Contents
What is Dressler syndrome
Dressler’s syndrome is a delayed type of pericarditis 1 — inflammation of the protective sac surrounding the heart (pericardium) (see Figures 1 and 2 below). Dressler’s syndrome is believed to be an immune system response after damage to heart tissue or to the pericardium, from events such as a heart attack, surgery or traumatic injury. Symptoms include chest pain, which may be similar to chest pain experienced during a heart attack.
Dressler’s syndrome may also be called postpericardiotomy syndrome, post-myocardial infarction syndrome and post-cardiac injury syndrome. With recent improvements in heart attack treatment, Dressler’s syndrome is less common than it used to be.
Dressler’s syndrome occurs from one week to several months after clinical onset of myocardial infarction with symptoms and manifestations similar to the post-cardiac injury syndrome. Dressler’s syndrome does not require transmural infarction 2 and can also appear as an extension of epistenocardiac pericarditis. Epistenocardiac pericarditis, caused by direct exudation, occurs in 5–20% of transmural myocardial infarctions but is clinically discovered rarely. The incidence of Dressler’s syndrome is 0.5–5% 3 and is still lower in patients treated with thrombolytics (<0.5%) 4, but was more frequent in cases of pericardial bleeding after antithrombotic treatment 5.
Symptoms are likely to appear weeks to months after a heart attack, surgery or injury to the chest 6.
Symptoms of Dressler’s syndrome might include:
- Chest pain that’s similar to a stabbing sensation, which may feel worse when swallowing
- Pain in the neck that may extend across the shoulders and/or arms
- An intermittent fever
- Nausea
- Light headedness, and
- In some cases, a sudden onset shortness of breath (if this occurs seek urgent medical attention).
The pain can resolve itself if sitting forward, allowing the heart to relax within the chest cavity.
Pericarditis causes chest pain and a high temperature (fever). It’s not usually serious, but it can cause complications. Get medical advice if you have chest pain.
The pericardium
The serous membrane is a thin double-layered membrane that covers, lines, partitions, or connects structures. The serous membrane lining the heart cavity and covering the heart is the pericardium. The visceral pericardium covers the surface of the heart; the parietal pericardium lines the chest wall. Between them is the pericardial cavity, filled with a small amount of lubricating serous fluid (see Figure 1).
The pericardium confines the heart to its position in the mediastinum, while allowing sufficient freedom of movement for vigorous and rapid contraction. The pericardium consists of two main parts: (1) the fibrous pericardium and (2) the serous pericardium (Figures 1 and 2). The superficial fibrous pericardium is composed of tough, inelastic, dense irregular connective tissue. It resembles a bag that rests on and attaches to the diaphragm; its open end is fused to the connective tissues of the blood vessels entering and leaving the heart. The fibrous pericardium prevents overstretching of the heart, provides protection, and anchors the heart in the mediastinum. The fibrous pericardium near the apex of the heart is partially fused to the central tendon of the diaphragm and therefore movement of the diaphragm, as in deep breathing, facilitates the movement of blood by the heart.
The deeper serous pericardium is a thinner, more delicate membrane that forms a double layer around the heart (Figure 2). The outer parietal layer of the serous pericardium is fused to the fibrous pericardium. The inner visceral layer of the serous pericardium, which is also called the epicardium, is one of the layers of the heart wall and adheres tightly to the surface of the heart. Between the parietal and visceral layers of the serous pericardium is a thin film of lubricating serous fluid. This slippery secretion of the pericardial cells, known as pericardial fluid, reduces friction between the layers of the serous pericardium as the heart moves. The space that contains the few milliliters of pericardial fluid is called the pericardial cavity.
Figure 1. Pericardium
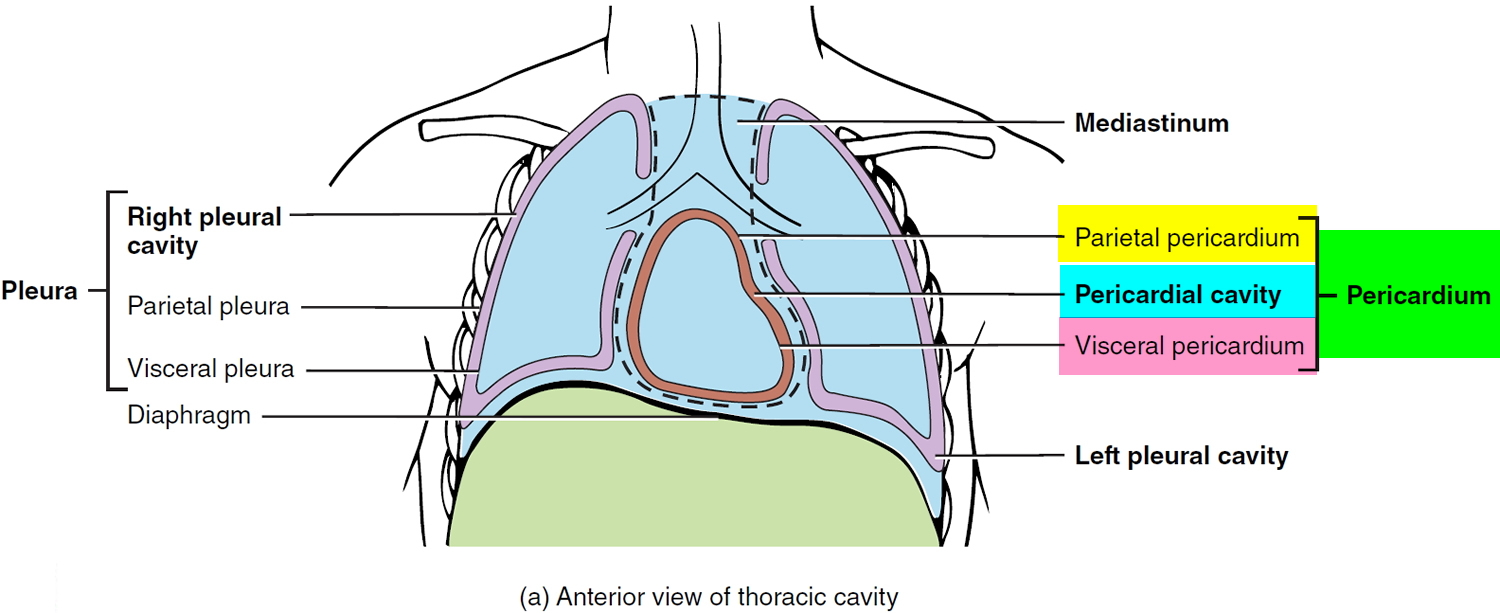 Figure 2. Pericardium, pericardial cavity and heart wall
Figure 2. Pericardium, pericardial cavity and heart wall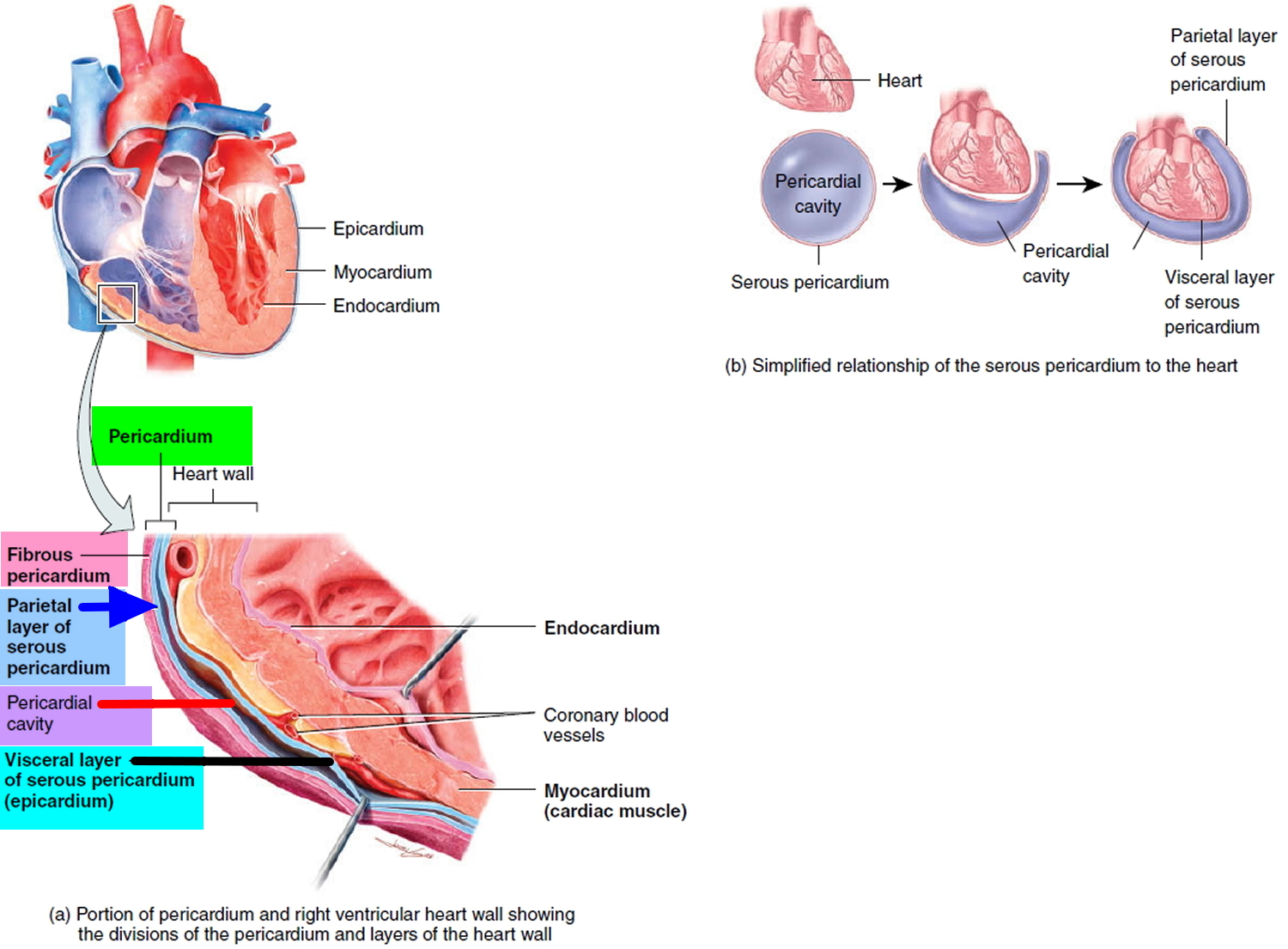
Dressler’s syndrome causes
Dressler’s syndrome is associated with an immune system response to heart damage. Your body reacts to the injured tissue by sending immune cells and proteins (antibodies) to clean up and repair the affected area. Sometimes this response causes excessive inflammation in the pericardium.
Postpericardiotomy syndrome might affect 10 to 40 percent of people who have had heart surgery.
Dressler syndrome outlook (prognosis)
Most people recover from pericarditis quickly, but for some it can take several months or never fully resolve, making long term sufferers vulnerable to physical and psychological issues. This can impact on quality of life for the sufferer and their families.
Unfortunately, pericarditis can come back despite medical or surgical intervention, so patients may feel uncertain about the future of their health. As this rare condition is not visible or associated with an unhealthy lifestyle, there is often a lack of understanding about the effects of living with pericarditis, meaning sufferers can often feel isolated, causing them to experience other effects such as anxiety, palpitations and panic.
Dressler’s syndrome complications
The immune system response that leads to Dressler’s syndrome might also cause fluid to accumulate in the membranes around your lungs (pleural effusion).
Rarely, Dressler’s syndrome can cause more-serious complications, including:
- Cardiac tamponade. Inflammation of the pericardium can cause fluids to accumulate in the sac (pericardial effusion). The fluid can put pressure on the heart, forcing it to work harder and reducing its ability to pump blood efficiently.
- Constrictive pericarditis. Recurring or chronic inflammation can cause the pericardium to become thick or scarred. The scarring can reduce the heart’s ability to pump blood efficiently.
Dressler’s syndrome diagnosis
Your doctor will conduct a thorough physical examination, including listening to your heart with a stethoscope. Certain characteristic sounds can indicate that your pericardium is inflamed or that fluid has accumulated around your heart.
Your doctor might then recommend tests, such as:
- Echocardiogram. Sound waves produce an image of your heart, helping your doctor to see if fluid is collecting around it.
- Electrocardiogram. Electrical impulses in your heart are recorded through wires attached to your skin. Certain changes in the electrical impulses can indicate pressure on your heart. But electrocardiogram readings may be abnormal after heart surgery, so your doctor likely won’t rely on this one test for a diagnosis of Dressler’s syndrome.
- Chest X-ray. An X-ray can help detect fluid building up around the heart or lungs and can help exclude other causes of your symptoms, such as pneumonia.
- Blood tests. The results of certain tests can indicate inflammatory activity that’s consistent with Dressler’s syndrome.
Dressler syndrome treatment
Postinfarction pericardial effusion >10 mm is most frequently associated with hemopericardium and two thirds of these patients may develop cardiac tamponade/free wall rupture 7. Urgent surgical treatment is life saving. However, if the immediate surgery is not available or contraindicated pericardiocentesis an intrapericardial fibrin-glue instillation could be an alternative in subacute cardiac tamponade 8.
Hospitalisation to observe for tamponade, differential diagnosis, and adjustments of treatment is needed. Corticosteroid therapy can be used for refractory symptoms only but could delay myocardial infarction healing 9.
The goals are to manage pain and reduce inflammation. Your doctor might recommend over-the-counter medications, such as:
- Ibuprofen (Advil, Motrin IB, others). Ibuprofen, which increases coronary flow, is the agent of choice 10.
- Aspirin, up to 650 mg every 4 hours for 2 to 5 days has also been successfully applied.
- Naproxen (Aleve)
Other nonsteroidal agents risk thinning the mycardial infarction zone 8.
If those medications don’t help, your doctor might prescribe:
- Colchicine. This anti-inflammatory medication might be used, along with over-the-counter medications, to treat Dressler’s syndrome. Some studies suggest that colchicine taken before cardiac surgery might help prevent postpericardiotomy. The effectiveness of colchicine for treating existing post-cardiac injury syndrome isn’t clear.
- Corticosteroids. These immune-system suppressants can reduce inflammation related to Dressler’s syndrome. Corticosteroids can have serious side effects and might interfere with the healing of damaged heart tissue after a heart attack or surgery. For those reasons, corticosteroids are generally used only when other treatments don’t work.
Treating complications
Complications of Dressler’s syndrome can require more-invasive treatments, including:
- Draining excess fluids. If you develop cardiac tamponade, your doctor will likely recommend a procedure (pericardiocentesis) in which a needle or small tube (catheter) is used to remove the excess fluid. The procedure is usually done using a local anesthetic.
- Removing the pericardium. If you develop constrictive pericarditis, you might need surgery to remove the pericardium (pericardiectomy).
Some research indicates that younger people and people who have symptoms of constrictive pericarditis soon after surgery are more likely to need invasive treatments for complications of Dressler’s syndrome.
- Sugiura T , Takehana K, Hatada K et al. Pericardial effusion after primary percutaneous transluminal coronary angioplasty in first Q-wave acute myocardial infarction. Am. J. Cardiol . 1998;81:1090–1093.[↩]
- Spodick DH . Post-myocardial infarction syndrome (Dressler’s syndrome). ACC Curr. J. Rev . 1995;4:35–37.[↩]
- Lichstein E . The changing spectrum of post-myocardial infarction pericarditis. Int. Cardiol . 1983;4:234–237.[↩]
- Shahar A , Hod H, Barabash GM et al. Disappearance of a syndrome: Dressler’s syndrome in the era of thrombolysis. Cardiology . 1994;85:255–258.[↩]
- Nagahama Y , Sugiura T, Takehana K et al. The role of infarction-associated pericarditis on the occurrence of atrial fibrillation. Eur. Heart J . 1998;19:287–292.[↩]
- Guidelines on the Diagnosis and Management of Pericardial Diseases Executive Summary: The Task Force on the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology, European Heart Journal, Volume 25, Issue 7, 1 April 2004, Pages 587–610, https://doi.org/10.1016/j.ehj.2004.02.002 https://academic.oup.com/eurheartj/article/25/7/587/654509[↩]
- Figueras J , Juncal A, Carballo J et al. Nature and progression of pericardial effusion in patients with a first myocardial infarction: relationship to age and free wall rupture. Am. Heart J . 2002;144(2):251–258.[↩]
- Joho S , Asanoi H, Sakabe M et al. Long-term usefulness of percutaneous intrapericardial fibrin-glue fixation therapy for oozing type of left ventricular free wall rupture: a case report. Circ. J . 2002;66(7):705–706.[↩][↩]
- Spodick DH . Pericardial diseases. Braunwald E, Zippes DP, Libby P. Heart disease. 6th ed. Philadelphia, London, Toronto, Montreal, Sydney, Tokyo: W.B. Saunders; 2001. p. 1823–1876.[↩]
- Spodick DH . Safety of ibuprofen for acute myocardial infarction pericarditis. Am. J. Cardiol . 1986;57(10):896.[↩]





{kind=link}