Contents
What is Dupuytren’s contracture
Dupuytren’s contracture (also called Dupuytren’s disease) is a painless progressive thickening, shortening and tightening (contracture) of palmar fascia (palmar aponeurosis) beneath the skin on the palm of your hand and fingers. Fascia is a type of connective tissue, which supports the body’s muscles, joints, organs, and skin and provides strength and flexibility to structures throughout the body. Dupuytren’s contracture is a condition that causes the fibrous tissue of the palmar fascia to shorten and thicken eventually creating a thick cord that can pull one or more fingers into a bent position. Permanently bent joints are called contractures. Dupuytren’s contracture initially presents as a firm nodule (or multiple nodules) on the palm of the hand proximal to the metacarpophalangeal joint. The fingers most commonly involved (in decreasing order) are the fourth, fifth, third, and second. The affected fingers can’t be straightened completely, which can complicate everyday activities such as face washing, preparing food, writing, hair combing, putting hands in your pockets, putting on gloves, shaking hands or play musical instruments.
Bilateral involvement is common, although one hand is usually more severely involved than the other 1. In about half of cases, Dupuytren contracture occurs in only one hand, affecting the right hand twice as often as the left. Which hand is affected does not seem to be related to whether the person is right-handed or left-handed.
Dupuytren’s contracture can be distinguished from other causes of hand contracture because it first appears as one or more small hard nodules that can be seen and felt under the skin of the palm. In some affected individuals the nodules remain the only sign of the disorder, and occasionally even go away without treatment, but in most cases the condition gradually gets worse. Over months or years, the abnormal fibrous tissue gets shorter and thicker, developing into tight bands of tissue called cords. These cords gradually draw the affected fingers downward so that they curl toward the palm. As the condition gets worse, it becomes difficult or impossible to extend the affected fingers, resulting in the contracture associated with this disorder. The ring finger is most often involved, followed by the little, middle, and index fingers. Occasionally the thumb is involved.
Dupuytren’s contracture is usually not painful, but in some cases people with this condition experience uncomfortable joint inflammation or sensations of burning or itching. Pressure or tension may also be experienced, especially when attempting to straighten affected joints.
People with Dupuytren’s contracture are at increased risk of developing other disorders in which similar connective tissue abnormalities affect other parts of the body. These include Garrod pads, which are nodules that develop on the knuckles; Ledderhose disease, also called plantar fibromatosis, in which contractures affect the foot; and, in males, Peyronie disease, which causes abnormal curvature of the penis.
Dupuytren’s contracture is more common in men older than 50 years; in persons of Northern European descent; and in persons who smoke, use alcohol, or have diabetes. In women, it is four times less common, and also tends to appear later and be less severe. However, Dupuytren contracture can occur at any time of life, including childhood. In patients younger than 50 years, Dupuytren’s contracture tends to progress faster than in older patients 2. The disease usually progresses in severity, although approximately 10 percent of cases regress without treatment 2. Smoking and alcohol use increase the chance that surgery will be needed.
Dupuytren’s contracture occurs in about 5 percent of people in the United States. Studies have identified Dupuytren’s contracture in persons of all racial groups 3, but the highest prevalence has been seen in northern Scotland, Iceland, Norway, and Australia 1 and Dupuytren contracture is less common in non-European populations. Dupuytren’s contracture is common in northern Europeans; 30 percent of Norwegian men over age 60 develop Dupuytren’s contracture. Studies suggest that a genetic predisposition to develop this disorder may have been spread through northern Europe and Britain by the Vikings. Evidence suggests an autosomal dominant pattern of inheritance with incomplete penetrance 4.
There is a strong association between diabetes and Dupuytren’s contracture. Studies have found a 3 to 33 percent prevalence of Dupuytren’s in patients with diabetes 1; however, these patients tend to have a mild form of Dupuytren’s contracture with slow progression 1. Greater alcohol intake per week is associated with increased risk of Dupuytren’s contracture, but most patients with the disease are not alcoholics 1. Smoking also increases the risk of the disease 5. Although the reason for this association is unclear, microvascular changes in smokers may play a role 5.
Other associations, such as trauma or epilepsy, are not well defined 1. Although trauma has been reported as a cause of Dupuytren’s contracture, studies have had mixed results 1. A connection between epilepsy and Dupuytren’s contracture has been reported 6 and some symptoms (e.g., palmar cords, knuckle pad thickening) have been shown to regress when anticonvulsant medications are discontinued 1. However, more recent, large cohort studies have not found an association between the disease and epilepsy or the use of epilepsy medication 7.
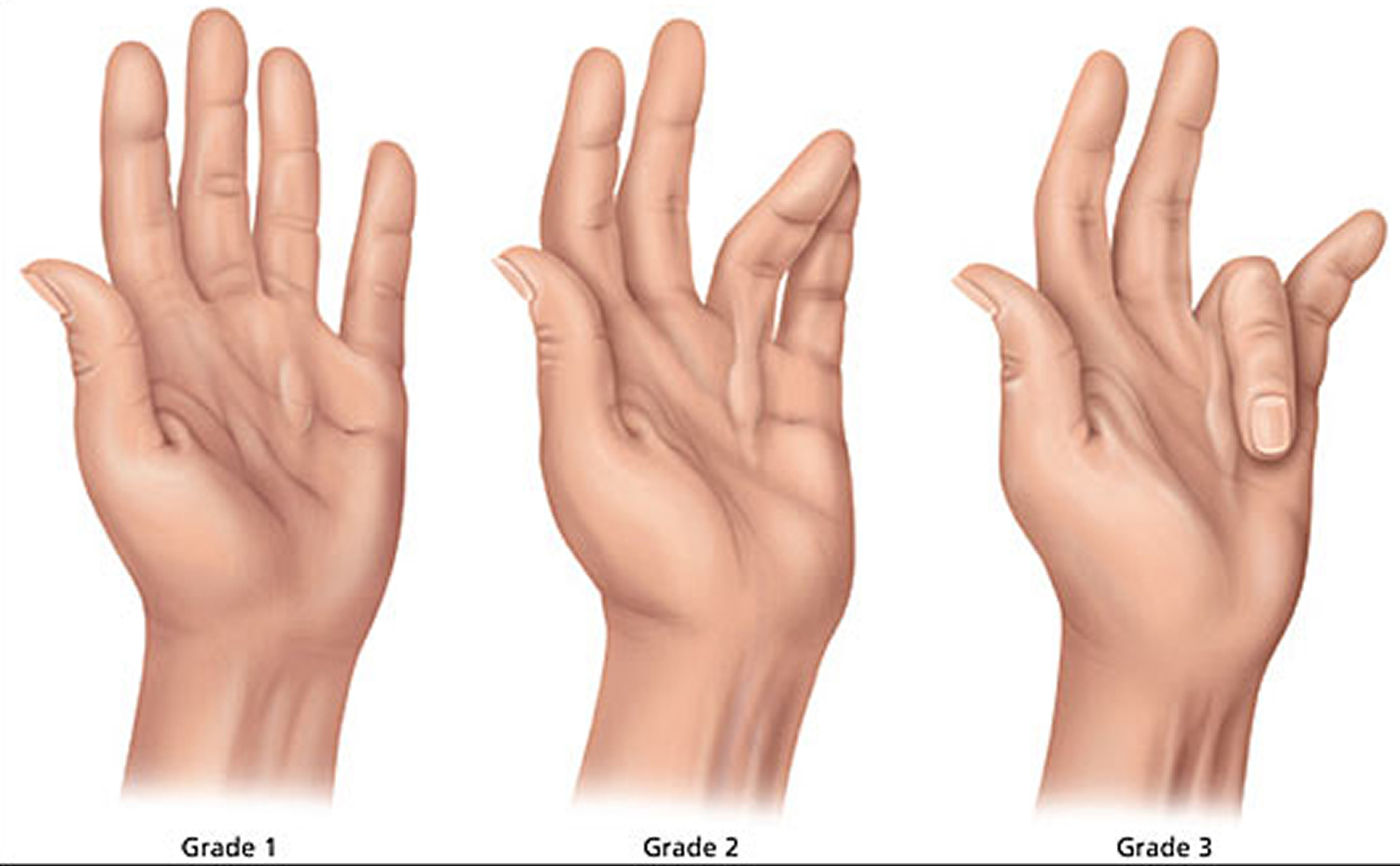
The Hueston tabletop test can help with the diagnosis. If a patient is unable to lay his or her palm flat on a tabletop, the test is positive. Disease progression is classified using a grading system (Figure 5) 8.
- Grade 1 disease presents as a thickened nodule and a band in the palmar aponeurosis; this band may progress to skin tethering, puckering, or pitting.
- Grade 2 presents as a peritendinous band, and extension of the affected finger is limited.
- Grade 3 presents as flexion contracture.
Soft tissue tumors of the palm and digits may be confused with Dupuytren’s contracture 1.
Dupuytren’s contracture initially can be managed with observation and non-surgical therapy. It will regress without treatment in approximately 10 percent of patients. Steroid injection into the nodule has been shown to reduce the need for surgery. Surgical referral should be made when metacarpophalangeal joint contracture reaches 30 degrees or when proximal interphalangeal joint contracture occurs at any degree. Timing of surgical intervention varies, but surgery is usually performed when the metacarpophalangeal joint contracture exceeds 40 degrees or when the proximal interphalangeal joint contracture exceeds 20 degrees. In-office percutaneous needle aponeurotomy is an alternative to surgery.
Figure 1. Palmar aponeurosis (palmar fascia which is continuous with the palmaris longus tendon)
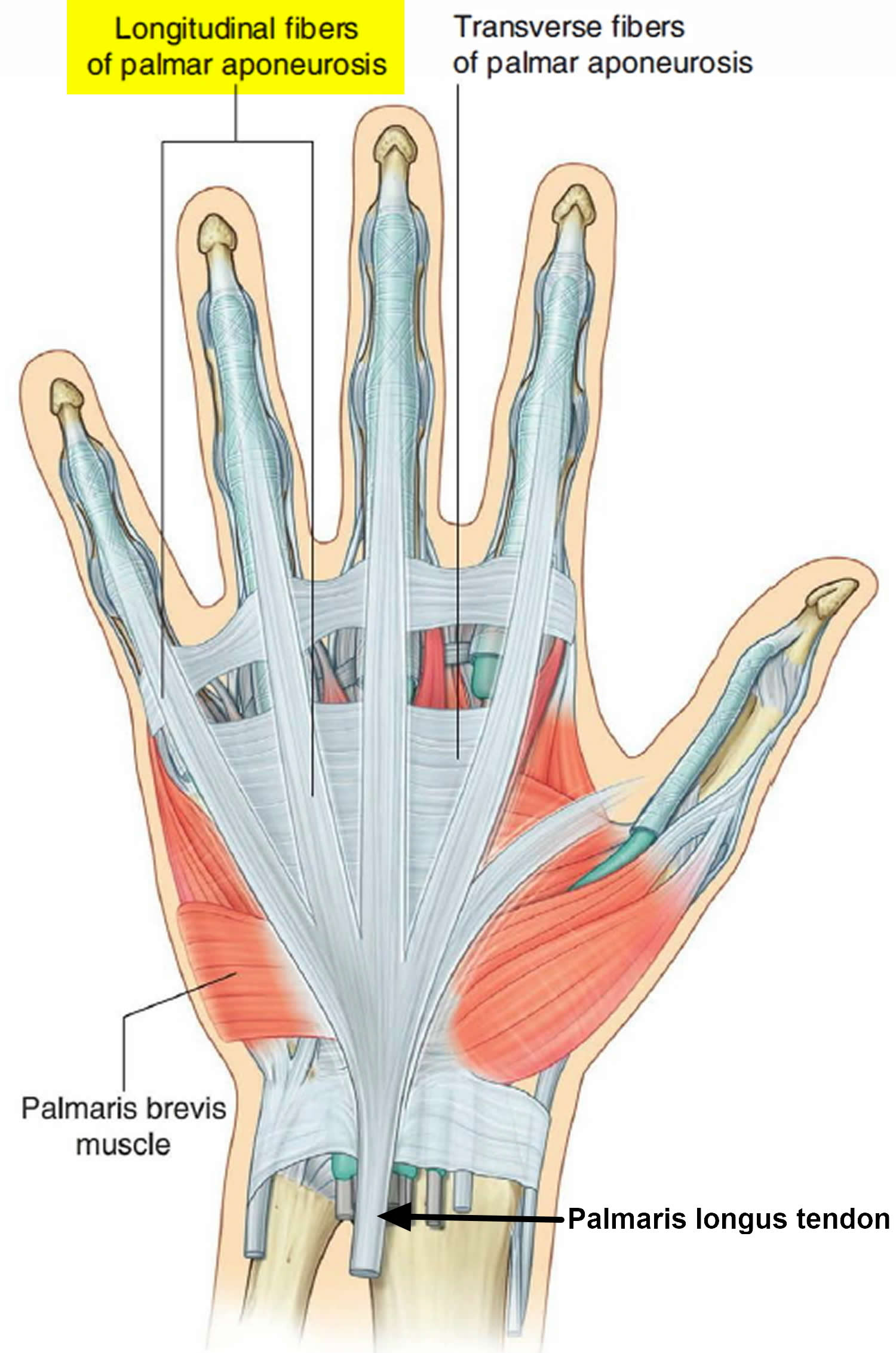 Figure 2. Palmaris longus muscle
Figure 2. Palmaris longus muscle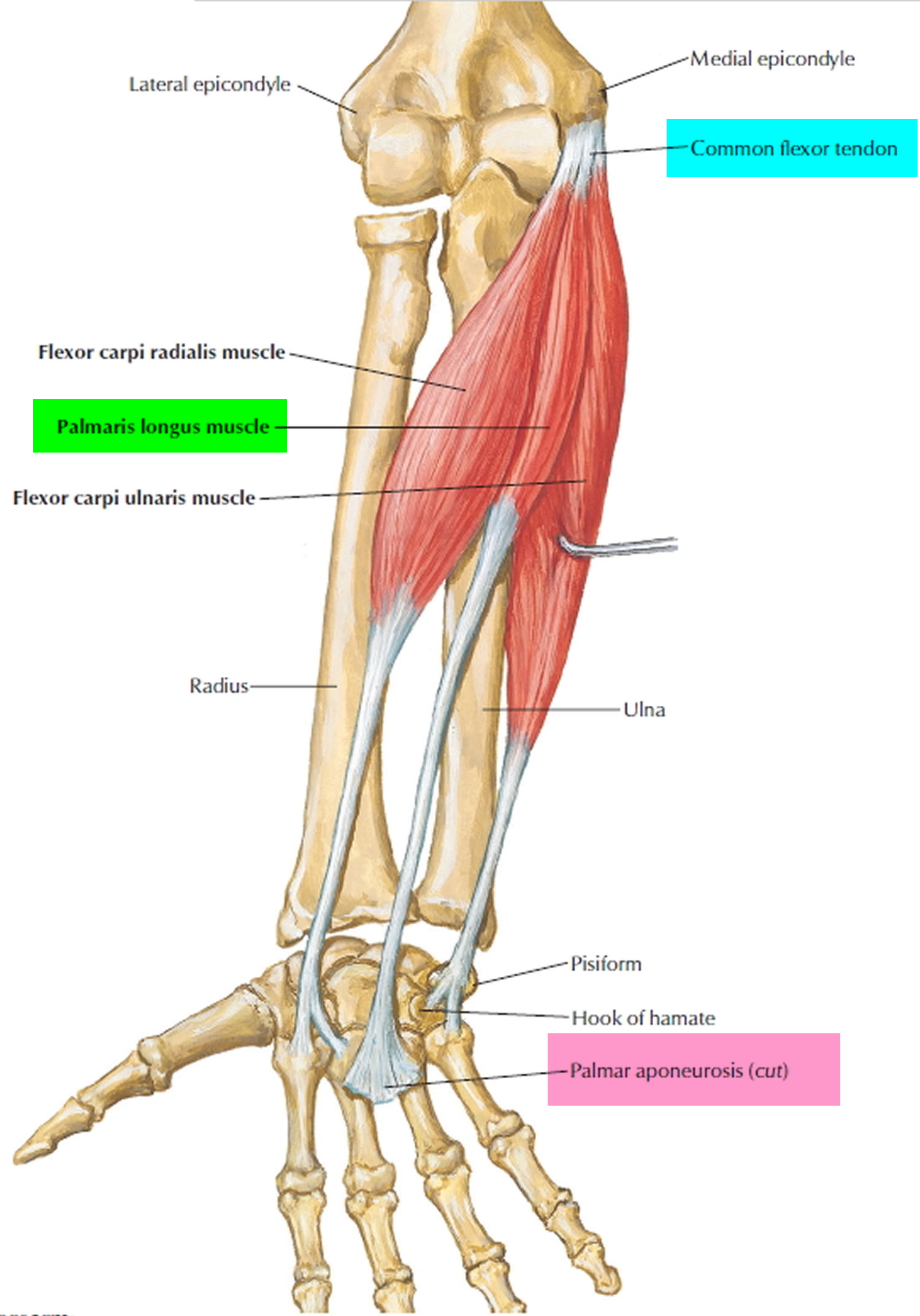
Figure 3. Metacarpophalangeal joint
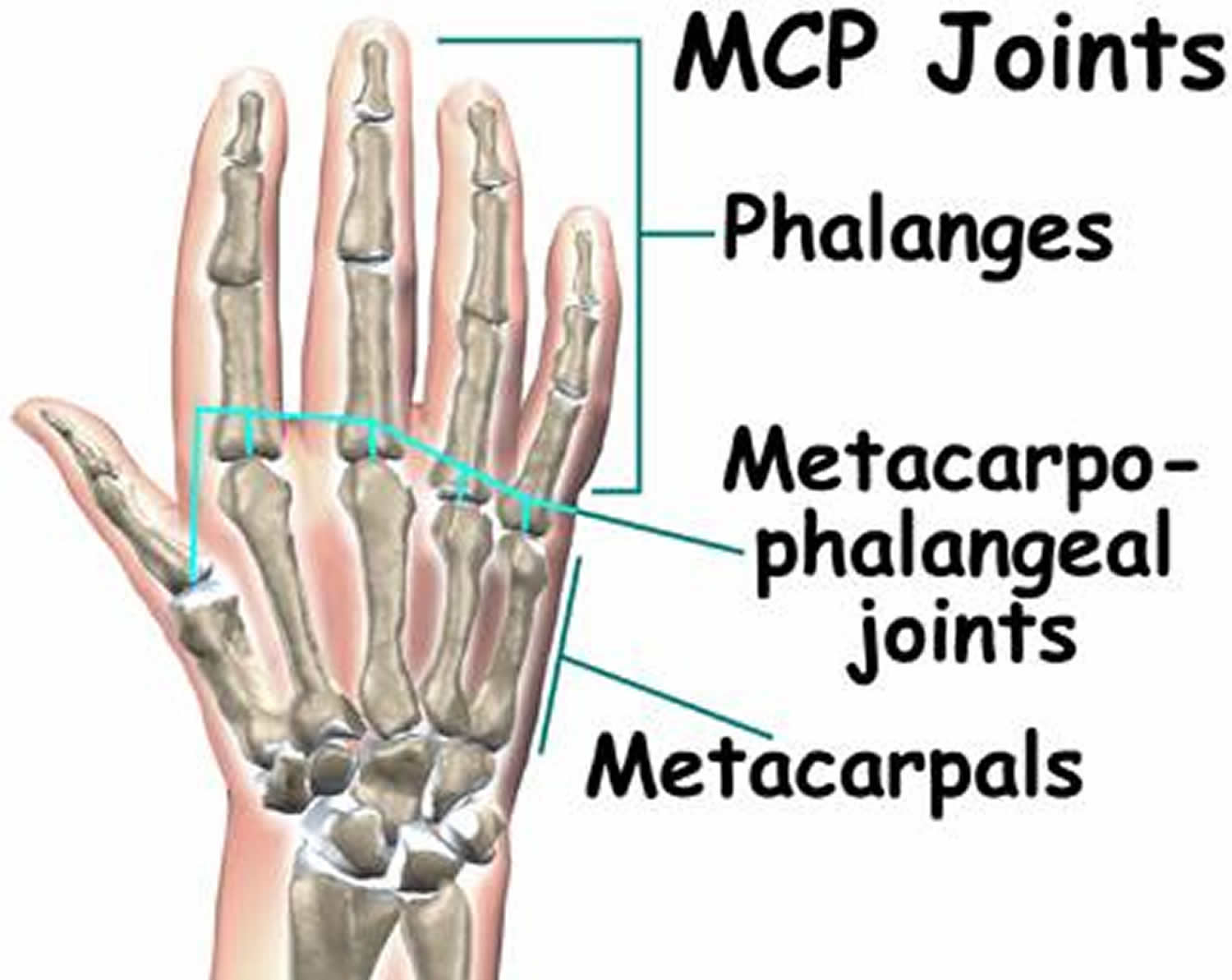
Figure 4. Dupuytren’s contracture

Figure 5. Dupuytren’s contracture severity grade
Dupuytren’s contracture complications
Dupuytren’s contracture can make it difficult to perform certain functions using your hand. Since the thumb and index finger aren’t usually affected, many people don’t have much inconvenience or disability with fine motor activities such as writing. But as Dupuytren’s contracture progresses, it can limit your ability to fully open your hand, grasp large objects or to get your hand into narrow places.
Dupuytren’s contracture causes
Doctors don’t know what causes Dupuytren’s contracture. There’s no evidence that hand injuries or occupations that involve vibrations to the hands cause the condition.
While the cause of Dupuytren contracture is unknown, changes in any of several genes are thought to affect the risk of developing this disorder. Some of these genes are involved in a biological process called the Wnt signaling pathway. This pathway promotes the growth and division (proliferation) of cells and is involved in the determination of the specialized functions a cell will have (differentiation).
Abnormal proliferation and differentiation of connective tissue cells called fibroblasts are important in the development of Dupuytren contracture. The palmar fascia of people with this disorder has an excess of myofibroblasts, which are a type of fibroblast containing protein strands called myofibrils. Myofibrils normally form the basic unit of muscle fibers, allowing them to contract. The increased number of myofibroblasts in this disorder cause abnormal contraction of the fascia and produce excess amounts of a connective tissue protein called type III collagen. The combination of abnormal contraction and excess type III collagen likely results in the shortening and thickening of fascia that occurs in Dupuytren contracture. However, it is unknown how changes in genes that affect the Wnt signaling pathway are related to these abnormalities and how they contribute to the risk of developing this disorder.
Other risk factors for developing Dupuytren contracture may include smoking; heavy alcohol use; liver disease; diabetes; high cholesterol; thyroid problems; certain medications, such as those used to treat epilepsy (anticonvulsants); and previous injury to the hand. The higher prevalence of the disorder in males than in females is thought to be due to sensitivity of the fascia to male sex hormones (androgens).
Risk factors for Dupuytren’s contracture
A number of factors are believed to increase your risk of the disease, including:
- Age. Dupuytren’s contracture occurs most commonly after the age of 50.
- Sex. Men are more likely to develop Dupuytren’s and to have more severe contractures than are women.
- Ancestry. People of Northern European descent are at higher risk of the disease.
- Family history. Dupuytren’s contracture often runs in families.
- Tobacco and alcohol use. Smoking is associated with an increased risk of Dupuytren’s contracture, perhaps because of microscopic changes within blood vessels caused by smoking. Alcohol intake also is associated with Dupuytren’s.
- Diabetes. People with diabetes are reported to have an increased risk of Dupuytren’s contracture.
Dupuytren contracture is usually passed down in families and is the most common inherited disorder of connective tissue. The inheritance pattern is often unclear. Some people who inherit gene changes associated with Dupuytren contracture never develop the condition.
In some families, Dupuytren contracture appears to be inherited in an autosomal dominant pattern, which means one copy of an altered gene in each cell is sufficient to cause the disorder. In these cases, an affected person usually has one parent with the condition.
In other families, the condition appears to be inherited in a mitochondrial pattern, which is also known as maternal inheritance. This pattern of inheritance applies to genes contained in mitochondrial DNA (mtDNA), a form of DNA found in energy-producing structures within cells (mitochondria). Because egg cells, but not sperm cells, contribute mitochondria to the developing embryo, children can inherit disorders resulting from mtDNA mutations only from their mother. These disorders can appear in every generation of a family and can affect both males and females, but fathers do not pass traits associated with changes in mtDNA to their children.
In some cases Dupuytren contracture is not inherited and occurs in people with no history of the condition in their family. These sporadic cases tend to begin later and be less severe than familial cases.
Dupuytren’s contracture symptoms
Dupuytren’s contracture typically progresses slowly, over years. The condition usually begins as a thickening of the skin on the palm of your hand. As it progresses, the skin on your palm might appear puckered or dimpled. A firm lump of tissue can form on your palm. This lump might be sensitive to the touch but usually isn’t painful.
In later stages of Dupuytren’s contracture, cords of tissue form under the skin on your palm and can extend up to your fingers. As these cords tighten, your fingers might be pulled toward your palm, sometimes severely into a permanently bent position.
The ring finger and pinky are most commonly affected, though the middle finger also can be involved. Only rarely are the thumb and index finger affected. Dupuytren’s contracture can occur in both hands, though one hand is usually affected more severely.
Dupuytren’s contracture diagnosis
In most cases, doctors can diagnose Dupuytren’s contracture by the look and feel of your hands. Other tests are rarely necessary.
Your doctor will compare your hands to each other and check for puckering on the skin of your palms. He or she will also press on parts of your hands and fingers to check for toughened knots or bands of tissue.
Your doctor also might check to see if you can put your hand flat on a tabletop or other flat surface. Not being able to fully flatten your fingers indicates you have Dupuytren’s contracture.
Dupuytren’s contracture treatment
If the disease progresses slowly, causes no pain and has little impact on your ability to use your hands for everyday tasks, you might not need treatment. Instead, you can wait and see if Dupuytren’s contracture progresses. You may wish to follow the progression with a tabletop test, which you can do on your own.
Treatment involves removing or breaking apart the cords that are pulling your fingers toward your palm. This can be done in several ways. The choice of procedure depends on the severity of your symptoms and other health problems you may have.
Percutaneous needle fasciotomy
A needle fasciotomy is also known as a needle aponeurotomy or a percutaneous needle fasciotomy (percutaneous means “performed through the skin”).It’s usually performed as an outpatient procedure , meaning you won’t need to be admitted to hospital. You’ll be given a local anesthetic to numb your hand without making you lose consciousness.
During the procedure, a sharp blade or a very fine needle will be inserted into the fibrous bands in the palm of your hand or your fingers. The blade or needle will be used to divide the cord under your skin.
By dividing the thickened tissue, your surgeon will release the tightness in your hand that’s forcing your finger to bend. The benefits of needle fasciotomy include:
- your fingers are less deformed
- you recover more quickly compared to more extensive surgery
- it’s suitable for people who are unable to have more extensive surgery, such as the very frail or elderly
- it has a low risk of complications (around 1%)
However, the rate of recurrence for Dupuytren’s contracture is very high: as many as 60% of people who have a needle fasciotomy experience Dupuytren’s contracture again within three to five years.
The main advantages of the needling technique are that there is no incision, it can be done on several fingers at the same time, and usually very little physical therapy is needed afterward. The disadvantage of percutaneous needle fasciotomy is some contractures are harder to treat with it and if the contracture is severe percutaneous needle fasciotomy will not get your finger as straight as other treatments. Moreover, the main disadvantage is that it can’t be used in some places in the finger because it could damage a nerve or tendon.
Dupuytren’s contracture enzyme injection
Injecting a type of enzyme into the taut cord in your palm can soften and weaken it — allowing your doctor to later manipulate your hand in an attempt to break the cord and straighten your fingers. The FDA has approved collagenase Clostridium histolyticum (Xiaflex) for this purpose. The advantages and disadvantages of the enzyme injection are similar to percutaneous needle fasciotomy.
This injection causes a degree of swelling and bruising of the hand. After having the injection, you’ll be monitored for around half an hour and then you can go home. You return to your doctor 24 hours later and they’ll straighten your bent finger and stretch it out for 10 to 20 seconds. This breaks the cord and should help to increase the range of movement in your bent finger. For approximately one to five days following the injection of the collagenase, the injected finger(s) are manipulated in the rooms with an injection of local anesthetic.
Don’t attempt to straighten your finger yourself within the first 24 hours, or squeeze or press the cord. Keeping your finger bent encourages the injected medicine to stay in the cord, which is where it needs to be. It also helps to keep the hand elevated to reduce swelling and prevent the medication leaking out.
If the first injection isn’t effective, you can have up to three injections in the same cord, with one month between each injection.
The most common side effects occur around the site of the injection and include:
- swelling
- itching
- bruising
- discoloration of skin, caused by bleeding
- pain
Some people may feel the lymph nodes in their arm pit are slightly enlarged for some days, while others may feel like they have a cold for a day or two after the injection.
These should improve within a week or two. Less common side effects include feeling sick or dizzy.
However, the long-term effects of collagenase clostridium histolyticum are unknown. And it may also not be widely available.
The collagenase injection has a significantly quicker recovery time compared to open surgery with less risk and produces nearly as good a contracture relief. There are risks of tendon or ligament rupture (very rare), and 1 in 8 patients have a small skin tear during manipulation which is treated by dressings for a few days.
A splint usually worn at night for approximately a month and exercises are undertaken some several weeks after collagenase treatment.
Dupuytren’s contracture steroid injection
Steroid injection for the treatment of Dupuytren’s contracture nodules should be proximal to and along the sides of the nodule (arrows). A study showed that injections with tri-amcinolone acetonide (Kenalog) monthly for up to five months, or every six weeks for up to three injections, followed by a six-month respite, lead to significant disease regression 9. In the study, an average of 3.2 injections per nodule was needed for improvement of the nodule and hand function 9.
Surgery was needed in fewer patients who received injections than would be anticipated in patients receiving expectant management alone 9. Possible complications of the procedure include tenderness, transient depigmentation, or atrophy at the injection site and rupture of the flexor tendon (more likely after repeated injections) 9.
Figure 6. Dupuytren’s contracture steroid injection

Dupuytren’s contracture surgery
Another option for people with advanced disease, limited function and progressing disease is to surgically remove the tissue in your palm affected by the disease. The main advantage to surgery is that it results in a more complete and longer-lasting release than that provided by the needle, steroid or enzyme methods. The main disadvantages are that physical therapy is usually needed after surgery, and recovery can take longer.
Patients requiring surgery have an increased overall and cancer-related mortality risk 10, probably secondary to smoking, alcohol use, and diabetes.
The two most common surgical techniques are:
- Open fasciotomy – where the shortened connective tissue is cut to relieve tension
- Fasciectomy – where the shortened connective tissue is removed
Open fasciotomy
An open fasciotomy is sometimes used to treat more severe cases of Dupuytren’s contracture. The procedure is more effective in the long term than a needle fasciotomy, but it’s also a more extensive operation and carries some additional risks.
Like a needle fasciotomy, an open fasciotomy will be carried out as an outpatient procedure under local anesthetic. The surgeon will make an incision in the skin of your hand, so they can gain access to the connective tissue underneath. They’ll then cut the thickened connective tissue to divide it up, allowing you to straighten your fingers.
After the surgery has finished, the cut on your hand is sealed with stitches and a dressing is applied. The recovery time for an open fasciotomy is slightly longer than that of a needle fasciotomy, because the wound will need time to heal.
Following the procedure, it’s likely that you’ll need to make another appointment to have your stitches removed, and you may be left with a small scar.
Fasciectomy Surgery
This procedure involves making some incisions in your hand and removing areas of the thickened fascia within the palm or finger(s) to allow the firm fibrous areas to be removed from your hand and your finger(s) to straighten. In some patients with severe contractures or contracture in several fingers, surgery may be the best option. If you want the maximum chance of improvement in contracture for the longest period possible, then surgery may also be the best choice for you. Surgery is most often carried out under an arm block, or general anesthetic. A tourniquet is used to reduce bleeding, and the wounds are dressed by a moderately large bandage or plaster splint following the procedure. The risks of surgery include infection (1-2%), stiffness, bruising, nerve injury numbness on the finger (under 1%), and blood vessel injury (rare). Also, recurrence of the Dupuytren’s contracture with time is likely over time. Dupuytren’s contracture can recur within 10 years after surgery in up to half of cases.
There are three variations of the fasciectomy procedure:
- Regional fasciectomy – where the affected connective tissue is removed through a single, larger incision; this is the most commonly used type of surgery for Dupuytren’s contracture
- Segmental fasciectomy – where one or more small cuts are made in the skin, through which small segments of connective tissue are removed
- Dermofasciectomy – where the affected connective tissue is removed, along with the overlying skin (which may also be affected by the disease) and the wound is sealed with a skin graft (where healthy skin is removed from another part of the body and used to cover the area of skin loss in your hand). People usually require months of intensive physical therapy afterward.
A fasciectomy is usually carried out under general anesthetic. This means you’ll be unconscious throughout the procedure and unable to feel pain. In some cases, regional anesthetic may be used. This is where local anesthetic is injected into the nerves near your neck, to numb your whole arm, but you remain conscious.
During the procedure, an incision will be made in your hand and the affected connective tissue will be removed. If it’s necessary to seal the wound using a skin graft, your surgeon will take a graft from an area of your body that’s usually covered by clothing, such as your upper arm, the front side of your elbow or your groin.
A fasciectomy is a more extensive operation than a fasciotomy, so the risk of complications is slightly higher, at around 5%. However, the results are longer-lasting. For example, the rate of recurrence of Dupuytren’s contracture following dermofasciectomy may be as low as 8%.
Fasciectomy Surgery Post-Operative Care
The hand must be elevated to prevent swelling for several days following the procedure. Hand therapy is commenced within a small number of days after surgery unless a skin graft is used, in which case hand therapy is delayed for a week. Absorbable sutures are used which do not require removal. A splint may be required at night time for several months following the operation, and extensive exercises under the control of our specialist hand therapists are required, both to maintain the correction of the contracture and to regain optimal hand function. The recovery time, rehabilitation time and intensity will be governed by the pre-operative degree of contracture, and the magnitude of surgery undertaken.
PIP (proximal interphalangeal) joint contractures are more likely to cause stiffness and less likely to respond to surgery if more severe 11. The longer a deformity is present, the greater the risk of an irreversible joint contracture.
Surgery risks
If your surgery is complex and extensive, your risk of developing complications will be greater than if you have a more minor procedure.
For needle fasciotomy, the rate of complications is low, at around 1%. For fasciectomy, studies have found complication rates to be higher, from around 5%. Some possible complications include:
- splitting the skin with the needle during a needle fasciotomy
- damage to the nerves supplying sensation to your fingertips – the nerves can be repaired, but it’s unlikely the fingers will recover their full sensation
- joint stiffness – this can be helped with hand therapy (see recovering from Dupuytren’s contracture for more information)
- wound failure – the wound or graft failing to heal (more likely to occur if you smoke)
- infection of the wound – usually treated with antibiotics
- hematoma – a blood-filled swelling that forms as the wound heals, usually in the palm; it can be drained to reduce the swelling
- scarring
- complex regional pain syndrome – a rare complication that causes the hand to become painful, stiff and swollen after surgery; it usually resolves within a few months, although it can sometimes be permanent
- finger loss (although this is very unlikely)
Discuss the risks of the surgical procedures used to treat Dupuytren’s contracture with your surgeon.
Recovery post surgery
Hand therapy
After surgery, you may need specialised hand therapy to help improve the function and range of movement of your hand. For example, you may need to have:
- physiotherapy – this could involve a number of techniques to help improve your range of movement, including massage, manipulation and exercise
- occupational therapy – if you’re struggling with everyday tasks and activities, either at work or at home, an occupational therapist will be able to provide you with practical support to make those tasks easier
How long you’ll need to have treatment or assistance for depends on the type of surgery you’ve had. For example, you may need hand therapy for up to six months after more extensive procedures.
Hand splinting
Splinting usually involves bandaging your fingers to a plastic strip while they’re in the straightest position you find comfortable. Splinting may initially be recommended all day, before being used only at night, and then not at all.
Splinting isn’t currently a standard procedure and some specialists prefer not to use splints. When splints are used, there’s often wide variation in the length of time they’re used for, the position of the fingers and how much force is used to keep the fingers straight.
Some specialists believe splints can positively influence the way that scar tissue forms after surgery, so that the scar doesn’t contract and cause the condition to return. Others believe splints can cause unnecessary pain, joint stiffness and swelling (edema), so prefer not to use them.
Several research studies have been carried out to try to determine whether or not using splints is effective in the recovery of Dupuytren’s contracture.
One study found that there was no difference between the range of hand movement experienced by a group of people who were routinely splinted after having types of surgery called a fasciectomy or a dermofasciectomy, and a group who received hand therapy and were only splinted if contractures occurred.
Driving
After having hand surgery, you can start driving as soon as you feel confident enough to control the car safely. This will usually be after about three weeks, but it may be longer if you’ve had a skin graft.
Work and sport
When you’ll be able to return to work depends on the nature of your job and the type of operation you’ve had.
If you do heavy manual work, you may not be able to return to work for six weeks after having a skin graft. If you work in an office, you may be able to return to light duties a few days after having a fasciotomy. The same advice applies to sport.
Recurrence
Surgery can help improve hand function in people affected by contractures, but it doesn’t stop the process that caused the contracture to develop in the first place. Therefore, there’s a chance the condition may return in the same place, or it may reappear somewhere else after treatment.
Recurrence is more likely to occur in younger people, people who had a severe contracture and those with a strong family history of the condition.
The chances of the condition returning after surgery also depend on the specific procedure you had. Dupuytren’s contracture recurs in more than half of people who have a type of minor procedure called a needle fasciotomy, but only about one in three people who have a fasciectomy. A dermofasciectomy is associated with the lowest risk of recurrence, with the condition reappearing in less than 1 in 10 people after the procedure.
The experience of the surgeon who carries out the procedure may also influence the chance of recurrence.
Home remedies
If you have mild Dupuytren’s contracture, you can protect your hands by:
- Avoiding a tight grip on tools by building up the handles with pipe insulation or cushion tape
- Using gloves with heavy padding during heavy grasping tasks
However, your condition may persist or worsen, despite these precautions.
No study has evaluated the effects of smoking cessation, decreased alcohol use, or diabetes control in patients with Dupuytren’s disease.
- Hart MG, Hooper G. Clinical associations of Dupuytren’s disease. Postgrad Med J. 2005;81:425–8.[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Gudmundsson KG, Arngrimsson R, Jonsson T. Eighteen years follow-up study of the clinical manifestations and progression of Dupuytren’s disease. Scand J Rheumatol. 2001;30:31–4.[↩][↩]
- Zerajic D, Finsen V. Dupuytren’s disease in Bosnia and Herzegovina. An epidemiological study. BMC Musculoskelet Disord. 2004;5:10.[↩]
- Hu FZ, Nystrom A, Ahmed A, Palmquist M, Dopico R, Mossberg I, et al. Mapping of an autosomal dominant gene for Dupuytren’s contracture to chromosome 16q in a Swedish family. Clin Genet. 2005;68:424–9.[↩]
- Godtfredsen NS, Lucht H, Prescott E, Sorensen TI, Gronbaek M. A prospective study linked both alcohol and tobacco to Dupuytren’s disease. J Clin Epidemiol. 2004;57:858–63.[↩][↩]
- Thurston AJ. Dupuytren’s disease. J Bone Joint Surg Br. 2003;85:469–77.[↩]
- Geoghegan JM, Forbes J, Clark DI, Smith C, Hubbard R. Dupuytren’s disease risk factors. J Hand Surg [Br]. 2004;29:423–6.[↩]
- Townley WA, Baker R, Sheppard N, Grobbelaar AO. Dupuytren’s contracture unfolded. BMJ. 2006;332:397–400.[↩]
- Ketchum LD, Donahue TK. The injection of nodules of Dupuytren’s disease with triamcinolone acetonide. J Hand Surg. 2000;25:1157–62.[↩][↩][↩][↩]
- Wilbrand S, Ekbom A, Gerdin B. A cohort study linked increased mortality in patients treated surgically for Dupuytren’s contracture. J Clin Epidemiol. 2005;58:68–74.[↩]
- Au-Yong IT, Wildin CJ, Dias JJ, Page RE. A review of common practice in Dupuytren surgery. Tech Hand Up Extrem Surg. 2005;9:178–87.[↩]





{kind=link}