Contents
What is capsicum
Capsicum is commonly known as red pepper or chili pepper that is a genus of flowering plants in the nightshade family Solanaceae with approximately 35 species, comprises the well-known sweet and hot chili peppers and several wild species 1. Capsicum species are native to the tropical and temperate Americas and distributed from Mexico to Brazil, Paraguay and Central Argentina, where they have been cultivated for thousands of years 2. The capsicum genus is of great economic importance because it includes the sweet and hot chili peppers, which are vegetables and spices cultivated and consumed worldwide. The economically most important species belong to the Capsicum annuum complex (Capsicum annuum, Capsicum chinense and Capsicum frutescens); two other species (Capsicum baccatum and Capsicum pubescens) are cultivated predominantly in Latin America 3.
The capsicum fruit (technically berries in the strict botanical sense) plants have a variety of names depending on place and type. The more piquant varieties are commonly called chili peppers, or simply chilis. The large, mild form is called bell pepper, or by color or both (green pepper, green bell pepper, red bell pepper, etc.) in North America and the United Kingdom, but typically called capsicum in New Zealand, Australia, South Africa, Singapore, and India. Capsicum fruits of several varieties with commercial value are called by various European-language names in English, such as jalapeño, peperoncini, and peperoncito; many of these are usually sold pickled. Paprika (in English) refers to a powdered spice made of dried Capsicum of several sorts, though in Hungary and some other countries it is the name of the fruit as well. Both whole and powered chili are frequent ingredients in dishes prepared throughout the world, and characteristic of several cuisine styles, including Mexican, Sichuan (Szechuan) Chinese, Cajun and Creole, along with most South Asian and derived (e.g. Jamaican) curries 4. The powdered form is a key ingredient in various commercially prepared foodstuffs, such as pepperoni (a sausage), and chili con carne (a stew), and hot sauces.
Capsicum species are shrubs (annuals in cultivation and as weeds) that produce flowers with mostly stellate to rotate corollas (exceptionally also urceolate or campanulate) that show diverse patterns of pigmentation, and fleshy, mostly globose berries of different sizes and colors (Figures 2 and 3). At the morphological level, Capsicum exhibits an exceptional feature in Solanaceae, which is an entire cup-shaped calyx, mostly with five to ten teeth as nerve prolongations (Figures 2 and 3), shared only with Lycianthes. The two genera differ in two main characters: the anther opening by longitudinal slits and the presence of a nectary in Capsicum, in contrast to the anther opening by apical pores and the absence of a nectary in Lycianthes. Another remarkable feature of Capsicum is the occurrence of dysploidy, as the base chromosome number can be either x = 12 or 13 5. Probably the most singular character in Capsicum is fruit pungency due to the production of capsaicinoids, an exclusive group of alkaloids synthesized in the placenta of the fruits 6 and also in the pericarp in ‘super-hot’ chili peppers 7. However, non-pungent fruits are produced in some species (e.g. Capsicum rhomboideum, Capsicum geminifolium) and particular cultivars 6.
Many varieties of the same species can be used in many different ways; for example, Capsicum annuum includes the “bell pepper” variety, which is sold in both its immature green state and its red, yellow, or orange ripe state. This same species has other varieties, as well, such as the Anaheim chillies often used for stuffing, the dried ancho (also sometimes referred to as poblano) chili used to make chili powder, the mild-to-hot jalapeno, and the smoked, ripe jalapeno, known as chipotle.
Capsicum is also taken by mouth for various problems with digestion including upset stomach, intestinal gas, stomach pain, diarrhea, and cramps. It is also used for conditions of the heart and blood vessels including poor circulation, excessive blood clotting, high cholesterol, and preventing heart disease. Some people use capsicum for burning mouth syndrome, improving exercise performance, irritable bowel syndrome (IBS), joint pain, stomach ulcers, weight loss, seasickness, toothaches, difficulty swallowing, alcoholism, malaria, and fever.
Some people apply capsicum to the skin for pain caused by shingles, osteoarthritis, rheumatoid arthritis, fibromyalgia, diabetes, HIV, and a certain condition that causes facial pain (trigeminal neuralgia). It is also used for muscular pain, back pain, and pain after surgery.
Some people apply capsicum to relieve muscle spasms, for skin eruptions (prurigo nodularis), to prevent nausea and vomiting after surgery, as a gargle for laryngitis, and to discourage thumb-sucking or nail-biting.
Some people put capsicum inside the nose to treat hay fever, migraine headache, cluster headache, and sinus infections (sinusitis).
One form of capsicum is currently being studied as a drug for migraine, osteoarthritis, and other painful conditions.
A particular form of capsicum causes intense eye pain and other unpleasant effects when it comes in contact with the face. This form is used in self-defense pepper sprays.
Peru is thought to be the country with the highest cultivated Capsicum diversity since varieties of all five domesticates are commonly sold in markets in contrast to other countries. Bolivia is considered to be the country where the largest diversity of wild Capsicum peppers are consumed. Bolivian consumers distinguish two basic forms: ulupicas, species with small round fruits including Capsicum eximium, Capsicum cardenasii, Capsicum eshbaughii, and Capsicum caballeroi landraces; and arivivis, with small elongated fruits including Capsicum baccatum var. baccatum and Capsicum chacoense varieties 8.
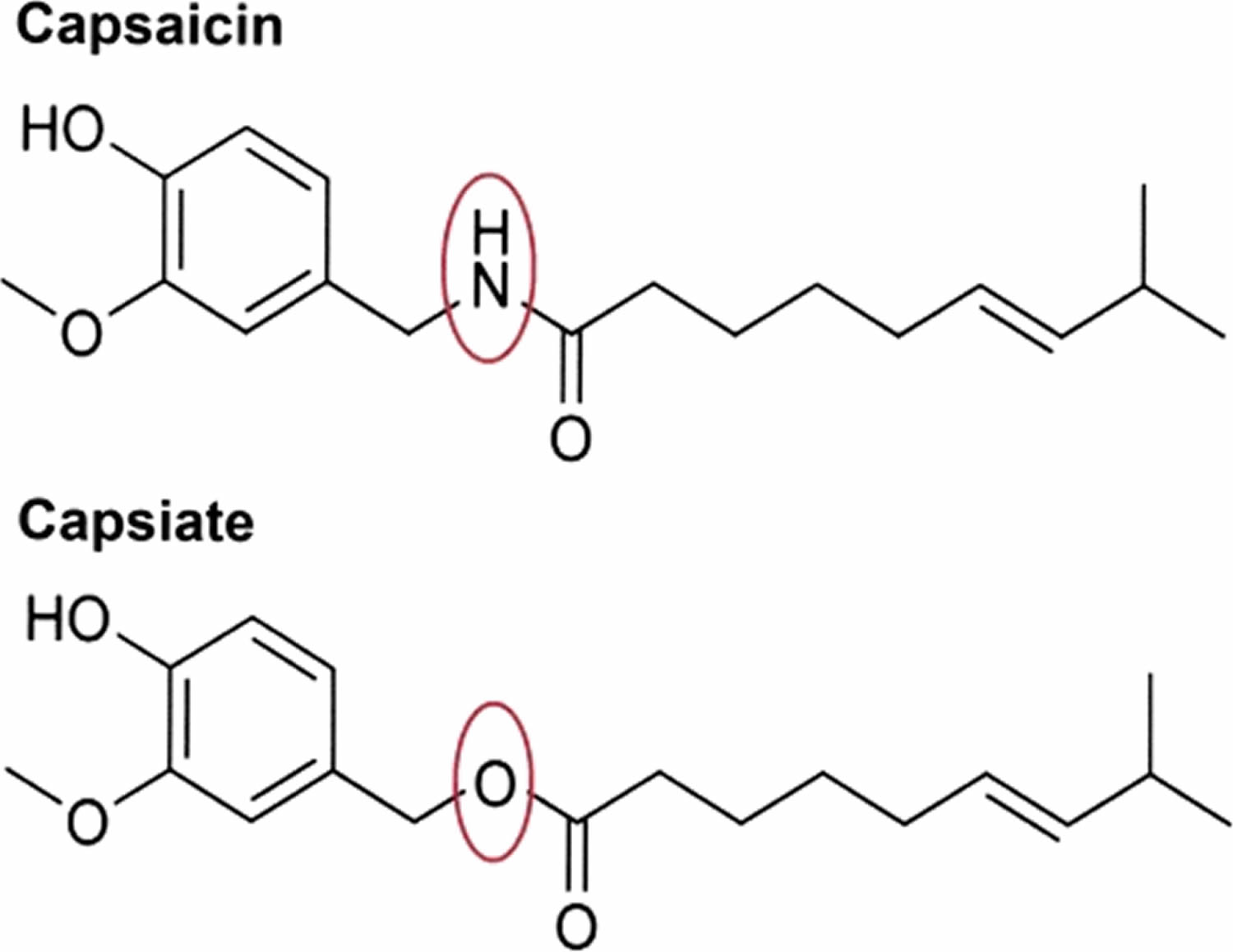
Hot red peppers contain pungent compounds called capsaicinoids. These include capsaicin, dihydrocapsaicin, nordihydrocapsaicin, and trace amounts of other compounds. Capsaicin (trans-8-methyl-N-vanillyl-6-nonenamide) is the major pungent agent, responsible for about 70% of the burn, of hot red peppers. The newly bred nonpungent red pepper variety, CH-19 Sweet (Capsicum annuum L.), contains capsinoids. These are nonpungent capsaicin analogs and include capsiate, dihydrocapsiate, and nordihydrocapsiate. Capsiate is the primary capsinoid present in CH-19 Sweet peppers 9.
The fruit of most species of capsicum contains Capsaicin (trans-8-methyl-N-vanillyl-6-nonenamide), a lipophilic chemical responsible for making chilli peppers hot when eaten. Capsaicin can produce a strong burning sensation (pungency or spiciness) in the mouth of the unaccustomed eater 10. Along with other related compounds, capsaicin belongs to a group of chemicals identified as capsaicinoids. Capsaicin produces a burning sensation when a tissue comes into contact with it. This occurs via binding to transient receptor potential vanilloid 1 (TRPV1) receptor (sensory receptors responsible for sending signals that cause the perception of pain), which controls movement of sodium and calcium ions across the cell membrane, which can be stimulated by heat and physical abrasion. Binding of capsaicin to transient receptor potential vanilloid 1 (TRPV1) results in a similar burning sensation. Initially, binding opens the ion channel (influx of sodium and calcium ions), causing depolarization and the production of action potentials, which are usually perceived as itching, pricking, or burning sensations. Repeated Capsaicin applications or high concentrations give rise to a long-lasting effect, which has been termed ‘defunctionalisation’, probably owing to a number of different effects that together overwhelm the cell’s normal functions, and can lead to reversible degeneration of nerve terminals 11.
Capsaicin is a chili pepper extract with analgesic properties. Capsaicin is a neuropeptide releasing agent selective for primary sensory peripheral neurons. Used topically, capsaicin aids in controlling peripheral nerve pain 10. Capsaicin has been used experimentally to manipulate substance P and other tachykinins. In addition, capsaicin may be useful in controlling chemotherapy- and radiotherapy-induced mucositis. As a topical medication, capsaicin has been used for neuralgias and psoriasis. Several similar compounds are currently being tested in clinical trials.
The secretion of capsaicin protects the fruit from consumption by insects and mammals, while the bright colors attract birds that will disperse the seeds. Besides capsaicin use as a food additive in various spicy cuisines, capsaicin is currently utilized for therapeutic purposes to treat various peripheral painful conditions such as rheumatoid arthritis and diabetic neuropathy 10.
The capsaicin content of green and red peppers ranges from 0. 1 to 1% 10. Capsaicin evokes numerous biological effects and thus has been the target of extensive investigations since its initial identification in 1919. One of the most recognized physiological properties of capsaicin is its selective effects on the peripheral part of the sensory nervous system, particularly on the primary afferent neurons. The compound is known to deplete the neurotransmitter of painful impulses known as substance P from the sensory nerve terminals, which provides a rationale for its use as a versatile experimental tool for studying pain mechanisms and also for pharmacotherapy to treat some peripheral painful states, such as rheumatoid arthritis, post-herpetic neuralgia, post-mastectomy pain syndrome and diabetic neuropathy. Considering the frequent consumption of capsaicin as a food additive and its current therapeutic application, correct assessment of any harmful effects of this compound is important from the public health standpoint. Ingestion of large amounts of capsaicin has been reported to cause histopathological and biochemical changes, including erosion of gastric mucosa and hepatic necrosis. However, there are contradictory data on the mutagenicity of capsaicin. A recent epidemiological study conducted in Mexico revealed that consumers of chili pepper were at higher risk for gastric cancer than non-consumers. However, it remains unclear whether capsaicin present in hot chili pepper is a major causative factor in the cause of gastric cancer in humans. A growing number of recent studies have focused on anticarcinogenic or antimutagenic phytochemicals, particularly those included in human diet. In summary, capsaicin has dual effects on chemically induced carcinogenesis and mutagenesis. Although a minute amount of capsaicin displays few or no deleterious effects, heavy ingestion of the compound has been associated with necrosis, ulceration and even carcinogenesis 10. Capsaicin is considered to be metabolized by cytochrome P-450-dependent mixed-function oxidases to reactive species 10.
Most of the capsaicin in a pungent (hot) pepper is concentrated in blisters on the epidermis of the interior ribs (septa) that divide the chambers, or locules, of the fruit to which the seeds are attached 12. A study on capsaicin production in fruits of Capsicum chinense showed that capsaicinoids are produced only in the epidermal cells of the interlocular septa of pungent fruits, that blister formation only occurs as a result of capsaicinoid accumulation, and that pungency and blister formation are controlled by a single locus, Pun1, for which there exist at least two recessive alleles that result in non-pungency of Capsicum chinense fruits 13. The seeds themselves do not produce any capsaicin, although the highest concentration of capsaicin can be found in the white pith around the seeds 14.
The amount of capsaicin in hot peppers varies significantly among varieties, and is measured in Scoville heat units (SHU). The world’s current hottest known pepper as rated in SHU is the ‘Carolina Reaper,’ which had been measured at over 2,200,000 SHU.
The amount of capsaicin in the fruit is highly variable and dependent on genetics and environment, giving almost all types of Capsicum varied amounts of perceived heat. Chili peppers are of great importance in Native American medicine, and capsaicin is used in modern medicine—mainly in topical medications—as a circulatory stimulant and analgesic. In more recent times, an aerosol extract of capsaicin, usually known as capsicum or pepper spray, has become used by law enforcement as a nonlethal means of incapacitating a person, and in a more widely dispersed form for riot control, or by individuals for personal defense. Pepper in vegetable oils, or as an horticultural product can be used in gardening as a natural insecticide 15.
Although black pepper causes a similar burning sensation, it is caused by a different substance—piperine.
Figure 1. Capsicum pepper

Figure 2. Flowers and fruits of the Andean capsicum
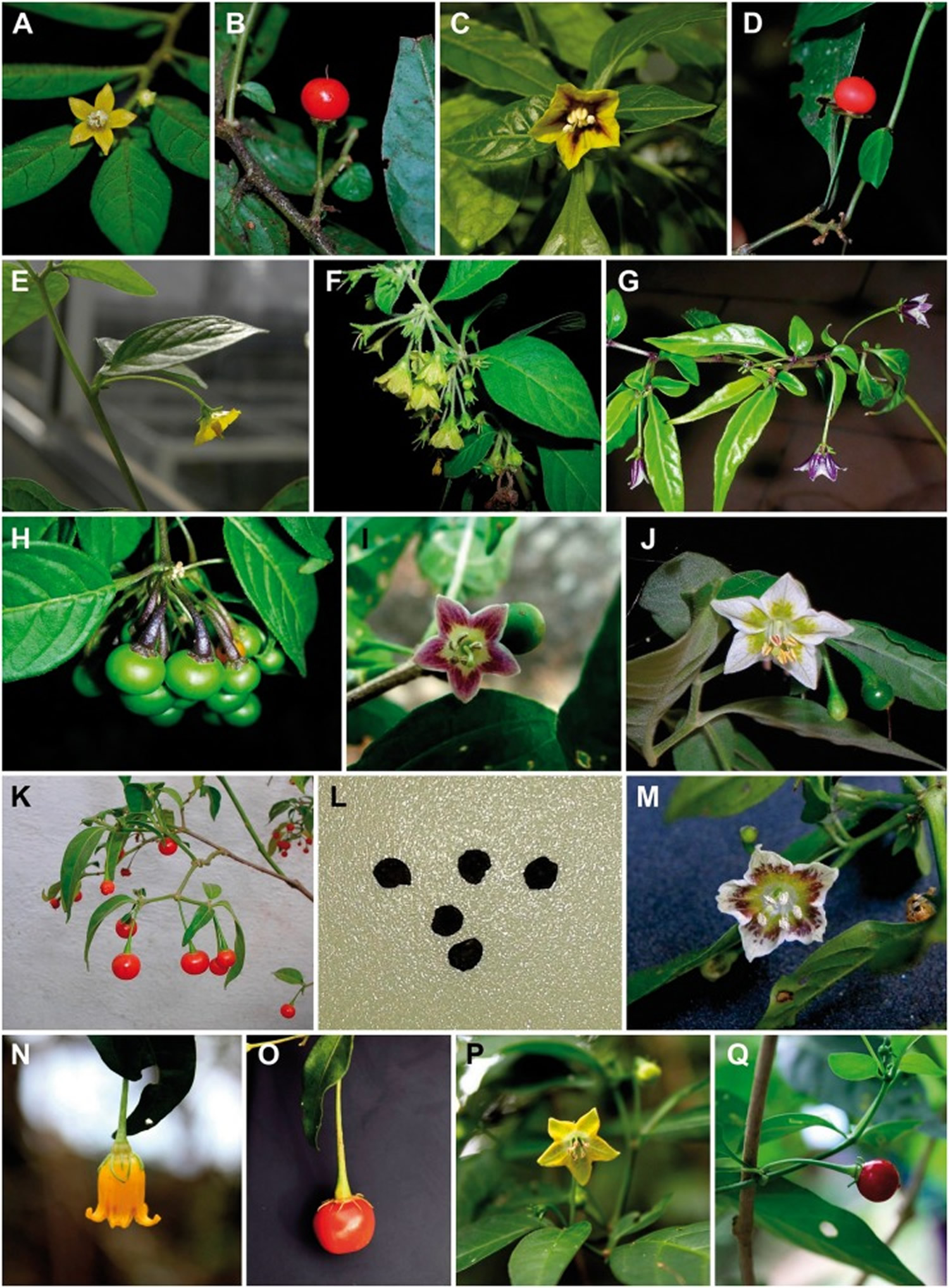
Footnotes: Flowers and fruits of the Andean (A–G), Caatinga (H, I), Flexuosum (J–M) and Bolivian (N–Q) clades. (A, B) Capsicum dimorphum flower (A) and fruit (B). (C, D) Capsicum geminifolium flower (C) and fruit (D). (E, F) Different accessions of C. rhomboideum showing variations in corolla shape (rotate-campanulate in E vs. campanulate in F) and flower arrangement (solitary flowers in E vs. multi-flowered fascicles in F); pedicels always non-geniculate. (G) Capsicum lanceolatum flowering branch showing non-geniculate pedicels and white and violet corollas. (H) Capsicum caatingae fascicle of immature fruits (note the toothless calyx). (I) Capsicum parvifolium flower and immature fruit. (J–L) Capsicum flexuosum flower (J), fruiting branch, showing red pendant mature fruits (K) and blackish brown seeds (L). (M) Capsicum aff. flexuosum flower. (N, O) Capsicum caballeroi flower (N) and mature fruit (O) showing fully yellow corolla, non-geniculate pedicels and red pericarp. (P, Q) Capsicum minutiflorum flower (P) and mature dark red fruit (Q).
[Source 16]Figure 3. Flowers and fruits of the Longidentatum capsicum

Footnotes: Flowers and fruits of the Longidentatum (A), Atlantic (B–I), Purple Corolla (J–K), Pubescens (L, M), Baccatum (N, O) and Annuum (P, Q) clades. (A) Capsicum longidentatum fruit. (B) Capsicum cornutum flower with stellate corolla and geniculate pedicel. (C) Capsicum pereirae flower with spotted stellate corolla. (D) Capsicum friburgense urceolate-campanulate corolla and pedicel geniculate. (E) Capsicum mirabile stellate corolla with dark red spots. (F) Capsicum hunzikerianum flower with spotted stellate corolla. (G, H) Capsicum sp. nov. (GEB & CCG 3637) stellate corolla with golden-green spots (G) and mature greenish-golden yellow fruit, without well-developed calyx teeth (H). Note the different patterns of spots in the corolla in C and E–G. (I) Capsicum villosum var. muticum immature fruit; note the absence of well-developed teeth. (J) Capsicum cardenasii pendant flower with shortly tubular corolla and non-geniculate flowering pedicel. (K) Capsicum eximium flower with stellate corolla. (L, M) Capsicum pubescens flower (L) and longitudinal section of a mature fruit showing large blackish brown seeds (M). (N) Capsicum baccatum var. pendulum flower showing the distinctive green spots in the corolla. (O) Capsicum chacoense flower showing immaculate white corolla and geniculate flowering pedicel. (P) Capsicum annuum var. annuum flowering and fruiting branch showing typical white corolla and entire calyx without well-developed teeth. (Q) Capsicum chinense flowering branch showing pendant flowers with non-geniculate flowering pedicels and entire calyx without well-developed teeth.
[Source 16]Capsicum nutrition
Capsicums are highly nutritious. They have more vitamin C than an orange, and a typical bell pepper contains more than 100% of the daily recommended value for vitamin C. Capsicums also have relatively high amounts of vitamin B6 (Pyridoxine). Fresh capsicum fruit is 94% water. Dried capsicum fruit has a much different nutritional value due to the dehydration and concentration of vitamins and minerals.
Table 1. Capsicum sweet, green and raw nutrition facts
| Nutrient | Unit | Value per 100 g | |||||||
| Approximates | |||||||||
| Water | g | 93.89 | |||||||
| Energy | kcal | 20 | |||||||
| Energy | kJ | 84 | |||||||
| Protein | g | 0.86 | |||||||
| Total lipid (fat) | g | 0.17 | |||||||
| Ash | g | 0.43 | |||||||
| Carbohydrate, by difference | g | 4.64 | |||||||
| Fiber, total dietary | g | 1.7 | |||||||
| Sugars, total | g | 2.4 | |||||||
| Sucrose | g | 0.11 | |||||||
| Glucose (dextrose) | g | 1.16 | |||||||
| Fructose | g | 1.12 | |||||||
| Lactose | g | 0 | |||||||
| Maltose | g | 0 | |||||||
| Galactose | g | 0 | |||||||
| Starch | g | 0 | |||||||
| Minerals | |||||||||
| Calcium, Ca | mg | 10 | |||||||
| Iron, Fe | mg | 0.34 | |||||||
| Magnesium, Mg | mg | 10 | |||||||
| Phosphorus, P | mg | 20 | |||||||
| Potassium, K | mg | 175 | |||||||
| Sodium, Na | mg | 3 | |||||||
| Zinc, Zn | mg | 0.13 | |||||||
| Copper, Cu | mg | 0.066 | |||||||
| Manganese, Mn | mg | 0.122 | |||||||
| Selenium, Se | µg | 0 | |||||||
| Fluoride, F | µg | 2 | |||||||
| Vitamins | |||||||||
| Vitamin C, total ascorbic acid | mg | 80.4 | |||||||
| Thiamin | mg | 0.057 | |||||||
| Riboflavin | mg | 0.028 | |||||||
| Niacin | mg | 0.48 | |||||||
| Pantothenic acid | mg | 0.099 | |||||||
| Vitamin B-6, Pyridoxine | mg | 0.224 | |||||||
| Folate, total | µg | 10 | |||||||
| Folic acid | µg | 0 | |||||||
| Folate, food | µg | 10 | |||||||
| Folate, DFE | µg | 10 | |||||||
| Choline, total | mg | 5.5 | |||||||
| Betaine | mg | 0.1 | |||||||
| Vitamin B-12 | µg | 0 | |||||||
| Vitamin B-12, added | µg | 0 | |||||||
| Vitamin A, RAE | µg | 18 | |||||||
| Retinol | µg | 0 | |||||||
| Carotene, beta | µg | 208 | |||||||
| Carotene, alpha | µg | 21 | |||||||
| Cryptoxanthin, beta | µg | 7 | |||||||
| Vitamin A, IU | IU | 370 | |||||||
| Lycopene | µg | 0 | |||||||
| Lutein + zeaxanthin | µg | 341 | |||||||
| Vitamin E (alpha-tocopherol) | mg | 0.37 | |||||||
| Vitamin E, added | mg | 0 | |||||||
| Tocopherol, beta | mg | 0 | |||||||
| Tocopherol, gamma | mg | 0 | |||||||
| Tocopherol, delta | mg | 0 | |||||||
| Vitamin D (D2 + D3) | µg | 0 | |||||||
| Vitamin D | IU | 0 | |||||||
| Vitamin K (phylloquinone) | µg | 7.4 | |||||||
| Lipids | |||||||||
| Fatty acids, total saturated | g | 0.058 | |||||||
| 04:00:00 AM | g | 0 | |||||||
| 06:00:00 AM | g | 0 | |||||||
| 8:0 | g | 0 | |||||||
| 10:0 | g | 0 | |||||||
| 12:0 | g | 0 | |||||||
| 14:0 | g | 0 | |||||||
| 15:0 | g | 0 | |||||||
| 16:0 | g | 0.05 | |||||||
| 17:0 | g | 0 | |||||||
| 18:0 | g | 0.008 | |||||||
| 20:0 | g | 0 | |||||||
| 22:0 | g | 0 | |||||||
| 24:0 | g | 0 | |||||||
| Fatty acids, total monounsaturated | g | 0.008 | |||||||
| 14:1 | g | 0 | |||||||
| 15:1 | g | 0 | |||||||
| 16:1 undifferentiated | g | 0 | |||||||
| 17:1 | g | 0 | |||||||
| 18:1 undifferentiated | g | 0.008 | |||||||
| 20:1 | g | 0 | |||||||
| 22:1 undifferentiated | g | 0 | |||||||
| Fatty acids, total polyunsaturated | g | 0.062 | |||||||
| 18:2 undifferentiated | g | 0.054 | |||||||
| 18:3 undifferentiated | g | 0.008 | |||||||
| 18:4 | g | 0 | |||||||
| 20:2 n-6 c,c | g | 0 | |||||||
| 20:3 undifferentiated | g | 0 | |||||||
| 20:4 undifferentiated | g | 0 | |||||||
| 20:5 n-3 (EPA) | g | 0 | |||||||
| 22:5 n-3 (DPA) | g | 0 | |||||||
| 22:6 n-3 (DHA) | g | 0 | |||||||
| Fatty acids, total trans | g | 0 | |||||||
| Cholesterol | mg | 0 | |||||||
| Phytosterols | mg | 9 | |||||||
| Amino Acids | |||||||||
| Tryptophan | g | 0.012 | |||||||
| Threonine | g | 0.036 | |||||||
| Isoleucine | g | 0.024 | |||||||
| Leucine | g | 0.036 | |||||||
| Lysine | g | 0.039 | |||||||
| Methionine | g | 0.007 | |||||||
| Cystine | g | 0.012 | |||||||
| Phenylalanine | g | 0.092 | |||||||
| Tyrosine | g | 0.012 | |||||||
| Valine | g | 0.036 | |||||||
| Arginine | g | 0.027 | |||||||
| Histidine | g | 0.01 | |||||||
| Alanine | g | 0.036 | |||||||
| Aspartic acid | g | 0.208 | |||||||
| Glutamic acid | g | 0.194 | |||||||
| Glycine | g | 0.03 | |||||||
| Proline | g | 0.024 | |||||||
| Serine | g | 0.054 | |||||||
| Other | |||||||||
| Alcohol, ethyl | g | 0 | |||||||
| Caffeine | mg | 0 | |||||||
| Theobromine | mg | 0 | |||||||
| Anthocyanidins | |||||||||
| Cyanidin | mg | 0 | |||||||
| Flavan-3-ols | |||||||||
| (+)-Catechin | mg | 0 | |||||||
| (-)-Epigallocatechin | mg | 0 | |||||||
| (-)-Epicatechin | mg | 0 | |||||||
| (-)-Epicatechin 3-gallate | mg | 0 | |||||||
| (-)-Epigallocatechin 3-gallate | mg | 0 | |||||||
| (+)-Gallocatechin | mg | 0 | |||||||
| Flavones | |||||||||
| Apigenin | mg | 0 | |||||||
| Luteolin | mg | 4.7 | |||||||
| Flavonols | |||||||||
| Kaempferol | mg | 0.1 | |||||||
| Myricetin | mg | 0 | |||||||
| Quercetin | mg | 2.2 | |||||||
| Isoflavones | |||||||||
| Daidzein | mg | 0 | |||||||
| Genistein | mg | 0 | |||||||
| Total isoflavones | mg | 0 | |||||||
| Proanthocyanidin | |||||||||
| Proanthocyanidin dimers | mg | 0 | |||||||
| Proanthocyanidin trimers | mg | 0 | |||||||
| Proanthocyanidin 4-6mers | mg | 0 | |||||||
| Proanthocyanidin 7-10mers | mg | 0 | |||||||
| Proanthocyanidin polymers (>10mers) | mg | 0 | |||||||
Table 2. Capsicum sweet, yellow and raw nutrition facts
| Nutrient | Unit | Value per 100 g | |||||
| Approximates | |||||||
| Water | g | 92.02 | |||||
| Energy | kcal | 27 | |||||
| Energy | kJ | 112 | |||||
| Protein | g | 1 | |||||
| Total lipid (fat) | g | 0.21 | |||||
| Ash | g | 0.45 | |||||
| Carbohydrate, by difference | g | 6.32 | |||||
| Fiber, total dietary | g | 0.9 | |||||
| Minerals | |||||||
| Calcium, Ca | mg | 11 | |||||
| Iron, Fe | mg | 0.46 | |||||
| Magnesium, Mg | mg | 12 | |||||
| Phosphorus, P | mg | 24 | |||||
| Potassium, K | mg | 212 | |||||
| Sodium, Na | mg | 2 | |||||
| Zinc, Zn | mg | 0.17 | |||||
| Copper, Cu | mg | 0.107 | |||||
| Manganese, Mn | mg | 0.117 | |||||
| Selenium, Se | µg | 0.3 | |||||
| Vitamins | |||||||
| Vitamin C, total ascorbic acid | mg | 183.5 | |||||
| Thiamin | mg | 0.028 | |||||
| Riboflavin | mg | 0.025 | |||||
| Niacin | mg | 0.89 | |||||
| Pantothenic acid | mg | 0.168 | |||||
| Vitamin B-6 | mg | 0.168 | |||||
| Folate, total | µg | 26 | |||||
| Folic acid | µg | 0 | |||||
| Folate, food | µg | 26 | |||||
| Folate, DFE | µg | 26 | |||||
| Vitamin B-12 | µg | 0 | |||||
| Vitamin A, RAE | µg | 10 | |||||
| Retinol | µg | 0 | |||||
| Carotene, beta | µg | 120 | |||||
| Vitamin A, IU | IU | 200 | |||||
| Vitamin D (D2 + D3) | µg | 0 | |||||
| Vitamin D | IU | 0 | |||||
| Lipids | |||||||
| Fatty acids, total saturated | g | 0.031 | |||||
| Fatty acids, total trans | g | 0 | |||||
| Cholesterol | mg | 0 | |||||
| Amino Acids | |||||||
| Tryptophan | g | 0.013 | |||||
| Threonine | g | 0.037 | |||||
| Isoleucine | g | 0.032 | |||||
| Leucine | g | 0.052 | |||||
| Lysine | g | 0.044 | |||||
| Methionine | g | 0.012 | |||||
| Cystine | g | 0.019 | |||||
| Phenylalanine | g | 0.031 | |||||
| Tyrosine | g | 0.021 | |||||
| Valine | g | 0.042 | |||||
| Arginine | g | 0.048 | |||||
| Histidine | g | 0.02 | |||||
| Alanine | g | 0.041 | |||||
| Aspartic acid | g | 0.143 | |||||
| Glutamic acid | g | 0.132 | |||||
| Glycine | g | 0.037 | |||||
| Proline | g | 0.044 | |||||
| Serine | g | 0.04 | |||||
| Anthocyanidins | |||||||
| Cyanidin | mg | 0 | |||||
| Flavones | |||||||
| Apigenin | mg | 0 | |||||
| Luteolin | mg | 1 | |||||
| Flavonols | |||||||
| Kaempferol | mg | 0 | |||||
| Myricetin | mg | 0.2 | |||||
| Quercetin | mg | 1 | |||||
Capsicum health benefits
In addition to the use of capsicum fruits as a food additive, in traditional medicine, capsicum has been used for the treatment of cough, toothache, sore throat, parasitic infections, rheumatism, wound healing 18 and also utilized as an antiseptic, counterirritant, appetite stimulator 19, antioxidant and immunomodulator 20 (Figure 4). Other effects such as antibacterial and anticancer are also related to chilies 19. Red pepper as a drug is given in atonic dyspepsia and flatulence 19 due to increasing the motility in the gastric antrum, duodenum, proximal jejunum and colon 20. It can also increase parietal, pepsin, and bile acid secretions 21. Chilies are known to protect against gastrointestinal ailments 22 including dyspepsia 20, loss of appetite, gastroesophageal reflux disease and gastric ulcer 20 due to the several mechanisms such as reducing the food transition time through the gastrointestinal tract and anti-Helico pylori effects 22. Moreover, the leaves of its plant have antioxidant activity 23.
Hot red peppers consist of spicy compounds called capsaicinoids which include capsaicin, dihydrocapsaicin, nordihydrocapsaicin and other compounds 24 (Figure 4).
Figure 4. Chemical structures of capsaicinoids
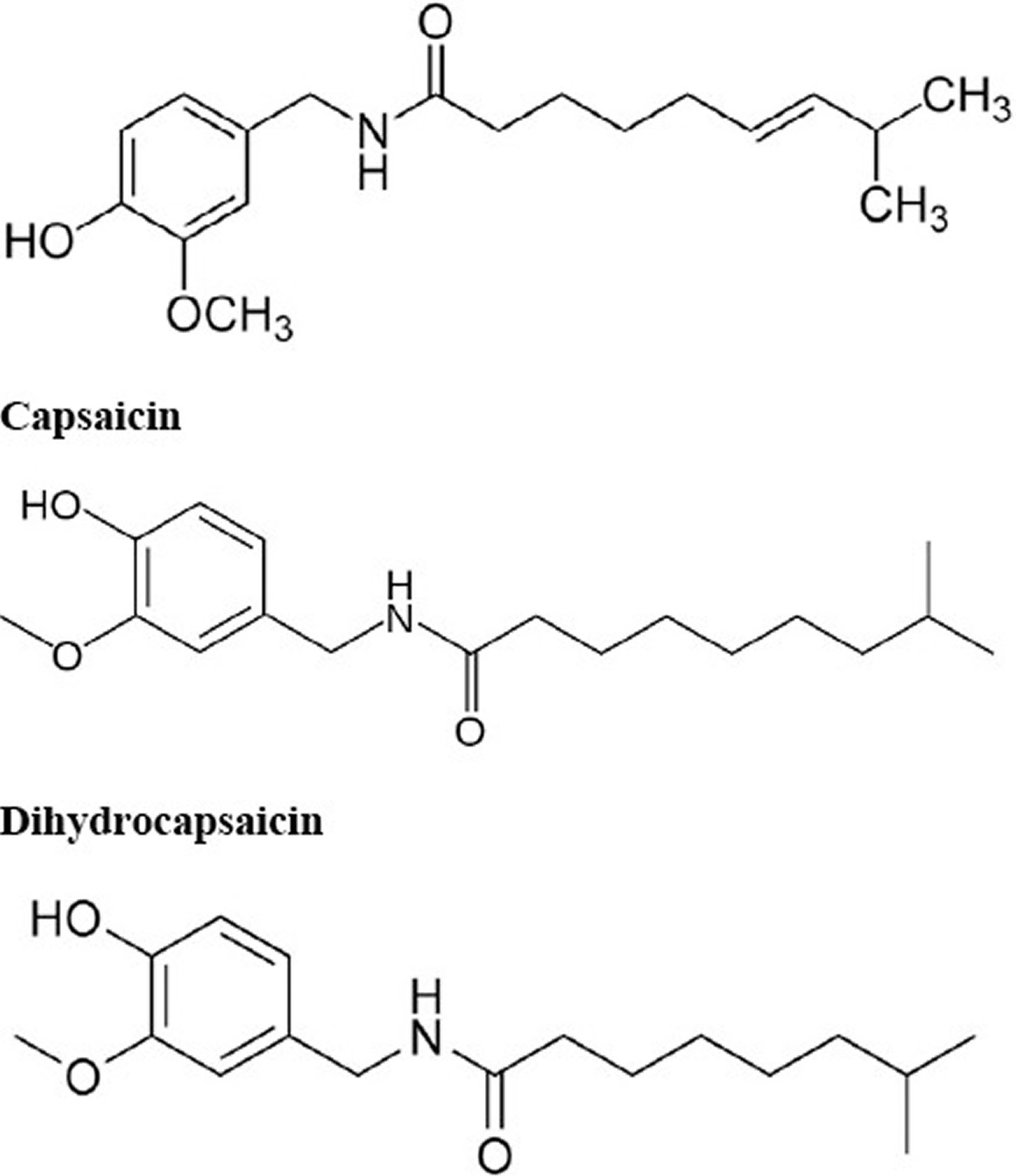
Figure 5. Chemical structures of capsaicin and capsiate
Capsaicin, water-insoluble derivative of homovanillic acid 27 and the main active ingredient in capsicum fruits, is responsible for hot sensation to the tongue 21 and is utilized for the treatment of inflammatory disorders such as psoriasis and rheumatoid arthritis 18, diabetic neuropathy, postherpetic neuralgia, cluster headache, postmastectomy syndrome, reflex sympathetic dystrophy 19, dermatitis or eczema itching 21, postoperative nausea and vomiting, bladder hyperactivity 28, gallstone 29, anorexia, haemorrhoids, liver congestion, foodborne gastrointestinal pathogens including Listeria monocytogenes, Salmonella typhimurium and Bacillus cereus 20, tonsillitis and rhinitis and fibromyalgia 18. It is also used as pesticides 30, analgesic, antiobesity, antihypertensive 18, antiarrhythmic, antiischemic 28, and gastroprotective agent 19. It can stimulate saliva and digestive enzymes of the pancreas, small intestine 20, and also stimulate hair growth in alopecia areata. Anticoagulant activity, prevention of aspiration pneumonia 27, protecting neuromuscular junctions from Clostridium botulinum neurotoxin A and improving cognitive function are also attributed to capsaicin beneficial properties 18.
Topically applied capsaicin is used in migrane, trigeminal neuralgia, herpes zoster 20, chronic musculoskeletal pain (26) and skin disorders 18.
Different studies indicated that red pepper and its active constituent, capsaicin, have therapeutic potential in different components of metabolic syndrome.
Capsicum likely effective for:
- Nerve damage related to diabetes. Some research shows that applying a cream or using a skin patch containing capsaicin, the active chemical found in capsicum, reduces pain in people with nerve damage caused by diabetes. A specific cream containing 0.075% capsaicin (Zostrix-HP, Link Medical Products Pty Ltd.) is approved by the US Food and Drug Administration (FDA) for treating this condition. Creams or gels that contain less capsaicin don’t seem to work.
- Pain. Applying creams and lotions containing capsaicin, the active chemical in capsicum, can temporarily relieve chronic pain from several conditions, including rheumatoid arthritis, osteoarthritis, back pain, jaw pain, psoriasis, and other conditions.
- Nerve damage caused by shingles. Applying a patch containing 8% capsaicin (Qutenza, NeurogesX Inc.), the active chemical in capsicum reduces pain over 24 hours by 27% to 37% for in people with nerve damage caused by shingles. This capsaicin patch is approved by the US Food and Drug Administration (FDA) for this use. It is only available by prescription.
Capsicum possibly effective for:
- Back pain. Some research shows that applying a plaster that contains capsicum to the back can reduce low back pain.
- Cluster headache. Some research shows that applying capsaicin, the active chemical in capsicum, inside the nose reduces the number and severity of cluster headaches. It’s best to apply capsicum to the nostril that is on the same side of the head as the headache.
- Runny nose not caused by allergies or infection (non-allergic rhinitis or perennial rhinitis). Research shows that applying capsaicin, the active chemical in capsicum, inside the nose can reduce runny nose in people without allergies or an infection. The benefits might last for 6-9 months.
- Preventing nausea and vomiting after surgery. Research shows that applying a plaster containing capsicum to specific points on the hand and forearm 30 minutes before anesthesia and leaving it in place for 6-8 hour daily for up to 3 days after surgery reduces nausea and vomiting after surgery.
- Pain after surgery. Research shows that applying a plaster containing capsicum to specific points on the hand and forearm 30 minutes before anesthesia and leaving it in place for 6-8 hour daily for up to 3 days after surgery reduces the need for painkillers within the first 24 hours after surgery.
Insufficient evidence to rate effectiveness for:
- Hay fever (allergic rhinitis). Early research suggests that inserting cotton wads in the nose that have been soaked in the capsicum active chemical capsaicin for 15 minutes and repeated over two days might reduce hay fever symptoms. But there is conflicting evidence that this might not improve symptoms.
- Burning mouth syndrome. Early research shows that using a mouth rinse containing capsaicin, the active chemical in capsicum, daily for 7 days slightly decreases burning discomfort in people with burning mouth syndrome.
- Heartburn. Early research suggests that red pepper powder (containing capsicum) in capsules taken 3 times daily before meals reduces symptoms of heartburn. But in some people, symptoms get worse before they get better.
- Exercise performance. Research shows that taking a supplement containing capsicum and other ingredients before exercise does not improve exercise performance in men.
- Fibromyalgia. Applying a cream containing 0.025% to 0.075% capsaicin, the active chemical in capsicum, 4 times daily to tender points might reduce tenderness in people with fibromyalgia. However, it doesn’t seem to reduce overall pain or improve physical function.
- Nerve damage caused by HIV. Some research suggest that applying a patch containing 8% capsaicin, the active chemical in capsicum, to the skin for 30-90 minutes reduce pain for up to 12 weeks in people with nerve damage caused by HIV. But other research suggests it might not provide any benefits. Applying cream containing 0.075% capsaicin does not seem to work.
- Irritable bowel syndrome (IBS). Early research shows that capsicum fruit taken by mouth does not help symptoms of IBS.
- Joint pain. Early research shows that taking capsules of a specific combination product containing capsaicin, the active ingredient in capsicum, and many other ingredients (Instaflex Joint Support) daily for 8 weeks reduces joint pain by about 21% compared to placebo. The effects of capsicum alone cannot be determined from this study.
- Migraine headache. Some reports suggest that using the active chemical in capsicum in the nose might help migraine headaches.
- Muscular pain. Early research shows that using a specific cream (Dipental Cream) that contains capsaicin, an active chemical in capsicum, in addition to a ketoprofen patch does not further relieve pain in people with muscular pain in the upper back.
- Stomach ulcers. People who eat capsicum fruit (chili) an average of 24 times per month appear to be less likely to have an ulcer than people who eat chili an average of 8 times per month. This applies to chili in the form of chili powder, chili sauce, curry powder, and other chili-containing foods. But there is other evidence that suggests eating chili peppers does not help heal ulcers.
- A skin condition called prurigo nodularis. Applying a cream containing capsaicin, the active chemical in capsicum, 4-6 times daily seems to relieve burning sensations, itching and other symptoms. But it may take 22 weeks to 33 months of treatment to see a benefit, and symptoms may return after stopping use cream.
- Polyps in the nose. Early research shows that putting capsicum in the nose improves symptoms and airflow in people with polyps.
- Swallowing difficulties. Some people, especially elderly people or those who have suffered a stroke, are more likely than other people to develop “aspiration pneumonia.” This is a kind of pneumonia that develops after food or saliva is sucked into the airways because the person couldn’t swallow properly. There is some evidence that dissolving a capsaicin-containing lozenge in the mouth of elderly people with swallowing problems before each meal can improve their ability to swallow.
- Weight loss. Some research shows that taking capsules containing capsicum twice daily 30 minutes before eating for 12 weeks reduces stomach fat but not weight in overweight and obese people. But other research shows that taking a combination supplement (Prograde Metabolism) containing capsicum extract (Capsimax, OmniActive Health Technologies) twice daily for 8 weeks reduces body weight, fat mass, waist circumference, and hip circumference when used along with a diet.
- Blood clots.
- Colic.
- Cramps.
- Fever.
- Heart disease.
- High cholesterol.
- Laryngitis.
- Muscle spasms.
- Nausea.
- Toothache.
- Other conditions.
More evidence is needed to rate the effectiveness of capsicum for these uses.
Capsicum effects on obesity
Abnormal metabolism of energy had led to storage of excess energy in fat cells. This is considered as obesity, another component of the metabolic syndrome, which is the most widespread disease 31.
Several studies reported that red chili pepper exhibited anti-obesity effect by different mechanisms including thermogenesis, satiety, fat oxidation 32, elevation of energy expenditure 33, reduction of energy intake 34, prevention of adipogenesis 35, restriction the activity of lipoprotein lipase 36 and pancreatic lipase 37, stimulation of lipolysis in adipose tissue 38, inhibition of the differentiation of adipocytes 39 and modulating adipokine release from adipose tissues 40. For examples, in animal studies, capsaicin exhibited antiobesity effects via inhibition of the generation white fat cells and restricted the activity of lipoprotein lipase 41.
Different clinical investigations showed that foods containing capsaicin increased fat oxidation and energy expenditure especially at high doses, promoted negative energy balance and restrained orexigenic sensations such as hunger and desire to eat 42 whether they received an oral or non-oral capsaicin 43. This study also showed that capsaicin increased core body and skin temperature, however, the magnitude of its thermogenic and appetitive effects is small 42.
Moreover, when red pepper was added to breakfast in 13 healthy Japanese females (age 25.8 ± 2.8 years, weight 54.2 ±6.4 kg, height 1.57 ± 0.04 m, body fat 25.3 ± 4.7%), protein and fat intakes at lunch time decreased but when it used as appetizer, carbohydrate and energy intakes at lunch time decreased in 10 healthy Caucasian males (age 32.9 ±7.8 years, weight 72.5± 10.1 kg, height 1.75±0.06m) 44.
Male and female Japanese has the same response in decreasing fat intake, this is dissimilar to Caucasians 45.
Study on the effect of dietary red pepper on energy metabolism in 13 Japanese female have shown that adding of the red pepper to high-fat meals, increased brown adipose tissue thermogenesis 46 induced by β adrenergic stimulation 47, and lipid oxidation 46. However, addition to high carbohydrate meals resulted in increasing the oiliness of the meal 46.
The findings of a study on 10 healthy men and 17 healthy women (mean age 26.9±6.3 years, mean BMI 22.2±2.7 kg/m²) for 6 weeks (3 weeks of positive energy balance and 3 weeks of negative energy balance) showed that the ingestion of capsaicin in combination with green tea caused significant reduction of energy intake in positive energy balance, increased satiety and restrained hunger in negative energy balance more than ingestion of capsaicin alone. In this study during negative energy balance body weight was decreased by 0.44 ± 0.2 kg, thus, it may be helpful in weight loss 34.
A single blind, randomized, crossover study which was conducted on 19 healthy women and 11 healthy men (BMI 20-30 kg/m², age 18-60 years) suggested that an acute lunch consist of capsaicin, increased plasma GLP1 and decreased plasma ghrelin concentrations, but, it had no impact on satiety, energy expenditure and peptide YY 48.
A randomized double-blind, placebo-controlled, cross-over study suggested that 4-week supplementation with 1g/day of red pepper spice in 62 obese females with the body mass index ≥27 kg/m² and the age of 40-75 years indicated that this culinary amount of red pepper, did not change inflammation in systematically inflamed obese females 49.
In a clinical trial, administration of capsaicinoids for 12 weeks at a dose of 6 mg/day in subjects with the age of 42 years and BMI 30.4, confirmed the effect of capsaicin on abdominal fat reduction 31.
According to the results of a study on 11 healthy volunteers, CH-19 sweet (a non-pungent cultivar of red pepper) can increase thermogenesis and energy consumption, less than that of observed in hot red pepper 50.
So, it could be suggested that the differences in red pepper’s colors and pungency led to different energy homeostasis 51.
According to clinical studies, the antiobesity mechanism of capsaicin is partially similar to phentermine, an anti-obesity drug, which both increased energy expenditure and decreased food intake. Orlistat, another antiobesity drug, has pancreatic lipase inhibitory activity, which is in common with one of the antiobesity mechanism of capsaicin. Orlistat (75 mg/kg/d) has better ability in controlling of weight gain than capsaicin (30 mg/kg/d) in rats fed a high fat diet for 5 weeks.
Taken together, these observations reinforce the idea that consumption of red chili pepper containing capsaicin, capsaicinoids and capsinoids could play beneficial effects in weight management via increase energy expenditure, satiety, fat oxidation and thermogenesis which are the main mechanisms of antiobesity effect of capsaicin (Table 3).
However, to aid weight management, additional investigation is warranted to explore: 1) the sustainability of energy balance effects; 2) the need to alter dose, form, and/or composition to improve long-term efficacy; 3) the combination of capsaicin and capsiate with other weight management strategies; and 4) the mechanisms by which capsaicin and capsiate can be most successfully incorporated into the diet.
Although capsaicin intake appears to be a safe practice, further studies will be needed to ascertain the safety of regular long-term consumption.
Table 3. Summary of the effects of Capsicum annuum and capsaicin on obesity
| Study design | Constituents | Results | Ref |
|---|---|---|---|
| In vivo, rodents | diet containing 0.014% capsaicin | ↓ visceral fat weight | 52 |
| In vivo, rats | capsaicin (addition to HFD and HCD) | ↓ weight of perineal adipose tissue ↓ weight of the epididymal adipose tissue | 53 |
| In vivo, obese rats | chitosan-capsaicin microsphere (3382 mg/kg/d) for 5 weeks | ability to control body weight > orlistat (75 mg/kg/d) | 54 |
| In vivo, mice (fed HFD) | 0.075% capsaicin (topical application) | ↓ weight gain ↓ visceral fat ↓ lipid accumulation in mesenteric adipose tissue ↑ insulin sensitivity | 55 |
| In vitro, 3T3-L1 cells | capsaicin (2 mg/kg) | prevent adipogenesis up-regulate adiponectin expression | 56 |
| In vitro, 3T3-L1 cells | methanolic extract of C. annuum (50-100-200 µg/ml) | ↓ activity of G3PD | 57 |
| In vitro, 3T3-L1 cells | capsaicin | inhibit the differentiation of adipocytes | 39 |
| In vitro | hot pepper seed extract (50-100-200 µg/ml) | ↓ lipid accumulation in the adipocyte | 58 |
| Human, healthy Japanese females | red pepper (added to breakfast) | ↓ protein and fat intakes at lunch time | 59 |
| Human, healthy Caucasian males | red pepper (used as appetizer) | ↓ carbohydrate and energy intakes at lunch time | 59 |
| Human, Japanese female | red pepper (added to high-fat meals) | ↑ BAT thermogenesis ↑ lipid oxidation | 60 |
| Human, healthy men and women | combination of capsaicin and green tea for 6 weeks | ↓ energy intake in positive energy balance ↑ satiety in negative energy balance | 61 |
| Human, a single blind, randomized, crossover study | lunch consist of capsaicin | ↑ plasma GLP1 ↓ plasma ghrelin ↓ abdominal fat | 62 |
| Human, clinical trial | capsaicinoids (6 mg/day) for 12 weeks | 31 |
Abbreviations: HFD = high fat diet; HCD = high carbohydrate diet; G3PD = glycerol 3 phosphate dehydrogenase; BAT = brown adipose tissue; GLP1 = glucagon-like peptide-1
Capsaicin for non‐allergic rhinitis
Rhinitis means inflammation of the nose. It affects 30% to 40% of the general population. There are many forms of rhinitis: rhinosinusitis (or simply sinusitis), allergic rhinitis and non-allergic rhinitis. Patients are diagnosed with non-allergic rhinitis when anatomic, infectious and allergic causes have been excluded and also do not have sinusitis 63. Non-allergic rhinitis symptoms include congestion of the nose, a blocked or obstructed sensation in the nose that causes difficulty breathing, clear nasal discharge (runny nose), sneezing and less frequently, nasal itching, can range from mild to debilitating. Non-allergic rhinitis affects between 25% and 50% of patients with rhinitis. There are several subtypes of non-allergic rhinitis: occupational (from exposure to chemicals), smoking, gustatory (related to eating food or drinking fluid), hormonal (from changes in hormone levels in the body), pregnancy, senile or elderly (mostly affecting the older population), medication-induced (for example, from overuse of decongestant nasal sprays) and local allergic (local allergy in the nose, while skin or blood allergy tests are negative). The most common subtype of non-allergic rhinitis is ‘idiopathic’ or ‘vasomotor’ rhinitis, which results from imbalance of the neural (nerve) system that manages the function of the nose. The mechanisms of many of these subtypes remain unknown. Non-allergic rhinitis affects about 25% to 50% of patients with rhinitis and is therefore very common.
Several medications are widely used in the treatment of non-allergic rhinitis, including oral and topical nasal antihistamines, intranasal and (rarely) systemic corticosteroids, and anticholinergics. Capsaicin, the active component of chili peppers, delivered intranasally, is considered a treatment option for non-allergic rhinitis.
Capsaicin affects the unmyelinated peptidergic sensory C fibres of the nasal mucosa, which are highly sensitive to it 64. It is hypothesised that repeated high doses of capsaicin lead to degeneration of these nerve fibres. Unmyelinated sensory C fibres play a role in neurogenic reflex mechanisms in the nasal mucosa, both local and central. Stimulation of these sensory fibres by non-specific stimuli can lead to a local reflex in the nasal mucosa with a release of neuropeptides (C-peptide, CGRP, VIP). At the same time, capsaicin does not affect the number of inflammatory cells in the nasal mucosa long-term 65. The same study also did not show a difference in neuronal tissue density as expressed by synaptophysin or neurofilament staining.
Although these mechanisms are not considered definitive, several studies have demonstrated a significant improvement of nasal symptoms after topical administration of capsaicin 66.
Intranasal capsaicin is currently considered one of the treatment options for non-allergic rhinitis. Capsaicin is also one of the active ingredients (along with eucalyptus oil) in Sinus Buster, an over-the-counter nasal spray available in the United States 67. The dose and frequency of intranasal capsaicin application have varied significantly in studies. Doses of capsaicin have ranged from 0.1 to 100 mg per application, given through one or several actuations of the spray depending on the capsaicin preparation in a particular study 68. The regimen of capsaicin treatment has also ranged widely from five times during the same day, to three times per day for three days, to once daily for five days, or once every two to three days for seven treatments. The local pharmacology of capsaicin in the nose is poorly understood. It is metabolised in the liver.
The side effects of using capsaicin in the nose include irritation, burning, sneezing and coughing, however there are no known long-term side effects of capsaicin use. Capsaicin is given in the form of brief treatments, usually during the same day. It works by down-regulating transient receptor potential vanilloid receptor expression on C-sensory fibres. Transient receptor potential vanilloid represents special ion channels involved in the sensations of pain, cold, hotness, tastes, pressure and vision. C fibres help to conduct some of these sensations. There is ongoing research into the effects of capsaicin on these mechanisms and its clinical uses.
A 2015 Cochrane Review found that Capsaicin may be an option in the treatment of idiopathic non-allergic rhinitis 69. Capsaicin is given in the form of brief treatments, usually during the same day. Capsaicin appears to have beneficial effects on overall nasal symptoms up to 36 weeks after treatment, based on a few, small studies (low-quality evidence). Well-conducted randomised controlled trials are required to further advance our understanding of the effectiveness of capsaicin in non-allergic rhinitis, especially in patients with non-allergic rhinitis of different types and severity, and using different methods of capsaicin application.
Interestingly, intranasal capsaicin has also been studied in allergic rhinitis. However, a 2006 Cochrane review on capsaicin in allergic rhinitis in adults did not find an evidence of intranasal capsaicin effect 70.
Capsaicin applied to the skin for chronic neuropathic pain in adults
Neuropathic pain is “pain caused by a lesion or disease of the somatosensory system” 71. Neuropathic pain is a consequence of a pathological maladaptive response of the nervous system to ‘damage’ from a wide variety of potential causes. It is characterized by pain in the absence of a noxious stimulus and may be spontaneous (continuous or paroxysmal) in its temporal characteristics or be evoked by sensory stimuli (dynamic mechanical allodynia where pain is evoked by light touch of the skin). Neuropathic pain is associated with a variety of sensory loss (numbness) and sensory gain (allodynia) clinical phenomena, the exact pattern of which vary between person and disease, perhaps reflecting different pain mechanisms operating in an individual person and therefore potentially predictive of response to treatment 72. Preclinical research hypothesises a bewildering array of possible pain mechanisms that may operate in people with neuropathic pain, which largely reflect pathophysiological responses in both the central and peripheral nervous systems, including neuronal interactions with immune cells 73. Overall, even the most effective of available drugs provide only modest benefit in treating neuropathic pain 74, and a robust classification of neuropathic pain is not yet available 75.
Neuropathic pain is usually divided according to the cause of nerve injury. There may be many causes, but common causes of neuropathic pain include diabetes (painful diabetic neuropathy), shingles (postherpetic neuralgia), amputation (phantom limb pain), neuropathic pain after surgery or trauma, stroke or spinal cord injury, trigeminal neuralgia, and HIV infection. Sometimes the cause is not known.
Many people with neuropathic pain conditions are significantly disabled with moderate or severe pain for many years. Chronic pain conditions comprised five of the 11 top-ranking conditions for years lived with disability in 2010 76, and are responsible for considerable loss of quality of life, employment, and increased healthcare costs 77.
In systematic reviews, the overall prevalence of neuropathic pain in the general population is reported to be between 7% and 10% 78, and about 7% in one systematic review of studies published since 2000 77. In individual countries, prevalence rates have been reported as 3.3% in Austria 79, 6.9% in France 80, and up to 8% in the UK 81. Some forms of neuropathic pain are increasing, particularly painful diabetic neuropathy and postsurgical chronic pain (which is often neuropathic in origin) 82. The prevalence of postherpetic neuralgia is likely to fall if vaccination against the herpes virus becomes widespread.
Estimates of incidence vary between individual studies for neuropathic pain associated with particular conditions, often because of small numbers of cases. In primary care in the UK between 2002 and 2005, the incidences (per 100,000 person-years’ observation) were 28 for postherpetic neuralgia, 27 for trigeminal neuralgia, 0.8 for phantom limb pain, and 21 for painful diabetic neuropathy 82. Other research groups have estimated an incidence of 4 in 100,000 per year for trigeminal neuralgia 83, and of 12.6 per 100,000 person-years for trigeminal neuralgia and 3.9 per 100,000 person-years for postherpetic neuralgia in one study of facial pain in the Netherlands 84.
Neuropathic pain is difficult to treat effectively, with only a minority of people experiencing a clinically relevant benefit from any one intervention. A multidisciplinary approach is now advocated, with pharmacological interventions being combined with physical or cognitive interventions, or both. Conventional analgesics are usually thought to be ineffective, but without evidence to support or refute that view. Some people with neuropathic pain may derive some benefit from a topical lidocaine patch or low-concentration topical capsaicin, though evidence about benefits is uncertain 85. The earlier review of high-concentration topical capsaicin indicated benefit in some people with postherpetic neuralgia 86. Treatment for neuropathic pain is more usually with so-called unconventional analgesics (pain modulators), for example, with antidepressants such as duloxetine and amitriptyline 87, or antiepileptic drugs such as gabapentin or pregabalin 88.
The proportion of people who achieve worthwhile pain relief (typically at least 50% pain intensity reduction) 89 with any one intervention is small, generally only 10% to 25% more than with placebo, with numbers needed to treat for an additional beneficial outcome usually between 4 and 10 90. Neuropathic pain is not particularly different from other chronic pain conditions in that only a small proportion of trial participants have a good response to treatment 91.
The current National Institute for Health and Care Excellence 92 guidance for the pharmacological management of neuropathic pain suggests offering a choice of amitriptyline, duloxetine, gabapentin, or pregabalin as initial treatment for neuropathic pain (with the exception of trigeminal neuralgia), with switching if first, second, or third drugs tried are not effective or not tolerated. This concurs with other recent guidance 74.
Topical agents are most likely to be used for localized, peripheral neuropathies. Topical medications are applied externally and are taken up through the skin. They exert their effects close to the site of application, and there is no substantial systemic uptake or distribution. This compares with transdermal application, where the medication is applied externally and is taken up through the skin, but relies on systemic distribution for its effect.
Low-concentration capsaicin creams have not convincingly been shown to be effective for neuropathic pain 93. The initial burning sensation felt on application of capsaicin limits the amount of active substance that can be applied at one time, which necessitates frequent (four times per day) application, and reduces compliance with treatment. The high-concentration (8%) patch was developed to increase the amount of capsaicin delivered to the skin, and improve tolerability. Rapid delivery is thought to improve tolerability because cutaneous nociceptors are ‘defunctionalised’ quickly, and the single application avoids both noncompliance and contamination of the home environment with particles of dried capsaicin cream 11. At the present time, the 8% patch is the only high-strength formulation of capsaicin commercially available, although different strengths and formulations have been investigated in clinical trials. A capsaicin concentration of 5% or greater is considered high.
The treatment is usually applied as a single application dermal patch over the area where painful symptoms are felt. Each patch (280 cm²) contains capsaicin 640 μg/cm², and can be cut to treat smaller areas and irregular shapes, or up to four patches can be used simultaneously to treat large areas, such as the back. The skin to which patches are applied should not be broken or irritated. The skin is usually treated with a topical local anaesthetic (e.g. topical lidocaine 4% for 60 minutes) before application because the capsaicin may cause an intense burning sensation, and the anaesthetic is then washed off thoroughly, and the skin dried, before the patch is applied. Studies suggest that skin cooling is as effective as topical anaesthetic for relieving initial burning 94, or that any form of pretreatment in unnecessary 95. The patch is left in place for 30 minutes when applied to the feet, or 60 minutes for other areas, before removal and careful cleansing of the skin with a specially formulated cleanser, to remove any residual capsaicin. Application must be carried out in a healthcare centre by trained personnel, and patients are usually monitored for up to two hours after treatment. Stringent conditions are required, and as well as using trained healthcare professionals, the treatment setting needs to be well ventilated and spacious due to the vapour of the capsaicin, and cough due to inhalation of capsaicin particles or dust is a hazard for both the healthcare professionals and the patients. Treatment can be repeated after 12 weeks if necessary.
High-concentration capsaicin is available by prescription only; it was first licensed in Europe and the US in 2009. It was originally licensed in the European Union to treat neuropathic pain in patients without diabetes, but in 2015 the restriction on patients with diabetes was lifted. In the US, it is licensed only to treat postherpetic neuralgia. The US Food and Drug Administration refused a license for neuropathic pain in HIV in 2012.
Topical creams with capsaicin are used to treat peripheral neuropathic pain. Following application to the skin, capsaicin causes enhanced sensitivity, followed by a period with reduced sensitivity and, after repeated applications, persistent desensitisation. High-concentration (8%) capsaicin patches were developed to increase the amount of capsaicin delivered; rapid delivery was thought to improve tolerability because cutaneous nociceptors are ‘defunctionalised’ quickly. The single application avoids noncompliance. Only the 8% patch formulation of capsaicin is available, with a capsaicin concentration about 100 times greater than conventional creams. High-concentration topical capsaicin is given as a single patch application to the affected part. It must be applied under highly controlled conditions, often following local anaesthetic, due to the initial intense burning sensation it causes. The benefits are expected to last for about 12 weeks, when another application might be made.
A 2017 Cochcrane Review found moderate quality evidence that high-concentration (8%) capsaicin patches can give moderate pain relief, or better, to a minority of people with postherpetic neuralgia, and very low quality evidence that it benefits those with HIV-neuropathy and peripheral diabetic neuropathy 96.
Capsicum dosage
The following doses have been studied in scientific research:
Applied to the skin:
- For nerve damage related to diabetes: A specific cream (Zostrix-HP, Link Medical Products Pty Ltd.) containing 0.075% capsaicin, the active chemical in capsicum, has been used 4 times daily for 8 weeks. Also, a specific patch (Qutenza, NeurogesX Inc.) containing 8% capsaicin has been applied once for 60-90 minutes.
- For nerve damage caused by shingles: A specific patch (Qutenza, NeurogesX Inc.) containing 8% capsaicin, the active chemical in capsicum, has been applied once for 60-90 minutes.
- For low back pain: Capsicum-containing plasters providing 11 mg of capsaicin per plaster or 22 mcg of capsaicin per square centimeter of plaster have been used. The plaster is applied once daily in the morning and left in place for 4-8 hours.
- For preventing nausea and vomiting after surgery: Capsicum-containing plasters have been used on acupoints on the hand and forearm for 30 minutes before anesthesia and left in place for 6-8 hours daily for up to 3 days.
- Preventing pain after surgery: Capsicum-containing plasters have been used on acupoints on the hand and forearm for 30 minutes before anesthesia and left in place for 6-8 hours daily for up to 3 days.
Be sure to wash your hands after applying capsaicin cream. A diluted vinegar solution works well. You won’t be able to get the capsaicin off with just water. Don’t use capsicum preparations near the eyes or on sensitive skin. It could cause burning.
Inside the nose:
- For cluster headache: 0.1 mL of a 10 mM capsaicin suspension, providing 300 mcg/day of capsaicin, applied to the nostril on the painful side of the head. Apply the suspension once daily until the burning sensation disappears. A capsaicin 0.025% cream (Zostrix, Rodlen Laboratories) applied daily for 7 days has been used to treat acute cluster headache attacks.
- For runny nose not caused by allergies or infection (perennial rhinitis): Solutions containing capsaicin, the active chemical in capsicum, have been applied inside the nose 3 times per day for 3 days, every other day for 2 weeks, or once weekly for 5 weeks.
Putting capsaicin in the nose can be very painful, so a local painkilling medicine such as lidocaine is often put into the nose first.
Capsicum side effects
Capsicum is likely safe when consumed in amounts typically found in food. Side effects can include stomach irritation and upset, sweating, flushing, and runny nose. Adverse events from capsaicin are mainly at the application site (burning, stinging, erythema), and systemic events are rare.
Medicinal lotions and creams that contain capsicum extract are also likely safe for most adults when applied to the skin. The active chemical in capsicum, capsaicin, is approved by the FDA as an over-the-counter medication. Side effects can include skin irritation, burning, and itching. Capsicum can also be extremely irritating to the eyes, nose, and throat. Don’t use capsicum on sensitive skin or around the eyes.
Capsicum is possibly safe when taken by mouth as medicine, short-term, when applied to the skin appropriately, and when used in the nose. No serious side effects have been reported, but application in the nose can be very painful. Nasal application can cause burning pain, sneezing, watery eyes, and runny nose. These side effects tend to decrease and go away after 5 or more days of repeated use.
Capsicum is possibly UNSAFE to take by mouth in large doses or for long periods of time. In rare cases, this can lead to more serious side effects like liver or kidney damage, as well as severe spikes in blood pressure.
Special precautions and warnings
Pregnancy and breast-feeding: Capsicum is likely safe when applied to the skin during pregnancy. But not enough is known about its safety when taken by mouth. Stay on the safe side and don’t use capsicum if you are pregnant.
If you are breast-feeding, using capsicum on your skin is likely safe. But it is possibly UNSAFE for your baby if you take capsicum by mouth. Skin problems (dermatitis) have been reported in breast-fed infants when mothers eat foods heavily spiced with capsicum peppers.
Children: Applying capsicum to the skin of children under two years of age is possibly UNSAFE. Not enough is known about the safety of giving capsicum to children by mouth. Don’t do it.
Bleeding disorders: While conflicting results exist, capsicum might increase the risk of bleeding in people with bleeding disorders.
Damaged or broken skin: Don’t use capsicum on damaged or broken skin.
Diabetes: In theory, capsicum might affect blood sugar levels in people with diabetes. Until more is known, monitor your blood sugar closely if you take capsicum. The dose of your diabetes medication might need to be changed.
High blood pressure: Taking capsicum or eating a large amount of chili peppers might cause a spike in blood pressure. In theory, this might worsen the condition for people who already have high blood pressure.
Surgery: Capsicum might increase bleeding during and after surgery. Stop using capsicum at least 2 weeks before a scheduled surgery.
Interactions with medications
Moderate
Be cautious with this combination.
Aspirin
Capsicum might decrease how much aspirin the body can absorb. Taking capsicum along with aspirin might reduce the effectiveness of aspirin.
Cefazolin
Capsicum might increase how much cefazolin the body can absorb. Taking capsicum along with cefazolin might increase the effects and side effects of cefazolin.
Ciprofloxacin
Capsicum might increase how much ciprofloxacin the body can absorb. Taking capsicum along with ciprofloxacin might increase the effects and side effects of ciprofloxacin.
Cocaine
Cocaine has many dangerous side effects. Using capsicum along with cocaine might increase the side effects of cocaine, including heart attack and death.
Medications for diabetes (Antidiabetes drugs)
Diabetes medications are used to lower blood sugar. Capsicum might also decrease blood sugar. Taking capsicum along with diabetes medications might cause your blood sugar to go too low. Monitor your blood sugar closely. The dose of your diabetes medication might need to be changed.
Some medications used for diabetes include glimepiride (Amaryl), glyburide (DiaBeta, Glynase PresTab, Micronase), insulin, pioglitazone (Actos), rosiglitazone (Avandia), and others.
Medications for high blood pressure (Antihypertensive drugs)
Some research shows that capsicum might increase blood pressure. In theory, taking capsicum along with medications used for lowering high blood pressure might reduce the effectiveness of these drugs.
Some medications for high blood pressure include captopril (Capoten), enalapril (Vasotec), losartan (Cozaar), valsartan (Diovan), diltiazem (Cardizem), Amlodipine (Norvasc), hydrochlorothiazide (HydroDiuril), furosemide (Lasix), and many others.
Medications that slow blood clotting (Anticoagulant / Antiplatelet drugs)
Capsicum might slow blood clotting. Taking capsicum along with medications that also slow clotting might increase the chances of bruising and bleeding.
Some medications that slow blood clotting include aspirin, clopidogrel (Plavix), diclofenac (Voltaren, Cataflam, others), ibuprofen (Advil, Motrin, others), naproxen (Anaprox, Naprosyn, others), dalteparin (Fragmin), enoxaparin (Lovenox), heparin, warfarin (Coumadin), and others.
Theophylline
Capsicum can increase how much theophylline the body can absorb. Taking capsicum along with theophylline might increase the effects and side effects of theophylline.
Warfarin (Coumadin)
Warfarin (Coumadin) is used to slow blood clotting. Capsicum might increase the effectiveness of warfarin (Coumadin). Taking capsicum along with warfarin (Coumadin) might increase the chances of bruising and bleeding. Be sure to have your blood checked regularly. The dose of your warfarin (Coumadin) might need to be changed.
Minor
Be watchful with this combination.
Medications for high blood pressure (ACE inhibitors)
Some medications for high blood pressure might cause a cough. There is one report of someone whose cough worsened when using a cream with capsicum along with these medications for high blood pressure. But is it not clear if this interaction is a big concern.
Some medications for high blood pressure include captopril (Capoten), enalapril (Vasotec), lisinopril (Prinivil, Zestril), ramipril (Altace), and others.
Interactions with herbs and supplements
Coca
Using capsicum (including exposure to the capsicum in pepper spray) and coca might increase the effects and risk of adverse effects of the cocaine in coca.
Herbs and supplements that might lower blood sugar
Capsicum might affect blood sugar. Using it along with other herbs and supplements that also affect blood sugar might cause blood sugar to drop too low in some people. Some of these products include bitter melon, ginger, goat’s rue, fenugreek, kudzu, willow bark, and others.
Herbs and supplements that might slow blood clotting
Capsicum might slow blood clotting. Taking capsicum with herbs and supplements that also slow clotting might increase the risk of bruising and bleeding in some people. Some herbs that slow blood clotting are angelica, clove, danshen, garlic, ginger, ginkgo, Panax ginseng, and others.
Iron
Using capsicum might reduce the ability for the body to absorb iron.
- Carrizo García C, Sterpetti M, Volpi P, Ummarino M, Saccardo F. 2013. Wild capsicums: identification and in situ analysis of Brazilian species In: Lanteri S, Rotino GL, editors. , eds. Breakthroughs in the genetics and breeding of Capsicum and eggplant. Turin: Eucarpia, 205–213[↩]
- Carrizo García C, Barfuss MHJ, Sehr EM, et al. Phylogenetic relationships, diversification and expansion of chili peppers (Capsicum, Solanaceae). Annals of Botany. 2016;118(1):35-51. doi:10.1093/aob/mcw079. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4934398/[↩]
- Pickersgill B. 1997. Genetic resources and breeding of Capsicum spp. Euphytica 96: 129–133.[↩]
- Capsicum. https://en.wikipedia.org/wiki/Capsicum[↩]
- Moscone EA, Scadalferro MA, Gabriele M , et al. 2007. The evolution of chili peppers (Capsicum – Solanaceae): a cytogenetic perspective. Acta Horticulturae 745: 137–169[↩]
- Genetic control of pungency in C. chinense via the Pun1 locus. Stewart C Jr, Mazourek M, Stellari GM, O’Connell M, Jahn M. J Exp Bot. 2007; 58(5):979-91.[↩][↩]
- Bosland PW, Coon D, Cooke PH. 2015. Novel formation of ectopic (nonplacental) capsaicinoid secreting vesicles on fruit walls explains the morphological mechanism for super-hot chile peppers. Journal of the American Society of Horticultural Sciences 140: 253–256.[↩]
- Van Zonneveld M, Ramirez M, Williams DE, et al. Screening Genetic Resources of Capsicum Peppers in Their Primary Center of Diversity in Bolivia and Peru. Vinatzer BA, ed. PLoS ONE. 2015;10(9):e0134663. doi:10.1371/journal.pone.0134663. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4581705/[↩]
- Iwai K, Yazawa A, Watanabe T. Roles as metabolic regulators of the non-nutrients, capsaicin and capsiate, supplemented to diets. Proc Jpn Acad. 2003;79:207–212[↩]
- Capsaicin in hot chili pepper: carcinogen, co-carcinogen or anticarcinogen? Food Chem Toxicol. 1996 Mar;34(3):313-6. https://www.ncbi.nlm.nih.gov/pubmed/8621114[↩][↩][↩][↩][↩][↩]
- Anand P, Bley K. Topical capsaicin for pain management: therapeutic potential and mechanisms of action of the new high-concentration capsaicin 8% patch. British Journal of Anaesthetics 2011;107(4):490-502.[↩][↩]
- Eliezer Zamski, Orna Shoham, Dan Palevitch, and Arieh Levy, “Ultrastructure of Capsaicinoid-Secreting Cells in Pungent and Nonpungent Red Pepper (Capsicum annuum L.) Cultivars,” Botanical Gazette 148, no. 1 (Mar., 1987): 1-6. https://www.journals.uchicago.edu/doi/10.1086/337620[↩]
- Charles Stewart, Michael Mazourek, Giulia M. Stellari, Mary O’Connell, Molly Jahn; Genetic control of pungency in C. chinense via the Pun1 locus, Journal of Experimental Botany, Volume 58, Issue 5, 1 March 2007, Pages 979–991, https://doi.org/10.1093/jxb/erl243 [↩]
- Pungency of Chile (Capsicum annuum L.) Fruit is Affected by Node Position. HORTSCIENCE 35(6):1174. 2000. https://cpi.nmsu.edu/wp-content/uploads/sites/60/2016/06/pungency_of_chile1.pdf[↩]
- https://www.gardenguides.com/119834-capsaicin-insecticide.html[↩]
- Carrizo García C, Barfuss MHJ, Sehr EM, et al. Phylogenetic relationships, diversification and expansion of chili peppers (Capsicum, Solanaceae). Annals of Botany. 2016;118(1):35-51. doi:10.1093/aob/mcw079 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4934398/[↩][↩]
- United States Department of Agriculture Agricultural Research Service. National Nutrient Database for Standard Reference Legacy Release. https://ndb.nal.usda.gov/ndb/search/list [↩][↩]
- Singletary K. Red pepper:overview of potential health benefits. Nut Today. 2011;46:33–47.[↩][↩][↩][↩][↩][↩]
- Pawar SS, Bharude NV, Sonone SS, Deshmukh RS, Raut AK, Umarkar AR. Chilles as food, spice and medicine:a perspective. Int J Pharm Biol Sci. 2011;1:311–318.[↩][↩][↩][↩][↩]
- Maji AK, Banerji P. Phytochemistry and gastrointestinal benefits of the medicinal spice Capsicum annuum L.(Chilli):a review. J Complement Integr Med. 2016;13:97–122.[↩][↩][↩][↩][↩][↩][↩]
- Barceloux DG. Pepper and capsaicin (Capsicum and Piper species) Dis Mon. 2009;55:380–390.[↩][↩][↩]
- Low Dog T. A reason to season:the therapeutic benefits of spices and culinary herbs. Explore (NY) 2006;2:446–449[↩][↩]
- Kim W-R, Kim EO, Kang K, Oidovsambuu S, Jung SH, Kim BS, et al. Antioxidant activity of phenolics in leaves of three red pepper (Capsicum annuum) cultivars. J Agric Food Chem. 2014;62:850–859.[↩]
- Ludy M-J, Moore GE, Mattes RD. The effects of capsaicin and capsiate on energy balance:critical review and meta-analyses of studies in humans. Chem Senses. 2012;37:103–21 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3257466/[↩]
- Sanati S, Razavi BM, Hosseinzadeh H. A review of the effects of Capsicum annuum L. and its constituent, capsaicin, in metabolic syndrome. Iranian Journal of Basic Medical Sciences. 2018;21(5):439-448. doi:10.22038/IJBMS.2018.25200.6238. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6000222/[↩]
- Ludy M-J, Moore GE, Mattes RD. The Effects of Capsaicin and Capsiate on Energy Balance: Critical Review and Meta-analyses of Studies in Humans. Chemical Senses. 2012;37(2):103-121. doi:10.1093/chemse/bjr100. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3257466/[↩]
- Papoiu AD, Yosipovitch G. Topical capsaicin. The fire of a ‘hot’medicine is reignited. Expert Opin Pharmacother. 2010;11:1359–1371[↩][↩]
- Hayman M, Kam PC. Capsaicin:a review of its pharmacology and clinical applications. Curr Anaesth Crit Care. 2008;19:338–343.[↩][↩]
- Srinivasan K. Spices as influencers of body metabolism:an overview of three decades of research. Food Res Int. 2005;38:77–86.[↩]
- Wesolowska A, Jadczak D, Grzeszczuk M. Chemical composition of the pepper fruit extracts of hot cultivars Capsicum annuum L. Acta Sci Pol Hortorum Cultus. 2011;10:171–184.[↩]
- Gamboa-Gomez CI, Rocha-Guzman NE, Gallegos-Infante JA, Moreno-Jimenez MR, Vazquez-Cabral BD, Gonzalez-Laredo RF. Plants with potential use on obesity and its complications. Excli J. 2015;14:809–831.[↩][↩][↩]
- Woo H-M, Kang J-H, Kawada T, Yoo H, Sung M-K, Yu R. Active spice-derived components can inhibit inflammatory responses of adipose tissue in obesity by suppressing inflammatory actions of macrophages and release of monocyte chemoattractant protein-1 from adipocytes. Life Sci. 2007;80:926–931[↩]
- Ludy M-J, Moore GE, Mattes RD. The effects of capsaicin and capsiate on energy balance:critical review and meta-analyses of studies in humans. Chem Senses. 2012;37:103–21[↩]
- Reinbach HC, Smeets A, Martinussen T, Møller P, Westerterp-Plantenga M. Effects of capsaicin, green tea and CH-19 sweet pepper on appetite and energy intake in humans in negative and positive energy balance. Clin Nut. 2009;28:260–265[↩][↩]
- Zhang H, Matsuda H, Nakamura S, Yoshikawa M. Effects of amide constituents from pepper on adipogenesis in 3T3-L1 cells. Bioorg Med Chem Lett. 2008;18:3272–3277[↩]
- Baek J, Lee J, Kim K, Kim T, Kim D, Kim C, et al. Inhibitory effects of Capsicum annuum L. water extracts on lipoprotein lipase activity in 3T3-L1 cells. Nutr Res Pract. 2013;7:96–102.[↩]
- Marrelli M, Menichini F, Conforti F. Hypolipidemic and Antioxidant Properties of Hot Pepper Flower (Capsicum annuum L.) Plant Foods Hum Nutr. 2016;71:301–306.[↩]
- Do MS, Hong SE, Ha JH, Choi SM, Ahn IS, yoon JY, et al. Increased lipolytic activity by high-pungency red pepper extract (var. chungyang) in rat adipocytes in vitro. J Food Sci Nutr. 2004;9:34–38.[↩]
- Hwang J-T, Park I-J, Shin J-I, Lee YK, Lee SK, Baik HW, et al. Genistein, EGCG, and capsaicin inhibit adipocyte differentiation process via activating AMP-activated protein kinase. Biochem Biophys Res Commun. 2005;338:694–699.[↩][↩]
- Kang J-H, Kim C-S, Han I-S, Kawada T, Yu R. Capsaicin, a spicy component of hot peppers, modulates adipokine gene expression and protein release from obese-mouse adipose tissues and isolated adipocytes, and suppresses the inflammatory responses of adipose tissue macrophages. Febs Lett. 2007;581:4389–4396.[↩]
- Baek J, Lee J, Kim K, Kim T, Kim D, Kim C, et al. Inhibitory effects of Capsicum annuum L. water extracts on lipoprotein lipase activity in 3T3-L1 cells. Nutr Res Pract. 2013;7:96–102[↩]
- Ludy M-J, Moore GE, Mattes RD. The effects of capsaicin and capsiate on energy balance:critical review and meta-analyses of studies in humans. Chem Senses. 2012;37:103–21. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3257466/[↩][↩]
- Whiting S, Derbyshire E, Tiwari BK. Capsaicinoids and capsinoids. A potential role for weight management? A systematic review of the evidence. Appetite. 2012;59:341–348[↩]
- Yoshioka M, St-Pierre S, Drapeau V, Dionne I, Doucet E, Suzuki M, et al. Effects of red pepper on appetite and energy intake. Br J Nutr. 1999;82:115–123[↩]
- Yoshioka M, Imanaga M, Ueyama H, Yamane M, Kubo Y, Boivin A, et al. Maximum tolerable dose of red pepper decreases fat intake independently of spicy sensation in the mouth. Br J Nut. 2004;91:991–995[↩]
- Yoshioka M, St-Pierre S, Suzuki M, Tremblay A. Effects of red pepper added to high-fat and high-carbohydrate meals on energy metabolism and substrate utilization in Japanese women. Br J Nutr. 1998;80:503–510.[↩][↩][↩]
- Westerterp-Plantenga M, Diepvens K, Joosen AM, Berube-Parent S, Tremblay A. Metabolic effects of spices, teas, and caffeine. Physiol Behav. 2006;89:85–91.[↩]
- Smeets AJ, Westerterp-Plantenga MS. The acute effects of a lunch containing capsaicin on energy and substrate utilisation, hormones, and satiety. Eur J Nutr. 2009;48:229–234[↩]
- Nieman DC, Cialdella-Kam L, Knab AM, Shanely RA. Influence of red pepper spice and turmeric on inflammation and oxidative stress biomarkers in overweight females:a metabolomics approach. Plant Foods Hum Nutr. 2012;67:415–421.[↩]
- Ohnuki K, Niwa S, Maeda S, Inoue N, Yazawa S, Fushiki T. CH-19 sweet, a non-pungent cultivar of red pepper, increased body temperature and oxygen consumption in humans. Biosci Biotechnol Biochem. 2016;5:2033–2036.[↩]
- Yang HJ, Kwon DY, Kim MJ, Kim DS, Kang S, Shin BK, et al. Red peppers with different pungencies and bioactive compounds differentially modulate energy and glucose metabolism in ovariectomized rats fed high fat diets. J Funct Foods. 2014;7:246–256.[↩]
- Leung FW. Capsaicin-sensitive intestinal mucosal afferent mechanism and body fat distribution. Life Sci. 2008;83:1–5. https://www.ncbi.nlm.nih.gov/pubmed/18541272[↩]
- Yoshioka M, St-Pierre S, Drapeau V, Dionne I, Doucet E, Suzuki M, et al. Effects of red pepper on appetite and energy intake. Br J Nutr. 1999;82:115–123. https://www.cambridge.org/core/services/aop-cambridge-core/content/view/9E2992B2F0EBED691DDBDD758187F1B5/S0007114599001269a.pdf/effects_of_red_pepper_on_appetite_and_energy_intake.pdf[↩]
- Tan S, Gao B, Tao Y, Guo J, Su Z-q. Antiobese Effects of Capsaicin–Chitosan Microsphere (CCMS) in Obese Rats Induced by High Fat Diet. J Agr Food Chem. 2014;62:1866–74 https://www.ncbi.nlm.nih.gov/pubmed/24479662[↩]
- Lee GR, Shin MK, Yoon DJ, Kim AR, Yu R, Park NH, et al. Topical application of capsaicin reduces visceral adipose fat by affecting adipokine levels in high-fat diet-induced obese mice. Obesity. 2013;21:115–122. https://www.ncbi.nlm.nih.gov/pubmed/23505175[↩]
- Zhang H, Matsuda H, Nakamura S, Yoshikawa M. Effects of amide constituents from pepper on adipogenesis in 3T3-L1 cells. Bioorg Med Chem Lett. 2008;18:3272–3277 https://www.ncbi.nlm.nih.gov/pubmed/18477507[↩]
- Gamboa-Gomez CI, Rocha-Guzman NE, Gallegos-Infante JA, Moreno-Jimenez MR, Vazquez-Cabral BD, Gonzalez-Laredo RF. Plants with potential use on obesity and its complications. Excli J. 2015;14:809–831 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4746997/[↩]
- Jeon G, Choi Y, Lee S-M, Kim Y, Jeong H-S, Lee J. Antiobesity activity of methanol extract from hot pepper (Capsicum annuum L.) seeds in 3T3-L1 adipocyte. Food Sci Biotechnol. 2010;19:1123–1127.[↩]
- Yoshioka M, St-Pierre S, Drapeau V, Dionne I, Doucet E, Suzuki M, et al. Effects of red pepper on appetite and energy intake. Br J Nutr. 1999;82:115–123.[↩][↩]
- Yoshioka M, St-Pierre S, Suzuki M, Tremblay A. Effects of red pepper added to high-fat and high-carbohydrate meals on energy metabolism and substrate utilization in Japanese women. Br J Nutr. 1998;80:503–510[↩]
- Reinbach HC, Smeets A, Martinussen T, Møller P, Westerterp-Plantenga M. Effects of capsaicin, green tea and CH-19 sweet pepper on appetite and energy intake in humans in negative and positive energy balance. Clin Nut. 2009;28:260–265.[↩]
- Smeets AJ, Westerterp-Plantenga MS. The acute effects of a lunch containing capsaicin on energy and substrate utilisation, hormones, and satiety. Eur J Nutr. 2009;48:229–234.[↩]
- Schroer B, Pien LC. Nonallergic rhinitis: common problem, chronic symptoms. Cleveland Clinic Journal of Medicine 2012;79(4):285-93.[↩]
- Stjarne P, Lundblad L, Anggard A, Hokfelt T, Lundberg JM. Tachykinins and calcitonin gene-related peptide: co-existence in sensory nerves of the nasal mucosa and effects on blood flow. Cell and Tissue Research 1989;256(3):439-46.[↩]
- Blom HM, Severijnen LA, Rijswijk JB, Mulder PG, Wijk RG, Fokkens WJ. The long-term effects of capsaicin aqueous spray on the nasal mucosa. Clinical and Experimental Allergy 1998;28(11):1351-8.[↩]
- van Rijswijk JB, Boeke EL, Keizer JM, Mulder PG, Blom HM, Fokkens WJ. Intranasal capsaicin reduces nasal hyperreactivity in idiopathic rhinitis: a double-blind randomized application regimen study. Allergy 2003;58(8):754-61.[↩]
- Bernstein J. A randomized, double-blind, parallel trial comparing capsaicin nasal spray with placebo in subjects with a significant component of nonallergic rhinitis. Annals of Allergy, Asthma, and Immunology 2011 Jun 29[↩]
- Ciabatti PG, D’Ascanio L. Intranasal capsicum spray in idiopathic rhinitis: a randomized prospective application regimen trial. Acta Oto-Laryngologica 2009;129(4):367-71.[↩]
- Gevorgyan A, Segboer C, Gorissen R, van Drunen CM, Fokkens W. Capsaicin for non-allergic rhinitis. Cochrane Database of Systematic Reviews 2015, Issue 7. Art. No.: CD010591. DOI: 10.1002/14651858.CD010591.pub2 http://cochranelibrary-wiley.com/doi/10.1002/14651858.CD010591.pub2/full[↩]
- Cheng J, Yang XN, Liu X, Zhang SP. Capsaicin for allergic rhinitis in adults. Cochrane Database of Systematic Reviews 2006, Issue 2. Art. No.: CD004460. DOI: 10.1002/14651858.CD004460.pub2. http://cochranelibrary-wiley.com/doi/10.1002/14651858.CD004460.pub2/full[↩]
- Jensen TS, Baron R, Haanpää M, Kalso E, Loeser JD, Rice AS, et al. A new definition of neuropathic pain. Pain 2011; Vol. 152, issue 10:2204-5.[↩]
- Helfert SM, Reimer M, Höper J, Baron R. Individualized pharmacological treatment of neuropathic pain. Clinical Pharmacology and Therapeutics 2015;97(2):135-42.[↩]
- Baron R, Wasner G, Binder A. Chronic pain: genes, plasticity, and phenotypes. Lancet Neurology 2012;11(1):19-21.[↩]
- Finnerup NB, Attal N, Haroutounian S, McNicol E, Baron R, Dworkin RH, et al. Pharmacotherapy for neuropathic pain in adults: a systematic review and meta-analysis. Lancet Neurology 2015;14(2):162-73.[↩][↩]
- Finnerup NB, Scholz J, Attal N, Baron R, Haanpää M, Hansson P, et al. Neuropathic pain needs systematic classification. European Journal of Pain 2013;17(7):953-6.[↩]
- Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012;380(9859):2163-96.[↩]
- Moore RA, Derry S, Taylor RS, Straube S, Phillips CJ. The costs and consequences of adequately managed chronic non-cancer pain and chronic neuropathic pain. Pain Practice 2014;14(1):79-94.[↩][↩]
- van Hecke O, Austin SK, Khan RA, Smith BH, Torrance N. Neuropathic pain in the general population: a systematic review of epidemiological studies. Pain 2014;155(4):654-62[↩]
- Gustorff B, Dorner T, Likar R, Grisold W, Lawrence K, Schwarz F, et al. Prevalence of self-reported neuropathic pain and impact on quality of life: a prospective representative survey. Acta Anaesthesiological Scandinavica 2008;52(1):132-6.[↩]
- Bouhassira D, Lantéri-Minet M, Attal N, Laurent B, Touboul C. Prevalence of chronic pain with neuropathic characteristics in the general population. Pain 2008;136(3):380-7.[↩]
- Torrance N, Smith BH, Bennett MI, Lee AJ. The epidemiology of chronic pain of predominantly neuropathic origin. Results from a general population survey. Journal of Pain 2006;7(4):281-9[↩]
- Hall GC, Carroll D, McQuay HJ. Primary care incidence and treatment of four neuropathic pain conditions: a descriptive study, 2002-2005. BMC Family Practice 2008;9:26.[↩][↩]
- Rappaport ZH, Devor M. Trigeminal neuralgia: the role of self-sustaining discharge in the trigeminal ganglion. Pain 1994;56:127-38[↩]
- Koopman JS, Dieleman JP, Huygen FJ, de Mos M, Martin CG, Sturkenboom MC. Incidence of facial pain in the general population. Pain 2009;147(1-3):122-7[↩]
- Derry S, Wiffen PJ, Moore RA, Quinlan J. Topical lidocaine for neuropathic pain in adults. Cochrane Database of Systematic Reviews 2014, Issue 7.[↩]
- Derry S, Sven-Rice A, Cole P, Tan T, Moore RA. Topical capsaicin (high concentration) for chronic neuropathic pain in adults. Cochrane Database of Systematic Reviews 2013, Issue 2.[↩]
- Lunn MP, Hughes RA, Wiffen PJ. Duloxetine for treating painful neuropathy, chronic pain or fibromyalgia. Cochrane Database of Systematic Reviews 2014, Issue 1[↩]
- Moore RA, Wiffen PJ, Derry S, McQuay HJ. Gabapentin for chronic neuropathic pain and fibromyalgia in adults. Cochrane Database of Systematic Reviews 2014, Issue 4.[↩]
- Moore RA, Straube S, Aldington D. Pain measures and cut-offs – ‘no worse than mild pain’ as a simple, universal outcome. Anaesthesia 2013;68(4):400-12[↩]
- Moore RA, Cai N, Skljarevski V, Tölle TR. Duloxetine use in chronic painful conditions – individual patient data responder analysis. European Journal of Pain 2014;18(1):67-75.[↩]
- Moore A, Derry S, Eccleston C, Kalso E. Expect analgesic failure; pursue analgesic success. BMJ 2013;346:f2690.[↩]
- National Institute for Health and Care Excellence (NICE). Neuropathic pain – pharmacological management: the pharmacological management of neuropathic pain in adults in non-specialist settings, 2013. www.nice.org.uk/guidance/cg173[↩]
- Derry S, Moore RA. Topical capsaicin (low concentration) for chronic neuropathic pain in adults. Cochrane Database of Systematic Reviews 2012, Issue 9[↩]
- Knolle E, Zadrazil M, Kovacs GG, Medwed S, Scharbert G, Schemper M. Comparison of cooling and EMLA to reduce the burning pain during capsaicin 8% patch application: a randomized, double-blind, placebo-controlled study. Pain 2013;154(12):2729-36.[↩]
- Kern KU, Nowack W, Poole C. Treatment of neuropathic pain with the capsaicin 8% patch: is pretreatment with lidocaine necessary?. Pain Practice 2014;14(2):E42-50.[↩]
- Derry S, Rice ASC, Cole P, Tan T, Moore RA. Topical capsaicin (high concentration) for chronic neuropathic pain in adults. Cochrane Database of Systematic Reviews 2017, Issue 1. Art. No.: CD007393. DOI: 10.1002/14651858.CD007393.pub4 http://cochranelibrary-wiley.com/doi/10.1002/14651858.CD007393.pub4/full[↩]





{kind=link}