
Contents
What is anaplasmosis
Anaplasmosis is a tickborne disease caused by the bacterium Anaplasma phagocytophilum 1). Anaplasmosis was previously known as human granulocytic ehrlichiosis and later as human granulocytic anaplasmosis. Both of these names refer to the same disease, now known as anaplasmosis. The Anaplasma phagocytophilum bacteria is primarily spread to people by tick bites from the blacklegged tick (Ixodes scapularis) in the Northeast and Midwestern United States and the western blacklegged tick (Ixodes pacificus) along the West Coast 2). Anaplasmosis is most commonly reported in the Northeastern and upper Midwestern states. In rare cases, Anaplasma phagocytophilum has been spread by blood transfusion.
Anaplasmosis occurs in parts of the United States and Europe. About 600–800 cases of anaplasmosis are reported in the United States each year, but this is also likely to be an underestimate as some people do not become ill or experience only very mild symptoms and do not seek medical treatment. Ixodes ticks are the principal tick vectors of anaplasmosis.
- People with anaplasmosis will often have fever, headache, chills, and muscle aches.
- Signs and symptoms vary greatly from person to person.
- Most people will have mild or moderate illness, though severe illness and death are possible.
- Signs and symptoms typically begin within 5–14 days after the bite of an infected tick. However, because tick bites are not painful, many people will not remember a tick bite.
Progression of anaplasmosis varies greatly from person to person and may depend on patient age, co-morbid conditions, immune status and time of treatment. Patients who are treated early may recover quickly with outpatient treatment with oral antibiotics, while those who experience a more severe course might require intravenous antibiotics, prolonged hospitalization or intensive care.
The diagnosis of anaplasmosis often is made based on clinical signs and symptoms, and can later be confirmed using specialized confirmatory laboratory tests. Treatment should not be delayed pending the receipt of laboratory test results, or withheld on the basis of an initial negative laboratory result. Doxycycline is the drug of choice for adults and children of all ages with anaplasmosis 3).
Figure 1. Ixodes scapularis (blacklegged tick)

Figure 2. Ixodes scapularis (blacklegged tick) geographic distribution
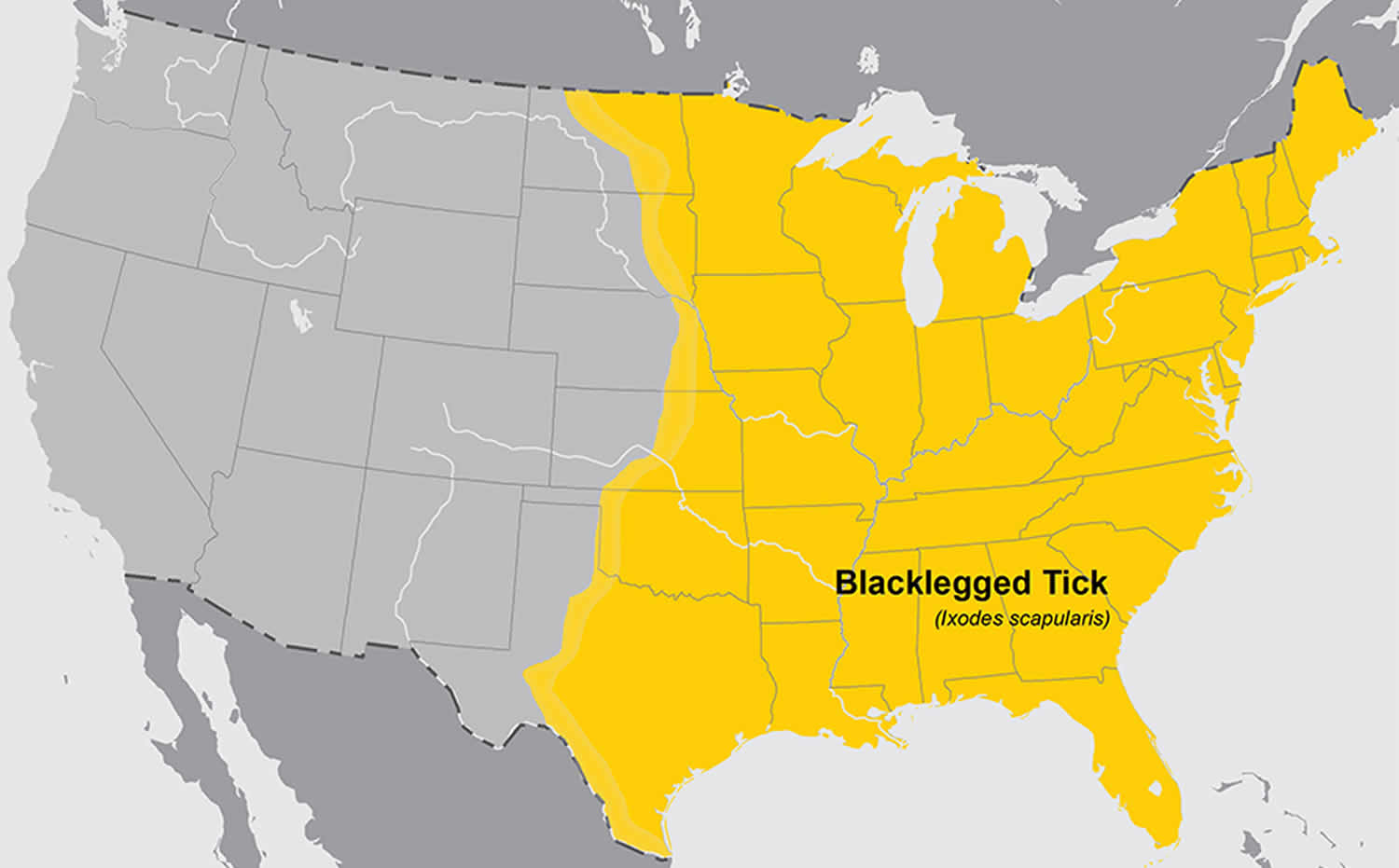
Figure 3. Ixodes pacificus (western blacklegged tick)

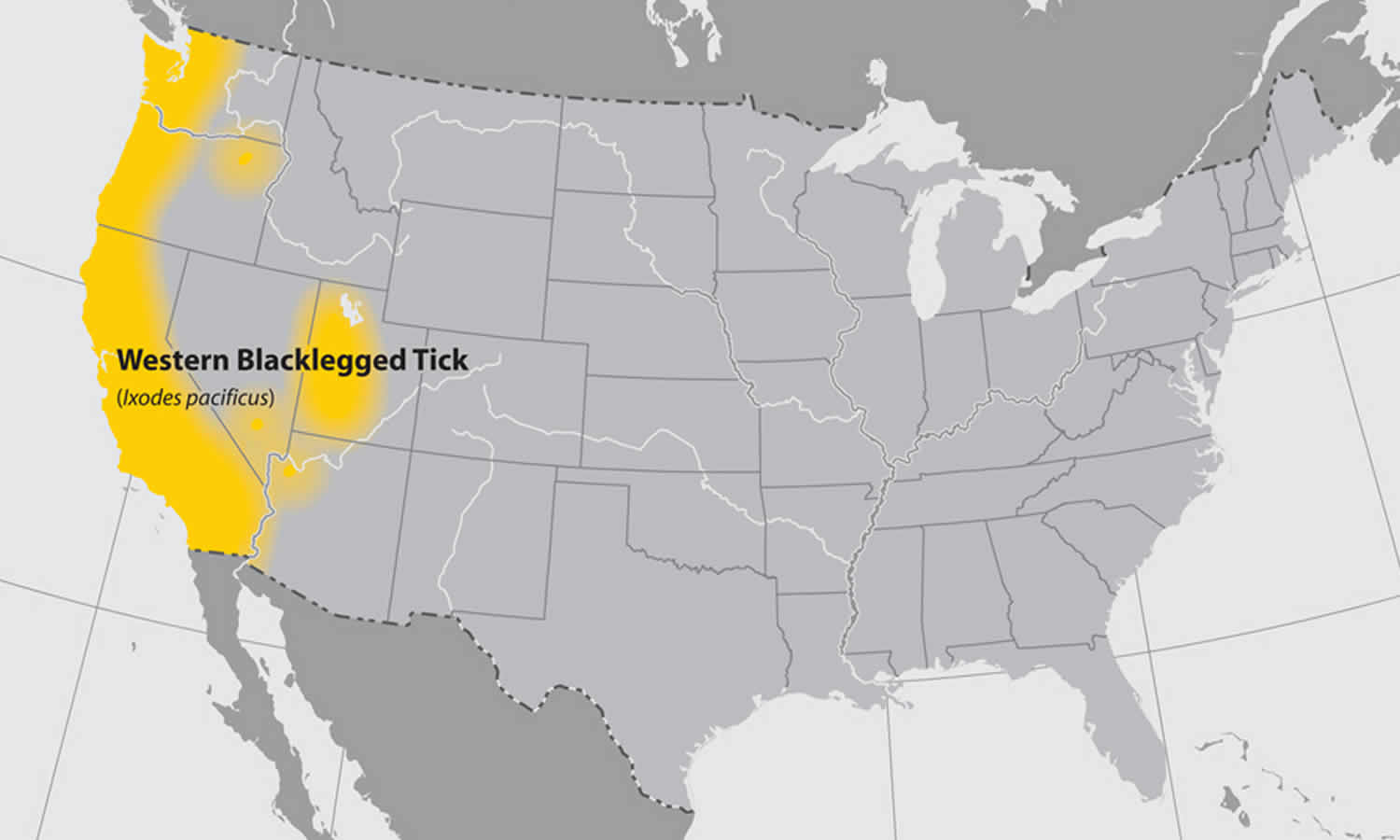
Figure 4. Ixodes pacificus (western blacklegged tick) geographic distribution
Is anaplasmosis contagious?
No. Anaplasmosis is a tickborne disease caused by the bacterium Anaplasma phagocytophilum 4). The Anaplasma phagocytophilum bacteria is primarily spread to people by tick bites from the blacklegged tick (Ixodes scapularis) in the Northeast and Midwestern United States and the western blacklegged tick (Ixodes pacificus) along the West Coast 5). Anaplasmosis is most commonly reported in the Northeastern and upper Midwestern states. In rare cases, Anaplasma phagocytophilum has been spread by blood transfusion.
Anaplasmosis prevention
There is no vaccine to prevent anaplasmosis. Prevent illness by preventing tick bites, preventing ticks on your pets, and preventing ticks in your yard.
Ticks live in grassy, brushy, or wooded areas, or even on animals, so spending time outside camping, gardening, or hunting will bring you in close contact with ticks. Protect yourself, your family, and your pets. Here’s how:
- Tick exposure can occur year-round, but ticks are most active during warmer months (April-September).
- Know which ticks are most common in your area.
Before You Go Outdoors
- Ticks live in grassy, brushy, or wooded areas, or even on animals. Spending time outside walking your dog, camping, gardening, or hunting could bring you in close contact with ticks. Many people get ticks in their own yard or neighborhood.
- Treat clothing and gear with products containing 0.5% permethrin. Permethrin can be used to treat boots, clothing and camping gear and remain protective through several washings.
- Use Environmental Protection Agency (EPA)-registered insect repellents containing DEET, picaridin, IR3535, Oil of Lemon Eucalyptus (OLE), para-menthane-diol (PMD), or 2-undecanone. Environmental Protection Agency’s (EPA) helpful search tool (https://www.epa.gov/insect-repellents/find-repellent-right-you) can help you find the product that best suits your needs. Always follow product instructions.
- Do NOT use insect repellent on babies younger than 2 months old.
- Do NOT use products containing Oil of Lemon Eucalyptus (OLE) or para-menthane-diol (PMD) on children under 3 years old.
- Avoid Contact with Ticks
- Avoid wooded and brushy areas with high grass and leaf litter.
- Walk in the center of trails.
After You Come Indoors
Check your clothing for ticks. Ticks may be carried into the house on clothing. Any ticks that are found should be removed. Tumble dry clothes in a dryer on high heat for 10 minutes to kill ticks on dry clothing after you come indoors. If the clothes are damp, additional time may be needed. If the clothes require washing first, hot water is recommended. Cold and medium temperature water will not kill ticks.
Shower soon after being outdoors. Showering within two hours of coming indoors has been shown to reduce your risk of getting Lyme disease and may be effective in reducing the risk of other tickborne diseases. Showering may help wash off unattached ticks and it is a good opportunity to do a tick check.
Check your body for ticks after being outdoors. Conduct a full body check upon return from potentially tick-infested areas, including your own backyard. Use a hand-held or full-length mirror to view all parts of your body. Check these parts of your body and your child’s body for ticks:
- Under the arms
- In and around the ears
- Inside belly button
- Back of the knees
- In and around the hair
- Between the legs
- Around the waist
Examine gear and pets. Ticks can ride into the home on clothing and pets, then attach to a person later, so carefully examine pets, coats, and daypacks.
Anaplasmosis symptoms
Signs and symptoms of anaplasmosis typically begin within 1–2 weeks after the bite of an infected tick. Tick bites are usually painless, and many people do not remember being bitten.
See your healthcare provider if you become ill after having been bitten by a tick or having been in the woods or in areas with high brush where ticks commonly live.
Maintain a high level of clinical suspicion for anaplasmosis or other tickborne diseases in cases of non-specific febrile illness of unknown origin, particularly during spring and summer months when ticks are most active. Early recognition and presumptive treatment is important to prevent severe illness.
Early anaplasmosis
Early signs and symptoms (days 1-5) are usually mild or moderate and may include:
- Fever, chills
- Severe headache
- Muscle aches
- Nausea, vomiting, diarrhea, loss of appetite
Rarely reported
- Rash (<10% of cases) in patients with anaplasmosis. The presence of a rash might indicate a coinfection with Lyme disease, or another tickborne disease.
- Nervous system involvement (e.g., meningoencephalitis, focal paralysis, etc.)
Late anaplasmosis
Rarely, if treatment is delayed or if there are other medical conditions present, anaplasmosis can cause severe illness. Prompt treatment can reduce your risk of developing severe illness.
Signs and symptoms of severe (late stage) anaplasmosis can include:
- Respiratory failure
- Renal failure
- Peripheral neuropathies
- Bleeding problems or disseminated intravascular coagulation (DIC)-like coagulopathies
- Rhabdomyolysis
- Hemorrhage
- Organ failure
- Death
Risk factors for severe anaplasmosis:
- Delayed treatment
- Age: being older puts you at risk
- Weakened immune system: People with weakened immune systems (such as those receiving some cancer treatments, individuals with advanced HIV infection, prior organ transplants, or people taking some medications) are at risk for severe illness.
Anaplasma co-infections
In addition to Anaplasma phagocytophilum, the blacklegged tick also transmits several other pathogens in certain geographic areas, including:
- Borrelia burgdorferi (the causative agent of Lyme disease),
- Babesia microti (the primary cause of human babesiosis),
- Borrelia mayonii (a newly discovered cause of borreliosis),
- Borrelia miyamotoi (a cause of tickborne relapsing fever)
- Powassan virus (cause of Powassan virus disease), and
- Ehrlichia muris eauclairensis
Risk of coinfection
- Anaplasma coinfection with non-rickettsial pathogens has been reported in <10% of patients.
- Rash is rarely reported (<10% of cases) in patients with anaplasmosis. The presence of a rash might indicate that the patient has a coinfection with Lyme disease, or another tickborne disease.
Anaplasmosis diagnosis
Because anaplasmosis can be difficult to diagnose, particularly in the early stages of illness, patients should treated presumptively based on clinical suspicion.
Always a thorough patient history, including:
- Recent tick bite. NOTE: Tick bites are often painless. Many people do not remember being bitten. Do not rule out a tickborne infection if you do not remember a tick bite.
- Exposure to areas where ticks are commonly found, including wooded areas or brushy areas with high grasses and leaf litter.
- Travel history (domestic and international) to areas where anaplasmosis is endemic.
- Laboratory confirmation is helpful for disease surveillance and understanding burden of anaplasmosis infection in the United States.
Your healthcare provider can order certain blood tests to look for evidence of anaplasmosis or other illnesses that cause similar symptoms.
Test results may take several weeks.
If your healthcare provider thinks you have anaplasmosis, or another tickborne infection, he or she may prescribe antibiotics while you wait for test results.
Anaplasmosis test
Diagnostic test should be run on those with illness clinically compatible with anaplasmosis. However, treatment should not be delayed on the basis of diagnostic testing.
- The optimal diagnostic test may depend on the timing relative to symptom onset and the type of specimen(s) available for testing.
- Testing for anaplasmosis should be considered for any person with a compatible illness and known risk factors, such as:
- Living in or having traveled to an area with anaplasmosis
- Illness occurring during times of year with high tick activity (spring, summer, or fall)
- Those who remember a tick bite
- Anaplasmosis is a nationally notifiable condition. Correct testing and reporting of anaplasmosis is important to improve our understanding of how common this disease is, where it occurs, and how disease trends change over time.
PCR
- Polymerase chain reaction (PCR) amplification is performed on DNA extracted from whole blood specimens.
- This method is most sensitive in the first week of illness, and decreases in sensitivity following the administration of appropriate antibiotics (within 24–48 hours).
- Although a positive polymerase chain reaction (PCR) result is helpful, a negative result does not rule out the diagnosis, and treatment should not be withheld due to a negative result.
- Polymerase chain reaction (PCR) might also be used to amplify DNA in solid tissue and bone marrow specimens.
Serology
- The standard serologic test for diagnosis of anaplasmosis is the indirect immunofluorescence antibody (IFA) assay for immunoglobulin G (IgG) using Anaplasma phagocytophilum antigen.
- IgG immunofluorescence antibody assays should be performed on paired acute and convalescent serum samples collected 2–4 weeks apart to demonstrate evidence of a fourfold seroconversion.
- Antibody titers are frequently negative in the first week of illness. Anaplasmosis cannot be confirmed using single acute antibody results.
- Immunoglobulin M (IgM) immunofluorescence antibody assays may also be offered by reference laboratories, however are not necessarily indicators of acute infection and might be less specific than IgG antibodies.
- Antibodies, particularly IgM antibodies, might remain elevated in patients for whom no other supportive evidence of a recent rickettsiosis infection exists. For these reasons, IgM antibody titers alone should not be used for laboratory diagnosis.
Persistent Antibodies
- Antibodies to phagocytophilum might remain elevated for many months after the disease has resolved.
- In certain people, high titers of antibodies againstAnaplasma phagocytophilum have been observed up to four years after the acute illness.
- Between 5–10% of healthy people in some areas might have elevated antibody titers due to past exposure to Anaplasma phagocytophilum or similar organisms.
- Comparison of paired, and appropriately timed, serologic assays provides the best evidence of recent infection.
- Single or inappropriately timed serologic tests, in relation to clinical illness, can lead to misinterpretation of results.
Blood-smear Microscopy
- During the first week of illness a microscopic examination of a peripheral blood smear might reveal morulae (microcolonies of anaplasmae) in the cytoplasm of granulocytes and is highly suggestive of a diagnosis.
- However, blood smear examination is relatively insensitive and should not be relied upon solely to diagnose anaplasmosis.
- The observance of morulae in a particular cell type cannot conclusively differentiate between Anaplasma and Ehrlichia species.
Immunohistochemical assays and culture
- Culture isolation and immunohistochemical assays of Anaplasma phagocytophilum are only available at specialized laboratories; routine hospital blood cultures cannot detect the organism.
- Polymerase chain reaction (PCR), culture, and immunohistochemical assays can also be applied to autopsy tissue specimens.
- If a bone marrow biopsy is performed as part of the investigation of cytopenias, immunostaining of the bone marrow biopsy specimen can diagnose Anaplasma phagocytophilum infection.
Anaplasmosis treatment
Doxycycline is the treatment of choice for anaplasmosis, and all other tickborne rickettsial diseases 6). Presumptive treatment with doxycycline is recommended in patients of all ages, including children <8 years 7).
Doxycycline is most effective at preventing severe complications from developing if it is started early in the course of disease.
Treatment Duration
- When treated with doxycycline, fever generally subsides within 24–48 hours.
- Lack of a clinical response to doxycycline suggests that the patient’s condition might not be due to anaplasmosis, or might be caused by other infections not responsive to doxycycline (see coinfections).
- Resistance to doxycycline or relapses in symptoms after the completion of the recommended course have not been documented.
Recommended Treatment and Dosage for Anaplasmosis
- Doxycycline is the first-line treatment for adults and children of all ages:
- Adults: 100 mg every 12 hours
- Children under 45 kg (100 lbs): 2.2 mg/kg body weight given twice a day
Patients with suspected anaplasmosis should be treated with doxycycline for 10–14 days to provide appropriate length of therapy for possible concurrent Lyme disease infection.
Treating Children and Pregnant Women
The use of doxycycline to treat suspected rickettsial disease in children is standard practice recommended by both CDC and the American Academy of Pediatrics Committee on Infectious Diseases.
- A recent study found that short courses of doxycycline (5–10 days) did not result in staining of permanent teeth or enamel hypoplasia. Use doxycycline as the first-line treatment for suspected anaplasmosis in patients of all ages.
- Use of antibiotics other than doxycycline increases the risk of severe illness and patient death.
Other Treatments
- In cases of life-threatening allergies to doxycycline, severe doxycycline intolerance, and in some pregnant patients for whom the clinical course of anaplasmosis appears mild, physicians should consider alternate antibiotics.
- Rifampin has been used successfully in several pregnant women with anaplasmosis, and studies suggest that this drug appears effective against A. phagocytophilum.
- Small numbers of children <8 years of age have also been treated successfully for anaplasmosis with rifampin following a 7–10 day course.
- However, rifampin is not effective in treating Rocky Mountain Spotted Fever, a disease that might be confused with anaplasmosis, nor is it an effective treatment for potential coinfection with Lyme disease.
- Healthcare providers should be cautious when exploring treatments other than doxycycline, which is highly effective in treating multiple tickborne diseases including anaplasmosis, ehrlichiosis, Lyme disease, and Rocky Mountain Spotted Fever.
Antibiotics as Prophylaxis
- Post-tick bite antibiotic prophylaxis is not recommended to prevent anaplasmosis.
- People who have been bitten by a tick should watch for signs and symptoms. They should see their healthcare provider if fever, rash, or other symptoms develop within two weeks of tick bite.
- Asymptomatic treatment for tick bites is not currently recommended.
References [ + ]





{kind=link}