
Contents
What is DCIS
DCIS (ductal carcinoma in situ), also called intraductal carcinoma and Stage 0 breast cancer. DCIS is a non-invasive or pre-invasive breast cancer, meaning it hasn’t spread out of the milk duct to invade other parts of the breast. Ductal carcinoma in situ (DCIS) means the cells that line the milk ducts have changed to cancer cells, but they have not spread through the walls of the ducts into surrounding breast tissue. DCIS is considered the earliest form of breast cancer.
Because DCIS hasn’t spread into the breast tissue around it, it can’t spread (metastasize) beyond the breast to other parts of the body.
DCIS is considered non-invasive or pre-invasive breast cancer. DCIS can’t spread outside the breast, but it still needs to be treated because it can sometimes go on to become invasive breast cancer (which can spread).
DCIS is usually found during a mammogram (x-rays of the breast) done as part of breast cancer screening or when there is another concern with a woman’s breast. Because of increased screening with mammograms, the rate at which DCIS is diagnosed has increased dramatically in recent years. Currently, more than 60,000 patients are diagnosed with DCIS in the United States each year 1.
While DCIS isn’t life-threatening, it does require treatment to prevent the condition from becoming invasive. It is estimated that women who have had DCIS are 4–12 times more likely to develop subsequent invasive breast cancer despite adequate treatment. No reliable factors have been identified which predispose people with DCIS to subsequently develop invasive breast cancer but the risk may be higher when the DCIS lesion displays certain microscopic features.
Most women with DCIS are cured with proper treatment. Treatment may include:
- Lumpectomy. This is a type of breast-conserving surgery (also called breast-sparing surgery). This may be followed by radiation therapy.
- Mastectomy. This is surgery to remove the breast or as much of the breast tissue as possible.
- Tamoxifen. This drug may also be taken to lower the chance that DCIS will come back after treatment or to prevent invasive breast cancer.
In most cases, a woman with DCIS can choose between breast-conserving surgery and radiation or simple mastectomy. But sometimes a mastectomy might be a better option.
Is DCIS cancer?
Yes. DCIS is Stage 0 breast cancer. Ductal carcinoma in situ (DCIS) means the cells that line the milk ducts have changed to cancer cells, but they have not spread through the walls of the ducts into surrounding breast tissue. Because DCIS hasn’t spread into the breast tissue around it, it can’t spread (metastasize) beyond the breast to other parts of the body.
DCIS is considered a pre-cancer because sometimes it can become an invasive cancer. This means that over time, DCIS may spread out of the duct into nearby tissue, and could metastasize (spread). Right now, though, there’s no good way to know for sure which will become invasive cancer and which ones won’t. So almost all women with DCIS will be treated.
Figure 1. Normal breast (female)
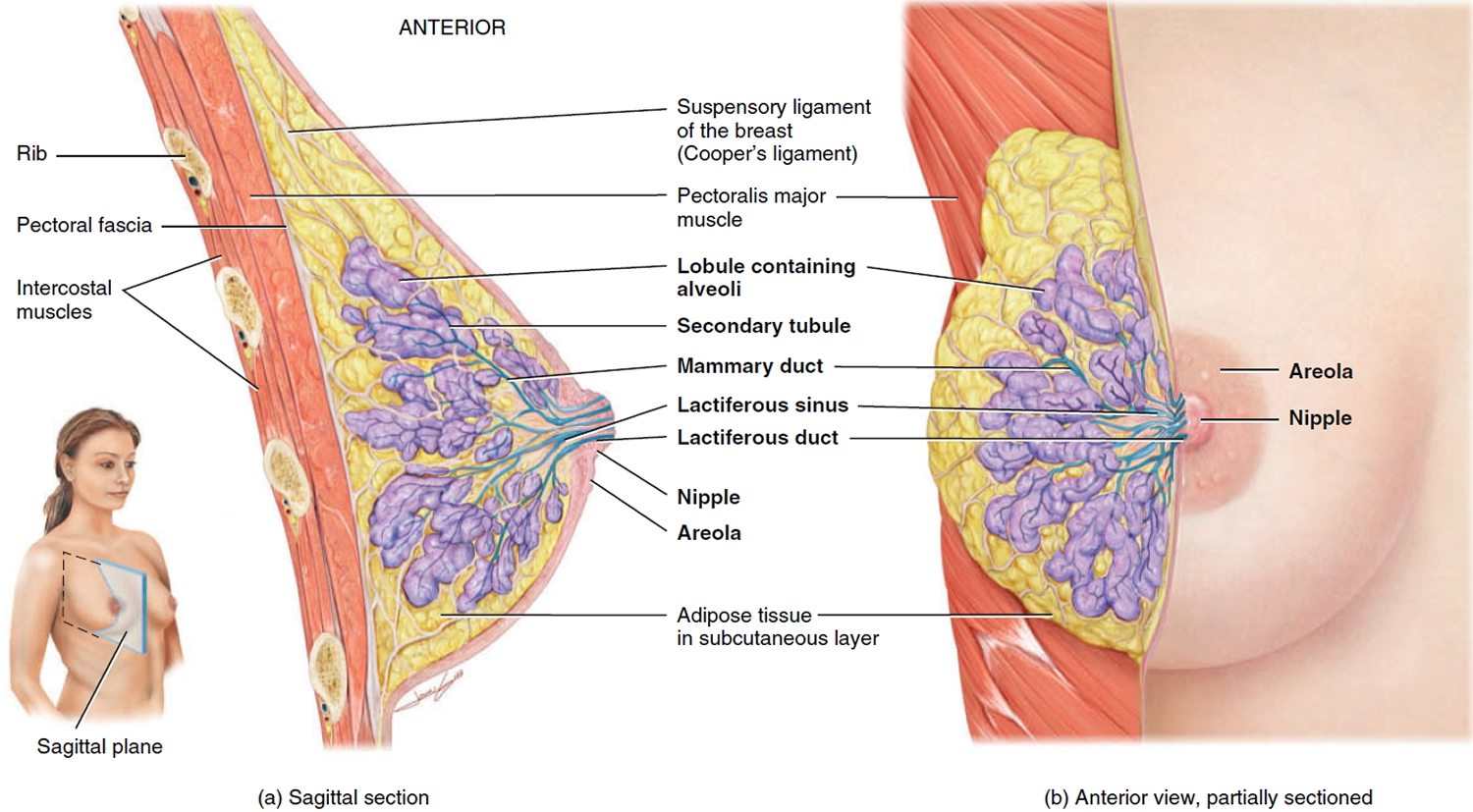
Figure 2. DCIS (Ductal Carcinoma In Situ)
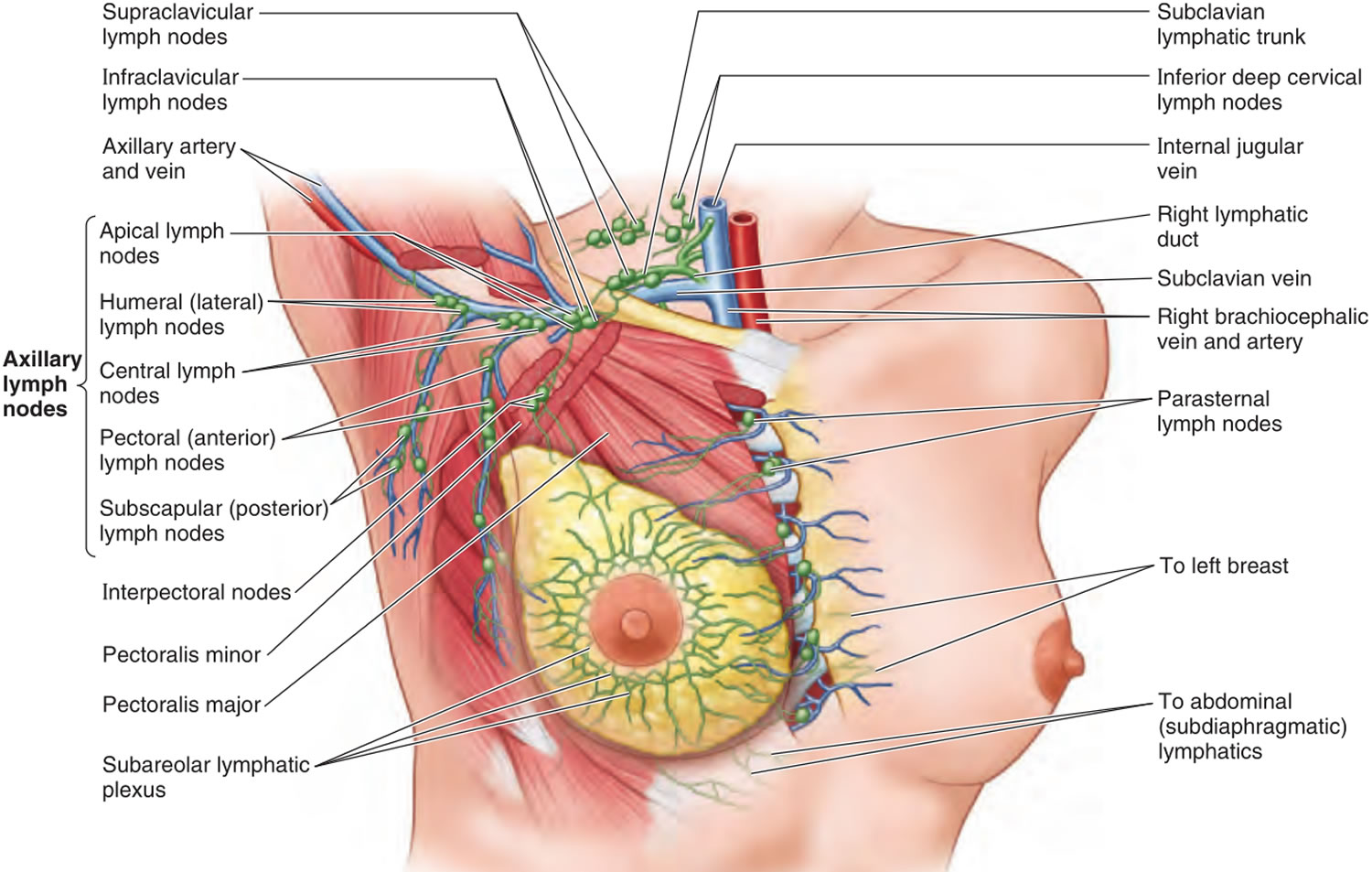
Figure 3. Lymph nodes associated with breast cancer spread
 DCIS prognosis
DCIS prognosis
The prognosis of DCIS depends on various factors including tumor size, grade (how abnormal tumor cells look on microscopy) and histology of the tumor (how the tumor appears under a microscope), margin width (represents completeness of excision) and presence of necrosis (cell death) within the tumor.
Women with DCIS are at increased risk of developing invasive breast cancer in the future. However, as most cases of DCIS are now treated, it is not known exactly how high this risk is, or how quickly the progression from DCIS to invasive cancer is likely to occur.
Local recurrence (the tumor regrowing in the same area) rates of DCIS depend on the type of treatment that is implemented. There is a 1.4% recurrence rate when DCIS is treated with both conservative breast surgery and radiotherapy.
DCIS survival rate
The 5-year relative survival rate for women with stage 0 (DCIS) breast cancer is close to 100% 2.
DCIS causes
It’s not clear what causes DCIS. DCIS forms when genetic mutations occur in the DNA of breast duct cells. The genetic mutations cause the cells to appear abnormal, but the cells don’t yet have the ability to break out of the breast duct.
Researchers don’t know exactly what triggers the abnormal cell growth that leads to DCIS. It’s likely that a number of factors may play a part, including genes passed to you from your parents, your environment and your lifestyle.
Risk factors for DCIS
Factors that may increase your risk of DCIS include:
- Female gender
- Increasing age
- Personal history of benign breast diseases, such as complex fibroadenoma (non-cancerous tumor of the breast), atypical hyperplasia (accumulation of abnormal cells in a breast duct), sclerosing adenosis (excessive growth of tissues in the breast lobules) and intraductal papilloma (non-cancerous tumor of the breast duct)
- Family history of breast cancer
- First pregnancy after age 30
- Previous history of DCIS
- Taking combination estrogen-progestin hormone replacement therapy for more than three to five years after menopause. Some evidence is emerging that long term estrogen therapy (either oral contraceptive pill or hormone replacement therapy (HRT)) may increase risk
- Hormonal factors: Women who begin menstruation early, women who have experience late menopause, late or few pregnancies, or who are obese.
- A diet which is high in fat
- Genetic mutations that increase the risk of breast cancer, such as in the breast cancer genes BRCA1 and BRCA2
- Obesity
- Exposure to radiation (e.g. from x-rays or CT)
DCIS symptoms
DCIS doesn’t cause any signs or symptoms in most cases. However, DCIS can sometimes cause signs and symptoms, such as:
- A breast lump
- Changes in the skin of the breast
- Bloody nipple discharge
DCIS is usually found on a mammogram and appears as small clusters of calcifications that have irregular shapes and sizes.
DCIS diagnosis
Any breast symptom, such as a lump or nipple discharge, is assessed with the ‘triple test’. This includes examination of the breast, imaging of the breast through mammography (breast x-ray) or ultrasound, and sampling of the breast tissue with fine needle aspiration (FNA), core biopsy or open biopsy.
Breast imaging
DCIS is most often discovered during a mammogram used to screen for breast cancer. If suspicious areas such as bright white specks (microcalcifications) that are in a cluster and have irregular shapes or sizes are identified on your mammogram, your radiologist likely will recommend additional breast imaging.
You may have a diagnostic mammogram, which takes views at higher magnification from more angles, to take a closer look at the microcalcifications to be able to determine whether they are a cause for concern and to evaluate both breasts.
If the area of concern needs further evaluation, the next step may be an ultrasound and breast biopsy.
Removing breast tissue samples for testing
To collect breast tissue for testing, you may undergo one or more types of breast biopsy procedures:
- Core needle biopsy. A radiologist or surgeon uses a hollow needle to remove tissue samples from the suspicious area, sometimes guided by ultrasound (ultrasound-guided breast biopsy). The tissue samples are sent to a lab for analysis.
- Stereotactic biopsy. This type of biopsy also involves removing tissue samples with a hollow needle, but with the help of stereo images — mammogram images of the same area obtained from different angles — to find (localize) the area of concern.
- Surgical biopsy (wide local excision or lumpectomy). If results from a core needle biopsy or stereotactic biopsy show areas of DCIS, you’ll likely be referred to a surgeon to discuss your options for surgically removing a wider area of breast tissue for analysis.
A pathologist will analyze the breast tissue from your biopsy to determine whether abnormal cells are present and how aggressive those abnormal cells appear.
If your mammogram showed microcalcifications, the pathologist will examine the biopsy sample for those abnormalities.
DCIS treatment
What is the treatment for DCIS stage 0
DCIS is considered non-invasive or pre-invasive breast cancer. DCIS can’t spread outside the breast, but it still needs to be treated because it can sometimes go on to become invasive breast cancer (which can spread).
In most cases, a woman with DCIS can choose between breast-conserving surgery (BCS) and simple mastectomy. But sometimes a mastectomy might be a better option.
Breast-conserving surgery (lumpectomy)
In breast-conserving surgery (lumpectomy), the surgeon removes the tumor and a small amount of normal breast tissue around it. Lymph node removal is not always needed with breast-conserving surgery, but it may be done if the doctor thinks the area of DCIS might also contain invasive cancer. The chances an area of DCIS contains invasive cancer goes up with tumor size and how fast the cancer is growing. If lymph nodes are removed, this is usually done as a sentinel lymph node biopsy.
If breast-conserving surgery (lumpectomy) is done, it is usually followed by radiation therapy. This lowers the chance of the cancer coming back in the same breast (either as more DCIS or as an invasive cancer). Breast-conserving surgery without radiation therapy is not a standard treatment, but it might be an option for certain women who had small areas of low-grade DCIS that were removed with large enough cancer-free surgical margins.
Research suggests that women treated with lumpectomy have a slightly higher risk of recurrence than women who undergo mastectomy; survival rates between the two groups are very similar.
For older women with multiple medical conditions, lumpectomy plus tamoxifen therapy, lumpectomy alone or no treatment may be an option.
Radiation therapy
Radiation therapy uses high-energy beams, such as X-rays, to kill abnormal cells. Radiation therapy after lumpectomy reduces the chance that DCIS will come back (recur) or that it will progress to invasive cancer.
A type of radiation therapy called external beam radiation is most commonly used to treat DCIS.
Radiation is typically used after lumpectomy. But for some women, radiation may not be necessary. This might include those with only a small area of DCIS that is considered low grade and was completely removed during surgery.
Mastectomy
Simple mastectomy (removal of the entire breast) and possibly the underarm lymph nodes (sentinel node biopsy) — may be needed if the area of DCIS is very large, if the breast has several areas of DCIS, or if breast-conserving surgery cannot remove the DCIS completely (that is, the breast-conserving surgery specimen and re-excision specimens still have cancer cells in or near the surgical margins). Many doctors will do a sentinel lymph node biopsy along with the mastectomy. This is because if an area of invasive cancer is found in the tissue removed during a mastectomy, the doctor won’t be able to go back and do the sentinel lymph node biopsy later, and so may have to do a full axillary lymph node dissection.
Women having a mastectomy for DCIS may choose to have breast reconstruction immediately or later.
Because breast-conserving surgery (lumpectomy) combined with radiation is equally effective, simple mastectomy is less common than it once was for treating DCIS.
Most women with DCIS are candidates for breast-conserving surgery (lumpectomy). However, mastectomy may be recommended if:
- You have a large area of DCIS. If the area is large compared with the size of your breast, a lumpectomy may not produce acceptable cosmetic results.
- There’s more than one area of DCIS (multifocal or multicentric disease). It’s difficult to remove multiple areas of DCIS with a lumpectomy. This is especially true if DCIS is found in different sections — or quadrants — of the breast.
- Tissue samples taken for biopsy show abnormal cells at or near the edge (margin) of the tissue specimen. There may be more DCIS than originally thought, meaning that a lumpectomy might not be adequate to remove all areas of DCIS. Additional tissue may need to be excised, which could require removing the breast (mastectomy) if the area of DCIS involvement is larger relative to the size of the breast. If the area of DCIS is large, relative to the size of your breast, lumpectomy also may produce unacceptable cosmetic results.
- You’re not a candidate for radiation therapy. Radiation is usually given after a lumpectomy. You may not be a candidate if you’re diagnosed in the first trimester of pregnancy, you’ve received prior radiation to your chest or breast, or you have a condition that makes you more sensitive to the side effects of radiation therapy, such as systemic lupus erythematosus.
- You prefer to have a mastectomy rather than a lumpectomy. For instance, you might not want a lumpectomy if you don’t want to have radiation therapy.
Surgery for DCIS typically doesn’t involve removal of lymph nodes from under your arm because it’s noninvasive. The chance of finding cancer in the lymph nodes is extremely small.
If tissue obtained during surgery leads your doctor to think abnormal cells may have spread outside the breast duct or you are having a mastectomy, then a sentinel node biopsy or removal of some lymph nodes may be done as part of the surgery.
Hormone therapy after surgery
If the DCIS is hormone receptor-positive (estrogen receptors [ER-positive] or progesterone receptors [PR-positive]), adjuvant treatment with tamoxifen (for any woman) or an aromatase inhibitor (for women past menopause) for 5 years after surgery can lower the risk of another DCIS or invasive cancer developing in either breast. If you have hormone receptor-positive DCIS, discuss the pros and cons of hormone therapy with your doctors.
How does hormone therapy work?
About 2 out of 3 breast cancers are hormone receptor-positive. Their cells have receptors (proteins) that attach to the hormones estrogen (ER-positive cancers) and/or progesterone (PR-positive cancers). For these cancers, high estrogen levels help the cancer cells grow and spread.
There are several types of hormone therapy, which use different ways to keep estrogen from helping the cancer grow. Most types of hormone therapy for breast cancer either lower estrogen levels or stop estrogen from acting on breast cancer cells.
Drugs that block estrogen receptors
These drugs work by stopping estrogen from stimulating breast cancer cells to grow.
Tamoxifen
This drug blocks estrogen receptors on breast cancer cells. It stops estrogen from connecting to the cancer cells and telling them to grow and divide. While tamoxifen acts like an anti-estrogen in breast cells, it acts like an estrogen in other tissues, like the uterus and the bones. Because of this, it is called a selective estrogen receptor modulator (SERM).
Tamoxifen can be used in several ways:
- For women with hormone receptor-positive breast cancer treated with surgery, tamoxifen can help lower the chances of the cancer coming back and raise the chances of living longer. It can also lower the risk of getting a new cancer in the other breast. Tamoxifen can be started either after surgery (adjuvant therapy) or before surgery (neoadjuvant therapy) and is usually taken for 5 to 10 years. For early- stage breast cancer, this drug is mainly used for women who have not yet gone through menopause. (If you have gone through menopause, aromatase inhibitors are usually used instead.)
- For women who have been treated for ductal carcinoma in situ (DCIS) that is hormone receptor-positive, taking tamoxifen for 5 years lowers the chance of the DCIS coming back. It also lowers the chance of getting an invasive breast cancer.
- For women with hormone-positive breast cancer that has spread to other parts of the body, tamoxifen can often help slow or stop the growth of the cancer, and might even shrink some tumors.
- In women at high risk of breast cancer, tamoxifen can be used to help lower the risk of developing breast cancer.
Toremifene (Fareston) is another selective estrogen receptor modulator (SERM) that works in a similar way, but it is used less often and is only approved to treat metastatic breast cancer. It is not likely to work if tamoxifen has already been used and has stopped workingThese drugs are taken by mouth as a pill. The most common side effects of tamoxifen and toremifene are:
- Hot flashes
- Vaginal dryness or discharge
- Mood swings
Some women with cancer spread to the bones may have a tumor flare with pain and swelling in the muscles and bones. This usually decreases quickly, but in some rare cases a woman may also develop a high calcium level in the blood that is hard to control. If this happens, the treatment may need to be stopped for a time.
Rare, but more serious side effects are also possible:
- If a woman has gone through menopause, these drugs can increase her risk of developing uterine cancer. Tell your doctor right away about any unusual vaginal bleeding (a common symptom of both of these cancers). Most uterine bleeding is not from cancer, but this symptom always needs prompt attention.
- Blood clots are another uncommon, but serious side effect. They usually form in the legs (called deep vein thrombosis or DVT), but sometimes a piece of clot may break off and end up blocking an artery in the lungs (pulmonary embolism or PE). Call your doctor or nurse right away if you develop pain, redness, or swelling in your lower leg (calf), shortness of breath, or chest pain, because these can be symptoms of a DVT or PE.
- Rarely, tamoxifen has been associated with strokes in post-menopausal women, so tell your doctor if you have severe headaches, confusion, or trouble speaking or moving.
Depending on a woman’s menopausal status, tamoxifen can have different effects on the bones. In pre-menopausal women, tamoxifen can cause some bone thinning, but in post-menopausal women it is often good to strengthen bone. The benefits of taking these drugs outweigh the risks for almost all women with hormone receptor-positive breast cancer.
Treatments that lower estrogen levels
Some hormone treatments work by lowering estrogen levels. Because estrogen encourages hormone receptor-positive breast cancers to grow, lowering the estrogen level can help slow the cancer’s growth or help prevent it from coming back.
Aromatase inhibitors
Aromatase inhibitors are drugs that stop estrogen production. Before menopause, most estrogen is made by the ovaries. But for women whose ovaries aren’t working, either due to menopause or certain treatments, a small amount of estrogen is still made in the fat tissue by an enzyme (called aromatase). Aromatase inhibitors work by blocking aromatase from making estrogen.
These drugs are useful in women who are past menopause, although they can also be used in premenopausal women in combination with ovarian suppression (see below).
There are 3 aromatase inhibitors that seem to work about equally well in treating breast cancer:
- Letrozole (Femara)
- Anastrozole (Arimidex)
- Exemestane (Aromasin)
These drugs are pills taken daily.
Use in adjuvant therapy: After surgery, taking an aromatase inhibitor, either alone or after tamoxifen, has been shown to work better than taking just tamoxifen for 5 years to reduce the risk of the cancer coming back .
Schedules that are known to be helpful include:
- Tamoxifen for 2 to 3 years, followed by an aromatase inhibitor to complete 5 years of treatment
- An aromatase inhibitor for 2 to 3 years followed by Tamoxifen to complete 5 years of treatment
- Tamoxifen for 5 years, followed by an aromatase inhibitor for 5 years
- An aromatase inhibitor for 5 years
- Tamoxifen for 5 to 10 years (if you are unable to take an aromatase inhibitor)
For most post-menopausal women whose cancers are hormone receptor-positive, most doctors recommend taking an AI at some point during adjuvant therapy. Right now, standard treatment is to take these drugs for about 5 years, or to alternate with tamoxifen for a total of at least 5 years, or to take in sequence with tamoxifen for at least 3 years. Studies are now being done to see if taking an aromatase inhibitor for more than 5 years would be more helpful. Tamoxifen is an option for some women who cannot take an aromatase inhibitor. Taking tamoxifen for 10 years is considered more effective than taking it for 5 years, but you and your doctor will decide the best schedule of treatment for you.
If you have early-stage breast cancer and had not gone through menopause when you were first diagnosed, your doctor might recommend taking tamoxifen first, and then taking an aromatase inhibitor later if you go through menopause during treatment. Another option is taking a drug called a luteinizing hormone-releasing hormone (LHRH) analog, which turns off the ovaries, along with an aromatase inhibitor. An aromatase inhibitor should not be taken alone for breast cancer treatment in pre-menopausal women because it is unsafe and can increase hormone levels.
Use in cancer that comes back or has spread: aromatase inhibitors can also be used to treat more advanced hormone-positive breast cancers, especially in post-menopausal women. They are often continued for as long as they are helpful.
Possible side effects: The AIs tend to have fewer serious side effects than tamoxifen. They don’t cause uterine cancers and very rarely cause blood clots. They can, however, cause muscle pain and joint stiffness and/or pain. The joint pain may be similar to a feeling of having arthritis in many different joints at one time. Switching to a different aromatase inhibitor may improve this side effect, but it has led some women to stop treatment. If this happens, most doctors recommend using tamoxifen to complete 5 to 10 years of hormone treatment.
Because aromatase inhibitors drastically lower the estrogen level in women after menopause, they can also cause bone thinning, sometimes leading to osteoporosis and even fractures. If you are taking an AI, your bone density may be tested and you may also be given drugs, such as bisphosphonates or denosumab, to strengthen your bones.
Ovarian suppression
For pre-menopausal women, removing or shutting down the ovaries (ovarian suppression), which are the main source of estrogen, effectively makes them post-menopausal. This may allow some other hormone therapies, such as aromatase inhibitors, to be used.
There are several ways to remove or shut down the ovaries to treat metastatic breast cancer, as well as some women with early-stage disease:
- Oophorectomy: Surgery to remove the ovaries. This is a form of permanent ovarian ablation.
- Luteinizing hormone-releasing hormone (LHRH) analogs: These drugs are used more often than oophorectomy. They stop the signal that the body sends to the ovaries to make estrogen, which causes temporary menopause. Common LHRH drugs include goserelin (Zoladex) and leuprolide (Lupron). They can be used alone or with other hormone drugs (tamoxifen, aromatase inhibitors, fulvestrant) as hormone therapy in pre-menopausal women.
- Chemotherapy drugs: Some chemo drugs can damage the ovaries of pre-menopausal women so they no longer make estrogen. Ovarian function returns months or years later in some women, but in others the damage to the ovaries is permanent and leads to menopause. This side effect can sometimes be a helpful (if unintended) consequence of chemotherapy with regard to breast cancer treatment.
All of these methods can cause symptoms of menopause, including hot flashes, night sweats, vaginal dryness, and mood swings.
Less common types of hormone therapy
Some other types of hormone therapy that were used more often in the past, but are rarely given now. These include:
- Megestrol acetate (Megace), a progesterone-like drug
- Androgens (male hormones)
- High doses of estrogen
These might be options if other forms of hormone therapy are no longer working, but they can often cause side effects.
Coping and support
A diagnosis of DCIS can be overwhelming and frightening. To better cope with your diagnosis, it may be helpful to:
- Learn enough about DCIS to make decisions about your care. Ask your doctor questions about your diagnosis and your pathology results. Use this information to research your treatment options. Look to reputable sources of information, such as the National Cancer Institute (https://www.cancer.gov/), to find out more. This may help you feel more confident as you make choices about your care.
- Get support when needed. Don’t be afraid to ask for help or to turn to a trusted friend when you need to share your feelings and concerns. Talk with a counselor or medical social worker if you need a more objective listener. Join a support group — in your community or online — of women going through a situation similar to yours.
- Control what you can about your health. Make healthy changes to your lifestyle, so you can feel your best. Choose a healthy diet that focuses on fruits, vegetables and whole grains. Try to be active for 30 minutes most days of the week.
- Get enough sleep each night so that you wake feeling rested. Find ways to cope with stress in your life.





 causes, symptoms, diagnosis, survival rate, prognosis, treatment. DCIS can’t spread outside the breast, but it still needs to be treated because it can sometimes go on to become invasive breast cancer (which can spread).){kind=link}