Contents
What is double uterus
A double uterus also called didelphys uterus, is a rare congenital abnormality – an embryological developmental malformation of the Müllerian (Wolffian) ducts , characterized by complete failure of the Müllerian (Wolffian) ducts to fuse, resulting in two separate uterine cavities and cervices 1. Sometimes a longitudinal or transverse vaginal septum varying from thin and easily displaceable to thick and inelastic may also be associated with double uterus 2. Further, because the Mullerian ducts develop often in association with Wolffian ducts, abnormalities of the kidneys may be found in conjunction with uterine abnormalities 3.
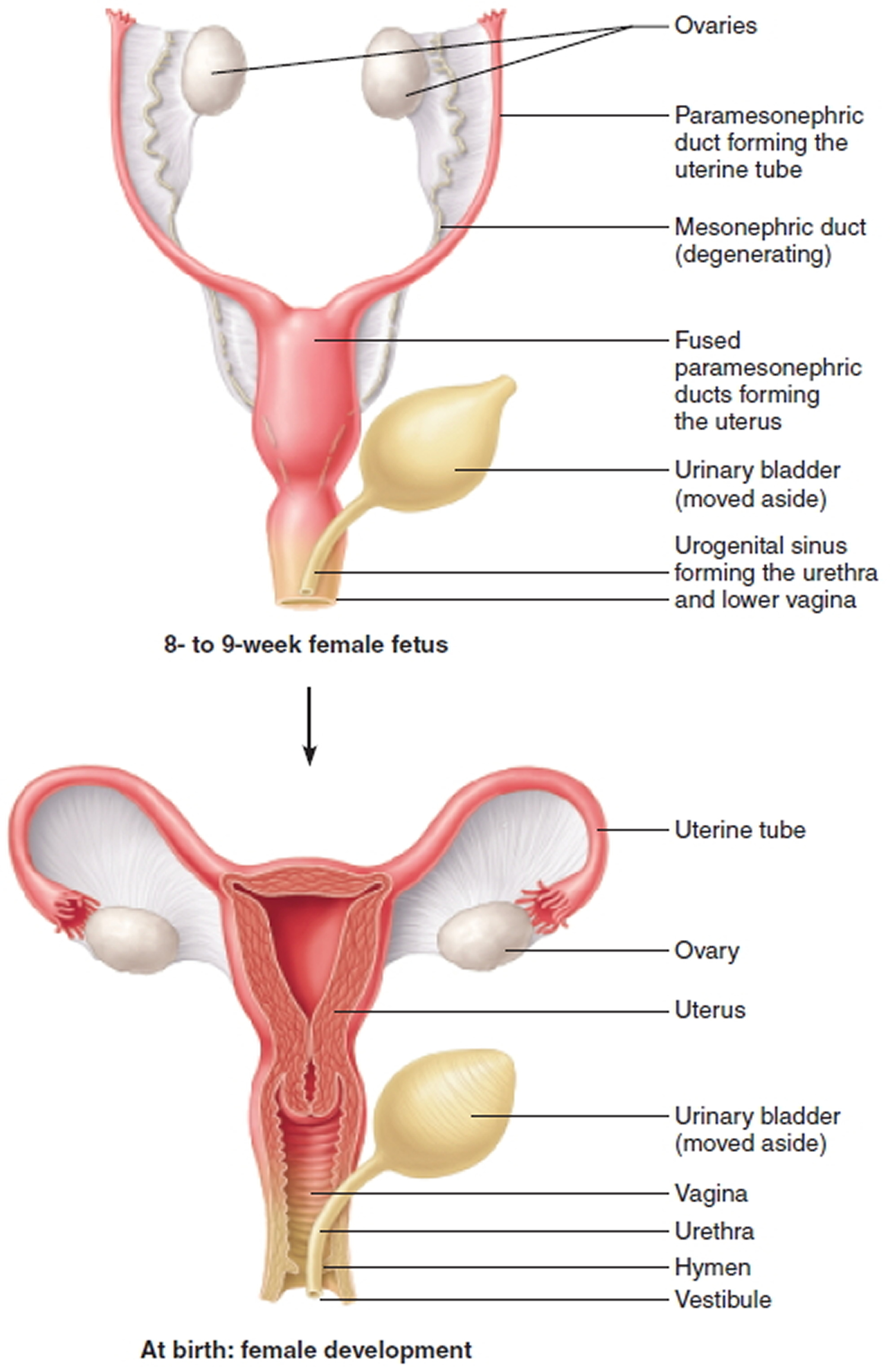
In a female fetus, the uterus starts out as two small tubes. As the fetus develops, the tubes normally join to create one larger, hollow organ — the uterus (Figure 1). Sometimes, however, the tubes don’t join completely. Instead, each one develops into a separate structure (Figure 2 and 3). A double uterus may have one opening (cervix) into one vagina, or each uterine cavity may have a cervix. In many cases, a thin wall of tissue runs down the length of the vagina, dividing it into two separate openings.
Women who have a double uterus often have successful pregnancies. But the condition can increase the risk of miscarriage or premature birth.
Double uterus is an embryological developmental malformation of the Müllerian (Wolffian) ducts with the incidence of approximately 8.3% of all Müllerian duct abnormalities 1. Among Müllerian duct anomalies, the septate uterus is the most common (35%) followed by bicornuate uterus (25%), arcuate uterus (20%), then unicornuate (9.6%), and complete agenesis (3%) 1. The occurrence of didelphys uterus is the second least common with the incidence of approximately 8.3% of all Müllerian (Wolffian) ducts abnormalities. The prevalence of double uterus (didelphys uterus) is reported to be 1 in 1000–1 in 30,000 women 2.
These uterine anomalies are associated with delayed natural conception and subfertility. In case of infertile women, double uterus has been found around 0.2%. For such cases, successful pregnancies can be achieved by artificial reproductive technique and embryo transfer 4, 5.
Natural twin conception in each cavity of double uterus (didelphys uterus) is a very rare entity and only a handful of cases are reported in the literature to date. Because of its rarity, double uterus (didelphys uterus) accompanying natural dicavitary twin conception without any fertility treatment has not been researched extensively in the literature, so the exact rate of occurrence is unknown in general population 2, 5.
Dicavitary twin in a double uterus was first described in 1927. The overall incidence of dicavitary twin gestation (ART/Natural conception) in double uterus (didelphys uterus) has been reported approximately 1 in 1,000,000.
Double uterus (didelphys uterus) accompanying dicavitary twin pregnancy is encountered as a very rare entity with overall incidence of about 1 in 1,000,000 2. Like other Müllerian duct anomalies, double uterus is associated with various obstetric complications like spontaneous miscarriages, malpresentation, preterm delivery, preterm rupture of membrane, intrauterine growth restriction, and the need for operative delivery 6, 7.
A case report of a 30 year old with a history of 4 pregnancies, 1 live birth and 2 miscarriages, her last pregnancy course was complicated by preterm labor at 34-week gestation and she delivered simultaneously both fetuses with the cephalic presentation by spontaneous vaginal delivery with good maternal and neonatal outcomes 1.
Figure 1. Female reproductive organs development
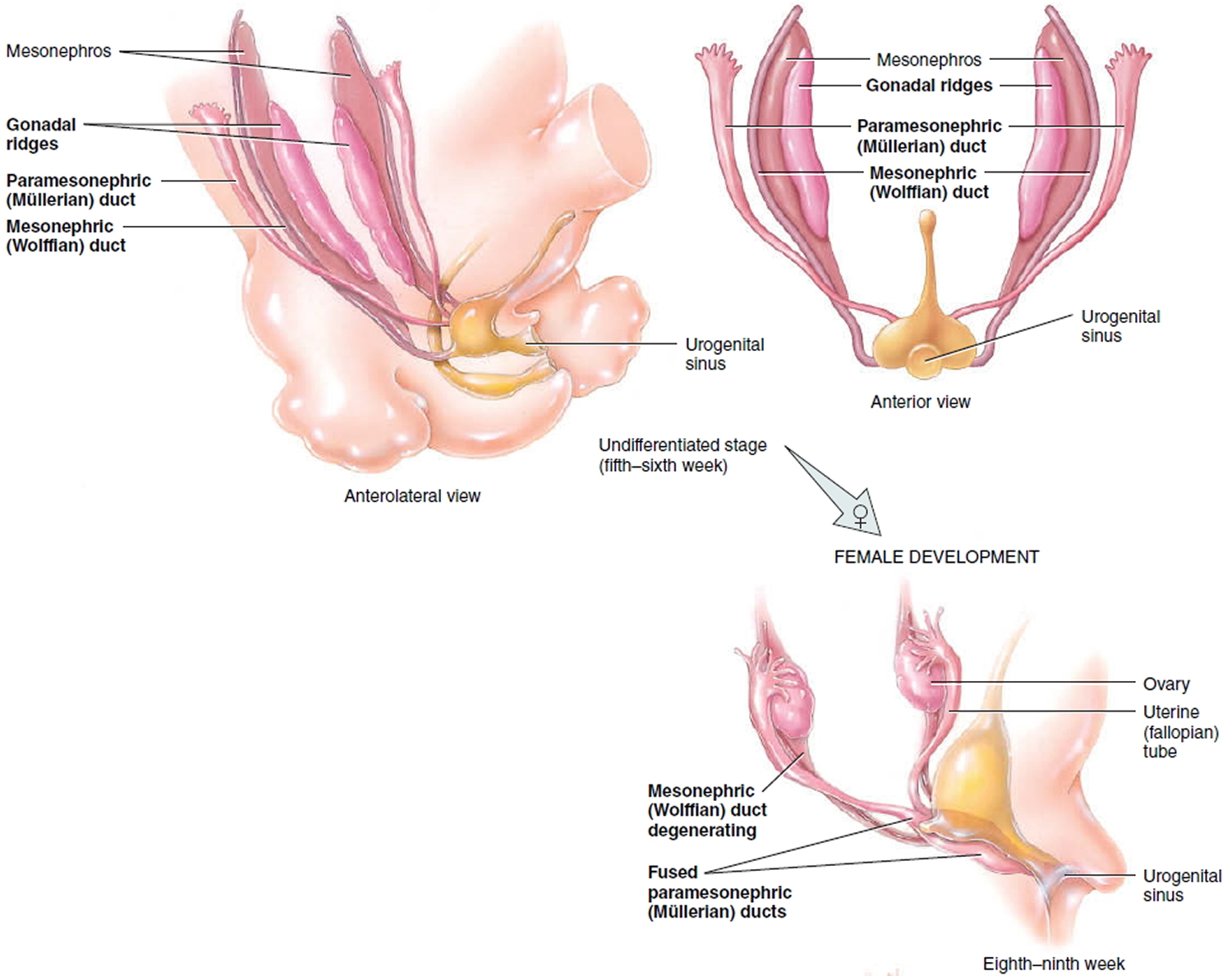
Figure 2. Female uterine development
 Mullerian duct anomalies
Mullerian duct anomalies
When classifying Mullerian duct anomalies solely based on abnormal development, four major types are apparent:
- Complete or partial failure of Mullerian duct development (agenesis; unicornuate uterus without a rudimentary horn);
- Failure of ducts to canalize (unicornuate uterus with a rudimentary horn without proper cavities);
- Incomplete fusion of Mullerian ducts (bicornuate or didelphys uterus) 8;
- Incomplete reabsorption of uterine septum (septate or arcuate uterus) 9.
Figure 3. Mullerian duct anomalies and Double uterus
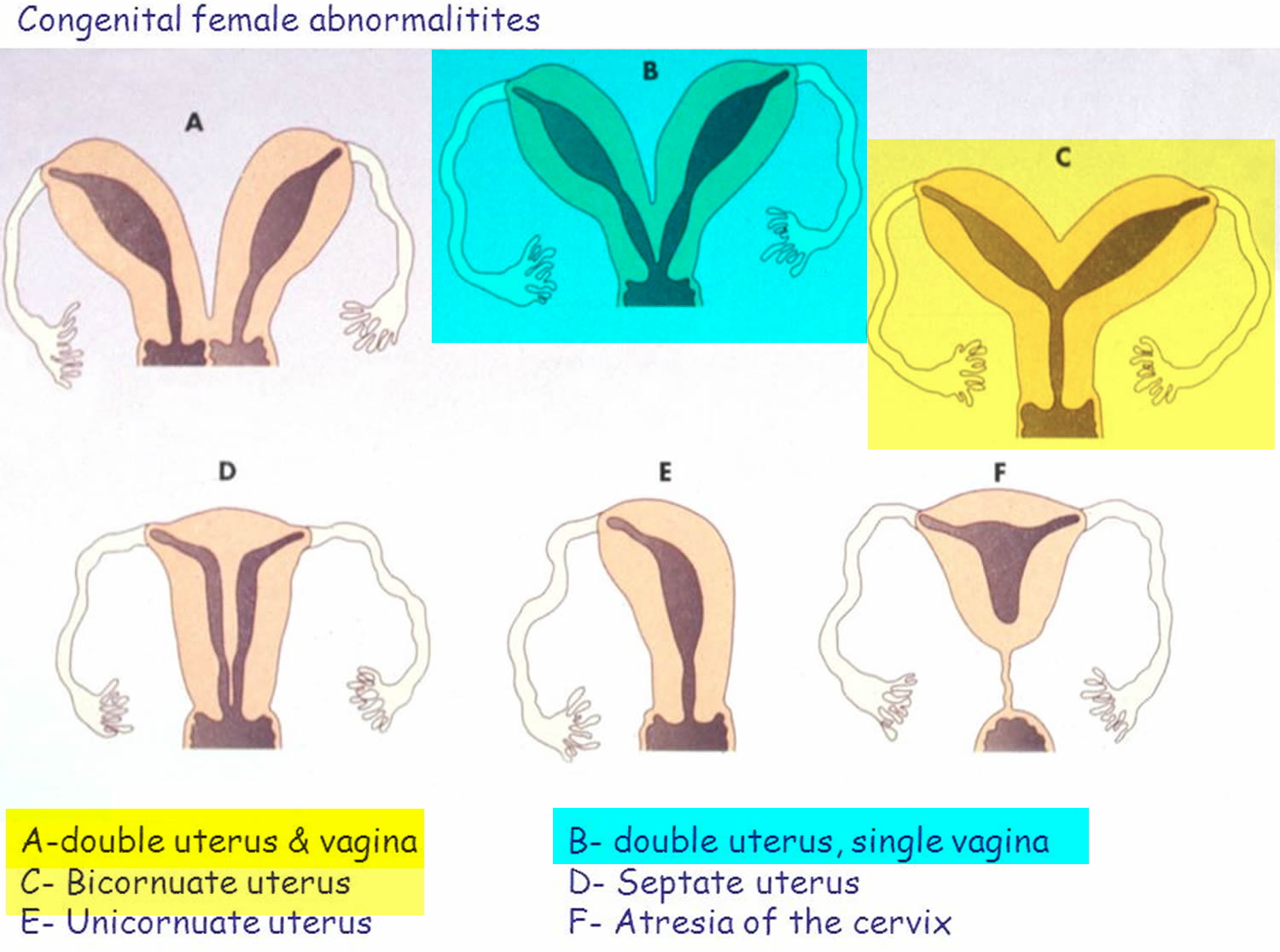
Figure 4. Double uterus and ovaries intraoperatively

Figure 5. Double uterus found during ultrasound examination

Note: RT UT = right uterus, LT UT = left uterus, BL = urinary bladder
What are congenital uterine conditions?
Congenital means that something is present at birth—it’s something you’re born with. About 3 in 100 females (3 percent) are born with a defect in the size, shape or structure of the uterus.
When a baby girl is developing in the womb, two small tubes call Mullerian ducts come together at about 10 weeks gestation (10 weeks of pregnancy) to form her uterus (see Figures 1 and 2 above). For some baby girls, the Mullerian ducts don’t come together completely. This can cause problems with the uterus, including:
- Septate uterus. This is the most common congenital uterine abnormality. In this condition, a band of muscle or tissue (called a septum) divides the uterus into two sections. This condition can cause women to have repeat miscarriages, so health care providers often recommend surgery to repair the uterus and reduce your risk of miscarriage. Miscarriage is the death of a baby in the womb before 20 weeks of pregnancy. Repeat miscarriage means a woman has two, three or more miscarriages in a row.
- Bicornate uterus (also called heart-shaped uterus). In this condition, the uterus has two cavities (spaces) instead of one large cavity. Most women with this condition don’t need surgery to repair it.
- Didelphic uterus (also called double uterus). In this condition, there are two small, separate cavities, each with its own cervix (opening).
- Unicornate uterus (also called one-sided uterus). This condition happens when only half the uterus forms. Surgery can’t make the uterus any larger.
Double uterus fertility and pregnancy
The body of literature on double uterus, although limited, generally shows that the anomaly may lead to better pregnancy outcomes in comparison to the other anomalies; however there are also studies that demonstrate the contrary. For example, Acién’s prospective observational study 10 of the reproductive outcome of women with different uterine anomalies in comparison to a normal uterus found the rate of term delivery for a double uterus significantly lower than the normal uterus group but the rate was not as low as that of the bicornuate group and septate group 10. Grimbizis et al. 9 also confirmed this conclusion in a review on the clinical implications of uterine malformations. Another study by Ludmir et al. 11 also found, with high-risk obstetric intervention, more pregnancies from a double uterus reached term and fetal survival rate was higher in comparison to the bicornuate and septate group.
On the other hand, a large retrospective longitudinal study of 3181 patients by Raga et al. 12 demonstrated poor reproductive performance in women with double uteri with a higher rate of preterm delivery, spontaneous abortion, and the lowest chance of having a term delivery than the other Mullerian duct anomalies. In addition, a long term retrospective follow-up of 49 women with didelphys uterus found no impairment with fertility and decreased rate of spontaneous abortion; however the rate of prematurity was increased in comparison to other known studies on septate and bicornuate uteri 3.
The association between having a Mullerian duct anomaly and fertility is debatable. The review by Grimbizis 9 demonstrated the incidence of Mullerian duct anomalies in infertile patients (3.4%) similar to that of the general population and/or fertile women (4.3%), which they concluded demonstrated that Mullerian duct anomalies may not have a negative impact on fertility. To go further, there are reported cases of women with double uteri pregnant with twins or triplets demonstrating the ability to conceive and support the healthy growth of a fetus in either one of the uteri 13. In contrast, the large retrospective study done by Raga et al. 12 found the incidence of Mullerian duct anomalies to be significantly higher in infertile women than in fertile women, suggesting a link between infertility and the Mullerian duct anomaly. A retrospective study on fertility and obstetric outcome done by Zhang et al. 14 in China demonstrated that women with a didelphys uterus more frequently required infertility treatments than with other anomalies to conceive.
Certain procedures may be undertaken to increase fertility, decrease chances of prematurity, and improve the quality of life. Surgical correction of a double uterus (metroplasty) is not usually indicated and the literature on women with double uterus who underwent metroplasty is very limited. With that said, metroplasty would only be considered on a case by case basis after all other ways in which reproductive performance could be improved are exhausted 9, 10, 15. Observational studies cite women with septate or bicornuate uteri with a history of repeated abortions and infertility demonstrating improvement in reproductive and gestational outcome after metroplasty 10. Longitudinal vaginal septum excision is considered if the woman is symptomatic, complaining of dyspareunia or pain from hematometrocolpos due to obstruction. Some septa can be easily displaced to the side to facilitate vaginal birth and others may be thick and inelastic, increasing the risks of vaginal dystocia and thus requiring excision. A didelphys uterus is not an indication for cesarean delivery and thus vaginal delivery should be considered first 7. Finally, cervical incompetence is not usually associated with didelphys uterus and thus cerclage is not routinely used unless there is a history of cervical incompetence or premature dilation is found on exam during early second trimester 3.
A double uterus has been shown in many case reports to occur as a part of a syndrome, more specifically called, Herlyn-Werner-Wunderlich (HWW) syndrome, also known as obstructed hemivagina and ipsilateral renal anomaly. It is a very rare congenital anomaly of the urogenital tract involving Mullerian ducts and Wolffian structures, and it is characterized by the triad of double uterus, obstructed hemivagina, and ipsilateral renal agenesis 16. This condition can cause hematometrocolpos (blood-filled distended uterus and vagina) or hematocolpos (a medical condition in which the vagina fills with menstrual blood) on the side of the obstructed hemivagina which produces a mass effect with subsequent lower abdominal pain 17. Most cases present after menarche as intense lower abdominal pain and/or a protruding mass over the vaginal introitus 17. Sudden, intense vaginal pain has been documented as a rare presenting symptom as well 18. A preliminary pelvic Ultrasound is done followed by an MRI to confirm the diagnosis. One case report identified this syndrome in a newborn who was diagnosed with renal agenesis in utero and born with a protruding vaginal mass and a hydrocolpos was found on imaging 19. Although this condition is extremely rare, it is important for a physician, especially an emergency room physician, to keep it in mind when a postpubertal female presents with sudden lower abdominal pain and all other causes have been ruled out 17.
Double uterus complications
Many women with a double uterus have normal sex lives, pregnancies and deliveries. But sometimes a double uterus and other abnormalities of uterine development are associated with:
- Infertility
- Miscarriage
- Premature birth
- Kidney abnormalities
Double uterus causes
Doctors aren’t certain why some fetuses develop a double uterus and others don’t. A genetic component may be a factor because this rare condition sometimes runs in families.
The internal genital organs and lower urinary tract derive from two paired urogenital structures that develop in both sexes—the Mesonephric (Wolffian) ducts and the Paramesonephric (Mullerian) ducts are the two paired urogenital structures from which the internal genital organs and the lower urinary tract derive 20 (see Figures 1 and 2). In the female, the Müllerian (paramesonephric) ducts, located just lateral to the Mesonephric (Wolffian) ducts, which act as inductor elements, grow downwards and towards the midline, crossing the Mesonephric (Wolffian) ducts, and come into contact with each other. They then fuse to form the uterovaginal canal, from which the fallopian tubes, uterus and the upper two-thirds of the vagina develop 21.
As a consequence of nondevelopment or failure of fusion of the distal segments of the Müllerian ducts, various types of uterine anomalies can ensue, such as hypoplasia/agenesis, unicornuate, didelphys (double uterus), bicornuate, septate and arcuate uterus, in addition to a peculiar anomaly of uterine morphology that is related to diethylstilbestrol. These malformations have been subdivided into seven classes by the American Society of Reproductive Medicine. After completing their fusion, the Müllerian ducts join the dorsal wall of the urogenital sinus, from which the lower third of the vagina develops, while the Wolffian ducts open laterally.
Due to the different embryological origin of the upper two-thirds of the vagina, which originates from the Müllerian ducts of mesodermal origin, and the lower third of the vagina, which originates from the urogenital sinus of endodermal origin, vaginal anomalies, such as hypoplasia/aplasia, duplication or septa, may exist alone or in association with Müllerian anomalies. A complete longitudinal vaginal septum is present in the majority (75%) of women with double uterus and in 25% of women with bicornuate bicollis uterus.
The Mesonephric (Wolffian) ducts and the Paramesonephric (Mullerian) ducts are the two paired urogenital structures from which the internal genital organs and the lower urinary tract derive 22 (see Figures 1 and 2). The fallopian tubes, uterus, and the upper two-thirds of the vagina develop from the bilateral Mullerian Ducts (4). As a result of any interruption in the development of this embryological event, different types of uterine anomalies can arise, such as agenesis, hypoplasia, unicornuate, didelphys, bicornuate, arcuate, and septate uterus. The American Society of Reproductive Medicine has classified these malformations under seven groups, while Acien et al 23 have more recently proposed a clinical embryological classification of all genital tract malformations.
Mullerian duct anomalies are congenital anomalies of the female genital tract resulting from non-development or non fusion of the mullerian ducts, or failed resorption of the uterine septum 24. Duplication of the uterus results from the lack of fusion of the paramesonephric ducts in a local area or throughout their normal line of fusion. In double uterus, individual horns are fully developed, normal in size with two cervices inevitably present. Each hemiuteri is associated with one fallopian tube. Ovarian malposition may also be present. A longitudinal or transverse vaginal septum may be noted.
The vagina may be single or double. Duplicated vagina is more likely in a double uterus. Ipsilateral renal agenesis with partial vaginal septum on the same side and double uterus is explained by embryologic arrest at the 8th week of gestation affecting simultaneously the mullerian and metanephric ducts 25. True prevalence of this anomaly is unknown as it may be discovered in later part of patients life when presenting with infertility. The incidence of mullerian duct anomalies in literature ranges from 0.5 and 5.0%. Approximately 11% of uterine malformations are double uterus 26.
Double uterus symptoms
A double uterus often causes no symptoms. The condition may be discovered during a regular pelvic exam or during imaging tests to determine the cause of repeated miscarriages.
Most women with a double uterus (didelphys uterus) are asymptomatic, but some present with dyspareunia or dysmenorrhea in the presence of a varying degree a thick, sometimes obstructing longitudinal vaginal septum. This obstructing vaginal septum can lead to hematocolpos (a medical condition in which the vagina fills with menstrual blood) or hematometrocolpos (blood-filled distended uterus and vagina) and thus present as chronic abdominal pain as well. Rarely, genital neoplasms and endometriosis are reported in association with cases of double uterus 27, 28. Women who have a double vagina along with a double uterus may initially consult a doctor for menstrual bleeding that isn’t stopped by a tampon. In these situations, the woman has placed a tampon in one vagina, but blood is still escaping from the second uterus and vagina. Rarely, genital neoplasms, hematocolpos/hematometrocolpos, and renal anomalies are reported in association with double uterus (didelphys uterus). Despite some of these complications, there are many cases of women with a double uterus (didelphys uterus) that did not exhibit any reproductive or gestational challenges.
Double uterus diagnosis
A double uterus may be diagnosed during a routine pelvic exam when your doctor observes a double cervix or feels an abnormally shaped uterus. If your doctor suspects an abnormality, he or she may recommend any of the following tests:
- Ultrasound. This test uses high-frequency sound waves to create images of the inside of your body. To capture the images, a device called a transducer is either pressed against your abdominal skin or inserted into your vagina (transvaginal ultrasound). Both types of ultrasound may be done to get the best view. A 3-D ultrasound may be used where available.
- Sonohysterogram. The sonohysterogram (son-o-HIS-ter-o-gram), an ultrasound scan, is done after fluid is injected through a tube into your uterus by way of your vagina and cervix. This allows your doctor to look for problems in the shape of your uterus.
- Magnetic resonance imaging (MRI). The MRI machine looks like a tunnel that has both ends open. You lie down on a movable table that slides into the opening of the tunnel. This painless procedure uses a magnetic field and radio waves to create cross-sectional images of the inside of your body.
- Hysterosalpingography. During a hysterosalpingography (his-tur-o-sal-ping-GOG-ruh-fe), a special dye is injected into your uterus through your cervix. As the dye moves through your reproductive organs, X-rays are taken to determine the shape and size of your uterus and whether your fallopian tubes are open.
The modalities for correct diagnosis frequently used include highly invasive methods such as hysteroscopy, hysterosalpingography, and laparoscopy/laparotomy. However, these methods rely on the clinician’s subjective interpretation rather than strict diagnostic criteria 29. A 2D ultrasound is usually the first type of imaging done; however it is inadequate for diagnosis as it cannot reliably differentiate between subtypes of Mullerian duct anomalies. The use of 3D ultrasound is becoming more commonly used for diagnosis as it is not only noninvasive, but it also overcomes the limitation of 2D ultrasound by providing a coronal view that enables examination of both the endometrial cavity and uterine fundus, thus giving all the information needed for morphological classification 29. Magnetic resonance imaging (MRI scan) is also just as accurate and valuable in diagnosing Mullerian duct anomalies as hysterosalpingograms, hysteroscopy, and laparoscopy are, even more so as it is noninvasive and can diagnose associated urinary tract abnormalities at the same time 30. Nonetheless, it is still difficult to distinguish between these different anomalies on imaging modalities due to subjectivity; differences in morphology are often subtle and changing classification systems 9. Despite these difficulties, a review of the prevalence of different types of uterine malformations done by Grimbizis et al. 9 revealed that the septate uterus is most common at 35% followed by bicornuate at 25%, then arcuate at 20%, then unicornuate at 9.6%, and complete agenesis at 3%. Double uterus was found to be the second least common at 8.3% of all Mullerian duct anomalies 9.
Double uterus treatment
If you have a double uterus but you don’t have signs or symptoms, treatment is rarely needed. Surgery to unite a double uterus is rarely done — although surgery may help you sustain a pregnancy if you have a partial division within your uterus and no other medical explanation for a previous pregnancy loss.
If you have a double vagina in addition to a double uterus, you might be a candidate for an operation that would remove the wall of tissue separating the two vaginas. This can make childbirth a little easier.
Double uterus pregnancy
A double uterus (didelphys uterus) is characterized by complete failure of the Mullerian ducts to fuse leading to separate uterine cavities and two cervices. A longitudinal vaginal septum is also present that may range from thin and easily displaced to thick and inelastic. Initial suspicion of the condition followed by the diagnosis usually begins with a routine speculum exam where visualization of anatomical abnormalities warrants further investigation.
The fertility of women with untreated ddouble uterus (didelphys uterus) has been shown by some sources to be better than those with other Mullerian duct abnormalities but still less than women with normal uterine anatomy. There is also an increased risk of spontaneous abortion, fetal growth retardation, and prematurity with an estimated 45% (or lower) chance of carrying a pregnancy to term in comparison to a normal uterus, which is similar to that of a unicornuate uterus. This indicates poor reproductive performance, but still not as poor as a septate or bicornuate uterus which are more common amongst the Mullerian duct anomalies 31.
It is generally accepted that having a uterine anomaly is associated with poorer pregnancy outcomes such as increased chances of spontaneous abortion, premature labor, cesarean delivery due to breech presentation, and decreased live births, compared to a normal uterus 3. However, the degree of these outcomes varies among different types of uterine anomalies.
Unicornuate and double uterus (didelphys uterus) have term delivery rates of ~45% and the pregnancy outcome of patients with untreated bicornuate and septate uterus is also poor with term delivery rates of only ~40% 9. Arcuate uterus is associated with a slightly better but still impaired pregnancy outcome with term delivery rates of ~65% 9.
In a retrospective study 32 that included 144 patients with and 1089 patients without Mullerian anomalies undergoing a first cycle of IVF (In Vitro Fertilisation) between April 2011 and June 2016. Patients with Mullerian anomalies had a significantly lower implantation rate per embryo transfer (19.0%) than did controls (34.2%). As well as the pregnancy rate per patient(27.7% versus 46.5%), first -trimester spontaneous rate (38.5% versus 10.4%), Miscarrage rate (46.2% versus 18.1%), Delivery rate (53.8% versus 81.9%). One hundred and twenty-eight patients conceived a total of 82 clinical pregnancies in 209 embryo transfer cycles. The clinical pregnancy rate was 82 of 209 (39.2%) per embryo transfer and 73 of 128 (57.0%) per patient. There were no significant differences in the implantation rates per embryo transfer and clinical pregnancy rates when the various forms of uterine malformation were compared. There was a trend for the group with unicornuate and the double uterus had the highest rate (21/33, 63.6%) of term delivery and the lowest rate (8/33, 24.2%) of spontaneous abortion compared with the group of septate, bicornuate and arcuate uterus, in whom the term delivery rate was 24 of 49 (49.0%) and the spontaneous abortion rate was 20 of 49 (40.8%). The bicornuate uterus had the highest first trimester spontaneous abortion rate (3/8, 37.5%) and highest preterm delivery rate (2/8, 25%). The multiple pregnancy rate was 5 of 56 (7.7%) for unicornuate , septate and arcuate uterus, lower when compared with 5 of 17 (29.4%) of double uterus and bicornuate uterus 32.
A failure in Müllerian duct fusion might result in a double uterus (didelphys uterus), as well as a complete or partial septate vagina.6 This anomaly was typically discovered when the woman experienced fertility problems or had recurrent miscarriages. Overall, uterus didelphys has been found in 0.2% of the infertile population 33.
Although infertility has been one of the main problems for women with uterine anomalies, successful pregnancies can be facilitated by assisted reproductive technology (ART) commonly referred to as IVF (In Vitro Fertilisation) and embryo transfers. Customarily, when a woman has been diagnosed with double uterus (didelphys uterus) with complete septate vagina, embryo transfers to only one uterus was performed.
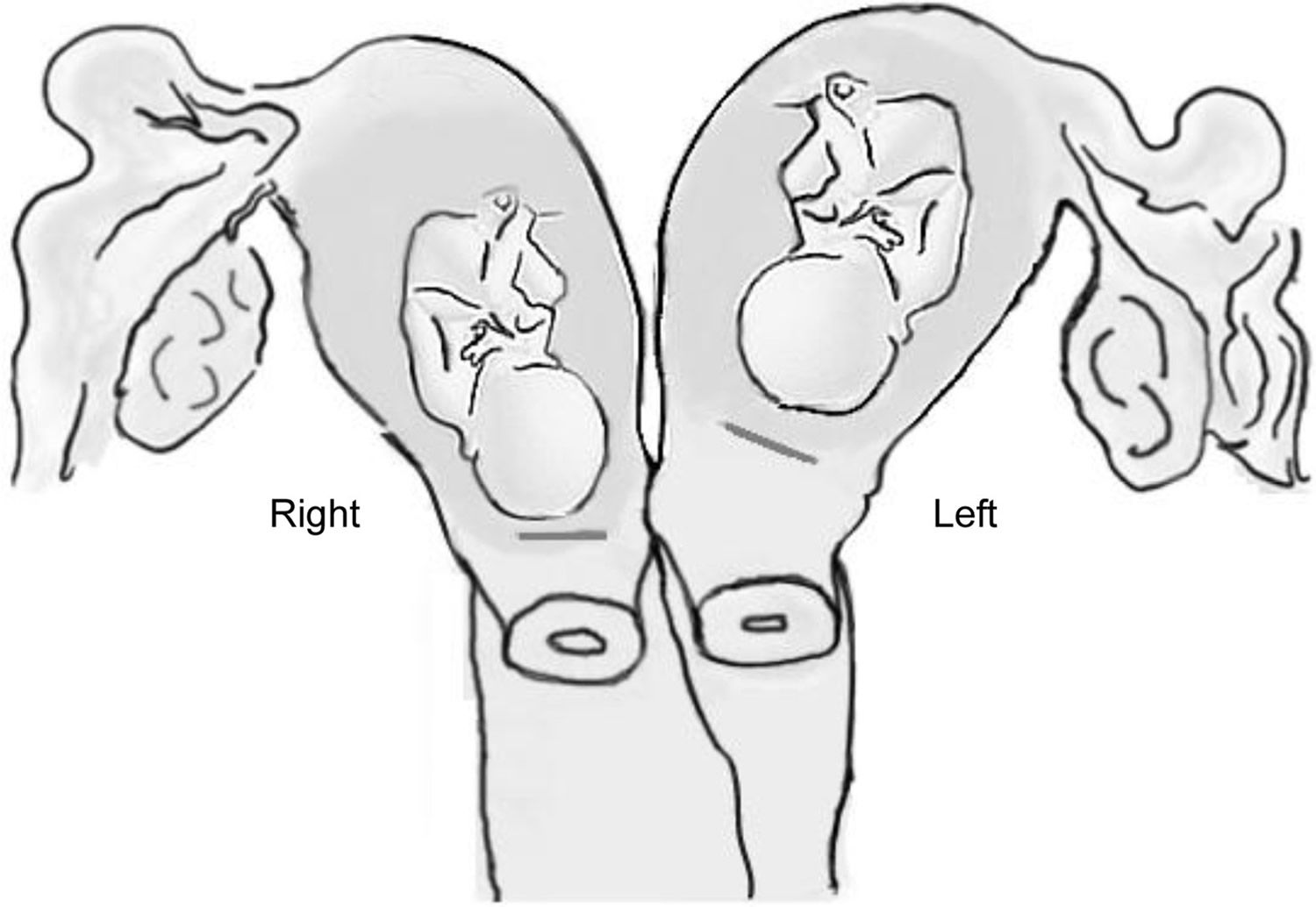
Figure 6. Double uterus pregnancy – note two embryos located separately with one in each uterus
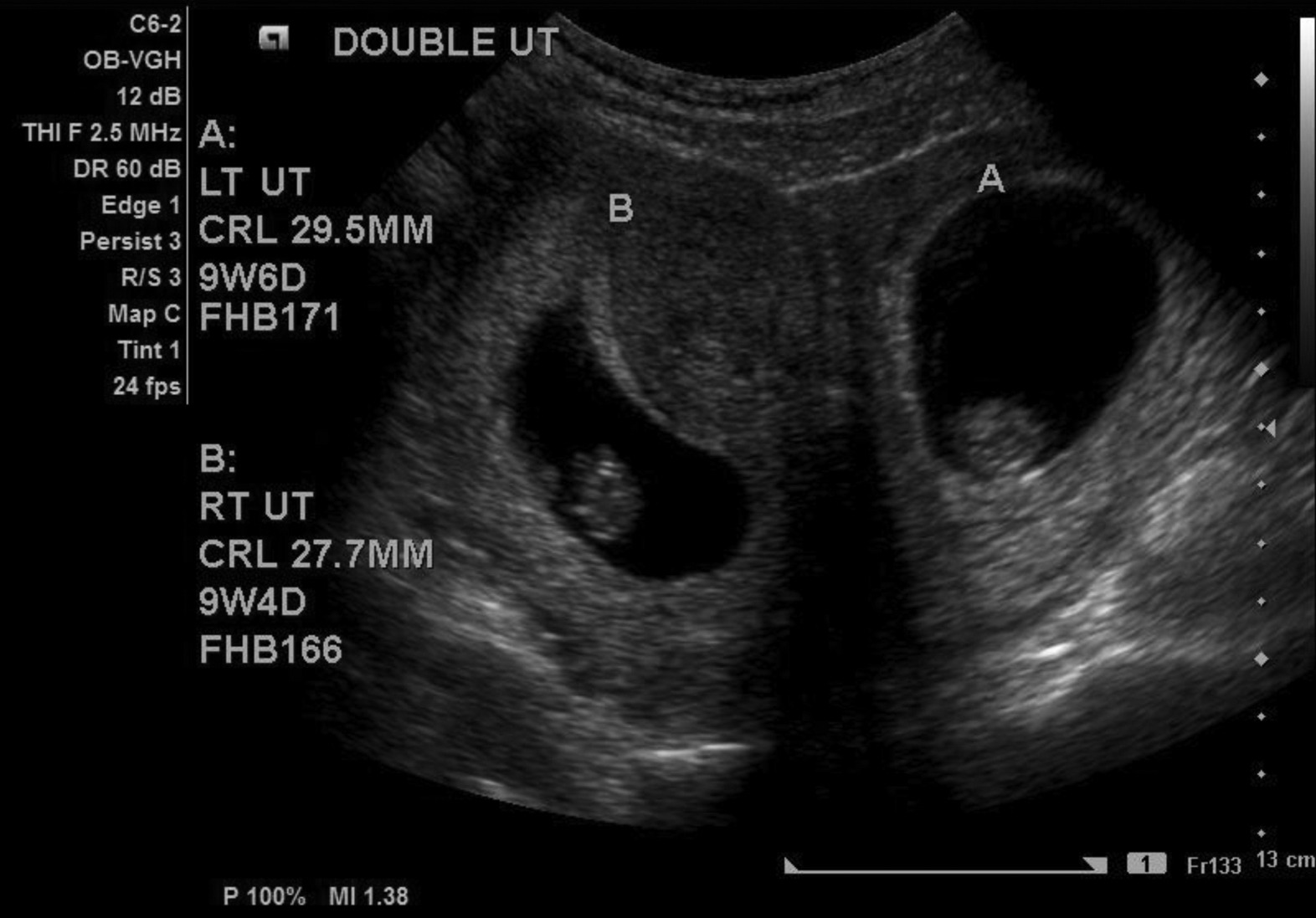
Note: A = Left uterus with a fetus, B = Right uterus with a fetus
Figure 7. Double singleton pregnancies in double uterus
 Double uterus pregnancy complications
Double uterus pregnancy complications
Women with double uterus have ovaries that function normally so they develop breasts, vulva, and pubic hair and can get pregnant. In addition, they experience no physical discomforts or difficulties engaging in sexual intercourse due to their internal abnormalities.
However, women with double uterus are more likely to have miscarriages and preterm births. Difficulties with pregnancy depend on the specific fusion disorder present. The only way to diagnose a fusion disorder is through ultrasound, magnetic resonance imaging (MRI) or a surgical procedure.
Double uterus is associated with varieties of obstetric complications including early and late miscarriages, malpresentation, intrauterine growth restriction, preterm delivery, and preterm rupture of membrane 34.
Cervical incompetence is not commonly occurred with double uterus so cervical cerclage is not routinely recommended unless there is an evidence of cervical incompetence or dilation either by clinical examination or ultrasonography during early second trimester. A case of double uterus with dicavitary twin was reported with the short cervix at 30 weeks of gestation with uterine contractions. They managed the case by tocolytic therapy with nifedipine until 34 weeks and then at 37 weeks of gestation cesarean section was done for both fetuses due to fetal distress of one twin. They did not observe any adverse effects of tocolytic therapy 35.
The overall obstetric outcome of double uterus is poor but still better than the other Mullerian duct abnormalities like the septate or bicornuate uterus. The reason behind this occurs is that in double uterus the blood supply through the collateral circulation in between two horns is better in comparison to other Mullerian duct abnormalities. The successful pregnancy rate with double uterus is 57%, and the fetal survival rate is documented around 64% 36, 34, 37.
Most of the previous studies regarding didelphys uterus with twin gestation had the history of fertility treatment, and the termination of pregnancy was required by cesarean section either due to fetal malpresentation or fetal distress 38.
Double uterus is associated with a twin pregnancy is a high-risk pregnancy. The early detection of this anomaly of the uterus and accompanying pregnancy by ultrasonography is of great value. Close monitoring of fetal growth, biophysical profile, and the cervical condition is recommended throughout the pregnancy. The time and mode of delivery should be planned and discussed in detail with the couple during antenatal follow-up 34.
- Al Yaqoubi HN, Fatema N. Successful Vaginal Delivery of Naturally Conceived Dicavitary Twin in Didelphys Uterus: A Rare Reported Case. Case Reports in Obstetrics and Gynecology. 2017;2017:7279548. doi:10.1155/2017/7279548. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5591991/[↩][↩][↩][↩]
- Ozyuncu O., Turgal M., Yazicioglu A., Ozek A. Spontaneous twin gestation in each horn of uterus didelphys complicated with unilateral preterm labor. Case Reports in Perinatal Medicine. 2014;3(1) doi: 10.1515/crpm-2013-0061.[↩][↩][↩][↩]
- Heinonen P. K. Clinical implications of the didelphic uterus: long-term follow-up of 49 cases. European Journal of Obstetrics & Gynecology and Reproductive Biology. 2000;91(2):183–190. doi: 10.1016/S0301-2115(99)00259-6. https://www.ncbi.nlm.nih.gov/pubmed/10869793[↩][↩][↩][↩]
- Rezai S., Bisram P., Lora Alcantara I., Upadhyay R., Lara C., Elmadjian M. Didelphys uterus: a case report and review of the literature. Case Reports in Obstetrics and Gynecology. 2015;2015:5. doi: 10.1155/2015/865821.865821 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4576003/[↩]
- Yang M., Tseng J., Chen C., Li H. Delivery of double singleton pregnancies in a woman with a double uterus, double cervix, and complete septate vagina. Journal of the Chinese Medical Association. 2015;78(12):746–748. doi: 10.1016/j.jcma.2015.06.020. http://www.jcma-online.com/article/S1726-4901(15)00242-7/fulltext[↩][↩]
- Allegrezza D. M. Uterus didelphys and dicavitary twin pregnancy. Journal of Diagnostic Medical Sonography. 2016;23(5):286–289. doi: 10.1177/8756479307307267.[↩]
- Magudapathi C. Uterus didelphys with longitudinal vaginal septum: normal deliver—case report. Journal of Clinical Case Reports. 2012;2, article 13 doi: 10.4172/2165-7920.1000194.[↩][↩]
- Chandler T. M., Machan L. S., Cooperberg P. L., Harris A. C., Chang S. D. Müllerian duct anomalies: from diagnosis to intervention. The British Journal of Radiology. 2009;82(984):1034–1042. doi: 10.1259/bjr/99354802. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3473390/[↩]
- Grimbizis G. F., Camus M., Tarlatzis B. C., Bontis J. N., Devroey P. Clinical implications of uterine malformations and hysteroscopic treatment results. Human Reproduction Update. 2001;7(2):161–174. doi: 10.1093/humupd/7.2.161. https://www.ncbi.nlm.nih.gov/pubmed/11284660[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Acién P. Reproductive performance of women with uterine malformations. Human Reproduction. 1993;8(1):122–126. https://www.ncbi.nlm.nih.gov/pubmed/8458914[↩][↩][↩][↩]
- Ludmir J., Samuels P., Brooks S., Mennuti M. T. Pregnancy outcome of patients with uncorrected uterine anomalies managed in a high-risk obstetric setting. Obstetrics & Gynecology. 1990;75(6):906–910. https://www.ncbi.nlm.nih.gov/pubmed/2342734[↩]
- Raga F., Bauset C., Remohi J., Bonilla-Musoles F., Simón C., Pellicer A. Reproductive impact of congenital Müllerian anomalies. Human Reproduction. 1997;12(10):2277–2281. doi: 10.1093/humrep/12.10.2277. https://www.ncbi.nlm.nih.gov/pubmed/9402295[↩][↩]
- Lewenthal H., Biale Y., Ben-Adereth N. Uterus didelphys with a pregnancy in each horn. Case case report. BJOG: An International Journal of Obstetrics & Gynaecology. 1977;84(2):155–156. doi: 10.1111/j.1471-0528.1977.tb12546.x. https://www.ncbi.nlm.nih.gov/pubmed/843485[↩]
- Zhang Y., Zhao Y. Y., Qiao J. Obstetric outcome of women with uterine anomalies in China. Chinese Medical Journal. 2010;123(4):418–422. https://www.ncbi.nlm.nih.gov/pubmed/20193480[↩]
- Maneschi I., Maneschi F., Parlato M., Fucà G., Incandela S. Reproductive performance in women with uterus didelphys. Acta Europaea Fertilitatis. 1989;20(3):121–124. https://www.ncbi.nlm.nih.gov/pubmed/2624066[↩]
- Stanislavsky A. Herlyn-Werner-Wunderlich syndrome (HWW), 2015. https://radiopaedia.org/articles/herlyn-werner-wunderlich-syndrome[↩]
- Madureira A. J., Mariz C. M., Bernardes J. C., Ramos I. M. Case 94: uterus didelphys with obstructing hemivaginal septum and ipsilateral renal agenesis. Radiology. 2006;239(2):602–606. doi: 10.1148/radiol.2392031187. http://pubs.rsna.org/doi/full/10.1148/radiol.2392031187[↩][↩][↩]
- Karaca L., Pirimoglu B., Bayraktutan U., Ogul H., Oral A., Kantarci M. Herlyn-Werner-Wunderlich syndrome: a very rare urogenital anomaly in a teenage girl. The Journal of Emergency Medicine. 2015;48(3):e73–e75. doi: 10.1016/j.jemermed.2014.09.064. http://www.jem-journal.com/article/S0736-4679(14)01108-1/fulltext[↩]
- Wu T. H., Wu T. T., Ng Y. Y., et al. Herlyn-Werner-Wunderlich syndrome consisting of uterine didelphys, obstructed hemivagina and ipsilateral renal agenesis in a newborn. Pediatrics & Neonatology. 2012;53(1):68–71. doi: 10.1016/j.pedneo.2011.11.014. http://www.pediatr-neonatol.com/article/S1875-9572(11)00178-1/fulltext[↩]
- Sadler TW, Langman J (eds) (2000) Langman’s medical embryology, 8th edn. Lippincott Williams & Wilkins, Philadelphia[↩]
- Kiechl-Kohlendorfer U, Geley TE, Unsinn KM et al (2001) Diagnosing neonatal female genital anomalies using saline-enhanced sonography. AJR 177:1041–1044 https://www.ajronline.org/doi/full/10.2214/ajr.177.5.1771041[↩]
- Orazi C, Lucchetti MC, Schingo PM, Marchetti P, Ferro F. Herlyn- Werner-Wunderlich syndrome: uterus didelphys, blind hemivagina and ipsilateral renal agenesis. Sonographic and MR findings in 11 cases. Pediatr Radiol. 2007;37:657–65. https://link.springer.com/article/10.1007%2Fs00247-007-0497-y[↩]
- Acién P, Acién M, Sánchez-Ferrer M. Complex malformations of the female genital tract. New types and revision of classification. Hum Reprod. 2004;19:2377–84. https://academic.oup.com/humrep/article/19/10/2377/589016[↩]
- Madureira AJ, Mariz CM, Bernardes JC, Ramos IM. Case 94: Uterus didelphys with obstructing hemivaginal septum and ipsilateral renal agenesis. Radiology 2006. May;239(2):602-606 10.1148/radiol.2392031187 http://pubs.rsna.org/doi/full/10.1148/radiol.2392031187[↩]
- Kim TE, Lee GH, Choi YM, Jee BC, Ku SY, Suh CS, et al. Hysteroscopic resection of the vaginal septum in uterus didelphys with obstructed hemivagina: a case report. J Korean Med Sci 2007. Aug;22(4):766-769 10.3346/jkms.2007.22.4.766 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2693837/[↩]
- Nahum GG. Uterine anomalies. How common are they, and what is their distribution among subtypes? J Reprod Med 1998. Oct;43(10):877-887 https://www.ncbi.nlm.nih.gov/pubmed/9800671[↩]
- Heinonen P. K. Clinical implications of the didelphic uterus: long-term follow-up of 49 cases. European Journal of Obstetrics & Gynecology and Reproductive Biology. 2000;91(2):183–190. doi: 10.1016/S0301-2115(99)00259-6. http://www.ejog.org/article/S0301-2115(99)00259-6/fulltext[↩]
- Martínez-Beltrán M., Giménez J., Acién P. Uterus didelphys with septate cervix and unilateral endometrial carcinoma: a case report. Journal of Genital System & Disorders. 2012;1, article 1 doi: 10.4172/2325-9728.1000101.[↩]
- Woelfer B., Salim R., Banerjee S., Elson J., Regan L., Jurkovic D. Reproductive outcomes in women with congenital uterine anomalies detected by three-dimensional ultrasound screening. Obstetrics & Gynecology. 2001;98(6):1099–1103. doi: 10.1016/s0029-7844(01)01599-x. https://www.ncbi.nlm.nih.gov/pubmed/11755560[↩][↩]
- Takagi H., Matsunami K., Noda K., Furui T., Imai A. Magnetic resonance imaging in the evaluating of double uterus and associated urinary tract anomalies: a report of five cases. Journal of Obstetrics & Gynaecology. 2003;23(5):525–527. doi: 10.1080/0144361031000153783. https://www.ncbi.nlm.nih.gov/pubmed/12963513[↩]
- Heinonen P. K. Uterus didelphys: a report of 26 cases. European Journal of Obstetrics & Gynecology and Reproductive Biology. 1984;17(5):345–350.[↩]
- The obstetric outcomes of uterine anomalies with assisted reproductive technology. Wang, J. Fertility and Sterility , Volume 108 , Issue 3 , e347-e348. http://www.fertstert.org/article/S0015-0282(17)31541-8/fulltext[↩][↩]
- Pavone, M.E., King, J.A., and Vlahos, N. Septate uterus with cervical duplication and a longitudinal vaginal septum: a Müllerian anomaly without a classification. (494.e9–10)Fertil Steril. 2006; 85 http://www.fertstert.org/article/S0015-0282(05)03862-8/fulltext[↩]
- Acien P. Embrological observations on the female genital tract. Hum Reprod. 1992;7:437–45. https://www.ncbi.nlm.nih.gov/pubmed/1522183[↩][↩][↩]
- Acién P, Acién M, Sánchez-Ferrer M. Complex malformations of the female genital tract. New types and revision of classification. Hum Reprod. 2004;19:2377–84. https://www.ncbi.nlm.nih.gov/pubmed/15333604[↩]
- Zurawin RK, Dietrich JE, Heard MJ, Edwards CL. Didelphic uterus and obstructed hemivagina with renal agenesis: case report and review of the literature. J Pediatr Adolesc Gynecol. 2004;17:137–41. http://www.jpagonline.org/article/S1083-3188(04)00017-8/fulltext[↩]
- Haddad B, Barranger E, Paniel BJ. Blind hemivagina: long-term follow-up and reproductive performance in 42 cases. Hum Reprod. 1999;14:1962–4. https://www.ncbi.nlm.nih.gov/pubmed/10438409[↩]
- Arıkan İİ, Harma M, Harma Mİ, Bayar Ü, Barut A. Herlyn-Werner-Wunderlich syndrome (uterus didelphys, blind hemivagina and ipsilateral renal agenesis) – a case report. Journal of the Turkish German Gynecological Association. 2010;11(2):107-109. doi:10.5152/jtgga.2010.011. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3939086/[↩]





{kind=link}