Contents
What is dislocated elbow
A dislocated elbow occurs when the bones that make up the elbow joint are forced out of alignment — typically when you land on an outstretched hand during a fall. The elbow is the second most commonly dislocated joint after the shoulder in adults, and the most commonly dislocated joint in children.
Elbow dislocations can be complete or partial, and usually occur after a trauma, such as a fall or accident. In a complete dislocation, the elbow joint surfaces are completely separated. In a partial elbow dislocation, the elbow joint surfaces are only partly separated. A partial dislocation is also called a subluxation.
A simple elbow dislocation does not have any major bone injury.
A complex elbow dislocation can have severe bone and ligament injuries.
In the most severe elbow dislocations, the blood vessels and nerves that travel across the elbow may be injured. If this happens, there is a risk of losing the arm.
Some people are born with greater laxity or looseness in their ligaments. These people are at greater risk for dislocating their elbows. Some people are born with an ulna bone that has a shallow groove for the elbow hinge joint. They have a slightly higher risk for dislocation.
Toddlers may experience a dislocated elbow, sometimes known as pulled elbow or nursemaid’s elbow, if they are lifted or swung by their forearms.
If you or your child has a dislocated elbow, seek immediate medical attention. Complications can occur if the dislocated elbow pinches or traps the blood vessels and the nerves that serve the lower arm and hand.
A dislocated elbow can usually be realigned without surgery. However, if your elbow is also fractured, you might need surgery.
The Elbow Joint
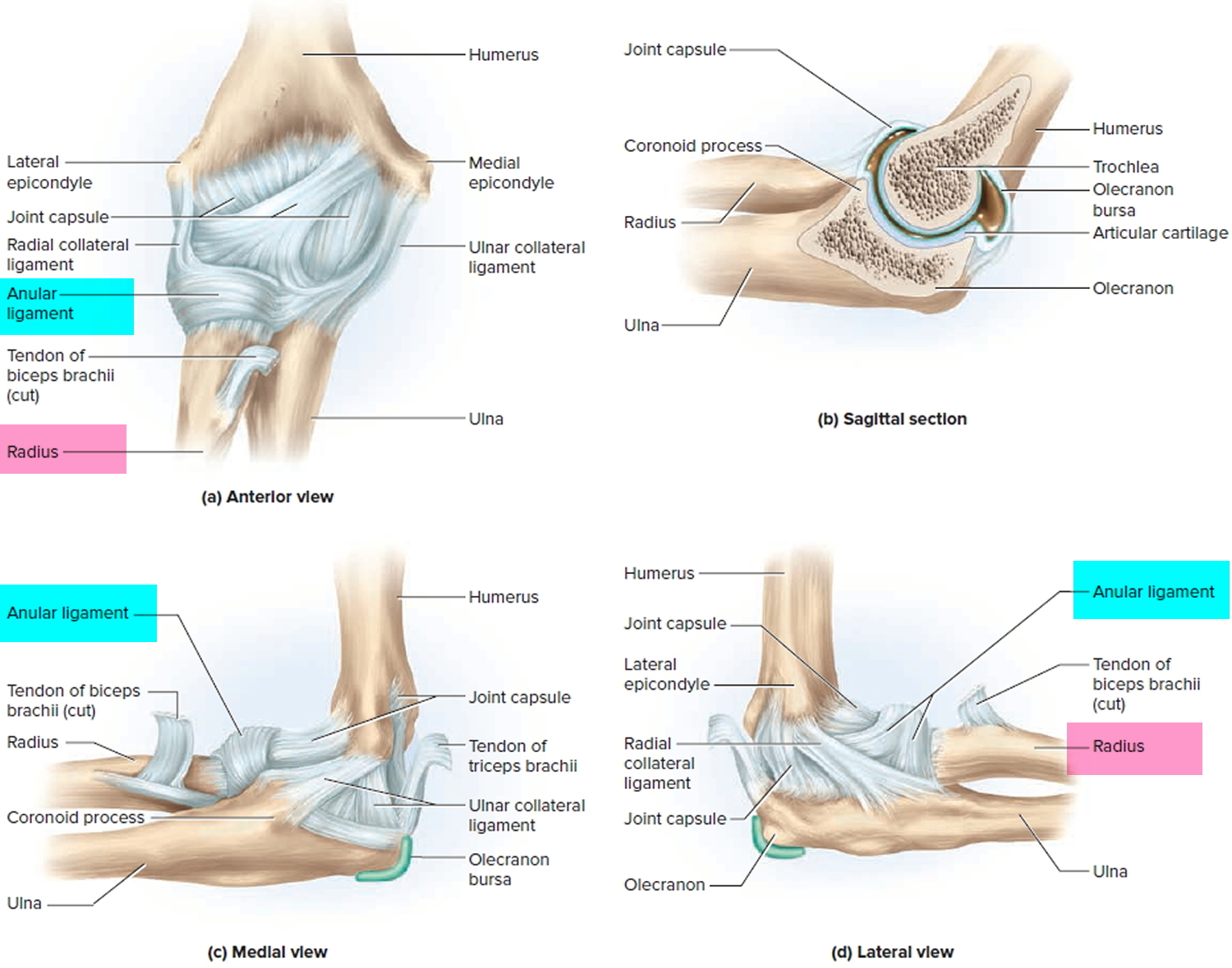
Three bones come together to make up the elbow joint. The humerus is the bone in the upper arm. Two bones from the forearm (the radius and the ulna) form the lower part of the elbow. Each of these bones has a very distinct shape.
Ligaments connected to the bones keep the elbow joint together and the bones in proper alignment. Side-to-side motions of the elbow joint are restricted by a pair of ligaments: the radial (lateral) collateral ligament and ulnar (medial) collateral ligament.
The elbow is both a hinge joint and a ball and socket joint. As muscles contract and relax, two unique motions occur at the elbow.
- Bending occurs through a hinge joint that allows the elbow to bend and straighten. This is called flexion and extension, respectively.
- Rotation occurs though a ball and socket joint that allows the hand to be rotated palm up and palm down. This is called supination and pronation, respectively.
Injuries and dislocations to the elbow can affect either of these motions.
Another joint occurs in the elbow region, the proximal radioulnar joint, but it is not involved in the hinge. At this joint, the edge of the disclike head of the radius fits into the radial notch of the ulna. It is held in place by the anular ligament, which encircles the radial head and is attached at each end to the ulna. The radial head rotates like a wheel against the ulna as the forearm is pronated or supinated.
The elbow is stable because of the combined stabilizing effects of bone surfaces, ligaments, and muscles. When an elbow dislocates, any or all of these structures can be injured to different degrees.
Figure 1. Elbow joint
Dislocated elbow toddler and child
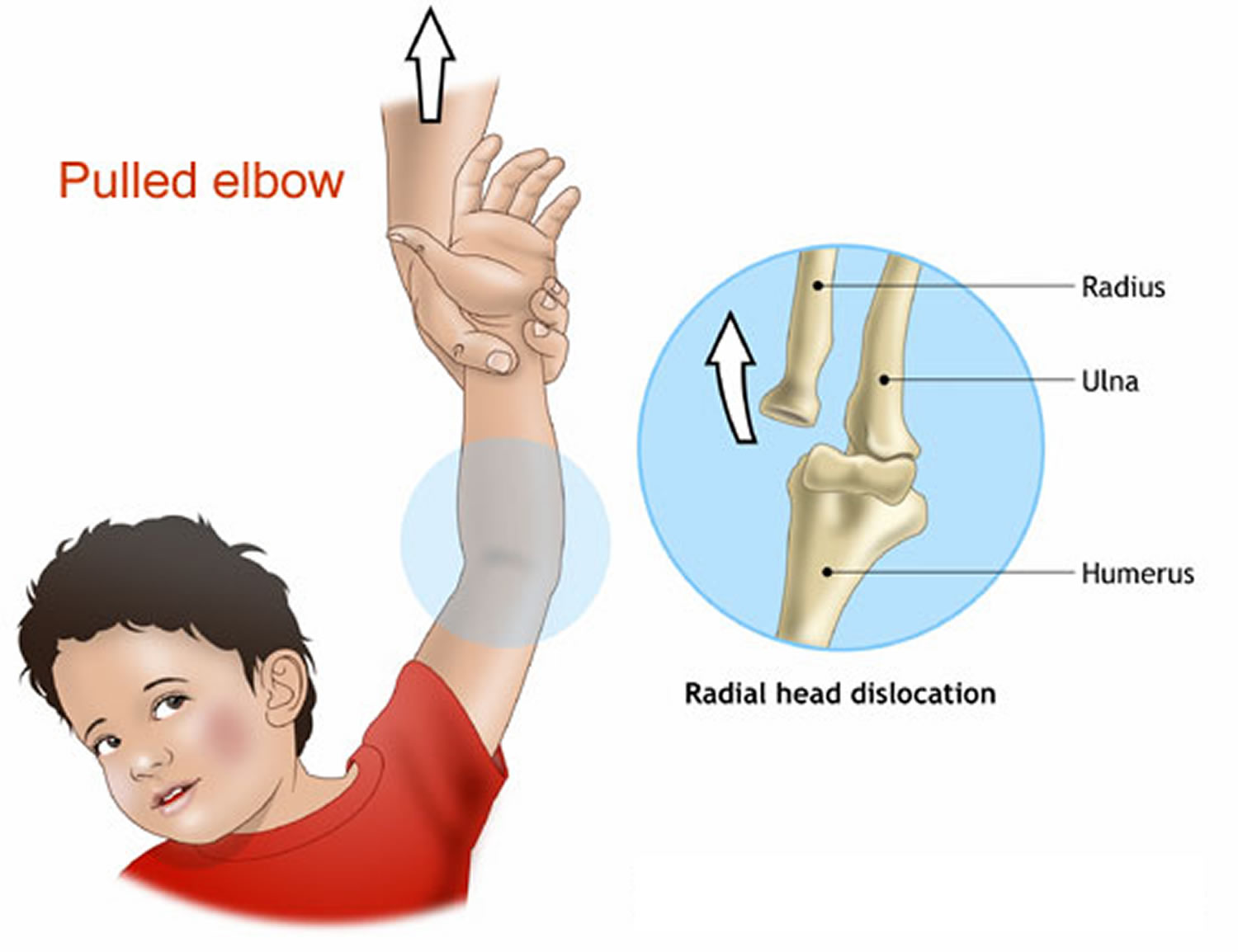
Pulled elbow is also called radial head dislocation or nursemaid’s elbow, is a common injury affecting children below the age of 5, but mostly 2 to 3 year olds. It is a mild dislocation of the elbow (head of radius), which is the result of the lower arm (radius bone) slipping out of its normal position at the elbow joint.
A ligament (annular ligament) (see Figure 1) normally holds the bone in place, but in some children the ligament is stretched (such as with a sudden pull) and the bone (radial head) partially slips out from underneath the ligament (see Figure 2).
A pulled elbow is caused by a sudden yank or pull on a child’s lower arm or wrist, such as when a child is lifted up by one arm, usually by an adult. It can also happen when a child falls. Typically this happens when the child is being taken somewhere they don’t want to go and is lifted up by one arm. The top of the radius (one of the 2 forearm bones) is pulled through the ligament that joins it to the neighboring ulna bone.
Other ways this injury may happen include:
- Stopping a fall with the arm
- Rolling over in an unusual way
- Swinging a young child from their arms while playing
In most cases, children with a pulled elbow will cry straightaway and not use the injured arm at all, or simply have it hanging by their side.
It is unusual for children over 5 to get a pulled elbow, as their joints and the structures around it are a lot stronger.
Figure 2. Dislocated elbow toddler / child
Dislocated elbow toddler and child symptoms
When the injury occurs:
- The child usually begins crying right away and refuses to use the arm because of elbow pain.
- The child may hold the arm slightly bent (flexed) at the elbow and pressed up against their belly (abdominal) area.
- The child will move the shoulder, but not the elbow. Some children stop crying as the first pain goes away, but continue to refuse to move their elbow.
Dislocated elbow toddler and child treatment
The partial dislocation will be reduced or manipulated (put back into place) by a nurse or doctor. The problem can be quickly rectified by your doctor holding the elbow firmly and quickly rotating the forearm in an outward direction. Often a ‘click’ will be heard and the child will soon regain the use of their arm. An X-ray is not usually required but may be done if your doctor suspects another injury, such as a fracture.
Your child will be observed for a short while to check that they are using their arm without any problems or pain. Using the arm normally may be possible almost immediately after the elbow is ‘reduced’, or it might take a bit longer. The longer the elbow has been out of place, the longer it takes to fully recover. Your child may be given medication for pain.
If a pulled elbow is not able to be put back into place or your child is still not using the injured arm, an X-ray may be ordered to check for other possible injuries such as a fracture (break). You will be advised if this is necessary.
Pulled elbow is not a serious injury and usually does not cause long-term damage.
Care at home
Generally after the elbow is manipulated, your child will use the arm normally and will not require any pain medication. If the elbow was ‘out’ for a while, then your child may need some pain medicine for that day. If your child is not moving the arm fully by the next day, their injury should be evaluated again.
What to expect
A pulled elbow will not cause any permanent or long term damage to your child. However, once the elbow dislocates, it is likely to do so again, especially in the 3 or 4 weeks after the injury. When dislocated elbow returns several times, your provider may teach you how to correct the problem yourself.
Some children are more likely than others to sustain this type of injury. It can happen more than once and in some children it occurs several times. This will not cause your child any long term or permanent damage if treated promptly and appropriately.
The longer the elbow has been dislocated the more painful and difficult it is to relocate, so prevention is the key.
Dislocated elbow toddler and child Prevention
Make sure you don’t pick your child up by the lower arms or wrists and teach others (such as grandparents and child care workers) to do the same. This is very important to save your child from having the same injury happen again.
Key points to remember
- A pulled elbow is caused by a sudden yank or pull on a child’s lower arm or wrist; or from a fall.
- A pulled elbow will not cause any permanent or long term damage to your child.
- It is unusual for children over five to have a pulled elbow.
- Don’t pick your child up by the lower arms or wrists and educate others to do the same. Prevention is the key.
Dislocated elbow causes
Elbow dislocations are not common. Elbow dislocations typically occur when a person falls onto an outstretched hand. When the hand hits the ground, the force is sent to the elbow. Usually, there is a turning motion in this force. This can drive and rotate the elbow out of its socket. Elbow dislocations can also happen in car accidents when the passengers reach forward to brace for impact. The force that is sent through the arm can dislocate the elbow, just as in a fall.
In adults, the most common causes of a dislocated elbow include:
- Falls. Falling onto an outstretched hand can pop the upper arm bone out of alignment within the elbow joint.
- Motor vehicle accidents. The same type of impact can occur when passengers in motor vehicle accidents reach forward to brace themselves before a collision.
In children or teenagers, falling onto an outstretched hand is also a common cause of a dislocated elbow.
In toddlers, the injury often occurs when an extra pulling motion is applied to an outstretched arm. The causes of such injuries include:
- Improper lifting. Trying to lift or swing a young child by the arms can cause the elbow to dislocate.
- Sudden pulling. Having the child suddenly step off a curb or stairstep as you’re holding his or her hand can pull the elbow out of alignment.
Risk factors for dislocated elbow
- Age. Young children’s elbows are much more flexible than those of adults. So it’s easier for younger elbows to become dislocated.
- Heredity. Some people are born with elbow ligaments that are looser than those of most people.
- Sports participation. Many elbow dislocations are sports-related. Sports that require weight bearing with the arms, such as gymnastics floor exercise, are especially risky for elbow dislocations.
Dislocated elbow complications
Complications of a dislocated elbow can include:
- Fracture. The force that dislocates the elbow might also cause a fracture in one of the elbow bones.
- Pinched nerves. Rarely, nerves that travel across the elbow can become pinched or trapped between the dislocated bones or within the joint when the bones are realigned. Pinched nerves can cause numbness in the arm and hand.
- Trapped arteries. Rarely, blood vessels that supply the arm and hand can become pinched or trapped between the dislocated bones or within the realigned joint. Lack of blood supply can cause severe pain and permanent tissue damage in the arm and hand.
- Avulsion fractures. In some elbow dislocations, a stretched ligament will pull off a tiny bit of bone from its attachment point. This type of damage is more common in children.
- Osteoarthritis. The dislocated joint may be at higher risk of developing osteoarthritis in the future.
Dislocated elbow symptoms
Signs and symptoms of a complete dislocated elbow include:
- Extreme pain
- Obvious distortion of the joint
A partial elbow dislocation or subluxation can be harder to detect. Typically, it happens after an accident. Because the elbow is only partially dislocated, the bones can spontaneously relocate and the joint may appear fairly normal. The elbow will usually move fairly well, but there may be pain. There may be bruising on the inside and outside of the elbow where ligaments may have been stretched or torn. Partial dislocations can continue to recur over time if the ligaments never heal.
Toddlers with a pulled elbow (nursemaid’s elbow) might experience pain only when the affected elbow is moved. A child often avoids using the arm and holds it slightly flexed next to the body.
Sometimes, the elbow is only partially dislocated. Partial dislocation can cause bruising and pain where the ligaments were stretched or torn.
Dislocated elbow diagnosis
Your doctor will carefully examine the injured joint and check if the arm or hand is cold or numb — which would indicate a pinched artery or nerve. Pulses at the wrist will be checked. If the artery is injured at the time of dislocation, the hand will be cool to touch and may have a white or purple hue. This is caused by the lack of warm blood reaching the hand.
It is also important to check the nerve supply to the hand. If nerves have been injured during the dislocation, some or all of the hand may be numb and not able to move.
You probably will need an X-ray to check for fracture in the bones that make up the elbow joint. X-rays are the best way to confirm that the elbow is dislocated. If bone detail is difficult to identify on an x-ray, a computed tomography (CT) scan may be done. If it is important to evaluate the ligaments, a magnetic resonance image (MRI) can be helpful, however, it is rarely required.
First, however, the doctor will set the elbow, without waiting for the CT scan or MRI. These studies are usually taken after the dislocated elbow has been put back in place.
How to fix a dislocated elbow
Some dislocated elbows go back into place by themselves. Most, however, need a doctor to manipulate the bones back into their proper alignment. This procedure is called a reduction.
Nonsurgical Treatment
The normal alignment of the elbow can usually be restored in an emergency department at the hospital. Before this is done, sedatives and pain medications usually will be given. The act of restoring alignment to the elbow is called a reduction maneuver. It is done gently and slowly.
Simple elbow dislocations are treated by keeping the elbow immobile in a splint or sling for 1 to 3 weeks, followed by early motion exercises. If the elbow is kept immobile for a long time, the ability to move the elbow fully (range of motion) may be affected. You might also need to do physical therapy exercises to improve the joint’s range of motion and strength. Early physical therapy is superior to immobilization in terms of short-term clinical outcome 1.
Some people will never be able to fully open (extend) the arm, even after physical therapy. Fortunately, the elbow can work very well even without full range of motion. Once the elbow’s range of motion improves, the doctor or physical therapist may add a strengthening program. X-rays may be taken periodically while the elbow recovers to ensure that the bones of the elbow joint remains well aligned.
Surgery
You might need surgery if:
- Any of the dislocated bones have also been broken
- Torn ligaments need to be reattached
- Damaged nerves or blood vessels need repair
In a complex elbow dislocation, surgery may be necessary to restore bone alignment and repair ligaments. It can be difficult to realign a complex elbow dislocation and to keep the joint in line.
After surgery, the elbow may be protected with an external hinge. This device protects the elbow from dislocating again. If blood vessel or nerve injuries are associated with the elbow dislocation, additional surgery may be needed to repair the blood vessels and nerves and repair bone and ligament injuries.
Late reconstructive surgery can successfully restore motion to some stiff elbows. This surgery removes scar tissue and extra bone growth. It also removes obstacles to movement.
Over time, there is an increased risk for osteoarthritis in the elbow joint if the alignment of the bones is not good; the elbow does not move and rotate normally; or the elbow continues to dislocate.
Some people with complex dislocations still have some type of permanent disability at the elbow. Treatment is evolving to improve results for these people.
One of the areas being researched is the best time to schedule surgery for the treatment of a complex dislocation. For some patients with complex dislocations, it seems that a slight delay for final surgery may improve results by allowing swelling to decrease. The dislocation still needs to be reduced right away, but then a brace, splint, or external fixation frame may rest the elbow for about a week before a specialist surgeon attempts major reconstructive surgery.
Moving the elbow early appears to be good for recovery for both simple and complex elbow dislocations kinds of dislocations. Early movement with complex dislocations can be difficult, however. Pain management techniques encourage early movement. Improved therapy and rehabilitation techniques, such as continuous motion machines, dynamic splinting (spring-loaded assist devices), and progressive static splinting can improve results.
Management of complications: ligament repair and ligament reconstruction
Elbow dislocation can vary in severity. O’Driscoll et al. 2 showed this on the basis of a biomechanical study and formulated an instability classification system for posterolateral rotatory instability. This ranges from a weak tendency to radial head subluxation to high instability of the whole elbow joint, even when immobilized in plaster.
If healing is incomplete, instability, usually slight, may remain and can lead to chronic pain, feelings of instability, and also movement limitations 3. Collateral ligament reconstruction using autologous or allogenous tendon grafts is now performed as standard treatment in cases of delayed surgery, because the ligamentous structures are often insufficient and scarred following incomplete healing 4.
The meta-analysis presented by O’Brien et al. 5 and Daluiski et al. 6 comes to the interesting conclusion that ligament repair after several months or even years leads to outcomes as good as those following acute ligament repair, and that collateral ligament reconstruction is not necessarily needed.
- Hackl M, Beyer F, Wegmann K, Leschinger T, Burkhart KJ, Müller LP. The Treatment of Simple Elbow Dislocation in Adults: A Systematic Review and Meta-analysis. Deutsches Ärzteblatt International. 2015;112(18):311-319. doi:10.3238/arztebl.2015.0311. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4455254/[↩]
- O’Driscoll SW. Classification and evaluation of recurrent instability of the elbow. Clin Orthop Relat Res. 2000;370:34–43. https://www.ncbi.nlm.nih.gov/pubmed/10660700[↩]
- Rafai M, Largab A, Cohen D, Trafeh M. [Pure posterior luxation of the elbow in adults: immobilization or early mobilization. A randomized prospective study of 50 cases] Chir Main. 1999;18:272–278. https://www.ncbi.nlm.nih.gov/pubmed/10855330[↩]
- Savoie FH, 3rd, O’Brien MJ, Field LD, Gurley DJ. Arthroscopic and open radial ulnohumeral ligament reconstruction for posterolateral rotatory instability of the elbow. Clin Sports Med. 2010;29:611–618. http://www.sportsmed.theclinics.com/article/S0278-5919(10)00048-7/fulltext[↩]
- O’Brien MJ, Lee Murphy R, Savoie FH., 3rd A preliminary report of acute and subacute arthroscopic repair of the radial ulnohumeral ligament after elbow dislocation in the high-demand patient. Arthroscopy. 2014;30:679–687. http://www.arthroscopyjournal.org/article/S0749-8063(14)00198-4/fulltext[↩]
- Daluiski A, Schrumpf MA, Schreiber JJ, Nguyen JT, Hotchkiss RN. Direct repair for managing acute and chronic lateral ulnar collateral ligament disruptions. J Hand Surg Am. 2014;39:1125–1129. http://www.jhandsurg.org/article/S0363-5023(14)00256-1/fulltext[↩]





{kind=link}