
Contents
- What is chronic fatigue syndrome
- Chronic fatigue syndrome causes
- Chronic fatigue syndrome symptoms
- Chronic fatigue syndrome diagnosis
- Chronic fatigue syndrome treatment
- Chronic fatigue syndrome diet
- Dietary interventions and chronic fatigue syndrome symptom alleviation
- Animal studies and polyphenols
- Dietary intake and poor vitamin or mineral status and chronic fatigue syndrome
- Tryptophan and glutamine amino acids and chronic fatigue syndrome
- Phosphate diabetes and consideration of differential diagnosis to chronic fatigue syndrome
What is chronic fatigue syndrome
Chronic fatigue syndrome long-term complex illness that causes extreme fatigue that can’t be explained by any underlying medical condition 1. This fatigue is not the kind of tired feeling that goes away after you rest. Instead, it lasts a long time and limits your ability to do ordinary daily activities.
- The main symptom of chronic fatigue syndrome/myalgic encephalomyelitis is extreme physical and mental tiredness (fatigue) that doesn’t go away with rest or sleep. This can make it difficult to carry out everyday tasks and activities.
- Most people with chronic fatigue syndrome/myalgic encephalomyelitis describe their fatigue as overwhelming and a different type of tiredness from what they’ve experienced before.
- Exercising usually makes the symptoms of chronic fatigue syndrome/myalgic encephalomyelitis worse. Sometimes the effect is delayed and you’ll feel very tired a few hours after you’ve exercised, or even the next day.
- The symptoms of chronic fatigue syndrome/myalgic encephalomyelitis are similar to the symptoms of some other illnesses, making chronic fatigue syndrome (myalgic encephalomyelitis) hard to diagnose. There are no tests for it and other illnesses can cause similar symptoms. Your doctor has to rule out other diseases before making a diagnosis of chronic fatigue syndrome (myalgic encephalomyelitis), that is why it’s so important to see your doctor to get a correct diagnosis.
Chronic fatigue syndrome is also known as myalgic encephalomyelitis 2. Chronic fatigue syndrome (myalgic encephalomyelitis) can affect anyone, including children. It’s more common in women in their 40s and 50s 3 and tends to develop between your mid-20s and mid-40s and being most common in people between 40 and 60 years old 2. Whites are diagnosed more than other races and ethnicities. But many people with chronic fatigue syndrome (myalgic encephalomyelitis) have not been diagnosed, especially among minorities.
There is not an established racial or educational predilection 4. Chronic Fatigue Syndrome is often mentally and emotionally debilitating, and persons with this diagnosis are twice as likely to be unemployed as persons with fatigue who do not meet formal criteria for chronic fatigue syndrome 5.
As noted in the Institute of Medicine report 6:
- An estimated 836,000 to 2.5 million Americans suffer from chronic fatigue syndrome (myalgic encephalomyelitis).
- About 90 percent of people with chronic fatigue syndrome (myalgic encephalomyelitis) have not been diagnosed.
- Chronic fatigue syndrome (myalgic encephalomyelitis) costs the U.S. economy about $17 to $24 billion annually in medical bills and lost incomes.
People with chronic fatigue syndrome (myalgic encephalomyelitis) are often not able to do their usual activities. At times, chronic fatigue syndrome (myalgic encephalomyelitis) may confine them to bed. People with chronic fatigue syndrome (myalgic encephalomyelitis) have overwhelming fatigue that is not improved by rest. Chronic fatigue syndrome (myalgic encephalomyelitis) may get worse after any activity, whether it’s physical or mental. This symptom is known as post-exertional malaise. Other symptoms can include problems with sleep, thinking and concentrating, pain, and dizziness. People with chronic fatigue syndrome (myalgic encephalomyelitis) may not look ill. However,
- People with chronic fatigue syndrome (myalgic encephalomyelitis) are not able to function the same way they did before they became ill.
- chronic fatigue syndrome (myalgic encephalomyelitis) changes people’s ability to do daily tasks, like taking a shower or preparing a meal.
- chronic fatigue syndrome (myalgic encephalomyelitis) often makes it hard to keep a job, go to school, and take part in family and social life.
- chronic fatigue syndrome (myalgic encephalomyelitis) can last for years and sometimes leads to serious disability.
- At least one in four chronic fatigue syndrome (myalgic encephalomyelitis) patients is bed- or house-bound for long periods during their illness.
There is no cure for chronic fatigue syndrome (myalgic encephalomyelitis), so the goal of treatment is to improve symptoms. Chronic fatigue syndrome (myalgic encephalomyelitis) affects people in different ways. You should work with your doctors to create a treatment program that best meets your own needs. It may include therapies to manage your symptoms, such as medicines to treat pain, sleep disorders, and other problems. It may also include coping techniques, and ways of managing your daily activities.
Chronic fatigue syndrome causes
Scientists have not yet identified what causes chronic fatigue syndrome (myalgic encephalomyelitis). It is possible that chronic fatigue syndrome (myalgic encephalomyelitis) has more than one cause, meaning that patients with chronic fatigue syndrome (myalgic encephalomyelitis) could have illness resulting from different causes. In addition, it is possible that two or more triggers might work together to cause the illness.
Potential triggers for chronic fatigue syndrome (myalgic encephalomyelitis) include:
- Viral infections. Because some people develop chronic fatigue syndrome after having a viral infection, researchers question whether some viruses might trigger the disorder. Suspicious viruses include Epstein-Barr virus, human herpes virus 6 and mouse leukemia viruses. No conclusive link has yet been found.
- Immune system problems. The immune systems of people who have chronic fatigue syndrome appear to be impaired slightly, but it’s unclear if this impairment is enough to actually cause the disorder
- Hormonal imbalances. People who have chronic fatigue syndrome also sometimes experience abnormal blood levels of hormones produced in the hypothalamus, pituitary glands or adrenal glands. But the significance of these abnormalities is still unknown.
Some of the areas that are being studied as possible causes of chronic fatigue syndrome (myalgic encephalomyelitis) are:
Infections
People with chronic fatigue syndrome (myalgic encephalomyelitis) often have their illness begin in a way that reminds them of getting the flu. This has made researchers suspect an infection may trigger chronic fatigue syndrome (myalgic encephalomyelitis). In addition, about one in ten people who become infected with Epstein-Barr virus, Ross River virus, or Coxiella burnetti will develop a set of symptoms that meet the criteria for chronic fatigue syndrome (myalgic encephalomyelitis). People with these infections who had severe symptoms are more likely than those with mild symptoms to later develop chronic fatigue syndrome (myalgic encephalomyelitis) symptoms. But not all people with chronic fatigue syndrome (myalgic encephalomyelitis) have had these infections.
Other infections that have been studied in connection with chronic fatigue syndrome (myalgic encephalomyelitis) are human herpesvirus 6, enterovirus, rubella, Candida albicans, bornaviruses, mycoplasma, and human immunodeficiency virus (HIV). However, these infections have not been found to cause chronic fatigue syndrome (myalgic encephalomyelitis).
Immune System Changes
It is possible that chronic fatigue syndrome (myalgic encephalomyelitis) is caused by a change in the person’s immune system and the way it responds to infection or stress. Chronic fatigue syndrome (myalgic encephalomyelitis) shares some features of autoimmune illnesses (diseases in which the immune system attacks healthy tissues in own body, like in rheumatoid arthritis). For example, both chronic fatigue syndrome (myalgic encephalomyelitis) and most autoimmune diseases are more common in women and both are characterized by increased inflammation. However, other signs of autoimmune disease, like tissue damage, are not found in patients with chronic fatigue syndrome (myalgic encephalomyelitis).
Scientists think that the immune system might be contributing to chronic fatigue syndrome (myalgic encephalomyelitis) in other ways, including:
- Chronic production of cytokines (cytokines are proteins that are produced by the immune system and regulate behavior of other cells). Higher levels of cytokines for a prolonged period can lead to changes in the body’s ability to respond to stress and might lead to the development of health conditions, including chronic fatigue syndrome (myalgic encephalomyelitis).
- Low-functioning natural killer (NK) cells. NK cells are cells of the immune system that help the body fight infections. Many patients with chronic fatigue syndrome (myalgic encephalomyelitis) have NK cells with lower functional ability to fight infections. Studies have found that the poorer the function of NK cells in chronic fatigue syndrome (myalgic encephalomyelitis) patients, the worse the severity of the illness. NK cell function tests are hard to do and their results are not reliable outside of research studies. Because of this problem, NK cell function testing is not yet useful for healthcare providers. Also, low NK cell function can occur in other illnesses and thus cannot be used to diagnose chronic fatigue syndrome (myalgic encephalomyelitis).
- Differences in markers of T-cell activation. T-cells are cells of the immune system that help activate and suppress immune responses to infections. If they become too active or not active enough, the immune response does not work as it should. However, not all patients with chronic fatigue syndrome (myalgic encephalomyelitis) appear to have these differences in markers of T-cell activation.
Stress Affecting Body Chemistry
Physical or emotional stress affects the hypothalamic-pituitary-adrenal axis (HPA axis). The hypothalamic-pituitary-adrenal axis is a complex network that controls our body’s reaction to stress and regulates a lot of body processes such as the immune response, digestion, energy usage, and mood. This occurs through connections between two glands of the nervous system (hypothalamus and pituitary) and adrenal glands (small organs that reside on top of the kidneys). The glands release various hormones, like corticotrophin-releasing hormone (CRH), cortisol, and others. When these hormones get out of balance, many body systems and functions, like the immune response, can be negatively affected. Cortisol, also called “the stress hormone,” helps to lower inflammation and calm down the immune system. Low levels of cortisol thus may lead to an increase in inflammation and chronic activation of the immune system.
Hypocortisolism (low blood cortisol) has been noted in persons with chronic fatigue syndrome; one study found cortisol levels in patients with chronic fatigue syndrome were about 5 mcg per dL (137.94 nmol per L) less than the levels in patients without chronic fatigue syndrome 7. This is likely secondary to impaired adrenal cortex responsiveness to adrenocorticotropic hormones and not to hypothalamopituitary dysfunction 8. It is unclear if such dysfunction is caused by infection, genetics, childhood trauma, unknown factors, or some combination of these.
Patients with chronic fatigue syndrome (myalgic encephalomyelitis) commonly report physical or emotional stress before they become ill. Some patients with chronic fatigue syndrome (myalgic encephalomyelitis) have lower levels of cortisol than healthy people, but their cortisol levels are still within the normal range. Therefore, doctors cannot use cortisol levels to diagnose or treat chronic fatigue syndrome (myalgic encephalomyelitis).
Changes in Energy Production
Scientists found differences between people with chronic fatigue syndrome (myalgic encephalomyelitis) and healthy people in the way cells in their bodies get their energy. However, more studies are needed to figure out how these findings may be contributing to the illness.
Possible Genetic Link
Members of the same family sometimes have chronic fatigue syndrome (myalgic encephalomyelitis). Studies done in twins and families suggest that both genes and environment might play a role in chronic fatigue syndrome (myalgic encephalomyelitis). One study found a difference in the expression of certain genes in patients with chronic fatigue syndrome after exercise that play a role in metabolism and immune responses 9. Another study has shown an association between specific genetic mutations, chronic fatigue syndrome, and certain viral infections that have been linked to chronic fatigue syndrome 10. Scientists have not yet found the exact genes or other factors from the environment that may be responsible. More research is needed.
Chronic fatigue syndrome (myalgic encephalomyelitis) is often associated with depression, which has led many physicians to believe that chronic fatigue syndrome (myalgic encephalomyelitis) is a purely somatic illness. Evidence supporting this conclusion is lacking. Strong evidence suggests that childhood trauma increases the risk of chronic fatigue syndrome (myalgic encephalomyelitis) by as much as sixfold. Some persons may assume that childhood trauma decreases resiliency, but there is evidence to suggest that it may also play an organic role by increasing the risk of adrenal system dysfunction 11. It is important to note that social support systems for persons with chronic fatigue syndrome (myalgic encephalomyelitis) tend to be less reliable than for those who are healthy 12. Treatment for chronic fatigue syndrome (myalgic encephalomyelitis) is less likely to succeed in persons with poor social adjustment 13.
Sleep and Nutrition
There is an association between delayed dim light melatonin onset and chronic fatigue syndrome (myalgic encephalomyelitis), suggesting that delayed circadian rhythm could contribute to chronic fatigue syndrome (myalgic encephalomyelitis) 14. Although melatonin is available over the counter for delayed dim light melatonin onset in the United States, there is no evidence for improvement in chronic fatigue syndrome (myalgic encephalomyelitis) with melatonin 15.
One study has shown that persons with chronic fatigue syndrome (myalgic encephalomyelitis) have lower ratios of omega-3 to omega-6 unsaturated fatty acids and lower zinc levels than healthy patients 16. However, studies of nutritional supplementation in those with chronic fatigue syndrome (myalgic encephalomyelitis) have shown no benefit 17.
Chronic fatigue syndrome symptoms
The main symptom of chronic fatigue syndrome (myalgic encephalomyelitis) is severe fatigue that lasts for 6 months or more. You also have at least four of these other symptoms:
- Feeling unwell for more than 24 hours after physical activity
- Muscle or joint pain
- Memory problems
- Headaches
- Pain in multiple joints
- Sleep problems
- Sore throat or sore glands that aren’t swollen and that happens often
- Tender lymph nodes in the neck or armpits
- Problems thinking, remembering or concentrating
- Flu-like symptoms
- Feeling dizzy or sick
- Fast or irregular heartbeats (heart palpitations)
- Digestive issues, like irritable bowel syndrome
- Chills and night sweats
- Allergies and sensitivities to foods, odors, chemicals, or noise
People who have chronic fatigue syndrome appear to be hypersensitive to even normal amounts of exercise and activity. Most people find overexercising makes their symptoms worse. Why this occurs in some people and not others is still unknown. Some people may be born with a predisposition for the disorder, which is then triggered by a combination of factors.
The severity of symptoms can vary from day to day, or even within a day.
Most cases of chronic fatigue syndrome/myalgic encephalomyelitis are mild or moderate, but up to one in four people have severe symptoms. If your symptoms are severe, a specialist should be involved in your treatment.
Chronic fatigue syndrome/myalgic encephalomyelitis symptoms can be considered:
- Mild – you’re able to carry out everyday activities, such as work, studies or housework, but with difficulty; you may need to give up hobbies or social activities so you can rest in your spare time
- Moderate – you may have difficulty moving around easily and problems carrying out daily activities; you may not be able to work or continue with your education and may need to rest often; and you may also have problems sleeping at night
- Severe – you may only be able to do very basic daily tasks, such as brushing your teeth; you may be housebound or even bedbound and may need a wheelchair to get around; and you may also have difficulty concentrating, be sensitive to noise and light, and take a long time to recover after activities involving extra effort, such as leaving the house or talking for long periods
There may be times when your symptoms get worse. These periods are known as setbacks or relapses.
Sleep Problems
Patients with chronic fatigue syndrome often feel less refreshed and restored after sleep than they did before they became ill. Common sleep complaints include difficulty falling or staying asleep, extreme sleepiness, intense and vivid dreaming, restless legs, and nighttime muscle spasms.
Good sleep habits are important for all people, including those with chronic fatigue syndrome. Some common tips for good sleep are:
- Start a regular bedtime routine with a long, calming wind-down period.
- Go to bed at same time each night and wake up at same time each morning.
- Limit daytime naps to 30 minutes in total during the day.
- Remove all TVs, computers, phones, and gadgets from bedroom.
- Use the bed only for sleep and sex and not for other activities (avoid reading, watching TV, listening to music, or using phones).
- Control noise, light, and temperature.
- Avoid caffeine, alcohol, and large meals before bedtime.
- Avoid exercise right before going to bed. Light exercise and stretching earlier in the day, at least four hours before bedtime, might improve sleep.
When people try these techniques but are still unable to sleep, their doctor might recommend taking medicine to help with sleep. First, people should try over-the-counter sleep products. If this does not help, doctors can offer a prescription sleep medicine, starting at the smallest dose and using for the shortest possible time.
People might continue to feel unrefreshed even after the medications help them to get a full night of sleep. If so, they should consider seeing a sleep specialist. Most people with sleep disorders, like sleep apnea (brief pause in breathing during sleep) and narcolepsy (uncontrollable sleeping), respond to therapy. However, for people with chronic fatigue syndrome, not all symptoms may go away.
Pain
People with chronic fatigue syndrome often have deep pain in their muscles and joints. They might also have headaches (typically pressure-like) and soreness of their skin when touched.
Patients should always talk to their healthcare provider before trying any medication. Doctors may first recommend trying over-the-counter pain-relievers, like acetaminophen, aspirin, or ibuprofen. If these do not provide enough pain relief, patients may need to see a pain specialist. People with chronic pain, including those with chronic fatigue syndrome, can benefit from counseling to learn new ways to deal with pain.
Other pain management methods include stretching and movement therapies, gentle massage, heat, toning exercises, and water therapy for healing. Acupuncture, when done by a licensed practitioner, might help with pain for some patients.
Depression, Stress, and Anxiety
Adjusting to a chronic, debilitating illness sometimes leads to other problems, including depression, stress, and anxiety. Many patients with chronic fatigue syndrome develop depression during their illness. When present, depression or anxiety should be treated. Although treating depression or anxiety can be helpful, it is not a cure for chronic fatigue syndrome.
Some people with chronic fatigue syndrome might benefit from antidepressants and anti-anxiety medications. However, doctors should use caution in prescribing these medications. Some drugs used to treat depression have other effects that might worsen other chronic fatigue syndrome symptoms and cause side effects. When healthcare providers are concerned about patient’s psychological condition, they may recommend seeing a mental health professional.
Some people with chronic fatigue syndrome might benefit from trying techniques like deep breathing and muscle relaxation, massage, and movement therapies (such as stretching, yoga, and tai chi). These can reduce stress and anxiety, and promote a sense of well-being.
Dizziness and Lightheadedness (Orthostatic Intolerance)
Some people with chronic fatigue syndrome might also have symptoms of orthostatic intolerance that are triggered when-or made worse by-standing or sitting upright. These symptoms can include:
- Frequent dizziness and lightheadedness
- Changes in vision (blurred vision, seeing white or black spots)
- Weakness
- Feeling like your heart is beating too fast or too hard, fluttering, or skipping a beat
For patients with these symptoms, their doctor will check their heart rate and blood pressure, and may recommend they see a specialist, like a cardiologist or neurologist.
For people with chronic fatigue syndrome who do not have heart or blood vessel disease, doctor might suggest patients increase daily fluid and salt intake and use support stockings. If symptoms do not improve, prescription medication can be considered.
Memory and Concentration Problems
Memory aids, like organizers and calendars, can help with memory problems. For people with chronic fatigue syndrome who have concentration problems, some doctors have prescribed stimulant medications, like those typically used to treat Attention-Deficit / Hyperactivity Disorder (ADHD). While stimulants might help improve concentration for some patients with chronic fatigue syndrome, they might lead to the ‘push-and-crash’ cycle and worsen symptoms. “Push-and-crash” cycles are when someone with chronic fatigue syndrome is having a good day and tries to push to do more than they would normally attempt (do too much, crash, rest, start to feel a little better, do too much once again).
Chronic fatigue syndrome diagnosis
Chronic fatigue syndrome (myalgic encephalomyelitis) is a clinical diagnosis that can be made only when other causes of fatigue have been excluded 18. Specific diagnostic criteria for chronic fatigue syndrome/myalgic encephalomyelitis were developed by the Centers for Disease Control and Prevention (CDC) in 1988 19. During this time, it was theorized that viral illness was the primary etiology of chronic fatigue syndrome/myalgic encephalomyelitis; therefore, the criteria focused on physical symptoms. To parallel the World Health Organization categorization of chronic fatigue syndrome/myalgic encephalomyelitis as a neurologic disorder, the Oxford criteria were developed in 1991 (Table 1) 20. These criteria emphasize mental fatigue over physical symptoms 20. The CDC’s criteria were revised in 1994 to broaden the definition, and at this time, are the most widely accepted diagnostic criteria for chronic fatigue syndrome/myalgic encephalomyelitis (Table 2) 21.
Table 1. Oxford Criteria for Chronic Fatigue Syndrome
Primary symptom is fatigue | |
Definite onset of symptoms | |
Fatigue is severe, disabling, and affects physical and mental functioning | |
Symptoms for at least six months and present more than 50 percent of the time | |
Other symptoms must be present, particularly myalgia, and mood and sleep disturbances | |
Certain patients should be excluded: | |
| |
| |
Note: All criteria must be met to make the diagnosis.
Primary Symptoms of chronic fatigue syndrome/myalgic encephalomyelitis
Also called “core” symptoms, these occur in most patients with chronic fatigue syndrome/myalgic encephalomyelitis. The three primary symptoms required for diagnosis are 22:
- Greatly lowered ability to do activities that were usual before the illness. This drop in activity level occurs along with fatigue and must last six months or longer. People with ME/CFS have fatigue that is very different from just being tired. The fatigue of chronic fatigue syndrome/myalgic encephalomyelitis:
- Can be severe.
- Is not a result of unusually difficult activity.
- Is not relieved by sleep or rest.
- Was not a problem before becoming ill (not life-long).
- Worsening of chronic fatigue syndrome/myalgic encephalomyelitis symptoms after physical or mental activity that would not have caused a problem before illness. This is known as post-exertional malaise. People with chronic fatigue syndrome/myalgic encephalomyelitis often describe this experience as a “crash,” “relapse,” or “collapse.” It may take days, weeks, or longer to recover from a crash. Sometimes patients may be house-bound or even completely bed-bound during crashes. People with chronic fatigue syndrome/myalgic encephalomyelitis may not be able to predict what will cause a crash or how long it will last. As examples:
- Attending a child’s school event may leave someone house-bound for a couple of days and not able to do needed tasks, like laundry.
- Shopping at the grocery store may cause a physical crash that requires a nap in the car before driving home or a call for a ride home.
- Taking a shower may leave someone with severe chronic fatigue syndrome/myalgic encephalomyelitis bed-bound and unable to do anything for days.
- Sleep problems. People with chronic fatigue syndrome/myalgic encephalomyelitis may not feel better or less tired, even after a full night of sleep. Some people with chronic fatigue syndrome/myalgic encephalomyelitis may have problems falling asleep or staying asleep.
In addition to these core symptoms, one of the following two symptoms is required for diagnosis:
- Problems with thinking and memory. Most people with chronic fatigue syndrome/myalgic encephalomyelitis have trouble thinking quickly, remembering things, and paying attention to details. Patients often say they have “brain fog” to describe this problem because they feel “stuck in a fog” and not able to think clearly.
- Worsening of symptoms while standing or sitting upright. This is called orthostatic intolerance. People with chronic fatigue syndrome/myalgic encephalomyelitis may be lightheaded, dizzy, weak, or faint while standing or sitting up. They may have vision changes like blurring or seeing spots.
Table 2. Centers for Disease Control and Prevention Diagnostic Criteria for Chronic Fatigue Syndrome
Severe fatigue for longer than six months, and at least four of the following symptoms: | |
Headache of new type, pattern, or severity | |
Multijoint pain without swelling or erythema | |
Muscle pain | |
Postexertional malaise for longer than 24 hours | |
Significant impairment in short-term memory or concentration | |
Sore throat | |
Tender lymph nodes | |
Unrefreshing sleep | |
To diagnose myalgic encephalomyelitis/chronic fatigue syndrome, your doctor or healthcare provider will:
- Ask about your medical history and your family medical history
- Do a thorough physical and mental status examination focusing on identifying the most bothersome symptoms and red flag symptoms (Table 3) that may indicate a more serious underlying illness based on the National Institute for Health and Clinical Excellence (NICE) guidelines 23.
- Mental status examination, including evaluation for depression, is present in 39 to 47 percent of patients with chronic fatigue syndrome 24.
- Order blood, urine or other tests.
To get a better idea about your illness, the healthcare provider will ask many questions. Questions might include:
- What are you able to do now? How does it compare to what you were able to do before?
- How long have you felt this way?
- Do you feel better after sleeping or resting?
- What makes you feel worse? What helps you feel better?
- What happens when you try to push to do activities that are now hard for you?
- Are you able to think as clearly as you did before becoming ill?
- What symptoms keep you from doing what you need or want to do?
Table 3. Red Flag Symptoms in Persons with Suspected Chronic Fatigue Syndrome
| Red flags | Disease process indicated |
|---|---|
Chest pain | Cardiac disease |
Focal neurologic deficits | Central nervous system malignancy or abscess, multiple sclerosis |
Inflammatory signs or joint pain | Autoimmune disease (e.g., rheumatoid arthritis, systemic lupus erythematosus) |
Lymphadenopathy or weight loss | Malignancy |
Shortness of breath | Pulmonary disease |
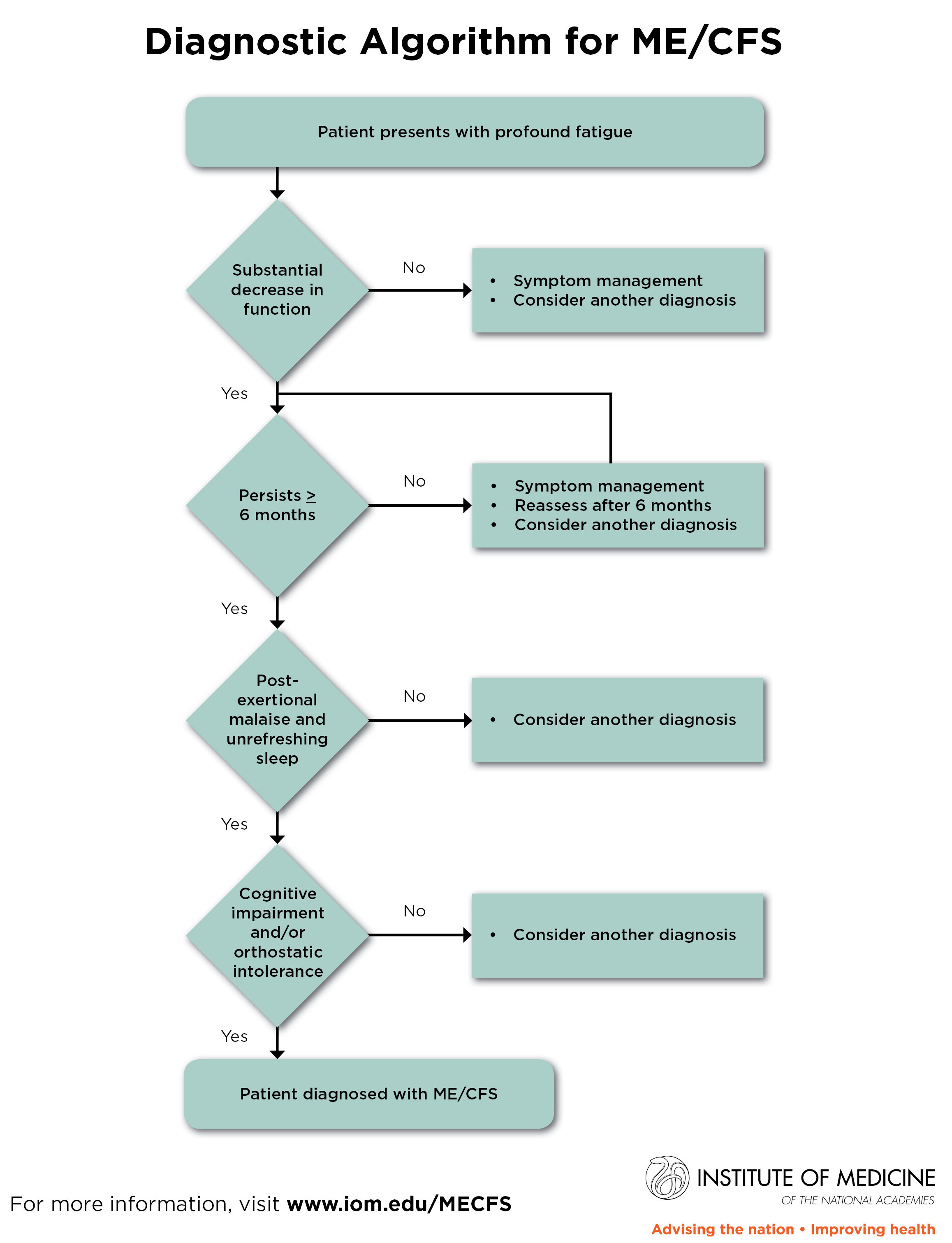
Figure 1. Diagnostic Algorithm for Chronic Fatigue Syndrome/Myalgic Encephalomyelitis
You may want to keep an activity journal. This could help you remember important details during your healthcare visit.
Doctors might refer you to see a specialist, like a neurologist, rheumatologist, or a sleep specialist, to check for other conditions that can cause similar symptoms. These specialists might find other conditions that could be treated. You can have other conditions and still have chronic fatigue syndrome. However, getting treatment for these conditions might help your condition, chronic fatigue syndrome, to feel better.
Although the differential diagnosis for patients presenting with chronic fatigue is broad (Table 4), approximately one-third meet the criteria for chronic fatigue syndrome 5. No laboratory tests can be used to diagnose chronic fatigue syndrome; instead, they are used to rule out other causes of fatigue that would preclude the diagnosis of chronic fatigue syndrome. The CDC 21 and NICE 23 recommend a minimal set of tests for patients presenting with chronic fatigue.
- The CDC recommends initial evaluation with urinalysis; complete blood count; comprehensive metabolic panel; and measurement of phosphorus, thyroid-stimulating hormone, and C-reactive protein 21.
- NICE also recommends using immunoglobulin A endomysial antibodies to screen for celiac disease, and if indicated by the history or physical examination, urine drug screening, rheumatoid factor testing, and antinuclear antibody testing 23. Viral titers are not recommended unless the patient’s history is suggestive of an infectious process, because they do not confirm or eliminate the diagnosis of Chronic Fatigue Syndrome.
Table 4. Differential Diagnosis of Chronic Fatigue
Endocrine | |
Addison disease | |
Adrenal insufficiency | |
Cushing disease | |
Diabetes mellitus | |
Hyperthyroidism | |
Hypothyroidism | |
Hematologic/oncologic | |
Anemia | |
Malignancy | |
Infectious | |
Chronic hepatitis | |
Human immunodeficiency virus | |
Lyme disease | |
Tuberculosis | |
Neurologic | |
Dementia | |
Multiple sclerosis | |
Narcolepsy | |
Parkinson disease | |
Psychiatric | |
Bipolar disorder | |
Eating disorder | |
Major depressive disorder | |
Schizophrenia | |
Somatoform disorders | |
Substance abuse | |
Rheumatologic | |
Dermatomyositis | |
Fibromyalgia | |
Polymyalgia rheumatica | |
Polymyositis | |
Rheumatoid arthritis | |
Sjögren syndrome | |
Systemic lupus erythematosus | |
Temporal arteritis | |
Other | |
Celiac disease | |
Heart failure | |
Heavy metal toxicity | |
Pharmacologic adverse effect | |
Sleep apnea | |
Vitamin deficiency | |
Chronic fatigue syndrome treatment
There is no cure for chronic fatigue syndrome. Most people with chronic fatigue syndrome get better over time, although some people don’t make a full recovery. It’s also likely there will be periods when your symptoms get better or worse. Children and young people with chronic fatigue syndrome are more likely to recover fully.
Treatment focuses on symptom relief including sleep disturbances, depression, and pain.
Patients are encouraged to take rest periods as necessary, and to practice relaxation techniques. Although there is no evidence these modalities are effective, they are unlikely to be harmful and may be helpful 25. There is substantial evidence for two treatments for chronic fatigue syndrome: cognitive behavior therapy (CBT) and graded exercise therapy. There is less clear evidence regarding the benefit of drug therapy for chronic fatigue syndrome in patients without comorbid depression or anxiety disorders.
Therapy
The most effective treatment for chronic fatigue syndrome appears to be a two-pronged approach that combines cognitive training with a gentle exercise program.
- Cognitive behavior therapy (CBT). Talking with a counselor can help you figure out options to work around some of the limitations that chronic fatigue syndrome imposes on you. Feeling more in control of your life can improve your outlook dramatically.
- Graded exercise therapy. A physical therapist can help determine what exercises are best for you. Inactive people often begin with range-of-motion and stretching exercises for just a few minutes a day. Gradually increasing the intensity of your exercise over time may help reduce your hypersensitivity to exercise, just like allergy shots gradually reduce a person’s hypersensitivity to a particular allergen.
Despite the positive results with cognitive behavior therapy (CBT) and graded exercise therapy, the effects are usually moderate and rarely lead to resolution of chronic fatigue syndrome. Patients with poor social adjustment, a strong belief in an organic cause for fatigue, or some sort of sickness benefit (i.e., financial incentive) tend to have worse responses to therapy 13. Unlike with many other illnesses, membership in a chronic fatigue syndrome support group was associated with worse outcomes 26.
Cognitive behavior therapy (CBT)
Trained psychotherapists providing cognitive behavior therapy (CBT) emphasize the role of thinking and its impact on how persons feel and act. They can help persons with chronic fatigue syndrome recognize how their fears of activity lead to behaviors that ultimately cause them to feel more fatigued and disabled. A large randomized controlled trial in adults with chronic fatigue syndrome confirmed that cognitive behavior therapy has positive effects on fatigue levels, work and social adjustment, depression, anxiety, and postexertional malaise. Most patients in this study rated themselves as “much” or “very much” better after completion 27.
A 2008 Cochrane review also supported the use of cognitive behavior therapy for chronic fatigue syndrome 28. Several other studies have shown similar results 29, 30, including in adolescents with chronic fatigue syndrome 31. One study found fewer school absences and improvements in fatigue and overall physical functioning in adolescents being treated with Internet-based cognitive behavior therapy 32. Cognitive behavior therapy has been studied in group settings 33 and in the form of self-guided instruction 34, with questionable effectiveness. Because of this, it is recommended that cognitive behavior therapy be individualized to maximize benefit 23. Disadvantages of cognitive behavior therapy include the need for expert consultation, time considerations, and cost. There are no data to suggest that cognitive behavior therapy provided by trained family physicians is better or worse than cognitive behavior therapy provided by psychotherapists.
Graded exercise therapy
Graded exercise therapy involves a gradual increase in physical activity in the hopes of increasing function. A randomized trial found that graded exercise therapy was as effective as cognitive behavior therapy (CBT) for fatigue and the other aspects of functional impairment mentioned previously, except depression 27. Participants in this trial were encouraged to gradually increase the duration of their physical activity over 52 weeks to a final goal of 30 minutes of light exercise five days per week, taking caution not to exceed a target heart rate to avoid overexertion. Most patients chose to walk for exercise. Once this goal was achieved, the patients worked with the supervising physiotherapists monthly to increase the intensity of their aerobic exercise.
Several other studies have found consistent results 35, 36, 37. There is some evidence that the benefits of graded exercise therapy do not correlate with increases in exercise capacity, suggesting that the benefits of graded exercise therapy, like cognitive behavior therapy (CBT), have more to do with decreasing symptom-focusing behavior in persons with chronic fatigue syndrome 38. Impediments to graded exercise therapy include time considerations and concerns from patients that exercise will exacerbate their condition.
Medications
Many people who have chronic fatigue syndrome are also depressed. Treating your depression can make it easier for you to cope with the problems associated with chronic fatigue syndrome. Low doses of some antidepressants also can help improve sleep and relieve pain.
There is no good evidence to support the use of antiviral medications, hydrocortisone, or fludrocortisone; only small or poorly designed studies exist 8, 39, 40.
One study showed some clinical improvement in chronic fatigue syndrome after treatment with staphylococcus toxoid 41; the authors theorized that the treatment stimulated the hypoactive immune systems of persons with chronic fatigue syndrome and subsequently improved their fatigue. However, the treatment needed to be continued to prevent relapse of symptoms. Staphylococcus toxoid is not widely available and cannot currently be recommended as a treatment for chronic fatigue syndrome 41.
Other treatments that did not improve chronic fatigue syndrome symptoms in clinical trials include methylphenidate 42, melatonin 15, citalopram (Celexa; used in patients without depression) 43 and galantamine (Razadyne) 44. More research is needed to clarify the cause of chronic fatigue syndrome to better target potential treatments.
Alternative medicine
Many alternative therapies have been promoted for chronic fatigue syndrome. It’s difficult to determine whether these therapies actually work, partly because the symptoms of chronic fatigue syndrome often respond to placebos.
Complementary therapies, like acupuncture, meditation, gentle massage, deep breathing, relaxation therapy, yoga, or tai chi, might be helpful to increase energy and decrease pain.
Coping and support
The experience of chronic fatigue syndrome varies from person to person. Emotional support and counseling may help you and your loved ones deal with the uncertainties and restrictions of this disorder.
You may find it therapeutic to join a support group and meet other people with chronic fatigue syndrome. Support groups aren’t for everyone, and you may find that a support group adds to your stress rather than relieves it. Experiment and use your own judgment to determine what’s best for you.
Chronic fatigue syndrome diet
It’s important you eat regularly and have a healthy, balanced diet. You should be offered practical advice about how to achieve this if, for example, your chronic fatigue syndrome symptoms are making it difficult for you to shop or prepare food.
Eating a healthy, balanced diet is an important part of maintaining good health, and can help you feel your best.
This means eating a wide variety of foods in the right proportions, and consuming the right amount of food and drink to achieve and maintain a healthy body weight.
If you feel sick (nauseous), eating starchy foods, eating little and often, and sipping drinks slowly may help. If this doesn’t work, medication can be prescribed.
Effective dietary changes, including effective communication and implementation of dietary interventions tailored to meet the needs of the chronic fatigue syndrome population, have not yet been substantiated within this review 45. Individualised clinical recommendations still need to focus on evidence-based advice and dietary counselling, alongside general promotion of healthy eating habits across all medically tolerable food groups to also reduce other chronic disease risks and avoid development of deficiencies 46, 47.
Diets that exclude certain food types aren’t recommended for people with chronic fatigue syndrome. There’s also insufficient evidence to recommend supplements, such as vitamin B12, vitamin C, magnesium, or co-enzyme Q10.
It is hoped that further research will focus on strengthening the level of evidence contributing to future research in this area to clarify and consolidate recommendations as well as ensure the distribution of accurate and useful information at a population level.
Dietary interventions and chronic fatigue syndrome symptom alleviation
Only one eligible study assessed a dietary intervention with reference to chronic fatigue syndrome symptoms alleviation 48. The experiment applied a 24-week intervention of a low-sugar low-yeast diet (LSLY), with intention to treat analysis showing no statistically significant difference for the intervention and guideline based healthy eating control between the primary outcome measures 48. Compliance was poor, and compliant analysis was performed only on baseline characteristics comparing those who completed their role in the experiment and those that did not 48.
Experimental low-sugar low-yeast diet (LSLY) dietary intervention was inconclusive. Although bias from poor compliance must be considered when interpreting these findings, compliance was not analysed against the measured outcome scores. Other reasons for such a finding may be potentially due to lack of power masking a result 48. The results may have been clouded from the beginning as the studies hypothesis relied on dietary treatment of a suggested cause of chronic fatigue syndrome. Both the suggested cause and use of dietary modification for this suggested cause (LSLY diet) lacked any supporting scientific data, are controversial, and to date have not been linked directly to chronic fatigue syndrome 48.
Animal studies and polyphenols
Three animal studies were included examining the effect of differing polyphenols and their impact on induced chronic fatigue syndrome symptoms in mice or rats 49, 50. These polyphenols included astragalus membranaceus flavonoids, epigallocatechin gallate (EGCG) and naringin.
The effect of astragalus membranaceus flavonoids oral administration in rats highlighted statistically significant increases in endurance through forced swimming compared to rats not administered with astragalus membranaceus flavonoids in the chronically fatigued groups 49. Spleen cell proliferation was statistically significantly increased with astragalus membranaceus flavonoids supplementation as well as abnormal cytokine production levels being regulated in chronically fatigued groups 49.
Daily epigallocatechin gallate (EGCG) oral administration highlighted a significant increase in endurance capacity during forced swimming and decreased post-swim fatigue levels compared to the chronic fatigue rat group at 28 days 50. Greater endurance and decreased post-fatigue levels were displayed with the administration of 100 mg/kg compared to 50 mg/kg 49. Use of epigallocatechin gallate (EGCG) prevented reductions in body weight and restored spleen and thymus induced hypotrophy compared to the chronic fatigue rat group, with significantly greater prevention of body weight reduction and spleen hypertrophy restoration using 100 mg/kg dose verse 50 mg/kg dose 49. In an elevated plus maze learning task, administration of epigallocatechin gallate (EGCG) decreased initial transfer latency compared to the chronic fatigued group 50. Use of an oral dose of epigallocatechin gallate (EGCG) also showed favourable statistically significant changes in measures of oxidative and nitrosative stress and pro-inflammatory cytokine levels, factors that may contribute to fatigue development 51.
For the polyphenol naringin, differing oral doses were administered to mice treated with lipopolysaccharide (LPS) or brucella abortus (BA) antigen, which induced immunological fatigue 51. Naringin use showed a statistically significant and dose-dependent decrease in the duration of immobility in immunologically induced fatigued mice and a significant increase in mean tail withdrawal latency compared to BA or LPS injected mice 51. A statistically significant dose dependant increase in reduced glutathione levels was also seen through naringin administration compared to BA or LPS injected mice 51. Again, as seen with use of the other polyphenols, statistically significant favourable changes in measures of oxidative and nitrosative stress and a pro-inflammatory cytokine were highlighted 51.
The included animal studies set a good platform for further human studies to be conducted in these areas of interest, with some encouraging significant results highlighted through polyphenol use in mice or rats displaying induced fatigue. Further studies in humans should consider supplementation of these isolated polyphenol compounds, as the results highlighted are unlikely to be obtained through normal dietary intake, for example, to obtain the effects seen from naringin around 50–200 mg/kg was administered 51. Mean values of several fruit varieties high in naringin, including red grapefruit, blond grapefruit and sweetie fruit, showed around 50 mg/100 g of fresh weight from fruit identified, further impeded by its bioavailability in the food matrix 52.
Dietary intake and poor vitamin or mineral status and chronic fatigue syndrome
Dietary intake patterns and poor vitamin or mineral status were not found to be associated with symptoms alleviation in the observational studies reviewed 46, 53, 54, 55. Some important trends were found within these studies. One study notably observed in their selected chronic fatigue syndrome cohort that almost half of the dietary exclusions were made based on information from practitioners of alternative therapy or experience 46.
One study considered the vitamin status and direct association of chronic fatigue syndrome symptoms alleviation. The analytical observational study examined mean serum 25 OH vitamin D levels. Levels were highlighted to be moderately to severely suboptimal in chronic fatigue syndrome participants at 60.1% for those not taking supplements. This finding was statistically significantly lower over winter/spring and summer/autumn compared to the general population control study arm 53, yet no observed relationship for alleviation of symptoms of chronic fatigue syndrome was seen 53
Very little correlation of abnormal biomarkers with inadequate nutritional intake in chronic fatigue syndrome patients was displayed in another descriptive observational study 55. The findings continued in a consistent manner, highlighting through an analytical observational study that 95% had poor fiber intake and 70% had unhealthy fat, fruit, and vegetable intake measured through defined cut off limits from questionnaire assessment tools 56. Yet, lifestyle factors including overweight and unhealthy dietary intake were not significantly associated with fatigue severity or functional impairment 56.
Those following this advice tended to have higher vitamin supplement intake, which may be detrimental, as discussed by Mursu et al. 57, who noted that vitamin and mineral supplements increased total mortality risk in a cohort of generally healthy women with a mean age of 60 years 57. Although this study displays a low level of evidence and had many limitations 46, these trends regarding food avoidance and its influence on the diets of those with chronic fatigue syndrome are important to note for research and clinical practice to ensure the information being distributed and followed within chronic fatigue syndrome populations is correct and has a sound evidence base. Some supplementation recommendations were highlighted in light of other findings. Due to the nature of chronic fatigue syndrome with increased indoor dwelling, potential increased osteoporosis risk, and significantly lower mean serum 25-OH vitamin D, vitamin D intake through the diet and supplements should be considered for general health, regardless of the study findings 53. The risk of chronic vitamin D deficiency mimicking chronic fatigue syndrome symptoms is also noted in two studies 53, 55. One study continues, suggesting that an underlying pathological process may be responsible for abnormal biomarkers that showed very little correlation with inadequate nutritional intake 55, an explanation that may also explain lifestyle factors of weight and dietary intake not significantly correlating with chronic fatigue syndrome symptoms.
Tryptophan and glutamine amino acids and chronic fatigue syndrome
The amino acid tryptophan (Trp) and its potential role in chronic fatigue syndrome symptoms expression was examined in two studies 58, 59. Within one, the selected chronic fatigue syndrome cohort displayed a significantly higher mean free (48%) and total tryptophan (Trp) (19%) 58. Serum free Trp to competing amino acids (CAA) ratio was significantly higher (43%) in the chronic fatigue syndrome cohort and the serum total Trp to CAA ratio was only significantly higher when co-varied with age and gender. Non-esterified fatty acid (NEFA) levels were significantly higher in the chronic fatigue syndrome cohort, as was serum glucose (p=0.0058) and a slightly higher albumin concentration was also seen in the CFS cohort. Total CAA concentration though was not significantly different between the healthy control cohort and CFS cohort 58. Within chronic fatigue syndrome participants if suggested serotonin parameters are applied there was a significant division in this cohort between those with high or normal serotonin status shown in free Trp and total Trp to competing amino acids (CAA) ratio and free Trp to competing amino acids (CAA) ratio.
Within the second study, the amino acid blood sample findings were related to the research question 59. These findings highlighted baseline free Trp was significantly lower in the chronic fatigue syndrome cohort with no difference seen in neutral amino acid (NAA) concentration between the two groups. Although lowered, there was no significant difference between groups for serum free Trp to NAA ratio and there was no difference for total Trp between the groups 59.
For the amino acid glutamine, the one experimental study revealed baseline measurements of participants with CFS had significantly lower mean plasma and muscle glutamine concentrations 60. Post-trial outcomes for those with chronic fatigue syndrome in the intervention group receiving a glutamine supplement highlighted there was a significant increase in plasma and muscle glutamine concentration. Those with chronic fatigue syndrome in the placebo group saw no significant increase in plasma or muscle glutamine concentrations 60. Although supplementation increased stores of glutamine for chronic fatigue syndrome participants, those with chronic fatigue syndrome in the intervention group showed no statistically significant change in their five category questionnaire scores assessing symptoms, whereas chronic fatigue syndrome participants in the placebo group showed a significant decrease in the two categories of emotionality and sleep problems 60. Grouping chronic fatigue syndrome participants to show clinical improvement or no clinical improvement displayed both the intervention and control groups in each category 60.
The chronic fatigue syndrome participants in the group that showed no clinical improvement did display significant increases in mean plasma glutamine concentration post trial as well as increases in their T-cell counts, T-helper cells and a decrease in natural killer cell counts and activated T-cells 60. These outcomes oppose the reported baseline measures in the initial assessment, yet were not seen in the group that displayed clinical improvement.
Findings again were inconsistent for those studies examining the role of tryptophan and glutamine amino acids and chronic fatigue syndrome 58. Chronic fatigue syndrome participants displayed a significantly higher serum free Trp to CAA ratio with increased Trp available to the brain, highlighting an excess of central serotonin by one analytic observational study 58. However, this was only due to higher serum free Trp as competing amino acids (CAA) concentration was not different between the two groups. Unfortunately, some of the chronic fatigue syndrome cohort had not fasted and this confounder significantly increased the concentration level of serum free Trp, hence affecting the validity of the serum free Trp to CAA ratio. In light of this result, conflicting findings are understood from another included analytical observational study 59. This data highlights potential implications for the management of chronic fatigue syndrome, proposing that chronic fatigue syndrome patients may be divided into sub-groups of those with normal or those with high serotonin status 58. It must be noted that within Vassallo et al. 59 observational study, the amino acid level investigation and results observed were reviewed, yet the other sub-sectors of this study were not relevant to the research question, having largely a neuroendocrine focus.
Glutamine amino acids findings showed experimentally that a chronic fatigue syndrome cohort at baseline displayed significantly lower mean plasma and muscle glutamine concentration, yet it is stated this is likely because of four participants’ low values 60. Post-trial outcomes show those with chronic fatigue syndrome in the intervention group saw a significant increase in plasma and muscle glutamine concentration as compared to chronic fatigue syndrome participants in the placebo group who saw no significant increases. This indicates the effectiveness of glutamine supplementation in increasing the body’s supply of the amino acid.
Inconsistent results were highlighted, however, with use of categorisation of chronic fatigue syndrome participants into clinical improvement or no clinical improvement groupings, with a statistically significant increase for those who did not show clinical improvement post-trial in mean plasma glutamine concentration. It is proposed that a rise in only plasma glutamine for this group indicates an issue of glutamine regulation rather than decreased availability of glutamine in those with chronic fatigue syndrome.
Overall, glutamine supplementation increased body supplies of glutamine but demonstrated inconsistent effects on reported symptoms or clinical improvement.
Phosphate diabetes and consideration of differential diagnosis to chronic fatigue syndrome
Mean serum phosphate concentration was outlined to be significantly lower in the chronic fatigue syndrome cohort, but still within reference range in the single included analytical observational study 61. Fourteen per cent of participants in the chronic fatigue syndrome cohort fulfilled diagnostic criteria for phosphate diabetes (PD), yet did not show a significant difference in symptoms when compared to those with chronic fatigue syndrome without a phosphate diabetes diagnosis. No statistically significant difference was seen between the intervention and control for mean overall values such as phosphate clearance, mean renal threshold phosphate concentration (TmPO4/GFR) and mean phosphate tubular re-absorption (PTR) rate values 61.
Phosphate diabetes chronic fatigue syndrome cohort findings were contradictory and although still within reference range, the chronic fatigue syndrome group did display a significantly lower mean serum phosphate concentration in the included analytical observational study 61. Fourteen per cent of the chronic fatigue syndrome cohort met the phosphate diabetes diagnostic criteria, whereas no one in the healthy control group met the diagnostic criteria. Further studies should rule out the need for consideration of phosphate diabetes upon clinical presentation of chronic fatigue syndrome symptoms to ensure the diagnosis and management are correct.
- Chronic fatigue syndrome. Mayoclinic. https://www.mayoclinic.org/diseases-conditions/chronic-fatigue-syndrome/symptoms-causes/syc-20360490[↩]
- Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. https://www.cdc.gov/me-cfs/about/index.html[↩][↩]
- Reeves WC, Jones JF, Maloney E, et al. Prevalence of chronic fatigue syndrome in metropolitan, urban, and rural Georgia. Popul Health Metr. 2007;5:5.[↩]
- Bierl C, Nisenbaum R, Hoaglin DC, et al. Regional distribution of fatiguing illnesses in the United States: a pilot study. Popul Health Metr. 2004;2(1):1[↩]
- Darbishire L, Ridsdale L, Seed PT. Distinguishing patients with chronic fatigue from those with chronic fatigue syndrome: a diagnostic study in UK primary care. Br J Gen Pract. 2003;53(491):441–445.[↩][↩]
- Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness. http://nationalacademies.org/hmd/reports/2015/me-cfs.aspx[↩]
- Cevik R, Gur A, Acar S, Nas K, Sarac AJ. Hypothalamic-pituitary-gonadal axis hormones and cortisol in both menstrual phases of women with chronic fatigue syndrome and effect of depressive mood on these hormones. BMC Musculoskelet Disord. 2004;5:47.[↩]
- Cleare AJ, Miell J, Heap E, et al. Hypothalamo-pituitary-adrenal axis dysfunction in chronic fatigue syndrome, and the effects of low-dose hydrocortisone therapy. J Clin Endocrinol Metab. 2001;86(8):3545–3554.[↩][↩]
- Whistler T, Jones JF, Unger ER, Vernon SD. Exercise responsive genes measured in peripheral blood of women with chronic fatigue syndrome and matched control subjects. BMC Physiol. 2005;5(1):5.[↩]
- Zhang L, Gough J, Christmas D, et al. Microbial infections in eight genomic subtypes of chronic fatigue syndrome/myalgic encephalomyelitis. J Clin Pathol. 2010;63(2):156–164.[↩]
- Heim C, Nater UM, Maloney E, Boneva R, Jones JF, Reeves WC. Childhood trauma and risk for chronic fatigue syndrome: association with neuroendocrine dysfunction. Arch Gen Psychiatry. 2009;66(1):72–80.[↩]
- Prins JB, Bos E, Huibers MJ, et al. Social support and the persistence of complaints in chronic fatigue syndrome. Psychother Psychosom. 2004;73(3):174–182.[↩]
- Chalder T, Godfrey E, Ridsdale L, King M, Wessely S. Predictors of outcome in a fatigued population in primary care following a randomized controlled trial. Psychol Med. 2003;33(2):283–287.[↩][↩]
- van Heukelom RO, Prins JB, Smits MG, Bleijenberg G. Influence of melatonin on fatigue severity in patients with chronic fatigue syndrome and late melatonin secretion. Eur J Neurol. 2006;13(1):55–60.[↩]
- Williams G, Waterhouse J, Mugarza J, Minors D, Hayden K. Therapy of circadian rhythm disorders in chronic fatigue syndrome: no symptomatic improvement with melatonin or phototherapy. Eur J Clin Invest. 2002;32(11):831–837.[↩][↩]
- Maes M, Mihaylova I, Leunis JC. In chronic fatigue syndrome, the decreased levels of omega-3 poly-unsaturated fatty acids are related to lowered serum zinc and defects in T cell activation. Neuro Endocrinol Lett. 2005;26(6):745–751.[↩]
- Brouwers FM, Van Der Werf S, Bleijenberg G, Van Der Zee L, Van Der Meer JW. The effect of a polynutrient supplement on fatigue and physical activity of patients with chronic fatigue syndrome: a double-blind randomized controlled trial. QJM. 2002;95(10):677–683.[↩]
- Chronic Fatigue Syndrome: Diagnosis and Treatment. Am Fam Physician. 2012 Oct 15;86(8):741-746. https://www.aafp.org/afp/2012/1015/p741.html[↩]
- Reyes M, Gary HE Jr, Dobbins JG, et al. Surveillance for chronic fatigue syndrome—four U.S. cities, September 1989 though August 1993. MMWR CDC Surveill Summ. 1997;46(2):1–13.[↩]
- Sharpe MC, Archard LC, Banatvala JE, et al. A report–chronic fatigue syndrome: guidelines for research. J R Soc Med. 1991;84(2):118–121.[↩][↩][↩]
- Fukuda K, Straus SE, Hickie I, Sharpe MC, Dobbins JG, Komaroff A; International Chronic Fatigue Syndrome Study Group. The chronic fatigue syndrome: a comprehensive approach to its definition and study. Ann Intern Med. 1994;121(12):953–959.[↩][↩][↩][↩]
- Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. https://www.cdc.gov/me-cfs/symptoms-diagnosis/symptoms.html[↩]
- National Collaborating Centre for Primary Care (Great Britain), Royal College of General Practitioners. Chronic Fatigue Syndrome/Myalgic Encephalomyelitis (or Encephalopathy): Diagnosis and Management of Chronic Fatigue Syndrome/Myalgic Encephalomyelitis (or Encephalopathy) in Adults and Children. London, England: National Collaborating Centre for Primary Care, Royal College of General Practitioners; 2007.[↩][↩][↩][↩][↩]
- Wilson A, Hickie I, Hadzi-Pavlovic D, et al. What is chronic fatigue syndrome? Heterogeneity within an international multicentre study. Aust N Z J Psychiatry. 2001;35(4):520–527.[↩]
- NatMost people with CFS get better over time, although some people don’t make a full recovery. It’s also likely there will be periods when your symptoms get better or worse. Children and young people with CFS/ME are more likely to recover fully.ional Collaborating Centre for Primary Care (Great Britain), Royal College of General Practitioners. Chronic Fatigue Syndrome/Myalgic Encephalomyelitis (or Encephalopathy): Diagnosis and Management of Chronic Fatigue Syndrome/Myalgic Encephalomyelitis (or Encephalopathy) in Adults and Children. London, England: National Collaborating Centre for Primary Care, Royal College of General Practitioners; 2007.[↩]
- Bentall RP, Powell P, Nye FJ, Edwards RH. Predictors of response to treatment for chronic fatigue syndrome. Br J Psychiatry. 2002;181:248–252.[↩]
- White PD, Goldsmith KA, Johnson AL, PACE trial management group, et al. Comparison of adaptive pacing therapy, cognitive behaviour therapy, graded exercise therapy, and specialist medical care for chronic fatigue syndrome (PACE): a randomised trial. Lancet. 2011;377(9768):823–836.[↩][↩]
- Price JR, Mitchell E, Tidy E, Hunot V. Cognitive behaviour therapy for chronic fatigue syndrome in adults. Cochrane Database Syst Rev. 2008(3):CD001027.[↩]
- O’Dowd H, Gladwell P, Rogers CA, Hollinghurst S,( Gregory A. Cognitive behavioural therapy in chronic fatigue syndrome: a randomised controlled trial of an outpatient group programme. Health Technol Assess. 2006; 10(37):iii–iv, ix–x, 1–121.[↩]
- Deale A, Husain K, Chalder T, Wessely S. Long-term outcome of cognitive behavior therapy versus relaxation therapy for chronic fatigue syndrome: a 5-year follow-up study. Am J Psychiatry. 2001;158(12):2038–2042.[↩]
- Stulemeijer M, de Jong LW, Fiselier TJ, Hoogveld SW, Bleijenberg G. Cognitive behaviour therapy for adolescents with chronic fatigue syndrome: randomised controlled trial [published correction appears in BMJ. 2005;330(7495):820]. BMJ. 2005;330(7481):14–21.[↩]
- Nijhof SL, Bleijenberg G, Uiterwaal CS, Kimpen JL, van de Putte EM. Effectiveness of internet-based cognitive behavioural treatment for adolescents with chronic fatigue syndrome (FITNET): a randomized controlled trial. Lancet. 2012;379(9824):1412–1418.[↩]
- Bazelmans E, Prins JB, Lulofs R, van der Meer JW, Bleijenberg G; Netherlands Fatigue Research Group Nijmegen. Cognitive behaviour group therapy for chronic fatigue syndrome: a non-randomised waiting list controlled study. Psychother Psychosom. 2005;74(4):218–224.[↩]
- Knoop H, van der Meer JW, Bleijenberg G. Guided self-instructions for people with chronic fatigue syndrome: randomised controlled trial. Br J Psychiatry. 2008;193(4):340–341.[↩]
- Powell P, Bentall RP, Nye FJ, Edwards RH. Patient education to encourage graded exercise in chronic fatigue syndrome: 2-year follow-up of randomised controlled trial. Br J Psychiatry. 2004;184:142–146.[↩]
- Moss-Morris R, Sharon C, Tobin R, Baldi JC. A randomized controlled graded exercise trial for chronic fatigue syndrome: outcomes and mechanisms of change. J Health Psychol. 2005;10(2):245–259.[↩]
- Wallman KE, Morton AR, Goodman C, Grove R, Guilfoyle AM. Randomised controlled trial of graded exercise in chronic fatigue syndrome. Med J Aust. 2004;180(9):444–448.[↩]
- Pardaens K, Haagdorens L, Van Wambeke P, Van den Broeck A, Van Houdenhove B. How relevant are exercise capacity measures for evaluating treatment effects in chronic fatigue syndrome? Results from a prospective, multidisciplinary outcome study. Clin Rehabil. 2006;20(1):56–66.[↩]
- Kogelnik AM, Loomis K, Hoegh-Petersen M, Rosso F, Hischier C, Montoya JG. Use of valganciclovir in patients with elevated antibody titers against human herpesvirus-6 (HHV-6) and Epstein-Barr virus (EBV) who were experiencing central nervous system dysfunction including long-standing fatigue. J Clin Virol. 2006;37(suppl 1):S33–S38.[↩]
- Blockmans D, Persoons P, Van Houdenhove B, Lejeune M, Bobbaers H. Combination therapy with hydrocortisone and fludrocortisone does not improve symptoms in chronic fatigue syndrome: a randomized, placebo-controlled, double-blind, crossover study. Am J Med. 2003;114(9):736–741.[↩]
- Zachrisson O, Regland B, Jahreskog M, Jonsson M, Kron M, Gottfries CG. Treatment with staphylococcus toxoid in fibromyalgia/chronic fatigue syndrome–a randomised controlled trial. Eur J Pain. 2002;6(6):455–466.[↩][↩]
- Blockmans D, Persoons P, Van Houdenhove B, Bobbaers H. Does methylphenidate reduce the symptoms of chronic fatigue syndrome? Am J Med. 2006;119(2):167.e23–167.e30.[↩]
- Hartz AJ, Bentler SE, Brake KA, Kelly MW. The effectiveness of citalopram for idiopathic chronic fatigue. J Clin Psychiatry. 2003;64(8):927–935.[↩]
- Blacker CV, Greenwood DT, Wesnes KA, et al. Effect of galantamine hydrobromide in chronic fatigue syndrome: a randomized controlled trial. JAMA. 2004;292(10):1195–1204.[↩]
- Jones, K. and Probst, Y. (2017), Role of dietary modification in alleviating chronic fatigue syndrome symptoms: a systematic review. Australian and New Zealand Journal of Public Health, 41: 338–344. doi:10.1111/1753-6405.12670 http://onlinelibrary.wiley.com/doi/10.1111/1753-6405.12670/full[↩]
- Trabal J, Leyes P, Fernández-Solá J, Forga M, Fernández-Huerta J. Patterns of food avoidance in chronic fatigue syndrome: Is there a case for dietary recommendations? Nutr Hosp. 2012; 27(2): 659–62. https://www.ncbi.nlm.nih.gov/pubmed/22732998[↩][↩][↩][↩]
- National Health and Medical Research Council. Australian Dietary Guidelines. Canberra (AUST): Government of Australia; 2013.[↩]
- Hobday RA, Thomas S, O’Donovan A, Murphy M, Pinching AJ. Dietary intervention in chronic fatigue syndrome. J Hum Nutr Diet. 2008; 21(2): 141–9. https://www.ncbi.nlm.nih.gov/pubmed/18339054[↩][↩][↩][↩][↩]
- Kuo YH, Tsai WJ, Loke SH, Wu TS, Chiou WF. Astragalus membranaceus flavonoids (AMF) ameliorate chronic fatigue syndrome induced by food intake restriction plus forced swimming. J Ethnopharmacol. 2009; 122(1): 28–34. https://www.ncbi.nlm.nih.gov/pubmed/19103273[↩][↩][↩][↩][↩]
- Sachdeva AK, Kuhad A, Chopra K. Epigallocatechin gallate ameliorates behavioral and biochemical deficits in rat model of load-induced chronic fatigue syndrome. Brain Res Bull. 2011; 86 (3–4): 165–72. https://www.ncbi.nlm.nih.gov/pubmed/21821105[↩][↩][↩]
- Vij G, Gupta A, Chopra K. Modulation of antigen-induced chronic fatigue in mouse model of water immersion stress by naringin, a polyphenolic antioxidant. Fundam Clin Pharmacol. 2009; 23(3): 331–7. https://www.ncbi.nlm.nih.gov/pubmed/19469804[↩][↩][↩][↩][↩][↩]
- Gorinstein S, Huang D, Leontowicz H, Leontowicz M, Yamamoto K, Soliva-Fortuny R, et al. Determination of naringin and hesperidin in citrus fruit by high-performance liquid chromatography, the antioxidant potential of citrus fruit. Acta Chromatogr 2006(17): 108–24.[↩]
- Berkovitz S, Ambler G, Jenkins M, Thurgood S. Serum 25-hydroxy vitamin D levels in chronic fatigue syndrome: A retrospective survey. Int J Vitam Nutr Res. 2009; 79(4): 250–4. https://www.ncbi.nlm.nih.gov/pubmed/20209476[↩][↩][↩][↩][↩]
- Goedendorp MM, Knoop H, Schippers GM, Bleijenberg G. The lifestyle of patients with chronic fatigue syndrome and the effect on fatigue and functional impairments. J Hum Nutr Diet. 2009; 22: 226–31. https://www.ncbi.nlm.nih.gov/pubmed/19226353[↩]
- Jenkins M, Rayman M. Nutrient intake is unrelated to nutrient status in patients with chronic fatigue syndrome. J Nutr Environ Med. 2005; 15(4): 177–89.[↩][↩][↩][↩]
- Goedendorp MM, Knoop H, Schippers GM, Bleijenberg G. The lifestyle of patients with chronic fatigue syndrome and the effect on fatigue and functional impairments. J Hum Nutr Diet. 2009; 22: 226–31. www.ncbi.nlm.nih.gov/pubmed/19226353[↩][↩]
- Mursu J, Robien K, Harnack LJ, Park K, Jacobs JDR. Dietary supplements and mortality rate in older women: The Iowa women’s health study. Arch Intern Med. 2011; 171(18): 1625–33. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4114071/[↩][↩]
- Badawy AAB, Morgan CJ, Llewelyn MB, Albuquerque SRJ, Farmer A. Heterogeneity of serum tryptophan concentration and availability to the brain in patients with the chronic fatigue syndrome. J Psychopharmacol. 2005; 19(4): 385–91.[↩][↩][↩][↩][↩][↩]
- Vassallo CM, Feldman E, Peto T, Castell L, Sharpley AL, Cowen PJ. Decreased tryptophan availability but normal post-synaptic 5-HT2C receptor sensitivity in chronic fatigue syndrome. Psychol Med. 2001; 31: 585–91. https://www.ncbi.nlm.nih.gov/pubmed/11352361[↩][↩][↩][↩][↩]
- Rowbottom D, Keast D, Pervan Z, Goodman C, Bhagat C, Kakulas B, et al. The role of glutamine in the aetiology of the chronic fatigue syndrome: A prospective study. J Chronic Fatigue Syndr. 1998; 4(2): 3–22.[↩][↩][↩][↩][↩][↩]
- De Lorenzo F, Hargreaves J, Kakkar VV. Phosphate diabetes in patients with chronic fatigue syndrome. Postgrad Med J. 1998; 74(870): 229–32. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2360873/[↩][↩][↩]





{kind=link}