
Contents
What is cystic hygroma
A cystic hygroma also called lymphangioma, lymphatic malformation or cavernous lymphangioma, is a benign congenital (present at birth) malformation of the lymphatic system consisting of a fluid-filled sac that results from a blockage in the lymphatic system that occurs in infant or children younger than 2 years of age 1). Cystic hygroma also known as water-tumor, is a benign malformation of lymphatic vessels which usually occurs when the lymphatic system fails to communicate with the normal jugular vein. It can occur in the head, neck, axilla, cervico-facial regions, groin, and below the tongue 2). Cystic hygroma are locally aggressive, benign lesions that are difficult to manage due to recurrence of the tumor following surgery with a recurrence rate of 21% 3). Cystic hygroma is usually histologically characterized by the proliferation of small lymphatic vessels with intervening fibrous tissue 4).
Cystic hygroma is most commonly located in the neck or head area, but can be located anywhere in the body. Cystic hygroma may be discovered in a fetus during a pregnancy ultrasound, or it may be apparent at birth as a soft bulge under the skin. When it is identified on pregnancy ultrasound, there is an increased risk for miscarriage. In some cases, it is not discovered until a person is older 5). Symptoms can vary depending on its size and specific location, and it can potentially cause problems with nearby structures or organs 6).
Cystic hygroma could be classified into septated (multiloculated) or nonseptated single cavity (nonloculated) types 7). There are three histological subtype of lymphangioma’s. Capillary cystic hygroma (composed of small lymphatics), cavernous cystic hygroma (composed of larger lymphatics), cystic cystic hygroma (cystic hygroma-composed of large macroscopic lymphatic spaces with collagen and smooth muscle). Cavernous cystic hygroma is the most common subtype 8).
A cystic hygroma may be caused by genetic or environmental factors that cause abnormal development of the lymphatic vascular system during embryonic growth. It may occur on its own or as part of a genetic syndrome with other features, such as Turner syndrome, Down syndrome or Noonan syndrome 9). In adults it may result from trauma, or from earlier respiratory infections 10). In many cases, the cause is not known 11).
Cystic hygromas are benign lesions and can remain asymptomatic in a patient for long duration. The indications of treatment are recurrent bouts of infection in the lesion, respiratory distress, dysphagia, haemorrhage inside cystic hygroma, sudden increase in the size of lesion, lymph discharging sinus and disfigurement. The respiratory distress can be of severe nature necessitating a tracheostomy due to complete or significant laryngeal or tracheal compressions by external and sometimes laryngeal cystic hygromas 12).
Treatment involves removing the cystic hygroma, although removing all of it may not be possible. Furthermore, cystic hygromas can often grow, making it impossible to remove all of the tissue. Other treatments that have been tried with limited success include chemotherapy, injection of sclerosing medicines, radiation therapy, and steroids 13).
Other treatments have been tried with only limited success. These include:
- Chemotherapy medicines
- Injection of sclerosing medicines
- Radiation therapy
- Steroids
The prognosis is good if surgery can totally remove the abnormal tissue. In cases where complete removal is not possible, the cystic hygroma commonly returns.
The long-term outcome may also depend on what other chromosomal abnormalities or birth defects, if any, are present.
Cystic hygroma in adults
Although cystic hygroma is well recognized in pediatric practice, it seldom presents de novo in adulthood 14). Cystic hygroma is very rare in adults, but it should be considered in the differential diagnosis of adult neck swellings. The cause of cystic hygroma in the adult population is controversial. Some authors attribute adult lymphangioma to delayed proliferation of the congenital or acquired lymphoid rests following trauma or preceding respiratory infections 15).
Most commonly cystic hygromas occur in the head and neck (80% of cases), although they have been described in a variety of other anatomical locations such as axilla (20%), mediastinum (5%), groin, retroperitoneal space and groin 16). Most lymphangiomas are asymptomatic. They have no gender predilection and present as a painless mass that progressively enlarges. Typically, the mass is soft, nontender and ill-defined. Symptoms may develop when the lymphatic malformation enlarges to where it compresses surrounding tissue. There may be obstructive symptoms such as dysphagia, dysphonia, and airway obstruction, however, this is rare in adults 17). Patients presenting with a painless, soft, fluctuant, and enlarging neck mass should have a careful history and physical examination along with radiological imaging to assist with diagnosis.
Until date, there have been fewer than 150 reports of adult cervicofacial cystic hygroma in the English language literature and the optimum management of these lesions is still a matter of debate 18). Diagnosis in adults is considered to present a greater challenge than in children, and final diagnosis is usually based on postoperative histology 19).
Surgical intervention is the treatment of choice for this rare condition 20). Complete excision of a cystic hygroma has been shown to have an 81% cure rate. When only part of a lymphatic malformation is excised, there is an 88% recurrence rate 21).
Cystic hygroma in fetus
Cystic hygroma in fetus or fetal cystic hygroma is a congenital (present at birth) malformation of the lymphatic system. The lymphatic system is a network of vessels that maintains fluids in the blood, as well as transports fats and immune system cells. Cystic hygromas are single or multiple cysts found mostly in the neck region 22). The defect results from failure of the embryonic lymphatic sacs to connect with the venous system during the development of the lymphatic system 23). Epidemiological studies have reported the prevalence of fetal cystic hygroma to be 1.1–5.3 per 10,000 births, and dependent on maternal age, race, residence, and sex 24). However, if stillbirth and elective terminations are included, the prevalence reaches 30 per 10,000 births, according to a hospital-based study 25). The growing incidence observed over recent decades is ascribed to the routine use of prenatal ultrasound screening 26).
Fetal cystic hygroma typically develops between late in the first trimester to early in the second trimester. Cystic hygroma in fetus usually occurs in the neck and axillary region 27). In the fetus, a cystic hygroma can progress to hydrops (an excess amount of fluid in the body) and eventually lead to fetal death. Some cases resolve leading to webbed neck, edema (swelling), and a lymphangioma (a benign yellowish-tan tumor on the skin composed of swollen lymph vessels). In other instances, the hygroma can progress in size to become larger than the fetus.
Cystic hygromas can be classified as septated (multiloculated) or nonseptated (simple). It is believed that a septated cyst results from complete obstruction of the lymphatic sacs, preventing communication with the jugular venous system and causing large multilocular cysts; while a nonseptated cyst results from temporary accumulation due to incomplete obstruction of lymphatic drainage 28).
Cystic hygromas can occur as an isolated finding or in association with other birth defects as part of a syndrome (chromosomal abnormalities or syndromes caused by gene mutations). Nine percent of cases occur in healthy children, while 2% occur in liveborns but with chromosome abnormalities 29) or various malformations 30). The majority of prenatally diagnosed cystic hygromas are associated with Turner syndrome or other chromosomal abnormalities like trisomy 21, 18, and 13 31). Isolated cystic hygroma can be inherited as an autosomal recessive disorder 32). Fetal cystic hygroma may result from environmental factors (maternal virus infection or alcohol abuse during pregnancy), genetic factors, or unknown factors.
Prenatal diagnosis by sonography and chromosome test provides parents the opportunity to terminate the abnormal fetus 33). Prenatal diagnosis is always made by ultrasound during the nuchal translucency test. About 70–80% of cystic hygromas occur in the neck 34), while the remaining 20–30% of the cystic hygromas occurs in the axillary region and other rare locations 35).
Fetal cystic hygroma have being treated with OK-432, a lyophilized mixture of Group A Streptococcus pyogenes and benzyl penicillin, and with serial thoracocentesis plus paracentesis 36).
Figure 1. Cystic hygroma ultrasound
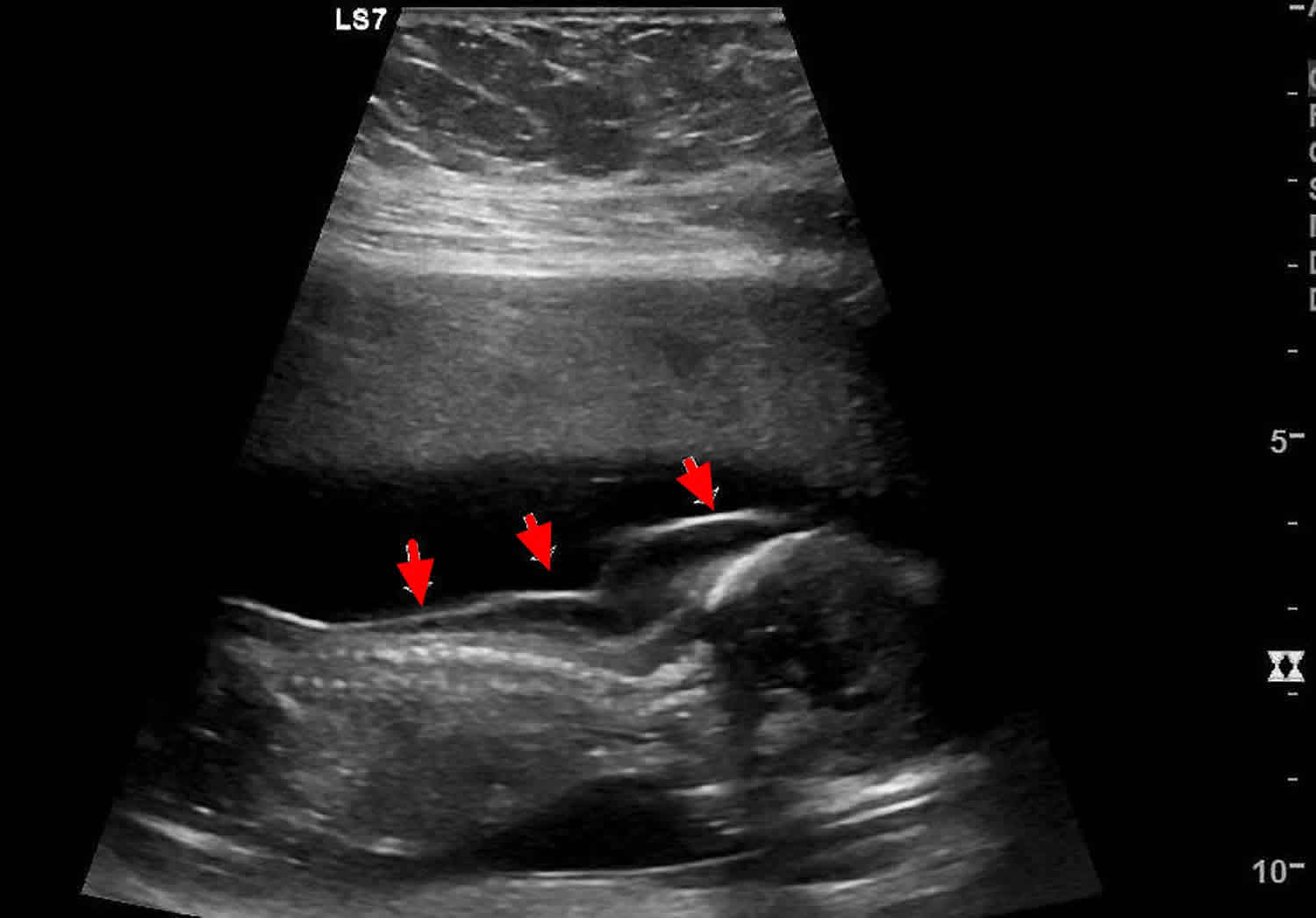
Footnote: Single live intrauterine fetus shows a cystic lesion involving posterior cervical region. It shows extension to thoracic region. There are multiple septa within the lesion. Rest of the fetal anatomical survey was normal for maturity which corresponded to the period of amenorrhea (13 wks 6 days).
[Source 37) ]Figure 2. Cystic hygroma of lumbar region

Fetal cystic hygroma survival rate
Sixty-two percent of cystic hygromas were associated with chromosomal abnormalities 39). The most common type is Turner syndrome, but other abnormalities include: trisomies 21, 18, and 13 40). A large proportion of infants and fetuses with cystic hygroma also have other structural abnormalities. The survival rate of liveborn babies with cystic hygroma is poor 41). Only 9% of cases result in healthy children with normal karyotypes, while the rest with chromosome or physical abnormalities are either terminated (89%) or liveborn (2%) 42). Thus chromosome examination should be recommended for cystic hygroma due to its association with poor outcome.
The cystic volume is not a determinant predictor for prognosis 43). Some cases with massive hygromas persist until surgical correction after birth 44). Their prognosis depends on infiltration of surrounding structures rather than size 45). The septa also cannot be considered as a reliable prognostic indicator. Compared with nonseptated cystic hygromas, septated cysts are thought to be more likely aneuploid, and less likely to be liveborn 46). Later studies do not concur with this 47), therefore, even if a cyst is massive and septated, close follow-up is still worthwhile when a chromosome test is normal 48). Other structural abnormalities, for example, cardiac defect, should be sought out carefully.
Malone et al 49) proposed step-by-step prenatal counseling when a diagnosis of septated cystic hygroma starts in the first trimester. Initial counseling should be set up immediately after sonographic diagnosis, and an overall risk of chromosome abnormality of one in two should be noted. A second counseling session should be offered after confirmation of a normal fetal karyotype. Then, a residual risk of one in two of a major structural fetal abnormality or spontaneous fetal death should be noted. After detailed fetal anatomical sonography, patients with normal findings can then be said to have a 95% chance of a promising perinatal outcome 50). Magnetic resonance imaging could be safe and helpful in distinguishing the extent of invasion of lymphangioma if necessary 51).
The favored treatment for cystic hygroma is complete surgical excision 52). Local recurrence is common when the tumor has infiltrated the subcutaneous layer. Cystic hygromas confined to the superficial dermis are more amenable to surgical correction, with a high rate of success. Recent advances in sclerotherapy have expanded contemporary lymphangioma management options 53). Sasaki and Chiba 54) had a promising experience with intrauterine treatment of a cystic hygroma with OK-432, a lyophilized mixture of Group A Streptococcus pyogenes and benzyl penicillin. However, Ogita et al 55) reported two cases of failure when it came to large septated tumors. Regular skin examination should be included in the follow-up treatment to evaluate recurrence and the response to treatment 56).
Cystic hygroma causes
A cystic hygroma may be caused by genetic or environmental factors that cause abnormal development of the lymphatic vascular system during embryonic growth. It may occur on its own or as part of a genetic syndrome with other features, such as Turner syndrome, Down syndrome or Noonan syndrome. In adults it may result from trauma, or from earlier respiratory infections. In many cases, the cause is not known.
Cystic hygroma diagnosis
Sometimes, a cystic hygroma is seen using a pregnancy ultrasound when the baby is still in the womb. This can mean that the baby has a chromosomal problem or other birth defects.
The following tests may be done:
- Chest x-ray
- Ultrasound
- CT scan
- MRI scan
If the cystic hygroma is detected during a pregnancy ultrasound, other ultrasound tests or amniocentesis may be recommended.
Cystic hygroma signs and symptoms
The signs and symptoms of a cystic hygroma can vary depending on its size and location. A common symptom is a neck growth. It may be found at birth, or discovered later in an infant after an upper respiratory tract infection (such as a cold). Regardless of size, a cystic hygroma can potentially cause functional impairment of nearby structures or organs, as well as disfigurement of affected areas 57). When identified after birth, it most often looks like a soft bulge under the skin 58). The overlying skin may have a bluish tint 59). The cystic hygroma typically grows as the child grows, and may become apparent after a sudden increase in size, due to an infection or bleeding within the cyst 60). Feeding difficulties and failure to thrive may be present. Rarely, a child with a cystic hygroma may have symptoms of obstructive sleep apnea. Other symptoms or complications may include airway obstruction, hemorrhage, infection, or deformation of surrounding bony structures or teeth (if it is left untreated) 61).
Cystic hygroma possible complications
Cystic hygromas are benign lesions; however, complications may arise. These lesions can get infected any time. The usual source of infection is seedling of microorganisms from a secondary focus of infection (respiratory tract infections), though they may get infected primarily also. During the course of infection, the cystic hygroma increases in size and becomes warm, red and tender. The patient may become febrile. The infection may involve entire cystic hygroma or a few of its cysts (Figure 3). During active infection, it may not remain transluminant. Sometimes cystic hygroma turns into an abscess, which needs to be drained for amelioration of the symptoms. The treatment is conservative with antibiotics, antipyretics and analgesics 62).
The other most frequently reported and observed complication is spontaneous bleeding in the cyst. In this case, the cysts get tense and hard. On aspiration, they yield haemorrhagic fluid. Spontaneous haemorrhage in the scrotal lymphangioma may have to be dealt surgically to avoid testicular ischemia 63). Kaur et al. 64) reported spontaneous rupture, on the fourth day after birth, of a giant cystic hygroma of neck, necessitating urgent surgical intervention.
The other complications include respiratory difficulties and dysphagia, especially in cystic hygroma of neck and oral cavity. Sometimes, the cystic hygroma of neck and oral cavity occurs concurrently in the same patient; thus, creating a difficult situation for the management of respiratory distress and dysphagia. Lymph discharging sinus, resulting from infection or trauma is another rare complication 65).
Cystic hygroma complications may include:
- Bleeding
- Damage to structures in the neck caused by surgery
- Infection
- Return of the cystic hygroma
Figure 3. Cystic hygroma of neck and oral cavity. The lower portion of cystic hygroma was infected

Cystic hygroma prognosis
The long-term outlook (prognosis) associated with a cystic hygroma may depend on when the cystic hygroma is detected, the size and location of the lesion, whether complications arise, and whether an underlying syndrome or chromosome abnormality is present. If surgery to remove the lesion is successful and all affected tissue is removed, the prognosis reportedly is good 67). If residual tissue is left behind, the recurrence rate is approximately 15% 68).
Cystic hygromas detected prenatally on ultrasound are associated with an increased risk for chromosome abnormalities (particularly Down syndrome) and birth defects (particularly heart defects). Both of these increase the risk for miscarriage, hydrops, fetal demise, and neonatal death. Increasing size is associated with an increasing risk of an underlying abnormality 69).
As a person with a cystic hygroma ages, morbidity is often related to cosmetic disfigurement and how the cystic hygroma affects other critical structures, such as nerves, blood vessels, lymphatics, and the airway 70). Quality of life can be significantly impaired in many cases. Recurrent inflammation can lead to cellulitis, which can cause pain and disfigurement of the affected area. Bleeding in the lesion can cause rapid pain, hardening, and swelling or enlargement of the affected area 71). Complications from surgery may also occur, and depending on the location may include damage to neurovascular structures (including cranial nerves), chylous fistula or chylothorax (leakage of lymphatic fluid), or hemorrhage 72). Specific possible complications, and areas of the head or body affected, will vary from person to person.
Some studies have reported an associated mortality rate of up to 2-6%, usually due to pneumonia, bronchiectasis, or airway compromise 73).
Cystic hygroma treatment
Treatment options for a cystic hygroma depend on the size, location and symptoms present. Options may include surgery (recommended when possible), percutaneous drainage, sclerotherapy, laser therapy, radiofrequency ablation, or medical therapy. These different treatment options may be used in various combinations. When surgery removes all abnormal tissue, the chance of complete recovery is good. If complete removal is not obtained, the cystic hygroma will often return. In very rare cases, a cystic hygroma will shrink or go away without treatment.
Surgical care
The mainstay of treatment of cystic hygromas is surgical excision 74). Although surgery is the criterion standard for treatment, both the operating team and the family of the patient should go forward with the knowledge that cystic hygroma is a benign lesion. If acute infection occurs prior to resection, surgery should be delayed at least 3 months.
The surgical team should attempt to remove the cystic hygroma completely or, failing that, to remove as much as possible, sparing all vital neurovascular structures. Complete excision has been estimated to be possible in roughly 40% of cases.
Cystic hygromas are ideally removed in a single procedure because secondary excisions are complicated by fibrosis and distorted anatomic landmarks.
Microcystic lesions are much more difficult to remove because of their intimate association with nearby tissues. Laser therapy is a recent advancement in the treatment of microcystic lesions.
The exceptions to excision at the time of diagnosis are few and include premature infants who are small in size and those with involvement of crucial neurovascular structures that are small and difficult to identify (eg, facial nerve). If no airway obstruction is present, surgery can be delayed until the child is aged 2 years or older, especially when the operation will be around the facial nerve in the parotid area.
Signs of airway obstruction necessitate surgical evaluation at the time of diagnosis. In emergency situations, aspiration with an 18-gauge or 20-gauge needle may obviate the need for an emergency tracheostomy.
Although traditional wisdom has dictated that lymphatic malformations not be aspirated, a study by Burezq et al 75) documented success with serial aspiration of cystic hygroma. In this series, 14 patients were treated with aspiration alone (three needed multiple aspirations), with a mean follow-up of 5.75 years. No failures were reported. This technique may hold promise for the future management of cystic hygroma. Other authors contend that aspiration has no role and believe that aspiration is often followed by recurrence, hemorrhage, or infection.
Radiofrequency ablation (RFA) has been advocated for use with intraoral lymphatic malformations, especially microcystic lesions. Kim et al 76) reported high long-term success rates with radiofrequency ablation (median follow-up, 47 months), with 81% of patients not requiring further treatment.
Magnetic resonance–controlled laser-induced interstitial thermotherapy is a newer therapy that has been proposed for treatment of cystic hygroma.
Cystic hygroma can present on routine prenatal ultrasonography as a large obstructing airway mass, as can other pathologic conditions (e.g., teratoma or rhabdomyosarcoma). If such a mass is visible on ultrasonography, MRI should be performed to delineate the mass further. In these cases, a multispecialty team, including a high-risk obstetrician, pediatric otolaryngologist, pediatric surgeon, and neonatologist, should be present at the ex-utero intrapartum treatment procedure.
A planned cesarean delivery is performed, and intubation or tracheostomy is used to establish an airway. Extracorporal membrane oxygenation (ECMO) should also be available. Excision of the cystic hygroma is delayed until the child is stable. Intrauterine cyst aspiration to facilitate vaginal delivery has been reported in the literature.
Surgical Complications
Complications from surgical excision of an cystic hygroma are myriad and are related to the location and structures adjacent to the mass; these include the following:
- Damage to a neurovascular structure (including cranial nerves)
- Chylous fistula
- Chylothorax
- Hemorrhage
- Recurrence – Most recurrences develop within the first year, but some have arisen as long as 10 years after excision
Medical treatment
Medical treatment of cystic hygromas consists of the administration of sclerosing agents, such as OK-432 (an inactive strain of group A Streptococcus pyogenes), bleomycin, pure ethanol, bleomycin, sodium tetradecyl sulfate, and doxycycline 77).
An infected cystic hygroma should be treated with intravenous antibiotics, and definitive surgery should be performed once the infection has resolved. Incision and drainage or aspiration results in only temporary shrinkage, and subsequent fibrosis can further complicate the resection. Radiotherapy has not been demonstrated to be effective. Some authors advocate that the preferred treatment of all cystic hygromas is surgical resection, positing that only resection can truly offer the potential for cure.
OK-432
Although not currently approved by the US Food and Drug Administration (FDA), OK-432 has been reported to be capable of successfully treating cystic hygroma 78). The mechanism of action is proposed to be an inflammatory response to the inactive bacteria, leading to fibrosis of the hygroma. OK-432 may be a viable option for large unilocular cysts.
Currently, OK-432 is available in the United States only by protocol. It does not work well for small cysts 79). Because the procedure for using OK-432 involves aspiration prior to injection of the sclerosant, some have hypothesized that the true effect is from the aspiration.
Bleomycin
Bleomycin is considered a poor choice because of its toxicity (pulmonary fibrosis); cystic hygroma is a benign disease, and other less toxic treatment options are available. Niramis et al studied 70 patients who underwent sclerotherapy with bleomycin; 83% obtained an excellent or good result, 43% had adverse reactions, and three patients died 80).
Sainsbury et al studied 75 patients, 83% of whom had a complete or significant response. Five adverse reactions were reported, with no severe morbidity or mortality (to include pulmonary fibrosis) 81).
Alcohol
Absolute alcohol as a sclerosing agent has been used with some success in some patients; alcohol works well in vascular malformations. Imperizzilli et al studied computed tomography (CT)-guided ethanol injection and obtained complete resolution in seven of eight patients without complications 82).
Interferon alfa-2a
This has been used in the treatment of hemangiomas, and its use has been proposed in lymphangiomas. However, its efficacy has never been documented, and it carries a serious side-effect profile 83).
Fibrin sealant
The use of a fibrin sealant after aspiration of cystic hygroma has been reported in the literature 84).
Doxycycline
Doxycycline has been reported as a potential sclerotherapy agent, with both safety and efficacy. Like most other sclerosant agents, it has shown the highest efficacy in macrocystic lesions and the lowest efficacy in microcystic ones 85).
Sildenafil
A limited case series has been reported using sildenafil for severe lymphatic malformations. A prospective trial has been performed, which did not demonstrate a significant effect on cystic hygroma 86).
Sirolimus
Sirolimus has been utilized in several small series, but the optimal dose and duration have not been identified 87).
References [ + ]





{kind=link}