
Contents
What is dysrhythmia
Dysrhythmia is also known as arrhythmia, which is a problem with the rate or rhythm of the heartbeat. During a dysrhythmia, the heart can beat too fast, too slowly, or with an irregular rhythm. When a heart beats too fast, the condition is called tachycardia. When a heart beats too slowly, the condition is called bradycardia.
Dysrhythmia is caused by changes in heart tissue and activity or in the electrical signals that control your heartbeat. These changes can be caused by damage from disease, injury, or genetics. Often there are no symptoms, but some people feel an irregular heartbeat. You may feel faint or dizzy or have difficulty breathing.
The most common test used to diagnose an arrhythmia is an electrocardiogram (EKG or ECG). Your doctor will run other tests as needed. She or he may recommend medicines, placement of a device that can correct an irregular heartbeat, or surgery to repair nerves that are overstimulating the heart. If dysrhythmia is left untreated, the heart may not be able to pump enough blood to the body. This can damage the heart, the brain, or other organs.
The heart’s electrical system
To understand the causes of cardiac dysrhythmia, it helps to understand how your heart’s internal electrical system works.
Your heart is made up of four chambers — two upper chambers (atria) and two lower chambers (ventricles).
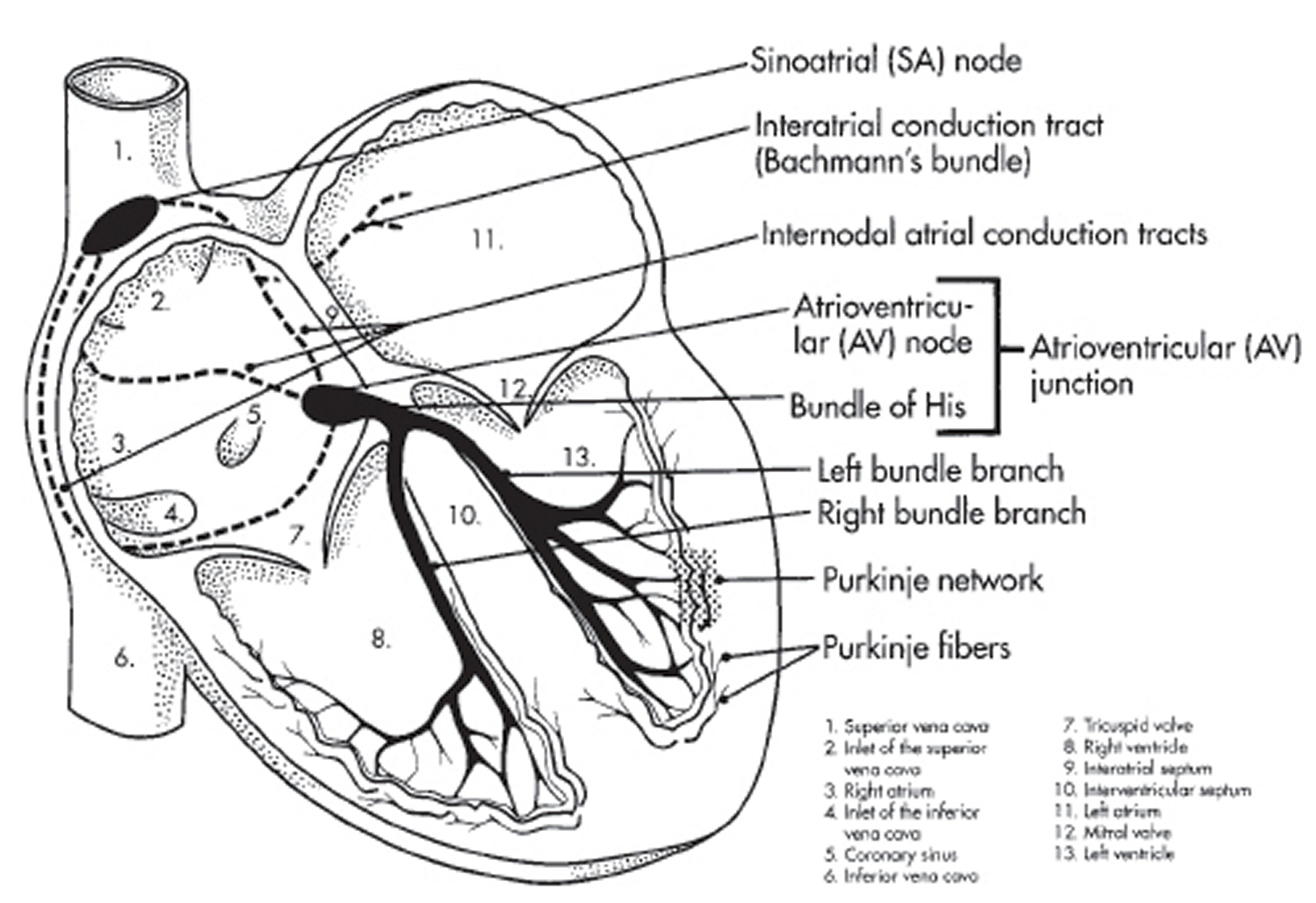
Your heart’s electrical system is made up of three main parts:
- The sinoatrial (SA) node, located in the right atrium of your heart
- The atrioventricular (AV) node, located on the interatrial septum close to the tricuspid valve
- The His-Purkinje system, located along the walls of your heart’s ventricles
Each beat of your heart is set in motion by an electrical signal from within your heart muscle. The signal is generated as the vena cavae fill your heart’s right atrium with blood from other parts of your body. The signal spreads across the cells of your heart’s right and left atria. In a normal, healthy heart, each beat begins with a signal from the natural pacemaker called the sinoatrial (SA) node — or sinus node — an area of specialized cells in the right atrium. This is why the sinoatrial (SA) node sometimes is called your heart’s natural pacemaker. Your pulse, or heart rate, is the number of signals the SA node produces per minute.
The sinoatrial (SA) node produces electrical impulses that normally start each heartbeat. This natural pacemaker produces the electrical impulses that trigger the normal heartbeat. From the sinus node, electrical impulses travel across the atria to the ventricles, causing them to contract and pump blood to your lungs and body.
From the sinoatrial (SA) node, electrical impulses travel across the atria, causing the atrial muscles to contract and pump blood into the ventricles.
The electrical impulses then arrive at a cluster of cells called the atrioventricular (AV) node — usually the only pathway for signals to travel from the atria to the ventricles.
The atrioventricular (AV) node slows down the electrical signal before sending it to the ventricles. This slight delay allows the ventricles to fill with blood.
The signal is released and moves along a pathway called the bundle of His, which is located in the walls of your heart’s ventricles. From the bundle of His, the signal fibers divide into left and right bundle branches through the Purkinje fibers. These fibers connect directly to the cells in the walls of your heart’s left and right ventricles.
The signal spreads across the cells of your ventricle walls, and both ventricles contract. However, this doesn’t happen at exactly the same moment.
The left ventricle contracts an instant before the right ventricle. This pushes blood through the pulmonary valve (for the right ventricle) to your lungs, and through the aortic valve (for the left ventricle) to the rest of your body.
As the signal passes, the walls of the ventricles relax and await the next signal.
This process continues over and over as the atria refill with blood and more electrical signals come from the SA node.
When electrical impulses reach the muscles of the ventricles, they contract, causing them to pump blood either to the lungs or to the rest of your body.
When anything disrupts this complex system, it can cause the heart to beat too fast (tachycardia), too slow (bradycardia) or with an irregular rhythm.
Your heart’s electrical system controls all the events that occur when your heart pumps blood. The electrical system also is called the cardiac conduction system. If you’ve ever seen the heart test called an EKG (electrocardiogram), you’ve seen a graphical picture of the heart’s electrical activity.
Figure 1. The heart’s electrical system

 What is the difference between arrhythmia and dysrhythmia?
What is the difference between arrhythmia and dysrhythmia?
There is no difference between arrhythmia and dysrhythmia. Arrhythmia is also known as dysrhythmia.
Types of dysrhythmia
Dysrhythmias differ from normal heartbeats in speed or rhythm. Dysrhythmias are also grouped by where they occur—in the upper chambers of the heart, in its lower chambers, or between the chambers. The main types of heart dysrhythmia are bradyarrhythmias; premature, or extra, beats; supraventricular arrhythmias; and ventricular arrhythmias.
Bradyarrhythmia
Bradyarrhythmia is a slow arrhythmia in a heart that beats too slowly—a condition called bradycardia. For adults, this means slower than 60 beats per minute. Some people, especially people who are young or physically fit, may normally have slow heart rates. For them, bradycardia is not dangerous and does not cause symptoms.
Premature or extra heartbeat
A premature heartbeat happens when the signal to beat comes early. It can feel like your heart skipped a beat. The premature, or extra, heartbeat creates a short pause, which is followed by a stronger beat when your heart returns to its regular rhythm. These extra heartbeats are the most common type of arrhythmia. They are called ectopic heartbeats and can trigger other arrhythmias.
Supraventricular arrhythmia
Arrhythmias that start in the heart’s upper chambers, called the atrium, or at the gateway to the lower chambers are called supraventricular arrhythmias. Supraventricular arrhythmias are known by their fast heart rates, or tachycardia. Tachycardia occurs when the heart, at rest, goes above 100 beats per minute. The fast pace is sometimes paired with an uneven heart rhythm. Sometimes the upper and lower chambers beat at different rates.
Types of supraventricular arrhythmias include:
- Atrial fibrillation. This is one of the most common types of arrhythmia. The heart can race at more than 400 beats per minute.
- Atrial flutter. Atrial flutter can cause the upper chambers to beat 250 to 350 times per minute. The signal that tells the upper chambers to beat may be disrupted when it encounters damaged tissue, such as a scar. The signal may find an alternate path, creating a loop that causes the upper chamber to beat repeatedly. As with atrial fibrillation, some but not all of these signals travel to the lower chambers. As a result, the upper chambers and lower chambers beat at different rates.
- Paroxysmal supraventricular tachycardia (PSVT). In paroxysmal supraventricular tachycardia (PSVT), electrical signals that begin in the upper chambers and travel to the lower chambers cause extra heartbeats. This arrhythmia begins and ends suddenly. It can happen during vigorous physical activity. It is usually not dangerous and tends to occur in young people.
Ventricular arrhythmia
These arrhythmias start in the heart’s lower chambers. They can be very dangerous and usually require medical care right away.
- Ventricular tachycardia is a fast, regular beating of the ventricles that may last for only a few seconds or for much longer. A few beats of ventricular tachycardia often do not cause problems. However, episodes that last for more than a few seconds can be dangerous. Ventricular tachycardia can turn into other more serious arrhythmias, such as ventricular fibrillation, or v-fib.
- Ventricular fibrillation occurs if disorganized electrical signals make the ventricles quiver instead of pumping normally. Without the ventricles pumping blood to the body, sudden cardiac arrest and death can occur within a few minutes. Torsades de pointes is a type of arrhythmia that causes a unique pattern on an EKG and often leads to ventricular fibrillation.
Dysrhythmia causes
Dysrhythmia is caused by changes to your heart tissue. Dysrhythmia can also occur suddenly as a result of exertion or stress, imbalances in the blood, medicines, or problems with electrical signals in the heart. Typically, a dysrhythmia is set off by a trigger, and the irregular heartbeat can continue if there is a problem in the heart. Sometimes the cause of a dysrhythmia is unknown.
Changes to the heart
The following conditions may cause dysrhythmia:
- Changes to the heart’s anatomy
- Reduced blood flow to the heart or damage to the heart’s electrical system
- Restoring blood flow as part of treating a heart attack
- Stiffening of the heart tissue, known as fibrosis, or scarring
Exertion or strain
Strong emotional stress, anxiety, anger, pain, or a sudden surprise can make the heart work harder, raise blood pressure, and release stress hormones. Sometimes these reactions can lead to dysrhythmias. If you have heart disease, physical activity can trigger dysrhythmia due to an excess of hormones such as adrenaline. Sometimes vomiting or coughing can trigger dysrhythmia.
Imbalances in the blood
An excess or deficiency of electrolytes, hormones, or fluids can alter your heartbeat.
- An excess of thyroid hormone can cause the heart to beat faster, and thyroid deficiency can slow your heart rate.
- Dehydration can cause the heart to race.
- Low blood sugar, from an eating disorder or higher insulin levels in someone who has diabetes, can lead to slow or extra heartbeats.
- Low levels of potassium, magnesium, or calcium can trigger dysrhythmia. These electrolyte disturbances can occur after a heart attack or surgery.
Medications
Certain medicines can cause dysrhythmia. These include medicines to treat high blood pressure and other conditions, including dysrhythmia, depression, and psychosis. Some people also need to be careful about taking certain antibiotics and over-the-counter medicines, such as allergy and cold medicines.
Problems with the electrical signals in the heart
An dysrhythmia can occur if the electrical signals that control the heartbeat are delayed or blocked. This can happen when the nerve cells that produce electrical signals do not work properly or when the electrical signals do not travel normally through the heart. Another part of the heart could start to produce electrical signals, disrupting a normal heartbeat.
Disorders of electrical signaling in the heart are called conduction disorders.
As part of daily living, your heart change pace to accommodate a wide range of activities, from sleeping to working out. These changes are controlled by the parasympathetic nervous system and the sympathetic nervous system. Overstimulation of either system can cause dysrhythmia.
- The parasympathetic nervous system slows your heart rate and prepares other functions when your body is at rest. It is stimulated by extreme cold or bouts of coughing. Nerve activity slows electrical signals in the heart and extends the time it takes for the heart to relax and fill. Overstimulation of the parasympathetic nervous system can lead to bradycardia.
- The sympathetic nervous system prepares your body for action, making your heart beat faster and making it easier for you to breathe. The adrenal glands release the hormone adrenaline that sparks these changes. The sympathetic nervous system is active in the body’s response to stress. Overstimulation from intense stress can also cause tachyarrhythmias.
Risk factors for developing cardiac dysrhythmia
You may have an increased risk of dysrhythmia because of your age, environment, family history and genetics, habits in your daily life, certain medical conditions, race or ethnicity, sex, or surgery.
Age
The chances of having dysrhythmia grow as we age, in part because of changes in heart tissue and in how the heart works over time. Older people are also more likely to have health conditions, including heart disease, that raise the risk of dysrhythmia.
Some types of dysrhythmia happen more often in children and young adults, including dysrhythmias due to congenital heart defects or inherited conduction disorders.
Environment
Some research suggests that exposure to air pollutants, especially particulates and gases, is linked to a short-term risk of dysrhythmia.
Family history and genetics
You may have an increased risk of some types of dysrhythmia if your parent or other close relative has had dysrhythmia, too. Also, some inherited types of heart disease can raise your risk of dysrhythmia. With some conduction disorders, gene mutations cause the ion channels that transmit signals through heart cells to work incorrectly or stop working.
Lifestyle habits
Your risk for dysrhythmia may be higher because of certain lifestyle habits, including:
- Drinking alcohol
- Smoking
- Using illegal drugs, such as cocaine or amphetamines
Other medical conditions
Dysrhythmias are more common in people who have diseases or conditions that weaken the heart, but many conditions can raise the risk for dysrhythmia. These include:
- Aneurysms
- Autoimmune disorders, such as rheumatoid arthritis and lupus
- Diabetes, which increases the risk of high blood pressure and coronary heart disease
- Diseases of the heart and blood vessels, including a heart that is larger than normal and heart inflammation
- Eating disorders, such as bulimia and anorexia, which cause electrolyte imbalance and severe malnutrition
- Heart attack
- Heart failure, which weakens the heart and changes the way electrical signals move through the heart
- Heart tissue that is too thick or stiff or that has not formed normally. dysrhythmias can be more common among people who have had surgery to repair a congenital heart defect.
- High blood pressure
- Influenza, or flu
- Kidney disease
- Heart valves. Leaking or narrowed heart valves make the heart work too hard and can lead to heart failure.
- Low blood sugar
- Lung diseases, such as chronic obstructive pulmonary disease (COPD)
- Musculoskeletal disorders
- Obesity
- Overactive or underactive thyroid gland, caused by too much or too little thyroid hormone in the body. The most common cause of excess thyroid hormone is Graves’ disease.
- Sepsis, a toxic immune response to infection
- Sleep apnea, which can stress the heart by preventing it from getting enough oxygen
Race or ethnicity
Studies suggest that white Americans may be more likely than African Americans to have some dysrhythmias, such as atrial fibrillation, although African Americans have higher rates of high blood pressure and other dysrhythmia risk factors.
Sex
Some studies suggest that men are more likely to have atrial fibrillation than women. However, women taking certain medicines appear to be at a higher risk of a certain type of dysrhythmia. Certain times of the menstrual cycle also appear to increase women’s risk of some dysrhythmia events. If you are a pregnant woman, you may notice that an existing dysrhythmia occurs more often. Benign extra beats are also more common during pregnancy. In some cases, the complications that can develop with dysrhythmia also differ by sex.
Surgery
You may be at a higher risk of developing atrial flutter in the early days and weeks after surgery involving the heart, lungs, or esophagus.
Dysrhythmia screening and prevention
If you or your child is at increased risk of dysrhythmia, the doctor may want to do a screening to assess the risk of a life-threatening event. Sometimes screening is required to participate in competitive sports. If your child carries a genetic risk of dysrhythmia, your child’s doctor may recommend regular screening to monitor your child’s heart or other family members’ health. The doctor may also ask about risk factors and may suggest genetic testing if your child, parent, or other family member has a known or suspected dysrhythmia or other heart condition. Heart-healthy lifestyle changes and other precautions can help decrease the risk of triggering dysrhythmia.
Screening tests
Your doctor may recommend screening tests based on your risk factors, such as age or family history.
An electrocardiogram (EKG or ECG) is the main test for detecting dysrhythmia. An EKG records the heart’s electrical activity. Your doctor may do the test while you are at rest or may do a stress test, which records the heart’s activity when it is working hard. Your doctor may also give you a portable monitor to wear for a day or several days if no dysrhythmia was detected during testing in the clinic. If you have a child who is at risk of dysrhythmia because of a genetic condition, the doctor may recommend regular testing for your child and his or her siblings.
Genetic testing can help you understand your risk when a family member has been diagnosed with a genetic condition. Testing is especially important if your newborn or another close relative died suddenly and had a genetic risk. Your doctor may also suggest genetic testing if you have a history of fainting or have survived cardiac arrest or near drowning.
Imaging tests, such as cardiac magnetic resonance imaging (MRI), can help detect scarring or other problems that can increase your risk of dysrhythmia.
Prevention strategies
Learn about prevention strategies that your doctor may recommend, including:
- Avoiding triggers, such as caffeine or stimulant medicines, that can cause dysrhythmias or make them worse. Your doctor can also help if you are trying to avoid illegal drugs.
- Getting an implantable or wearable cardioverter defibrillator to prevent sudden cardiac arrest from dysrhythmia if you have heart disease. Defibrillators can correct dysrhythmias by sending an electric shock to the heart.
- Making heart-healthy lifestyle changes, such as heart-healthy eating, being physically active, aiming for a healthy weight, quitting smoking, and managing stress
- Monitoring you after surgery, if you are having heart surgery. The surgical team may also use medicine and maintain or supplement electrolyte levels during or after the procedure to prevent dysrhythmia.
If you are the parents of a child with an inherited condition that increases the risk of dysrhythmia, discuss prevention strategies with your pediatrician as part of your child’s care.
- If your child is a newborn, follow safe sleep recommendations to help reduce the risk of SIDS.
- Your doctor may recommend routine assessments of your child’s heart activity to detect patterns or symptoms of dysrhythmia that emerge over time.
Dysrhythmia signs and symptoms
An dysrhythmia may not cause any obvious signs or symptoms. You may notice something that occurs only occasionally, or your symptoms may become more frequent over time. Keep track of when and how often dysrhythmia occurs, what you feel, and whether these things change over time. They are all important clues your doctor can use. If left untreated, dysrhythmia can lead to life-threatening complications such as stroke, heart failure, or sudden cardiac arrest.
You may be able to feel a slow or irregular heartbeat or notice pauses between heartbeats. If you have palpitations, you may feel like your heart skipped a beat or may notice it pounding or racing. These are all symptoms of dysrhythmia.
More serious signs and symptoms include:
- Anxiety
- Blurred vision
- Chest pain
- Difficulty breathing
- Fainting or nearly fainting
- Foggy thinking
- Fatigue
- Sweating
- Weakness, dizziness, and light-headedness
Some dysrhythmias tend to happen at certain times or under certain circumstances. If you notice signs or symptoms of dysrhythmia, note when they happened and what you were doing. This information can help your doctor diagnose what is going on and find the right treatment. Here are questions to ask yourself.
- Did it happen at night?
- Did you stand up after sitting or lying down?
- Were you lying down?
- Were you playing a sport or otherwise exerting yourself?
- Were you swimming or diving?
Dysrhythmia complications
Dysrhythmias that are unrecognized or left untreated can cause sometimes life-threatening complications affecting the heart and brain.
- Cognitive impairment and dementia. Alzheimer’s disease and vascular dementia are more common in people who have dysrhythmia. This may be due to reduced blood flow to the brain over time.
- Heart failure. Repeat dysrhythmias can lead to a rapid decline in the ability of the lower chambers to pump blood. Heart failure is especially likely to develop or to grow worse as a result of dysrhythmia when you already have heart disease.
- Stroke. This can occur in some patients who have atrial fibrillation. With dysrhythmia, blood can pool in the atria, causing blood clots to form. If a clot breaks off and travels to the brain, it can cause a stroke.
- Sudden cardiac arrest. The heart may suddenly and unexpectedly stop beating as a result of ventricular fibrillation.
- Sudden infant death syndrome (SIDS). SIDS can be attributed to an inherited conduction disorder that causes dysrhythmia.
- Worsening dysrhythmia. Some dysrhythmias trigger another type of dysrhythmia or get worse over time.
Dysrhythmia diagnosis
To diagnose dysrhythmia, your doctor will ask you about your symptoms, your medical history, and any signs of dysrhythmia in your family. Your doctor may also do an EKG and a physical exam as part of your diagnosis. Additional tests may be necessary to rule out another cause or to help your doctor decide on treatment.
Medical history
To diagnose an dysrhythmia, your doctor will ask about your eating and physical activity habits, family history, and other risk factors for dysrhythmia. Your doctor may ask whether you have any other signs or symptoms. This information can help your doctor determine whether you have complications or other conditions that may be causing you to have dysrhythmia.
Physical exam
During a physical exam, your doctor may take these steps:
- Check for swelling in your legs or feet, which could be a sign of an enlarged heart or heart failure
- Check your pulse to find out how fast your heart is beating
- Listen to the rate and rhythm of your heartbeat
- Listen to your heart for a heart murmur
- Look for signs of other diseases, such as thyroid disease, that could be causing the dysrhythmia
Diagnostic tests and procedures
Your doctor may order some of the following tests to diagnose dysrhythmia:
- Blood tests to check the level of certain substances in the blood, such as potassium and thyroid hormone, that can increase your risk of dysrhythmia.
- Cardiac catheterization to see whether you have complications from heart disease.
- Chest X-ray to show whether your heart is larger than normal.
- Echocardiography (echo) to provide information about the size and shape of your heart and how well it is working. Echocardiography may also be used to diagnose fetal dysrhythmia in the womb.
- EKG, or ECG, to see how fast the heart is beating and whether its rhythm is steady or irregular. This is the most common test used to diagnose dysrhythmias.
- Electrophysiology study (EPS) to look at the electrical activity of the heart. The study uses a wire to electrically stimulate your heart and trigger an dysrhythmia. If your doctor has already detected another condition that raises your risk, an EPS can help him or her assess the possibility that an dysrhythmia will develop. An EPS also allows your doctor to see whether a treatment, such as medicine, will stop the problem.
- Holter or event monitor to record your heart’s electrical activity over long periods of time while you do your normal activities.
- Implantable loop recorder to detect abnormal heart rhythms. It is placed under the skin and continuously records your heart’s electrical activity. The recorder can transmit data to the doctor’s office to help with monitoring. An implantable loop recorder helps doctors figure out why a person may be having palpitations or fainting spells, especially if these symptoms do not happen very often.
- Sleep study to see whether sleep apnea is causing your dysrhythmia.
- Stress test or exercise stress test to detect dysrhythmias that happen while the heart is working hard and beating fast. If you cannot exercise, you may be given medicine to make your heart work hard and beat fast.
- Tilt table testing to help find the cause of fainting spells. You lie on a table that moves from a lying-down position to an upright position. The change in position may cause you to faint. Your doctor watches your symptoms, heart rate, EKG reading, and blood pressure throughout the test.
- Ultrasound to diagnose a suspected fetal dysrhythmia in the womb.
Dysrhythmia treatment
Common dysrhythmia treatments include heart-healthy lifestyle changes, medicines, surgically implanted devices that control the heartbeat, and other procedures that treat abnormal electrical signals in the heart.
Healthy lifestyle changes
Your doctor may recommend that you adopt the following lifelong heart-healthy lifestyle changes to help lower your risk for conditions such as high blood pressure and heart disease, which can lead to dysrhythmia.
- Aiming for a healthy weight
- Being physically active
- Heart-healthy eating
- Managing stress
- Quitting smoking
Medications
Your doctor may give you medicine for your dysrhythmia. Some medicines are used in combination with each other or together with a procedure or a pacemaker. If the dose is too high, medicines to treat dysrhythmia can cause an irregular rhythm. This happens more often in women.
- Adenosine to slow a racing heart. Adenosine acts quickly to slow electrical signals. It can cause some chest pain, flushing, and shortness of breath, but any discomfort typically passes soon.
- Atropine to treat a slow heart rate. This medicine may cause difficulty swallowing.
- Beta blockers to treat high blood pressure or a fast heart rate or to prevent repeat episodes of dysrhythmia. Beta blockers can cause digestive trouble, sleep problems, and sexual dysfunction and can make some conduction disorders worse.
- Blood thinners to reduce the risk of blood clots forming. This helps prevent stroke. With blood-thinning medicines, there is a risk of bleeding.
- Calcium channel blockers to slow a rapid heart rate or the speed at which signals travel. Typically, they are used to control dysrhythmias of the upper chambers. In some cases, calcium channel blockers can trigger ventricular fibrillation. They can also cause digestive trouble, swollen feet, or low blood pressure.
- Digitalis, or digoxin, to treat a fast heart rate. This medicine can cause nausea and may trigger dysrhythmias.
- Potassium channel blockers to slow the heart rate. They work by lengthening the time it takes for heart cells to recover after firing, so that they do not fire and squeeze as often. Potassium channel blockers can cause low blood pressure or another dysrhythmia.
- Sodium channel blockers to block transmission of electrical signals, lengthen cell recovery periods, and make cells less excitable. However, these drugs can increase risks of sudden cardiac arrest in people who have heart disease.
Procedures
If medicines do not treat your dysrhythmia, your doctor may recommend one of these procedures or devices.
- Cardioversion
- Catheter ablation
- Implantable cardioverter defibrillators (ICDs)
- Pacemakers
Other treatments
Treatment may also include managing any underlying condition, such as an electrolyte imbalance, high blood pressure, heart disease, sleep apnea, or thyroid disease.
Your doctor may use supplements to treat magnesium or electrolyte deficiencies. Electrolytes can also be an alternative to medicines that treat dysrhythmia if your doctor is concerned that those medicines might trigger an dysrhythmia.
Your doctor may also perform certain techniques to slow your heart rate. The exercises stimulate your body’s natural relaxation processes. They do this by affecting the vagus nerve, which helps control the heart rate. Techniques can include:
- Having you cough or gag
- Having you hold your breath and bear down, which is called the Valsalva maneuver
- Having you lie down
- Putting a towel dipped in ice-cold water over your face
Follow up care
If you have been diagnosed and treated for dysrhythmia, make sure to follow your treatment plan. Your ongoing care may focus on reducing the chance that you will have another episode or a complication. Keep your regular appointments with your doctor. Ask about heart-healthy lifestyle changes that you can make to keep your dysrhythmia from happening again or getting worse.
How often you need to see your doctor for follow-up care will depend on your symptoms and treatment.
- Get regular vaccinations, including a flu shot every year.
- Follow your doctor’s recommendations for adopting lifelong lifestyle changes, such as heart-healthy eating, being physically active, quitting smoking, managing stress, and aiming for a healthy weight. Your doctor may also recommend that you reduce or stop drinking alcohol and consuming coffee, tea, soda, chocolate, or other sources of caffeine, to avoid triggering dysrhythmia.
- Keep all of your medical appointments. Bring a list of all the medicines you take to every doctor and emergency room visit. This will help your doctors know exactly what medicines you are taking, which can help prevent medicine errors.
- See your doctor for regular checkups if you are taking blood-thinning medicines. Your doctor may recommend blood thinners to prevent stroke, even if your heart rhythm has returned to normal. You may need routine blood tests to check how the medicines are working or the effect they are having on your organs.
- Take your medicines as prescribed. Your doctor may also ask you to check your pulse regularly to monitor the effectiveness of the medicines.
- Tell your doctor if you have side effects from your medicines, such as depression, light-headedness, or palpitations. Some of the medicines can cause low blood pressure or a slow heart rate or can make heart failure worse.
- Tell your doctor if your symptoms are getting worse or if you have new symptoms. Over time, dysrhythmias can become more common, last longer, or get worse. This can sometimes make dysrhythmia resistant to medicines. Some dysrhythmias can also make it more likely for other types of dysrhythmia to develop.
Monitor your condition
To monitor your condition, your doctor may recommend the following tests.
- Blood tests to check the effects of medicines you are taking
- Echocardiography (echo) to check your heart function if you have underlying heart disease
- EKGs to monitor changes in heart rhythm
- Holter or event monitors to record your heart’s electrical activity over several days
- Smartphone-based monitors to record heart rhythms and detect when atrial fibrillation occurs. A band that can record a 30-second EKG has been approved by the U.S. Food and Drug Administration.
Learn the warning signs of serious complications and have a plan
Dysrhythmia can lead to serious complications, such as sudden cardiac arrest and severe bleeding in the brain. If you suspect any of the following in yourself or someone else, call your local emergency services number immediately:
- Bleeding in the brain or digestive system. If you take too high a dose of blood-thinning medicines, it may cause bleeding in the brain or digestive system. Signs and symptoms may include bright red vomit; bright red blood in your stool or black, tarry stools; severe pain in the abdomen or head; sudden, severe changes in your vision or ability to move your arms or legs; or memory loss. A lot of bleeding after a fall or injury or easy bruising or bleeding may mean that your blood is too thin. Excessive bleeding is bleeding that will not stop after you apply pressure to a wound for 10 minutes. Call your doctor right away if you have any of these signs.
- Heart attack. Signs of heart attack include mild or severe chest pain or discomfort in the center of the chest or upper abdomen that lasts for more than a few minutes or goes away and comes back. It can feel like pressure, squeezing, fullness, heartburn, or indigestion. There may also be pain down the left arm. Women may also have chest pain and pain down the left arm, but they are more likely to have other symptoms, such as shortness of breath, nausea, vomiting, unusual tiredness, and pain in the back, shoulders, or jaw. Read more about the signs and symptoms of a heart attack.
- Stroke. If you think someone may be having a stroke, act F.A.S.T. and do the following simple test.
- F—Face: Ask the person to smile. Does one side of the face droop?
- A—Arms: Ask the person to raise both arms. Does one arm drift downward?
- S—Speech: Ask the person to repeat a simple phrase. Is their speech slurred or strange?
- T—Time: If you observe any of these signs, call your local emergency services number immediately. Every minute matters.
- Sudden cardiac arrest. Usually, the first sign of sudden cardiac arrest is fainting. At the same time, no heartbeat can be felt. Some people may have a racing heartbeat or feel dizzy or light-headed just before they faint. Within an hour before cardiac arrest, some people have chest pain, shortness of breath, nausea, or vomiting. Call your local emergency services number right away if someone has signs or symptoms of sudden cardiac arrest. Look for a defibrillator nearby and follow the instructions.
Learn about other precautions to help you stay safe
If you have dysrhythmia, you will need to learn ways to care for your condition at home. You will also need to avoid activities that may trigger your dysrhythmia.
- Ask your doctor whether you can continue your daily activities without any changes. Your doctor may recommend low or moderate activity; avoiding competitive sports; eliminating activities that might trigger an dysrhythmia, such as swimming or diving; or participating in activities with a partner.
- Carry a medical device ID card with information about your defibrillator or pacemaker and contact information for the health care provider who oversees your care. Medical bracelets with information about your condition can also be helpful in the event of an emergency.
- Check with your doctor before taking over-the-counter medicines, nutritional supplements, or cold and allergy medicines. Some of these products can trigger rapid heart rhythms or interact poorly with heart rhythm medicines.
- Learn how to take your pulse. Discuss with your doctor what pulse rate is normal for you. Keep a record of changes in your pulse rate, and share this information with your doctor.
- Lie down if you feel dizzy or faint or if you feel palpitations. Do not try to walk or drive. Let your doctor know about these symptoms.
- Talk to your doctor about techniques that you can do at home if you notice your heart racing. These include breathing out without letting your breath escape or putting a cold, wet towel over your face.





{kind=link}