Contents
- What is adenosine
What is adenosine
Adenosine is a ribonucleoside that is composed of adenine bound to ribose with vasodilatory, antiarrhythmic and analgesic activities. Adenosine treats arrhythmias (uneven heartbeat) and is also used during a heart stress test. Adenosine injection is used in combination with Thallium-201 as a pharmacologic stress agent for myocardial perfusion scintigraphy in patients unable to undergo adequate exercise stress. This medicine works by dilating the arteries (vasodilator) of the heart and increase blood flow to help identify coronary artery disease. Adenosine is to be given only by or under the direct supervision of a doctor.
Adenosine has far-reaching effects as an extracellular signaling molecule inducing vasodilation in most vascular beds, regulating activity in the sympathetic nervous system, having antithrombotic properties, and reducing blood pressure and heart rate 1. Such properties are some of the reasons why adenosine and its derivatives have therapeutic effects in most organ systems.
One of the most common reasons for using adenosine in the cardiovascular system is for the production of vasodilation in the coronary microcirculation to produce hyperemia 2. This property of adenosine to modify microcirculatory function has been used for diagnostic and therapeutic effects for many years and is widely adopted as the gold-standard method of diagnosing ischemia invasively and noninvasively.
Adenosine is a white crystalline powder. Adenosine is soluble in water and practically insoluble in alcohol. Solubility increases by warming and lowering the pH. Adenosine is not chemically related to other antiarrhythmic drugs. Adenosine injection, USP (United States Pharmacopeia) is a sterile, nonpyrogenic solution for rapid bolus intravenous injection. Each mL contains 3 mg Adenosine and 9 mg sodium chloride in water for injection. The pH of the solution is between 4.5 and 7.5.
- Adenosine is used to treat certain types of abnormal heartbeats.
- Adenosine is used during a stress test of the heart.
- Adenosine may be given to you for other reasons. Talk with the doctor.
Adenosine is a naturally occurring endogenous purine nucleoside composed of an adenine molecule attached to a ribose sugar moiety 3 (ribofuranose) via a beta-N9-glycosidic bond (6-amino-9-β-d-ribofuranosyl-9-H-purine). It is the nucleoside base of both adenosine triphosphate (ATP) and the signaling molecule cyclic adenosine monophosphate (cAMP). Adenosine is rapidly transported into vascular endothelial cells and erythrocytes where it is catabolized by adenosine deaminase to inosine 4. Dipyridamole, a commonly used vasoactive medication 5 exerts its effects through inhibition of adenosine deaminase. Adenosine is (re)phosphorylated by adenine kinase forming adenosine monophosphate, which is incorporated into the high-energy phosphate pool 6. Adenosine levels can rise rapidly in ischemic tissue due to adenosine kinase inhibition 3.
Adenosine is also a naturally occurring breakdown product of adenosine triphosphate (ATP), which is hydrolyzed and dephosphorylated to produce adenosine 7. Adenosine may be produced inside the cells (intracellular) by the action of enzyme 5′-nucleotidase on 5′-AMP. On the other hand, adenosine in the extracellular space is formed by the action of enzyme ecto-5′ nucleotidase 8. Apart from a simple degradation product, adenosine produces multiple physiological effects such as regulation of blood flow, heart rate and heart contractility through activation of different adenosine receptors 9. Four types of adenosine receptors, A1, A2A, A2B and A3 have been identified and all are G-protein coupled receptors. The A1 and A3 are Gi-coupled receptors that inhibit adenylyl cyclase activity and cAMP production; whereas, A2A and A2B are Gs-coupled receptors that activates adenylyl cyclase and cAMP production. Furthermore, A2B receptors also couple to Gq proteins to activate phospholipase C 10. Adenosine receptors are widely expressed in the body. The A1 receptors are highly expressed throughout the CNS (central nervous system – brain and spinal cord), heart muscles and in inflammatory cells 11. The A2 receptors are located in pre- and postsynaptic nerve terminals, mast cells, heart (smooth muscle and endothelial cells) and in circulating leukocytes. A3 receptors are found in the heart (endothelial cells of the aorta, smooth muscle cells), kidney, testis, mast cells, eosinophils, neutrophils and in brain cortex 12.
Adenosine triphosphate (ATP) is at the root of all organisms energetics. Adenosine triphosphate (ATP) provides the energy for all muscle movements, heart beats, nerve signals and chemical reactions inside the body. It is estimated that the human body uses roughly 2 × 1026 transient molecules of ATP or more than the bodies weight; 160 kg of ATP in a day 13. Adenosine triphosphate (ATP) stores energy in a high energy phosphate bond, the third phosphate bond. The cutting of one phosphate bond, ATP + H2O → ADP + Pi liberates about 30.6 kJ/mole 13.
Adenosine diphosphate (ADP) is a platelet agonist that is stored in platelet-dense granules. When a platelet is activated, ADP is released and binds to platelet surface receptors, P2Y1 and P2Y12, thus recruiting additional platelets to form a platelet plug. Adenosine diphosphate (ADP) receptor inhibitors such as clopidogrel (Plavix®) and ticlopidine (Ticlid®) prevent platelet aggregation by selectively and irreversibly binding the platelet surface receptor P2Y12. Platelet aggregation is inhibited for the remainder of the platelet lifespan (7–10 days). Clopidogrel is indicated for treatment of acute ST and non-ST elevation myocardial infarction, peripheral arterial disease, arteriosclerotic vascular disease, and stroke. Ticlopidine is indicated after placement of coronary stents and after thromboembolic stroke 14.
Proper use of adenosine
A nurse or other trained health professional will give you adenosine. Adenosine is given through a needle placed into one of your veins.
Precautions while using adenosine
It is very important that your doctor check your progress very closely while you are receiving adenosine. This will allow your doctor to see if adenosine is working properly and to decide if you should continue to receive it.
Heart attack and death may occur after receiving adenosine. Make sure your doctor knows if you have any heart problems (eg, unstable angina or cardiovascular instability) before you have a heart stress test. Check with your doctor right away if you have chest pain or discomfort, nausea, pain or discomfort in arms, jaw, back or neck, sweating, or vomiting.
Do not take anything that contains caffeine before you receive adenosine. This includes medicines, foods, and beverages with caffeine, such as coffee, tea, and cola drinks.
Do not take other medicines unless they have been discussed with your doctor. This includes prescription or nonprescription (over-the-counter [OTC]) medicines and herbal or vitamin supplements.
What do I need to tell my doctor BEFORE I take Adenosine?
- If you have an allergy to adenosine or any other part of adenosine.
- If you are allergic to any drugs like this one, any other drugs, foods, or other substances. Tell your doctor about the allergy and what signs you had, like rash; hives; itching; shortness of breath; wheezing; cough; swelling of face, lips, tongue, or throat; or any other signs.
- If you have any of these health problems: Certain types of abnormal heartbeats (heart block, sick sinus syndrome) without a working pacemaker.
- If you have a certain type of chest pain (unstable angina).
- If you have any of these health problems: Asthma or other breathing problems like COPD (chronic obstructive pulmonary disease).
This is not a list of all drugs or health problems that interact with adenosine.
Tell your doctor and pharmacist about all of your drugs (prescription or OTC, natural products, vitamins) and health problems. You must check to make sure that it is safe for you to take adenosine with all of your drugs and health problems. Do not start, stop, or change the dose of any drug without checking with your doctor.
Side effects of adenosine
All drugs may cause side effects. However, many people have no side effects or only have minor side effects. Call your doctor or get medical help if any of these side effects or any other side effects bother you or do not go away:
- Dizziness.
- Flushing.
- Headache.
- Belly pain.
More Common
- chest discomfort
- difficult or labored breathing
- lightheadedness or dizziness
- throat, neck, or jaw discomfort
- tightness in the chest
Less Common
- chest pain
- confusion
- dizziness, faintness, or lightheadedness when getting up suddenly from a lying or sitting position
- fainting
- fast, slow, or irregular heartbeat
- sweating
- troubled breathing
- unusual tiredness or weakness
Rare
- fast, irregular, pounding, or racing heartbeat or pulse
- headache
- nervousness
- pounding in the ears
Some side effects of adenosine may occur that usually do not need medical attention. If you have questions about side effects, call your doctor. Call your doctor for medical advice about side effects. These side effects may go away during treatment as your body adjusts to the medicine. Also, your health care professional may be able to tell you about ways to prevent or reduce some of these side effects. Check with your health care professional if any of the following side effects continue or are bothersome or if you have any questions about them.
Call your doctor right away if you notice any of these side effects:
- Allergic reaction: Itching or hives, swelling in your face or hands, swelling or tingling in your mouth or throat, chest tightness, trouble breathing
- Chest pain that may spread to your arms, jaw, back, or neck, trouble breathing, nausea, unusual sweating
- Fast, slow, or uneven heartbeat
- Lightheadedness, dizziness, or fainting
- Numbness of weakness on one side of your body, sudden or severe headache, problems with vision, speech, or walking
- Throat, neck, or jaw discomfort, pain, or tightness
Figure 1. The heart’s electrical system

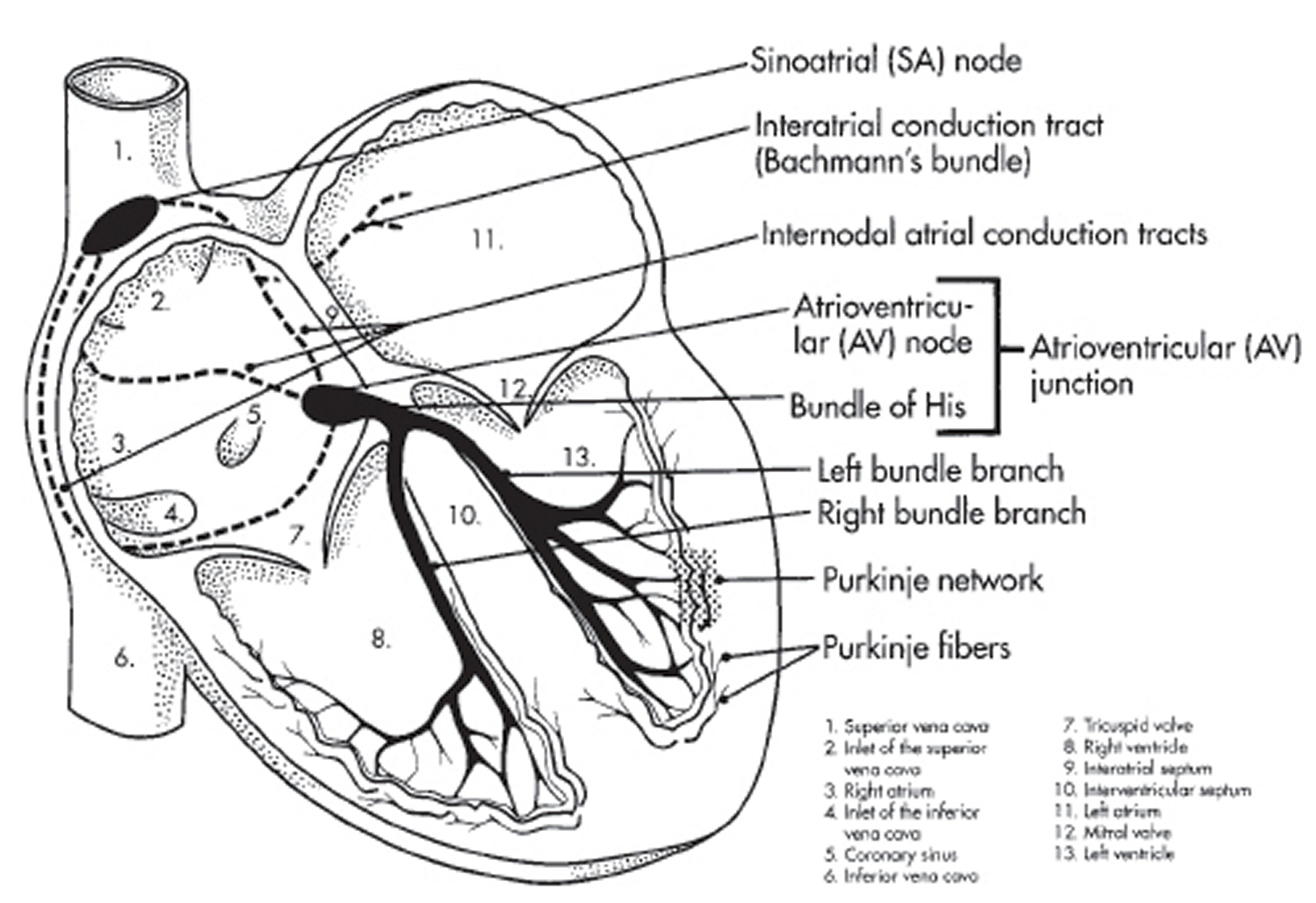
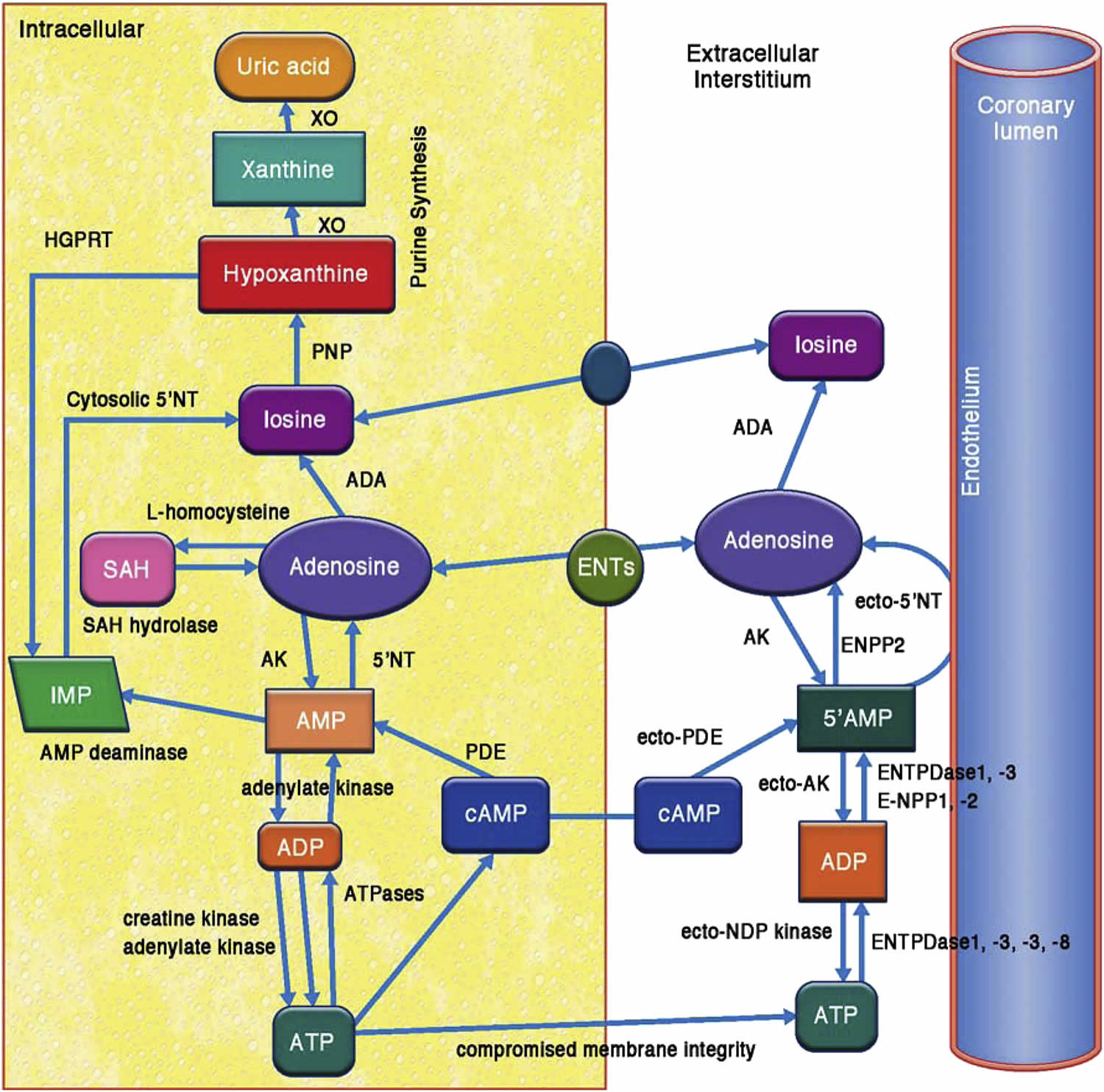
Figure 2. Adenosine Metabolism
Before using adenosine
In deciding to use a medicine, the risks of taking the medicine must be weighed against the good it will do. This is a decision you and your doctor will make. For adenosine, the following should be considered:
Allergies
Tell your doctor if you have ever had any unusual or allergic reaction to adenosine or any other medicines. Also tell your health care professional if you have any other types of allergies, such as to foods, dyes, preservatives, or animals. For non-prescription products, read the label or package ingredients carefully.
Children
Appropriate studies have not been performed on the relationship of age to the effects of adenosine injection in the pediatric population. Safety and efficacy have not been established. However, intravenous adenosine has been used for the treatment of PSVT in neonates, infants, children and adolescents.
Older Adults
Appropriate studies performed to date have not demonstrated geriatric-specific problems that would limit the usefulness of adenosine injection in the elderly.
Pregnancy
Pregnancy Category C (all Trimesters): Animal studies have shown an adverse effect and there are no adequate studies in pregnant women OR no animal studies have been conducted and there are no adequate studies in pregnant women. As adenosine is a naturally occurring material, widely dispersed throughout the body, no fetal effects would be anticipated. However, since it is not known whether adenosine can cause fetal harm when administered to pregnant women, adenosine should be used during pregnancy only if clearly needed.
Breastfeeding
There are no adequate studies in women for determining infant risk when using adenosine during breastfeeding. Weigh the potential benefits against the potential risks before taking adenosine while breastfeeding.
Interactions with other medicines
Although certain medicines should not be used together at all, in other cases two different medicines may be used together even if an interaction might occur. In these cases, your doctor may want to change the dose, or other precautions may be necessary. When you are receiving adenosine, it is especially important that your healthcare professional know if you are taking any of the medicines listed below. The following interactions have been selected on the basis of their potential significance and are not necessarily all-inclusive.
Using adenosine with any of the following medicines is usually not recommended, but may be required in some cases. If both medicines are prescribed together, your doctor may change the dose or how often you use one or both of the medicines.
- Aminophylline
- Carbamazepine
- Dimenhydrinate
- Dyphylline
- Pentoxifylline
- Theophylline
- Verapamil
Intravenous adenosine injection has been effectively administered in the presence of other cardioactive drugs, such as quinidine, beta-adrenergic blocking agents, calcium channel blocking agents, and angiotensin converting enzyme inhibitors, without any change in the adverse reaction profile. Digoxin and verapamil use may be rarely associated with ventricular fibrillation when combined with Adenosine (see Warnings). Because of the potential for additive or synergistic depressant effects on the SA (sinoatrial node) and AV (atrioventricular) nodes, however, Adenosine should be used with caution in the presence of these agents. The use of adenosine in patients receiving digitalis may be rarely associated with ventricular fibrillation.
Carbamazepine has been reported to increase the degree of heart block produced by other agents. As the primary effect of adenosine is to decrease conduction through the A-V node, higher degrees of heart block may be produced in the presence of carbamazepine.
Using adenosine with any of the following medicines may cause an increased risk of certain side effects, but using both drugs may be the best treatment for you. If both medicines are prescribed together, your doctor may change the dose or how often you use one or both of the medicines.
- Dipyridamole
Adenosine effects are potentiated by dipyridamole. Thus, smaller doses of Adenosine may be effective in the presence of dipyridamole.
Other Interactions
Certain medicines should not be used at or around the time of eating food or eating certain types of food since interactions may occur. Using alcohol or tobacco with certain medicines may also cause interactions to occur. The following interactions have been selected on the basis of their potential significance and are not necessarily all-inclusive.
Using adenosine with any of the following is usually not recommended, but may be unavoidable in some cases. If used together, your doctor may change the dose or how often you use this medicine, or give you special instructions about the use of food, alcohol, or tobacco.
- Caffeine
The effects of adenosine are antagonized by methylxanthines such as caffeine and theophylline. In the presence of these methylxanthines, larger doses of adenosine may be required or adenosine may not be effective.
Other Medical Problems
The presence of other medical problems may affect the use of adenosine. Make sure you tell your doctor if you have any other medical problems, especially:
- Angina, unstable or
- Unstable heart or blood vessel problem (eg, cardiovascular instability)—Avoid use, as adenosine may increase the risk for heart attack.
- Atrial fibrillation (heart rhythm problem), or history of or
- Breathing problems or lung disease (eg, bronchitis, emphysema) or
- Hypertension (high blood pressure) or
- Hypotension (low blood pressure) or
- Seizures or
- Stroke, history of—Use with caution. May make these conditions worse.
- Heart block, second or third degree (type of abnormal heart rhythm), without a pacemaker or
- Sinus node disease (such as sick sinus syndrome), without a pacemaker—Should not be used in patients with these conditions, unless patients have a pacemaker that works.
- Breathing problems or lung disease (e.g., asthma)—Should not be used in patients with these conditions.
- Heart or blood vessel disease (e.g., coronary artery stenosis, ischemia, pericardial effusion, pericarditis) or
- Heart valve disease or
- Hypovolemia (low blood volume), uncorrected—May increase risk for more serious side effects.
What are some things I need to know or do while I take Adenosine?
- Tell all of your health care providers that you take adenosine. This includes your doctors, nurses, pharmacists, and dentists.
- Have an ECG checked often. Talk with your doctor.
- High or low blood pressure may happen with adenosine. Have your blood pressure checked as you have been told by your doctor.
- Avoid use of caffeine (for example, tea, coffee, cola) and chocolate.
- If you are taking aminophylline, dipyridamole, theophylline, or any drug containing caffeine, talk with doctor. These drugs can affect how well adenosine works.
- Heart attacks and very bad fast heartbeat have rarely happened with adenosine. Sometimes this has been deadly. Talk with the doctor.
- Tell your doctor if you are pregnant or plan on getting pregnant. You will need to talk about the benefits and risks of using adenosine while you are pregnant.
- Tell your doctor if you are breast-feeding. You will need to talk about any risks to your baby.
How is this medicine (Adenosine) best taken?
Use adenosine as ordered by your doctor. Read all information given to you. Follow all instructions closely.
It is given as a shot into a vein.
What do I do if I miss a dose?
Call your doctor to find out what to do.
What does adenosine do
Adenosine injection slows conduction time through the A-V node, can interrupt the reentry pathways through the A-V node, and can restore normal sinus rhythm in patients with paroxysmal supraventricular tachycardia (PSVT), including PSVT associated with Wolff-Parkinson-White Syndrome.
Adenosine is antagonized competitively by methylxanthines such as caffeine and theophylline, and potentiated by blockers of nucleoside transport such as dipyridamole. Adenosine is not blocked by atropine.
Hemodynamics
The intravenous bolus dose of 6 or 12 mg Adenosine usually has no systemic hemodynamic effects. When larger doses are given by infusion, Adenosine decreases blood pressure by decreasing peripheral resistance.
Adenosine Clinical Trial Results
In controlled studies in the United States, bolus doses of 3, 6, 9, and 12 mg were studied. A cumulative 60% of patients with paroxysmal supraventricular tachycardia had converted to normal sinus rhythm within one minute after an intravenous bolus dose of 6 mg Adenosine (some converted on 3 mg and failures were given 6 mg), and a cumulative 92% converted after a bolus dose of 12 mg. Seven to sixteen percent of patients converted after 1 to 4 placebo bolus injections. Similar responses were seen in a variety of patient subsets, including those using or not using digoxin, those with Wolff-Parkinson-White Syndrome, males, females, blacks, Caucasians, and Hispanics.
Adenosine is not effective in converting rhythms other than PSVT, such as atrial flutter, atrial fibrillation, or ventricular tachycardia, to normal sinus rhythm.
Adenosine Pharmacokinetics
Intravenously administered Adenosine is rapidly cleared from the circulation via cellular uptake, primarily by erythrocytes and vascular endothelial cells. This process involves a specific transmembrane nucleoside carrier system that is reversible, nonconcentrative, and bidirectionally symmetrical. Intracellular Adenosine is rapidly metabolized either via phosphorylation to Adenosine monophosphate by Adenosine kinase, or via deamination to inosine by Adenosine deaminase in the cytosol. Since Adenosine kinase has a lower Km and Vmax than Adenosine deaminase, deamination plays a significant role only when cytosolic Adenosine saturates the phosphorylation pathway. Inosine formed by deamination of Adenosine can leave the cell intact or can be degraded to hypoxanthine, xanthine, and ultimately uric acid. Adenosine monophosphate formed by phosphorylation of Adenosine is incorporated into the high-energy phosphate pool. While extracellular Adenosine is primarily cleared by cellular uptake with a half-life of less than 10 seconds in whole blood, excessive amounts may be deaminated by an ecto-form of Adenosine deaminase. As Adenosine requires no hepatic or renal function for its activation or inactivation, hepatic and renal failure would not be expected to alter its effectiveness or tolerability.
Adenosine contraindications
Adenosine is not right for everyone. You should not receive adenosine if you had an allergic reaction to adenosine, or if you have asthma or certain heart rhythm problems.
Intravenous Adenosine injection is contraindicated in:
- Second- or third-degree A-V block (except in patients with a functioning artificial pacemaker).
- Sinus node disease, such as sick sinus syndrome or symptomatic bradycardia (except in patients with a functioning artificial pacemaker).
- Known hypersensitivity to Adenosine.
Heart Block
Adenosine injection exerts its effect by decreasing conduction through the A-V node and may produce a short lasting first-, second- or third-degree heart block. Appropriate therapy should be instituted as needed. Patients who develop high-level block on one dose of Adenosine should not be given additional doses. Because of the very short half-life of Adenosine, these effects are generally self-limiting. Appropriate resuscitative measures should be available.
Transient or prolonged episodes of asystole have been reported with fatal outcomes in some cases. Rarely, ventricular fibrillation has been reported following Adenosine administration, including both resuscitated and fatal events. In most instances, these cases were associated with the concomitant use of digoxin and, less frequently with digoxin and verapamil. Although no causal relationship or drug-drug interaction has been established, Adenosine should be used with caution in patients receiving digoxin or digoxin and verapamil in combination.
Arrhythmias at Time of Conversion
At the time of conversion to normal sinus rhythm, a variety of new rhythms may appear on the electrocardiogram. They generally last only a few seconds without intervention, and may take the form of premature ventricular contractions, atrial premature contractions, atrial fibrillation, sinus bradycardia, sinus tachycardia, skipped beats, and varying degrees of A-V nodal block. Such findings were seen in 55% of patients.
Bronchoconstriction
Adenosine injection is a respiratory stimulant (probably through activation of carotid body chemoreceptors) and intravenous administration in man has been shown to increase minute ventilation (Ve) and reduce arterial PCO2 causing respiratory alkalosis.
Adenosine administered by inhalation has been reported to cause bronchoconstriction in asthmatic patients, presumably due to mast cell degranulation and histamine release. These effects have not been observed in normal subjects. Adenosine has been administered to a limited number of patients with asthma and mild to moderate exacerbation of their symptoms has been reported. Respiratory compromise has occurred during Adenosine infusion in patients with obstructive pulmonary disease. Adenosine should be used with caution in patients with obstructive lung disease not associated with bronchoconstriction (e.g., emphysema, bronchitis, etc.) and should be avoided in patients with bronchoconstriction or bronchospasm (e.g., asthma). Adenosine should be discontinued in any patient who develops severe respiratory difficulties.
What is adenosine used for
Intravenous Adenosine injection is indicated for the following:
- Conversion to sinus rhythm of paroxysmal supraventricular tachycardia (PSVT), including that associated with accessory bypass tracts (Wolff-Parkinson-White Syndrome). When clinically advisable, appropriate vagal maneuvers (e.g., Valsalva maneuver), should be attempted prior to Adenosine administration.
It is important to be sure the Adenosine injection solution actually reaches the systemic circulation.
Adenosine injection does not convert atrial flutter, atrial fibrillation, or ventricular tachycardia to normal sinus rhythm. In the presence of atrial flutter or atrial fibrillation, a transient modest slowing of ventricular response may occur immediately following Adenosine administration.
Adenosine dose
Adenosine Injection, USP is supplied as a sterile non-pyrogenic solution in normal saline as follows:
| Adenosine Injection, USP (3 mg per mL) | Package Factor |
| 6 mg/2 mL Single-Dose Vial | 10 vials per carton |
| 12 mg/4 mL Single-Dose Vial | 10 vials per carton |
Adenosine injection should be given as a rapid bolus by the peripheral intravenous route. To be certain the solution reaches the systemic circulation, it should be administered either directly into a vein or, if given into an IV line, it should be given as close to the patient as possible and followed by a rapid saline flush.
Store at 20° to 25°C (68° to 77°F); excursions permitted between 15° and 30°C (59° and 86°F). [See USP Controlled Room Temperature.]
Store upright.
DO NOT REFRIGERATE as crystallization may occur. If crystallization has occurred, dissolve crystals by warming to room temperature. The solution must be clear at the time of use. Contains no preservatives. Discard unused portion.
The container closure is not made with natural rubber latex.
Sterile, Nonpyrogenic, Preservative-free.
Adult Patients
The dose recommendation is based on clinical studies with peripheral venous bolus dosing. Central venous (CVP or other) administration of Adenosine injection has not been systematically studied.
The recommended intravenous doses for adults are as follows:
- Initial dose: 6 mg given as a rapid intravenous bolus (administered over a 1 to 2 second period).
- Repeat administration: If the first dose does not result in elimination of the supraventricular tachycardia within 1 to 2 minutes, 12 mg should be given as a rapid intravenous bolus. This 12 mg dose may be repeated a second time if required.
Pediatric Patients
The dosages used in neonates, infants, children and adolescents were equivalent to those administered to adults on a weight basis.
Pediatric Patients with a Body Weight < 50 kg:
- Initial dose: Give 0.05 to 0.1 mg/kg as a rapid IV bolus given either centrally or peripherally. A saline flush should follow.
- Repeat administration: If conversion of PSVT does not occur within 1 to 2 minutes, additional bolus injections of Adenosine can be administered at incrementally higher doses, increasing the amount given by 0.05 to 0.1 mg/kg. Follow each bolus with a saline flush. This process should continue until sinus rhythm is established or a maximum single dose of 0.3 mg/kg is used.
Pediatric Patients with a Body Weight ≥ 50 kg: Administer the adult dose.
Doses greater than 12 mg are not recommended for adult and pediatric patients.
NOTE: Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration.
Adenosine side effects
Along with its needed effects, a medicine may cause some unwanted effects. Although not all of these side effects may occur, if they do occur they may need medical attention.
Check with your doctor or nurse immediately if any of the following side effects occur:
More common
- chest discomfort
- difficult or labored breathing
- lightheadedness or dizziness
- throat, neck, or jaw discomfort
- tightness in the chest
Less common
- chest pain
- confusion
- dizziness, faintness, or lightheadedness when getting up suddenly from a lying or sitting position
- fainting
- fast, slow, or irregular heartbeat
- sweating
- troubled breathing
- unusual tiredness or weakness
Rare
- fast, irregular, pounding, or racing heartbeat or pulse
- headache
- nervousness
- pounding in the ears
Some side effects may occur that usually do not need medical attention. These side effects may go away during treatment as your body adjusts to the medicine. Also, your health care professional may be able to tell you about ways to prevent or reduce some of these side effects. Check with your health care professional if any of the following side effects continue or are bothersome or if you have any questions about them:
More Common
- diarrhea
- feeling of warmth
- indigestion
- loss of appetite
- nausea or vomiting
- passing of gas
- redness of the face, neck, arms, and occasionally, upper chest
- stomach pain, fullness, or discomfort
Rare
- area of decreased vision
- cough
- discomfort in the back, ears, or tongue
- drowsiness
- dry mouth
- metallic taste
- mood changes
- shakiness in the legs, arms, hands, or feet
- stuffy nose
- trembling or shaking of the hands or feet
These are not all of the side effects that may occur. If you have questions about side effects, call your doctor. Call your doctor for medical advice about side effects.
Side effects that applies to adenosine: compounding powder, intravenous solution, sublingual spray
General
The most common adverse reactions are flushing, chest discomfort, dyspnea, facial flushing, headache, throat/neck/jaw discomfort, gastrointestinal discomfort, and lightheadedness/dizziness.
Cardiovascular
- Very common (10% or more): Flushing (44%), facial flushing (18%)
- Common (1% to 10%): First degree atrioventricular block, second degree atrioventricular block, hypotension, arrhythmias, ventricular tachycardia
- Uncommon (0.1% to 1%): Bradycardia, sinus tachycardia, palpitations
- Very rare (less than 0.01%): Atrial fibrillation, ventricular fibrillation, Torsade de pointes, severe bradycardia
- Frequency not reported: Myocardial infarction, ventricular arrhythmia, third degree atrioventricular block, sinus exit block, sinus pause, hypertension, skipped beats, atrial extrasystoles, ventricular extrasystoles
- Postmarketing reports: Cardiac arrest/asystole, cardiac failure, tachycardia, prolonged asystole, transient increase in blood pressure
Other side effects
- Very common (10% or more): Chest discomfort (40%)
- Common (1% to 10%): ST segment depression, chest pressure
- Uncommon (0.1% to 1%): Feeling of general discomfort/weakness/pain
- Rare (less than 0.1%): Tinnitus, nipple discomfort
- Frequency not reported: Chest pain, feeling of thoracic constriction/oppression, weakness, T wave changes, ear discomfort, tongue discomfort, heaviness in arms, pressure in groin
- Postmarketing reports: ST segment elevation
Respiratory
- Very common (10% or more): Dyspnea (up to 28%)
- Uncommon (0.1% to 1%): Hyperventilation
- Rare (0.01% to 0.1%): Bronchospasm, nasal congestion
- Very rare (less than 0.01%): Respiratory failure
- Frequency not reported: Cough, throat tightness
- Postmarketing reports: Respiratory arrest/apnea
Nervous system
- Very common (10% or more): Headache (up to 18%), lightheadedness/dizziness (12%)
- Common (1% to 10%): Paresthesia, tingling in arms, numbness, burning sensation
- Uncommon (0.1% to 1%): Metallic taste, head pressure
- Rare (0.01% to 0.1%): Tremor, drowsiness
- Very rare (less than 0.01%): Intracranial hypertension worsening
- Frequency not reported: Scotomas, convulsions
- Postmarketing reports: Cerebrovascular accident, intracranial hemorrhage, seizure, tonic clonic seizures, loss of consciousness/syncope
Musculoskeletal
Very common (10% or more): Throat/neck/jaw discomfort (15%)
Common (1% to 10%): Upper extremity discomfort
Frequency not reported: Back discomfort, lower extremity discomfort, neck and back pain
Gastrointestinal
Very common (10% or more): Gastrointestinal discomfort (13%)
Common (1% to 10%): Dry mouth, nausea
Frequency not reported: Abdominal discomfort
Postmarketing reports: Vomiting
Psychiatric
Common (1% to 10%): Nervousness, apprehension
Frequency not reported: Emotional instability
Dermatologic
Uncommon (0.1% to 1%): Sweating
Postmarketing reports: Angioedema, urticaria, rash
Ocular
Uncommon (0.1% to 1%): Blurred vision
Genitourinary
Rare (less than 0.1%): Urinary urgency
Frequency not reported: Vaginal pressure
Local
Very rare (less than 0.01%): Injection site reaction
Postmarketing reports: Infusion site pain
Hypersensitivity
Postmarketing reports: Hypersensitivity, anaphylaxis
Serious side effects
Even though it may be rare, some people may have very bad and sometimes deadly side effects when taking a drug. Tell your doctor or get medical help right away if you have any of the following signs or symptoms that may be related to a very bad side effect:
- Signs of an allergic reaction, like rash; hives; itching; red, swollen, blistered, or peeling skin with or without fever; wheezing; tightness in the chest or throat; trouble breathing, swallowing, or talking; unusual hoarseness; or swelling of the mouth, face, lips, tongue, or throat.
- Signs of high or low blood pressure like very bad headache or dizziness, passing out, change in eyesight.
- Weakness on 1 side of the body, trouble speaking or thinking, change in balance, drooping on one side of the face, or blurred eyesight.
- Chest pain or pressure.
- Fast or slow heartbeat.
- A heartbeat that does not feel normal.
- Shortness of breath.
- Seizures.
- Throat, neck, or jaw pain.
Adenosine Adverse Reactions
The following reactions were reported with intravenous Adenosine injection used in controlled U.S. clinical trials. The placebo group had a less than 1% rate of all of these reactions.
Cardiovascular
Facial flushing (18%), headache (2%), sweating, palpitations, chest pain, hypotension (less than 1%).
Respiratory
Shortness of breath/dyspnea (12%), chest pressure (7%), hyperventilation, head pressure (less than 1%).
Central Nervous System
Lightheadedness (2%), dizziness, tingling in arms, numbness (1%), apprehension, blurred vision, burning sensation, heaviness in arms, neck and back pain (less than 1%).
Gastrointestinal
Nausea (3%), metallic taste, tightness in throat, pressure in groin (less than 1%).
Post Marketing Experience (see Warnings)
The following adverse events have been reported from marketing experience with Adenosine. Because these events are reported voluntarily from a population of uncertain size, are associated with concomitant diseases and multiple drug therapies and surgical procedures, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure. Decisions to include these events in labeling are typically based on one or more of the following factors: (1) seriousness of the event, (2) frequency of the reporting, (3) strength of causal connection to the drug, or a combination of these factors.
Cardiovascular
Prolonged asystole, ventricular tachycardia, ventricular fibrillation, transient increase in blood pressure, bradycardia, atrial fibrillation, and Torsade de Pointes.
Respiratory
Bronchospasm
Central Nervous System
Seizure activity, including tonic clonic (grand mal) seizures, and loss of consciousness.
Adenosine Overdose
The half-life of adenosine injection is less than 10 seconds. Thus, adverse effects are generally rapidly self-limiting. Treatment of any prolonged adverse effects should be individualized and be directed toward the specific effect. Methylxanthines, such as caffeine and theophylline, are competitive antagonists of Adenosine.
- Adenosine: Physiology, Pharmacology, and Clinical Applications. JACC: Cardiovascular Interventions Volume 7, Issue 6, June 2014, Pages 581-591 https://ac.els-cdn.com/S1936879814006323/1-s2.0-S1936879814006323-main.pdf?_tid=56b2f949-90e2-414c-bd77-3fda8baea8d2&acdnat=1530881194_ba45771fb1415199fc0fa525de108b47[↩]
- The crux of maximum hyperemia: the last remaining barrier for routine use of fractional flow reserve. J Am Coll Cardiol Intv, 4 (2011), pp. 1093-1095[↩]
- Adenosine: an old drug newly discovered. Anesthesiology, 111 (2009), pp. 904-915[↩][↩]
- Involvement of adenosine deaminase and adenosine kinase in regulating extracellular adenosine concentration in rat hippocampal slices. Neurochem Int, 26 (1995), pp. 387-395[↩]
- Dipyridamole stress echocardiography. Cardiol Clin, 17 (1999), pp. 481-499[↩]
- Adenosine kinase and ribokinase–the RK family of proteins. Cell Mol Life Sci, 65 (2008), pp. 2875-2896[↩]
- Singh L, Kulshrestha R, Singh N, Jaggi AS. Mechanisms involved in adenosine pharmacological preconditioning-induced cardioprotection. The Korean Journal of Physiology & Pharmacology : Official Journal of the Korean Physiological Society and the Korean Society of Pharmacology. 2018;22(3):225-234. doi:10.4196/kjpp.2018.22.3.225. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5928336/[↩]
- Sheth S, Brito R, Mukherjea D, Rybak LP, Ramkumar V. Adenosine receptors: expression, function and regulation. Int J Mol Sci. 2014;15:2024–2052 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3958836/[↩]
- Layland J, Carrick D, Lee M, Oldroyd K, Berry C. Adenosine: physiology, pharmacology, and clinical applications. JACC Cardiovasc Interv. 2014;7:581–591 https://www.sciencedirect.com/science/article/pii/S1936879814006323[↩]
- Headrick JP, Ashton KJ, Rose’meyer RB, Peart JN. Cardiovascular adenosine receptors: expression, actions and interactions. Pharmacol Ther. 2013;140:92–111 https://www.ncbi.nlm.nih.gov/pubmed/23764371[↩]
- Ohta A, Sitkovsky M. The adenosinergic immunomodulatory drugs. Curr Opin Pharmacol. 2009;9:501–506 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2756083/[↩]
- Sachdeva S, Gupta M. Adenosine and its receptors as therapeutic targets: an overview. Saudi Pharm J. 2013;21:245–253 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3744929/[↩]
- Adenosine Triphosphate Energetics. Biology of Life Biochemistry, Physiology and Philosophy 2016, Pages 65-77[↩][↩]
- Commonly used drugs in hematologic disorders. Handbook of Clinical Volume 120, 2014, Pages 1125-1139[↩]





{kind=link}