Contents
What is carpal tunnel syndrome
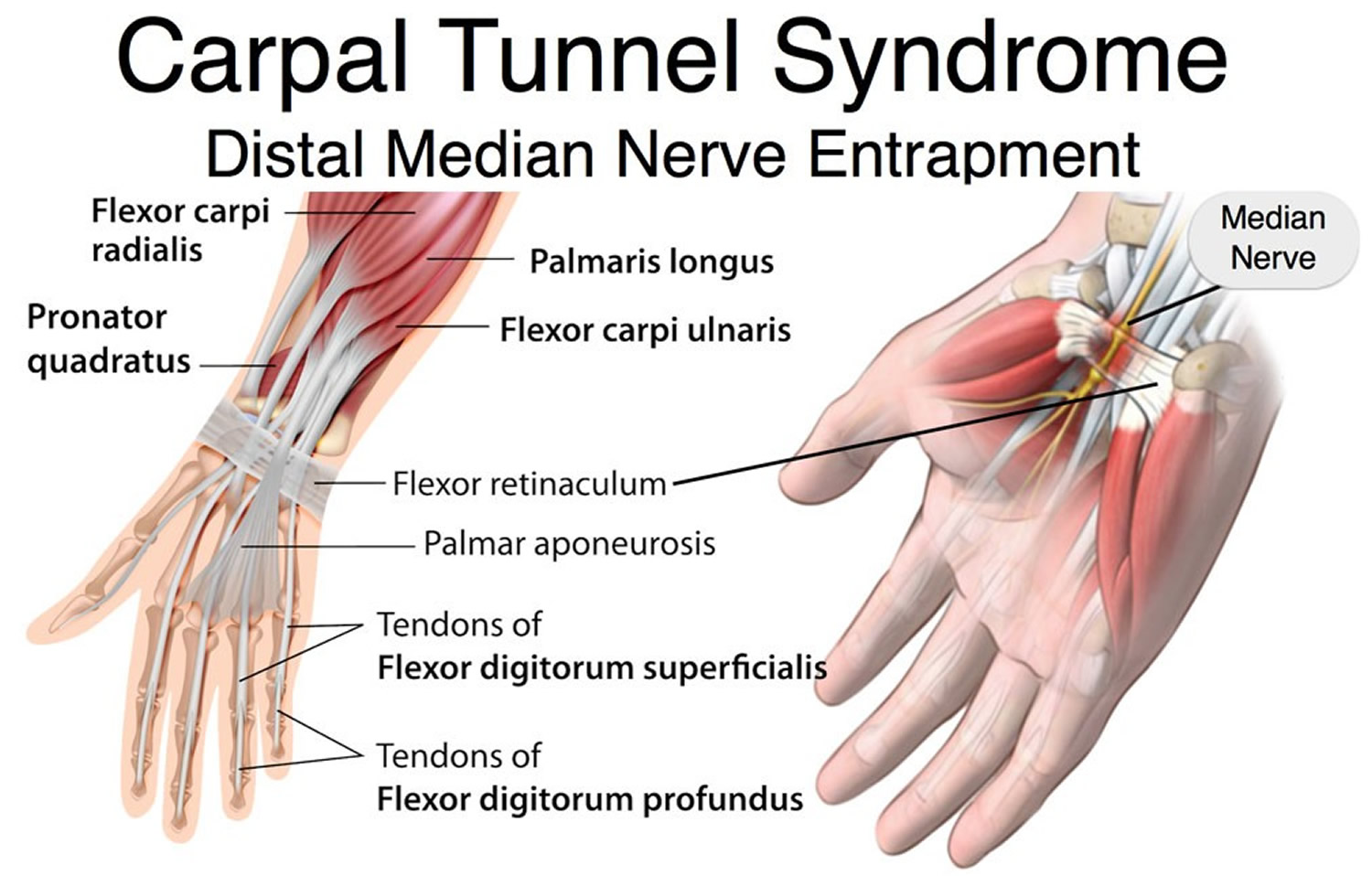
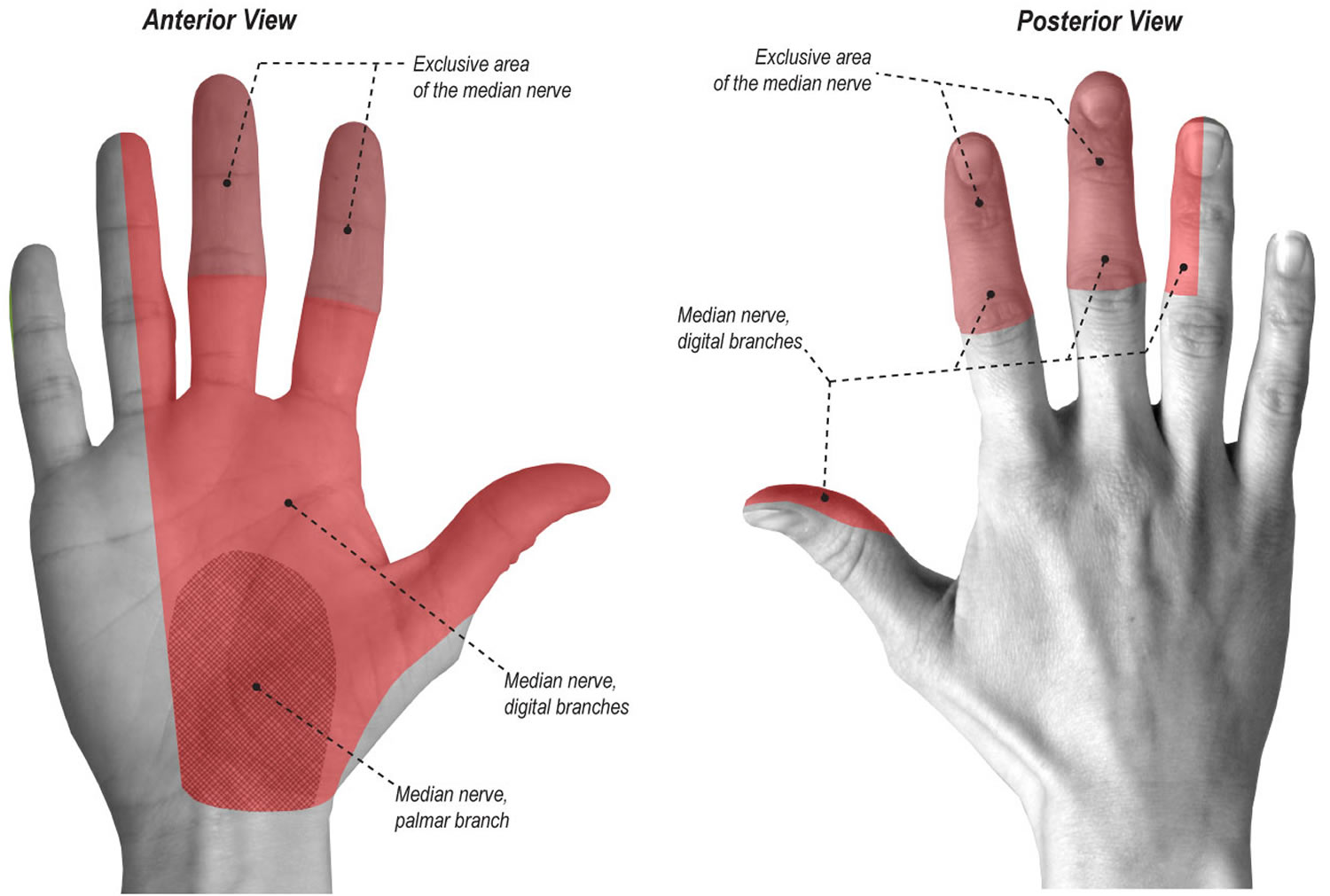
Carpal tunnel syndrome occurs when the median nerve, which runs from the forearm into the palm of the hand, becomes pressed or squeezed at the wrist 1. The carpal tunnel is a narrow, rigid passageway of ligament and bones at the base of the hand—houses the median nerve and the tendons that bend the fingers (see Figures 1 and 2). The median nerve provides feeling to the palm side of the thumb and to the index, middle, and part of the ring fingers (although not the little finger) (see Figure 3). It also controls some small muscles at the base of the thumb.
Sometimes, thickening from the lining of irritated tendons or other swelling narrows the tunnel and causes the median nerve to be compressed. The result may be numbness, tingling, weakness, or sometimes pain in the hand and wrist, or occasionally in the forearm and arm. Carpal tunnel syndrome is the most common and widely known of the entrapment neuropathies, in which one of the body’s peripheral nerves is pressed upon.
Carpal tunnel syndrome is the most common entrapment neuropathy, affecting approximately 3 to 6 percent of adults in the general population 2. Although the prevalence of bilateral symptoms is uncertain, one study in the United Kingdom reported bilateral symptoms in more than 50 percent of cases 3. The mean annual crude incidence of carpal tunnel syndrome was found to be 329 cases per 100,000 person-years 4.
The Carpal Tunnel
The carpal tunnel is a tight space between the flexor retinaculum and carpal bones. The flexor retinaculum is located over the palmar surface of the carpal bones. The long flexor tendons of the digits and wrist and the median nerve pass deep to the flexor retinaculum. The flexor retinaculum and carpal bones form a narrow space called the carpal tunnel. Through this tunnel pass the median nerve and tendons of the flexor digitorum superficialis, flexor digitorum profundus, and flexor pollicis longus muscles (Figures 1 and 2). The median nerve lies immediately under the palmaris longus tendon, at the midpoint of the wrist and medial to the flexor carpi radialis tendon 5.
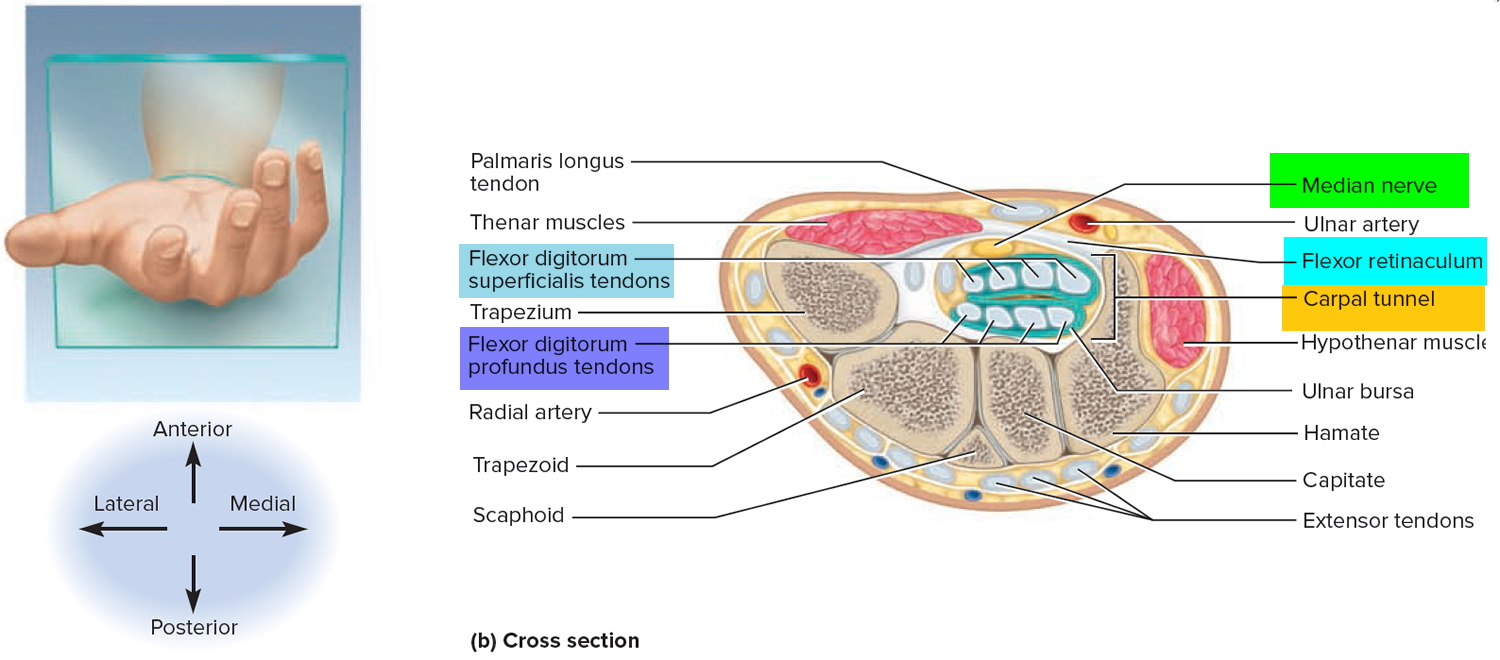
Prolonged, repetitive motions of the wrist and fingers can cause tissues in the carpal tunnel to become inflamed, swollen, or fibrotic. Since the carpal tunnel cannot expand, swelling puts pressure on the median nerve of the wrist, which passes through the carpal tunnel with the flexor tendons (Figure 2). This pressure causes tingling and muscular weakness in the palm and medial side of the hand and pain that may radiate to the arm and shoulder. This condition, called carpal tunnel syndrome, is common among keyboard operators, pianists, meat cutters, and others who spend long hours making repetitive wrist motions. Carpal tunnel syndrome is treated with aspirin and other anti-inflammatory drugs, immobilization of the wrist, and sometimes surgical removal of part or all of the flexor retinaculum to relieve pressure on the nerve.
Figure 1. Carpal tunnel (anterior view)
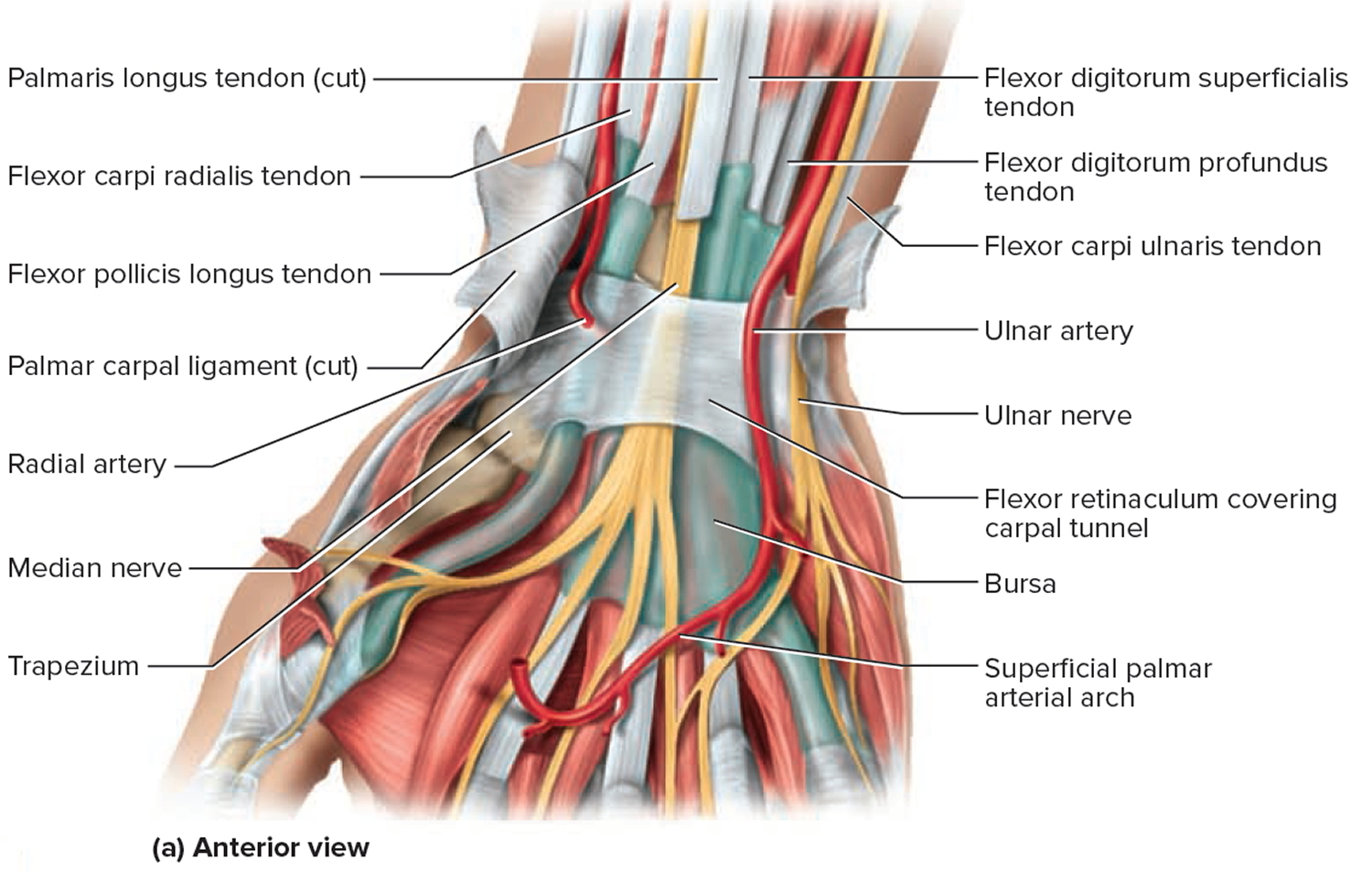
Figure 2. Carpal tunnel (cross section view)
Signs and symptoms of carpal tunnel syndrome
Carpal tunnel syndrome symptoms usually start gradually. The first symptoms often include numbness or tingling in your thumb, index and middle fingers that comes and goes.
Carpal tunnel syndrome may also cause discomfort in your wrist and the palm of your hand. Common carpal tunnel syndrome symptoms include:
Tingling or numbness. You may experience tingling and numbness in your fingers or hand. Usually the thumb and index, middle or ring fingers are affected, but not your little finger. Sometimes there is a sensation like an electric shock in these fingers.
The sensation may travel from your wrist up your arm. These symptoms often occur while holding a steering wheel, phone or newspaper. The sensation may wake you from sleep.
Many people “shake out” their hands to try to relieve their symptoms. The numb feeling may become constant over time.
Weakness. You may experience weakness in your hand and a tendency to drop objects. This may be due to the numbness in your hand or weakness of the thumb’s pinching muscles, which are also controlled by the median nerve.
The pain and paresthesias (burning, pins and needles or prickling sensation) characterizing carpal tunnel syndrome are typically along the distribution of the median nerve (i.e., thumb, index finger, and middle finger) see Figure 3. At times, these symptoms may occur in all the fingers, but should not occur in the dorsum or palm of the hand.
Figure 3. Median nerve palmar distribution
Pain and paresthesias may radiate proximally into the forearm, and even into the arm and shoulder. Patients may say that their fingers seem swollen and useless, but do not have swelling. They may also report loss of strength when gripping or performing certain tasks. The patient may be awakened with nighttime pain, with a history of shaking the hand or flicking the wrist in an attempt to alleviate the discomfort, which is known as the flick sign. The flick sign predicts electrodiagnostic abnormalities in 93 percent of cases and has a false-positive rate of less than 5 percent 6.
What causes Carpal tunnel syndrome
Carpal tunnel syndrome is caused by pressure on the median nerve.
The median nerve runs from your forearm through a passageway in your wrist (carpal tunnel) to your hand. It provides sensation to the palm side of your thumb and fingers, except the little finger. It also provides nerve signals to move the muscles around the base of your thumb (motor function).
Anything that squeezes or irritates the median nerve in the carpal tunnel space may lead to carpal tunnel syndrome. A wrist fracture can narrow the carpal tunnel and irritate the nerve, as can the swelling and inflammation resulting from rheumatoid arthritis.
There is no single cause in many cases. It may be that a combination of risk factors contributes to the development of the condition.
Risk factors for Carpal tunnel syndrome
A number of factors have been associated with carpal tunnel syndrome. Although they may not directly cause carpal tunnel syndrome, they may increase your chances of developing or aggravating median nerve damage. These include:
- Anatomic factors. A wrist fracture or dislocation, or arthritis that deforms the small bones in the wrist, can alter the space within the carpal tunnel and put pressure on the median nerve.
People with smaller carpal tunnels may be more likely to have carpal tunnel syndrome.
- Sex. Carpal tunnel syndrome is generally more common in women. This may be because the carpal tunnel area is relatively smaller in women than in men.
Women who have carpal tunnel syndrome may also have smaller carpal tunnels than women who don’t have the condition.
- Nerve-damaging conditions. Some chronic illnesses, such as diabetes, hypothyroidism, amyloidosis, sarcoidosis, multiple myeloma, leukemia increase your risk of nerve damage, including damage to your median nerve.
- Inflammatory conditions. Illnesses that are characterized by inflammation, such as rheumatoid arthritis, can affect the lining around the tendons in your wrist and put pressure on your median nerve.
- Obesity. Being obese is a significant risk factor for carpal tunnel syndrome.
- Alterations in the balance of body fluids. Fluid retention may increase the pressure within your carpal tunnel, irritating the median nerve. This is common during pregnancy and menopause. Carpal tunnel syndrome associated with pregnancy generally resolves on its own after pregnancy.
- Other medical conditions. Certain conditions, such as menopause, obesity, thyroid disorders and kidney failure, may increase your chances of carpal tunnel syndrome.
- Workplace factors. It’s possible that working with vibrating tools or on an assembly line that requires prolonged or repetitive flexing of the wrist may create harmful pressure on the median nerve or worsen existing nerve damage.
However, the scientific evidence is conflicting and these factors haven’t been established as direct causes of carpal tunnel syndrome.
Several studies have evaluated whether there is an association between computer use and carpal tunnel syndrome. However, there has not been enough quality and consistent evidence to support extensive computer use as a risk factor for carpal tunnel syndrome, although it may cause a different form of hand pain.
Prevention of carpal tunnel syndrome
There are no proven strategies to prevent carpal tunnel syndrome, but you can minimize stress on your hands and wrists with these methods:
- Reduce your force and relax your grip. If your work involves a cash register or keyboard, for instance, hit the keys softly. For prolonged handwriting, use a big pen with an oversized, soft grip adapter and free-flowing ink.
- Take frequent breaks. Gently stretch and bend hands and wrists periodically. Alternate tasks when possible. This is especially important if you use equipment that vibrates or that requires you to exert a great amount of force.
- Watch your form. Avoid bending your wrist all the way up or down. A relaxed middle position is best. Keep your keyboard at elbow height or slightly lower.
- Improve your posture. Incorrect posture rolls shoulders forward, shortening your neck and shoulder muscles and compressing nerves in your neck. This can affect your wrists, fingers and hands.
- Change your computer mouse. Make sure that your computer mouse is comfortable and doesn’t strain your wrist.
- Keep your hands warm. You’re more likely to develop hand pain and stiffness if you work in a cold environment. If you can’t control the temperature at work, put on fingerless gloves that keep your hands and wrists warm.
Carpal tunnel syndrome diagnosis
The diagnosis of carpal tunnel syndrome is primarily based on history and physical examination findings. Adjunctive tests are useful when the diagnosis is uncertain. Electrodiagnostic testing is indicated for selected patients, whereas ultrasonography, magnetic resonance imaging, and computed tomography generally are not helpful 7.
Nerve conduction studies and electromyography can be used for confirmation of diagnosis in patients with an intermediate pretest probability or with an atypical presentation. Nerve conduction studies and electromyography can also be used to quantify and stratify disease severity, which may aid in treatment decisions 8. A slowed median nerve conduction velocity supports the diagnosis. Nerve conduction studies have a sensitivity of 56 to 85 percent and a specificity of at least 94 percent for carpal tunnel syndrome 9. Electromyography is often paired with nerve conduction studies to differentiate primary muscle conditions from muscle weakness caused by neurologic disorders. In patients with a high probability of carpal tunnel syndrome based on history and physical examination, nerve conduction studies and electromyography generally are not indicated 8.
Your doctor may ask you questions and conduct one or more of the following tests to determine whether you have carpal tunnel syndrome:
History of symptoms. Your doctor will review the pattern of your symptoms. For example, because the median nerve doesn’t provide sensation to your little finger, symptoms in that finger may indicate a problem other than carpal tunnel syndrome.
Carpal tunnel syndrome symptoms usually occur include while holding a phone or a newspaper, gripping a steering wheel, or waking up during the night.
Physical examination. Your doctor will conduct a physical examination. He or she will test the feeling in your fingers and the strength of the muscles in your hand.
Bending the wrist, tapping on the nerve or simply pressing on the nerve can trigger symptoms in many people.
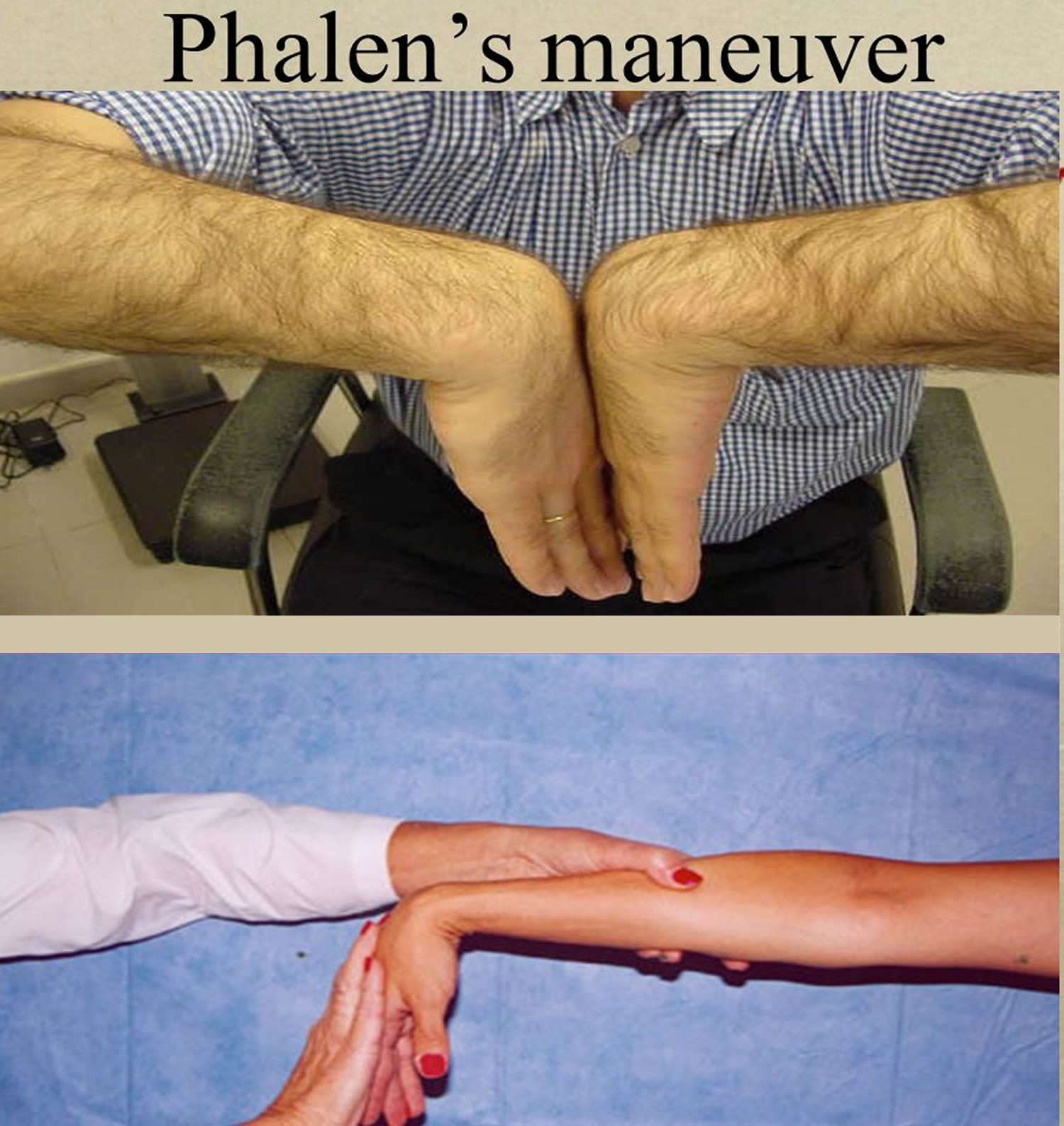
Phalen maneuver: The patient is asked to hold their wrist in complete and forced flexion (pushing the dorsal surfaces of both hands together) for 30–60 seconds. The lumbricals attach in part to the flexor digitorum profundus tendons. As the wrist flexes, the flexor digitorum profundus contracts in a proximal direction, drawing the lumbricals along with it. In some individuals, the lumbricals can be “dragged” into the carpal tunnel with flexor digitorum profundus contraction. As such, Phalen’s maneuver can moderately increase the pressure in the carpal tunnel via this mass effect, pinching the median nerve between the proximal edge of the transverse carpal ligament and the anterior border of the distal end of the radius. By compressing the median nerve within the carpal tunnel, characteristic symptoms (such as burning, tingling or numb sensation over the thumb, index, middle and ring fingers) conveys a positive test result and suggests carpal tunnel syndrome. Because not all individuals will draw the lumbricals into the carpal tunnel with this maneuver, this test cannot be perfectly sensitive or specific for carpal tunnel syndrome.
Figure 4. Phalen maneuver
X-ray. Some doctors recommend an X-ray of the affected wrist to exclude other causes of wrist pain, such as arthritis or a fracture.
Electromyogram. This test measures the tiny electrical discharges produced in muscles. During this test, your doctor inserts a thin-needle electrode into specific muscles to evaluate the electrical activity when muscles contract and rest. This test can identify muscle damage and also may rule out other conditions.
Nerve conduction study. In a variation of electromyography, two electrodes are taped to your skin. A small shock is passed through the median nerve to see if electrical impulses are slowed in the carpal tunnel. This test may be used to diagnose your condition and rule out other conditions.
Table 1. Carpal tunnel syndrome test and the diagnostic Value of History and Physical Examination Findings for Carpal Tunnel Syndrome
| Finding | Sensitivity (%) | Specificity (%) | Positive likelihood ratio | Negative likelihood ratio |
|---|---|---|---|---|
Flick sign | 93 | 96 | 21.4 | 0.1 |
Hypalgesia | 39 | 88 | 3.1 | 0.7 |
Square wrist sign | 53 | 80 | 2.7 | 0.6 |
Classic or probable pattern on hand symptom diagram | 64 | 73 | 2.4 | 0.5 |
Abduction weakness | 65 | 65 | 1.8 | 0.5 |
Thenar atrophy | 16 | 90 | 1.6 | 0.94 |
Tinel sign | 36 | 75 | 1.4 | 0.8 |
Phalen maneuver | 57 | 58 | 1.3 | 0.7 |
Nighttime or morning symptoms | 70 | 43 | 1.2 | 0.7 |
Table 2. Disease Classification in Carpal Tunnel Syndrome
| Classification | Duration | Two-point discrimination test | Weakness | Atrophy | Electromyography* | Nerve conduction studies* |
|---|---|---|---|---|---|---|
Mild | Shorter than one year | Normal | Absent | Absent | No denervation | No to mild velocity decrease |
Moderate | Shorter or longer than one year | Possible abnormality | Minimal presence | Minimal presence | No to mild denervation | No to mild velocity decrease |
Severe | Longer than one year | Marked abnormality | Marked presence | Marked presence | Marked denervation | Marked velocity decrease |
[Source 10]
Carpal tunnel syndrome treatment
Treat carpal tunnel syndrome as early as possible after symptoms start. Management of carpal tunnel syndrome should be based on severity. Patients with mild to moderate carpal tunnel syndrome have normal to mildly abnormal nerve conduction study and electromyography findings. Severe disease is suggested by worsening clinical symptoms and clearly abnormal electrodiagnostic studies (Table 2).
Take more frequent breaks to rest your hands. Avoiding activities that worsen symptoms and applying cold packs to reduce swelling also may help.
Other treatment options include wrist splinting, medications and surgery. Splinting and other conservative treatments are more likely to help if you’ve had only mild to moderate symptoms for less than 10 months.
Six weeks to three months of conservative treatment is reasonable in patients with mild disease 11. Cock-up and neutral wrist splints and oral nonsteroidal anti-inflammatory drugs (NSAIDs) are considered first-line therapies, with local corticosteroid injections used for refractory symptoms. Patients with moderate to severe disease, or those with persistent symptoms despite conservative treatment, may be referred for surgical evaluation 12.
Nonsurgical therapy
If the condition is diagnosed early, nonsurgical methods may help improve carpal tunnel syndrome, including:
Lifestyle Modification. The most important nonsurgical treatment is looking at the activities that you’re doing and making sure you’re not doing any of these awkward activities with the wrist bent, strong pinching, strong gripping, that might predispose or aggravate people to have carpal tunnel syndrome.
After the activity modifications, it’s important for people to remember to take frequent rest breaks, perhaps five minutes every hour, to do something a little bit different with their hands, to give their hands a chance to get some more circulation back into their hands as they’re doing activities throughout the day, and to vary your activities as much as you can throughout the day. So activity modification is very important.
Using ergonomic equipment (e.g., wrist rest, mouse pad), taking breaks, using keyboard alternatives (e.g., digital pen, voice recognition and dictation software), and alternating job functions have traditionally been advocated for management of carpal tunnel syndrome. However, there is inconsistent evidence to support or refute the effectiveness of any of these interventions.
Wrist splinting. A carpal tunnel syndrome splint that holds your wrist still while you sleep can help relieve nighttime symptoms of tingling and numbness. Splinting is very helpful, especially at night and may be a good option if you’re pregnant.
Many people wake up in the middle of the night with their hands numb and tingling. It’s a very common symptom of carpal tunnel syndrome. That symptom can often times be controlled by wearing a brace on your wrist at night. Wearing a brace during the day usually just makes you do things differently and may actually aggravate the symptoms of carpal tunnel syndrome because you’re doing things in a more awkward fashion. But at night, splinting can be very helpful.
The other time that splinting is useful is when you’re driving a car or something like that where you’re doing prolonged gripping, and again, the splint helps to hold your wrist in a straighter position that can be helpful.
Figure 5. A neutral wrist splint for carpal tunnel syndrome

Nonsteroidal anti-inflammatory drugs (NSAIDs). NSAIDs, such as ibuprofen (Advil, Motrin IB, others), may help relieve pain from carpal tunnel syndrome in the short term.
There isn’t evidence, however, that these drugs improve carpal tunnel syndrome.
Corticosteroids. Your doctor may inject your carpal tunnel with a corticosteroid such as cortisone to relieve pain. Sometimes your doctor uses an ultrasound to guide these injections.
Corticosteroids decrease inflammation and swelling, which relieves pressure on the median nerve. Oral corticosteroids aren’t considered as effective as corticosteroid injections for treating carpal tunnel syndrome 13. Although effectiveness is primarily short-term, corticosteroid injection may be particularly useful for patients wanting to delay surgical treatment.
The procedure involves placing a small bolus of corticosteroid beneath the flexor retinaculum and within the carpal tunnel. A correlation between corticosteroid dose and symptom reduction has not been observed, and there are no good data supporting a specific type of corticosteroid formulation over another 14. Traditionally, 20 mg of triamcinolone acetonide (Kenalog) without lidocaine (Xylocaine) is injected using a 1-mL syringe with a 25-gauge, 1.25-inch needle 5. Median nerve injection injury is the major potential complication of these injections.
Doctors don’t know exactly how it works, but it does seem to provide at least temporary relief in almost everybody with carpal tunnel syndrome, and in about a third of people, it can provide quite long-lasting relief.
If carpal tunnel syndrome is caused by rheumatoid arthritis or another inflammatory arthritis, then treating the arthritis may reduce symptoms of carpal tunnel syndrome. However, this is unproven.
Carpal tunnel syndrome surgery
Surgery may be appropriate if your symptoms are severe or don’t respond to other treatments.
The goal of carpal tunnel surgery is to relieve pressure by cutting the ligament pressing on the median nerve.
Five-year outcomes regarding carpal tunnel syndrome symptom relief have been shown to be equivalent using open or endoscopic surgical techniques 15. Surgical treatment of carpal tunnel syndrome relieves symptoms significantly more than splinting, but not necessarily more than corticosteroid injection 16. On average, postsurgical patients were able to return to driving in nine days, to activities of daily living in 13 days, and to work in 17 days, with a satisfaction rate of more than 90 percent 17.
Figure 6. Carpal tunnel surgery (carpal tunnel release)
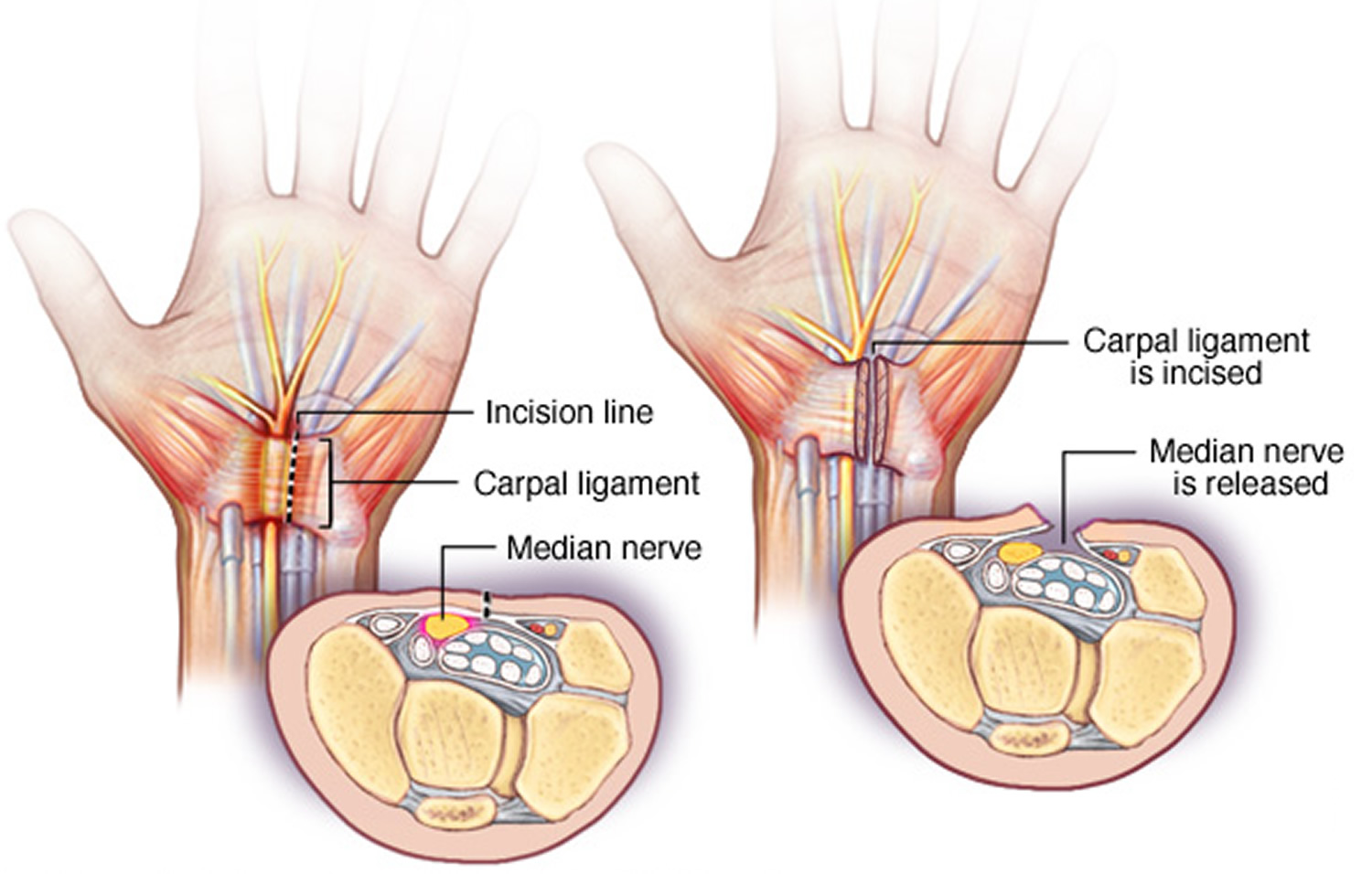
Note: During carpal tunnel release, a surgeon makes an incision in the palm of your hand over the carpal tunnel ligament and cuts through the ligament to relieve pressure on the median nerve. The surgery may be done by making one incision on the palm side of the wrist, or by making several small incisions.
The surgery may be performed with two different techniques:
- Endoscopic surgery. Your surgeon uses a telescope-like device with a tiny camera attached to it (endoscope) to see inside your carpal tunnel. Your surgeon cuts the ligament through one or two small incisions in your hand or wrist.
Endoscopic surgery may result in less pain than does open surgery in the first few days or weeks after surgery.
- Open surgery. Your surgeon makes an incision in the palm of your hand over the carpal tunnel and cuts through the ligament to free the nerve.
Discuss the risks and benefits of each technique with your surgeon before surgery. Surgery risks may include:
- Incomplete release of the ligament
- Wound infections
- Scar formation
- Nerve or vascular injuries
During the healing process after the surgery, the ligament tissues gradually grow back together while allowing more room for the nerve. This internal healing process typically takes several months, but the skin heals in a few weeks.
Lifestyle and home remedies for carpal tunnel syndrome
These steps may provide temporary symptom relief:
- Take short breaks from repetitive activities involving the use of your hands.
- Lose weight if you are overweight or obese.
- Rotate your wrists and stretch your palms and fingers.
- Take a pain reliever, such as aspirin, ibuprofen (Advil, Motrin IB, others) or naproxen sodium (Aleve).
- Wear a snug, not tight, wrist splint at night. You can find these over-the-counter at most drugstores or pharmacies.
- Avoid sleeping on your hands.
If pain, numbness or weakness recurs and persists, see your doctor.
Carpal tunnel syndrome exercises
Would regular hand and wrist exercises help me avoid surgery?
Probably not. Carpal tunnel exercises alone aren’t likely to relieve symptoms, such as pain and numbness. These exercises are most effective when combined with other treatments, such as behavior changes or wrist splints, for mild to moderate carpal tunnel syndrome. If your symptoms are severe, you’ll likely still need surgery to get relief.
Carpal tunnel syndrome is caused by compression of the median nerve as it passes through the carpal tunnel and under the transverse carpal ligament at the wrist. Nerve-gliding exercises — one type of carpal tunnel exercise — might help the median nerve move normally, but might worsen symptoms. If a median nerve remains trapped, nerve-gliding exercises can stretch, irritate or injure the nerve.
Despite their limitations, carpal tunnel exercises might help:
- To complement another treatment. Carpal tunnel exercises might help mild to moderate symptoms when combined with other treatments, such as changing your activities, wrist splinting or corticosteroid injections.
- After surgery to prevent nerve scarring. Range-of-motion exercises — which may include nerve-gliding exercises — might help heal significant trauma to the wrist, such as a wrist fracture that requires surgery or repair near the carpal tunnel.
If your doctor recommends carpal tunnel exercises, start them gradually to ensure they don’t cause more harm than good.
Alternative medicine
Integrate alternative therapies into your treatment plan to help you cope with carpal tunnel syndrome. You may have to experiment to find a treatment that works for you. Always check with your doctor before trying any complementary or alternative treatment.
- Yoga. Yoga postures designed for strengthening, stretching and balancing the upper body and joints may help reduce pain and improve grip strength.
- Hand therapy. Early research suggests that certain physical and occupational hand therapy techniques may reduce symptoms of carpal tunnel syndrome.
- Ultrasound therapy. High-intensity ultrasound can be used to raise the temperature of a targeted area of body tissue to reduce pain and promote healing.
- Research shows inconsistent results with this therapy, but a course of ultrasound therapy over several weeks may help reduce symptoms.
- Carpal Tunnel Syndrome Fact Sheet. https://www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Fact-Sheets/Carpal-Tunnel-Syndrome-Fact-Sheet[↩]
- Atroshi I, Gummesson C, Johnsson R, Ornstein E, Ranstam J, Rosén I. Prevalence of carpal tunnel syndrome in a general population. JAMA. 1999;282(2):153–158.[↩]
- Bland JD, Rudolfer SM. Clinical surveillance of carpal tunnel syndrome in two areas of the United Kingdom, 1991–2001. J Neurol Neurosurg Psychiatry. 2003;74(12):1674–1679.[↩]
- Mondelli M, Giannini F, Giacchi M. Carpal tunnel syndrome incidence in a general population. Neurology. 2002;58(2):289–294.[↩]
- Saunder S, Longworth S, Maddison P. Injection Techniques in Orthopaedics and Sports Medicine: A Practical Manual for Doctors and Physiotherapists. 3rd ed. Edinburgh, U.K.: Elsevier/Churchill Livingstone; 2006:82–83.[↩][↩]
- D’Arcy CA, McGee S. The rational clinical examination. Does this patient have carpal tunnel syndrome? [published correction appears in JAMA. 2000;284(11):1384]. JAMA. 2000;283(23):3110–3117.[↩][↩]
- Graham B. The value added by electrodiagnostic testing in the diagnosis of carpal tunnel syndrome. J Bone Joint Surg Am. 2008;90(12):2587–2593.[↩]
- Pastare D, Therimadasamy AK, Lee E, Wilder-Smith EP. Sonography versus nerve conduction studies in patients referred with a clinical diagnosis of carpal tunnel syndrome [published correction appers in J Clin Ultrasound. 2010;38(4):226]. J Clin Ultrasound. 2009;37(7):389–393.[↩][↩]
- Keith MW, Masear V, Chung K, et al. Diagnosis of carpal tunnel syndrome. J Am Acad Orthop Surg. 2009;17(6):389–396.[↩]
- Carpal Tunnel Syndrome. Am Fam Physician. 2011 Apr 15;83(8):952-958. https://www.aafp.org/afp/2011/0415/p952.html[↩]
- Shrivastava N, Szabo RM. Decision making in the management of entrapment neuropathies of the upper extremity. J Musculoskeletal Med. 2008;25(6):278–289.[↩]
- Piazzini DB, Aprile I, Ferrara PE, et al. A systematic review of conservative treatment of carpal tunnel syndrome. Clin Rehabil. 2007;21(4):299–314.[↩]
- Marshall S, Tardif G, Ashworth N. Local corticosteroid injection for carpal tunnel syndrome. Cochrane Database Syst Rev. 2007;(2):CD001554.[↩]
- Boyer MI. Corticosteroid injection for carpal tunnel syndrome. J Hand Surg Am. 2008;33(8):1414–1416.[↩]
- Atroshi I, Hofer M, Larsson GU, Ornstein E, Johnsson R, Ranstam J. Open compared with 2-portal endoscopic carpal tunnel release: a 5-year follow-up of a randomized controlled trial. J Hand Surg Am. 2009;34(2):266–272.[↩]
- Verdugo RJ, Salinas RA, Castillo JL, Cea JG. Surgical versus non-surgical treatment for carpal tunnel syndrome. Cochrane Database Syst Rev. 2010;(8):CD001552.[↩]
- Acharya AD, Auchincloss JM. Return to functional hand use and work following open carpal tunnel surgery. J Hand Surg Br. 2005;30(6):607–610.[↩]





{kind=link}