
Contents
What is ectopic pregnancy
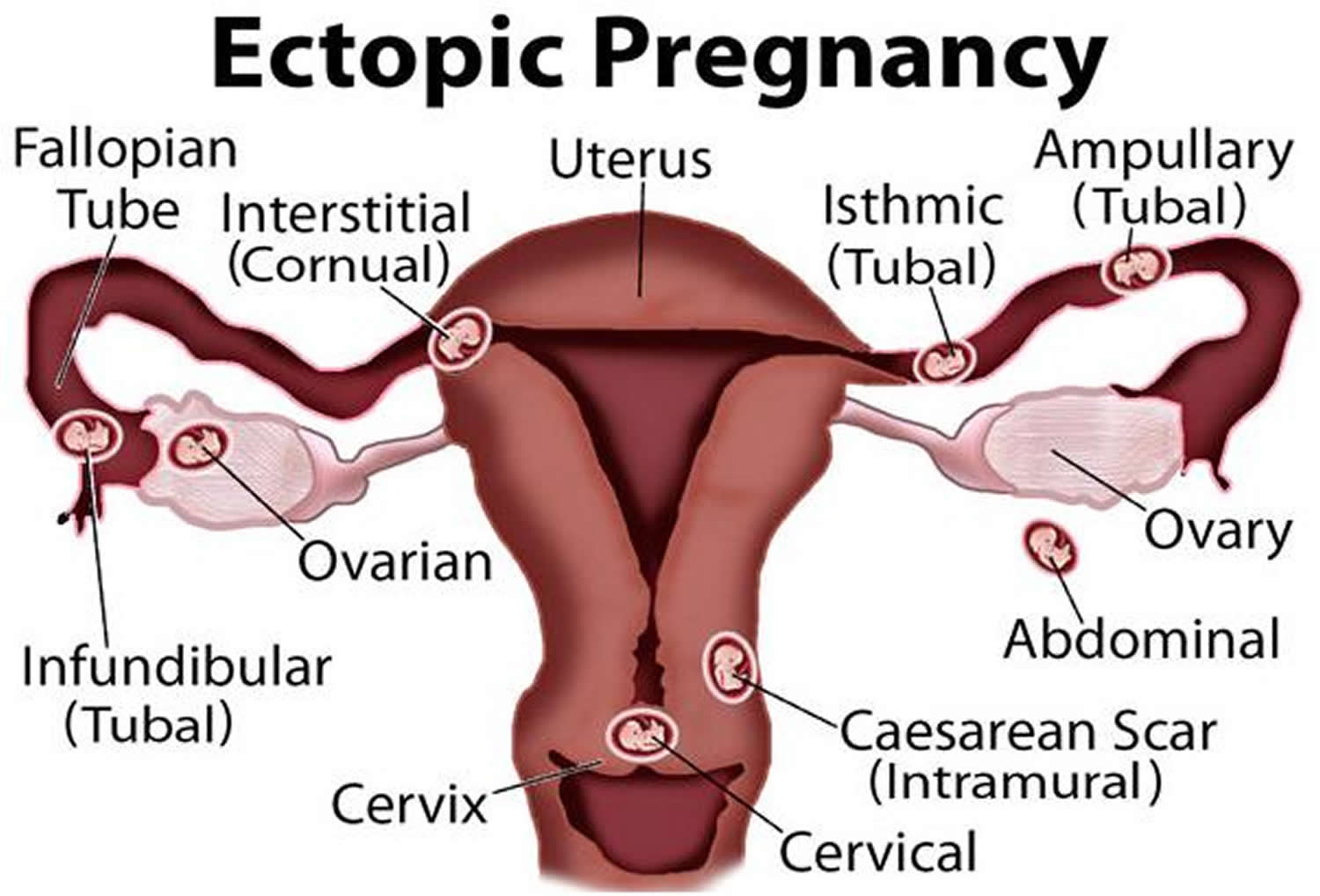
An ectopic pregnancy is when a fertilized egg (an embryo) implants itself outside of the womb (uterus), usually in one of the Fallopian tubes (uterine tubes) or less commonly it attaches to an ovary, the cervix or your abdomen (belly). These areas don’t have enough space or the right tissue for a baby to grow. Left untreated, ectopic pregnancy is a life threatening condition. It is the leading cause of death in the first trimester of pregnancy and the fourth leading cause of all maternal deaths in the United Kingdom. Ectopic pregnancy is also a leading cause of early pregnancy death in United States.
Ectopic pregnancy locations
In the vast majority of cases, the ectopic implantation site is within a Fallopian tube (uterine tubes).
- Fallopian tubal ectopic pregnancy: 93-97%
- Ampullary ectopic pregnancy: most common ~70% of tubal ectopics and ~65% of all ectopics
- Isthmal ectopic: ~12% of tubal ectopics and ~11% of all ectopics
- Fimbrial ectopic: ~11% of tubal ectopics and ~10% of all ectopics
- Interstitial ectopic/cornual ectopic pregnancy: 3-4%; also essentially a type of tubal ectopic
- Ovarian ectopic pregnancy: ovarian pregnancy; 0.5-1%
- Cervical ectopic pregnancy: cervical pregnancy; rare <1%
- Scar ectopic pregnancy: site of previous Caesarian section scar; rare
- Abdominal ectopic pregnancy: rare ~1.4%
The fallopian tubes are the tubes connecting the ovaries to the womb. If an egg gets stuck in them, it won’t develop into a baby and your health may be at risk if the pregnancy continues. Without treatment, an ectopic pregnancy can cause the place where it’s attached to bleed heavily or burst. This can lead to serious bleeding and even death in the pregnant woman.
- Unfortunately, it’s not possible to save the pregnancy. An ectopic pregnancy always ends in pregnancy loss. Ectopic pregnancy usually has to be removed using medicine or an operation before it grows too large.
The main treatment options are:
- expectant management – your condition is carefully monitored to see whether treatment is necessary
- medication – a medicine called methotrexate is used to stop the pregnancy growing
- surgery – surgery is used to remove the pregnancy, usually along with the affected fallopian tube
These options each have advantages and disadvantages that your doctor will discuss with you.
In the US, the overall incidence has increased over the last few decades and is currently thought to affect 1-2% (around 1 in every 50) of pregnancies. The risk is as high as 18% for first trimester pregnancies with bleeding 1.
Increasing incidence of ectopic pregnancy is in part due to improvements in the way ectopic pregnancy is diagnosed (e.g. ultrasound, which is the usual way to diagnose ectopic pregnancy today, was much less accessible several decades ago). Other factors thought to play a role in the changing incidence of ectopic pregnancy include changes in smoking patterns in women and increased incidence of pelvic inflammatory disease (PID) and chlamydia trachomatis, a sexually transmitted infection (STI). There is also an increased incidence associated with in-vitro fertilisation (IVF) pregnancies.
An ectopic pregnancy may start out with usual signs and symptoms of pregnancy, like missing your period or having nausea (feeling sick to your stomach or morning sickness) and tender breasts. Or you may not have any signs or symptoms and not even know you’re pregnant.
- Light vaginal bleeding with abdominal or pelvic pain is often the first warning sign of an ectopic pregnancy.
- The most common symptoms of ectopic pregnancy are lower abdominal pain (reported by over 90% of women with ectopic pregnancy) and abnormal menstrual bleeding (reported by over 80% of women). If left untreated, the consequences of ectopic pregnancy include damage to the reproductive organs, reduced fertility and in the most severe cases, death.
Early treatment of an ectopic pregnancy can help preserve the chance for future healthy pregnancies.
Who is at risk for having an ectopic pregnancy?
Any woman can have an ectopic pregnancy. But the risk is higher if you:
- Are older than 35. The risk of ectopic pregnancy increases with age. Women who are more than 40 years of age are 2.9 times more likely to develop an ectopic pregnancy if they become pregnant, than women who are 25-29 years.
- Smoking. A French study reported that cigarette smoking accounted for 35% of the risk associated with ectopic pregnancy. The more a woman smokes, the more likely she is to develop an ectopic pregnancy. Women who smoke more than 20 cigarettes per day are almost four times more likely to experience an ectopic pregnancy than those who have never smoked. Women who smoke less than 10 cigarettes per day are less than 2 times more likely to develop ectopic pregnancy than those who never smoked;
- Have more than one sex partner. This can put you at risk for getting a sexually transmitted infection (also called STI). An STI is an infection you can get from having sex with someone who is infected. Sexually transmitted infections can lead to pelvic inflammatory disease (also called PID), an infection that can damage the fallopian tubes, uterus and other organs.
- History of pelvic inflammatory disease. Pelvic inflammatory disease (PID) often leads to scarring and deformation of the pelvic cavity, which is thought to increase risk for ectopic pregnancy. A French study reported the risk of ectopic in women with a history of pelvic inflammatory disease to be 3.4 times higher than in women who had never experienced pelvic inflammatory disease.
- History of sexually transmitted infection (particularly chlamydia and gonorrhoea): Women with a history of sexually transmitted infection are more likely to develop an ectopic pregnancy and a history of multiple sexually transmitted infections may increase the risk even further. Sexually transmitted infections are associated with pelvic infection, post inflammatory scarring and distortion of normal reproductive anatomy which appear to cause the increased risk of ectopic pregnancy.
Medical conditions that increase your risk for having an ectopic pregnancy include:
- You’ve had a previous ectopic pregnancy.
- You’ve had surgery on a fallopian tube, or you have problems, like a birth defect in a fallopian tube. A birth defect is a health condition that is present at birth. It can change the shape or function of one or more parts of the body. It can cause problems in overall health, in how the body develops, or in how the body works.
- History of tubal surgery: Women who have undergone surgery involving the fallopian tubes are 4 times more likely to have an ectopic pregnancy than those who have not had tubal surgery;
- Sterilization: Pregnancy in general is uncommon following sterilization, however when it does occur, pregnancy is usually ectopic. Women sterilized using the bipolar coagulation technique had the highest rate of ectopic pregnancy following sterilization (17.3 events per 1000 sterilisations), while women sterilized by postpartum partial salpingectomy, had the lowest rate of ectopic pregnancy (1.5 per 1000). Women under 30 years of age at the time of sterilization had a higher risk of ectopic pregnancy than those who were aged 30 or more when sterilized.
- You have scars inside the pelvic area from a (ruptured) burst appendix or from past surgeries. Your appendix is part of your digestive tract that helps you process the food you eat.
- You’ve had endometriosis. This is when tissue from the uterus grows somewhere outside the uterus.
- You’ve had a history of infertility: Women who have been infertile in the past are more likely to develop an ectopic pregnancy than those who have not been infertile. The risk of developing an ectopic pregnancy increases with the number of years of infertility. Women who have been infertile for two or more years are 2.7 times more likely, women who have been infertile for 1-2 years are 2.6 times more likely, and those who have been infertile for less than one year 2.1 times more likely to develop an ectopic pregnancy than women who have never been infertile.
- You’ve had fertility treatment to help you get pregnant. Ectopic pregnancies account for some 4% of all pregnancies in women who have used assisted reproductive techniques, compared to estimated 2% of pregnancies in total.
- You got pregnant while using an intreauterine device (also called IUD) or after tubal ligation (also called having your tubes tied). An IUD is a form of birth control that your provider places inside your uterus. Tubal ligation is surgery to close the fallopian tubes to prevent you from getting pregnant. Women who have previously used an intrauterine device are 1.3 times more likely to develop an ectopic pregnancy than those who have not. When a woman who is using an intrauterine device becomes pregnant (a rare event), there is a high chance the pregnancy is ectopic.
- Previous miscarriage: The risk of ectopic pregnancy increases with the number of miscarriages a woman has previously experienced. Women who have experienced 1-2 miscarriages in the past are 1.2 times more likely to develop an ectopic pregnancy than women who have never miscarried. Three or more miscarriages in the past increases the risk of developing an ectopic pregnancy to three times that of women who have never had a miscarriage.
- Previous medically induced abortion: Women who have medically terminated a pregnancy are 2.8 times more likely to experience ectopic pregnancy than those who had never induced abortion. There is no increased risk associated with a history of induced surgical abortion.
If you’ve had an ectopic pregnancy before, can you go on to have a healthy pregnancy?
Yes. About 1 in 3 women (33 percent) who have had one ectopic pregnancy go on to have a healthy pregnancy later. Women who have had one ectopic pregnancy in the past are about seven times more likely to develop an ectopic pregnancy in the future than women who have never had an ectopic pregnancy. Women who have had two or more ectopic pregnancies in the past are over 70 times more likely to develop an ectopic pregnancy in the future.
Seek emergency medical help if you experience any signs or symptoms of an ectopic pregnancy, including:
- Severe abdominal or pelvic pain accompanied by vaginal bleeding
- Bleeding from the vagina
- Feeling faint, lightheadedness or dizzy. This can be caused by blood loss which can cause low blood pressure. Blood pressure is the force of blood that pushes against the walls of your arteries. Arteries are blood vessels that carry blood away from your heart to other parts of the body.
- Pain in your lower back or even your shoulder
- Pain in your pelvic area (the part of your body between the stomach and legs). The pain may be mainly on one side. It can come and go, start out mild and then become sharp and stabbing.
Uterus anatomy
The uterus is supported by the muscular floor of the pelvis and folds of peritoneum that form supportive ligaments around the organ, as they do for the ovary and uterine tube. The broad ligament has two parts: the mesosalpinx mentioned earlier and the mesometrium on each side of the uterus. The cervix and superior part of the vagina are supported by cardinal (lateral cervical) ligaments extending to the pelvic wall. A pair of uterosacral ligaments attaches the posterior side of the uterus to the sacrum, and a pair of round ligaments arises from the anterior surface of the uterus, passes through the inguinal canals, and terminates in the labia majora.
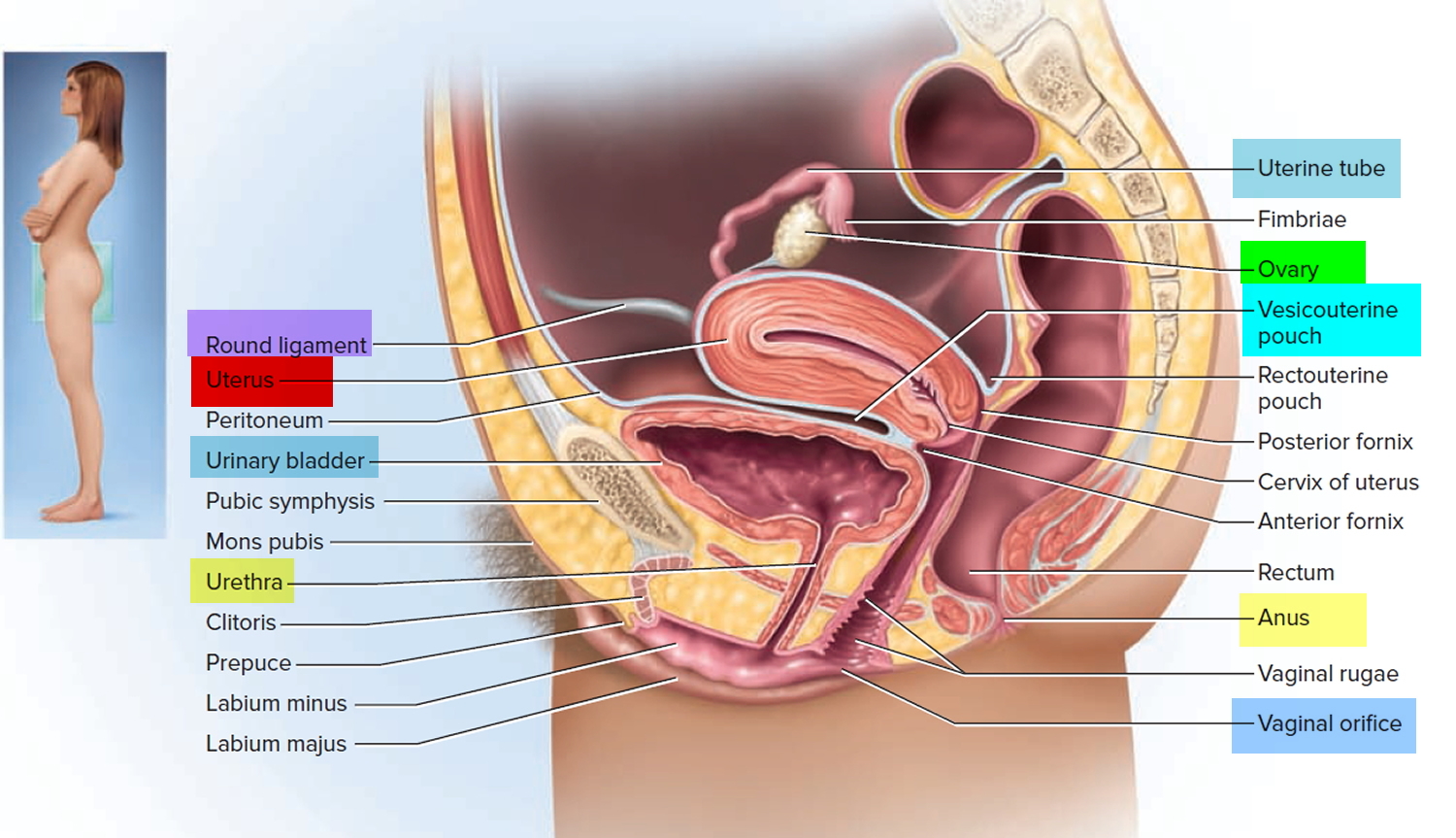
As the peritoneum folds around the various pelvic organs, it creates several dead-end recesses and pouches (extensions of the peritoneal cavity). Two major ones are the vesicouterine pouch, which forms the space between the uterus and urinary bladder, and rectouterine pouch between the uterus and rectum (see Figure 3).
The uterine blood supply to the uterus is particularly important to the menstrual cycle and pregnancy. A uterine artery arises from each internal iliac artery and travels through the broad ligament to the uterus (Figure 2). It gives off several branches that penetrate into the myometrium and lead to arcuate arteries. Each arcuate artery travels in a circle around the uterus and anastomoses with the arcuate artery on the other side. Along its course, it gives rise to smaller arteries that penetrate the rest of the way through the myometrium, into the endometrium, and give off spiral arteries. The spiral arteries wind tortuously between the endometrial glands toward the surface of the mucosa. They rhythmically constrict and dilate, making the mucosa alternately blanch and flush with blood.
Figure 1. Uterus anatomy
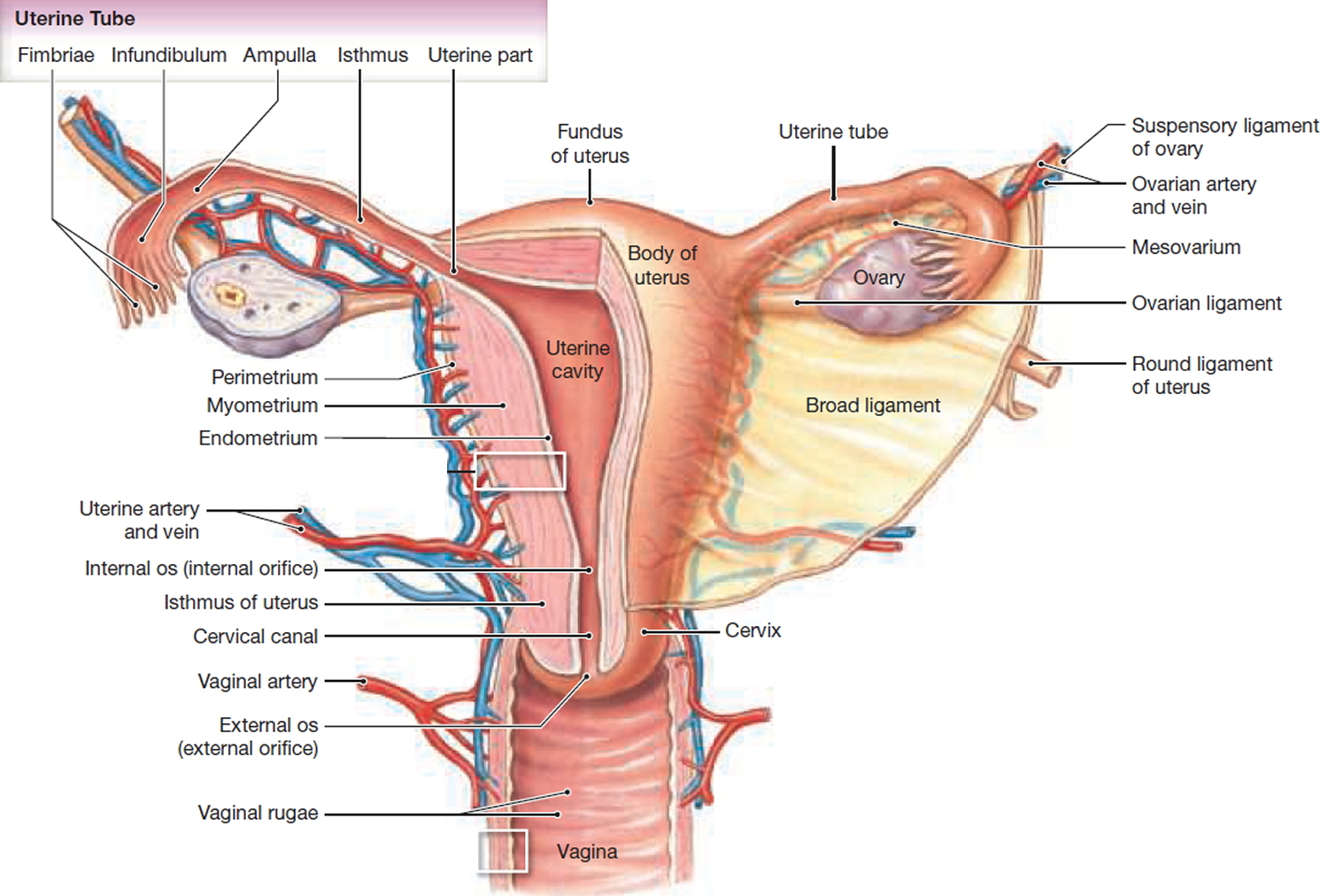
Figure 2. Blood supply to the uterus
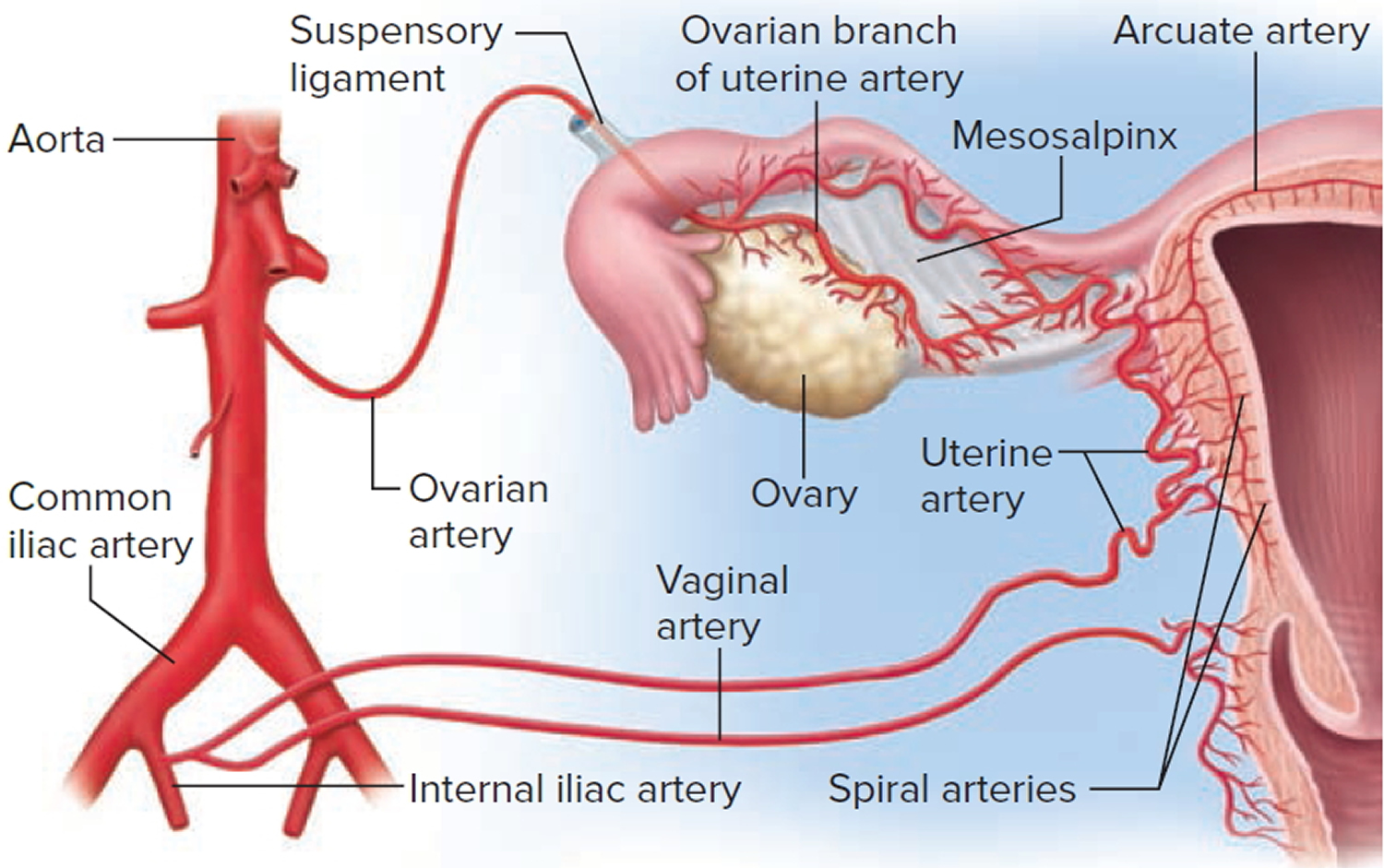
Figure 3. Uterus location
Ectopic pregnancy prognosis
Ectopic pregnancy is potentially life threatening if left untreated, however a proportion of cases will resolve naturally and can be managed using expectant techniques (i.e. a “wait and see” approach, in which the woman is monitored for signs that the pregnancy has resolved). However in most cases ectopic pregnancies require either medical or surgical intervention. Both techniques are effective in removing the abnormal embryo and the majority of women are able to fall pregnant again after either medical or surgical treatments.
Ectopic pregnancy complications
When you have an ectopic pregnancy, the stakes are high. Without treatment, the embryo can grow too large to be accommodated by the surrounding organs. In this case the embryo can cause a rupture and considerably damage the reproductive organs. In very serious cases, ectopic pregnancy also poses a threat to the pregnant woman’s life because a ruptured fallopian tube could lead to life-threatening bleeding.
Ectopic pregnancy causes
What causes ectopic pregnancy
A tubal ectopic pregnancy — the most common type of ectopic pregnancy — happens when a fertilized egg gets stuck on its way to the uterus, often because the fallopian tube is damaged by inflammation or is misshapen. Hormonal imbalances or abnormal development of the fertilized egg also might play a role.
Risk factors for ectopic pregnancy
Various factors are associated with ectopic pregnancy, including:
- Are older than 35. The risk of ectopic pregnancy increases with age. Women who are more than 40 years of age are 2.9 times more likely to develop an ectopic pregnancy if they become pregnant, than women who are 25-29 years.
- In vitro fertilisation (IVF)
- Fertility issues. Some research suggests an association between difficulties with fertility — as well as use of fertility drugs — and ectopic pregnancy.
- Prior ectopic pregnancy. If you’ve had one ectopic pregnancy, you’re more likely to have another.
- Tubal injury or surgery / tubal ligation
- Pelvic inflammatory disease (sexually transmitted infections). Often, these infections are caused by gonorrhea or chlamydia. Pelvic inflammatory disease (PID) often leads to scarring and deformation of the pelvic cavity, which is thought to increase risk for ectopic pregnancy. A French study reported the risk of ectopic in women with a history of pelvic inflammatory disease to be 3.4 times higher than in women who had never experienced pelvic inflammatory disease.
- Salpingitis isthmica nodosa. Inflammation of the fallopian tube (salpingitis) or an infection of the uterus, fallopian tubes or ovaries (pelvic inflammatory disease) increases the risk of ectopic pregnancy.
- Endometrial injury or congenital anomalies. An ectopic pregnancy is more likely if you have an unusually shaped fallopian tube or the fallopian tube was damaged, possibly during surgery. Even surgery to reconstruct the fallopian tube can increase the risk of ectopic pregnancy.
- Use of intrauterine contraceptive devices. Pregnancy when using an intrauterine device (IUD) is rare. If pregnancy occurs, however, it’s more likely to be ectopic. The same goes for pregnancy after tubal ligation — a permanent method of birth control commonly known as “having your tubes tied.” Although pregnancy after tubal ligation is rare, if it happens, it’s more likely to be ectopic. Women who have previously used an intrauterine device are 1.3 times more likely to develop an ectopic pregnancy than those who have not. When a woman who is using an intrauterine device becomes pregnant (a rare event), there is a high chance the pregnancy is ectopic.
- Smoking. Cigarette smoking just before you get pregnant can increase the risk of an ectopic pregnancy. And the more you smoke, the greater the risk.
- Previous miscarriage: The risk of ectopic pregnancy increases with the number of miscarriages a woman has previously experienced. Women who have experienced 1-2 miscarriages in the past are 1.2 times more likely to develop an ectopic pregnancy than women who have never miscarried. Three or more miscarriages in the past increases the risk of developing an ectopic pregnancy to three times that of women who have never had a miscarriage.
- Previous medically induced abortion: Women who have medically terminated a pregnancy are 2.8 times more likely to experience ectopic pregnancy than those who had never induced abortion. There is no increased risk associated with a history of induced surgical abortion.
- History of tubal surgery: Women who have undergone surgery involving the fallopian tubes are 4 times more likely to have an ectopic pregnancy than those who have not had tubal surgery;
- Sterilization: Pregnancy in general is uncommon following sterilization, however when it does occur, pregnancy is usually ectopic. Women sterilized using the bipolar coagulation technique had the highest rate of ectopic pregnancy following sterilization (17.3 events per 1000 sterilisations), while women sterilized by postpartum partial salpingectomy, had the lowest rate of ectopic pregnancy (1.5 per 1000). Women under 30 years of age at the time of sterilization had a higher risk of ectopic pregnancy than those who were aged 30 or more when sterilized.
- History of sexually transmitted infection (particularly chlamydia and gonorrhoea): Women with a history of sexually transmitted infection are more likely to develop an ectopic pregnancy and a history of multiple sexually transmitted infections may increase the risk even further. Sexually transmitted infections are associated with pelvic infection, post inflammatory scarring and distortion of normal reproductive anatomy which appear to cause the increased risk of ectopic pregnancy.
- Many lifetime sexual partners.
- History of infertility: Women who have been infertile in the past are more likely to develop an ectopic pregnancy than those who have not been infertile. The risk of developing an ectopic pregnancy increases with the number of years of infertility. Women who have been infertile for two or more years are 2.7 times more likely, women who have been infertile for 1-2 years are 2.6 times more likely, and those who have been infertile for less than one year 2.1 times more likely to develop an ectopic pregnancy than women who have never been infertile.
- You’ve had fertility treatment to help you get pregnant. Ectopic pregnancies account for some 4% of all pregnancies in women who have used assisted reproductive techniques, compared to estimated 2% of pregnancies in total.
Ectopic pregnancy prevention
You can’t prevent an ectopic pregnancy, but you can decrease certain risk factors. For example, limit your number of sexual partners and use a condom when you have sex to help prevent sexually transmitted infections and reduce the risk of pelvic inflammatory disease. Quitting smoking before you attempt to get pregnant may also reduce your risk.
Ectopic pregnancy signs and symptoms
At first, an ectopic pregnancy might not cause any signs or symptoms and may only be detected during a routine pregnancy scan. Symptoms of an ectopic pregnancy usually develop between the 4th and 12th weeks of pregnancy.
In other cases, early signs and symptoms of an ectopic pregnancy might be the same as those of any pregnancy — a missed period, breast tenderness and nausea.
- You may have an ectopic pregnancy if you miss a period, have a positive pregnancy test, and have other signs of pregnancy, in addition to any of the symptoms listed below.
If you take a pregnancy test, the result will be positive. Still, an ectopic pregnancy can’t continue as normal.
Early signs of ectopic pregnancy
Light vaginal bleeding with abdominal or pelvic pain is often the first warning sign of an ectopic pregnancy. If blood leaks from the fallopian tube, it’s also possible to feel shoulder pain or an urge to have a bowel movement — depending on where the blood pools or which nerves are irritated. If the fallopian tube ruptures, heavy bleeding inside the abdomen is likely — followed by lightheadedness, fainting and shock.
Signs of ectopic pregnancy
If you do have symptoms, they tend to develop between the 4th and 12th week of pregnancy.
Symptoms can include a combination of:
- a missed period and other signs of pregnancy
- tummy pain low down on one side
- vaginal bleeding or a brown watery discharge
- pain in the tip of your shoulder
- discomfort when peeing or pooing
But these symptoms aren’t necessarily a sign of a serious problem. They can sometimes be caused by other problems, such as a stomach bug.
Vaginal bleeding
Vaginal bleeding tends to be a bit different to your regular period. It often starts and stops, and may be watery and dark brown in color.
Some women mistake this bleeding for a regular period and don’t realize they’re pregnant.
Vaginal bleeding during pregnancy is relatively common and isn’t necessarily a sign of a serious problem, but you should seek medical advice if you experience it.
Tummy pain
You may experience tummy pain, typically low down on one side. It can develop suddenly or gradually, and may be persistent or come and go.
Tummy pain can have lots of causes, including stomach bugs and trapped wind, so it doesn’t necessarily mean you have an ectopic pregnancy.
But you should get medical advice if you have it and think you might be pregnant.
Shoulder tip pain
Shoulder tip pain is an unusual pain felt where your shoulder ends and your arm begins.
It’s not known exactly why it occurs, but it can be a sign of an ectopic pregnancy causing some internal bleeding, so you should get medical advice right away if you experience it.
Discomfort when going to the toilet
You may experience pain when going for a pee or poo. You may also have diarrhea.
Some changes to your normal bladder and bowel patterns are normal during pregnancy, and these symptoms can be caused by urinary tract infections and stomach bugs.
But it’s still a good idea to seek medical advice if you experience these symptoms and think you might be pregnant.
Ruptured ectopic pregnancy
In a few cases, an ectopic pregnancy can grow large enough to split open the fallopian tube. This is known as a ruptured ectopic pregnancy.
Ruptures are very serious, and surgery to repair the fallopian tube needs to be carried out as soon as possible.
Signs of a ruptured ectopic pregnancy include a combination of:
- a sharp, sudden and intense pain in your tummy
- feeling very dizzy or fainting
- feeling sick
- looking very pale
Call your local emergency number for an ambulance or go to your nearest hospital accident and emergency (A&E) department immediately if you experience these symptoms.
Ectopic pregnancy diagnosis
It can be difficult to diagnose an ectopic pregnancy from the symptoms alone, as they can be similar to other conditions.
If your doctor suspects an ectopic pregnancy, he or she might do a pelvic exam to check for pain, tenderness, or a mass in the fallopian tube or ovary. A physical exam alone usually isn’t enough to diagnose an ectopic pregnancy, however. The diagnosis is typically confirmed with blood tests and imaging studies, such as an ultrasound.
Ectopic pregnancy test
Your provider may do these tests to look for an ectopic pregnancy:
- A pelvic exam
- Blood tests to measure the levels of a pregnancy hormone called human chorionic gonadotropin (hCG). In an ectopic pregnancy the level of hCG tends to be lower and can cause hCG levels to rise more slowly than a healthy pregnancy. The results of the test can also be useful in determining the best treatment for an ectopic pregnancy.
- Ultrasound. This test uses sound waves and a computer screen to show a picture of your baby inside the womb. During an ultrasound, your health care provider uses a wand-like tool called a transducer on your belly (also called a transabdominal ultrasound) or inside the vagina (also called a transvaginal ultrasound). Providers often use transvaginal ultrasound to find an ectopic pregnancy because it can show a pregnancy earlier than a transabdominal ultrasound.
Sometimes it’s too soon to detect a pregnancy through ultrasound. If the diagnosis is in question, your doctor might monitor your condition with blood tests until the ectopic pregnancy can be confirmed or ruled out through ultrasound — usually by four to five weeks after conception. It’s hard to see a pregnancy less than 5 weeks after your last period. In an emergency situation — if you’re bleeding heavily, your provider may need to do surgery to diagnose and treat an ectopic pregnancy.
Ectopic pregnancy ultrasound
It is useful to know a quantitative beta HCG prior to scanning as this will guide what the sonographer expect to see. At levels <2000 IU, a normal early pregnancy may not be visible.
The most reliable sign of ectopic pregnancy is visualisation of an extra-uterine gestation, but this is not seen in 15-35% of ectopic pregnancies 2.
The ultrasound exam should be performed both transabdominally and transvaginally. The transabdominal component provides a wider overview of the abdomen, whereas a transvaginal scan is important for diagnostic sensitivity.
Positive sonographic findings include:
uterus
- empty uterine cavity or no evidence of intrauterine pregnancy
- pseudogestational sac or decidual cyst: may be seen in 10-20% of ectopic pregnancies
- current evidence suggests that one should not initiate treatment for an ectopic pregnancy in a hemodynamically stable woman on the basis of a single hCG value 3
- decidual cast
- thick echogenic endometrium
tube and ovary
- simple adnexal cyst: 10% chance of an ectopic pregnancy
- complex extra-adnexal cyst/mass: 95% chance of a tubal ectopic pregnancy (if no intra-uterine pregnancy)
- an intra-adnexal cyst/mass is more likely to be a corpus luteum
- solid hyperechoic mass is possible, but non-specific
- tubal ring sign
- 95% chance of a tubal ectopic pregnancy if seen
- described in 49% of ectopics and in 68% of unruptured ectopics
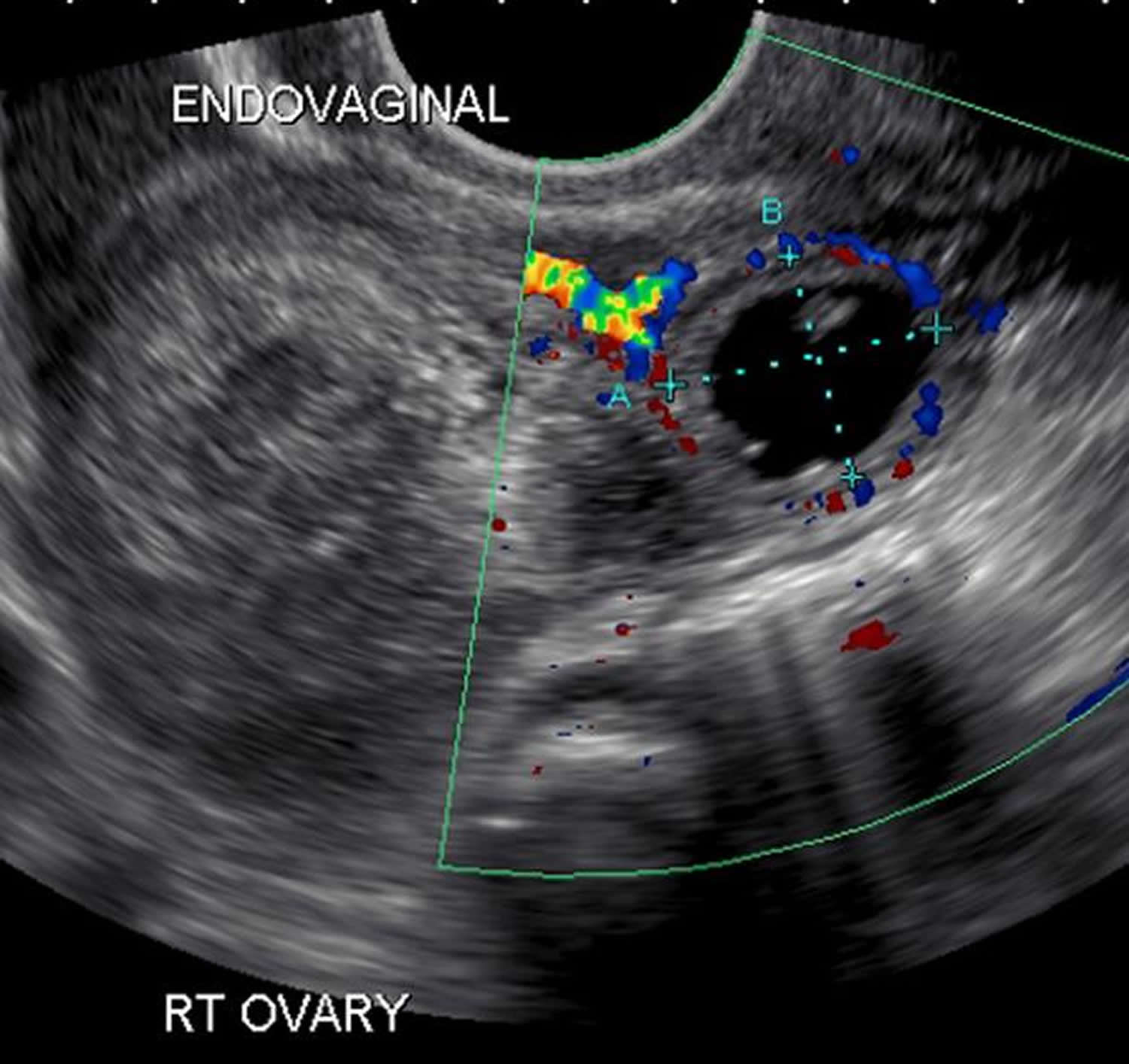
- ring of fire sign: can be seen on colour Doppler in a tubal ectopic pregnancy, but can also be seen in a corpus luteum
- absence of color Doppler flow does not exclude an ectopic pregnancy
- live extrauterine pregnancy (i.e. extra-uterine fetal cardiac activity): 100% specific, but only seen in a minority of cases
peritoneal cavity
- free pelvic fluid or hemoperitoneum in the pouch of Douglas
- the presence of free intraperitoneal fluid in the context of a positive beta HCG and empty uterus is
- ~70% specific for an ectopic pregnancy 4
- ~63% sensitive for ectopic pregnancy 4
- not specific for ruptured ectopic (seen in 37% of intact tubal ectopics)
- the presence of free intraperitoneal fluid in the context of a positive beta HCG and empty uterus is
- live pregnancy: 100% specific, but only seen in a minority of cases
In patients receiving in vitro fertilisation (IVF), it is important not to be completely reassured by the presence of a live intrauterine pregnancy 8, as there is a possibility of a coexisting ectopic pregnancy in ~1:500 (i.e. heterotopic pregnancy). In patients not receiving IVF, the risk of heterotopic pregnancy is minuscule (1:30,000).
Figure 4. Ectopic pregnancy ultrasound
Ectopic pregnancy treatment
A fertilized egg can’t develop normally outside the uterus. To prevent life-threatening complications, the ectopic tissue needs to be removed.
Expectant management
If you have no symptoms or mild symptoms and the pregnancy is very small or can’t be found, you may only need to be closely monitored, as there’s a good chance the pregnancy will dissolve by itself.
This is known as expectant management.
The following is likely to happen:
- You’ll have regular blood tests to check that the level of hCG in your blood is going down – these will be needed until the hormone is no longer found.
- You may need further treatment if your hormone level doesn’t go down or it increases.
- You’ll usually have some vaginal bleeding – use sanitary pads or towels, rather than tampons, until this clears up.
- You may experience some tummy pain – take paracetamol to relieve this.
- You’ll be told what to do if you develop more severe symptoms.
The main advantage of monitoring is that you won’t experience any side effects of treatment.
A disadvantage is that there’s still a small risk of your fallopian tubes splitting open (rupturing) and you may eventually need treatment.
There are two treatments for ectopic pregnancy:
- Medicine. Your doctor gives you an injection of medicine called methotrexate to stop the embryo from growing. This treatment works best if the embryo is small and in the fallopian tube. Methotrexate (a folate antagonist) either administered systemically or by direct ultrasound guided injection or potassium chloride (direct injection only obviously).
- Relative contraindications to methotrexate include 4:
- rupture
- mass >3.5 cm
- fetal cardiac activity
- bHCG >6000-15,000 mIU/mL
- Relative contraindications to methotrexate include 4:
- Surgery. Your doctor removes the embryo with surgical instruments placed through very small cuts in the belly. This type of surgery is called laparoscopic surgery.
These options each have advantages and disadvantages that your doctor will discuss with you.
They’ll recommend what they think is the most suitable option for you, depending on factors such as your symptoms, the size of the pregnancy, and the level of pregnancy hormone (human chorionic gonadotropin, or hCG) in your blood.
If the ectopic pregnancy is detected early, an injection of the drug methotrexate is sometimes used to stop cell growth and dissolve existing cells. It’s imperative that the diagnosis of ectopic pregnancy is certain before this treatment is undertaken. After the injection, your healthcare provider regularly checks your hCG levels until they return to zero. This can take a few weeks. If your levels stay high, it may mean that you still have ectopic tissue in your body. If so, you may need more treatment with methotrexate or surgery to remove the tissue.
If using the drug methotrexate, you’ll need to use reliable contraception for at least 3 months after treatment.
This is because methotrexate can be harmful for a baby if you become pregnant during this time.
It’s also important to avoid alcohol until you’re told it’s safe, as drinking soon after receiving a dose of methotrexate can damage your liver.
Other side effects of methotrexate include:
- tummy pain – this is usually mild and should pass within a day or two
- dizziness
- feeling and being sick
- diarrhea
There’s also a chance of your fallopian tubes rupturing after treatment. You’ll be told what to look out for and what to do if you think this has happened.
Ectopic pregnancy surgery
In most cases, ectopic pregnancy is usually treated with laparoscopic (keyhole) surgery. In this procedure, you’re given general anesthetic, so you’re asleep while it’s carried out and a small incision is made in the abdomen, near or in the navel. Then your doctor uses a thin tube equipped with a camera lens and light (laparoscope) to view the area.
Other instruments can be inserted into the tube or through other small incisions to remove the ectopic tissue and repair the fallopian tube. If the fallopian tube is significantly damaged, it might need to be removed.
Removing the affected fallopian tube is the most effective treatment and isn’t thought to reduce your chances of becoming pregnant again.
Your doctor will discuss this with you beforehand, and you’ll be asked whether you consent to having the Fallopian tube removed.
Most women can leave hospital a few days after surgery, although it can take 4 to 6 weeks to fully recover.
If the ectopic pregnancy is causing heavy bleeding or your fallopian tube has already ruptured, you’ll need emergency surgery.
The surgeon will make a larger incision in your tummy (laparotomy) to stop the bleeding and repair your fallopian tube, if that’s possible.
After either type of surgery, a treatment called anti-D rhesus prophylaxis will be given if your blood type is RhD negative. This involves an injection of a medicine that helps to prevent rhesus disease in future pregnancies.
Your doctor will monitor your HCG levels after surgery to be sure all of the ectopic tissue was removed. If HCG levels don’t come down quickly, an injection of methotrexate may be needed.
Coping and support
Losing a pregnancy is devastating, even if you’ve only known about it for a short time. Recognize the loss, and give yourself time to grieve. Talk about your feelings and allow yourself to experience them fully.
Rely on your partner, loved ones and friends for support. You might also seek the help of a support group, grief counselor or other mental health provider.
Most women who have ectopic pregnancies go on to have other, healthy pregnancies. If one fallopian tube was injured or removed, an egg can be fertilized in the other tube before entering the uterus.
If both fallopian tubes were injured or removed, in vitro fertilization might be an option. With this procedure, mature eggs are fertilized in a lab and then implanted into the uterus.
If you choose to conceive again, seek your doctor’s advice. Early blood tests and ultrasound imaging can offer prompt detection of another ectopic pregnancy — or reassurance that the pregnancy is developing normally.
- Histed SN, Deshmukh M, Masamed R, Jude CM, Mohammad S, Patel MK. Ectopic Pregnancy: A Trainee’s Guide to Making the Right Call: Women’s Imaging. Radiographics : a review publication of the Radiological Society of North America, Inc. 36 (7): 2236-2237. doi:10.1148/rg.2016160080 https://pubs.rsna.org/doi/10.1148/rg.2016160080[↩]
- Levine D. Ectopic pregnancy. Radiology. 2007;245 (2): 385-97. doi:10.1148/radiol.2452061031 https://www.ncbi.nlm.nih.gov/pubmed/17940301[↩]
- Lipscomb GH, Stovall TG, and Ling FW. Nonsurgical Treatment of Ectopic Pregnancy. N Engl J Med 2000; 343:1325-1329[↩]
- Bachman EA, Barnhart K. Medical management of ectopic pregnancy: a comparison of regimens. Clin Obstet Gynecol. 2012;55 (2): 440-7. doi:10.1097/GRF.0b013e3182510a73 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3329644/[↩]





{kind=link}