
Contents
What is airplane ear
Airplane ear is the stress exerted on your eardrum and other middle ear tissues when the air pressure in your middle ear and the air pressure in the environment are out of balance. You may experience airplane ear at the beginning of a flight when the airplane is climbing or at the end of a flight when the airplane is descending. These fast changes in altitude cause air pressure changes and can trigger airplane ear.
Airplane ear is also called ear barotrauma, barotitis media, serous otitis media or aerotitis media (aero-otitis media).
As the plane ascends or descends, discomfort may be felt in the ears and sinuses. This is because the pocket of air inside the middle ear is very sensitive to changes in the surrounding air pressure. As an airplane climbs, the pressure in the cabin lowers, causing gases to expand. When the plane is descending, the increasing pressure causes gases to contract.
Normally as the plane ascends, air escapes from the middle ear, resulting in a popping sensation in the ear. When the plane descends, the air needs to flow back into the middle ear through the Eustachian tube. This action serves to maintain equal pressure on both sides of the ear drum. If it doesn’t happen, the ears and sinuses may feel blocked and painful until the pressure is relieved.
When the Eustachian tube (auditory tube) is blocked, the middle ear pressure cannot be equalized, so the air already there is absorbed. This creates a vacuum, sucking the ear drum inward and stretching it. As a result, sound is muffled. If the tube stays blocked, fluid can leak into the area and cause serous otitis. Children have much smaller Eustachian tubes and so are especially vulnerable to blockages.
Usually self-care steps — such as yawning, swallowing or chewing gum — can prevent or correct the differences in air pressure and improve airplane ear symptoms. However, a severe case of airplane ear may need to be treated by a doctor.
Ear pain is experienced by about 15% of children during descent. Babies cannot intentionally pop their ears, but popping can be induced by giving them something to suck on, such as a bottle or pacifier (dummy). To prevent discomfort while the plane is descending, do not allow them to sleep. Older children should chew gum, or they can be instructed to perform the Valsalva manoeuvre.
Individuals with a cold or ear, nose or sinus infection should avoid flying because the inability to equalise pressure may result in pain and injury. If travel can’t be avoided, applying decongestant nasal drops just before flight and again before descent may help.
Air travel over long distances can expose you to a number of factors that may have an impact on your health and wellbeing. The environmental conditions inside the cabin of an airplane flying at 12,000 meters are vastly different to those on the ground. The plane environment subjects your body to reduced atmospheric pressure, reduced availability of oxygen, relative humidity, noise and vibration. Additionally, there is the risk of acquiring an infection from fellow passengers. Time zone changes can affect performance and enjoyment of your holiday at your destination.
Everyone is affected differently by air travel. People with less than optimal health are at an increased risk of suffering health related problems while traveling on a plane. These may range from minor issues such as dry skin or motion sickness, to more serious ones such as developing a blood clot.
Health risks can be minimized by planning carefully and taking some precautions before, during and after the flight. Some general advice that will help make your in-flight experience more bearable and holiday more enjoyable include:
- Make sure you are as healthy as possible by getting enough rest before leaving.
- An optimal immune system will protect you from catching any colds or other bugs from other passengers.
- Plane food is generally heavily processed and refined, and full of starches and sugar which can make you feel sluggish, so consider taking some healthy snacks such as fruit or nuts.
- Try to avoid alcohol and caffeine, and drink as much water as possible before and during the flight.
Cabin air quality
Effects of cabin air humidity
The humidity in cabin aircraft is usually very low, around 20%, meaning that the air is very dry. Such low humidity can cause dryness of the skin, mouth, nose and other mucous membranes.
Using moisturizing lotion on the skin and a saline nasal spray to moisturize the nasal passages can help counteract these effects. For contact lens wearers, using glasses during the flight instead will help prevent the discomfort and irritation of dry eyes.
Risk of infection
The air inside a plane is changed 20-30 times per hour. The cabin air is carefully controlled and most ventilation systems recirculate 50% of the air after it has passed through filters, which trap particles, bacteria, fungi and viruses.
Infections may be transmitted between passengers who are seated near each other when an infected person sneezes or coughs, or by touch. If you are concerned and are sitting beside someone who is ill, you can ask to move to another available seat. Some other measures that can be taken include carrying antiseptic wipes to clean seat handles, and using an antibacterial hand gel to wash your hands.
Effects of cabin air pressure
The cabin air pressure is lower than the air pressure at sea level. The result of this is that less oxygen is taken up by the blood, and gases within the body expand. Healthy passengers adapt reasonably well to these changes, but the very young, the elderly and anyone with a medical condition (e.g. heart or lung disease, anemia) may not be able to tolerate the lower oxygen level very well. Such passengers can request an additional oxygen supply during the flight.
As the plane takes off, the oxygen in the cabin lowers and your respiratory system adjusts by increasing the rate and volume of breathing. This can make you feel drowsy and you may have difficulty concentrating.
Another consequence of the lower cabin air pressure is swelling or edema of the legs and feet. Sitting still for extended periods of time leads to the accumulation of excess fluid in the tissue, which may cause the lower limbs to swell. This condition, also known as ‘jet flight leg’, is more common in women over 30 and people with varicose veins. The severity of swelling is related to the cabin temperature and cruising altitude of the aircraft. It tends to become worse the longer the flight and the lower the cabin pressure. Elastic compression stockings applied before the flight can help prevent swelling in those who have recurrent moderate or severe jet flight leg.
Why do ears pop?
Normally, swallowing causes a little click or popping sound in the ear. This occurs because a small bubble of air has entered the middle ear, up from the back of the nose. It passes through the Eustachian tube (auditory tube), a membrane-lined tube about the size of a pencil lead that connects the back of the nose with the middle ear (see Figures 2 and 3). The air in the middle ear is constantly being absorbed by its membranous lining and re-supplied through the Eustachian tube. In this manner, air pressure on both sides of the eardrum stays about equal. If, and when, the air pressure is not equal the ear feels blocked.
The Eustachian tube can be blocked or obstructed, for a variety of reasons. When that occurs, the middle ear pressure cannot be equalized. The air already there is absorbed and a vacuum occurs, sucking the eardrum inward and stretching it (see Figure 1 – Tympanic membrane). Such an eardrum cannot vibrate naturally, so sounds are muffled or blocked and the stretching can be painful. If the tube remains blocked, fluid (like blood serum) will seep into the area from the membranes in an attempt to overcome the vacuum. This is called fluid in the ear, serous otitis media or aero-otitis media. Uncommon problems include developing a hole in the ear drum, hearing loss and dizziness.
The most common cause for a blocked Eustachian tube is the common cold. Sinus infections and nasal allergies are also common causes. A stuffy nose leads to stuffy ears because the swollen membranes block the opening of the Eustachian tube.
Figure 1. Ear structure
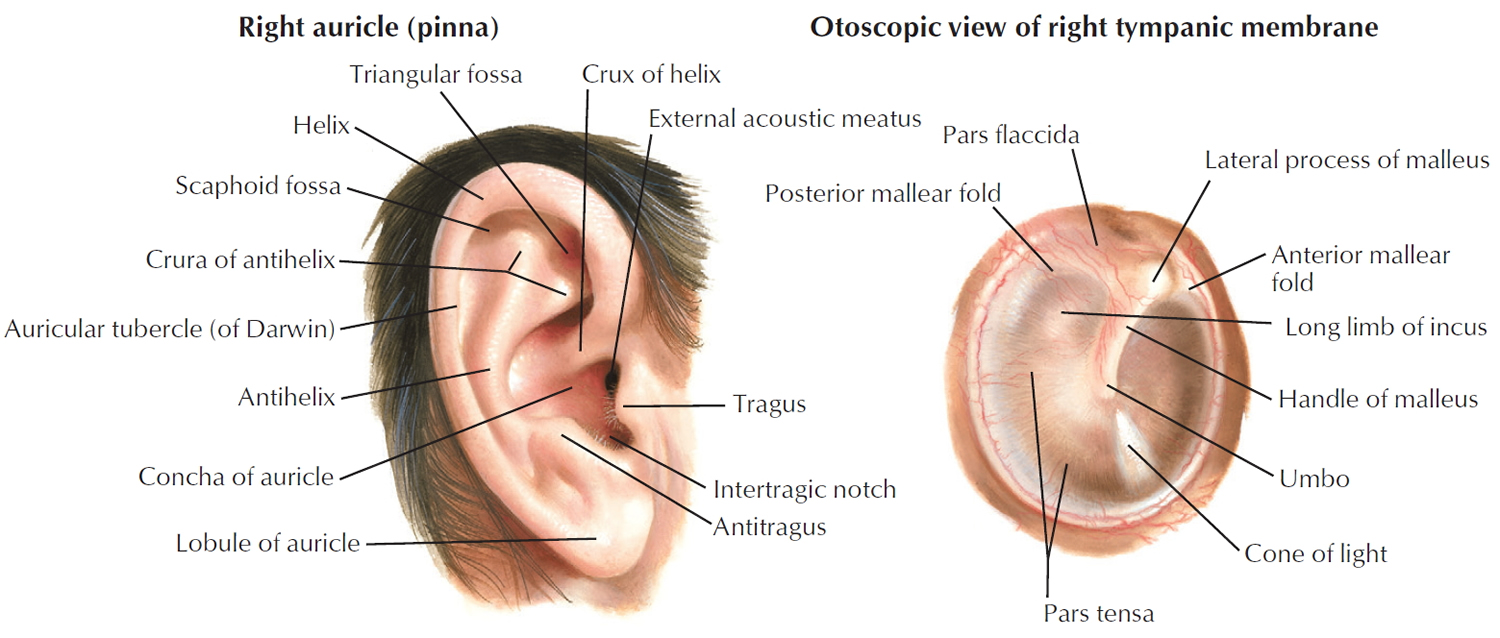
Figure 2. Ear anatomy

Middle Ear
The middle ear is a small, air-filled cavity in the petrous portion of the temporal bone that is lined by epithelium. It is separated from the external ear by the tympanic membrane and from the internal ear by a thin bony partition that contains two small openings: the oval window and the round window.
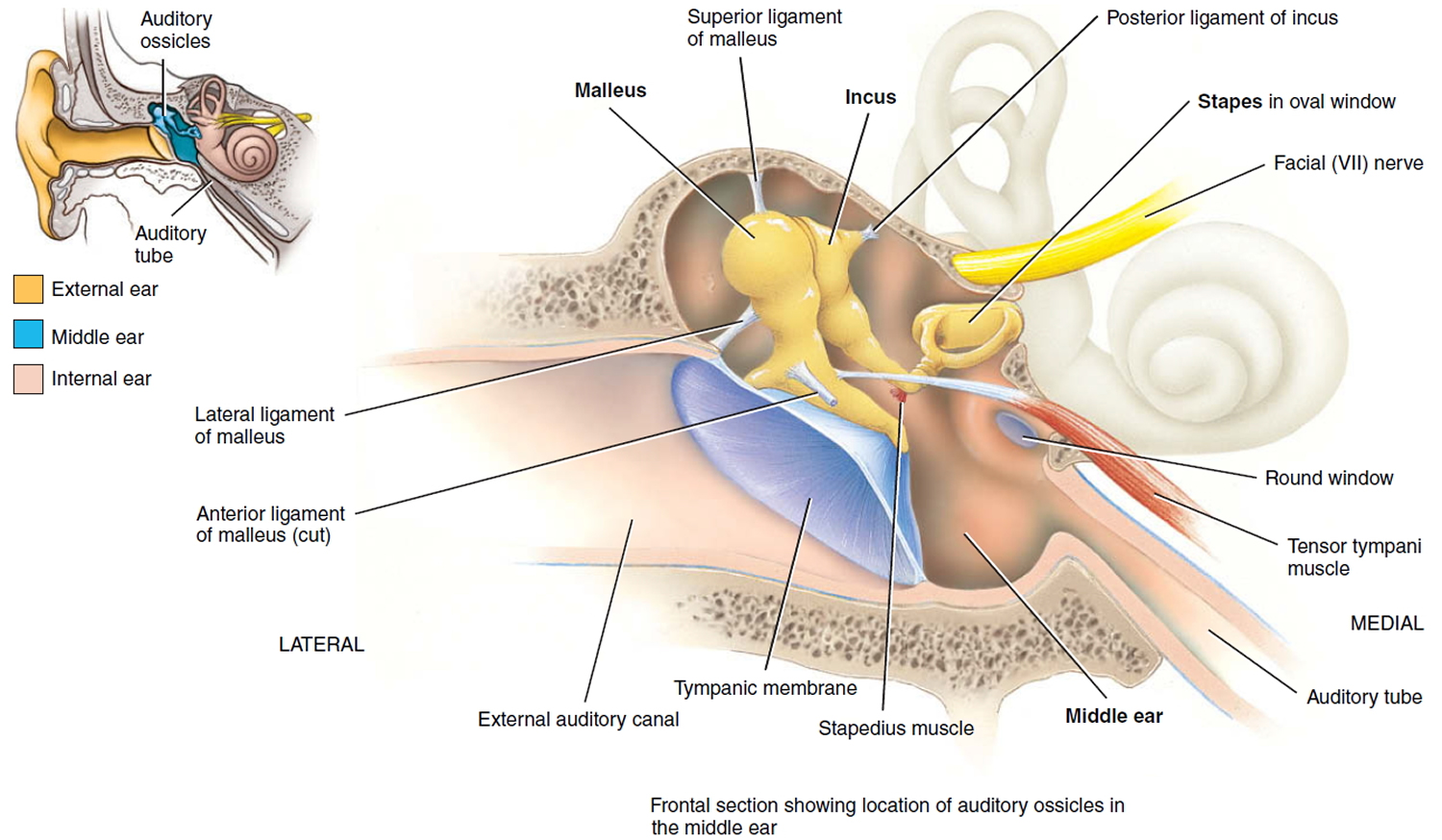
Extending across the middle ear and attached to it by ligaments are the three smallest bones in the body, the auditory ossicles, which are connected by synovial joints. The bones, named for their shapes, are the malleus, incus, and stapes—commonly called the hammer, anvil, and stirrup, respectively. The “handle” of the malleus attaches to the internal surface of the tympanic membrane. The head of the malleus articulates with the body of the incus. The incus, the middle bone in the series, articulates with the head of the stapes. The base or footplate of the stapes fits into the oval window. Directly below the oval window is another opening, the round window, which is enclosed by a membrane called the secondary tympanic membrane. Besides the ligaments, two tiny skeletal muscles also attach to the ossicles (Figure 3).
The tensor tympani muscle, which is supplied by the mandibular branch of the trigeminal (V) nerve, limits movement and increases tension on the eardrum to prevent damage to the inner ear from loud noises. The stapedius muscle, which is supplied by the facial (VII) nerve, is the smallest skeletal muscle in the human body. By dampening large vibrations of the stapes due to loud noises, it protects the oval window, but it also decreases the sensitivity of hearing. For this reason, paralysis of the stapedius muscle is associated with hyperacusia, which is abnormally sensitive hearing. Because it takes a fraction of a second for the tensor tympani and stapedius muscles to contract, they can protect the inner ear from prolonged loud noises but not from brief ones such as a gunshot.
The anterior wall of the middle ear contains an opening that leads directly into the auditory tube or pharyngotympanic tube, commonly known as the eustachian tube. The auditory tube, which consists of both bone and elastic cartilage, connects the middle ear with the nasopharynx (superior portion of the throat). It is normally closed at its medial (pharyngeal) end. During swallowing and yawning, it opens, allowing air to enter or leave the middle ear until the pressure in the middle ear equals the atmospheric pressure. Most of us have experienced our ears popping as the pressures equalize. When the pressures are balanced, the tympanic membrane vibrates freely as sound waves strike it. If the pressure is not equalized, intense pain, hearing impairment, ringing in the ears, and vertigo could develop. The auditory tube also is a route for pathogens to travel from the nose and throat to the middle ear, causing the most common type of ear infection.
Figure 3. Middle ear and auditory ossicles
How can air travel cause hearing problems?
Air travel is sometimes associated with rapid changes in air pressure. To maintain comfort, the Eustachian tube (auditory tube) must open frequently and wide enough to equalize the changes in pressure. This is especially true when the airplane is landing, going from low atmospheric pressure down closer to earth where the air pressure is higher.
During flight on a commercial airplane, the middle ear has to equalize about 20% of its gas volume with the ambient pressure. This equalization must happen within 15 to 20 minutes of ascent and descent in order to avoid barotrauma 1.
Actually, any situation in which rapid altitude or pressure changes occur creates the problem. It may be experienced when riding in elevators or when diving to the bottom of a swimming pool. Deep sea divers, as well as pilots, are taught how to equalize their ear pressure. Anybody can learn the trick too.
How to unblock ears?
Swallowing activates the muscles that open the Eustachian tube (auditory tube). Swallowing occurs more often when chewing gum or when sucking on hard candies. These are good air travel practices, especially just before take-off and during descent. Yawning is even better. Avoid sleeping during descent because swallowing may not occur often enough to keep up with the pressure changes.
During decent, if yawning and swallowing are not effective, pinch the nostrils shut, you can try the ‘Valsalva manoeuvre‘ by taking a mouthful of air, and direct the air into the back of the nose as if trying to blow the nose gently, you should feel a pressure buildup but do not let the air out your mouth The ears have been successfully unblocked when a pop is heard. This may have to be repeated several times during descent.
Even after landing, continue the pressure equalizing techniques and the use of decongestants and nasal sprays. If the ears fail to open or if pain persists, seek the help of a physician who has experience in the care of ear disorders. The ear specialist may need to release the pressure or fluid with a small incision in the ear drum.
For some people, these techniques may not work. If you fly frequently and have chronic issues with pressure or pain, you doctor may recommend placing small pressure equalization tubes.
Is the use of decongestants and nose sprays recommended?
Many experienced air travelers use a decongestant pill or an over the counter nasal spray an hour or so before descent. This will shrink the membranes and help the ears pop more easily. Travelers with allergy problems should take their medication at the beginning of the flight for the same reason. However, avoid making a habit of over the counter nasal sprays. After a few days, they may cause more congestion than relief.
Decongestant tablets and sprays can be purchased without a prescription. However, they should be avoided by people with heart disease, high blood pressure, irregular heart rhythms, thyroid disease, or excessive nervousness. Such people should consult their physicians before using these medicines. Pregnant women should likewise consult their physicians first.
How to help babies unblock their ears?
Babies cannot intentionally pop their ears, but popping may occur if they are sucking on a bottle or pacifier. Feed the baby during the flight, and do not allow him or her to sleep during descent. Children are especially vulnerable to blockages because their Eustachian tubes are narrower than in adults.
Complications of airplane ear
Airplane ear usually isn’t serious and responds to self-care. Long-term complications may occur when the condition is serious or prolonged or if there’s damage to middle or inner ear structures.
Rare complications may include:
- Permanent hearing loss
- Ongoing (chronic) tinnitus
Airplane ear symptoms
Airplane ear can occur in one or both ears. Airplane ear signs and symptoms may include:
- Moderate discomfort or pain in your ear
- Feeling of fullness or stuffiness in your ear
- Muffled hearing or slight to moderate hearing loss
If airplane ear is severe or lasts more than a few hours, you may experience:
- Severe pain
- Pressure in your ear similar to being underwater
- Moderate to severe hearing loss
- Ringing in your ear (tinnitus)
- Spinning sensation (vertigo)
- Vomiting resulting from vertigo
- Bleeding from your ear
Causes of airplane ear
Airplane ear occurs when an imbalance in the air pressure in the middle ear and air pressure in the environment prevents your eardrum (tympanic membrane) from vibrating as it should. Air pressure regulation is the work of a narrow passage called the eustachian tube. One end is connected to the middle ear. The other end has a tiny opening where the back of the nasal cavity and the top of the throat meet (nasopharynx).
When an airplane climbs or descends, the air pressure in the environment changes rapidly, and your eustachian tube often doesn’t react quickly enough. Swallowing or yawning activates muscles that open the eustachian tube and allow the middle ear to replenish its air supply, often eliminating the symptoms of airplane ear.
Ear barotrauma also may be caused by:
- Scuba diving
- Hyperbaric oxygen chambers
- Explosions nearby
You may also experience a minor case of barotrauma while riding an elevator in a tall building or driving in the mountains.
Risk factors of airplane ear
Any condition that blocks the eustachian tube or limits its function can increase the risk of airplane ear. Common risk factors include:
- A small Eustachian tube, especially in infants and toddlers
- The common cold
- Sinus infection
- Hay fever (allergic rhinitis)
- Middle ear infection (otitis media)
- Sleeping on an airplane during ascent and descent
Frequent or severe airplane ear may damage the tissues of the inner ear or Eustachian tube, which increases your chances of experiencing the problem again.
Prevention of airplane ear
Follow these tips to avoid airplane ear:
- Yawn and swallow during ascent and descent. Yawning and swallowing activate the muscles that open your eustachian tubes. You can suck on candy or chew gum to help you swallow.
- Use the Valsalva maneuver during ascent and descent. Gently blow, as if blowing your nose, while pinching your nostrils and keeping your mouth closed.
- Repeat several times, especially during descent, to equalize the pressure between your ears and the airplane cabin.
- Don’t sleep during takeoffs and landings. If you’re awake during ascents and descents, you can do the necessary self-care techniques when you feel pressure on your ears.
- Reconsider travel plans. If possible, don’t fly when you have a cold, sinus infection, nasal congestion or ear infection. If you’ve recently had ear surgery, talk to your doctor about when it’s safe to travel.
- Use filtered earplugs. These earplugs slowly equalize the pressure against your eardrum during ascents and descents. You can purchase these at drugstores, airport gift shops or your local hearing clinic.
- Use an over-the-counter decongestant nasal spray. If you have nasal congestion, use a nasal decongestant about 30 minutes to an hour before takeoff and landing. Avoid overuse, however, because nasal decongestants taken over several days can increase congestion.
- Use oral decongestant pills cautiously. Oral decongestants may be helpful if taken 30 minutes to an hour before an airplane flight. However, if you have heart disease, a heart rhythm disorder or high blood pressure, or if you’ve experienced possible medication interactions, avoid taking an oral decongestant unless your doctor approves. If you’re a man older than age 50, you may experience serious side effects after taking decongestants containing pseudoephedrine (Actifed, Sudafed) such as urinary retention, especially if you have an enlarged prostate. If you’re pregnant, talk to your doctor before taking oral decongestants.
- Take allergy medication. If you have allergies, take your medication about an hour before your flight.
If you’re prone to severe airplane ear and must fly often, your doctor may surgically place tubes in your eardrums to aid fluid drainage, ventilate your middle ear, and equalize the pressure between your outer ear and middle ear.
Helping children prevent airplane ear
These additional tips can help young children avoid airplane ear:
- Encourage swallowing. Give a baby or toddler a beverage during ascents and descents to encourage frequent swallowing. A pacifier also may help. Have the child sit up while drinking. Children older than age 4 can try chewing gum, drinking through a straw or blowing bubbles through a straw.
- Consider eardrops. Talk to your child’s doctor about prescribing your child eardrops that contain a pain reliever and numbing agent for the flight.
- Avoid decongestants. Decongestants aren’t recommended for young children.
Who should avoid flying?
- Infants less than 2 days old
- Women after the 36th week of pregnancy
- Recent recipients of coronary bypass graft or transluminal coronary angioplasty (unless clearance is given by your doctor)
- Those suffering from:
- Unstable angina pectoris or chest pain
- Recent heart attack or stroke
- Increased intracranial pressure due to trauma, hemorrhage or infection
- Infection of sinuses of ear and nose
- Recent surgery or injury where trapped gases may be present (e.g. abdominal trauma and gastrointestinal surgery, craniofacial and ocular injuries, brain operation and eye operations involving penetration of the eyeball)
- Severe chronic respiratory disease or unresolved pneumothorax
- Sickle cell disease
- Psychotic illness except when fully controlled
- Any active contagious disease
- Frequent or poorly controlled asthmatic attacks
- Decompression sickness after diving
If you have any of these conditions and are planning to fly, you must receive clearance from your general practitioner.
Passengers with mild chronic obstructive pulmonary disease (COPD) who are symptom free can travel safely. However, people with severe COPD must consider using inflight oxygen, as the low oxygen concentration in cabin air can further stress an already compromised oxygen transport system.
Patients with bronchial asthma should carry medication with them.
Tips for healthy air travel
Some preventative measures that may help you beat sickness and leave the plane feeling refreshed are:
- Drink lots of water: This helps keep you hydrated and helps your body function optimally.
- Stretch whenever possible, especially on long flights, to get the blood circulating properly.
- Dress appropriately: The temperature inside the plane can be quite cold.
- Vitamin C: Take a vitamin C tablet daily for a week before you leave, and also during the flight.
- Schedule time to rest as soon as you arrive at your destination.
- Carry medication in your carryon luggage. If you are epileptic or diabetic, or have any other chronic condition, carry a notification and ID card with you.
- Avoid alcoholic and caffeinated drinks.
- Take a decongestant before you get on the plane, especially if you have a cold or swollen sinuses. Also drink plenty of fluids. Remember to swallow often and chew gum.
- To prevent motion sickness, eat a light meal or snack before and during travel.
Airplane ear diagnosis
Your doctor will likely be able to make a diagnosis based on questions he or she asks and an examination of your ear with a lighted instrument (otoscope). Signs of airplane ear might include a slight outward or inward bulging of your eardrum. If your condition is more severe, your doctor may see a tear in the eardrum or a pooling of blood or other fluids behind your eardrum.
If you’re experiencing a spinning sensation (vertigo), there may be damage to structures of your inner ear. Your doctor may suggest a hearing test (audiometry) to determine how well you detect sounds and whether the source of hearing problems is in the inner ear.
Airplane ear treatment
For most people, airplane ear usually heals with time. When the symptoms persist, you may need treatments to equalize pressure and relieve symptoms.
How to get rid of airplane ear
Your doctor may prescribe medications or direct you to take over-the-counter medications to control conditions that may prevent the eustachian tubes from functioning well. These drugs may include:
- Decongestant nasal sprays
- Oral decongestants
- Oral antihistamines
To ease discomfort, you may want to take a nonsteroidal anti-inflammatory drug, such as ibuprofen (Advil, Motrin IB, others) or naproxen sodium (Aleve, others), or an analgesic pain reliever, such as acetaminophen (Tylenol, others).
Airplane ear pain remedies
With your drug treatment, your doctor will instruct you to use a self-care method called the Valsalva maneuver. To do this, you pinch your nostrils shut, close your mouth and gently force air into the back of your nose, as if you were blowing your nose. Once the medications have improved the function of the eustachian tubes, use of the Valsalva maneuver may force the tubes open.
Airplane ear surgery
Surgical treatment of airplane ear is rarely necessary. However, your doctor may make an incision in your eardrum (myringotomy) to equalize air pressure and drain fluids.
Severe injuries, such as a ruptured eardrum or ruptured membranes of the inner ear, usually will heal on their own. However, in rare cases, surgery may be needed to repair them.
- Barotrauma Vis-a-Vis the “Chronic Otitis Media Syndrome”: Two Conditions with Middle Ear Gas Deficiency: Is Secretory Otitis Media a Contraindication to Air Travel? Annals of Otology, Rhinology & Laryngology Vol 112, Issue 3, pp. 230 – 235. http://journals.sagepub.com/doi/abs/10.1177/000348940311200307[↩]





{kind=link}