
Contents
What is compartment syndrome
Compartment syndrome is a painful and potentially serious condition when pressure caused by bleeding or swelling within the muscle compartment builds to dangerous levels – known as a muscle compartment. Each group of muscles in the arms and legs, together with nearby blood vessels and nerves, is contained in a space surrounded by tissue called fascia (see Figures 1 to 3 below). Compartment syndrome occurs when the pressure within a compartment increases, restricting the blood flow to the area and potentially damaging the muscles and nearby nerves.
It usually occurs in the legs, feet, arms or hands, but can occur wherever there’s an enclosed compartment inside the body.
This pressure can decrease blood flow, which prevents nourishment and oxygen from reaching nerve and muscle cells.
Compartment syndrome can be either acute or chronic.
- Acute compartment syndrome is a medical emergency. Acute compartment syndrome happens suddenly and needs urgent treatment. It is usually caused by a severe injury. Without treatment, it can lead to permanent muscle damage.
- Chronic compartment syndrome, also known as exertional compartment syndrome, is usually not a medical emergency. It is most often caused by athletic exertion.
Muscle Compartments of the Arms and Legs
Dense fibrous connective tissue called the fascia divides the muscles of the limbs into anatomical compartments. The role of the fascia is to keep the tissues in place, and, therefore, the fascia does not stretch or expand easily. These fascial compartments group muscles of similar developmental origin and function. Muscles in the same compartment have similar actions and often function synergistically to produce a particular movement. Muscles in opposite compartments function as agonist/antagonist pairs. In most cases, each compartment is innervated by a single named nerve.
Upper Limb
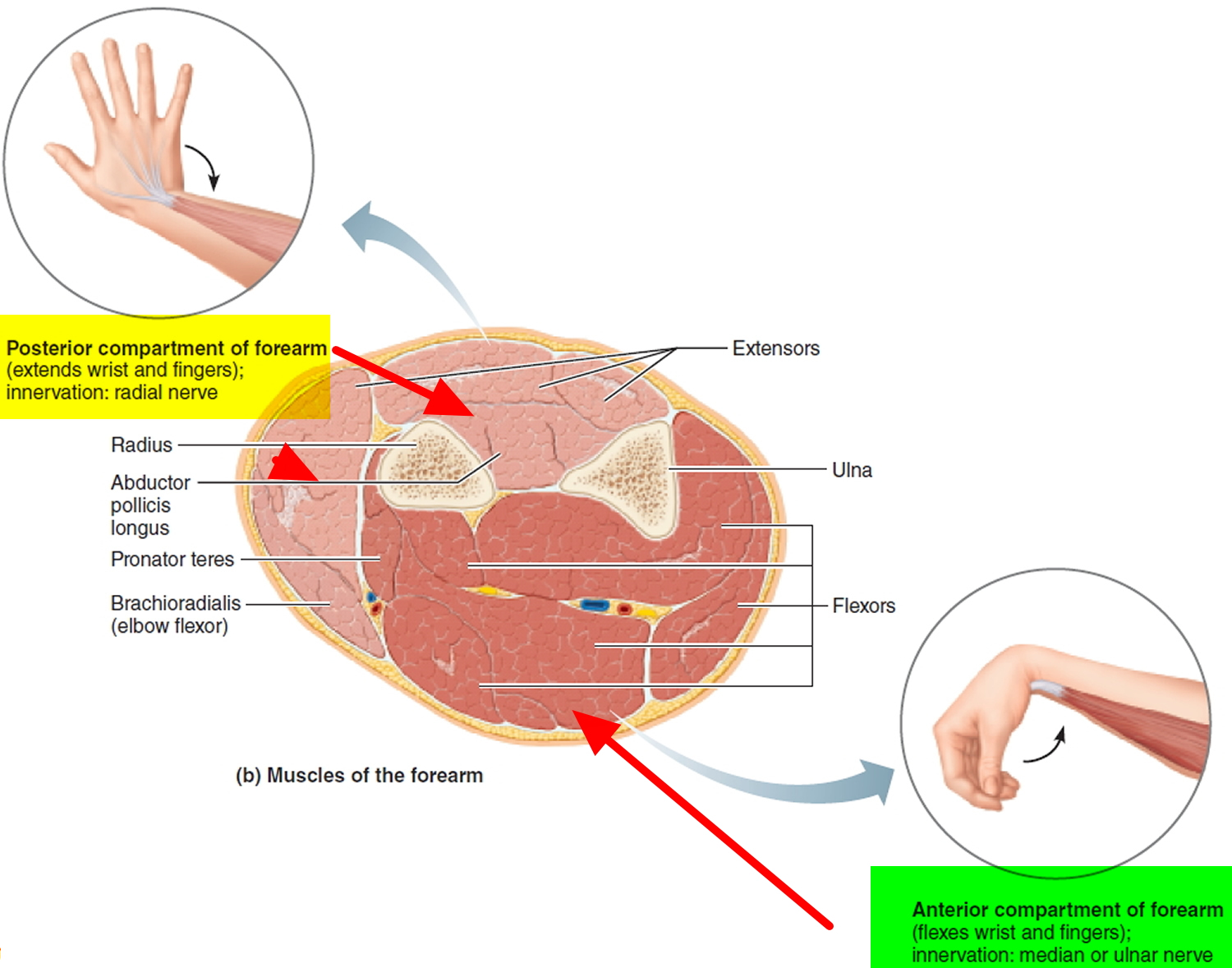
The upper limb has two compartments: anterior and posterior. The muscles in the anterior compartment of the arm flex the arm at the shoulder or flex the forearm at the elbow and are innervated by the musculocutaneous nerve. The muscles of the anterior compartment of the forearm are wrist and digital flexors and pronators innervated by either the median nerve or the ulnar nerve. The muscles of the posterior compartments of the arm and forearm extend the elbow and wrist, respectively. These muscles, plus the supinator and brachioradialis (developmentally posterior compartment muscles), are all innervated by branches off the radial nerve. Functionally, the supinator supinates the forearm, and the brachioradialis, which crosses the anterior side of the elbow, acts as a forearm flexor.
Figure 1. Muscle compartments of arm
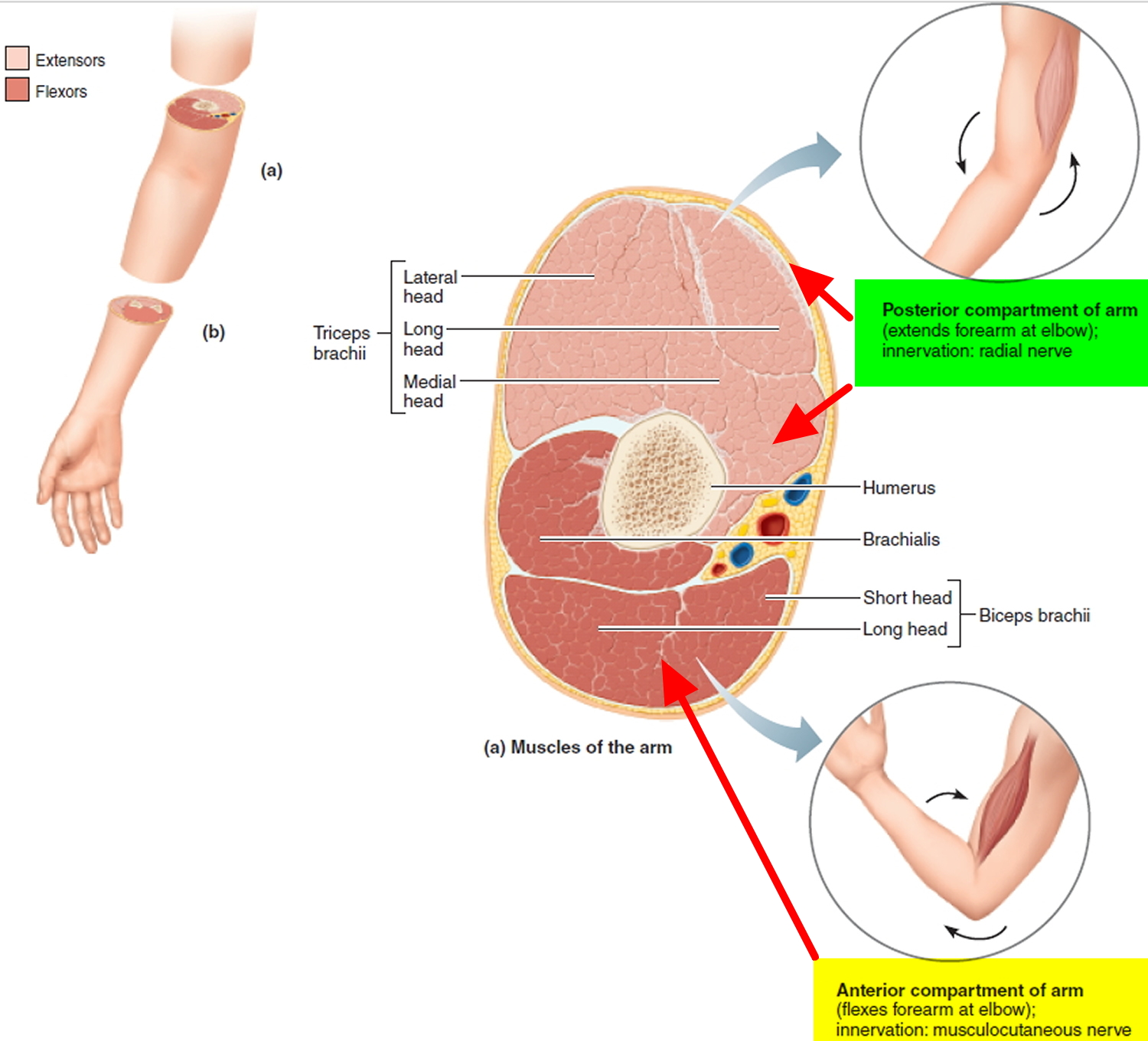
Figure 2. Muscle compartments of forearm
Lower Limb
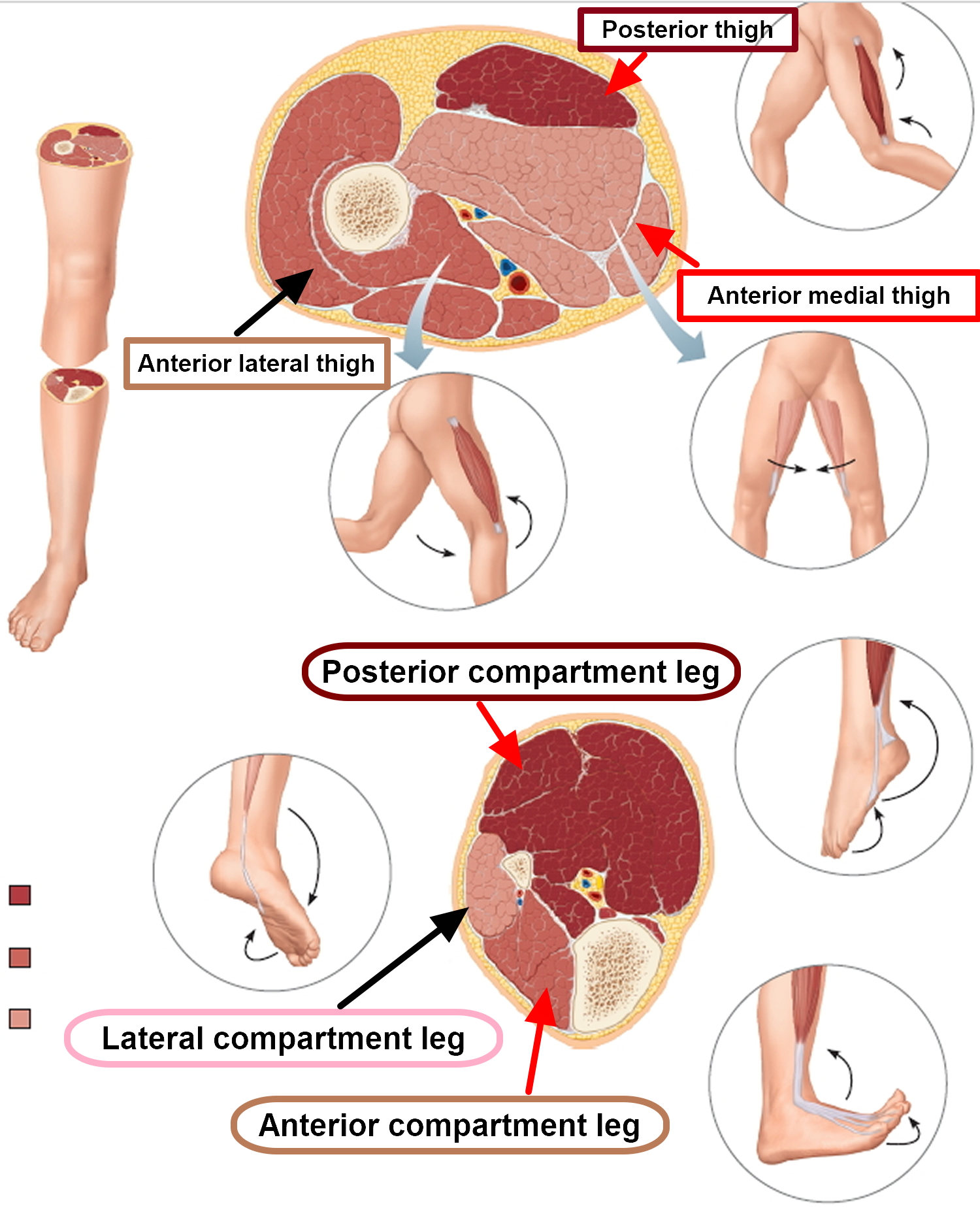
The thigh portion of the lower limb has three compartments: posterior, anterior, and medial. The muscles of the posterior compartment extend the thigh at the hip and flex the leg at the knee and are innervated by the tibial branch of the sciatic nerve. The muscles of the anterior compartment flex the thigh at the hip and extend the leg at the knee and are innervated by the femoral nerve. The muscles of the medial compartment adduct the thigh and are innervated primarily by the obturator nerve.
The leg also has three compartments: posterior, anterior, and lateral. The posterior compartment contains the digital flexor muscles and plantar flexors innervated by the tibial nerve. The anterior compartment contains the digital extensor muscles and dorsiflexors, all innervated by the deep fibular nerve. The lateral compartment contains the fibularis muscles that plantar flex and evert the foot and are innervated by the superficial fibular nerve.
Figure 3. Muscle compartments of thigh and leg
 Acute compartment syndrome
Acute compartment syndrome
- happens suddenly, usually after a bone fracture, crush injury or severe injury
- is a medical emergency and requires urgent treatment
- can lead to permanent muscle damage if not treated quickly
Acute compartment syndrome is a medical emergency and ideally needs to be treated in hospital within a few hours to avoid permanent damage to the muscles or nerves.
Acute compartment syndrome causes
Acute compartment syndrome can be caused by:
- A broken bone or a crush injury – this is the most common cause
- A plaster cast or tight bandage being applied to a limb before it has stopped swelling
- Burns, which can cause the skin to become scarred and tight
- Surgery to repair a damaged or blocked blood vessel (once blood is able to flow back into a muscle, it can lead to swelling)
- Reestablished blood flow after blocked circulation. This may occur after a surgeon repairs a damaged blood vessel that has been blocked for several hours. A blood vessel can also be blocked during sleep. Lying for too long in a position that blocks a blood vessel, then moving or waking up can cause this condition. Most healthy people will naturally move when blood flow to a limb is blocked during sleep. The development of compartment syndrome in this manner usually occurs in people who are neurologically compromised. This can happen after severe intoxication with alcohol or other drugs.
- Other causes include:
- Very tight bandages or plaster casts
- Severe bruising
- Anabolic steroid use. Taking steroids is a possible factor in compartment syndrome.
- Blood flow returning after blocked circulation
In rare cases, it can occur without any obvious injury.
Chronic compartment syndrome
Chronic exertional compartment syndrome is an exercise-induced muscle and nerve condition that causes pain, swelling and sometimes disability in the affected muscles of your legs or arms. Anyone can develop the condition, but it’s more common in athletes who participate in activities that involve repetitive impact, such as running.
- happens gradually, usually during and immediately after repetitive exercise (such as running or cycling)
- usually passes within minutes of stopping the activity
- is not a medical emergency and doesn’t cause permanent damage
Chronic exertional compartment syndrome isn’t a life-threatening condition and usually doesn’t cause lasting damage if you get appropriate treatment. However, continuing to exercise despite pain can be difficult if severe weakness or numbness is present.
Chronic exertional compartment syndrome may respond to non-operative treatment and activity modification. If non-operative treatment doesn’t help, your doctor might recommend surgery. Surgery is successful for many people, and might allow you to return to your sport.
Chronic compartment syndrome causes
The exact cause is unknown.
Chronic compartment syndrome usually occurs in young people who do regular repetitive exercise, such as running, swimming, or cycling. This is usually relieved by discontinuing the exercise, and is usually not dangerous.
When you exercise, increased blood flow to working muscles expands them. If the connective tissue (fascia) that binds the muscle fibers in a compartment doesn’t also expand, pressure builds up in the compartment. Over time, the pressure cuts off some of the muscle’s blood supply.
Some experts suggest that how you move (biomechanics) might have a role in causing chronic exertional compartment syndrome. Other causes might include having enlarged muscles, an especially thick or inelastic band of tissue (fascia) surrounding a section of muscle, or high pressure within your veins (venous hypertension).
Risk factors for exertional compartment syndrome
Certain factors increase your risk of developing chronic exertional compartment syndrome, including:
- Age. Although people of any age can develop chronic exertional compartment syndrome, the condition is most common in male and female athletes under 30.
- Type of exercise. Repetitive impact activity — such as running or fast walking — increases your risk of developing the condition.
- Overtraining. Working out too intensely or too frequently also can raise your risk of chronic exertional compartment syndrome.
Compartment syndrome symptoms
Acute compartment syndrome
Symptoms of acute compartment syndrome usually develop after an injury and get quickly worse.
Symptoms can include:
- intense pain, especially when the muscle is stretched, which seems much worse than would normally be expected for the injury
- your skin may look pale and feel cold to touch
- tenderness in the affected area
- tightness in the muscle
- a tingling or burning sensation
- in severe cases, numbness or weakness (these are signs of permanent damage)
Chronic compartment syndrome
Symptoms of chronic compartment syndrome tend to develop gradually during exercise and improve with rest.
The signs and symptoms associated with chronic exertional compartment syndrome might include:
- Aching, burning or cramping pain in the affected limb — usually the lower leg
- Tightness in the affected limb
- Numbness or tingling in the affected limb
- Weakness of the affected limb
- Foot drop, in severe cases, if legs are affected
- Often occurs in the same compartment of both legs
- Occasionally, swelling or bulging as a result of a muscle hernia
Pain due to chronic exertional compartment syndrome typically follows this pattern:
- Begins after a certain time, distance or intensity of exertion after you start exercising the affected limb
- Progressively worsens as you exercise
- Subsides within 10 to 20 minutes of stopping the activity
- Over time, recovery time after exercise often increases
Taking a complete break from exercise or performing only low-impact activity might relieve your symptoms, but usually only temporarily. Once you take up running again, for instance, those familiar symptoms usually come back.
Compartment syndrome diagnosis
Acute Compartment Syndrome
Go to an emergency room immediately if there is concern about acute compartment syndrome. This is a medical emergency. Your doctor will measure the compartment pressure to determine whether you have acute compartment syndrome.
Chronic (Exertional) Compartment Syndrome
To diagnose chronic compartment syndrome, your doctor must rule out other conditions that could also cause pain in the lower leg. For example, your doctor may press on your tendons to make sure you do not have tendonitis. He or she may order an X-ray to make sure your shinbone (tibia) does not have a stress fracture.
Imaging studies
Your doctor might suggest imaging studies such as MRI or near infrared spectroscopy (NIRS). A typical MRI scan of your legs can be used to evaluate the structure of the muscles in the compartments and rule out other possible causes of your symptoms.
A newer, special MRI scan can help assess the fluid volumes of the compartments during exercise. It has been found to be accurate in detecting compartment syndrome, and may reduce the need for the invasive compartment pressure testing.
NIRS is a newer technique that uses light wavelengths to measure tissue oxygen saturation in your blood. This helps to determine if your muscle compartment has decreased blood flow.
Compartment pressure testing
If imaging studies fail to uncover an abnormality such as a stress fracture or similar cause of pain, your doctor might suggest measuring the pressure within your muscle compartments.
This test, often called compartment pressure measurement, is the gold standard for diagnosing chronic exertional compartment syndrome. Because it’s invasive and mildly painful, involving insertion of needles into your muscles, compartment pressure measurement usually isn’t performed unless your medical history and other tests strongly suggest you have this condition.
To confirm chronic compartment syndrome, your doctor will measure the pressures in your compartment before and after exercise. If pressures remain high after exercise, you have chronic compartment syndrome.
Compartment syndrome treatment
Acute compartment syndrome
Acute compartment syndrome must be treated in hospital using a surgical procedure called an emergency fasciotomy.
The doctor or surgeon makes an incision to cut open your skin and fascia surrounding the muscles to immediately relieve the pressure inside the muscle compartment.
The wound will usually be closed a few days later. Occasionally, a skin graft may be required to cover the wound.
Chronic compartment syndrome
Chronic compartment syndrome isn’t usually dangerous, and can sometimes be relieved by stopping the exercise that triggers it and switching to a less strenuous activity.
Nonsurgical treatment. Physiotherapy, orthotics (inserts for shoes), and non-steroidal anti-inflammatory medicines are sometimes suggested. They have had questionable results for relieving symptoms.
Your symptoms may subside if you avoid the activity that caused the condition. Cross-training with low-impact activities may be an option. Some athletes have symptoms that are worse on certain surfaces (concrete vs. running track, or artficial turf vs. grass). Symptoms may be relieved by switching surfaces.
To help relieve the pain of chronic exertional compartment syndrome, try the following:
- Wear better athletic shoes.
- Limit your physical activities to those that don’t cause pain, especially focusing on low impact activities such as cycling or an elliptical trainer. For example, if running bothers your legs, try swimming. Or try running on softer surfaces.
- Apply ice to the affected area after exercising.
Surgical treatment. If conservative measures fail, surgery may be an option. Similar to the surgery for acute compartment syndrome, the operation is designed to open the fascia so that there is more room for the muscles to swell.
Usually, the skin incision for chronic compartment syndrome is shorter than the incision for acute compartment syndrome. Also, this surgery is typically an elective procedure — not an emergency.





{kind=link}