clots. This includes:
- aspirin
- clopidogrel
- arthritis medicines
- warfarin or heparin
- apixaban or rivaroxaban
- ticagrelor
Your doctor will tell you if you need to stop taking these or any other medicines for a while before your treatment.
You can’t eat for 4 to 6 hours before the ablation but you might be able to drink sips of water up to 2 hours before your appointment. Your doctor or nurse gives you written instructions about this before.
Talk to your doctor if not eating could be a problem for you. For example, if you have diabetes.
Having treatment
You go into hospital on the day of your treatment or the evening before.
A specialist doctor called an interventional radiologist carries out the procedure. Radiographers and nurses will also be with you in the room.
First you get changed into a hospital gown. You lie on your back on the x-ray table. Your doctor or nurse puts a small tube (cannula) into your arm or back of your hand. They use the cannula to give you any medicines you might need, such as antibiotics, sedation, or pain relief. Your nurse regularly checks your heart rate and blood pressure. You might have oxygen through a small plastic tube or sponge which sits just inside your nostril.
You might have radiofrequency ablation (RFA) or microwave ablation (MWA) under general anaesthetic, which means you are unconscious. Or you will have a drug that makes you very sleepy (sedation) and a local anaesthetic to numb the skin above the liver. You will also have strong painkillers during treatment.
Your radiologist uses either an ultrasound scan or a CT scan to guide a special needle through your skin into the cancer. Once it is in the correct place, the needle is heated using electrical or microwave energy. The needle heats the cancer cells and destroys them.
The time your treatment takes can vary. It can take anything from 30 minutes to a couple of hours in total.
After treatment
Your doctor removes the needle when the treatment has finished and covers the area with a dressing. You go back to the ward where your nurse will monitor you. Let them know if you feel sick or have any pain.
You usually have to stay in bed for a few hours after the procedure. You can start eating and drinking once you are fully awake and feel up to it. You usually stay in hospital for the night. You should be back to doing your normal activities after about a week.
You usually have a scan about 4 to 6 weeks after ablation treatment to check how well it has worked.
Side effects of ablation therapies
Possible side effects after ablation therapy can can vary depending on which treatment is used and other factors, but they might include:
- Skin irritation where the treatment is given. You will probably have some discomfort or mild pain where the needles went into your skin.
- Abdominal pain (especially with ethanol (alcohol) ablation). Treatment to the liver can also cause shoulder pain. This is caused by pain travelling along a nerve near the liver, which connects to nerves in the shoulder. It’s called referred pain. You will have painkillers to take home, although you may not need to use them. Contact your doctor if your painkillers are not working. Also let your doctor know if your pain isn’t getting better, or if the pain gets worse.
- Bleeding. There is a risk of bleeding caused by the needle going into the liver. This is rare. Your doctor and nurses monitor you closely during and after treatment. So if this happens, they deal with it straight away. You might need to have a procedure, such as an angiogram, to stop the bleeding. You may also have a blood transfusion if you have lost a lot of blood.
- Damage to the surrounding area. During the ablation procedure, there is a small risk of damaging structures near the liver. For example, damage to the bile ducts, bowel or gallbladder. This is rare because the doctor uses scans to help guide the probe to the right place. The heat only travels a short distance, so it doesn’t generally affect the rest of your liver tissue.
- Infection in the liver
- Fever
- Flu-like symptoms (post ablation syndrome). Some people have flu-like symptoms that start about 3 to 5 days after treatment. You feel tired, generally unwell, have body aches and you may feel sick. This might last 1 to 2 weeks. This is due to a side effect called post ablation syndrome. Before you go home, your doctor will explain post ablation syndrome to you. They will go through what medicines you can take to relieve your symptoms. Contact your oncology team if you feel unwell after this time or have a temperature above 38°C. You may have an infection that needs treatment.
- Abnormal blood tests of liver function
- Risk of your cancer coming back. There is a risk that thermal ablation does not completely get rid of the cancer. Or that it grows back (recurs). You may be able to have the area treated again. This can be done a few weeks after the first ablation.
Serious complications aren’t common, but they are possible.
Radiofrequency ablation (RFA)
Radiofrequency ablation (RFA) uses high-energy radio waves to heat and destroy tumors. Radiofrequency ablation (RFA) uses a thin, needle-like probe that is inserted through the skin and moved forward until the end of the probe is in the tumor. Ultrasound or CT scan is used to guide the probe into place. Once it is in place, an electric current is passed through the tip of the probe. This heats the tumor and destroys the cancer cells.
Microwave ablation (MWA)
In microwave ablation (MWA), imaging tests are used to guide a needle-like probe (antenna) into the tumor. Electromagnetic microwaves are then created at the tip of the probe to heat to destroy the tumor.
Cryoablation (cryotherapy)
Cryoablation destroys a tumor by freezing it using a thin metal probe. The probe is guided into the tumor, and then very cold gasses are passed through the probe to freeze the tumor, which causes the cancer cells to die.
This technique is sometimes used along with surgery to remove part of the liver. It isn’t used as often by itself as RFA or MWA are, as it tends to be a more complex procedure.
Ethanol (alcohol) ablation
Ethanol (alcohol) ablation is also known as percutaneous ethanol injection (PEI). Concentrated alcohol is injected directly into the tumor to damage cancer cells. Sometimes several treatments of alcohol ablation are needed.
Ethanol (alcohol) ablation is used less often than radiofrequency ablation (RFA) or microwave ablation (MWA), although it might be helpful in some situations where it would be hard to use those other approaches.
Histotripsy
Histotripsy is a newer type of ablation treatment for liver tumors. It uses an ultrasound machine to aim strong, focused sound waves through the skin to the area that needs treatment. The sound waves break down the tumor’s tissue and turn it into liquid, so this is sometimes described as liquefying the tumor.
Unlike other types of ablation, histotripsy does not require anything to be inserted into the body. It works by directly damaging the tumor’s tissue, which helps protect the healthy tissue and cells around the tumor.
Embolization treatment (TAE or TACE)
Embolization therapy is a treatment that blocks or reduces the blood supply to the cancer by injecting substances directly into an artery in your liver to block or reduce the blood flow to a tumor in your liver. Your liver has 2 blood supplies. Most normal liver cells are fed by the portal vein, whereas cancer in the liver is mainly fed by the hepatic artery. Blocking the part of the hepatic artery that feeds the tumor helps kill off the cancer cells, but it leaves most of the healthy liver cells unharmed because they get their blood supply from the portal vein.
You might have trans-arterial embolization (TAE) to cut off the blood supply to the cancer. Your doctor does this by injecting a substance such as a gel or tiny beads to block the liver’s blood supply.
Some people have chemotherapy directly to the area of your liver that contains the cancer before the blood supply is blocked. This is called chemoembolization or trans-arterial chemoembolization (TACE).
You usually have this treatment if you can’t have surgery, or to help control the cancer while you are waiting for a liver transplant. Or you may have this treatment to shrink a tumor so that it then becomes small enough to remove with surgery.
Embolization is an option for some people with liver tumors that cannot be removed by surgery. It can be used for people with tumors that are too large to be treated with ablation (usually larger than 5 centimeters, or about 2 inches, across) and who also have adequate liver function. It can also be used along with ablation. This treatment is sometimes used in people waiting for a liver transplant.
While embolization can sometimes be helpful, in general it is not used by itself to try to cure liver cancer.
Embolization can reduce some of the blood supply to the normal liver tissue, so it may not be a good option for some people whose liver has been damaged by diseases such as hepatitis or cirrhosis.
It isn’t yet clear which type of embolization has a better long-term outcome.
People getting this treatment typically do not need to stay in the hospital overnight.
Embolization side effects
Possible complications after embolization include:
- Abdominal pain
- Fever
- Nausea
- Infection in the liver
- Blood clots in the main blood vessels of the liver
Sometimes, it can take several weeks to fully recover from the procedure. Because healthy liver tissue can be affected, there is a risk that liver function will get worse after embolization. This risk is higher if a large branch of the hepatic artery is embolized.
Serious complications are not common, but they are possible.
Trans-arterial embolization (TAE)
During trans-arterial embolization (TAE), a catheter (a thin, flexible tube) is put into an artery in the inner thigh through a small cut and eased up into the hepatic artery in the liver. A dye is usually injected into the bloodstream to help the doctor watch the path of the catheter. Once the catheter is in place, small particles are injected into the artery to plug it up, blocking oxygen and key nutrients from the tumor.
Trans-arterial chemoembolization (TACE)
Trans-arterial chemoembolization (TACE) is usually the first type of embolization used for large liver cancers that can’t be treated with surgery or ablation. It combines embolization with chemotherapy (chemo). Most often, this is done by giving a chemo drug through the catheter directly into the artery, then plugging up the artery, so the chemo can stay close to the tumor.
Drug-eluting bead chemoembolization (DEB-TACE)
Drug-eluting bead chemoembolization (DEB-TACE) combines trans-arterial chemoembolization (TACE) with drug-eluting beads (tiny beads that contain a chemo drug). The procedure is essentially the same as TACE except that the artery is blocked after drug-eluting beads are injected. Because the chemo is physically close to the cancer and because the drug-eluting beads slowly release the chemo, the cancer cells are more likely to be damaged and die.
The most common chemo drugs used for TACE or DEB-TACE are cisplatin and doxorubicin.
Radioembolization (RE)
Radioembolization combines embolization with radiation therapy. This is done by injecting small beads called microspheres that have a radioactive isotope yttrium-90 or Y-90 attached to them into the hepatic artery. Once infused, the beads lodge in the blood vessels near the tumor, where they give off small amounts of radiation to the tumor site for several days. The radiation travels a very short distance, so its effects are limited mainly to the tumor.
Radiation therapy
Radiation therapy also called radiotherapy uses high-energy rays (X-rays) or particles to kill cancer cells.
There are different types of radiotherapy for liver cancer:
- Stereotactic ablative radiotherapy (SABR) also called stereotactic body radiotherapy (SBRT) or stereotactic radiotherapy
- Selective internal radiotherapy treatment (SIRT)
Radiation might be part of your treatment if:
- Your liver tumor(s) cannot be removed by surgery
- Your liver tumor(s) cannot be treated with ablation or embolization or did not respond well to those treatments
- Your liver cancer has spread to other parts of your body, such as your brain or bones
- Large liver tumors are causing pain
- A tumor thrombus (a collection of liver cancer cells) is blocking the portal vein
Radiation might not be a good option for some people whose liver has been extensively damaged by diseases such as hepatitis or cirrhosis.
When used to treat liver cancer, radiation therapy is most often given using a machine that creates and focuses beams of radiation on the cancer. This is known as external radiation therapy (EBRT). Getting this type of radiation therapy is much like getting an x-ray, but the radiation is stronger. The procedure itself is painless. Each treatment lasts only a few minutes, although the setup time (getting you into place for treatment) usually takes longer. The number of treatments you need, and the length of treatment will depend on why it’s being given.
Although liver cancer cells are sensitive to radiation, the treatment is planned carefully to avoid damaging normal liver tissue as much as possible.
For example, treatment is often given using image-guided radiation therapy (IGRT), where an imaging scan (like a CT or MRI) is done just before each treatment. Because the tumor’s position in the body can change slightly from day to day, image-guided radiation therapy (IGRT) can help ensure the radiation is aimed more precisely, which might result in fewer side effects.
Newer radiation techniques, such as stereotactic body radiation therapy (SBRT) or stereotactic ablative radiotherapy (SABR), can help doctors target liver tumors while reducing the radiation to nearby healthy tissues. Stereotactic body radiation therapy (SBRT) uses very focused beams of high-dose radiation that are aimed at the tumor from many different angles. To focus the radiation precisely, the person is put in a specially designed body frame for each treatment. Because of the higher doses of radiation, stereotactic body radiation therapy (SBRT) can be given over a shorter time compared to standard radiation therapy, often in 3 to 6 treatments.
Stereotactic body radiation therapy (SBRT)
Stereotactic body radiotherapy (SBRT) also called stereotactic ablative radiotherapy (SABR) or stereotactic radiotherapy. It is a type of external targeted radiotherapy that can treat small cancers.
The machine aims radiation beams from different positions around the body. This means the tumor gets a high dose of radiation to kill cancer cells. But the tissues near the tumor only get a low dose of radiation which lowers the risk of side effects.
Planning stereotactic body radiotherapy (SBRT) treatment
Before you start treatment you have a planning appointment. This is to make sure that your treatment is as accurate as possible. You will have some scans and you may have some small markings made on your skin. You won’t be allowed to eat or drink for a couple of hours before your scan, and before each treatment.
Having stereotactic body radiotherapy (SBRT) treatment
You usually have stereotactic body radiotherapy (SBRT) as an outpatient. You may have between 3 and 5 treatments over 1 or 2 weeks. Each treatment usually takes up to an hour.
You won’t feel anything while you have your treatment and the machine doesn’t touch you. This type of radiotherapy won’t make you radioactive. It’s safe to be around other people, including pregnant women and children.
Side effects of stereotactic body radiotherapy (SBRT)
Some of the more common side effects of radiation therapy include:
- Skin changes in areas getting radiation, ranging from redness to blistering and peeling
- Nausea and vomiting
- Fatigue. Radiotherapy can make you feel tired. This usually increases towards the end of a course of treatment. You may feel more tired than usual for a few days or weeks after you finish treatment.
- Diarrhea. Because your liver is near your stomach and intestines, radiotherapy can cause sickness or diarrhea. Your doctor will give you medicines to help.
- Loss of appetite
These effects typically go away within a few weeks after treatment ends.
A more serious side effect of radiation therapy to the liver is radiation-induced liver disease (RILD), in which other parts of the liver are damaged. This is less common than in the past, now that radiation beams can be aimed more precisely at the cancer. If radiation-induced liver disease (RILD) does develop, it is most often 3 to 4 months after treatment and usually only lasts for a set time, but sometimes it can be life-threatening. Signs and symptoms of radiation-induced liver disease (RILD) can include abnormal blood liver test results, an enlarged liver and spleen, ascites (fluid buildup in the abdomen), and jaundice. You will have blood tests to check for this.
Ask your doctor what side effects to expect and if there are things you can do to help prevent or relieve them.
Selective internal radiotherapy (SIRT)
Selective Internal Radiation Therapy (SIRT) also called radioembolization or trans arterial radioembolization (TARE) is a form of targeted radiation therapy used to treat liver cancers and is sometimes used for larger liver cancers. Selective internal radiotherapy (SIRT) involves delivering radioactive beads or radioactive microspheres directly into the blood vessels that supply the tumor, minimizing damage to healthy tissue. This treatment is often considered when surgery is not an option, and it can be used for both primary liver cancers and liver metastases.
Before selective internal radiotherapy (SIRT) treatment
You have a test called an angiogram to help plan selective internal radiotherapy (SIRT). An angiogram looks at the blood supply to the cancer. This is to check that selective internal radiotherapy (SIRT) is a suitable treatment for you. It also helps your doctors plan where the radioactive beads or radioactive microspheres need to go.
You might have a local anaesthetic for your angiogram. Or you may have drugs to make you sleepy (sedation). You won’t be allowed to eat or drink for a few hours beforehand if you have sedation. Your appointment letter will give more detail about this.
Having selective internal radiotherapy (SIRT) treatment
You have treatment 1 or 2 weeks after your planning. It is very similar to your planning appointment. Your doctor injects the microspheres into the blood vessel that takes blood to the cancer. The microspheres get stuck in the small blood vessels in and around the cancer. The radiation destroys the cancer cells.
At the end of the treatment you have a scan to check the amount of radiation to your liver. You might stay in hospital overnight.
The range of radiation from the beads is very small. But as a precaution, they may tell you to avoid close contact with young children and pregnant women. Your oncology team will give you information about this..
Side effects of selective internal radiotherapy (SIRT)
The radiation only travels a few millimeters from where the beads are trapped. So there should be little damage to the surrounding healthy tissue. The side effects are usually mild and include:
- a small bruise where the catheter was put in
- damage to the blood vessel by the catheter
- a raised temperature and chills
- feeling sick
- diarrhea
- stomach ache
- tiredness
Very rarely, selective internal radiotherapy (SIRT) can cause damage to your liver.
Immunotherapy
Immunotherapy is the use of medicines that help a person’s own immune system find and destroy cancer cells. It can be used to treat some people with liver cancer.
Immune checkpoint inhibitors
An important part of the immune system is its ability to keep itself from attacking normal cells in the body. To do this, it uses “checkpoint” proteins on immune cells, which act like switches that need to be turned on (or off) to start an immune response. Cancer cells sometimes use these checkpoint proteins to avoid being attacked by the immune system. Drugs that target these checkpoints, known as checkpoint inhibitors, are now an important part of the treatment for many people with liver cancer, especially if the cancer can’t be removed with surgery.
PD-1 and PD-L1 inhibitors
PD-1 is a checkpoint protein on immune cells called T cells. When PD-1 attaches to PD-L1, a protein on other cells in the body, it acts as a type of “off switch” that tells the T cell to leave the other cell alone. Some cancer cells have large amounts of PD-L1, which helps them hide from an immune attack.
Drugs that target either PD-1 or PD-L1 can block this binding and boost the immune response against cancer cells.
Atezolizumab (Tecentriq) and Durvalumab (Imfinzi) target the PD-L1 protein. Blocking this protein can help boost the immune response against cancer cells. This can shrink some tumors or slow their growth.
- Atezolizumab can be used along with the targeted drug bevacizumab (Avastin and other brand names) as the first treatment for liver cancer that cannot be treated by surgery or that has spread to other organs.
- Durvalumab can be used with the immunotherapy drug tremelimumab (Imjudo) as the first treatment for liver cancer that cannot be removed with surgery.
These drugs are given as an infusion into a vein (IV), typically once every 2, 3, or 4 weeks. Atezolizumab (Tecentriq Hybreza) can also be injected under the skin (subcutaneously) over several minutes, typically once every 3 weeks.
Pembrolizumab (Keytruda) and nivolumab (Opdivo) are drugs that target PD-1, which can help boost the immune response against cancer cells. This can shrink some tumors or slow their growth. These drugs can be used in people with advanced liver cancer.
- Nivolumab can be used with the immunotherapy drug ipilimumab (Yervoy – see below), either as the first treatment or after other treatments have been tried.
- Pembrolizumab can be used by itself, typically after other medicines have been tried.
These drugs are given as an intravenous (IV) infusion, typically every 2, 3, 4, or 6 weeks.
CTLA-4 inhibitors
Ipilimumab (Yervoy) and Tremelimumab (Imjudo) are immune checkpoint inhibitors with a different target. They block CTLA-4, another protein on T cells that normally helps keep them in check.
- Tremelimumab can be used with durvalumab (see above) as the first treatment for liver cancer that can’t be removed with surgery. It is given as an intravenous (IV) infusion, typically once every 4 weeks.
- Ipilimumab can be used with nivolumab (see above) to treat liver cancer, typically after other medicines have been tried (such as the targeted drug sorafenib). This drug is given as an intravenous (IV) infusion, usually once every 3 weeks for 4 treatments.
Possible side effects of checkpoint inhibitors
Common side effects of these drugs can include:
- Feeling tired or weak
- Fever
- Cough
- Nausea
- Itching
- Skin rash
- Loss of appetite
- Muscle or joint pain
- Constipation or diarrhea
Less common but more serious side effects can include:
- Infusion reactions: Some people might have an infusion reaction while getting these drugs. This is like an allergic reaction, and can include fever, chills, flushing of the face, rash, itchy skin, feeling dizzy, wheezing, and trouble breathing. It’s important to tell your doctor or nurse right away if you have any of these symptoms while getting these drugs.
- Autoimmune reactions: These drugs work by basically removing one of the safeguards on the body’s immune system. Sometimes the immune system starts attacking other parts of the body, which can cause serious or even life-threatening problems in the lungs, intestines, liver, hormone-making glands, kidneys, skin, or other organs.
Serious side effects seem to occur more often with CTLA-4 inhibitors than with the PD-1 and PD-L1 inhibitors.
It’s very important to report any new side effects to your oncology team promptly. If serious side effects do occur, treatment may need to be stopped, and you may get high doses of corticosteroids to suppress your immune system.
Targeted Drug Therapy
Targeted cancer drugs work by targeting the differences in cancer cells that help them to grow and survive. There are many different types of targeted drugs. You might hear some targeted drugs called biological therapies.
Targeted drugs enter the bloodstream and reach almost all areas of the body, which can make them useful against cancers that have spread to distant parts of the body.
Targeted cancer drugs might be an option if liver cancer can’t be treated by surgery or if it has spread to other organs.
Kinase inhibitors
Kinases are proteins inside cells that normally help tumor cells grow in one of two ways:
- Some kinases help tumor cells grow.
- Some kinases help tumors form the new blood vessels they need in order to get bigger (a process called angiogenesis).
Many of the targeted drugs used to treat liver cancer are kinase inhibitors. These drugs block several kinase proteins. Blocking these proteins can often help stop the growth of the cancer.
These drugs are most often used after immunotherapy drugs (see above) have been tried.
Kinase inhibitors that can be used to treat liver cancer include:
- Sorafenib (Nexavar)
- Lenvatinib (Lenvima)
- Regorafenib (Stivarga)
- Cabozantinib (Cabometyx)
These drugs are pills, taken typically once or twice a day, depending on the drug.
Side effects of kinase inhibitors
Common side effects of kinase inhibitors drugs can include:
- Fatigue
- Loss of appetite
- Hand-foot syndrome (redness and irritation of the hands and feet)
- Rash
- Hair loss
- High blood pressure
- Weight loss
- Diarrhea
- Abdominal (belly) pain
Less common but more serious side effects can include:
- Problems with blood flow to the heart
- Bleeding
- Blood clots
- Abnormal thyroid test results
- Damage to other organs (such as the liver or kidneys)
- Perforations (holes) in the stomach or intestines
Other side effects are also possible, depending on which drug you’re getting. Ask your cancer care team what you should look out for.
Monoclonal antibodies
Monoclonal antibodies are man-made versions of immune system proteins (antibodies) that are designed to attach to a specific target. The monoclonal antibodies used to treat liver cancer affect a tumor’s ability to form new blood vessels, which it needs to grow. This new blood vessel growth is called angiogenesis, so these drugs are often referred to as angiogenesis inhibitors.
Side effects of angiogenesis inhibitors
Common side effects of these drugs can include:
- High blood pressure
- Tiredness (fatigue)
- Bleeding
- Low white blood cell counts with increased risk of infections
- Headaches
- Mouth sores
- Loss of appetite
- Diarrhea
Less common but possibly serious side effects can include:
- Blood clots
- Severe bleeding
- Holes (perforations) in the stomach or intestines
- Heart problems
- Slow wound healing
Bevacizumab
Bevacizumab (Avastin and other brand names) is a monoclonal antibody that targets vascular endothelial growth factor (VEGF), a protein that helps new blood vessels to form.
Bevacizumab can be used along with the immunotherapy drug atezolizumab (Tecentriq) as the first treatment for liver cancer that can’t be treated by surgery or that has spread to other organs.
Bevacizumab drug is given as an infusion into a vein (IV), typically once every 3 weeks.
Ramucirumab
Ramucirumab (Cyramza) is a monoclonal antibody that targets a VEGF receptor (VEGFR) protein on cells, which can help stop the formation of new blood vessels.
Ramucirumab can be used to treat advanced liver cancer, typically after other medicines have been tried.
Ramucirumab is given as an infusion into a vein (IV), usually once every 2 weeks.
Chemotherapy
Chemotherapy (chemo) is treatment with certain kinds of drugs that destroy cancer cells. Chemo may be an option for people whose liver cancer can’t be treated with surgery or other local therapies such as ablation or embolization.
In the past, chemo was often the first treatment for more advanced liver cancers. But newer types of treatment, such as immunotherapy and targeted therapy drugs, are more likely to be helpful, so these drugs are now typically used first instead.
Chemo might still be an option for people who have already had these treatments or can’t get them for some reason.
Hepatic artery infusion of chemo might also be an option for some people whose cancer can’t be removed completely.
Chemo drugs that might be used to treat liver cancer include:
- Gemcitabine
- Oxaliplatin
- Cisplatin
- Doxorubicin (or pegylated liposomal doxorubicin)
- 5-fluorouracil (5-FU)
- Capecitabine
- Mitoxantrone
Sometimes, combinations of 2 or 3 of these drugs are used, if a person can tolerate it. For example:
- GEMOX (gemcitabine plus oxaliplatin) might be an option for people who are healthy enough tolerate more than one drug.
- FOLFOX (5-FU, oxaliplatin and leucovorin) might be another option for some people.
Side effects of chemotherapy
Chemo drugs attack cells in the body that are dividing quickly, which can lead to side effects.
The side effects depend on the type and dose of chemo drugs, as well as how long they are given. Common side effects include:
- Hair loss
- Mouth sores
- Loss of appetite
- Nausea and vomiting
- Diarrhea
- Increased chance of infections (from having too few white blood cells)
- Easy bruising or bleeding (from having too few blood platelets)
- Feeling tired (from having too few red blood cells)
These side effects usually go away after treatment is finished. There are often ways to lessen them. For example, drugs can be given to help prevent or reduce nausea and vomiting. Be sure to ask your cancer care team about medicines to help reduce side effects.
Along with the possible side effects above, some drugs may have their own specific side effects. Ask your cancer care team what you can expect.
Be sure to tell your oncology team about any side effects that you notice while getting chemo so that you can be treated right away. In some cases, the doses of the chemo drugs may need to be reduced, or treatment may need to be delayed or stopped to keep the side effects from getting worse.
How is chemotherapy given for liver cancer
Chemo can be given in different ways.
Systemic chemotherapy
In this approach, chemo drugs are given into a vein (IV) or taken by mouth. The chemo drugs enter your blood and reach almost all areas of your body, which can make this treatment useful for cancers that have spread to other parts of the body.
For some people, IV chemo might be given through a slightly larger and sturdier tube known as a central venous catheter (CVC), central venous access device (CVAD), or central line. This device is put in place with a minor surgical procedure. It stays in the body and can be used to put medicines, blood products, nutrients, or fluids right into your blood. It can also be used to take out blood for testing.
Doctors give chemo in cycles, with each period of treatment followed by a rest period to give you time to recover from the effects of the medicine. Cycles are most often 2 or 3 weeks long. The schedule varies depending on the medicines used. For example, with some medicines, the chemo is given only on the first day of the cycle. With others, it is given for a few days in a row, or once a week.
The length of chemo treatment will be based on how well it is working and what side effects you have.
Hepatic artery infusion
During hepatic artery infusion (HAI), chemo is given directly into the hepatic artery, a large artery that feeds into the liver. This focuses the chemo on the cancer cells in the liver. The drug enters the liver and affects the cancer cells, while the healthy liver cells break down most of the drug before it can reach the rest of the body. This method gets a higher dose of chemo to the tumor than systemic chemo while limiting side effects in the rest of the body.
Hepatic artery infusion is slightly different from chemoembolization because a surgery is needed to put an infusion pump under the skin of the abdomen (belly). The pump is attached to a catheter that connects to the hepatic artery. This is done while a person is under general anesthesia (in a deep sleep so they won’t feel pain). The chemo is then injected with a needle through the skin into the pump’s reservoir, and it is released slowly and steadily into the hepatic artery.
Hepatic artery infusion (HAI) may be used for people with very large liver cancers that cannot be removed with surgery or cannot be treated entirely with trans-arterial chemoembolization (TACE). But many people with liver cancer may not be able to tolerate surgery to insert the pump and catheter, and not all centers offer this type of treatment.
Liver Cancer Treatment by Stage
Although the AJCC (TNM) staging system (see Liver Cancer Stages above) is often used to describe the spread of a liver cancer, doctors use more practical system to determine a person’s treatment options:
- Potentially resectable cancer
- Potentially eligible for a liver transplant
- Unresectable (inoperable) cancer that has not spread
- Advanced cancer
- Recurrent liver cancer
Potentially resectable (removable) liver cancer
If your liver cancer is at an early stage and the rest of your liver is healthy enough for you to have surgery, a partial hepatectomy (removing the part of the liver with the cancer) may cure you.
Only a small number of people with liver cancer can have this type of surgery. Important factors to consider include the size of the tumor(s) and if nearby blood vessels are affected. Larger tumors or those that invade blood vessels are more likely to come back in the liver or spread elsewhere after surgery. Your overall health and how well your liver is working are also important.
Clinical trials are now looking at if people who have a partial hepatectomy might be helped by getting other treatments in addition to surgery. But more research is needed to know is this is helpful.
Other options for people in this situation might include:
- Some type of ablation procedure such as radiofrequency ablation (RFA) or microwave ablation (MWA) to destroy the tumor, if it is small enough.
- Stereotactic body radiation (SBRT), which carefully focuses beams of high-dose radiation at the tumor from many different angles.
- A liver transplant. This is a complex operation that can have some long-term side effects, but removing and replacing the whole liver can lower the risk of developing a new liver cancer.
Potentially eligible for a liver transplant
If your liver cancer is at an early stage, but you wouldn’t have enough healthy liver left if the part with the cancer was removed, you may be able to be treated with a liver transplant. A liver transplant may also be an option if the tumor is in a part of the liver that makes it hard to remove such as very close to a large blood vessel.
People who are eligible for a liver transplant might have to wait a long time for a donor liver to become available, and there’s a chance that the cancer might grow during that time to the point where surgery might no longer be possible. Because of this, people are often given other treatments, such as ablation or embolization, to help keep the cancer under control. This is known as bridge therapy.
Unresectable (inoperable) liver cancer that has not spread
These include cancers that haven’t yet spread to lymph nodes or distant parts of the body, but that can’t be treated safely with surgery (partial hepatectomy or liver transplant).
This might be because:
- The tumor is too large or is in a part of the liver (such as very close to a large blood vessel) that makes it hard to remove safely.
- There are several tumors.
- The person has other health issues that would make it unsafe for them to have liver surgery.
Treatment options might include ablation, embolization, or both for the liver tumor(s). Other options may include targeted therapy, immunotherapy, chemotherapy (either systemic or by hepatic artery infusion), and/or radiation therapy. These treatments aren’t likely to cure the cancer, but they can often reduce a person’s symptoms and help them live longer.
For some of these cancers, treatment may shrink the tumor(s) enough so that surgery (partial hepatectomy or transplant) may become possible.
Because these cancers can be hard to treat, clinical trials of newer treatments may be a good option in many cases.
Advanced (metastatic) liver cancer
Advanced liver cancer has spread outside the liver, either to the lymph nodes or to other organs. Because these cancers are widespread, they can’t be removed with surgery.
For people whose liver is functioning well enough, initial treatment options might include:
- The immunotherapy drug atezolizumab (Tecentriq) plus the targeted drug bevacizumab (Avastin)
- The immunotherapy drugs durvalumab (Imfinzi) and tremelimumab (Imjudo)
- The immunotherapy drugs nivolumab (Opdivo) and ipilimumab (Yervoy)
- Either of the targeted drugs sorafenib (Nexavar) or lenvatinib (Lenvima)
- The immunotherapy drug durvalumab alone
If these drugs are no longer working or if they can’t be given for some reason, other options might include:
- Other targeted drugs such as regorafenib (Stivarga), cabozantinib (Cabometyx), or ramucirumab (Cyramza)
- Other immunotherapy drugs such as pembrolizumab (Keytruda), or nivolumab combined with ipilimumab
- Chemotherapy drugs
As with unresectable liver cancer that has not spread, clinical trials of newer treatments may be helpful.
Treatments such as radiation might also be used to help relieve pain and other symptoms. Please be sure to discuss any symptoms you have with your cancer team, so they can treat them effectively.
Recurrent liver cancer
Cancer that comes back after treatment is called recurrent. Recurrence can be local (in or near the same place it started) or distant (spread to organs such as the lungs or bone).
Treatment of liver cancer that returns after initial therapy depends on many factors, including where it comes back, which treatment(s) a person has had before, and how well the liver is functioning.
People with resectable cancer that recurs in the liver might be eligible for further surgery or local treatments like ablation, embolization, or radiation therapy.
If the cancer is widespread, targeted therapy, immunotherapy, or chemotherapy drugs may be options. A clinical trial testing a newer treatment might also be an option for some people.
Please be sure to tell your cancer care team about any symptoms you have. You can also get treatment to relieve pain and other side effects.
Considering complementary and alternative methods
You may hear about complementary or alternative methods that your doctor hasn’t mentioned to treat your cancer or relieve symptoms. These methods can include vitamins, herbs, and special diets, or other methods such as acupuncture or massage, to name a few.
Complementary methods refer to treatments that are used along with your regular medical care. Alternative treatments are used instead of a doctor’s medical treatment. Although some of these methods might be helpful in relieving symptoms or helping you feel better, many have not been proven to work. Some might even be dangerous.
As you consider your options, look for “red flags” that might suggest fraud.
- Does the method promise to cure all or most cancers?
- Are you told not to have regular medical treatments?
- Is the treatment a “secret” that requires you to visit certain providers or travel to another country?
Be sure to talk to your cancer care team about any method you are thinking about using. They can help you learn what is known (or not known) about the method, which can help you make an informed decision.
Choosing to stop treatment or choosing no treatment at all
For some people, when treatments have been tried and are no longer controlling the cancer, it could be time to weigh the benefits and risks of continuing to try new treatments. Whether or not you continue treatment, there are still things you can do to help maintain or improve your quality of life.
Some people, especially if the cancer is advanced, might not want to be treated at all. There are many reasons you might decide not to get cancer treatment, but it’s important to talk this through with your doctors before you make this decision. Remember that even if you choose not to treat the cancer, you can still get help for pain or other symptoms.
Help getting through treatment
Your cancer care team will be your first source of information and support, but there are other resources for help when you need it. Hospital- or clinic-based support services are an important part of your care. These might include nursing or social work services, financial aid, nutritional advice, rehab, or spiritual help.
Liver Cancer Prognosis
The natural course of early tumors is poorly known because most hepatocellular carcinoma patients are treated. However, older reports have described 3-year survival rates of 13% to 21% without any specific treatment 26, 27. At present, only 10% to 23% of patients with hepatocellular carcinoma may be surgical candidates for curative-intent treatment 28, 29. The 5-year overall survival rate for patients with early hepatocellular carcinoma who are undergoing liver transplant is 44% to 78%; and for patients undergoing a liver resection, the OS rate is 27% to 70% 30.
Liver transplantation, surgical resection, and ablation offer high rates of complete responses and a potential for cure in patients with early hepatocellular carcinoma 11.
The natural course of advanced-stage hepatocellular carcinoma is better known. Untreated patients with advanced disease usually survive less than 6 months 31. The survival rate of untreated patients in 25 randomized clinical trials ranged from 10% to 72% at 1 year and 8% to 50% at 2 years 32.
Unlike most patients with solid tumors, the prognosis of patients with hepatocellular carcinoma is affected by the tumor stage at presentation and by the underlying liver function. The following prognostic factors guide the selection of treatment:
- Anatomic extension of the tumor (i.e., tumor size, number of lesions, presence of vascular invasion, and extrahepatic spread).
- Performance status.
- Functional hepatic reserve based on the Child-Pugh score 33, 34.
Liver cancer survival rates
Survival rates tell you what part of people with the same type and stage of cancer are still alive a certain amount of time (usually 5 years) after they were diagnosed. These numbers can’t tell you how long you will live, but they may help give you a better understanding about how likely it is that your treatment will be successful.
Keep in mind that survival rates are estimates and are often based on previous outcomes of large numbers of people who had a specific cancer, but they can’t predict what will happen in any person’s case. These statistics can be confusing and may lead you to have more questions. Ask your doctor how these numbers might apply to you.
What is a 5-year relative survival rate?
A relative survival rate compares people with the same type and stage of cancer to people in the overall population. For example, if the 5-year relative survival rate for a specific stage of liver cancer is 37.6%, it means that people who have that cancer are, on average, about 37.6% as likely as people who don’t have that cancer to live for at least 5 years after being diagnosed.
But remember, survival rates are estimates – your outlook can vary based on a number of factors specific to you. Your doctor can tell you how these numbers apply to you, as he or she is familiar with your situation.
Cancer survival rates don’t tell the whole story
Survival rates are often based on previous outcomes of large numbers of people who had the disease, but they can’t predict what will happen in any particular person’s case. Your doctor can tell you how the numbers below may apply to you, as he or she is familiar with the aspects of your particular situation.
Survival rates for liver cancer
The numbers below come from the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) database, and are based on patients who were diagnosed with liver cancer (hepatocellular type) between 2015 and 2021 3.
The Surveillance, Epidemiology, and End Results (SEER) database does not divide liver cancer survival rates by AJCC TNM stages. Instead, it groups cancer cases into summary stages:
- Localized means the cancer is still confined to the liver, and no sign that the cancer has spread outside of the liver. This includes a wide range of cancers, some of which are easier to treat than others. The 5-year relative survival rate for people with localized liver cancer and intrahepatic bile duct cancer is about 37.6%.
- Regional means the cancer has spread outside the liver to nearby structures or lymph nodes. For regional stage liver cancer, the 5-year relative survival rate is about 13.2%.
- Distant means that the cancer has spread to distant parts of the body, such as the lungs or bones. The 5-year relative survival rate for distant stage liver cancer is about 3.5%.
In general, survival rates are higher for people who can have surgery to remove their cancer, regardless of the stage. For example, studies have shown that patients with small, resectable (removable) tumors who do not have cirrhosis or other serious health problems are likely to do well if their cancers are removed. For people with early-stage liver cancers who have a liver transplant, the 5-year survival rate is in the range of 60% to 70%.
- What Is Liver Cancer? American Cancer Society. https://www.cancer.org/cancer/liver-cancer/about/what-is-liver-cancer.html[↩]
- Key Statistics About Liver Cancer. https://www.cancer.org/cancer/types/liver-cancer/about/what-is-key-statistics.html[↩][↩]
- Liver and Intrahepatic Bile Duct Cancer — Cancer Stat Facts. https://seer.cancer.gov/statfacts/html/livibd.html[↩][↩][↩]
- Llovet JM, Burroughs A, Bruix J: Hepatocellular carcinoma. Lancet 362 (9399): 1907-17, 2003. https://www.ncbi.nlm.nih.gov/pubmed/14667750[↩][↩]
- Childhood Liver Cancer. https://www.cancer.gov/types/liver/childhood-liver-cancer[↩]
- Key Statistics About Liver Cancer. American Cancer Society. https://www.cancer.org/cancer/liver-cancer/about/what-is-key-statistics.html[↩]
- What Is Liver Cancer ? American Cancer Society. https://www.cancer.org/cancer/liver-cancer/about/what-is-liver-cancer.html[↩][↩][↩][↩][↩][↩]
- Mavros MN, Mayo SC, Hyder O, et al.: A systematic review: treatment and prognosis of patients with fibrolamellar hepatocellular carcinoma. J Am Coll Surg 215 (6): 820-30, 2012. https://www.ncbi.nlm.nih.gov/pubmed/22981432[↩][↩]
- Hepatoblastoma. https://www.cancer.gov/types/liver/childhood-liver-cancer/hepatoblastoma[↩]
- Liver (Hepatocellular) Cancer Prevention. National Cancer Institute, National Institutes of Health. https://www.cancer.gov/types/liver/patient/liver-prevention-pdq#section/_21[↩]
- Bruix J, Sherman M; American Association for the Study of Liver Diseases: Management of hepatocellular carcinoma: an update. Hepatology 53 (3): 1020-2, 2011. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3084991/[↩][↩]
- Bosch FX, Ribes J, Borràs J: Epidemiology of primary liver cancer. Semin Liver Dis 19 (3): 271-85, 1999. https://www.ncbi.nlm.nih.gov/pubmed/10518307[↩]
- Beasley RP, Hwang LY, Lin CC, et al.: Hepatocellular carcinoma and hepatitis B virus. A prospective study of 22 707 men in Taiwan. Lancet 2 (8256): 1129-33, 1981. https://www.ncbi.nlm.nih.gov/pubmed/6118576[↩]
- Beasley RP: Hepatitis B virus. The major etiology of hepatocellular carcinoma. Cancer 61 (10): 1942-56, 1988. https://www.ncbi.nlm.nih.gov/pubmed/2834034[↩]
- Sun CA, Wu DM, Lin CC, et al.: Incidence and cofactors of hepatitis C virus-related hepatocellular carcinoma: a prospective study of 12,008 men in Taiwan. Am J Epidemiol 157 (8): 674-82, 2003. https://www.ncbi.nlm.nih.gov/pubmed/12697571[↩]
- Lok AS, Seeff LB, Morgan TR, et al.: Incidence of hepatocellular carcinoma and associated risk factors in hepatitis C-related advanced liver disease. Gastroenterology 136 (1): 138-48, 2009. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3749922/[↩]
- Bruix J, Sherman M. Management of hepatocellular carcinoma: An update. Hepatology (Baltimore, Md). 2011;53(3):1020-1022. doi:10.1002/hep.24199. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3084991/[↩]
- Farinati F, Floreani A, De Maria N, et al.: Hepatocellular carcinoma in primary biliary cirrhosis. J Hepatol 21 (3): 315-6, 1994. https://www.ncbi.nlm.nih.gov/pubmed/7530737[↩]
- Forner A, Llovet JM, Bruix J: Hepatocellular carcinoma. Lancet 379 (9822): 1245-55, 2012. https://www.ncbi.nlm.nih.gov/pubmed/22353262[↩]
- Hessheimer AJ, Forner A, Varela M, et al.: Metabolic risk factors are a major comorbidity in patients with cirrhosis independent of the presence of hepatocellular carcinoma. Eur J Gastroenterol Hepatol 22 (10): 1239-44, 2010. https://www.ncbi.nlm.nih.gov/pubmed/20505515[↩]
- Jaskiewicz K, Banach L, Lancaster E: Hepatic siderosis, fibrosis and cirrhosis: the association with hepatocellular carcinoma in high-risk population. Anticancer Res 17 (5B): 3897-9, 1997 Sep-Oct. https://www.ncbi.nlm.nih.gov/pubmed/9427800[↩]
- Sun Z, Lu P, Gail MH, et al.: Increased risk of hepatocellular carcinoma in male hepatitis B surface antigen carriers with chronic hepatitis who have detectable urinary aflatoxin metabolite M1. Hepatology 30 (2): 379-83, 1999. https://www.ncbi.nlm.nih.gov/pubmed/10421643[↩]
- Signs and Symptoms of Liver Cancer. American Cancer Society. https://www.cancer.org/cancer/liver-cancer/detection-diagnosis-staging/signs-symptoms.html[↩]
- Can Liver Cancer Be Found Early ? American Cancer Society. https://www.cancer.org/cancer/liver-cancer/detection-diagnosis-staging/detection.html[↩]
- Liver Cancer Stages. American Cancer Society. https://www.cancer.org/cancer/liver-cancer/detection-diagnosis-staging/staging.html[↩]
- Barbara L, Benzi G, Gaiani S, et al.: Natural history of small untreated hepatocellular carcinoma in cirrhosis: a multivariate analysis of prognostic factors of tumor growth rate and patient survival. Hepatology 16 (1): 132-7, 1992. https://www.ncbi.nlm.nih.gov/pubmed/1352268[↩]
- Ebara M, Ohto M, Shinagawa T, et al.: Natural history of minute hepatocellular carcinoma smaller than three centimeters complicating cirrhosis. A study in 22 patients. Gastroenterology 90 (2): 289-98, 1986. https://www.ncbi.nlm.nih.gov/pubmed/2416627[↩]
- Shah SA, Smith JK, Li Y, et al.: Underutilization of therapy for hepatocellular carcinoma in the medicare population. Cancer 117 (5): 1019-26, 2011. https://www.ncbi.nlm.nih.gov/pubmed/20945363[↩]
- Sonnenday CJ, Dimick JB, Schulick RD, et al.: Racial and geographic disparities in the utilization of surgical therapy for hepatocellular carcinoma. J Gastrointest Surg 11 (12): 1636-46; discussion 1646, 2007. https://www.ncbi.nlm.nih.gov/pubmed/17912593[↩]
- Dhir M, Lyden ER, Smith LM, et al.: Comparison of outcomes of transplantation and resection in patients with early hepatocellular carcinoma: a meta-analysis. HPB (Oxford) 14 (9): 635-45, 2012. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3461390/[↩]
- Okuda K, Ohtsuki T, Obata H, et al.: Natural history of hepatocellular carcinoma and prognosis in relation to treatment. Study of 850 patients. Cancer 56 (4): 918-28, 1985. https://www.ncbi.nlm.nih.gov/pubmed/2990661[↩]
- Llovet JM, Bruix J: Systematic review of randomized trials for unresectable hepatocellular carcinoma: Chemoembolization improves survival. Hepatology 37 (2): 429-42, 2003. https://www.ncbi.nlm.nih.gov/pubmed/12540794[↩]
- Llovet JM, Brú C, Bruix J: Prognosis of hepatocellular carcinoma: the BCLC staging classification. Semin Liver Dis 19 (3): 329-38, 1999. https://www.ncbi.nlm.nih.gov/pubmed/10518312[↩]
- A new prognostic system for hepatocellular carcinoma: a retrospective study of 435 patients: the Cancer of the Liver Italian Program (CLIP) investigators. Hepatology 28 (3): 751-5, 1998. https://www.ncbi.nlm.nih.gov/pubmed/9731568[↩]




{kind=link}