
Contents
What are crows feet
Hoping to avoid crow’s feet ? Sun damage is a primary cause of wrinkles. You can minimize the likelihood of developing wrinkles around your eyes by applying sunscreen (SPF 30+, broad spectrum sunscreen, but not too close to the eye) and wearing protective eyewear, such as wraparound sunglasses. To make an informed decision when selecting a sunscreen product, it is important to know that more thorough coverage is provided by broad spectrum formulations. These sunscreens offer not only UVB (ultraviolet B) protection, but they also include UVA (ultraviolet A) blocking agents – UVA rays cause most of the damage that leads to premature aging of the skin. Make sunscreen a part of your daily routine, re-apply sunscreen every two hours or more frequently if you are active in the water or perspiring a lot. The minerals contained in physical sunscreens, such as titanium dioxide or zinc oxide, work by forming a surface layer on the skin that will absorb, reflect and scatter the sun’s harmful UV rays before they can penetrate into the skin itself. Be generous with the amount of sunscreen that you apply (the recommendation is 2mg/cm2) – most people underestimate the necessary amount and therefore, do not receive the intended protective effect indicated by the SPF level listed on the packaging. Do not forget your wide-brimmed hat and sunglasses too!
Some wrinkles are produced by repeated movement of the skin.
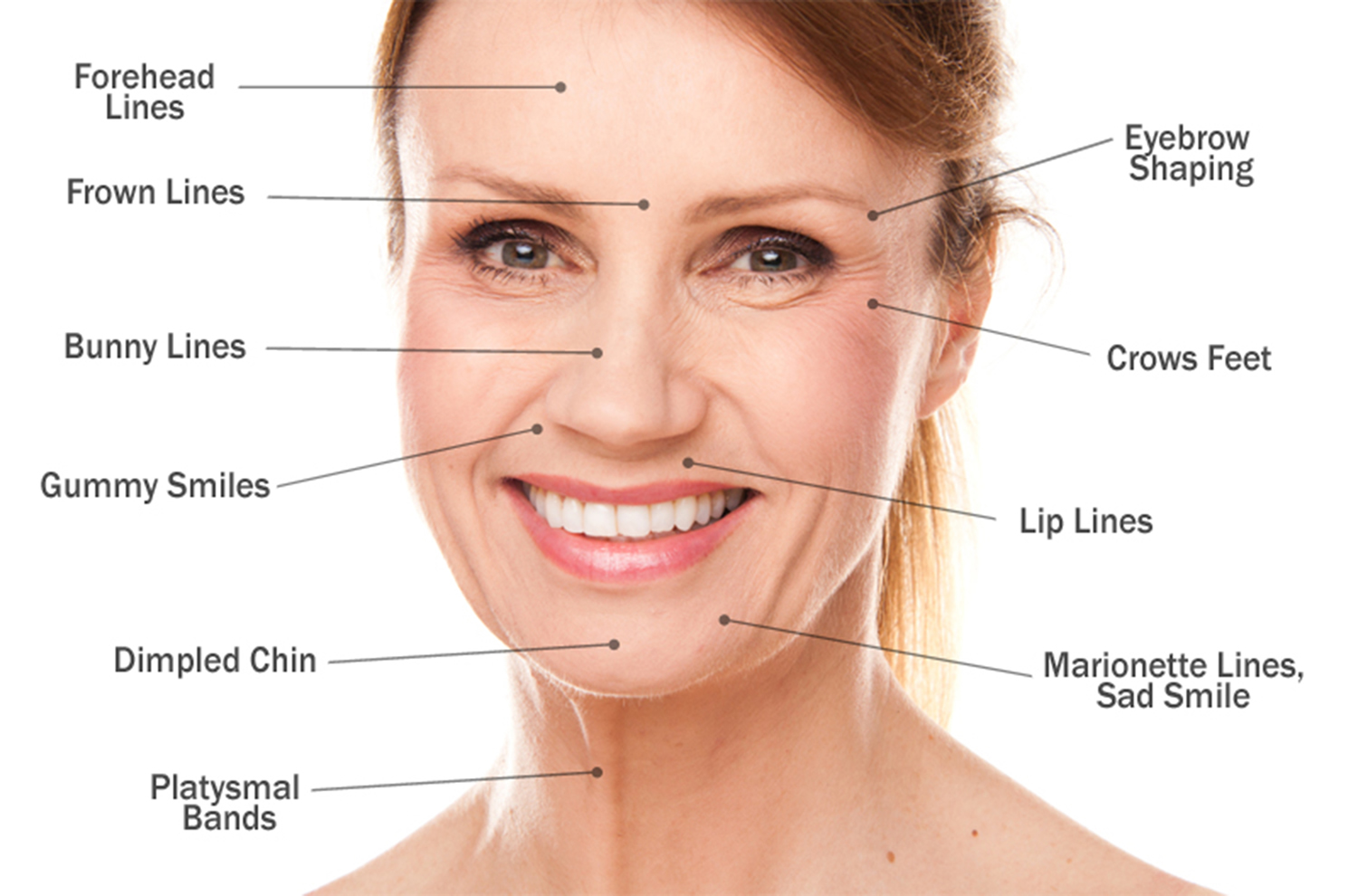
Figure 1. Crows feet

Wrinkles on the skin are divided into:
- Wrinkles produced by Movement of the skin and
- Wrinkles that are present when the skin of the face is at Rest.
Moisturizers can only work by minimizing the appearance of fine lines in skin at rest that are caused by dehydration of the skin.
Premature aging of the skin is most often the product of years of unprotected sun exposure combined with your genetic makeup. The amount of incidental ultraviolet radiation that you receive when you take the dog out, drive to work on a sunny day, or walk to a nearby cafe, accounts for 80% of all sun exposure. The cumulative effects of prolonged or unnecessary UV exposure can lead to premature aging of your skin and increase your risk for skin cancer.
The process of aging causes the skin to thin, become less elastic and more fragile. Your body also produces less natural protective oils, which makes the skin drier. Do not over wash your face or scrub too hard. Cleaning too often can strip away essential oils and dry out your skin. Wash your face twice a day by using a cleanser that is appropriate for your particular skin type. Lather-up the cleanser with water and massage your face in a circular motion. Limit the use of products containing particles (scrubs) to no more than twice weekly, as they can irritate your skin. If you have sensitive skin, try foam formulations or cleansing cloths – they will gently, but effectively, clean without causing dryness or irritation. Finish off with a moisturizer; using one with at least an SPF of 15 will provide the necessary UV protection.
In addition, the fat located in the deeper layers of the skin, that gives your skin a plump appearance, starts to diminish over time. The combination of these factors causes loose, saggy and wrinkly skin. Keeping your skin adequately moisturized will lessen the appearance of wrinkles.
Furthermore, regimented use of a sunscreen will help to minimize any further sun damage. A simple way to achieve comprehensive coverage is to find a minimum SPF30 moisturizer that provides broad spectrum protection against both UVA and UVB rays. Most sunscreens do a good job blocking UVB light, but fewer sunscreens filter out UVA radiation. UVB rays are responsible for causing sunburn, but UVA rays have the ability to penetrate into deeper layers of the skin and cause premature aging and skin cancer. A product providing broad spectrum coverage will offer a more complete range of UV protection.
How do facial lines and wrinkles form ?
Facial lines and wrinkles (rhytides) form because of the following factors:
- Aging processes
- Sun damage
- Muscle movement
- Gravity
- Injury
- Surgery
- Acne
- Other skin diseases with a tendency to scar (e.g. discoid lupus)
- Smoking
There is often a degree of asymmetry to the lines, as people tend to smile or frown more on one side than the other, or consistently sleep on the right or the left cheek.
Fine lines
Fine lines and wrinkles arise because of irregular thickening of the dermis and because of a decrease in the amount of water held by the epidermis. This is mainly caused by sun damage and exposure to environmental toxins particularly tobacco smoke.
Furrows
Deeper lines or furrows are classified as dynamic or static. Dynamic lines appear with movement i.e. the activity of facial muscles. Static lines are unchanged with muscle movement. Eventually dynamic lines become static.
- Crow’s feet around the eyes are due to smiling and activity of the eyelid muscles (orbicularis oculi).
- Worry lines on the forehead are due to contraction of the frontalis muscle when raising the eyebrows
- Frown lines between the eyebrows are due to contraction of corrugator supercilii muscles and procerus muscle when concentrating or angry
Sags and bags
Skin laxity or drooping is caused by several factors:
- A reduction of the fat cells under the skin (subcutaneous tissue)
- Loss of collagen and elastin fibres in the dermis reducing cutaneous strength and elasticity
- Gravity, which allows the lax tissue to sag
The result is:
- Brow ptosis (the forehead sags so the eyebrows drop over the eyelids, which then feel heavy)
- Eyelid ptosis (the upper eyelid drops, sometimes obscuring the pupil)
- Baggy upper and lower eyelids
- Sagging lower eyelids, revealing the reddened mucosal surface (ectropion)
- Hollow look to the eyes
- Tired-looking eyes with a prominent groove beside the nose (tear-trough deformity)
- Jowls (loss of jaw line)
- Loss of neckline
- Elongated earlobes
- Dropping of the tip of the nose
- Thinning of the upper lip.
Figure 2. Facial lines and wrinkles
What is ageing skin ?
Aging skin describes the changes in the appearance and characteristics of the skin that occur as people get older. Aging changes are particularly pronounced on the face and hands 1.
Over time, skin loses its youthful appearance. This natural ageing process is often accelerated by:
- Hereditary factors
- Sun exposure
- Cigarette smoking
- Chicken pox and acne
The visible results are superficial blemishes – broken capillaries, freckles (lentigos), and keratoses (dry spots), scars, fine wrinkles and deep furrows.
Who gets prematurely aged skin ?
Skin appears prematurely aged in people that are chronically exposed to sunlight, a process known as sun damage or photoageing. People with marked signs of photoageing 1:
- Often live in the tropics or subtropics
- May live at high altitude
- Usually work outdoors or spend long periods outdoors for recreation
- Have sometimes been exposed to artificial sources of ultraviolet radiation (UV), such as indoor tanning
- Often have fair skin (skin skin phototypes I and II), with blond hair and blue eyes
- Rarely have a genetic predisposition to premature ageing (most marked in progeria )
Premature ageing of the skin also affects tobacco smokers and those chronically exposed to other environmental pollutants.
What causes the skin to age ?
Intrinsic ageing
Intrinsic ageing of the skin is inevitable, and is genetically predetermined. It occurs because of accumulation of reactive oxygen species, biological aging of cells, and reduced cellular supply of nutrients and oxygen.
- The rate of epidermal cell proliferation slows, affecting structure and function of the skin. The skin thins and flattens, with less resistance to shearing forces and injury.
- Water content in the stratum corneum reduces, with less transepidermal water loss.
- Hair thins and greys.
- The numbers of melanocytes reduce.
- Sebum production reduces.
- The dermis has reduced vascularity.
- There are fewer dermal mast cells and fibroblasts, and reduced glycosaminoglycans, hyaluronic acid and ground substance.
- There is reduced collagen and elastin turnover, and increased glycation.
- Volume of subcutaneous fat diminishes, especially on face hands and feet—whereas, it increases on thighs, waist and abdomen.
- Ageing is immune suppressing, leading to increased risk of skin cancer.
Menopause in females
In women, loss of oestrogen levels at menopause contribute to premature aging, as compared with similarly aged men.
Photoaging
Photoaging is due to damage caused by solar radiation. Cell damage occurs because of the formation of reactive oxygen species.
- High energy, short wavelength UVB damages DNA and other components of the epidermis.
- Longer-wavelength UVA is 100 times more prevalent than UVB at the earth’s surface, but is of lower energy, so is less damaging to DNA. UVA penetrates more deeply into the dermis, damaging elastic tissue, collagen, blood vessels and immune cells.
- Infrared radiation penetrates to the deeper dermis and subcutaneous tissue, where it may also contribute to sun damage.
Smoking
Smoking exposes the skin to several damaging factors.
- Nicotine narrows blood vessels, reducing blood flow, and thus impairs oxygen and important nutrients reaching the cells.
- Many other chemicals in tobacco smoke increase dermal matrix metalloproteinases, degrading collagen and elastin.
- The heat from burning cigarettes, and facial muscle movements associated with smoking, contribute to wrinkles.
- Nitrosamines and tar are carcinogens.
Immune dysfunction
Immune dysfunction also affects skin ageing. Examples include:
- Immune deficiency diseases
- Immunosuppressive agents
- Chronic psychological stress
What are the clinical features of ageing skin ?
Intrinsic aging
- Ageing skin is thin and inelastic, tearing easily.
- It recovers more slowly from mechanical depression than younger skin.
- Women have thinner skin then men.
- Skin is dry, especially after frequent washing with soap and water.
- Dry skin increases the risk of asteatotic eczema
- The barrier function of the skin is less effective than when younger
- Pigmentation is uneven due to melanocyte activation (melanosis) and inactivation (guttate hypomelanosis)
In those genetically predisposed, ageing skin develops:
- Telangiectases and cherry angiomas
- Seborrhoeic keratoses
Photoageing
Photoageing results in:
- Fine lines and wrinkles
- Discoloration
- Textural changes
- Thin skin that easily blisters, tears and grazes
- Solar elastosis/heliosis
- Solar lentigos and freckles
- Solar comedones and colloid milia
- Senile/solar purpura
- Scarring, eg from sunburn
- Actinic keratoses (tender dry spots)
- Skin cancer (destructive growths)
Smoking
Compared to non-smokers of the same age, long-term smokers have:
- More facial lines
- Baggy eyelids and jawline
- Yellowish sallow complexion
- Open and closed comedones and cysts (Favre-Racouchot syndrome )
- Greater risk of skin cancer
Complications of ageing skin
Ageing skin is prone to keratinocytic skin cancer and some types of melanoma. The most common form of skin cancer is basal cell carcinoma. However, excessively photoaged skin is at increased risk of intraepidermal carcinoma, squamous cell carcinoma, lentiginous forms of melanoma, and rare forms of skin cancer such as merkel cell carcinoma.
How can the signs of ageing skin be prevented ?
Intrinsic ageing is inevitable. In perimenopausal women, systemic hormone replacement may delay skin thinning; the skin is less dry, with fewer wrinkles, and wound healing is faster than prior to treatment. Replacement is less effective at improving skin ageing in the postmenopausal decades. The effects of topical oestrogens, phyto-oestrogens and progestins are under investigation.
Protection from solar UV is essential at all ages.
- Be aware of daily UV index levels, eg adhere to Sun Protection Alert advice.
- Avoid outdoor activities during the middle of the day.
- Wear sun-protective clothing: broad-brimmed hat, long sleeves and trousers/skirts.
- Apply very high sun-protection factor, broad-spectrum sunscreens to exposed skin.
Do not smoke and where possible, avoid exposure to pollutants. Take plenty of exercise—active people appear younger than inactive people. Eat fruit and vegetables daily to provide natural antioxidants.
Many oral supplements with antioxidant and anti-inflammatory properties have been advocated to retard skin ageing and to improve skin health. They include carotenoids, polyphenols, chlorophyll, aloe vera, vitamins B, C and E, red ginseng, squalene, and omega-3 fatty acids. Their role is unclear.
Crows feet treatment options
Facial lines and wrinkles
Ageing skin droops and develops wrinkles, lines and furrows. The severity of these changes in an individual depends on genetic tendency, skin phototype and exposure to environmental factors.
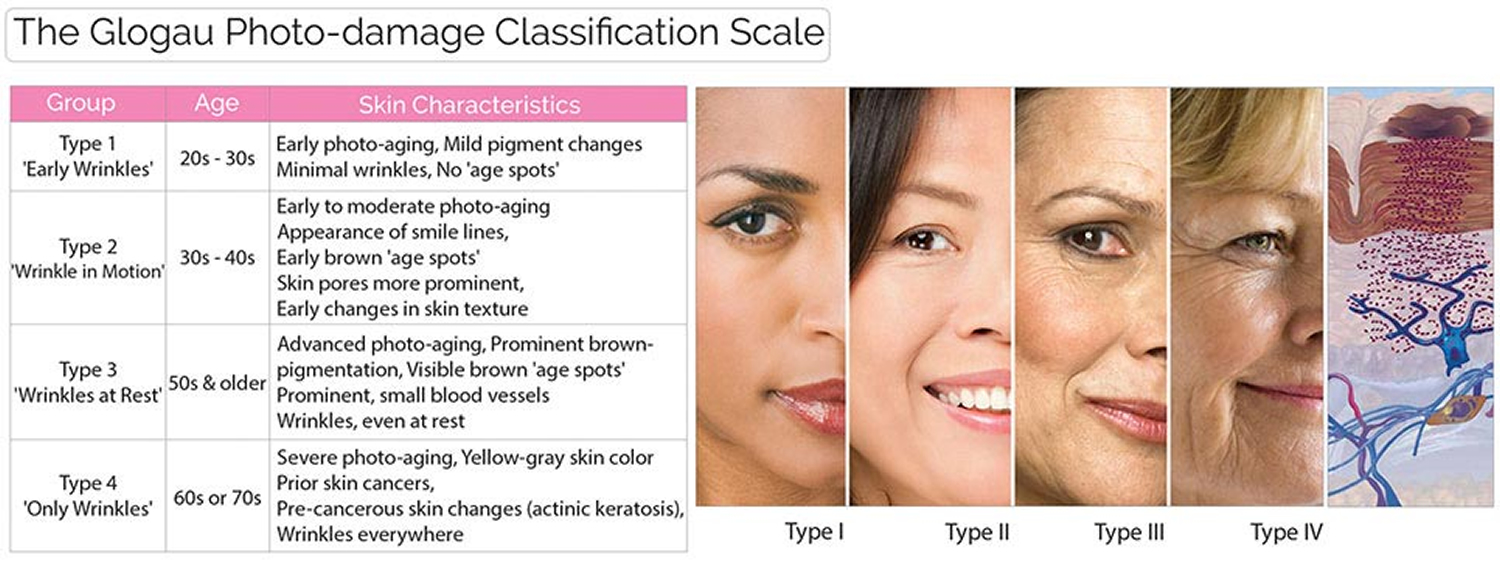
Classification of photoaging
Dermatologists and cosmetic surgeons often use Glogau’s classification when describing these ageing changes.
- Mild – Few wrinkles, requires little or no make-up for coverage
- Moderate – Early wrinkling, sallow complexion, requires little makeup
- Advanced – Persistent wrinkling, skin discolouration with broken blood vessels and actinic keratoses, often wears make-up
- Severe – Severe wrinkling and furrows, actinic keratoses, often wears make-up but it may not hide the ageing changes.
Glogau classified the degree of sun damage by its clinical signs.
Type I, Mild, “no wrinkles”
- Mild pigment changes
- Minimal wrinkles
- No keratoses
Type II, Moderate, “wrinkles in motion”
- Appearance of lines only when face moves
- Early lentigines
- Skin pores more prominent
- Early changes in skin texture
Type III, Advanced, “wrinkles at rest”
- Prominent pigmentation
- Noticeable solar lentigines
- Prominent small blood vessels
- Wrinkles present when face at rest
Type IV, severe, “only wrinkles.”
- Wrinkles at rest or moving
- Yellow-gray skin color
- Prior skin cancers
- Actinic keratoses.
Figure 3. Glogau’s photo-aging classification
The Fitzpatrick classification of facial lines refers to the degree of wrinkling around the mouth and eyes:
- Class I: Fine wrinkles
- Class II: Fine-to-moderately deep wrinkles and moderate number of lines
- Class III: Fine-to-deep wrinkles, numerous lines, and possibly redundant folds
How are the signs of skin aging treated ?
Moisturisers will help improve dry and flaky skin. Moisturizers replenish both lost water and water-binding ingredients (such as glycerin) that help to retain hydration in the skin. Moisturizers are specifically formulated to prevent moisture loss, act as a protective layer that traps dirt and pollutants and they can also serve as a base layer that smoothes out the skin to create a more even surface for makeup application.
Alpha-hydroxy acids (AHA), vitamin C, alpha-lipoic acid, soy isoflavones or retinoid creams applied regularly long term reduce dryness. They may also reduce the number of fine wrinkles and even out pigmentation. Many other products are under investigation but their benefits are unclear.
Dry and discolored skin
Moisturizers
Moisturizers restore water content to the epidermis, and provide a soothing protective film. They improve the appearance and tactile properties of dry and aging skin, restore the normal barrier function of the skin, and reduce the release of inflammatory cytokines. Moisturizers comprise an important therapeutic component in the management of various skin conditions (e.g., eczema, psoriasis, pruritus, and aged skin) 2.
Furthermore, there are moisturizers containing silicone to fill and seal facial lines by effectively targeting wrinkle prone areas, such as around the eyes, mouth and forehead. The treatment creates a smoother surface for makeup application and the effect can last all day. Another innovative option includes makeup foundations that can seamlessly minimize the look of fine lines and diminish the appearance of blemishes or other skin imperfections. These specialized formulas provide natural-looking, balanced camouflage. Furthermore, many newer generation foundations are multi-purposed with the addition of conditioning agents, such as antioxidants to help balance skin tone, vitamins (niacinamide) to strengthen the barrier function of the skin and encourage collagen production, and UV filters to guard against sun damage. With so many benefits, why not choose a less invasive approach to treat wrinkles and rejuvenate your complexion ?
How do Moisturizers work ?
Moisturizers slow down the natural evaporation of moisture in the skin by replacing natural skin oil, which covers microscopic fissures in the skin. Moisturizers not only increase water content within the skin and provide a protective film, it restores the skin’s ability to store water, and reduces natural water loss.
Do Moisturizers remove wrinkles ?
Moisturizers have the effect of smoothing the skin over. This has the effect of making wrinkles less apparent. However, they will not have any long-term effect of reducing or removing existing wrinkles.
What should I be looking for in a product ?
While hype and exaggerated advertising are certainly a problem in the skincare industry, moisturizers are an important part of basic skincare. For those with dry skin, or those that have skin problems that cause dryness, they are essential and help improve quality of life.
You are looking for products that help to smooth out the skin, and allow the skin to retain moisture. Other good traits are quick absorption and long lasting effects. Depending on your skin type, make sure that the product fits your unique needs. Consider how sensitive your skin is, and look for these—non allergenic, non-sensitizing, fragrance free, or non-comedogenic products as your needs require.
Are there more ways of differentiating products ?
Moisturizers vary considerably in quality, but also in consistency and secondary factors like fragrance and look. There are indeed many products on the shelves, and few ways to differentiate between them. There isn’t a single product that is ideal for all skin types, so the product that your best friend recommends may not work for you. Knowing your skin type is important, as many moisturizer products are designed with a certain skin type in mind. Those with normal to oily skin should use lighter moisturizers that don’t clog the pores.
However, there are general ingredients that dermatologists look for in a moisturizer.
- Humectants, which are water binding agents, do not necessarily help the skin retain moisture, but heals sun damaged skin.
- Occlusives block water loss in the skin layers and are included in products like Petrolatum, lanolin, mineral oil, and dimethicone, and act as a protective barrier for the skin.
- Emollients such as plant and mineral oils, shea or cocoa butter, petrolatum, or silicone are used as lubricating agents to soften the skin and allow it to retain moisture better.
- Anti-irritants such as aloe, licorice root, green tea, or chamomile extracts are commonly added to moisturizers to help reduce potential reaction to other irritants in the solution.
- Alpha hydroxyl acids such as lactic or glycolic acids can help treat rough or scaly skin.
- The opinion on vitamins and certain antioxidants can be varied, even among experts.
- Remember that products must have a certain quantity of a certain substance to have a positive effect on the skin. Just because a product contains a beneficial substance does not mean that it contains the substance in adequate quantities to make a noticeable difference.
Are there any downsides to using moisturizers ?
Like any cosmetic products, moisturizers can contain substances that your skin may not react well to. General irritation to certain solvents, or lactic acids are common, as are cases of allergic contact dermatitis, reacting to fragrances or preservatives that are in the moisturizer. Photo contact dermatitis, as well as sweat retention are also known reactions to certain moisturizers if you have a sensitivity to certain products. If you notice any of these symptoms, we suggest that you visit a doctor and discontinue use of the product.
Should I buy high end brands or generic moisturizers ?
Not necessarily. There are both good and bad moisturizers at all price ranges. A better indicator for choosing the appropriate product is what skin type the product is designed for. Moisturizers should be used regularly, so you should be looking for a price range that you would be comfortable using daily.
Each person’s skin is unique, and you will need to experiment a little to see what works best for you. However, experts generally agree that low cost brands are just as effective as their more expensive counterparts. One general advice is to apply your moisturizer when your hands are damp as it increases skin absorption, requiring less application.
Any other advice ?
Avoid products that have added fragrance preservatives or botanicals, as these can be irritants for dry skin or cause allergic contact dermatitis. Much like food labelling, the order of the ingredients are listed in order of content. If an ingredient like vitamin C is at the bottom of the list, chances are that there is very little of it. Moisturizers will not increase natural collagen production or elastin; substances that have these effects cannot penetrate the skin.
Do not wash your face too often as it can dehydrate your skin. Use a gentle cleanser formulated for dry skin, twice a day at most. Finally, adding olive oil or lavender oil can make your skin feel smooth.
Alpha-hydroxy acids (AHA)
Alpha hydroxyl acids are compounds that are derived from certain food products such as sugar canes, sour milk, apples, grape wine, and citric fruits, that can have beneficial effects on the skin 3. Also referred to as fruit acids, they are a common ingredient found in cosmeceutical products.
Examples include:
- Citric acid
- Glycolic acid
- Lactic acid
- Malic acid
- Pyruvic acid
- Tartaric acid
Of those AHAs, glycolic acid, which is derived from sugar canes, have the smallest molecular size, which is beneficial in penetrating the skin, where it can have an effect on the cells.
Glycolic acids can have varying effects on the skin depending on concentration levels. At the lower concentrations (5 to 10%) glycolic acids have the effect of reducing cell adhesion, promoting exfoliation of the outer skin, which creates a smoother feel after treatment. Over the counter products such as Reversa® contain this concentration of glycolic acids. This exfoliating effect can also help with the treatment of acne, photodamage, or wrinkling, which makes these products extremely appealing. Unfortunately for some people, especially those with sensitive skin, glycolic acid can be an irritant, and recent formulations often combine glycolic acid with amino acids, which reduce the risk of irritation while maintaining the benefits of the glycolic acid. At these lower concentrations, daily use is considered to be without risk.
At higher concentrations (10 to 50%), the benefits of glycolic acid are more pronounced. The effects, like those below 10%, are however, temporary. Higher concentration glycolic acids work on contact, and have effects similar to chemical peels. The acid promotes the splitting of cells, and is an effective treatment of acne or photodamage, but must be applied under careful supervision of a qualified physician 3. Multiple treatments of high concentration glycolic acids can have beneficial results for the skin. However, as with chemical peels, risks and side effects may include hyperpigmentation, redness, minor scarring, and activation of cold sores in those that have the virus latent in their systems.
In conclusion, alpha hydroxyl acids have an important place in total skin care, and skin doctors expect further study and development in treatments based on the use of these acids that extend beyond skin exfoliation.
Vitamin C
Vitamin C (L-ascorbic acid) is a natural exfoliant and antioxidant that’s found in citrus fruits and dark green leafy vegetables. It can reduce the signs of sun-damage on the skin, as well as decrease the appearance of brown patches 4. Because vitamin C is essential for both stimulating the production of collagen and the protection of cell membranes, this key ingredient has the ability to defend against free radical damage, and thereby, exert restorative effects to the skin. The stability and effectiveness of products containing this agent depends upon the type of vitamin C, how the preparation is formulated, and more importantly, on the concentration of the key active. Vitamin C is one of few topical agents whose effectiveness against wrinkles and fine lines is supported by scientific research. However, the practical use of vitamin C in skin care products presents difficulties due to its instability when formulated. Upon exposure to air, vitamin C undergoes oxidation and becomes ineffective, or even potentially harmful (oxidized vitamin C may increase the formation of free radicals). Stabilized commercial preparations are available, but they must be properly used and stored in order to maintain their effectiveness. Advances in vitamin C research has produced newer derivatives, such as ascorbyl palmitate and magnesuim ascorbyl phosphate, that appear to have improved skin penetration and efficacy.
Niacinamide (Vitamin B3)
Niacinamide is a potent antioxidant that is generally well tolerated. It improves the lipid barrier component of the epidermis, thus reducing transepidermal water loss, and acts as an inhibitor of melanosome transfer, resulting in reduced hyperpigmentation. Studies have revealed significant reduction in fine lines and wrinkles, hyperpigmented spots, red blotchiness, and skin sallowness, as well as improved skin elasticity 5, 6.
Alpha-lipoic Acid (ALA)
Alpha-lipoic acid has anti-inflammatory properties and acts as an exfoliant. In a split face study, topical 5% ALA applied b.i.d. for 12 weeks reduced skin roughness, lentigines and fine wrinkles 7). This agent does not protect against UV-induced erythema or reduce the number of sunburn cells.
Topical Peptides
Topical peptides are regarded as cellular messengers that are formed from amino acids and are designed to mimic peptide fragments with endogenous biologic activity. These pentapeptides (e.g., KTTKS) are comprised of a subfragment of type I collagen propeptide and play a role in signalling fibroblasts to produce collagen in the skin 8, which can improve the appearance of wrinkles.
One variation, the palmitoyl pentapeptide known as Pal-KKTKS (Matrixyl™, Sederma) was tested in a controlled, double-blind, left-right randomized, split-face study of 93 women between 35 and 55 years of age who had Fitzpatrick I-III type skin. Pal-KTTKS concentration was 3ppm; both groups were treated twice daily for 12 weeks. Improvements in wrinkle appearance and length were observed 9.
Retinoid creams
Topical retinoids are creams, lotions and gels containing one or other of group of medicines derived from Vitamin A. These compounds result in proliferation and reduced keratinisation of skin cells independent of their functions as a vitamin 10.
Many brand-name creams containing the retinoids retinol and retinaldehyde can be obtained over the counter at pharmacies and supermarkets.
The more potent topical retinoids available on prescription are:
- ReTrieve™ cream (tretinoin)
- Retin-A™ Cream (tretinoin or retinoic acid)
- Retinova™ Cream (tretinoin emollient)
- Isotrex™ Gel (isotretinoin)
There is extensive literature on the use of tretinoin, which is considered to be one of the most potent compounds for treating the signs of aging and/or photodamaged skin, including fine lines, hyperpigmented spots, and wrinkles 11, 12, 13.
What are Topical retinoids used for ?
In addition for their use in mild to moderately severe acne. Tretinoin has also been shown to reverse some of the changes due to photo-aging, i.e. sun damage. If used long term, it may reduce some fine wrinkles, freckles, solar comedones (whiteheads and blackheads), and actinic keratoses (tender, dry sun-spots).
They may also be used in bleaching creams to reduce pigmentation in melasma.
Topical retinoids can be applied to any area but are most often used on the face, the neck and the back of hands.
Do topical retinoids have any side effects ?
Topical retinoids can irritate the skin, especially when they are first used. This is more likely in those with sensitive skin, resulting in stinging. Excessive use results in redness, swelling, peeling and blistering in treated areas. It may cause or aggravate eczema, particularly atopic dermatitis.
By peeling off the top layer of skin, they may increase the chance of sunburn. Irritation may also be aggravated by exposure to wind or cold, use of soaps and cleansers, astringents, peeling agents and certain cosmetics.
Some people have reported a flare of acne in the first few weeks of treatment. This usually settles with continued use.
- Retinoids taken by mouth may cause birth deformities. Manufacturers recommend that topical retinoids are not used in pregnancy or breastfeeding as negative animal studies are not always predictive of human response.
How to use topical retinoids
Follow these instructions carefully:
- In general, a cream is less irritating than a gel. If there is a choice, start with a lower concentration product.
- Use your topical retinoid on alternate nights at first. If you have sensitive skin, wash it off after an hour or so. If it irritates, apply it less often. If it doesn’t, try every night, and if possible twice daily. In most people, the skin gradually gets used to it.
- To reduce stinging, apply it to dry skin, that is, 30 minutes or longer after washing.
- Apply a tiny amount to all the areas affected, and spread it as far as it will go.
- Don’t get it in your eyes or mouth.
- Apply a sunscreen to exposed skin in the morning.
- Wear your usual make-up if you wish, and use gentle cleansers (avoid soap) and apply non-greasy moisturisers as often as required.
- If your skin goes scarlet and peels dramatically even with cautious use, the retinoid may be unsuitable for your sensitive skin.
- Tolerance to topical retinoids often develops over time.
Depigmenting Agents
Skin-lightening agents added to product formulations have become increasingly popular. Common depigmenting ingredients include hydroquinone, ascorbic acid (vitamin C), kojic acid, and licorice extract (glabridin).
Hydroquinone
Hydroquinone has been the agent of choice for skin lightening. However, there are concerns over exogenous ochronosis and permanent depigmentation, as well as possible carcinogenicity 14 and it has been banned as an over-the-counter depigmenting agent in Europe, Australia and Japan 15. The US FDA has proposed concentrations between 1.5% and 2% in skin lighteners 16. A recent report suggested that this concern has been based mainly on studies with animal models utilizing long-term exposure at high dosages. Routine topical application may pose no greater risk than that from levels present in common foods 17.
Ascorbic acid (Vitamin C)
Ascorbic acid is a naturally occurring antioxidant found in citrus fruits and leafy green vegetables. It is hydrophilic, so skin penetration is low.
Kojic acid
Kojic acid is a less commonly used bleaching agent. When combined with dipalmitate, there is improved skin penetration and greater stability, but there is little research to support its efficacy 18.
Licorice Extract (Glabridin)
Several studies on melasma have shown good efficacy with only mild irritation that disappeared with discontinuation 16.
Facial rejuvenation
Procedures that aim to rejuvenate photoaged skin include:
- Fillers (hyaluronic acid, polytetrafluoroethylene, fat grafts) to disguise facial expression lines
- Botulinum toxin injections to reduce frowning and lessen deep furrows.
- Vascular laser treatment and sclerotherapy to remove facial veins and angiomas
- Resurfacing procedures (dermabrasion, chemical peels, and laser resurfacing)
- Cosmetic surgery to remove redundant sagging skin, eg, surgical or laser blepharoplasty for baggy eyelids, meloplasty (face lift) to tighten jowls
- Antiageing creams are applied to the face, neck and hands long term. These may contain:
- Sunscreens
- Fruit acids
- Vitamin-C
- Topical retinoids
- Growth factors
Fillers
Fillers (implants) can be injected under the skin to disguise crows’ feet lines, whistle lines and some scars. These include:
- Collagen
- Hyaluronic acid
- Fat
The use of various hyaluronic acid (Restylane® and Perlane®) and collagen (Cosmoderm® and Cosmoplast®) for filling creases, wrinkles, and scars have become increasingly popular. Fillers are versatile, and can also be used to enhance fullness of the lips. These fillers have proven effective and safe, and has created competition in the market and has advanced new filler technologies, resulting in varied choices for consumers 19.
The drawback of fillers is that its effects are temporary as the body absorbs the fillers over time, requiring retreatment to maintain the same appearance. Collagen treatments generally last from 3 to 6 months, while hyaluronic acids tend to last longer at 6 to 12 months. New competitors, Evolence®, Radiesse®, and Artecoll® have been used for many years in the United States, Europe, and Israel. Here is a brief introduction to some of these products.
- Artecoll® is a filler material that is used to enhance and correct lines and creases or augment the lips, and is long-lasting, often lasting for several years. Artecoll® stimulates the body’s natural collagen production, where the substance is injected. The procedure is incremental, conducted over several small treatments several months apart, so that the Artecoll® blends in well with your skin. This can be an advantage to those who wish to treat their skin in a discrete manner, as the improvement will not be sudden and noticeable, as other surgical procedures can be.
- Evolence® is a long lasting, and well tolerated for of collagen. Prior skin testing is not required for this treatment. The effects can last up to 12 months, and can be used to treat any part of your body.
- Radiesse® is an injectable filler that is particularly effective for filling in deep creases on the face. It is also used to treat frown lines on the forehead. One of the benefits of Radiesse® is that it lasts for up to 18 months.
- BOTOX® treatments can be combined with fillers, to treat permanent frown line creases, or more severe and deeper lines. In these cases, BOTOX® is used to relax the muscles that are responsible for the frowning look, while the filler corrects the creases.
The availability of new filler products give consumers and dermatologists a wide range of choices in facial rejuvenation and general skin treatment.
Dermal fillers and augmentation procedures
Dermal fillers and other implants are used for facial augmentation. They can be chosen for reconstructive or cosmetic purposes. It has become increasingly popular for the ‘normal’ everyday person to seek dermal fillers to fill in acne scars and facial lines or to enhance a specific facial area. Dermal fillers are injected just below the skin surface. Other materials are implanted in the subcutaneous area to restore or replace fat 20.
Over the years many filling agents have been developed. However, the search is still on for the ideal facial implant material.
What are dermal fillers and other implants used for ?
Dermal fillers and facial implants can be used in reconstructions for areas that may have been scarred or altered by trauma. This may be done in conjunction with minor or major plastic surgery. The other increasing use of dermal fillers is in cosmetic surgery where patients seek these treatments to improve their appearance.
They are mainly used for the removal or improvement of scars caused by acne, correction of facial (wrinkle) lines, and enhancement or filling in of certain specific facial features such as the lips or chin.
Facial lines and features that can be corrected using dermal fillers:
- Frown lines (glabellar lines)
- Smoker’s lines (perioral lines)
- Marionette lines (oral commissures)
- Worry lines (forehead lines)
- Crow’s feet (periorbital lines)
- Deep smile lines (nasolabial furrows)
- Smile lines (nasolabial lines)
- Cheek depressions
- Lip enhancement
- Witch’s chin (chin augmentation)
- Acne scars
- Facial scars
What products are available ?
There are numerous substances that add bulk to tissue. The decision as to which you should use will depend on what you are trying to achieve and on the expert advice of your health practitioner. Each has their place and specific uses in facial augmentation.
The following are injectable augmentation products:
- Collagen (excluding Alloderm®)
- Hyaluronic acid
- Polymethyl-methacrylate (PMMA)
- Hydrophilic polyacrylamide gel
- Poly-L-lactic acid
These products provide facial augmentation with less downtime. Collagen and hyaluronic acid provide only a temporary solution as they are reabsorbed into the body over time (3 to 12 months); top-up treatments are necessary to maintain the desired correction. PMMA and hydrophilic polyacrylamide gel are recent additions of injectable augmentation products and give more long-lasting results (months to years).
Side effects from using facial implants
All dermal fillers and facial implants currently used have some side effects that preclude them from being the ideal agent. Some of the side effects and complications that may occur include:
- tenderness, bleeding and bruising
- Lumps, nodules, overcorrection, blue appearance from too superficial injection
- allergic reactions
- non-allergic inflammatory reactions eg granulomatous reactions weeks to years after injection: nonpainful lumps
- numbness due to nerve palsy
- vascular injury
- infections e.g., reactivation of herpes virus, staphylococcal infection, infectious granulomas and biofilms: painful fluctuating lump
- movement or extrusion of implant
Botulinum toxin injections (Botox)
Botox®, manufactured by Allergan Inc., belongs to a class of drugs called botulinum toxins, which derive from the bacterium Clostridium botulinum 21. Although there are seven different types of botulinum toxin (A, B, C1, D, E, F, and G), most of the research conducted to date has focused on type A—called BTX-A, manufactured as Botox®.
The bacterium produces a protein that blocks the release of acetylcholine, which normally transmits messages from the nerves to the muscles to make them contract and move. Once transmission has been blocked, muscles relax, providing relief to patients with overactive muscles, reducing spasms and pain. The effect is completely reversible and generally lasts for a few months in most clinical uses.
Botox® has been officially approved only for use in the treatment of frown lines, many physicians have used it for a number of other cosmetic areas for years. It has been found effective in smoothing out horizontal lines in the forehead, crow’s feet, mouth frown, dimpled chins, and lines on the neck (Carruthers A 2001). Botox® is now being used in more artistic manners, to lift the brow and shape eyebrows (Huang 2000; Carruthers A 2001; Fagien 2001), widen the eyes to produce a more rounded look 22, shape the jaw and sides of the face 23, and to balance asymmetrical features (due to injury or surgery).
In addition, studies have found that the addition of Botox® to traditional cosmetic surgery or other procedures (such as laser resurfacing) enhances the result 24.
Botox: Side Effects and Safety
As with any medication, potential side effects of Botox® do exists, and vary according to injection site, dose, frequency of injections, and the amount of physician expertise. Most side effects— such as pain, tenderness, or bruising at the injection site—are temporary and occur within a few days after treatment.
The most common side effects of injections around the eyes and in the face include temporary bruising, eyelid drooping (ptosis), dry eyes, and double vision (diplopia) 25, 26, and facial droop can occur with injections into the cheek. It is generally agreed that in the hands of experienced physicians, these side effects are considered rare.
Potential complications when using Botox® in the face and neck occur when too much toxin is injected or when the right amount is injected into the wrong muscle. Inaccurate injections in the forehead or around the eyes can cause drooping lids; too much injected in the neck can cause muscle weakness and difficulty swallowing. In general, when used at recommended doses by skilled physicians, Botox® is safe and is not known to cause any long-term side effects.
What long-term clinical data exist show a medication with a good record of safety. In a study of 65 patients who received repeated injections for 10 years, side effects were all temporary and mild and decreased after repeated injections 27. Examination of the eye muscles after Botox® has shown that repeated injections do not cause irreversible muscle atrophy (wasting) or any other degenerative changes 28, and muscle function after injection reverts to normal 29. A large study of 235 patients who received Botox® injections for cervical dystonia, hemifacial spasm, and blepharospasm showed a 75% benefit from treatment for up to 10 years. Although side effects occurred in 27% of study participants at any one time, only 1.3% stopped receiving injections because of intolerable adverse effects 25.
Resurfacing
Resurfacing refers to surgical or laser procedures that take off the top layer of skin, smoothing it out.
- Skin needling
- Chemical peels
- Dermabrasion
- Ablative laser resurfacing
- Nonablative resurfacing: e.g., fractional laser treatment, intense pulsed light and radiothermoplasty.
Skin needling
Skin needling is also called micro-needling therapy or collagen induction therapy. It is a minimally-invasive non-surgical and nonablative procedure for facial rejuvenation that involves the use of a micro-needling device to create controlled skin injury 30.
As each fine needle punctures the skin, it creates a channel or micro-wound. The controlled injury triggers the body to fill these micro-wounds by producing new collagen and elastin in the papillary dermis. In addition, new capillaries are formed. This neovascularisation and neocollagenesis following treatment leads to reduction of scars and skin rejuvenation, i.e., improved skin texture, firmness and hydration.
There are various skin needling devices including Dermaroller® (Dermaroller GmbH); Dermapen™ (Equipmed Pty Ltd; Australia) Derma-Stamps™ (Dermaroller USA) and radial discs incorporating fine microneedles of various diameter and length, fabricated from a wide range of materials such as silicon, glass, metals, and polymers. The needles are up to 3 mm in length.
Professional skin needling is considered to be one of the safest skin treatment procedures. Unlike chemical peels, dermabrasion and laser treatments, skin needling causes minimal damage to the skin.
What is skin needling used for ?
Skin needling is effectively used for:
- Reducing scars (including hypertrophic scars) caused by acne, surgery or thermal burns
- Fading stretch marks
- Reducing fine lines and deep wrinkles
- Dyspigmentation e.g in melasma
- Tightening sagging skin.
Microneedle technology also offers a minimally invasive and painless route of transdermal drug administration e.g. vaccines. This technology, is currently being investigated by several research groups and companies. To enhance transdermal drug transport, microneedles can be inserted into the skin to increase its permeability, after which the drug is applied (poke with patch). Drugs could also be coated onto the microneedles and then inserted into the skin (coat and poke). Hollow microneedles are used to inject drug solutions into the skin.
Benefits of skin needling
- Reduced risk of hyperpigmentation and scarring therefore safe on ethnic or dark skin.
- Suitable for thin and sensitive skin
- The treatment can be performed in an office setting and does not need any extensive special training or expensive instruments.
- The procedure is well tolerated and well accepted by the patients,
- It is cost-effective, and can be done on areas of skin not suitable for peeling or laser resurfacing, such as near eyes.
- As opposed to ablative laser resurfacing, the epidermis remains intact and is not damaged. For this reason, the operation can be safely repeated if needed.
- Treatment does not result in a line of demarcation between treated and untreated skin, as usually occurs with other resurfacing procedures. This allows for specific areas of scarring to be treated without the need to “blend” or “feather” at the treatment edges.
- The patient can resume regular activities within a few days, depending on the depth of penetration of the needles. Treatment options like laser resurfacing or dermabrasion are often associated with considerable morbidity and downtime from daily activities of the patient in the post-treatment period.
What is the skin needling procedure like ?
The procedure is well tolerated. It takes a few minutes up to an hour to complete, depending on the area to be treated and the severity of the problem.
- No lotions, makeup or other topical products are applied on the treatment area on the day of the procedure.
- The medical professional then applies a numbing cream (topical) on the treatment area or injects local anaesthetic.
- The skin is punctured in a specific pattern using a skin needling device. The device is rolled over the skin multiple times for best results.
- As each fine needle punctures the skin, it creates a channel or micro-wound stimulating skin cell regeneration.
- Depending on the condition treated it may take 5-60 minutes to complete the procedure.
- A minimum of six weeks is recommended between two treatments as it takes that long for new natural collagen to form.
Postprocedure care
- Skin needling is well tolerated by patients but dryness, scaling, redness and swelling may be seen after treatment, lasting for several days or longer, depending on the depth of penetration of the needles.
- Sun protection for several weeks is recommended.
- In the case of acne scars, after the skin needling procedure, the face should be cleaned with a gentle cleanser before bed. The next day, the face may be cleansed and makeup, lotions and other topical products applied as usual.
- As the microholes close quickly, postoperative wound infection is rare.
- Emollients or antibiotic creams may be prescribed, if considered necessary.
- Rejuvenation of skin may be seen as soon as 2 weeks and as long as 6-8 months after the medical procedure.
- Burn scars are slow to respond. It can take up to 6 months to 1 year to see the final results from a single treatment.
Practical tips
- Good quality instruments should be used; there are many instruments from different companies. Using poor instruments may lead to breakage of needles in the skin.
- The patient should be counselled that multiple sessions may be needed.
- Other treatments such as subcision (surgical procedure using a needle to cut fibrous bands between fat lobules), and punch elevation may need to be combined for optimal results in acne scarring.
- Application of local anaesthetic cream can prevent procedure pain and help in performing the procedure properly.
How many skin needling procedures does one need ?
The number of needling procedures depends on the individual skin condition. Three to four treatments may be needed for moderate acne scars. Scars from Thermal burns and stretch marks (striae) may require up to 5 procedures.
In the case of wrinkles associated with ageing skin, one or two refresher skin needling treatments are recommended every year.
Specially designed home skin needling models with short fine needles (0.2 mm depth) may be used 2-3 times per week to:
- reduce pore size
- reduce oil levels in the skin (seborrhoea)
- help to reduce wrinkles and fine lines
- enhance delivery and effectiveness of medical grade skincare creams
- minimise acne outbreaks.
Side effects from skin needling
Generally the treated areas recover rapidly from skin needling. However there are occasional side effects, which include:
- Oozing and swelling during the recovery phase.
- Skin infection with bacteria (rare) or herpes simplex virus (cold sores).
- Milia, which can be easily removed.
- Acne flare, which is usually mild.
Chemical peels
A chemical facial peel refers to the application of one or more chemicals to the face which ‘burn’ off damaged cells 31.
Chemical peels are sometimes applied to other sites such as the hands. They may be used to treat damage caused by exposure to the sun (photoageing), to remove pigmentation such as freckles and melasma and fine lines and wrinkles.
A peel removes several layers of sun damaged skin cells, leaving fresh skin which has a more even surface and color. It may stimulate new collagen to be formed improving skin texture. Peels may result in superficial, moderate depth or deep skin injury.
A nurse or aesthetician (beauty therapist) may perform superficial peels. A dermatologist or plastic surgeon usually performs moderate to deeper peels.
Peels can be repeated as necessary; some people have superficial peels every few weeks. It is wise to wait 3 to 6 months before repeating a moderate depth peel.
Glycolic acid, salicylic acid and Jessner peels result in superficial skin injury and are well tolerated – the ‘lunchtime’ peel. They remove thin lesions on the skin surface, reducing pigment and surface dryness. The result of the first peel may be disappointing, but after repeated peels, significant improvement is usually evident.
Trichloracetic acid (TCA) is the most common chemical used for a medium depth peel. The results depend on its concentration, usually 20 to 35%. The treatment is painful and treated areas are swollen, red and crusted for the next week or so. It can lead to an impressive improvement in skin texture with a reduction in blotchy pigmentation, freckling and actinic keratoses (dry sunspots). Although fine wrinkles and some acne scars are less obvious, the TCA peel has no effect on deep furrows.
Phenol results in deep skin injury. It is rarely used for facial peels nowadays because of the risk of scarring and because of its toxicity. Absorption of phenol through the skin results in potentially fatal heart rhythm disturbances and nerve damage. However, it is very effective at improving both surface wrinkles and deep furrows. After a phenol peel, the treated skin is pale and smooth but it may be waxy and “mask-like”.
Before the peel
It is essential to assess the patient’s needs and skin type prior to the peel. Determine whether the peel is required for a focal lesion or for the entire face. Undertake a pre-peel classification.
- Fitzpatrick skin phototype: lighter peels are undertaken in darker skin because of the risk of postinflammatory pigmentation
- Previous experience of skin peels
- Tendency for skin to develop increased and/or loss of pigmentation at the sites of skin injury
Pre-treatment creams are applied to the face at night for several weeks prior to the peel. By exfoliating the skin and reducing pigmentation themselves, they improve the results seen from chemical peeling. They may also reduce the time needed for healing. The creams usually include one or more of the following:
- Tretinoin
- Alpha hydroxy acid e.g. glycolic or lactic acid
- Hydroquinone for tanned or dark skinned patients or those with melasma
Broad spectrum SPF 50+ sunscreen should be used during the day.
The peel
Superficial chemical peels are a minor procedure and no special arrangements are needed. But you may need painkillers, sedation, local anaesthetic or even a general anaesthetic for deeper peels.
First the face is thoroughly washed to remove surface oil. The peeling agent is then applied for several minutes. It stings – how badly and for how long depends on the chemical, its concentration, whether you’ve had pre-treatment with aspirin, and individual factors. A fan can help. The peel is then neutralised, and the burning sensation lessens.
Individual treatments may include peels with several agents on the same occasion, with the aim of improving results and reducing risks.
Antibiotics and oral antiviral agents may be recommended after deeper peels.
What happens after the peel ?
Superficial peels result in mild facial redness and occasional swelling which usually resolve within 48 hours. The peeling is similar to sunburn. Most people can continue their normal activities. Make-up can be applied a few hours after the procedure.
Moderate depth peels result in intense inflammation and swelling, which resolve within a week. The peeling is more marked. Mild redness can persist for several weeks. Most people take a week off from work after a moderate depth peel.
Looking after the skin after the peel
- Keep treated areas cool (use a water spray).
- Do not pick! Picking delays healing and causes scarring
- Moisturise – use light preparations after a superficial peel, thicker moisturisers after a deeper peel
- Protect from the sun – especially for the first 6 months
- If advised to do so, continue to use tretinoin, glycolic acid and/or hydroquinone at night long term
Complications of chemical peels
Complications are uncommon if the health professional performing the peel is properly trained and experienced.
- Comedones (blocked pores) or acne may result from the peel itself or from thick moisturisers used afterwards; ask your dermatologist for treatment.
- Infection due to bacteria (Staphylococcus aureus), yeast (Candida albicans), or virus (Herpes simplex); you may need antibiotics.
- Scarring may result from infection or picking the scabs, and can be permanent.
- Blotchy pigmentation is most likely in those with darker skin or who had a pigmentation problem before the peel; keep out of the sun and use hydroquinone.
- Persistent actinic keratoses may require treatment. Your dermatologist may choose cryotherapy, 5-fluorouracil cream or biopsy a lesion in case it is skin cancer.
Dermabrasion
Dermabrasion is a skin resurfacing technique that is used to treat facial scarring. When it was first developed in the early 1950’s it was used predominantly to improve acne scars, chicken pox marks and scars resulting from accidents or disease. Nowadays, dermabrasion is also used to treat deep facial lines and wrinkles, severe sun damage, pigmentation disorders and certain types of skin lesions 32.
Dermabrasion equipment
Dermabrasion is a surgical procedure that uses a power-driven hand held tool that looks a bit like a dentist’s drill. The tool has an abrasive end piece such as a serrated metal wheel, diamond fraise, or a wire brush. Fraises come in a variety of shapes, sizes and grades of coarseness. The doctor moves the rapidly spinning wheel gently over the surface of the scar causing the topmost layers of the skin to be worn away.
Preparation for dermabrasion
Before you can receive dermabrasion, your doctor will take a complete medical history and will carefully examine the skin lesion or defect. The doctor will need to know the following factors:
- Skin type – mid range skin types (III-IV) that tan easily are more likely to show transient hyperpigmentation (dark marks) 4-8 weeks after the surgery and hypopigmentation (pale marks) 12-18 months post surgery. However, discolouration can be a problem with all skin types.
- Tendency to form keloids (deposits of fibrous tissue) or hypertrophic scarring – patients with a history of keloid formation may need to have a test spot performed first before any full face resurfacing.
- Herpes simplex lesions (cold sores) – active herpes infection usually necessitates postponement of the procedure until the lesions have cleared.
- Other active facial skin diseases such as acne, rosacea and dermatitis – these may flare after dermabrasion.
- Recent isotretinoin therapy – this can delay healing and cause scarring so dermabrasion should be postponed for 6-12 months.
The doctor will tell you about the procedure, possible risks and complications and what results might realistically be expected. Photographs are usually taken before and after surgery to help evaluate the degree of improvement.
Medical treatment for dermabrasion
Dermabrasion can precipitate herpes simplex infection causing unpleasant blistering and possibly permanent scarring so aciclovir, famciclovir or valacyclovir tablets are used to prevent it. Those with a history of cold sores may require larger doses than normal.
Most patients are only prescribed antibiotics if infection occurs after the procedure. The exceptions are immunosuppressed patients or patients with a recent history of impetigo, or who are carriers of Staphylococcus aureus, who may be started on antibiotics beforehand.
For two to three weeks prior to dermabrasion, tretinoin cream may be prescribed to apply each night to the area to be treated. Tretinoin appears to decrease the time for reepithelialization (new skin growth).
Dermabrasion may be perfomed using general anaesthetic but local anaesthetic may be preferred for small areas. Sedating medications may be used to induce a calming effect prior to and after surgery.
Dermabrasion procedure
Dermabrasion may require admission to hospital or it may be done as an outpatient procedure in a doctor’s surgery. The procedure begins with thoroughly cleaning the area to be ‘sanded’ with antiseptic cleansing agent. A numbing spray may be applied to freeze and firm the surface that is being treated. The doctor will then carefully manoeuvre the dermabrasion tool over the area to carefully remove layers of skin until he/she reaches the desired level that will make the scar or wrinkle less visible, aiming to avoid more scarring.
For small areas the procedure should only take a few minutes. For larger areas, the procedure can take 1-2 hours to perform.
Care after dermabrasion
Following the procedure the treated skin will be red, swollen and tender. A compress or special dressing is usually applied to reduce any tingling, burning or stinging sensation and to speed up healing. Instructions will be given on caring for the wound until new skin starts to grow; this usually takes 7-10 days. The face may itch as the new skin grows and may be slightly swollen, sensitive, and bright pink for several weeks after dermabrasion.
The following measures should be taken to ensure rapid healing and prevent any complications.
- Inform your doctor of any yellow crusting or scabs – this may be the start of an infection.
- Swelling and redness should subside after a few days to a month. Persistent redness of an area could be the sign of a scar forming so contact your doctor immediately.
- Continue antiviral medication for several days beyond the new skin forming.
- To avoid pigmentation, once the new skin is healed, keep out of the sun and apply a broad spectrum sunscreen daily for at least 3 months after dermabrasion. Even the sun through window-glass can promote unwanted pigmentation.
Microdermabrasion
Microdermabrasion was developed in Italy in 1985 and has since become a popular skin resurfacing technique. It has the advantages of low risk and rapid recovery compared with other techniques such as standard dermabrasion, chemical peeling and laser resurfacing.
Microdermabrasion is similar to dermabrasion but as its name suggests, it uses tiny crystals to remove the surface skin layers. It is promoted for correcting fine lines and more superficial scars.
Advantages include:
- Anaesthesia is not required
- It is almost painless
- Facial redness is minimised
- Simple and quick to perform
- Can be repeated at short intervals
- Does not disrupt the patient’s life greatly
The disadvanges of microdermabrasion are that multiple treatments are needed and there may be minimal improvement in appearance.
Microdermabrasion is now possible using home kits that use virbating foam applicator to massage a moisturising cream containing aluminium oxide crystals on the surface of the skin.
Laser resurfacing
Over the last 20 years there have been major advances in the field of nonsurgical skin rejuvenation. With advances in laser technology it is now possible to reduce, and in some cases remove, facial wrinkles, acne scars and other facial scars, and a variety of skin growths and blemishes with minimal disruption and downtime for the patient.
Who is suitable for laser resurfacing ?
People with mild, moderate or severe facial wrinkles and sun-damaged skin can all benefit from laser resurfacing. Those who are concerned about the risks of complications, and who wish to avoid long recovery times are the best candidates for non-ablative laser resurfacing. However, they must understand that results may not be as effective as ablative resurfacing.
All wrinkles are reduced, but those caused by the sun, especially those around the eyes and lips respond best. It is never too late – or too early – to treat wrinkles once they are established. Acne scars and facial scars from surgery or trauma may be reduced but very deep scars cannot be completely removed. Many benign skin growths and scaly patches on the face and elsewhere are removed with ease.
Dark skinned and tanned patients may experience some dyspigmentation of the skin after treatment with non-ablative laser therapy. A test spot should be performed in these patients and they should avoid direct sunlight and use sunscreens after treatments.
What are the results ?
In most cases the results are a moderate to marked reduction in facial lines and wrinkles, a more even skin tone and texture, and fresher, healthier-looking skin. Ablative laser resurfacing therapy produces the best result and is still considered the gold standard against which all other facial rejuvenation systems are compared. Although the results with non-ablative laser therapy are not as significant as those seen with ablative laser therapy it has the huge advantage of low risk and rapid recovery.
Ablative laser resurfacing
The procedure does provide a general ‘lift’ to the face, but a face lift is necessary to reverse advanced sagging of the skin of the face. Wrinkles on the lips and around the eyes usually do not respond to face lifting but respond well to laser resurfacing. In some instances both procedures are necessary to achieve the best results.
Ablative laser treatments are typically more painful than non-ablative laser treatments. When treating small areas topical anaesthetic agents are usually applied when using ablative laser systems. For larger procedures, in addition to topical anaesthetics, injectable or inhaled local or regional anaesthetics may also be used.
Ablative laser resurfacing is associated with a long post-recovery period. There may be swelling, redness, exudation and sloughing of the treated area. For the first few days’ treatment with ice packs and keeping the head raised at night should help. Healing is greatly aided by the use of a skin-coloured adhesive dressing for the first couple of days. In some cases an occlusive healing ointment is preferred as it improves patient comfort and has shown to speed up the growth of new skin. Usually it takes two weeks to heal completely, with a range from one to four weeks depending on the treatment performed and the depth of skin removal. After two weeks, it is possible to wear camouflage make-up. Sun protection with a non-irritating sunscreen is vital until the redness subsides completely.
Nonablative resurfacing
Non-ablative laser systems target only the dermis, leaving the epidermis intact. The results are not as effective as with ablative laser resurfacing but the excellent safety profile and rapid recovery post-treatment have made these systems are popular. These systems have been divided into 3 main groups, mid-infrared lasers and the two visible light lasers, the pulsed dye laser (PDL) and intense pulsed light (IPL) systems.
Non-ablative laser resurfacing is minimally painful and may not require any anaesthesia. If necessary, topical anaesthetic agents are used and applied one hour before the start of the procedure. Cold packs may also be applied immediately after treatment to minimise any discomfort.
The huge advantage of non-ablative laser resurfacing is that there is little, if any post-recovery period. In most cases patients can apply makeup and return to normal daily life immediately following treatment.
Surgery
Surgery is necessary to disguise or remove sagging and loose skin.
- Full face lift includes muscle/facial tightening for jowls
- Neck lift for loose skin and muscles of the neck
- Temporal lift or endoscopic forehead lift for sagging of the forehead and eyebrow
- Blepharoplasty to remove baggy eyelids.
- Ageing skin. https://www.dermnetnz.org/topics/ageing-skin/[↩][↩]
- Gupta AK, Gover MD, Nouri K, et al. The treatment of melasma: a review of clinical trials. J Am Acad Dermatol 55(6):1048-65;2006 Dec.[↩]
- Alpha Hydroxy Acids and Their Potential. http://www.skininformation.com/articles/page.php?id=21[↩][↩]
- A brief lesson in vitamin C for the skin. http://www.skininformation.com/tips/page.php?id=161[↩]
- Bissett DL, Miyamoto K, Sun P, et al. Topical niacinamide reduces yellowing, wrinkling, red blotchiness, and hyperpigmented spots in aging facial skin. Int J Cosmet Sci 26(5):231-8;2004 Oct.[↩]
- Bissett DL, Oblong JE, Berge CA. Niacinamide: A B vitamin that improves aging facial skin appearance. Dermatol Surg 31(7 Pt 2):860-5;2005 Jul.[↩]
- Beitner H. Randomized, placebo-controlled, double blind study on the clinical efficacy of a cream containing 5% alpha-lipoic acid related to photoageing of facial skin. Br J Dermatol 149(4):841-9 (2003 Oct[↩]
- Cosmetic Ingredient Review Expert Panel.Safety assessment of salixylic acid, butyloctyl salicylates, calcium salicylates, C12-15 Alkyl salicylates, capryloyl salicylic acid, hesyldodecyl salicylates, isocetyl salicylates, isodecyl salicylates, magnesium salicylates, MEA salicylates, ethylhexyl salicylates, potassium salicylates, methyl salicylate, sodium salicylates, TEA-salicylate, and tridecyl salicylate. Int J Toxicol 22(Suppl 3):1-108;2003.[↩]
- Buraczewska I, Berne B, Lindberg M, et al. Changes in skin barrier function following long-term treatment with moisturizers, a randomized controlled trial. Br J Dermatol 156(3):492-8;2007 Mar.[↩]
- Topical retinoids. https://www.dermnetnz.org/topics/topical-retinoids/[↩]
- Sorg O, Antille C, Kaya G, et al. Retinoids in cosmeceuticals. Dermatol Ther 19(5):289-96;2006 Sep-Oct[↩]
- Oblong JE, Bissett DL. Retinoids. In: Draelos ZD, ed. Cosmeceuticals. Philadelphia: Elsevier Saunders pp 36-42;2005.[↩]
- Mukherjee S, Date A, Patravale V, et al. Retinoides in the treatment of skin aging: an overview of clinical efficacy and safety. Clin Interv Aging 1(4):327-48;2006.[↩]
- Khanna S, Venojarvi M, Roy S, et al. Dermal wound healing properties of redox-active grape seed proanthocianidins. Free Radic Biol Med 33(8):1089-96;2002 Oct 15.[↩]
- Bagchi D, Bagchi M, Stohs SJ, et al. Free radicals and grape seed proanthocyanidin extract: importance in human health and disease prevention. Toxicology 148(2-3):187-97;2000 Aug.[↩]
- Badreshia-Bansal S, Draelos ZD. Insight into skin lightening cosmeceuticals for women of color. J Drugs Dermatol 6(1):32-9;2007 Jan.[↩][↩]
- Rendon MI, Gaviria JI. Skin lightening agents. In: Draelos ZD, ed. Cosmeceuticals. Philadelphia: Elsevier Saunders pp 103-9;2005.[↩]
- Dermal Safety. In: Gillner M, Moore GS, Cederberg H, et al. Environmental Health Criteria 157. Published under the joint sponsorship of the United Nations Environment Programme, the International Labour Organisation, and the World Health Organization. Available at: http://www.inchem.org/documents/ehc/ehc/ehc157.htm[↩]
- Important Filler Facts. http://www.skininformation.com/articles/page.php?id=18[↩]
- Dermal fillers and augmentation procedures. https://www.dermnetnz.org/topics/dermal-fillers-and-augmentation-procedures/[↩]
- Botox: Background. http://www.botoxfacts.ca/background.html[↩]
- Carruthers A, Carruthers J. Botulinum toxin type A: History and current cosmetic use in the upper face. Semin Cutan Med Surg 2001;20:71-84.[↩]
- Park MY, Ahn KY, Jung DS. Application of botulinum toxin A for treatment of facial contouring in the lower face. Dermatol Surg 2003;29:477-483.[↩]
- Fagien S, Brandt FS. Primary and adjunctive use of botulinum toxin type A (Botox) in facial aesthetic surgery : Beyond the glabella. Clin Plast Surg 2001;28 :127-148.[↩]
- Hsiung GY, Das SK, Ranawaya R, Lafontaine AL, Suchowersky O. Long-term efficacy of botulinum toxin A in treatment of various movement disorders over a 10-year period. Mov Disord 2002;17:1288-1293.[↩][↩]
- Tan NC, Chan LL, Tan EK. Hemifacial spasm and involuntary facial movements. QJM 2002;95:493-500.[↩]
- Defazio G, Abbruzzese G, Girlanda P, et al. Botulinum toxin A treatment for primary hemifacial spasm: A 10-year multicenter study. Arch Neurol 2002;59:418-420.[↩]
- Borodic GE, Ferrante R. Effects of repeated botulinum toxin injections on orbicularis oculi muscle. J Clin Neuroophthalmol 1992;12:121-127.[↩]
- De Paiva A, Meunier FA, Molgo J, Aoki KR, Dolly JO. Functional repair of motor endplates after botulinum neurotoxin typ A poisoning: Biphasic switch of synaptic activity between nerve sprouts and their parent terminals. Proc Natl Acad Sci USA 1999;96:3200-3205.[↩]
- Skin needling. https://www.dermnetnz.org/topics/skin-needling/[↩]
- Chemical peels. https://www.dermnetnz.org/topics/chemical-peels/[↩]
- Dermabrasion. https://www.dermnetnz.org/topics/dermabrasion/[↩]





{kind=link}