Contents
- Subgaleal hemorrhage
- Subgaleal hemorrhage newborn causes
- Subgaleal hemorrhage newborn prevention
- Subgaleal hemorrhage newborn signs and symptoms
- Subgaleal hemorrhage complications
- Subgaleal hemorrhage newborn diagnosis
- Subgaleal hemorrhage newborn differential diagnosis
- Subgaleal hemorrhage newborn treatment
- Subgaleal hemorrhage prognosis
Subgaleal hemorrhage
Subgaleal hemorrhage is a rare but potentially lethal bleeding condition in newborns caused by the rupture of emissary veins in the loose connective tissue within the subgaleal space or the loose connective tissue layer located between the epicranial aponeurosis (galea aponeurotica) and the periosteum (the membrane covering the skull bone) (see Figures 2 and 4 below) 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11. Subgaleal hemorrhage only occurs during a vaginal delivery. Sometimes, things don’t go as planned during a vaginal delivery. Subgaleal hemorrhages most often occur if your obstetrician needs to use tools, like a vacuum extractor or forceps, to assist your baby out of your birth canal during a difficult labor process. When the emissary veins that pass through a connective opening of your baby’s scalp break during childbirth, blood gathers between the skin and the scalp bone where the veins ruptured (subgaleal space), causing a subgaleal hemorrhage. Subgaleal hemorrhage can result in blood accumulating in the space between the skull’s periosteum and the galea aponeurosis. Due to being superficial to the periosteum, subgaleal hematomas are able to cross suture lines and surround the entire skull. As the subgaleal space extends into the neck, a subgaleal hematoma may also extend into your baby’s neck. A 1 cm increase in depth of the of the subgaleal space may contain 40 ml to 260 ml of blood, the circulating blood volume of a baby is around 90 ml/kg 12, subgaleal hemorrhage can lead to significant blood loss, newborns can lose 50% to 70% of their circulating blood volume into the subgaleal space, leading to hypovolemic shock, anemia, bleeding disorder and potentially death, especially after difficult vaginal delivery requiring the use a vacuum extractor. Early recognition of subgaleal hemorrhage combine with early close monitoring, and aggressive treatment, including blood product administration, are critical to prevent and reduce mortality and morbidity from subgaleal hemorrhage 12.
The scalp refers to the layers of skin and subcutaneous tissue (also known as the hypodermis, the deepest layer of the skin that lies beneath the dermis) that cover the bones of your skull. The scalp consists of 5 layers. The mnemonic ‘SCALP’ can be a useful way to remember the layers of the scalp: Skin, Connective Tissue, Epicranial Aponeurosis, Loose Areolar Connective Tissue and Periosteum (see Figure 2 below). The first three layers are tightly bound together and move as a collective structure.
- Skin – the skin contains numerous hair follicles and sebaceous glands (a small gland in the skin found in your hair follicles that secrete sebum or an oily substance that protects your skin from drying out).
- Dense Connective tissue – the connective tissue connects your skin to the epicranial aponeurosis. The connective tissue has a very dense network of blood vessels and nerves. Furthermore, the blood vessels within the connective tissue layer are highly adherent to the connective tissue. This renders them unable to constrict fully if lacerated so the scalp can be a site of profuse bleeding.
- Epicranial Aponeurosis also known as the galea aponeurotica – The epicranial aponeurosis is a strong, thin, fibrous sheet that forms the middle, or third, layer of the scalp. The epicranial aponeurosis is a large, flat tendon that connects the front and back bellies of the occipitalis and frontalis muscles, allowing the scalp and eyebrows to move. This structure is important for facial expressions and provides a strong, yet movable, layer for the scalp.
- Loose Areolar Connective Tissue – The loose areolar connective tissue is a thin connective tissue layer that separates the periosteum of the skull from the epicranial aponeurosis. The loose areolar connective tissue contains numerous blood vessels, including emissary veins which connect the veins of the scalp to the diploic veins and intracranial venous sinuses.
- Periosteum – The periosteum is the sheath outside of the skull bones that supplies them with blood, nerves and the cells that help them grow and heal. The periosteum becomes continuous with the endosteum at the suture lines. The endosteum is a thin vascular membrane of connective tissue that lines the center of your skull bones that contain bone marrow. The endosteum is also known as lining membrane of the bone marrow cavity.
Subgaleal hemorrhage in newborn is most common after a vacuum extractor assisted vaginal delivery, but may also be seen following head trauma or minor head trauma such as hair braiding or hair pulling or occur spontaneously because of bleeding disorders or rupture of arteries or arteriovenous fistulas 13, 14, 15, 16, 17, 18, 19, 20, 21, 22. The vacuum, which connects to your baby’s head, can pull the skin on their scalp away from their skull. This can loosen the connective tissue in the subgaleal space of your baby’s head, allowing blood to accumulate outside of their skull. Bleeding occurs as a result of rupture to emissary veins which drain the baby’s scalp veins into the dural sinuses. If too much blood gathers in the area of the skull with loose connective tissue, it could be life-threatening for your baby. Due to being superficial to the periosteum, subgaleal hematomas are able to cross suture lines and surround the entire skull.
The clinical features of subgaleal hemorrhage are variable, however it is recommended that the diagnosis is considered in a newborn with a 5 minute Apgar score of < 7 and no evidence of asphyxia, especially if the delivery was prolonged or there was a vacuum delivery 23. The mean time for diagnosis of subgaleal hemorrhage is 1 to 6 hours after birth and the Royal Australian and New Zealand College of Obstetricians and Gynaecologists have a recommended neonatal surveillance regimen for neonates at risk of subgaleal hemorrhage 23. In the at risk but asymptomatic newborn, the Newborn Royal Australian and New Zealand College of Obstetricians and Gynaecologists recommend that cord pH, lactate, hematocrit and platelet count are taken at birth and basic observations taken hourly for the first 2 hours of life and then 2 hourly for a further 6 hours 23.
After your baby is born, symptoms of a subgaleal hemorrhage will appear. Approximately 6% of subgaleal hemorrhage cases are asymptomatic, 15-20% are mild, 40-50% are moderate and 25-33% are severe.
Symptoms of a subgaleal hemorrhage include:
- Bruising on the skin.
- Swelling on baby’s head that has a liquid-like movement (boggy swelling) due to internal bleeding that can cross suture lines and may extend into the baby’s neck. Palpation of the scalp has been described as a leather pouch filled with fluid.
- This is in contrast to a cephalohematoma which remains confined to the skull and does not cross suture lines.
- Increasing head circumference. Your baby’s head circumference may increase over time. Massive subgaleal hematoma should be considered in cases where children’s head circumference increases rapidly, with or without a clear history of trauma and the presence of any possible risk factors.
- As the hemorrhage progresses, elevation and displacement of the ear lobes and peri orbital edema (puffy eyelids) can be observed.
- Signs of blood loss: Pallor, lethargy, poor feeding.
- Irritability and pain on handling will be noted.
- Fast heart rate (tachycardia).
- Low blood pressure (hypotension).
- Pale skin tone (pallor).
- Reduced levels of hemoglobin and hematocrit in their blood due to major blood loss.
- Days later bruising appears behind the ears and or the eyelids.
Life-threatening symptoms occur in less than 25% of all cases of a subgaleal hemorrhage and include:
- Signs of shock: rapid heart rate (tachycardia) with heart rate >160 beats per minute, rapid breath with respiratory rate > 60 breaths per minute and abnormally low muscle tone (hypotonia).
- Excessive internal bleeding or clotting (bleeding disorder).
- Extensive fluid loss when their heart cannot pump enough blood throughout their body (hypovolemic or hemorrhagic shock).
- Difficulty breathing (respiratory distress).
- Lack of oxygen to your baby’s brain during birth (intrapartum hypoxia).
- Organ failure.
As blood loss can be massive before hypovolemia is recognized, subgaleal hemorrhage can be a devastating and potentially fatal result of birth trauma.
Symptomatic subgaleal hemorrhage is a medical emergency with a high morbidity and mortality. Immediate discussion with a neonatologist experienced in the management of actual or potential hemorrhagic shock is recommended. Prompt evaluation, resuscitation and supportive treatment is essential once the subgaleal hemorrhage diagnosis is suspected. With timely diagnosis and appropriate resuscitation, full recovery can be anticipated.
- Subgaleal hemorrhage is a clinical diagnosis. Stabilization should not be delayed by any attempts to confirm the diagnosis with imaging.
- Aggressive resuscitation to restore circulating blood volume, provide circulatory support, correct acidosis and to correct bleeding disorder is the mainstay of management.
- Head wrapping may be difficult to perform and does not appear to be of benefit.
- Frequent re-evaluation of hemodynamic stability and response to blood and blood products is necessary.
- Intramuscular vitamin K prophylaxis should be encouraged in all neonates as soon as practicable after birth, but this is particularly important for babies that have had an instrument assisted birth.
Newborns diagnosed with a subgaleal hemorrhage, will likely stay in the Neonatal Intensive Care Unit (NICU) until your baby’s doctor approves your baby is healthy enough to go home. After your baby receives treatment to alleviate symptoms of subgaleal hemorrhage, your baby will need follow-up evaluations during their first year to verify that treatment was successful and no lingering symptoms are affecting your child.
Figure 1. Normal skull of newborn
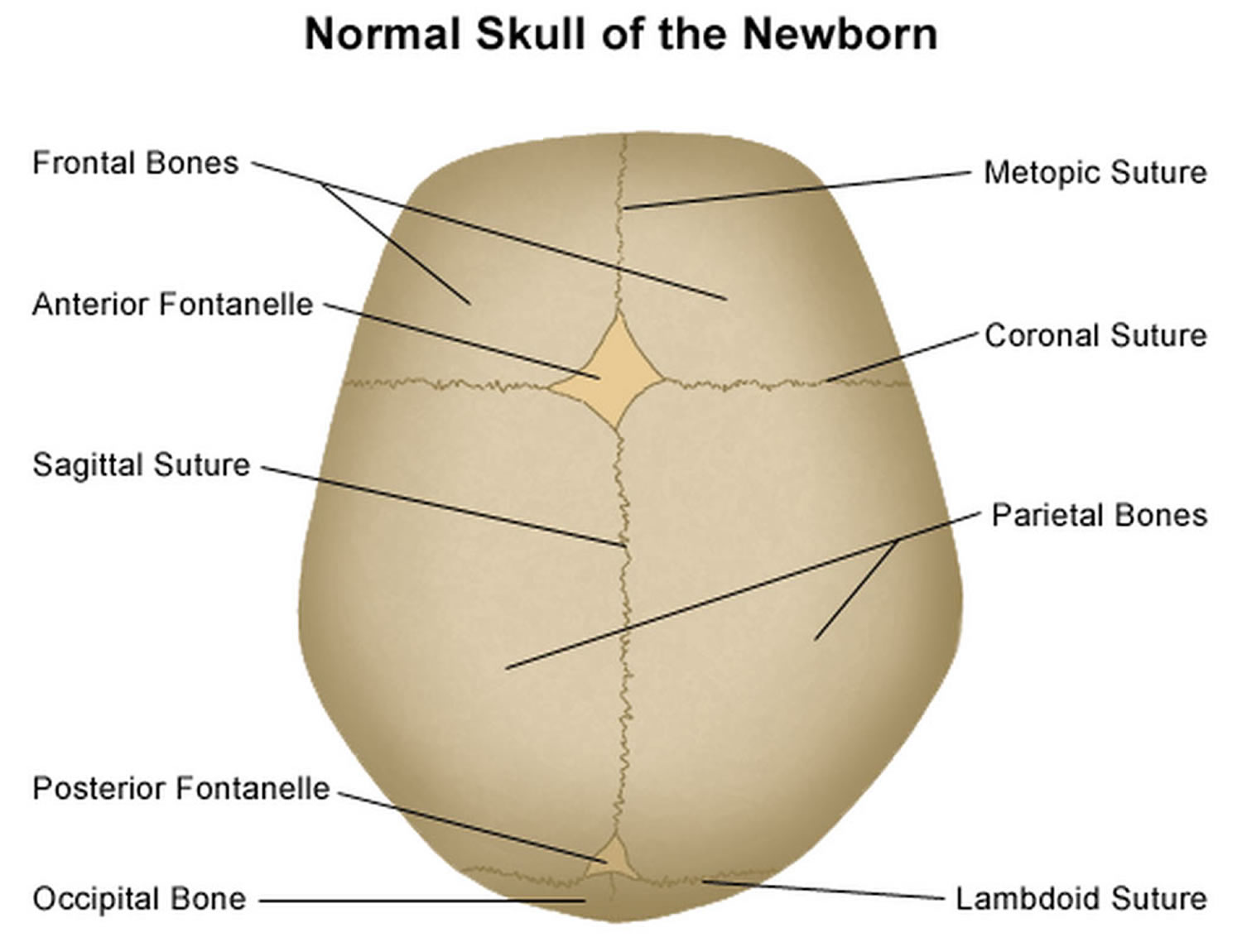
Figure 2. Scalp anatomy
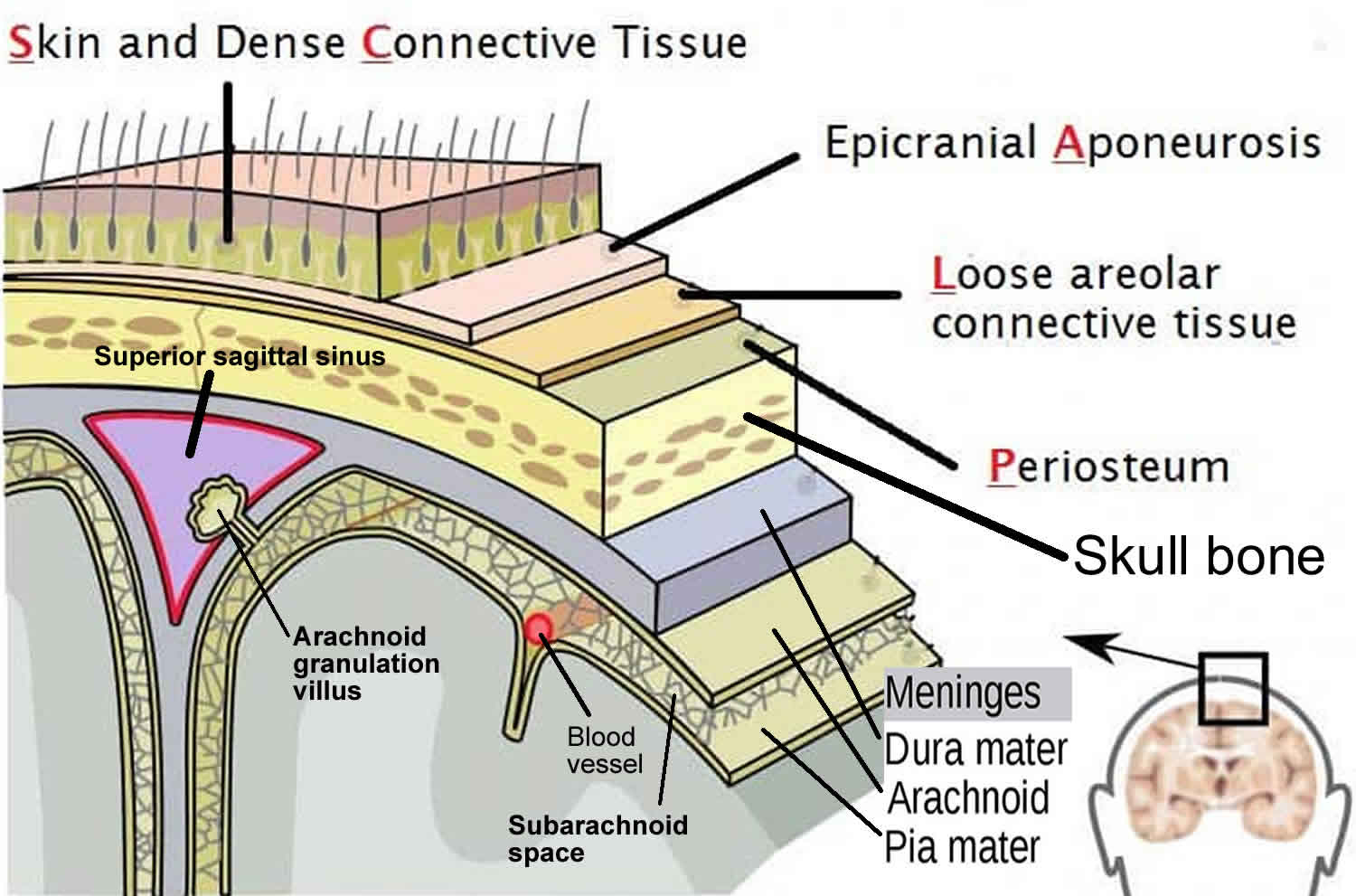
Figure 3. Scalp nerves and arteries
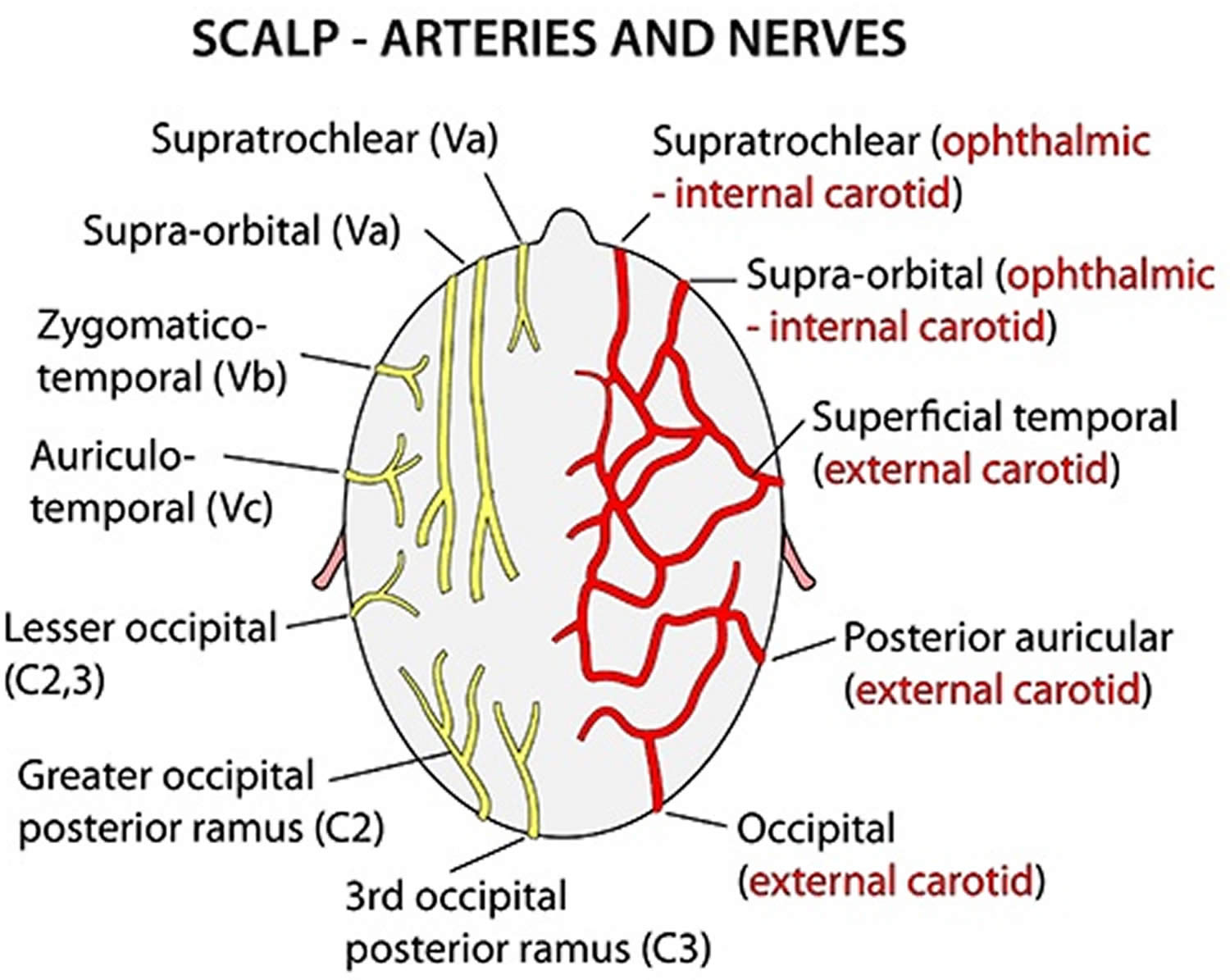
Footnotes: Illustration includes supratrochlear nerve, supraorbital nerve, zygomaticotemporal nerve, auriculotemporal nerve, lesser occipital nerve, greater occipital nerve, supratrochlear artery, supratorbital artery, zygomaticotemporal artery, superficial temporal artery, posterior auricular artery, and occipital artery.
[Source 24 ]Figure 4. Subgaleal hemorrhage
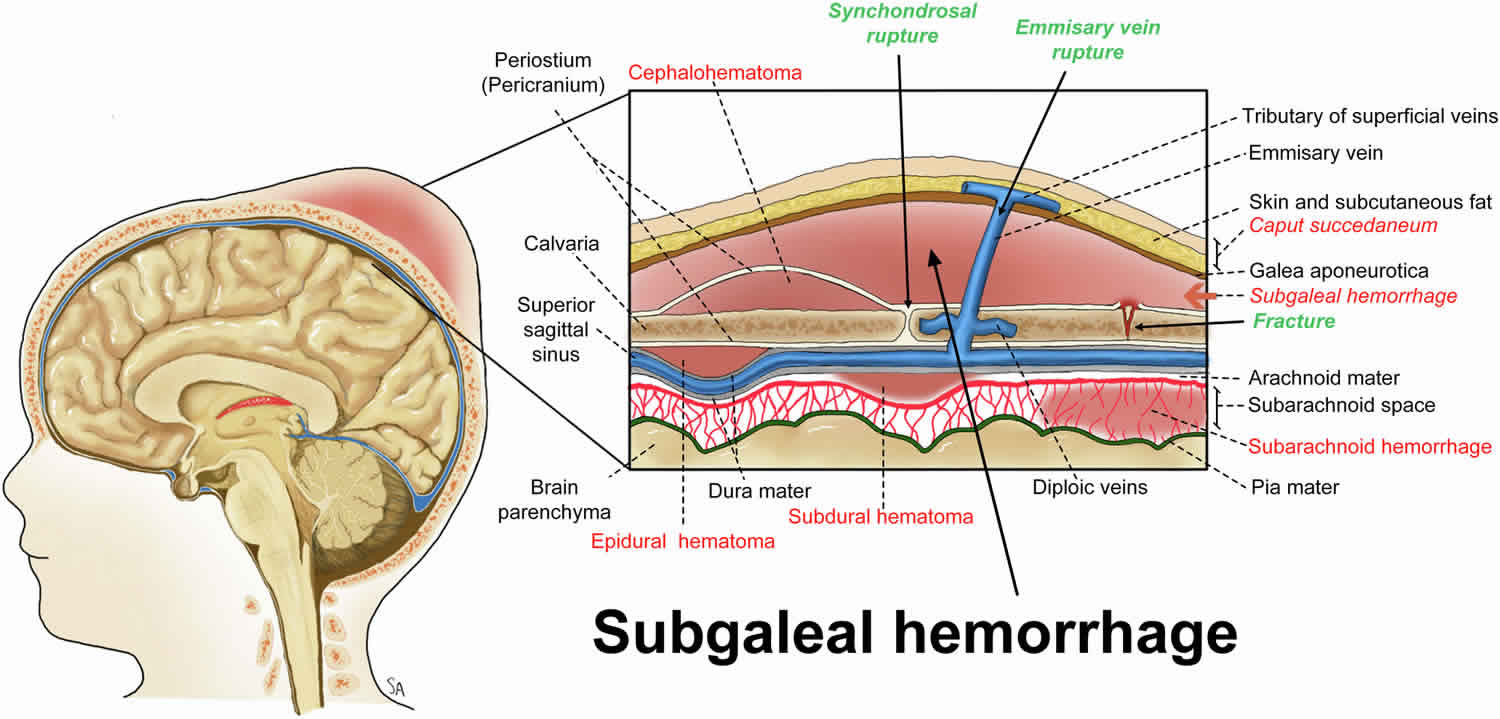
Figure 5. Hemorrhages by location within the different layers of the scalp (right of image) and meninges (left of image)
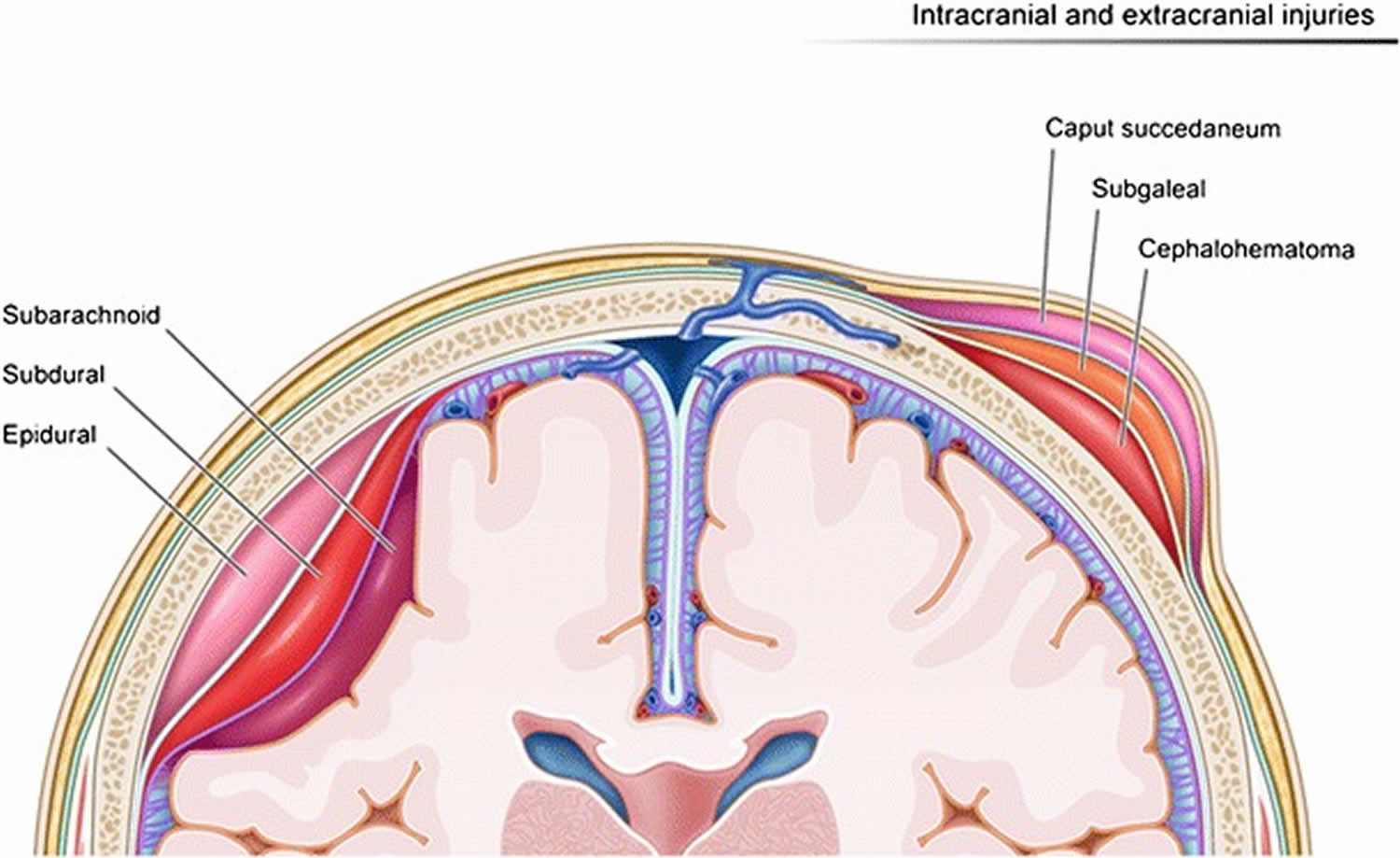
Footnote: Caput succedaneum is collection within the subcutaneous fibrofatty tissues superficial to galea aponeurosis. Cephalohematoma is bleeding into the fetal scalp that is located in the subperiosteal space.
Figure 6. Subgaleal hematoma CT scan
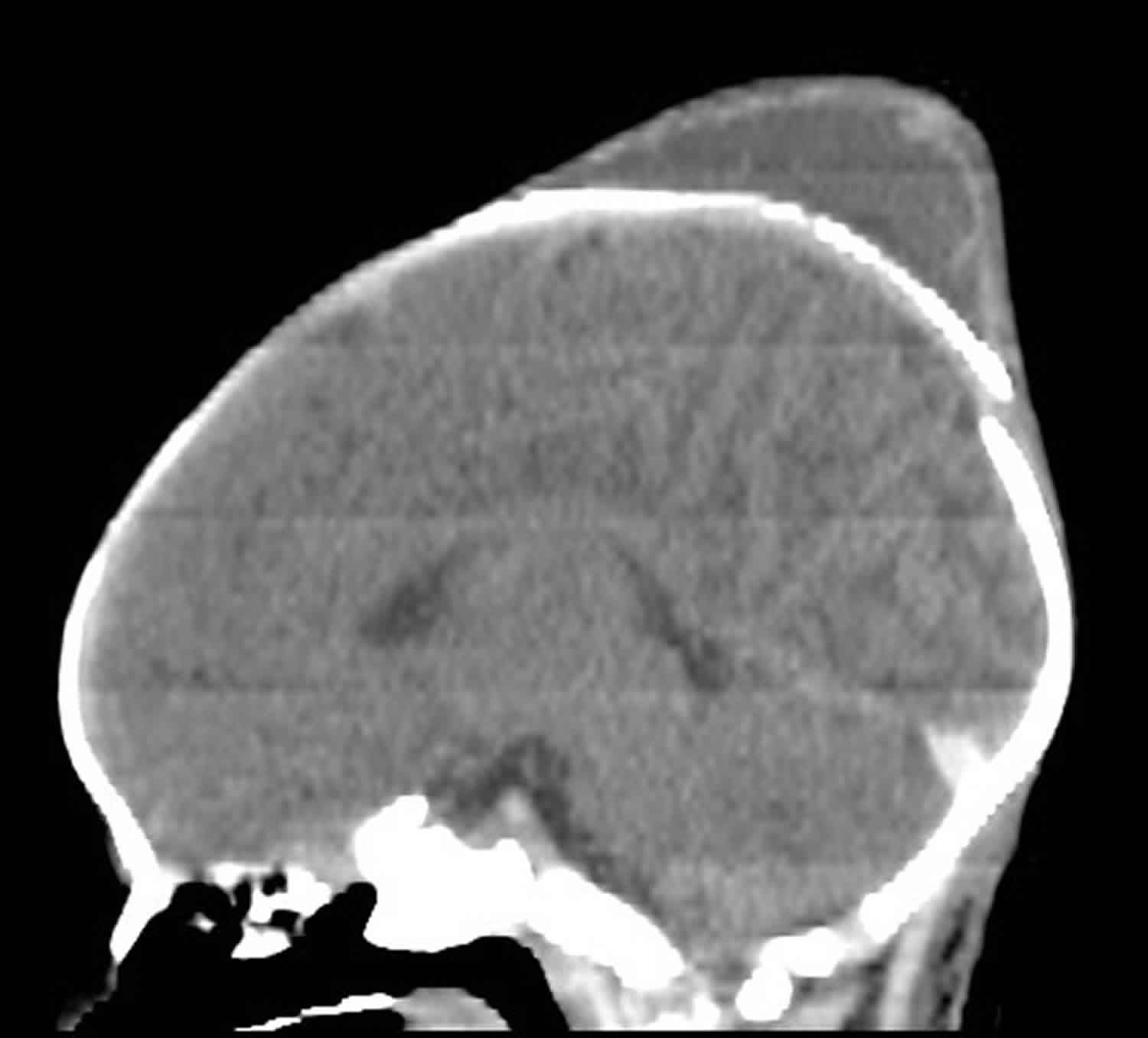
Footnotes: A 2 day old infant with abnormal head shape and swelling after vacuum delivery at the hospital. CT head without contrast showed a large mainly left-sided subgaleal hematoma with smaller contralateral extension to the right side. It extends to the right parietal region exceeding the sagittal suture. Crossing the suture line is the hallmark and differentiating point of subgaleal hematoma from cephalohematoma. A cephalohematoma will remain confined to the skull and will not cross suture lines 25. It shows fluid/fluid level likely to be blood degradation on the left side of the scalp. Ill-defined hyperdensities are seen in the posterior fossa and occipital lobes suggesting subarachnoid bleed.
[Source 26 ]Figure 7. Subgaleal hematoma after head trauma
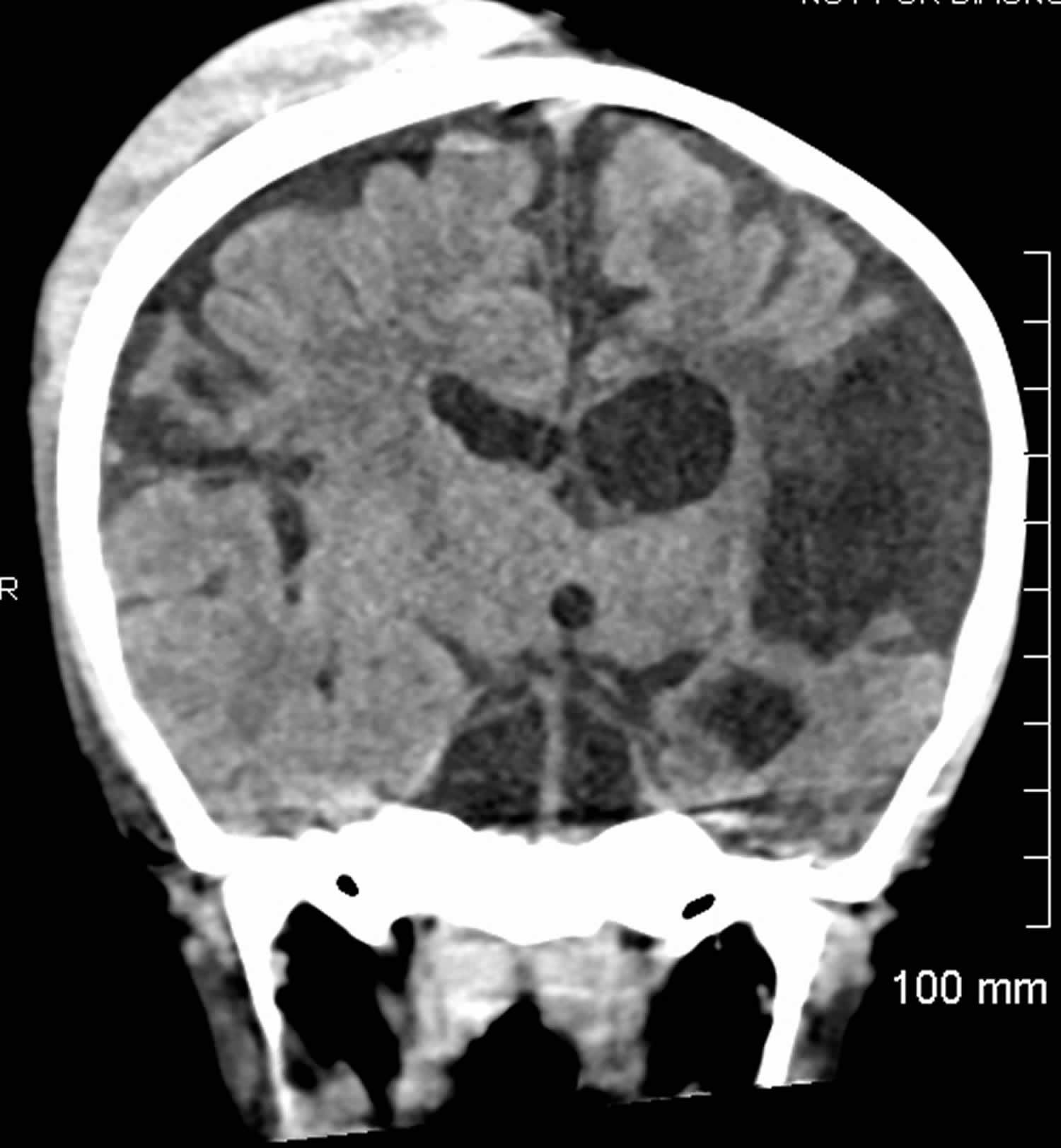
Footnotes: A 5 year old boy had a fall one day ago, followed by headache, altered mental status, and scalp swelling. No vomiting, loss of consciousness or seizures. Coronal view of the head computed tomography scan without contrast revealing a large right-sided subgaleal hematoma without any underlying skull fracture. No recent intracranial hemorrhage, mass effect or midline shift. Old ischemic insult in the left cerebral hemisphere with ex vacuo dilatation of ipsilateral lateral ventricle. Incidental finding of parietal foramina.
[Source 27 ]Who does a subgaleal hemorrhage affect?
Subgaleal hemorrhage can affect any baby born via vaginal delivery, forceps delivery and cesarean section (C-section) and it is most frequently associated with the rotation and traction forces applied with a vacuum assisted birth. Subgaleal hemorrhage is more common to happen if your baby isn’t safely coming down your birth canal and your obstetrician needs to use tools like a vacuum or forceps to help during your baby’s delivery. Over the past 3 decades, increasing use of vacuum assisted births has resulted in an increase in the prevalence of subgaleal hemorrhage 12. Other risk factors for subgaleal hemorrhage include:
- Nulliparity (a woman who has never given birth to a live baby), 5-minute Apgar score < 8, cup marks on the sagittal suture, leading edge of cup < 3 cm from anterior fontanelle or failed vacuum extraction were significant risk factors for subgaleal hemorrhage.
- Macrosomia (a baby with excessive birth weight, often defined as over 8 pounds and 13 ounces or >4000 g at birth), neonatal coagulopathy (Vitamin K deficiency, Hemophilia A [factor VIII deficiency], Hemophilia B [factor IX deficiency]), low birthweight (baby weighing less than 5 pounds and 8 ounces or <2,500 grams at birth), male sex (2:1 to 8:1), need for resuscitation at birth and cord blood acidosis, fetal malpresentation.
How common is a subgaleal hemorrhage?
Subgaleal hemorrhages are rare and occur about 4 times out of every 10,000 vaginal deliveries when tools aren’t used and is rarely reported in non-traumatic cesarean sections 28. Subgaleal hemorrhage most commonly occurs after vacuum-assisted and forceps delivery, but may also be seen following head trauma or minor head trauma such as hair braiding or hair pulling or occur spontaneously because of bleeding disorders or rupture of arteries or arteriovenous fistulas 13, 14, 15, 16, 17, 18, 19, 20, 21, 22. The rate of subgaleal hemorrhage occurrence with vacuum extraction is as high as 89% of cases, with about 60 cases out of 10,000 deliveries that use a vacuum extractor 29, 25. In patients with intracranial hemorrhage or skull fractures, the incidence of subgaleal hemorrhage is increased 25. Boo et al 30 reported a 21% incidence of subgaleal hemorrhage following vacuum extraction in a Malaysian hospital where a formal surveillance program for subgaleal hemorrhage was in place. The diagnosis of subgaleal hemorrhage was made at a median of 1 hour of age, and the mortality of subgaleal hemorrhage in this series was only 2.8% 30.
How long does a subgaleal hemorrhage last?
After treatment, your baby’s subgaleal hemorrhage symptoms will resolve within two to three weeks. Your baby’s doctor will need to closely monitor your baby’s health after treatment to make sure there weren’t any complications from the treatment and that the swelling goes away and your baby’s organs are properly functioning.
Subgaleal hemorrhage newborn causes
Subgaleal hemorrhage in newborn is most common after a vacuum extractor assisted vaginal delivery, but may also be seen following head trauma or minor head trauma such as hair braiding or hair pulling or occur spontaneously because of bleeding disorders or rupture of arteries or arteriovenous fistulas 13, 14, 15, 16, 17, 18, 19, 20, 21, 22. The vacuum, which connects to your baby’s head, can pull the skin on their scalp away from their skull. This can loosen the connective tissue in the subgaleal space of your baby’s head, allowing blood to accumulate outside of their skull. Bleeding occurs as a result of rupture to emissary veins which drain the baby’s scalp veins into the dural sinuses. If too much blood gathers in the area of the skull with loose connective tissue, it could be life-threatening for your baby. Due to being superficial to the periosteum, subgaleal hematomas are able to cross suture lines and surround the entire skull.
Subgaleal hemorrhage causes:
- Operative vaginal delivery: The most significant risk factor, especially using a vacuum extractor.
- Other birth complications: It can also occur following forceps delivery, normal vaginal birth, or cesarean section.
- Ruptured emissary veins: The bleeding originates from the rupture of emissary veins, which connect the scalp veins to the dural venous sinuses.
Sometimes, things don’t go as planned during a vaginal delivery. Subgaleal hemorrhages most often occur if your obstetrician needs to use tools, like a vacuum extractor or forceps, to assist your baby out of your birth canal during a difficult labor process. Your obstetrician will decide to use tools to assist if:
- Your baby’s head or body is too large to fit through your pelvis (cephalopelvic disproportion).
- Your baby isn’t coming down your birth canal safely (fetal dystocia).
- Your baby’s size is large (macrosomia).
- Your labor fails to progress after more than 20 hours (prolonged labor).
- Your labor moves quickly and your baby is ready to be born within three hours of contractions (precipitous labor).
Risk factors for subgaleal hemorrhage
Risk factors for subgaleal hemorrhage may include:
- Vacuum extraction. Subgaleal hemorrhage is often preceded by a difficult vacuum extraction with either incorrect positioning of the cup, prolonged extraction time (>20 minutes), >3 pulls or >2 cup detachments or failed vacuum extraction. Boo and colleagues 30 also showed that nulliparity (a woman who has never given birth to a live baby), 5-minute Apgar score < 8, cup marks on the sagittal suture, leading edge of cup < 3 cm from anterior fontanelle or failed vacuum extraction were significant risk factors for subgaleal hemorrhage.
- Maternal factors: Premature rupture of membranes (when the amniotic sac breaks before labor begins) >12 hours, maternal exhaustion and prolonged second stage, previous high or mid cavity forceps delivery.
- Neonatal factors: Macrosomia (a baby with excessive birth weight, often defined as over 8 pounds and 13 ounces or >4000 g at birth), neonatal coagulopathy (Vitamin K deficiency, Factor VIII deficiency [hemophilia A], Factor IX deficiency [hemophilia B]), low birthweight (baby weighing less than 5 pounds and 8 ounces or <2,500 grams at birth), male sex (2:1 to 8:1), low Apgar score (< 8 at 5 minutes), need for resuscitation at birth and cord blood acidosis, fetal malpresentation.
Subgaleal hemorrhage newborn prevention
It’s difficult to prevent subgaleal hemorrhage from occurring because it’s the result of a difficult vaginal delivery process that often isn’t identifiable until you’re in labor. During prenatal ultrasounds, your obstetrician will examine your baby’s position and assess whether or not a vaginal delivery is the safest option for both you and your baby.
Vacuum extraction is absolutely contraindicated in the following situations:
- Less than 34 weeks gestation and relatively contraindicated at < 36 weeks, where shearing forces are more likely to be associated with tearing of fragile blood vessels resulting in excessive bleeding.
- Among infants diagnosed or suspected of having a bleeding disorder, such as hemophilia, or thrombocytopenia of any cause (e.g. alloimmune disease).
The importance of adequate training and supervision in vacuum delivery should emphasized. To minimize the risk of subgaleal hemorrhage, shearing forces on the scalp should be minimized. This includes placing the center of the cup over the flexion point which is situated on the sagittal suture three centimeters (3 cm) in front of the posterior fontanelle and six centimeters (6 cm) from the anterior fontanelle 23:
- (A). Cup placement should be:
- Placed evenly across the sagittal suture, rather than being applied to one or other parietal bone to avoid asynclitism with traction.
- The edge of the cup should be placed at least 3 cm from the anterior fontanelle to avoid extension of the fetal head during traction (assuming a standard 6 cm cup is being used).
- Appropriate cup placement may be impossible if there is significant deflexion or asynclitism of the head and a “large soft-stemmed” device is being used, because it cannot be placed
sufficiently posteriorly.
- (B). Traction should be steady, applied only with contractions and only with maternal effort.
- (C). Adequate descent should be verified (with the non-pulling hand) during each pull.
- (D). Traction should not be unduly prolonged.
Experts vary in the maximum time allowed, number of pulls and number of allowable cup detachments.
- Time. Vacca 31 suggests an upper limit of 20 minutes from cup application. Where delivery is not imminent after 15 minutes, operators should evaluate whether further traction is warranted, and consider recourse to cesarean section. It should be noted that where the head is deeply engaged in the maternal pelvis (and macrosomia is not anticipated), that completion of vaginal delivery by vacuum extraction or forceps may still be safer than a cesarean section.
- Number of pulls. Many experts suggest a maximum of three pulls (defined as three contractions, even if there are multiple maternal ‘pushes’ within each contraction), although several more pulls may be acceptable if the head has descended to the level of the perineum especially if delivery is attempted without an episiotomy 31.
- Cup detachments. Cup detachment should not be regarded as a safety feature of the vacuum extractor, as the rapid decompression may result in vessel damage and predispose to subgaleal hemorrhage. The acceptable number of detachments will depend on whether detachment was due to equipment failure, or to poor application and/or excessive traction. Two detachments, but certainly no more than three, would generally be considered acceptable, but re-application of the cup should only be considered where there has been definite progress with preceding pulls, or the head is on the perineum.
Subgaleal hemorrhage newborn signs and symptoms
After your baby is born, symptoms of a subgaleal hemorrhage will appear. Approximately 6% of subgaleal hemorrhage cases are asymptomatic, 15-20% are mild, 40-50% are moderate and 25-33% are severe.
Symptoms of a subgaleal hemorrhage include:
- Bruising on the skin.
- Swelling on baby’s head that has a liquid-like movement (boggy swelling) due to internal bleeding that can cross suture lines and may extend into the baby’s neck. Palpation of the scalp has been described as a leather pouch filled with fluid.
- This is in contrast to a cephalohematoma which remains confined to the skull and does not cross suture lines.
- Increasing head circumference. Your baby’s head circumference may increase over time. Massive subgaleal hematoma should be considered in cases where children’s head circumference increases rapidly, with or without a clear history of trauma and the presence of any possible risk factors.
- As the hemorrhage progresses, elevation and displacement of the ear lobes and peri orbital edema (puffy eyelids) can be observed.
- Signs of blood loss: Pallor, lethargy, poor feeding.
- Irritability and pain on handling will be noted.
- Fast heart rate (tachycardia).
- Low blood pressure (hypotension).
- Pale skin tone (pallor).
- Reduced levels of hemoglobin and hematocrit in their blood due to major blood loss.
- Days later bruising appears behind the ears and or the eyelids.
Life-threatening symptoms occur in less than 25% of all cases of a subgaleal hemorrhage and include:
- Signs of shock: rapid heart rate (tachycardia) with heart rate >160 beats per minute, rapid breath with respiratory rate > 60 breaths per minute and abnormally low muscle tone (hypotonia).
- Excessive internal bleeding or clotting (bleeding disorder).
- Extensive fluid loss when their heart cannot pump enough blood throughout their body (hypovolemic or hemorrhagic shock).
- Difficulty breathing (respiratory distress).
- Lack of oxygen to your baby’s brain during birth (intrapartum hypoxia).
- Organ failure.
As blood loss can be massive before hypovolemia is recognized, subgaleal hemorrhage can be a devastating and potentially fatal result of birth trauma.
Subgaleal hemorrhage complications
Subgaleal hemorrhage is a medical emergency requiring immediate and aggressive treatment to prevent or reduce mortality and morbidity. Early and close monitoring of vital signs and head circumference is crucial, especially in newborns with risk factors like assisted delivery with vacuum or forcep.
Subgaleal hemorrhage complications include hypovolemic shock, acute anemia, and bleeding disorder due to significant blood loss, which can lead to death if not treated promptly. Associated complications can include neurological damage, such as cerebral palsy and brain damage, especially if there are also intracranial hemorrhages 5.
Immediate and life-threatening complications
- Hypovolemic shock: The most serious complication, caused by the rapid and extensive loss of blood volume into the subgaleal space, which can be life-threatening.
- Acute anemia: Significant blood loss leads to a dangerously low red blood cell count, affecting the body’s ability to carry oxygen.
- Bleeding disorder: The blood’s ability to clot is severely impaired, often leading to DIC (disseminated intravascular coagulation).
Airway compression
Airway compression is a rare complication of a traumatic subgaleal hematoma. Nichter et al 32 described a 12-year-old healthy child who suffered a mild blow to the head leading to a massive hematoma of the head and neck resulting in airway compression. Emergency tracheostomy and surgical drainage was required, with concern for impending skin necrosis 32. In their report, the mechanism leading to the massive swelling remained unclear, but the hypothesis was that the attachment of the galea to the zygomatic arch can be delicate and a large hematoma could cross this boundary. The patient described in their report had a favorable outcome at twelve months follow up with only spotty hypopigmentation in the forehead region.
Orbital compartment syndrome
Orbital compartment syndrome has also been described as a complication of subgaleal hematoma, with extension of the hematoma to the orbital subperiosteum 33, 34, 35, 36, 37, 38, 39, 40. Individuals usually present with a history of head trauma and progressive bulging or protruding of one or both eyeballs (exophthalmia), blurred vision, drooping of the upper eyelid (ptosis), and pain. In such cases, prompt surgical drainage of the hematoma may be required, as blindness secondary to increased intraocular pressure is a possible outcome of untreated orbital compartment syndrome.
Infection
Infection of subgaleal hematomas secondary to a scalp laceration during instrumented delivery has been well described in the neonatal period 41. In older children, subgaleal hematomas can also get infected through local spread of bacteria, but hematogenous dissemination during an upper respiratory infection has also been reported. Barry et al 41 reported a healthy 8-month-old girl who presented with an infected subgaleal hematoma following a minor fall. Physical examination revealed no scalp laceration, yet cultures of the hematoma grew Streptococcus pneumoniae. The origin of the infection was hypothesized to be hematogenous spread of Streptococcus pneumoniae colonizing the nasopharynx, through one of the anastomoses of the facial vascular system. The patient underwent four weeks of intravenous antibiotics regimen before hospital discharge.
Need for transfusion
It is worth noting that even though the relative volume of blood in traumatic hematomas is usually less important than subgaleal hemorrhage in newborns, transfusion might be needed in some cases 32, 22. Scheier et al 22 described a case requiring a blood transfusion; a 10-year-old girl presented with a subgaleal hematoma following non accidental hair pulling. The patient underwent surgical drainage (250 ml of blood), and a transfusion was required for a hemoglobin nadir of 7.1 g/L, associated with tachycardia and fatigue. The outpatient follow-up showed no coagulopathy and no recurrence of the hematoma.
Other potential complications
- Neurological damage: In severe cases, especially those with associated intracranial hemorrhage, there is a risk of neurological deficits.
- Brain damage: This can manifest as cerebral palsy, seizure disorders, hydrocephalus, intellectual disabilities, and developmental delays.
- Hyperbilirubinemia: The breakdown of red blood cells from the hemorrhage can increase bilirubin levels, potentially leading to jaundice.
- Metabolic acidosis: An imbalance in the body’s pH level can occur.
- Infection: Although rare, the hematoma can become a site of infection, requiring more complex treatment.
- Death: If left untreated, severe blood loss and shock can be fatal.
Subgaleal hemorrhage newborn diagnosis
After your baby is born, your baby’s doctor will carefully examine your baby for physical symptoms of subgaleal hemorrhage, like pale skin, swelling of their scalp and bruising. If your baby’s doctor suspects a subgaleal hemorrhage, your baby’s doctor will order an imaging test, like an ultrasound, CT scan, MRI or an X-ray of your baby’s head to examine the cause of bleeding beneath your baby’s scalp skin.
If your doctor used a vacuum extractor to help deliver your baby, your baby need be closely monitored in the nursery even if your baby doesn’t present any immediate physical signs of a subgaleal hemorrhage because blood accumulation in the subgaleal area of the scalp, along with skin discoloration that indicates tissue damage can happen over time within an hour to 72 hours after your baby is born.
Level 1 Neonatal Surveillance
Indication: Minimum surveillance regimen for all infants delivered by instrumental delivery or second-stage cesarean section.
Protocol:
- Baseline set of post-delivery observations including activity, color, heart rate and respiratory rate at one hour of age.
- Hats and bonnets should be avoided or removed frequently, so that changing head shape or size is noted.
- Changing head circumference and/or scalp appearance is crucial to early diagnosis of subgaleal haemorrhage and should immediately prompt escalation to ‘Level 2’ surveillance.
- Concerns regarding neonatal behavior (poor feeding, poor activity, pallor) should prompt a further full set of observations, and institution of ‘Level 2’ surveillance.
Level 2 Neonatal Surveillance
Indication: One or more of the following:
- Total vacuum extraction time > 20 minutes and/or > 3 pulls and/or > 2 cup detachments.
- 5 minute Apgar score < 7.
- At clinician request (e.g. if the delivery was felt to have been otherwise ‘difficult’ or the cup placement was found to be paramedian or non-flexing).
- Level 1 neonatal surveillance observations are causing concern such as diffuse boggy head swelling, or increasing head circumference.
Protocol:
If Level 2 surveillance established at delivery, neonatal blood should be taken for assessment of:
- Acid base status (cord pH and/or lactate levels).
- Hematocrit and platelet count.
- Formal neonatal observations for subgaleal hemorrhage should continue for at least the first 12 hours of life. The median time of diagnosis of subgaleal hemorrhage in the study of Chang et al 11 was 7.8 hours of life.
- Hourly for the first 2 hours of life, and then 2-hourly for a further 6 hours. A pulse oximeter on the postnatal ward may assist staff with accurate recording of heart rate, so that the onset of
progressive tachycardia may be more easily recognized. - These infants should have a full set of observations performed (activity, colour, heart rate, respiratory rate, review of head size (formal measurement of head circumference) and shape
for location and nature of swelling).
Level 3 Neonatal Surveillance
Indications:
- Where there is a clinical suspicion of subgaleal hemorrhage immediately following birth.
- Where abnormalities are noted on Level 2 surveillance.
Protocol:
- The infant should be reviewed by a pediatrician. These infants will likely be admitted to the special care unit/nursery, with institution of resuscitation (if necessary) and further laboratory
assessment including hematocrit, platelet count and coagulation profile.
Subgaleal hemorrhage newborn differential diagnosis
A thorough history and physical should be completed on every neonate that presents with scalp swelling to differentiate subgaleal hemorrhage from caput succedaneum, a benign self-resolving condition and from more life-threatening causes of scalp swelling that require closer monitoring and further management. Other common causes of neonatal scalp swelling that present similarly include but are not limited to:
- Caput succedaneum is a common benign boggy diffuse swelling with poorly defined margins that is observed on an infant’s scalp shortly after vaginal birth, which can make baby’s head appearing cone-shaped. Caput succedaneum is associated with serosanguinous and/or hemorrhagic fluid collection above the epicranial aponeurosis (a strong, large flat tendon sheet that forms the middle, or third, layer of the scalp) and beneath the overlying skin of the scalp 42. Caput succedaneum is observed on a newborn’s scalp shortly after delivery, is poorly defined and crosses suture lines and resolves on its own within a few days without long-term effects, although it can increase the risk of jaundice 42. Caput succedaneum is a birth-related trauma to the baby’s scalp due to molding of the baby’s head during vaginal birth. During childbirth (vaginal birth), the baby’s head is subjected to pressure in the mother’s birth canal by both the uterine and vaginal walls as it passes through the cervix. Caput succedaneum is more often associated with a prolonged labor in vertex delivery. Vertex delivery refers to a vaginal birth where the baby is positioned head-first, with the back of the baby’s head called the “vertex” entering the birth canal first, and the baby’s chin tucked to its chest 43. Vertex delivery is the most common and safest presentation for birth, as it presents the smallest part of the baby’s head to the mother’s pelvis 43.
- Cephalohematoma is a collection of blood or hematoma between the scalp and the skull periosteum, located in the subperiosteal space and as such, is contained anatomically to a single skull bone, typically caused by ruptured blood vessels during childbirth, and it usually resolves on its own within a few weeks to months 44, 45, 46, 47. Cephalhematoma usually involves the parietal or occipital bone, sharply limited by the margins of the bone and does not cross the suture lines 48. During the birthing process, shearing forces on the skull and scalp result in the separation of the periosteum from the underlying skull bone, resulting in the subsequent rupture of emissary or diploic veins 49. Over time, the body resorbs the blood. Depending on the size, most cephalohematomas take two weeks to three months to disappear completely. If the area of bleeding is large, some babies may develop jaundice as the red blood cells break down or anemia (a condition of not having enough healthy red blood cells or hemoglobin to carry oxygen to the body’s tissues).
- Subdural hemorrhage refers to hemorrhage associated with birth trauma that occurs between the dura and arachnoid space 50, 51.
Subgaleal hemorrhage newborn treatment
Symptomatic subgaleal hemorrhage is a medical emergency with a high morbidity and mortality. If your baby’s doctor diagnoses your baby with a subgaleal hemorrhage, she/he will immediately begin treatment to restore blood volume in your baby’s body through blood and plasma transfusions in the newborn intensive care unit (NICU). Intramuscular vitamin K prophylaxis should be encouraged in all neonates as soon as practicable after birth, but this is particularly important for babies that have had an instrument assisted birth. In rare adult subgaleal hemorrhage cases, aspiration may be considered, but the focus for newborns with subgaleal hemorrhage is on immediate resuscitation and blood and plasma transfusions to prevent hypovolemic shock.
Your baby’s doctor will closely monitor your baby’s vital signs and blood levels to verify that their hemoglobin and hematocrit counts are where they’re supposed to be and not too low. Your baby’s doctor will also perform hourly measurement your baby’s head circumference to check to make sure the swelling is decreasing and not increasing in size.
If the subgaleal hemorrhage is severe and treatment with blood and plasma transfusions isn’t adequate, emergency surgery on the subgaleal area of their scalp will be necessary to stop the internal bleeding.
Drainage
Surgical drainage may be necessary in some cases, after weighing the risks and benefits of the procedure. Drainage however carries a risk of complications, particularly infection, as emissary veins communicate with the dural sinuses.
Subgaleal hematomas might also lead to calcification, motivating drainage to avoid such complications. In rare cases, calcifications can lead to cranial deformation requiring reconstructive surgery, especially in patients with hematologic disease such as Kasabach-Merrit phenomenon, also known as hemangioma with thrombocytopenia, a rare disease, usually of infants, in which a vascular tumor leads to decreased platelet counts and sometimes other bleeding problems 52, 53.
Concern for potential development of calcifications is however not a criterion for drainage, as calcifications are not prevalent, particularly in individuals with no underlying disease. The decision to surgically treat hence depends on patient risk factors, symptoms intensity and evolution, and complications. A similar approach is also described in adult studies and reports 54.
When calcifications or complications are present, however, surgical drainage and evacuation may be warranted. Edmondson et al 55 report a case of a 16-year-old boy who presented with a large subgaleal hematoma following hair braiding 10 days prior, with magnetic resonance imaging revealing areas of calcification. There were no arguments for an underlying vascular malformation, however, because of hematoma extension to the periorbital space, the patient underwent drainage of calcified clots via multiple small incisions.
Embolization
Embolization has also been described after subgaleal hematoma 56, 57. Wajima et al 57 report an otherwise healthy adolescent presenting to the emergency department with two days of headache and no recall of head injury. Swelling of the scalp was noted and a head CT confirmed a subgaleal hematoma. He was drained on initial presentation and returned two weeks later with further scalp swelling and pain. Because of the recurrence of the hematoma, the patient underwent embolization. The outcome was favorable with no recurrence of the hematoma.
How soon after treatment will my baby feel better?
After the internal bleeding caused by the subgaleal hemorrhage stops with treatment, the swelling will decrease and your baby’s symptoms will resolve over a couple of weeks. It’s important to follow up with your baby’s doctor through routine visits during your child’s first year to monitor whether or not the subgaleal hemorrhage caused any other symptoms that will affect your child’s development. If treatment is successful, which occurs in an estimated 75% of subgaleal hemorrhage cases, your child will have a good prognosis and will be able to leave the nursery with you.
Subgaleal hemorrhage prognosis
Subgaleal hemorrhage prognosis is good for over 75% of newborns diagnosed with a subgaleal hemorrhage. Early diagnosis and treatment of the subgaleal hemorrhage leads to the best outcome for your child. Unfortunately, an estimated 10% to 25% of babies born with a subgaleal hemorrhage died during early infancy from their condition due to severe internal bleeding 11, 58, 59, 60.
- Babata, K., Vadlamudi, G., Bailey, N.A. et al. Subgaleal hemorrhage in neonates: a comprehensive review and summary recommendations. J Perinatol 45, 167–179 (2025). https://doi.org/10.1038/s41372-024-02116-w[↩][↩]
- Patchana T, Ghanchi H, Taka T, Calayag M. Subgaleal hematoma evacuation in a pediatric patient: A case report and review of the literature. Surg Neurol Int. 2020 Aug 15;11:243. doi: 10.25259/SNI_207_2020[↩]
- Halim, D., Faried, A. Massive subgaleal hematoma: a potentially fatal rare entity—a case-based review. Childs Nerv Syst 39, 1977–1983 (2023). https://doi.org/10.1007/s00381-023-05933-0[↩]
- Matsumura K, Muto J, Tanaka M, Joko M, Yoshikawa T, Hirose Y. Usefulness of three-dimensional computed tomography venography differentiating calvarium subperiosteal hematoma crossing the suture lines due to hair pulling from subgaleal hematoma: case report and review of the literature. Childs Nerv Syst. 2022 Oct;38(10):2017-2020. doi: 10.1007/s00381-022-05517-4[↩]
- Aubert B, Cadoux M, Sahyoun C. Traumatic subgaleal hematoma drainage in an adolescent: a case report and review of the literature. Front Pediatr. 2023 May 30;11:1182899. doi: 10.3389/fped.2023.1182899[↩][↩]
- Chen C, Xiong Y, Huang X, Guo X, Kang X, Zhou J, Pan Z, Zheng H, Zheng S, Wang L, Hu W, Zhuang L, Zheng F. Subperiosteal/subgaleal drainage vs. subdural drainage for chronic subdural hematoma: A meta-analysis of postoperative outcomes. PLoS One. 2023 Aug 1;18(8):e0288872. doi: 10.1371/journal.pone.0288872[↩]
- Halim D, Faried A. Massive subgaleal hematoma: a potentially fatal rare entity-a case-based review. Childs Nerv Syst. 2023 Jul;39(7):1977-1983. doi: 10.1007/s00381-023-05933-0[↩]
- de Carvalho Barros L, Avancini C, Gurgel RQ, de Amorim RLO, Kolias AG, Paiva WS, Oliveira AMP. Subgaleal/subperiosteal versus subdural drainage for chronic subdural hematoma: a systematic review and meta-analysis. Neurosurg Rev. 2025 May 23;48(1):437. doi: 10.1007/s10143-025-03596-w[↩]
- Song L, Zhou K, Wang C, Chen J, Feng B, Deng X, Du X. Comparison of subperiosteal or subgaleal drainage and subdural drainage in patients with chronic subdural hematoma: A systematic review and meta-analysis. Medicine (Baltimore). 2023 Oct 27;102(43):e35731. doi: 10.1097/MD.0000000000035731[↩]
- Gurses ME, Bahadir S, Bilginer B. Traumatic subgaleal hematoma in patient with Ehlers-Danlos syndrome: A rare case report. Surg Neurol Int. 2022 Jun 23;13:265. doi: 10.25259/SNI_186_2022[↩]
- Chang HY, Peng CC, Kao HA, Hsu CH, Hung HY, Chang JH. Neonatal subgaleal hemorrhage: clinical presentation, treatment, and predictors of poor prognosis. Pediatr Int. 2007 Dec;49(6):903-7. doi: 10.1111/j.1442-200X.2007.02482.x[↩][↩][↩]
- Colditz MJ, Lai MM, Cartwright DW, Colditz PB. Subgaleal haemorrhage in the newborn: A call for early diagnosis and aggressive management. J Paediatr Child Health. 2015 Feb;51(2):140-6. doi: 10.1111/jpc.12698[↩][↩][↩]
- Kato T, Hattori H, Yorifuji T, Tashiro Y, Nakahata T. Intracranial aneurysms in Ehlers-Danlos syndrome type IV in early childhood. Pediatr Neurol. 2001;25:336–9. doi: 10.1016/s0887-8994(01)00315-0[↩][↩][↩]
- Koizumi K, Suzuki S, Utsuki S, Nakahara K, Niki J, Mabuchi I, et al. A case of non-traumatic subgaleal hematoma effectively treated with endovascular surgery. Interv Neuroradiol. 2010;16:317–21. doi: 10.1177/159101991001600315[↩][↩][↩]
- Nakamura M, Yajima J, Oikawa Y, Ogasawara K, Uejima T, Abe K, et al. Vascular Ehlers-Danlos syndrome. All three coronary artery spontaneous dissections. J Cardiol. 2009;53:458–62. doi: 10.1016/j.jjcc.2008.09.007[↩][↩][↩]
- Wimmer PJ, Howes DS, Rumoro DP, Carbone M. Fatal vascular catastrophe in Ehlers-Danlos syndrome: A case report and review. J Emerg Med. 1996;14:25–31. doi: 10.1016/0736-4679(95)02039-x[↩][↩][↩]
- Adeleye A. Subgaleal hematoma extending into the orbit following blunt head trauma as a cause of permanent blindness: A case illustrated review. Niger J Ophthalmol. 2017;25:1.[↩][↩][↩]
- Fujimoto S, Ota T, Mizutani T. Life-threatening large subcutaneous hematoma after minor head trauma: A young female patient who was suspected of having new EhlersDanlos syndrome. Asian J Neurosurg. 2015;10:148–50. doi: 10.4103/1793-5482.154985[↩][↩][↩]
- Edmondson SJ, Ramman S, Hachach-Haram N, Bisarya K, Fu B, Ong J, et al. Hair today; scalped tomorrow: Massive subgaleal haematoma following sudden hair pulling in an adolescent in the absence of haematological abnormality or skull fracture. J Craniofac Surg. 2016;27:1261–2. doi: 10.1097/SCS.0000000000002710[↩][↩][↩]
- Henderson FC, Austin C, Benzel E, Bolognese P, Ellenbogen R, Francomano CA, et al. Neurological and spinal manifestations of the Ehlers-Danlos syndromes. Am J Med Genet Part C Semin Med Genet. 2017;175:195–211. doi: 10.1002/ajmg.c.31549[↩][↩][↩]
- Barry J, Fridley J, Sayama C, Lam S. Infected subgaleal hematoma following blunt head trauma in a child: case report and review of the literature. Pediatr Neurosurg. (2015) 50(4):223–8. 10.1159/000433442[↩][↩][↩]
- Scheier E, Ben-Ami T, Guri A, Balla U. Subgaleal Hematoma from a Carnival Costume. Isr Med Assoc J. 2019 Jun;21(6):422-423. https://www.ima.org.il/FilesUploadPublic/IMAJ/0/363/181657.pdf[↩][↩][↩][↩][↩]
- Royal Australian and New Zealand College of Obstetricians and Gynaecologists. Prevention, Detection and Management of Subgaleal Haemorrhage in the Newborn Royal Australian and New Zealand College of Obstetricians and Gynaecologists. 2009. https://www.ranzcog.edu.au/wp-content/uploads/Subgaleal-Haemorrhage.pdf[↩][↩][↩][↩]
- Tajran J, Gosman AA. Anatomy, Head and Neck, Scalp. [Updated 2023 Jul 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK551565[↩]
- Sharman AM, Kirmi O, Anslow P. Imaging of the skin, subcutis, and galea aponeurotica. Semin Ultrasound CT MR. 2009 Dec;30(6):452-64. doi: 10.1053/j.sult.2009.08.001[↩][↩][↩]
- Subgaleal hematoma. https://radiopaedia.org/cases/subgaleal-haematoma[↩]
- Subgaleal hematoma with orbital extension. https://radiopaedia.org/cases/subgaleal-hematoma-with-orbital-extension-1[↩]
- Wetzel EA, Kingma PS. Subgaleal hemorrhage in a neonate with factor X deficiency following a non-traumatic cesarean section. J Perinatol. 2012 Apr;32(4):304-5. doi: 10.1038/jp.2011.122[↩]
- Plauché WC. Subgaleal Hematoma: A Complication of Instrumental Delivery. JAMA. 1980;244(14):1597–1598. doi:10.1001/jama.1980.03310140055031[↩]
- Boo NY, Foong KW, Mahdy ZA, Yong SC, Jaafar R. Risk factors associated with subaponeurotic haemorrhage in full-term infants exposed to vacuum extraction. BJOG. 2005 Nov;112(11):1516-21. doi: 10.1111/j.1471-0528.2005.00732.x[↩][↩][↩]
- Vacca A. Handbook of Vacuum Delivery in Obstetric Practice. 2nd edition 2003.[↩][↩]
- Nichter LS, Bolton LL, Reinisch JF, Sloan GM. Massive subgaleal hematoma resulting in skin compromise and airway obstruction. J Trauma. (1988) 28(12):1681–3. 10.1097/00005373-198812000-00014[↩][↩][↩]
- Pope-Pegram LD, Hamill MB. Post-traumatic subgaleal hematoma with subperiosteal orbital extension. Surv Ophthalmol. (1986) 30(4):258–62. 10.1016/0039-6257(86)90122-0[↩]
- Lee KS, Bae HG, Yun IG. Bilateral proptosis from a subgaleal hematoma. Case report. J Neurosurg. (1988) 69(5):770–1. 10.3171/jns.1988.69.5.0770[↩]
- Pomeranz AJ, Ruttum MS, Harris GJ. Subgaleal hematoma with delayed proptosis and corneal ulceration. Ann Emerg Med. (1995) 26(6):752–4. 10.1016/S0196-0644(95)70051-X[↩]
- Fujisawa H, Yonaha H, Oka Y, Uehara M, Nagata Y, Kajiwara K, et al. A marked exophthalmos and corneal ulceration caused by delayed massive expansion of a subgaleal hematoma. Childs Nerv Syst. (2005) 21(6):489–92. 10.1007/s00381-004-1054-8[↩]
- Karcioglu ZA, Hoehn ME, Lin YP, Walsh J. Ocular involvement after subgaleal hematoma. J Pediatr Ophthalmol Strabismus. (2008) 12(5):521–3. 10.1016/j.jaapos.2008.03.004[↩]
- Kichari JR, Gielkens H. Massive traumatic subgaleal haematoma. Emerg Med J. (2013) 30(4):344. 10.1136/emermed-2012-201729[↩]
- Jenkins TL, Zheng CX, Murchison AP, Bilyk JR. Orbital compartment syndrome following post-traumatic subgaleal hematoma. Ophthalmic Plast Reconstr Surg. (2017) 33(2):e33–6. 10.1097/IOP.0000000000000684[↩]
- Puri S, Duff SM, Mueller B, Prendes M, Clark J. Hairpulling causing vision loss: a case report. Orbit. (2019) 38(2):162–5. 10.1080/01676830.2018.1459739[↩]
- Barry J, Fridley J, Sayama C, Lam S. Infected Subgaleal Hematoma Following Blunt Head Trauma in a Child: Case Report and Review of the Literature. Pediatr Neurosurg. 2015;50(4):223-8. doi: 10.1159/000433442[↩][↩]
- Jacob K, Hoerter JE. Caput Succedaneum. [Updated 2023 Aug 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK574534[↩][↩]
- Makajeva J, Ashraf M. Delivery, Face and Brow Presentation. [Updated 2024 Nov 25]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK567727[↩][↩]
- Raines DA, Krawiec C, Weisbrod LJ, et al. Cephalohematoma. [Updated 2024 Jun 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470192[↩]
- Ali UA, Norwitz ER. Vacuum-assisted vaginal delivery. Rev Obstet Gynecol. 2009;2(1):5-17. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2672989/[↩]
- Hung TY, Coates E, McAlpine A, Tam J, Goldfarb DM, McDonald PJ, Zelman M, Halverson M, Seaton C. Cephalohaematoma: Not always a benign bump. J Paediatr Child Health. 2022 Jun;58(6):1094-1096. https://doi.org/10.1111/jpc.15769[↩]
- Xi M, Shi H, Zhang G. Management of neonatal cephalohematoma and ossified cephalhematoma -281 cases of personal 10-year experience. Childs Nerv Syst. 2025 Jan 2;41(1):77. doi: 10.1007/s00381-024-06740-x[↩]
- Nicholson L. Caput succedaneum and cephalohematoma: the cs that leave bumps on the head. Neonatal Netw. 2007 Sep-Oct;26(5):277-81. doi: 10.1891/0730-0832.26.5.277[↩]
- Meng A, Purohith A, Huang A, Litvinchuk T. Traumatic Birth Injury in a Term Neonate. Cureus. 2022 Dec 20;14(12):e32737. doi: 10.7759/cureus.32737[↩]
- Shekhar S, Rana N, Jaswal RS. A prospective randomized study comparing maternal and fetal effects of forceps delivery and vacuum extraction. J Obstet Gynaecol India. 2013 Apr;63(2):116-9. doi: 10.1007/s13224-012-0282-1[↩]
- Jayawant S, Parr J. Outcome following subdural haemorrhages in infancy. Arch Dis Child. 2007 Apr;92(4):343-7. doi: 10.1136/adc.2005.084988[↩]
- Hall, G.W. (2001), Kasabach–merritt syndrome: pathogenesis and management. British Journal of Haematology, 112: 851-862. https://doi.org/10.1046/j.1365-2141.2001.02453.x[↩]
- Stalder MW, Dorafshar AH, Redett RJ. Calcified subgaleal hematoma with secondary cranial deformity in a patient with Kasabach-Merritt phenomenon. J Craniofac Surg. (2011) 22(1):208–11. 10.1097/SCS.0b013e3181f753d6[↩]
- Chen CE, Liao ZZ, Lee YH, Liu CC, Tang CK, Chen YR. Subgaleal hematoma at the contralateral side of scalp trauma in an adult. J Emerg Med. (2017) 53(5):e85–e8. 10.1016/j.jemermed.2017.06.007[↩]
- Edmondson SJ, Ramman S, Hachach-Haram N, Bisarya K, Fu B, Ong J, et al. Hair today; scalped tomorrow: massive subgaleal haematoma following sudden hair pulling in an adolescent in the absence of haematological abnormality or skull fracture. J Craniofac Surg. (2016) 27(5):1261–2. 10.1097/SCS.0000000000002710[↩]
- Koizumi K, Suzuki S, Utsuki S, Nakahara K, Niki J, Mabuchi I, et al. A case of non-traumatic subgaleal hematoma effectively treated with endovascular surgery. Interv Neuroradiol. (2010) 16(3):317–21. 10.1177/159101991001600315[↩]
- Wajima D, Nakagawa I, Kotani Y, Wada T, Yokota H, Park YS, et al. A case of refractory subgaleal hematoma in adolescence treated with aspiration and endovascular surgery. Acta Neurochir (Wien). (2017) 159(8):1565–9. 10.1007/s00701-017-3207-z[↩][↩]
- Doumouchtsis SK, Arulkumaran S. Head trauma after instrumental births. Clin Perinatol. 2008;35(1):69–83. viii. doi: 10.1016/j.clp.2007.11.006[↩]
- Gebremariam A. Subgaleal haemorrhage: risk factors and neurological and developmental outcome in survivors. Ann Trop Paediatr. 1999;19(1):45–50. doi: 10.1080/02724939992626[↩]
- Christensen RD, Baer VL, Henry E. Neonatal subgaleal hemorrhage in a multihospital healthcare system: prevalence, associations, and outcomes. e-J Neonatol Res. 2011;1(1):1–8.[↩]





{kind=link}