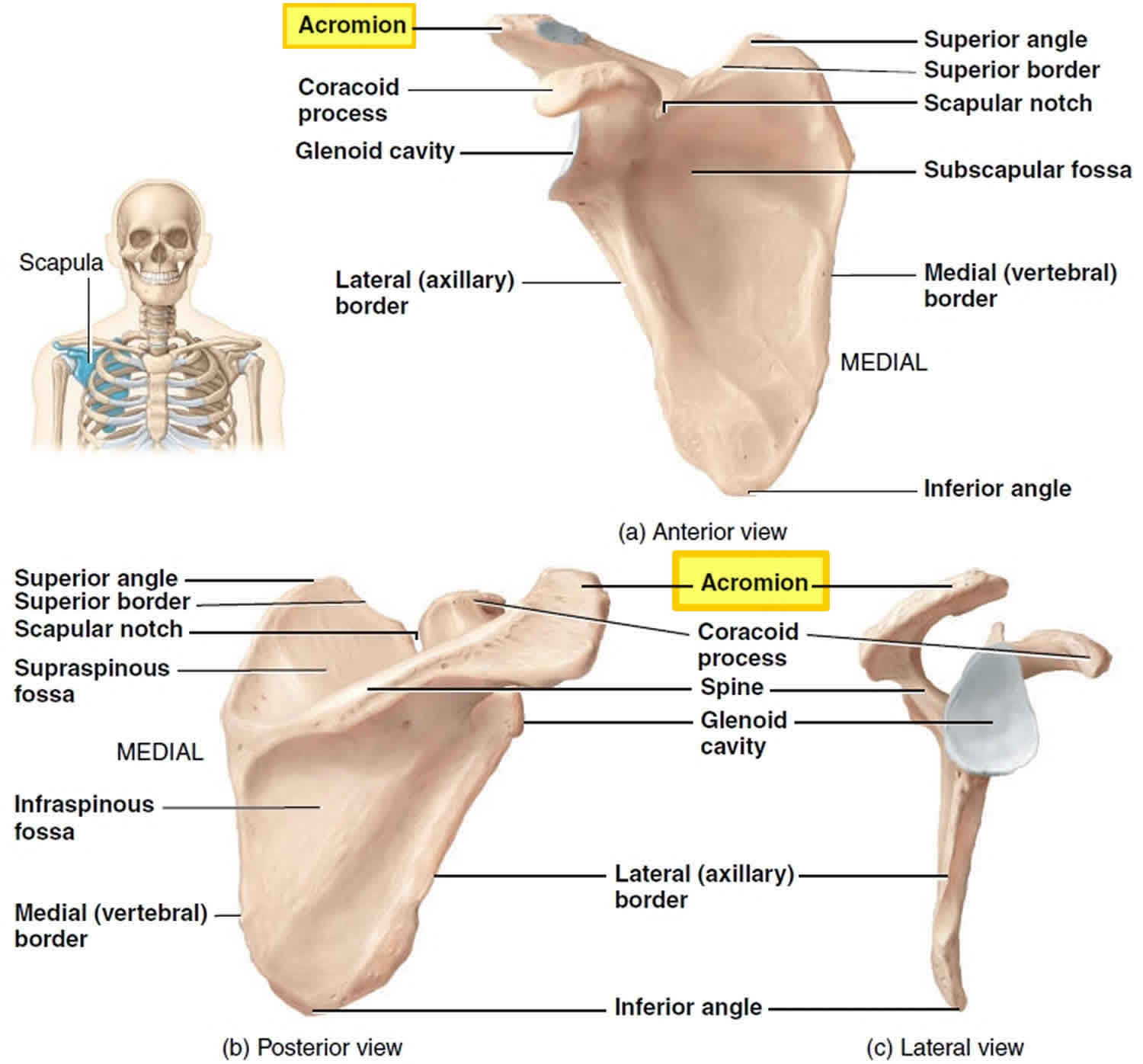
What is the acromion
Acromion is an anterolateral oblong projection of the spine of scapula (shoulder blade) that runs laterally then anteriorly above the supraspinous fossa and is the summit of the shoulder on palpation. The acromion arches over the glenohumeral joint and articulates with the clavicle (collarbone) to form the acromioclavicular joint. Injury to the acromioclavicular joint is a common injury among athletes and young individuals. The acromioclavicular joint receives stabilization from the coracoacromial, coracoclavicular, and super and inferior acromioclavicular ligaments.
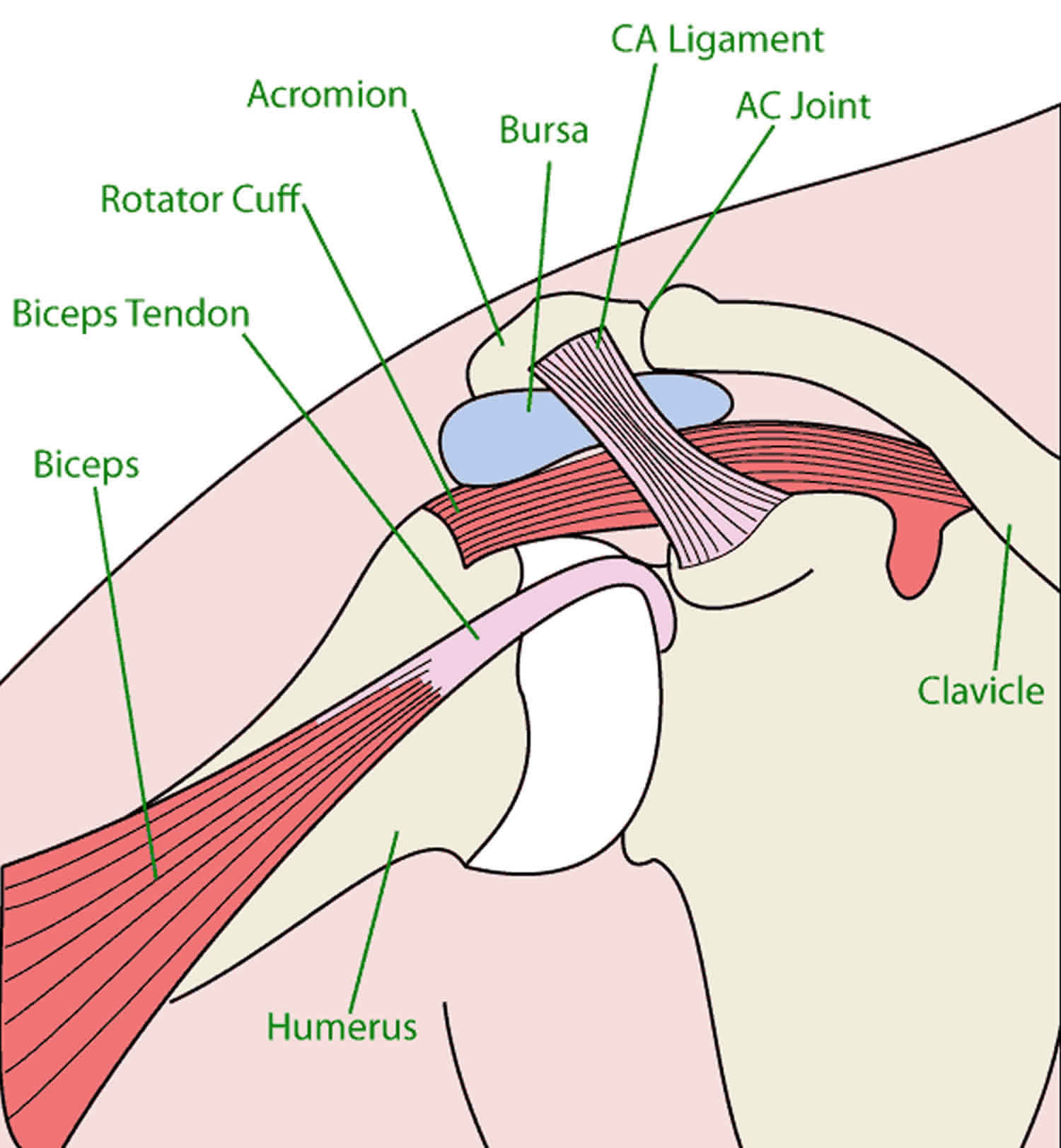
Your shoulder is made up of three bones: your upper arm bone (humerus), your shoulder blade (scapula), and your collarbone (clavicle).
Your arm is kept in your shoulder socket by your rotator cuff. These muscles and tendons form a covering around the head of your upper arm bone and attach it to your shoulder blade.
There is a lubricating sac called a bursa between the rotator cuff and the acromion. The bursa allows the rotator cuff tendons to glide freely when you move your arm. Shoulder impingement is a very common condition that occurs when there is inflammation of the rotator cuff tendons acromion and the sub-acromial bursa (bursitis) around them.
Shoulder impingement is characterized by pain in the shoulder usually going into the upper arm and often down towards your elbow. Shoulder motion is restricted principally on elevating the limb to the side. The pain often prevents you getting your hand behind your back. Lying on your affected shoulder at night often causes pain resulting in you waking. The symptoms can come on acutely for single, or several short episodes. Episodes may become a recurring or constant problem.
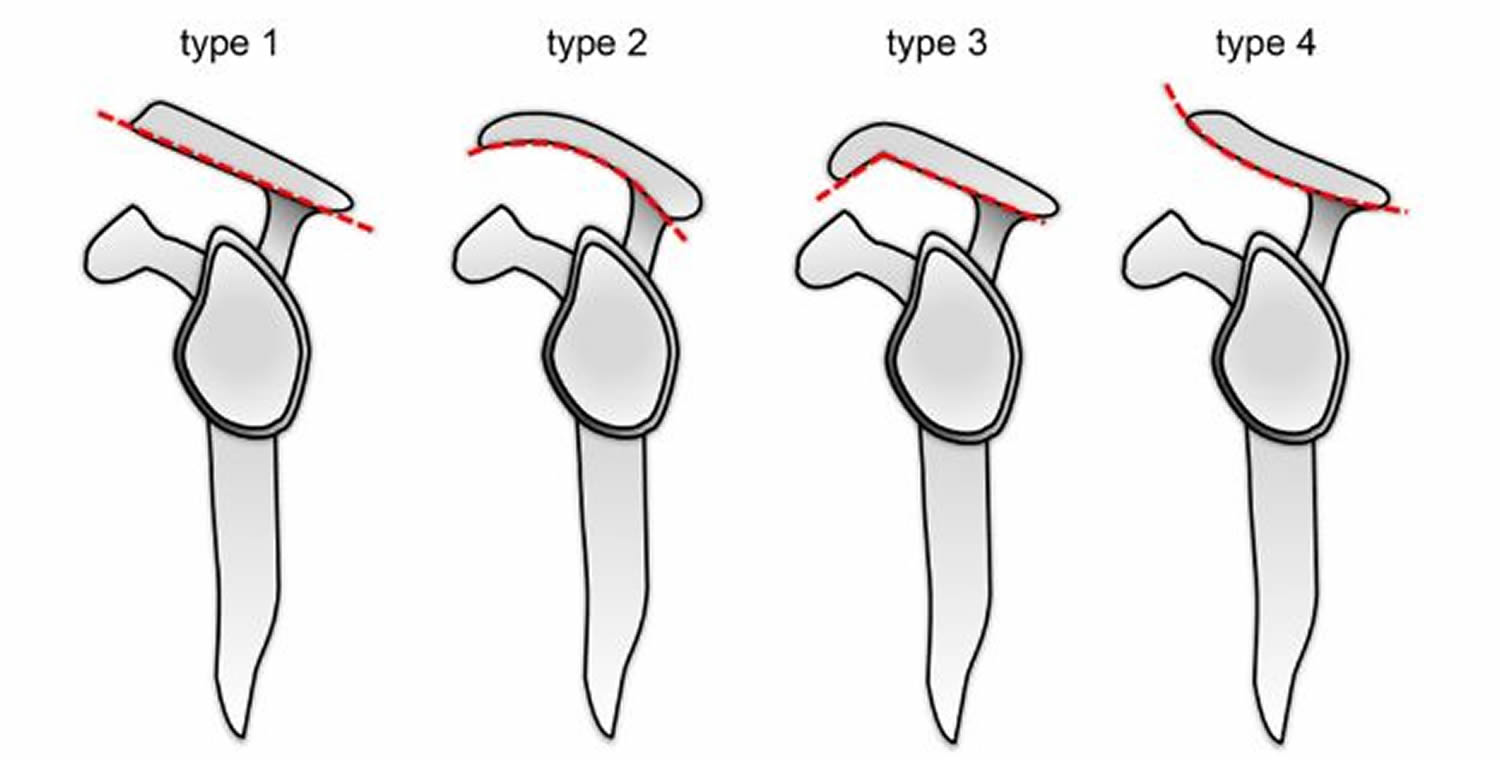
The subacromial space between the acromion and humeral head is narrowed when the shoulder is in certain positions. In subacromial impingement, the rotator cuff tendons and bursa tend to become swollen. In the majority of people the undersurface of the acromion is flat (type 1), but for some people the undersurface can be curved (type 2), or hooked (type 3), with type 2 and 3 acromions reducing the space available for the tendons and the bursa (see Figure 2 below).
The subacromial space may be reduced due to a spur of bone on the front of the acromion, or a thickening of the coracoacromial ligament, or from the rotator cuff becoming less efficient at centring the gleno-humeral joint. Sometimes there may be some mild or modest fraying of the rotator cuff tendon (described as partial or full thickness tear on your ultrasound or MRI report) which may also result in the tendon being bulkier in the subacromial space.
As a result, the rotator cuff tendon and bursa compress in the space, and this causes pain. It is also possible for pain to come from other causes in addition to subacromial impingement such as rotator cuff tears or arthritis.
Figure 1. Shoulder joint
Frequently the symptoms of subacromial impingement are mild or will resolve over some days or weeks without intervention. Restricting activities and using painkillers for a period of time is often all that is required to settle the condition, although it is possible for it to recur in the future.
Should your symptoms worsen or become persistent, treatment would usually consist of a steroid (cortisone) injection into the subacromial space and/or physiotherapy. Steroid injections work by reducing the inflammation and thus the swelling in the subacromial space, thereby gives the bursa and tendon more room. The reduction in swelling may resolve the condition on a long term basis, or relief may only be temporary.
Should a period of rest, steroid injection(s) and physiotherapy fail to provide relief, an operation to make more room in the subacromial space is often a good solution. The procedure is called subacromial decompression or acromioplasty and is carried out under general anaesthetic. During the surgery, a portion of the undersurface of the acromion is removed to create sufficient room for the tendon. Usually, this procedure is undertaken arthroscopically using an arthroscope (telescope) and small shavers (small surgical instruments designed to remove damaged or unwanted tissues) through three small cuts (incisions) around the shoulder.
The risks of this surgery include infection, prolonged stiffness, acromial fracture (rare), nerve and blood vessel injury (rare) and a failure to resolve symptoms. A discussion of surgical risks is within this booklet. Please read that section before your operation.
Acromion types
The shape of the acromion has been initially divided into 3 types (which was known as the Bigliani classification), to which a fourth has been added:
- Type 1 acromion: Flat inferiorly
- Type 2 acromion: Curved – parallel to the humeral head with convex undersurface – considered commonest type
- Type 3 acromion: Hooked – the most anterior portion of the acromion has a hooked shape ,associated with increase incidence of shoulder impingement
- Type 4 acromion: Convex (upturned), this is the most recent classification of acromion process. In type 4 acromion, the undersurface is convex near the distal end. There is no convincing correlation between a type 4 acromion and impingement syndrome exists
Figure 2. Acromion types
Acromion fracture
Acromion fractures are extremely rare. Acromion fractures constitute 8%–16% of scapula fractures 1. Recently, acromion fractures are seen at the rate of 5%–6.9% as the complication of reverse shoulder arthroplasty 2. Acromion fractures may occur as a result of shoulder trauma and overuse injuries. Acromion fractures may occur with glenoid process, scapula or clavicle distal fractures and disruption of superior shoulder suspensory complex 3. There are no common accepted treatment schemes and fixation methods for acromion fractures 4.
In patients with polytrauma, diagnosis and treatment of acromion fractures can be delayed or overlooked 4. In improperly treated acromion fractures; pain, movement restriction, subacromial impingement, rotator cuff injury and symptomatic nonunion can occur 5.
Early surgical intervention to the patient can have a positive effect on fracture healing. Kim et al. 6 compared early and late treated acromion fractures and found out that while all the early surgically treated patients came back to their pre-fracture activities, the rate for late treated patients is 44%. On his study, Hill 7 showed that late treated patients can also get back to their work just as early treated patients do and reported that their shoulder scores are good. In our case, patient with polytrauma got back to his work 8 weeks after surgery and gained his preoperative activities 12 weeks after surgery.
There are three classifications in acromion fractures. Ogawa and Naniwa 8 classified the fractures of spinoglenoid notch lateral as Type 1 and fractures of medial as Type 2. Kuhn 9 used a classification algorithm based on fracture displacement. He classified acromion fractures as follows; Type 1, minimally displaced, Type 2, displaced but do not reduce subacromial space and Type 3, cause a reduction in subacromial space. American Orthopaedic/Orthopaedic Trauma Association (AO/OTA) 10 classification is based on the level of comminution and displacement.
Acromion fractures can be treated with K-wires 11, tension band 12, cannulated screw 13, and plate screw 14. Fixation with K-wires is not recommended because it may cause early implant failure and stable reconstruction may not be achieved after surgery 15. Goss 16 suggests tension band technique and reports good results. Hill 17 applied plate to all acromion fractures in a study carried out with 13 patients and reported that they removed only one plate due to implant irritation. In a recent study that Zhu 18 evaluated an acromion pedicle fracture, he analyzed perpendicular double-plate with a locking system and reported good results. In our study, we chose cannulated screw because the fracture was on the lateral side of acromion and it was not comminuted. Çiçekli et al 4 showed that compression with a good reduction and screw can make the fracture healing complete successfully. It is important to avoid screw penetration into subacromial space during fixation.
In acromion fractures, implant failure can be seen after fixation with K-wire. Irritation and infection can be seen after fixation with plate screw 17. Zhu 19 reports temporary suprascapular nerve entrapment on patients with double-plate.
- Lantry J.M., Roberts C.S., Giannoudis P.V. Operative treatment of scapular fractures: a systematic review. Injury. 2008;39:271–283[↩]
- Crosby L.A., Hamilton A., Twiss T. Scapula fractures after reverse total shoulder arthroplasty: classification and treatment. Clin. Orthop. Relat. Res. 2011;469:2544–2549[↩]
- Mulawka B., Jacobson A.R., Schroder L.K., Cole P.A. Triple and quadruple disruptions of the superior shoulder suspensory complex. J. Orthop. Trauma. 2015;29(June 6:264–270[↩]
- Çiçekli Ö, Akar A, Topçu HN. Displaced acromion fracture: A rare injury, case report. Int J Surg Case Rep. 2017;39:313–316. doi:10.1016/j.ijscr.2017.08.051 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5602832/[↩][↩][↩]
- Lee C.H., Choi Y.A., Lee S.U. Ultrasonographic diagnosis of non-displaced avulsion fracture of the acromion: a case report. Ann. Rehabil. Med. 2015;39, June 3:473–476[↩]
- Kim D.S., Yoon Y.S., Kang D.H. Comparison of early fixation and delayed reconstruction after displacement in previously nondisplaced acromion fractures. Orthopedics. 2010;33:392.[↩]
- Hill B.W., Anavian J., Jacobson A.R., Cole P.A. Surgical management of isolated acromion fractures: technical tricks and clinical experience. J. Orthop. Trauma. 2014;28, May 5:e107–e113[↩]
- Ogawa K., Naniwa T. Fractures of the acromion and the lateral scapular spine. J. Shoulder Elbow Surg. 1997;6:544–548[↩]
- Kuhn J.E., Blasier R.B., Carpenter J.E. Fractures of the acromion process: a proposed classification system. J. Orthop. Trauma. 1994;8:6–13[↩]
- Marsh J.L., Slongo T.F., Agel J. Fracture and dislocation classification compendium—2007: Orthopaedic Trauma Association classification, database and outcomes committee. J. Orthop. Trauma. 2007;21:S1–S133[↩]
- Mehdi Nasab S.A. Isolated displaced fracture of the acromion: a rare case report and the consequence of treatment by open reduction and pin fixation. Arch Trauma Res. 2013;1 Winter 4:184–186.[↩]
- Peckett W.R., Gunther S.B., Harper G.D., Hughes J.S., Sonnabend D.H. Internal fixation of symptomatic os acromiale: a series of twenty-six cases. J. Shoulder Elbow Surg. 2004;13(4):381–385.[↩]
- Mardy A., Mechchat A., El Ghazi A., El Idrissi M., Shimi M., El Ibrahimi A., El Mrini A. Open fracture of the acromion associated with a supraspinatus tendon rupture: an exceptional case report. Pan Afr. Med. J. 2014;26(November 19:325[↩]
- Zhu J., Pan Z., Zheng R., Lan S. Le Perpendicular double-plate fixation with locking system for acromion pedicle fracture. Acta Ortop Bras. 2016;24(March-April (2):107–110[↩]
- Bauer G., Fleischmann W., Dussler E. Displaced scapular fractures: indication and long-term results of open reduction and internal fixation. Arch. Orthop. Trauma Surg. 1995;114:215–219.[↩]
- Goss T.P. The scapula: coracoid, acromial, and avulsion fractures. Am. J. Ortho. (Belle Mead N. J.) 1996;25:106–115.[↩]
- Hill B.W., Anavian J., Jacobson A.R., Cole P.A. Surgical management of isolated acromion fractures: technical tricks and clinical experience. J. Orthop. Trauma. 2014;28(May 5:e107–e113[↩][↩]
- Zhu J., Pan Z., Zheng R., Lan S. Le Perpendicular double-plate fixation with locking system for acromion pedicle fracture. Acta Ortop Bras. 2016;24(March-April 2:107–110[↩]
- Zhu J., Pan Z., Zheng R., Lan S. Le Perpendicular double-plate fixation with locking system for acromion pedicle fracture. Acta Ortop Bras. 2016;24, March-April 2:107–110[↩]





{kind=link}