Contents
- What is eczema
- Types of eczema
- What triggers eczema?
- Eczema symptoms
- Eczema causes
- Eczema treatment
- Common eczema treatment
- Moisturizing
- Eczema cream
- Prescription topicals
- Phototherapy
- Immunosuppressants
- Biologics
- Home remedies for eczema
- Complementary and Alternative Treatments
- Baby eczema
- Eczema Herpeticum
- Dyshidrotic eczema
- Outlook (prognosis) for dyshidrotic eczema (pompholyx)?
- Complications of dyshidrotic eczema (pompholyx)?
- What causes dyshidrotic eczema?
- What are the clinical features of dyshidrotic eczema?
- Dyshidrotic eczema (pompholyx) diagnosis
- Aggravating factors of dyshidrotic eczema (pompholyx)
- Dyshidrotic eczema (pompholyx) treatment
- Nummular eczema
- Eczema on hands
- Who gets hand eczema?
- Hand eczema causes
- What does hand eczema look like?
- Types hand eczema
- Hand eczema diagnosis
- Hand eczema treatment
- Home remedies to help control hand eczema
- Some basic things you can do at work to help control your hand eczema
- What type of moisturizer is good for hand eczema?
- What are emollients and moisturizers?
- Why use emollients and moisturizers?
- What do emollients and moisturizers contain?
- Adverse reactions to emollients
- Eczema on scalp
- Allergic eczema
- Who gets allergic contact dermatitis?
- What causes allergic contact dermatitis?
- What are the clinical features of allergic contact dermatitis?
- What are the complications of allergic contact dermatitis?
- How is allergic contact dermatitis diagnosed?
- What is the treatment for allergic contact dermatitis?
- What is the outcome for allergic contact dermatitis?
What is eczema
Eczema is also called dermatitis, which simply means inflammation of the skin. Eczema is a common skin condition that affects both children and adults causing red, itchy and dry/blister/weep/peeling skin, which can be very irritating 1. Eczema is also known as atopic eczema, atopic dermatitis and allergic eczema. Eczema can range from mild, moderate, to severe.
There are eight types of eczema in all. Atopic dermatitis is a severe and chronic (long-lasting) form of eczema. It is caused by a combination of genes and an environmental trigger such as an irritant or allergen.
The term “eczema” is often used interchangeably with “atopic dermatitis.” However, each type of eczema, including atopic dermatitis, has somewhat different triggers, symptoms and treatments. That’s why it’s important to know which type or types (since a person can have more than one type at the same time) you have, so that you are best able to manage it.
Eczema is very common. And in many cases, it’s also manageable. In fact, over 30 million Americans have some form of eczema.
It’s most common for babies and children to develop eczema on their face (especially the cheeks and chin), but it can appear anywhere on the body and symptoms may be different from one child to the next. More often than not, eczema goes away as a child grows older, though some children will continue to experience eczema into adulthood.
Adults can develop eczema, too, even if they never had it as a child.
Most types of eczema cause dry, itchy skin and rashes on the face, inside the elbows and behind the knees, and on the hands and feet. Scratching the skin can cause it to turn red, and to swell and itch even more. Living with eczema can be an ongoing challenge.
Nobody knows exactly what causes eczema, but it can run in families. Many people with eczema also have other allergic conditions, including hay fever and asthma.
People with eczema find it hard to keep the moisture in their skin, so it becomes dry and easily irritated. This causes chemicals to be released, which worsens the irritation and makes you want to scratch. But scratching only makes your skin more itchy and so the cycle repeats itself. This can be very frustrating. But there are many ways to manage eczema and with your doctor’s help, you will likely find out what works for you.
There is no cure for eczema but there are treatments. Depending on age and eczema severity, these treatments include over-the-counter (OTC) remedies, prescription topical medications, phototherapy, immunosuppressants, and biologic drugs. Many people with eczema also find success with specific natural and alternative treatments.
For most types of eczema, managing flares comes down to these basics:
- Know your triggers so that you can avoid exposure
- Implement a daily bathing and moisturizing routine
- Use OTC and prescription medication consistently and as prescribed
Is eczema contagious?
Eczema is not contagious. You can’t “catch it” from someone else. While the exact cause of eczema is unknown, researchers do know that people who develop eczema do so because of a combination of genes and environmental triggers. When an irritant or an allergen “switches on” the immune system, skin cells don’t behave as they should causing an eczema flare-up.
Types of eczema
Eczema is the name for a group of conditions that cause the skin to become red, itchy and inflamed. There are eight types of eczema:
- Atopic dermatitis,
- Contact dermatitis,
- Dyshidrotic eczema,
- Hand eczema,
- Lichen simplex chronicus,
- Nummular eczema,
- Seborrheic dermatitis,
- Stasis dermatitis.
What triggers eczema?
There are some everyday elements in your surroundings that might trigger you or your child’s eczema or cause it to get worse.
Knowing what triggers your eczema or makes it worse will help you keep your symptoms under control. It’s important to remember that eczema is different for everyone. The triggers you have may not be the same as the triggers for others with eczema. You or your child may experience triggers or worsening of your eczema at particular times of the year and/or in certain situations.
There are many things, known as triggers, that can make eczema symptoms worse, including:
- Dry skin. When your skin gets too dry, it can easily become brittle, scaly, rough, or tight, which can lead to an eczema flare up.
- scratching the affected area
- viral or bacterial infections
- chemicals from swimming pools
- sand, especially from sandpits
- contact with some types of carpet or grass
- allergens that you can breathe in, such as pollen
- artificial colors and preservatives
- perfumes, soap and chemicals
- woollen or synthetic fabrics
- heat or very hot rooms
- stress.
Not all of these things will trigger a person’s eczema. It varies from person to person.
Irritants
There are everyday products and even natural substances that can cause your skin to burn and itch, or become dry and red.
These could be products that you use on your body or in your home — hand and dish soap, laundry detergent, shampoo, bubble bath and body wash, or surface cleaners and disinfectants. Even some natural liquids, like the juice from fresh fruit, vegetables, or meats, can irritate your skin when you touch them.
Some common eczema irritants include:
- Metals, in particular, nickel
- Cigarette smoke
- Soaps and household cleaners
- Fragrances
- Certain fabrics such as wool and polyester
- Antibacterial ointment like neomycin and bacitracin
- Formaldehyde, which is found in household disinfectants, some vaccines, glues and adhesives
- Isothiazolinones an antibacterial that is found in personal care products like baby wipes
- Cocamidopropyl betaine used to thicken shampoos and lotions
- Paraphenylene-diamine, which is used in leather dyes and temporary tattoos, among others
Stress
Emotional stress considered an eczema trigger, but we are not exactly sure why. Some people’s eczema symptoms get worse when they’re feeling “stressed.” Others may become stressed, just knowing they have eczema, and this can make their skin flare up.
Climate and sweating
Many people with eczema become itchy, or experience a “prickly heat” sensation when they sweat, or get too hot. This can happen when you exercise or wear too many clothes to bed. During the cold winter months, your skin may also get too dry — leading to irritation and an eczema flare up.
Your eczema also may flare when the air is too dry or too humid. Or if you take long, hot showers or baths.
Infection
Your eczema can become infected with bacteria or viruses that live in the environment. Staphylococcus aureus (“staph”) is one of the most common types. The molluscum virus, herpes virus (fever blisters and cold sores), and certain kinds of fungus (ringworm or athlete’s foot) are other common triggers for infection. It’s important to know the symptoms of these different infections and what causes them, so that your eczema does not get worse.
Allergens
There are everyday materials in the environment that can cause you to have an allergic reaction and trigger an eczema flare up. Some of the most common are: seasonal pollen, dust mites, pet dander from cats and dogs, mold and dandruff.
Allergens that cause symptoms to stick around a lot longer, or to come back, are much harder to pinpoint. It’s important to know the allergens that could cause a flare up, so that you can help keep your symptoms under control.
Hormones
Hormones are substances produced by the body that can cause a wide variety of symptoms. When the levels of certain hormones in your body increase or decrease, some people with eczema (especially women) may experience flare ups.
Eczema symptoms
The most important thing to remember is that eczema and its symptoms are different for everyone. Your eczema may not look the same on you as it does on another adult, or on your child. It may even appear in different areas of the body at different times.
Eczema is usually itchy. For many people, the itch is usually only mild, or moderate. But in some cases it can become much worse and you might develop extremely inflamed skin. Sometimes the itch gets so bad that people scratch it until it bleeds, which can make your eczema worse. This is called the “itch-scratch cycle.”
What to look for:
- Dry, sensitive skin
- Red, inflamed skin
- Very bad itching
- Dark colored patches of skin
- Rough, leathery or scaly patches of skin
- Oozing or crusting
- Areas of swelling
You might have all of these symptoms of eczema or only just a few. You might have some flare ups or your symptoms could go away entirely. But the only way to know if you have eczema for sure, is to visit your doctor so he or she can look at your skin and ask you about your symptoms.
Eczema causes
Doctors don’t know what exactly causes eczema. However for most types of eczema, researchers believe a combination of environmental factors and genetics are involved.
People with eczema tend to have an over-reactive immune system that when triggered by an allergen or irritant, attacks the body instead of protecting it. This results in too much inflammation, which leads to red, itchy and painful skin.
Research also shows that people with eczema may have a mutation of the gene responsible for creating filaggrin – a protein that contributes to creating a healthy protective layer – or skin barrier – on the very top layer of our skin. Without enough filaggrin to build a strong skin barrier, moisture can escape and bacteria can enter. This is why people with eczema have extremely dry skin and a tendency to get infections.
Eczema treatment
The key to staying healthy while living with eczema is to keep symptoms under control. That’s why it’s good to know about the everyday “triggers” in your surroundings — like dry skin, irritants, allergens and stress — that might make your or your child’s eczema flare up, or get worse.
In many cases eczema is manageable, especially with a proper skin care routine. This includes bathing and moisturizing daily, sometimes in combination with prescription medications and/or alternative therapies.
There are many different treatments that people who live with eczema can use to relieve symptoms.
These include:
- Over-the-counter remedies such as gentle, non-soap cleansers, petroleum jelly, tar-based products and mineral oil
- Medications available only with a prescription from a doctor, such as topical corticosteroids, topical calcineurin inhibitors (TCIs) and systemic oral drugs
- Phototherapy, which exposes the affected area to light under medical supervision
- Complementary and alternative therapies, including acupuncture, supplements and stress reduction techniques
Remember that eczema symptoms can be different for everyone. Not everyone will respond to a treatment in the same way, so it’s best to familiarize yourself with all of the options and talk to your doctor to find a treatment regimen that works for you.
How to get rid of eczema and what you can do to help control eczema:
- Setting up a good skin care routine that includes daily bathing and moisturizing is very important for managing eczema symptoms and preventing flares. Establish a daily skin care routine — just like you would for other activities such as brushing your teeth. Try not to miss treatments, but be flexible if your symptoms change.
- Recognize stressful situations and events — and learn to avoid or cope with them by using techniques for stress management. You may do this on your own, or with the help of your doctor or psychologist.
- Be mindful of scratching and rubbing — and limit contact with materials or substances that may irritate your skin. Dress in soft, breathable clothing and avoid itchy fabrics like wool, that can further irritate your eczema.
- Bleach baths are thought to reduce the risk of staph infections by decreasing bacteria on the skin and reducing inflammation in both children and adults.
- During particularly intense eczema flare-ups, wet wrap therapy can work wonders to rehydrate and calm the skin.
Common eczema treatment
Over-the-counter (OTC) products
Over-the-counter (OTC) treatments are products or medications you can buy without a prescription. Some OTC eczema treatments are used for moisturizing skin; some are used to help skin symptoms such as rash, redness and itch; and some are for gently cleaning skin to prevent infection.
Bathing
The most effective way to treat dry skin is to give it the moisture it needs through proper bathing and moisturizing. Soak in a warm bath or take a shower and then moisturize immediately afterward (within three minutes). You can help calm specific symptoms of eczema by adding bleach, vinegar, salt, oatmeal or baking soda to your bath water.
Why is bathing so effective?
When your skin is dry, it’s not because it doesn’t contain enough oil. It’s because your skin isn’t doing a very good job of retaining its moisture (water). Wind, low humidity, cold temperatures, harsh soaps and too much washing without the use of a moisturizer can lead to dry skin, which can irritate your eczema and even make it worse.
The most effective way to treat dry skin is to give it the moisture it needs. Proper bathing and moisturizing are important for this reason — especially if you have eczema. The best way to replace moisture in the skin is to soak in a bath or take a shower and then moisturize immediately afterward.
Some things to remember when bathing:
- Take at least one bath or shower a day
- Bathe or shower in lukewarm (not hot) water for 10 to 15 minutes
- Avoid scrubbing your skin with a washcloth or loofah
- Use a gentle cleanser (not soap)
- During severe flare-ups, limit the use of cleansers to further avoid irritation
Some things to remember when moisturizing:
- Use a high-oil content moisturizer twice a day to improve hydration and protect the skin barrier
- Moisturize hands every time you wash them or they come into contact with water
- Schedule your bathing and moisturizing routine at night, just before bed. This can help your skin better retain its moisture
- If you have hand eczema, soak your hands in water, then follow with an application of your prescription medication (if you use one) and moisturizer. Wear cotton gloves over your hands while you sleep to help “lock in” the moisturizer.
What kinds of products should I use when bathing?
You should always look for skin products that are unscented, fragrance-free and dye-free so that you don’t further irritate your skin.
Try to avoid waterless, antibacterial cleansers, which often contain ingredients like alcohol and solvents that are very hard on your skin (especially during flare-ups). Remember not to scrub your skin while cleansing and to gently pat your skin dry when you’re done. As always, moisturize your skin immediately afterward.
Are there special types of baths that treat eczema?
Soaking in a tub of lukewarm (not hot) water can help your skin better absorb moisture, but bathing is also very relaxing and can help ease stress. Just remember not to soak longer than 10 to 15 minutes and avoid scrubbing your skin with a washcloth or loofah.
Some specific bath treatments you might try:
- Bath oil bath
Using gentle oils in your bath water can help keep you moisturized. Be sure to use oils that do not contain fragrances or bubble bath solutions that could further irritate your skin. Be careful — oils can make the tub very slippery.
- Baking soda bath
Adding a quarter-cup of baking soda to your bath or applying it to the skin directly in the form of a paste, is a common treatment used to help relieve itching.
- Bleach bath
A mild bleach and water solution is thought to decrease inflammation and bacteria on the skin, which can lead to skin infections. Use a half-cup of household bleach for a full tub of water, one-quarter cup for a half tub. 2 tablespoons for a baby bathtub (approx. 4 gallons). Soak up to 10 minutes, then rinse off with warm tap water. Proceed with daily skin care routine. Best when done two to three times per week.
Taking bleach baths two to three times per week is thought to reduce inflammation and the risk of developing staph infections by safely decreasing bacteria on the skin. This bleach bath recipe has the same level of chlorine in your average swimming pool.
Things to remember about bleach bath:
- DO NOT use excessively hot or cold water (fill bath tub with lukewarm water)
- DO NOT add any other products or ingredients to the bath
- DO NOT soak for longer than 15 minutes
- DO NOT submerge your head or face under the water
- DO consult with your health care provider first before trying a bleach bath or giving one to your child for the first time.
- Oatmeal bath
Adding colloidal oatmeal to your bath or applying it to the skin directly in the form of a paste, is also a common treatment used to help relieve itching.
- Salt bath
If you’re experiencing a severe flare-up, bathing may cause your skin to sting. Adding one cup of table salt to your bath water can help ease this symptom.
- Vinegar baths
Add one cup to one pint of vinegar to the bath. Can be used as a wet dressing, too, as the vinegar is thought to kill bacteria.
Is a bath or shower better for my eczema?
Water is an effective way to put moisture back into the skin, but only if you use lukewarm (not hot) water, avoid scrubbing and apply a moisturizer within three minutes after bathing or showering. As long as you follow these rules, both bathing and showering are equally effective in keeping the skin barrier healthy and flexible, so that it can better lock in moisture and keep irritants out.
However, too much contact with water or improper bathing can actually cause irritation. Especially if you repeatedly get your skin wet without moisturizing it immediately afterward. This causes your skin to lose its moisture content and become dry and irritated.
Moisturizing
When your skin gets too dry, it can become irritated and cause your eczema to flare. Wind, low humidity, cold temperatures, harsh soaps and too much washing without the use of a moisturizer immediately after, all can lead to dry skin.
Bathing and properly moisturizing are two of the most important things you can do to help control your condition. It’s important to understand how and when to properly moisturize, and which products are best to use when you have eczema.
Eczema cream
The importance of moisturizing cannot be over emphasized as a treatment for eczema and sensitive skin. Moisturizers maintain skin hydration and barrier function. Generic petroleum jelly and mineral oil (without additives) are two of the safest, most effective moisturizing products.
What type of moisturizer is good for eczema?
The more water there is in a lotion or moisturizer, the more likely it is to worsen your hand eczema. Moisturizers usually contain more water than oil, and when the water evaporates it can dry out the skin. The best moisturizer for hand eczema is a greasy ointment, such as petroleum jelly. Be sure to read the label to determine which moisturizer has the least amount of water.
Apply the moisturizer to your hands immediately after you bathe and each time you wash your hands.
Remember that it can take a few months for a flare-up to clear. Even if your hands appear eczema-free, you will sometimes need to take special care with them to avoid a return of symptoms.
Look for cleansers and moisturizers with National Eczema Association’s Seal of Acceptance™ on the label. These products are intended for use by people with eczema or sensitive skin. You should always test a small amount on your skin before full use to ensure there are not personal sensitivities to ingredients.
Tips for choosing a moisturizer
Finding a moisturizer that works for you or someone you care for can be a challenge. What works for one person may not work for another. As the condition of your skin changes so can the effectiveness of a product. A manufacturer may also change the formulation of a product from one year to the next. Take the following steps when introducing a new product to your skin.
- If you know you are allergic to a particular ingredient check the label before you buy.
- Review the list of moisturizers that have received the National Eczema Association Seal of Acceptance™.
- The first time you apply a new product use a small amount (about the size of a pea) to the pulse of your wrist or the crook of your elbow. Do not wash the area for 24-48 hours and watch for any allergic reaction such as redness, a rash, any form of breakouts on the skin, itchiness, pain, flaking etc.
There are three basic classes of moisturizers:
- Ointments
Ointments are semi-solid greases that help to hydrate the skin by preventing water loss. Petroleum jelly has no additional ingredients, whereas other ointments contain a small proportion of water or other ingredients to make the ointment more spreadable. Ointments are very good at helping the skin retain moisture but they are often disliked because of their greasiness.
- Creams
Creams are thick mixtures of greases in water or another liquid. They contain a lower proportion of grease than ointments, making them less greasy. A warning: creams often contain stabilizers and preservatives to prevent separation of their main ingredients, and these additives can cause skin irritation or even allergic reactions for some people.
- Lotions
Lotions are mixtures of oil and water, with water being the main ingredient. Most lotions do not function well as moisturizers for people with dry skin conditions because the water in the lotion evaporates quickly.
Note: Nut oil, food/plant derivatives, and some natural ingredients can raise allergy issues for some individuals, and be of concern for pediatric patients. Each National Eczema Association Seal of Acceptance™ Review will alert consumers to the presence of nut oils and similar natural ingredients. Contact your medical professional for guidance.
What are emollients and moisturizers?
Emollients are products used to soften skin. Moisturizers are products used to add moisture to the skin. There are numerous emollients and moisturisers on sale at general stores and pharmacies. Options include:
- Oils
- Lotions
- Creams
- Ointments
Emollients and moisturizers are most effective when applied immediately after bathing but can also be applied at other times
Why use emollients and moisturizers?
Uses of emollients and moisturizers include:
- To relieve dryness and scaling of the skin
- To disguise fine lines and wrinkles
- To treat mild irritant contact dermatitis
- As a base for make-up
What do emollients and moisturizers contain?
Active ingredients of emollients and moisturizers are occlusives and humectants. They often include other ingredients such as surfactants (non-soap cleansers), fragrances and preservatives.
Occlusive moisturizers
Occlusives are oils of non-human origin, often mixed with water and an emulsifier to form a lotion or cream. They provide a layer of oil on the surface of the skin to reduce water loss from the stratum corneum.
- Bath oil deposits a thin layer of oil on the skin upon rising from the water.
- Lotions are more occlusive than oils.
- Creams are more occlusive again. Thicker barrier creams containing dimeticone are particularly useful for hand dermatitis.
- Ointments are the most occlusive, and include pure oil preparations such as equal parts of white soft and liquid paraffin or petroleum jelly.
The choice of occlusive emollient depends upon the area of the body and the degree of dryness and scaling of the skin.
- Lotions are used for the scalp and other hairy areas and for mild dryness elsewhere
- Creams are used when more emollience is required.
- Ointments are prescribed for dry, thick, scaly areas, but many patients find them too greasy.
Sorbolene cream is general-purpose moisturizer that is non-greasy, cheap and available in bulk without prescription.
The minimum quantity for an occlusive emollient is 250 g (or ml) and often 500 g or 1 kg is needed: liberal and regular usage is to be encouraged. How frequently it is applied depends on how dry the skin is: very dry skin may benefit from a greasy emollient every couple of hours, but slightly dry skin may only need a light moisturizer at night.
Humectants
Humectants increase the water holding capacity of the stratum corneum. They include:
- Glycerine
- Urea
- Alpha hydroxy acids such as lactic acid or glycolic acid.
- Salicylic acid
Urea and the acidic preparations often sting if applied to scratched or fissured skin. They are also keratolytic, that is they have a descaling or peeling effect, important in management of ichthyosis.
Adverse reactions to emollients
Irritant reactions
People with sensitive skin associated with atopic dermatitis or rosacea often describe irritant reactions to emollients and moisturisers such as burning and stinging. If irritation is transient, the product can continue to be used. It should be discontinued if contact dermatitis appears.
Contact allergy
Contact allergy to moisturisers and emollients is rare. Suspected contact allergy to preservative, fragrance or vehicle can be investigated by patch testing.
Folliculitis
Occlusive emollients can cause or aggravate acne, perioral dermatitis, folliculitis and boils.
Thermal burns
Thermal burns from paraffin-containing ointments on the skin, clothing or bedding, can be dangerous and may occur if exposed to cigarettes or a lighted fire.
Prescription topicals
Prescription topical medications include corticosteroids (steroids), topical calcineurin inhibitors (TCIs) and PDE4 inhibitors. Available through your doctor, these medications are applied to the affected area of the skin to help ease redness, rash and itching.
Topical steroids
One of the most commonly prescribed medications for eczema is topical corticosteroids, or just “steroids,” which can ease redness and reduce inflammation and itching so that your skin can begin to heal.
Steroids are naturally occurring substances that our bodies make in order to regulate growth and immune function. Corticosteroids have been used for more than 50 years in topical medications (applied to the skin) to treat many kinds of inflammatory skin conditions including eczema.
There are a number of different topical steroid types and a few different vehicles (ointment, cream, lotion, spray) that they’re contained in.
Topical steroids are classified by strength, which ranges from “super potent” (Class I), to “least potent” (Class 7). Many brand-name topical steroids also have generic versions. If your doctor feels it’s important to treat your eczema with a particular steroid formulation, they may not prescribe the generic version. If your doctor wants you to try a brand name steroid, check drug manufacturer’s website for any kind of co-pay assistance program.
Some topical steroids, from most potent to least potent:
Strength, by class
Class 1 – Super potent
- 0.05% clobetasol propionate
- 0.05% halobetasol propionate
- 0.1% fluocinonide
Class 2 – Potent
- 0.05% diflorasone diacetate
- 0.05% halobetasol propionate
- 0.01% fluocinonide
- 0.25% desoximetasone
Class 3 – Upper mid-strength
- 0.05% fluocinonide
- 0.05% desoximetasone
Class 4 – Mid-strength
- 0.1% clocortolone pivalate
- 0.1 mometasone furoate
- 0.1% triamcinolone acetonide
- 0.1%betamethasone valerate
- 0.025% fluocinolone acetonide
- 0.05% desoximetasone
Class 5 – Lower mid-strength
- 0.05% fluticasone propionate
- 0.1% prednicarvate
- 0.1% hydrocortisone probutate
- 0.1% triamcinolone acetonide
- 0.025% fluocinolone acetonide
Class 6 – Mild
- 0.05% alclometasone dipropionate
- 0.05% desonide
- 0.025% triamcinolone acetonide
- 0.01% hydrocortisone butyrate
- 0.01% fluocinolone acetonide
Class 7 – Least Potent
- 2%/2.5% hydrocortisone
- 0.5 – 1% hydrocortisone
What you need to know when using a topical steroid
- Only apply the steroid to eczema-affected areas of your skin as prescribed by your doctor
- Steroids are most effective when applied within three minutes after bathing
- Only use the steroid as prescribed by your doctor — more often increases the risks of side effects. For many topical steroids, once-a-day application is enough
- Do not use a steroid as a moisturizer
- After you apply the steroid, follow up with a moisturizer on top
- Avoid using large quantities of steroids for long periods of time
Certain areas or types of skin — the face, genitals, raw or thin skin, and areas that rub together, such as beneath the breasts, or between the buttocks or thighs — absorb more medication and care must be taken when applying steroids to these areas
If you apply a dressing over the area of skin you’re treating with the steroid, it will increase the potency and absorption of the medication into your skin. Only use dressings with topical steroids as advised by your physician.
Once inflammation is under control, reduce or stop using the steroid. If you are using high-potency steroids and/or have been using steroids for awhile, please consult your health care provider to avoid the risk of a “rebound” flare after stopping the medication.
Risks to using topical steroids
There are side effects to using topical steroids. It’s important to remember that steroid medications are safest when used as prescribed: in the right quantity, for the appropriate length of time.
Common side effects of steroids include:
- Thinning of the skin (atrophy)
- Skin thickening (lichenification)
- Stretch marks (striae)
- Darkening of the skin
Some of these, like stretch marks, usually only appear in limited areas of the body (on the upper, inner thighs, under the arms, and in the creases of your elbows and knees), and are very rarely permanent with proper use of the medication. However, frequent use of steroid medications on certain parts of the body like on the face and around the mouth may cause more severe side effects, especially when used for long periods of time.
Less common, but more severe side effects of steroids include:
- Glaucoma (damage to the eye’s optic nerve)
- Cataracts (clouding of the eye lens)
- Tiny pink bumps on the skin
- Acne
- Red, pus-filled hair follicles (folliculitis)
- Adrenal suppression
- Topical Steroid Addiction/Withdrawal
Topical calcineurin inhibitors
Topical calcineurin inhibitors (TCIs) are nonsteroidal medications that are applied to the parts of the skin affected by eczema. Once absorbed in the skin, topical calcineurin inhibitors work by stopping a piece of the immune system from “switching on,” preventing it from causing certain eczema symptoms such as redness and itch.
Meant to be used after other topical treatments have failed or another treatment is not recommended, topical calcineurin inhibitors are intended to be used for a short period of time to bring symptoms under control.
Topical calcineurin inhibitors can be applied to all affected areas of the skin, including the eyelids. Topical calcineurin inhibitors do not cause certain side effects associated with steroid overuse, such as thinning of the skin, or stretch marks, spider veins or skin discoloration.
Common side effects with topical calcineurin inhibitors include mild burning or stinging sensation when the medication is first applied to the skin. A very few number of patients on Elidel received a diagnosis of skin cancer or lymphoma, a type of blood cancer. However, a link to Elidel and these cancers has not been shown.
As with any new medication, it’s important that you talk to your doctor about the benefits and risks of using a TCI to control your eczema.
Some things to remember:
- Use topical calcineurin inhibitors only on areas of the body where the skin is affected by eczema
- Do NOT use topical calcineurin inhibitors on children under two years old
- Do NOT use topical calcineurin inhibitors continuously for longer than six weeks
Topical calcineurin inhibitors should not be used at the same time as phototherapy treatments. Take care to cover and protect your skin when out in the direct sunlight while using topical calcineurin inhibitors.There are two topical calcineurin inhibitors available by prescription, Protopic and Elidel.
Topical PDE4 inhibitor
This drug blocks or “inhibits” an enzyme called phosphodiesterase 4, or PDE4 from allowing too much inflammation in the body. PDE4 is produced by cells in your immune system and helps the body function in part by controlling cytokines. Cytokines are bits of protein also produced by your cells that contribute to inflammation. When cytokines are mistakenly triggered in the body, the resulting inflammation can contribute to the development of certain diseases, including atopic dermatitis.
Currently, there is one topical PDE4 inhibitor for atopic dermatitis. Approved by the U.S. Food and Drug Administration in late 2016, Eucrisa (crisaborole) is available for people with mild to moderate atopic dermatitis ages 2 years and up.
In clinical trials, Eucrisa (crisaborole) was shown to reduce symptoms of atopic dermatitis such as itching, redness, lichenification (thickened skin), weepy rash, and raw, scratched lesions. Overall, participants in the clinical trial achieved clear or almost clear skin after 28 days of use.
Reported side effects include skin irritation where the ointment is applied, and hypersensitivity to Eucrisa’s active ingredient, crisaborole.
Eucrisa (crisaborole) comes in a 2% topical ointment and is applied to the skin two times a day.
Phototherapy
Phototherapy, also called light therapy, means treatment with a special kind of light.
In phototherapy, a special machine is used to emit narrowband ultraviolet B (UVB) light onto the skin in order to help reduce itching and inflammation, increase vitamin D production and bacteria-fighting systems in the skin.
Broadband UVB phototherapy, PUVA (Psoralen and UVA), and UVA1 are other forms of phototherapy that may be used in special circumstances to treat eczema.
Phototherapy helps to:
- Reduce itch
- Calm inflammation
- Increase vitamin D production
- Ramp up bacteria-fighting systems in the skin
Phototherapy is used for eczema that is all over the body (widespread) or for localized eczema (such as hands and feet) that has not gotten better with topical treatments.
About 70% of people with eczema get better with phototherapy. Some people find that phototherapy puts their eczema in a “remittive” or “quiet” state long past the end of the treatment.
What should you consider before starting phototherapy
Before you start phototherapy, there are some things to consider:
- For it to be effective, phototherapy generally requires 2 to 3 treatments per week in the office.
- Risks: burns, increased aging and increased risk of skin cancer over time are all significant risks with any type of phototherapy. Eye protection must be worn for every treatment to prevent damage to the eyes.
What should you expect with phototherapy
- During your visit you will apply a moisturizing oil to the skin and stand in the cabinet undressed except for underwear and protective goggles
- The machine will be activated for a short time, usually just seconds to minutes, and will treat the entire body, or just certain exposed areas
- Careful records are kept of your response and the light is slowly increased with each treatment
- After several months of treatment, the frequency of the visits can sometimes be reduced to once or twice weekly
- If things continue to improve, phototherapy can be stopped for a period to see if the eczema is in remission
- If successful, some patients may restart the cycle or simply come once or twice weekly to maintain their improvement
- When it does work, it is not a rapid improvement like some treatments: generally 1-2 months of steady treatment is necessary to start to see improvement.
Immunosuppressants
The root cause of atopic dermatitis is still not fully known. However, it is known that the immune system goes haywire and causes inflammation in the skin. This inflammation can cause some symptoms of atopic dermatitis such as itching and redness. For moderate to severe cases of atopic dermatitis, your doctor may prescribe a systemic medication to stop your immune system from overreacting.
This class of medication is considered “off-label,” which means that it’s not approved by the Food and Drug Administration (FDA) to specifically treat atopic dermatitis and other forms of eczema.
How do immunosuppressants work?
Immunosuppressants help to stop the itch-scratch cycle of eczema; allow the skin to heal; and reduce the risk of skin infection.
There are a number of immunosuppressants, but the three most commonly used for treating eczema are:
- Cyclosporine is a medication first used to prevent the body from rejecting a transplanted organ, such as a kidney or the heart.
- Methotrexate is a medication used frequently in psoriasis and different types of arthritis.
- Mycophenolate mofetil is used in transplant patients and for other diseases of the immune system.
What are the side effects of immunosuppressants?
Immunosuppressants have some potential side effects, including:
- Increased risk of infections
- Upset stomach and vomiting
- Increased risk for certain types of cancers
- Increased blood pressure with cyclosporine
- Increased risk of kidney damage with cyclosporine and methotrexate
- Risk of liver damage with methotrexate
In general, immunosuppressants are used for some months to get the eczema under control, and then are tapered off. For many people, the improvement in their eczema on immunosuppressants helps to control symptoms with topical medications in the long term.
Biologics
Biologic drugs or “biologics” take an “inside out” approach by treating atopic dermatitis internally. They contain genetically engineered proteins derived from human genes and are administered subcutaneously (through the skin) or intravenously (through the vein) as infusions to target specific parts of the immune system that trigger inflammation.
How do biologics work?
The human body contains a certain type of protein called an interleukin, or IL, that helps our immune system fight off harmful viruses and bacteria. But for those of us with inflammatory diseases like atopic dermatitis, our immune systems tend to “overreact” or go haywire, triggering certain ILs to mistakenly attack the body instead of protecting it. This results in chronic inflammation that leads to those itchy, red patches on your skin.
Biologics block ILs from binding to their cell receptors, which stops the immune system from overreacting. A calmer immune system means lower or less severe inflammation and therefore fewer symptoms of atopic dermatitis.
What are the risks of biologics?
As you would with any medication, consult with your doctor to weigh the benefits vs. the risks to determine whether a biologic is the right treatment for you, especially if you are nursing, pregnant or trying to conceive.
Dupixent (dupilumab)
Dupixent (dupilumab) is the first biologic medication approved by the U.S. Food and Drug Administration (FDA) for adults with moderate to severe atopic dermatitis for whom topical treatments have not worked or are not advised.
Dupixent (dupilumab) works on two interleukins believed to contribute to atopic diseases: IL-4 and IL-13. By blocking IL-4 and IL-13 from binding to their cell receptors, Dupixent limits the immune system from overreacting, lowering the severity of inflammation and decreasing the symptoms of atopic dermatitis.
In clinical trials, more than half of patients using Dupixent for 16 weeks reported their symptoms of atopic dermatitis were reduced by 75 percent. The most common side effects reported were conjunctivitis (pink eye), injection site reactions and cold sores on the mouth or lips.
Due to the chronic nature of atopic dermatitis, patients are encouraged to remain on Dupixent to continue experiencing the benefits of the drug.
Dupixent is taken by subcutaneous (under the skin) injection every other week after an initial loading dose and is available on prescription only.
Home remedies for eczema
Eczema is a recurring condition that results in dry, easily irritated, itchy skin. The best way to keep it under control is to establish a daily skincare regimen and stick with it. Here’s how to care for eczema in three easy steps.
- Take at least one bath or shower daily, using lukewarm — not hot — water for 5-10 minutes. Many dermatologists recommend bathing at night before bedtime, when the skin is more likely to lock in moisture while keeping irritants out. Use a gentle cleanser recommended for sensitive skin with no added fragrances or dyes and a low PH (below 5.5). Avoid rubbing or scrubbing the affected skin with a washcloth or loofah.
- After bathing, pat the skin lightly with a towel leaving it slightly damp. Water softens the skin and enables it to better absorb medication and moisturizer. Now apply a thin coat of the topical medication prescribed by your doctor to affected areas of the skin only. Always follow your doctor’s dosage and application recommendations as well as any directions for applying certain medications to specific areas of the body.
- Now liberally apply a moisturizer all over the body (not just the eczema areas) to lock in moisture. Ointments and creams are more beneficial than lotions for people with dry skin conditions because the water in lotion evaporates quicker. Dispense moisturizer with a pump or clean spoon to avoid contamination. Apply it with your palms, stroking lightly in a downward direction. Wait a few minutes to let the moisturize absorb into the skin before dressing. Don’t limit moisturizing to bath time. Slather it on throughout the day whenever the skin starts to itch or feel dry.
Complementary and Alternative Treatments
Many people with eczema use products and practices that are outside Western, or conventional, medicine to help manage their symptoms. If you use these natural therapies with doctor-prescribed medications, you are using a “complementary” method to manage your eczema. If you are using natural therapies in place of conventional medicine, you are using an “alternative” method.
Before you consider any kind of treatment, it’s important to understand what triggers your eczema. Learning about the irritants in your everyday surroundings can help you better manage the condition whether you use traditional medications, alternative therapies, or both.
The following complementary and alternative therapies have been studied and found to benefit certain symptoms of eczema in adults. Check with your health care provider if you are interested in trying alternative therapies on your child’s eczema.
Natural remedies for eczema
Coconut oil
Studies show that applying coconut oil topically reduces the amount of staph bacteria on the skin, which reduces the chance of infection.
Apply coconut oil once or twice a day to damp skin. Be sure to choose coconut oils that are “virgin” or “cold pressed.” This method of oil extraction does not use chemicals, which could further irritate skin.
Sunflower oil
Sunflower oil boosts the skin’s barrier function, helping it to retain moisture. It also has anti-inflammatory properties. Apply sunflower oil to adult skin twice a day, with one of those times being shortly after bathing while skin is still wet.
Avoid using sunflower oil, if you have a known allergy to sunflower seeds.
Cardiospermum
Cardiospermum is a flowering tropical vine native to India and Africa. When extracted and put into a topical ointment, cardiospermum can help reduce inflammation, itch and bacteria on the skin.
Topical vitamin B12
Topical vitamin B12 has been shown to be effective on eczema symptoms in both adults and children. However, there is no commercial product as of this writing, and so it must be compounded. Dr. Peter Lio, a dermatologist at Chicago Integrative Eczema Center and member of the NEA Board of Directors and Scientific Advisory Committee, shares this recipe for a B12 compound, Pink Magic.
Pink Magic
- 0.07 g cyanocobalamin (vitamin B12)
- 46 g persea gratissima Oil (avocado oil)
- 45.42 g water
- 8 g TEGO® Care PS or methyl glucose stearate (an emulsifier)
- 0.26 g potassium sorbate (a preservative)
- 0.25 g citric acid
You can also mix 0.07 grams of vitamin B12 in a moisturizer base.
Mind-body approach
Stress is a known trigger for atopic dermatitis flares. Though the exact relationship between stress and atopic dermatitis is unknown, experts believe that when you experience a stressful situation, your body produces inflammation. And inflammation is an underlying cause of atopic dermatitis symptoms.
Training the mind
Some experts believe that there is a strong connection between the mind and skin disorders. In fact, some doctors practice what is known as “psychodermatology” to help the patient with stress, anxiety and other emotional disorders that may worsen his or her symptoms. Psychodermatology is more commonly practiced in Europe than the U.S.
Some techniques used include:
- Hypnosis
- Biofeedback
- Meditation
Acupressure
Acupressure is similar to acupuncture but with physical pressure applied to certain points on the body, rather than needles, to unblock “life energy.” Limited studies show that acupressure can help relieve the symptoms of itch and lichenification — thick, leathery skin.
Massage
It is well known that massage helps relieve stress, which may then help reduce eczema flares. It’s important to go to a massage therapist who is accredited and experienced with working with people with non-contagious skin conditions. Prior to your appointment, check with your massage therapist to be sure the oils and lotions used will not trigger your eczema or make it worse. Bring your own, if you are unsure.
Baby eczema
Atopic dermatitis is one of the most common types of eczema, affecting 13% of all children under the age of 18 in the United States.
Both atopic dermatitis and other forms of eczema are conditions that infants, toddlers, and older children can develop. Symptoms include skin redness and itch. Atopic dermatitis is considered a chronic, inflammatory condition that is a result of genes and environmental triggers and may last into the child’s teenage years and beyond.
Eczema looks and acts differently in infants and toddlers than it does in older children. The location and appearance of eczema changes as they grow, so it’s important to know what to look for during every stage of your infant or toddler’s life.
Infants (first 6 months)
Eczema usually appears on the face, cheeks, chin, forehead and scalp. It can also spread to other areas of the body, but not usually in the diaper area, where moisture protects the skin. The skin at this stage also tends to look more red and “weepy.”
Babies (6-12 months)
At this stage, eczema often appears on your baby’s elbows and knees — places that are easy to scratch or rub as they’re crawling. If the eczema rash becomes infected, it may form a yellow crust, or very small, “pus bumps” on the skin.
Toddlers (2-5 years)
Around the age of two, your toddler’s eczema is more likely to appear in the creases of the elbows and knees, or on their wrists, ankles and hands. It may also appear on the skin around your toddler’s mouth and the eyelids. Your toddler’s skin may start to look dry and scaly at this stage and become thick with deeper lines — this is called “lichenification.”
Children (5 years+)
Eczema usually appears in the folds of the elbows and/or knees. Sometimes, it’s only on a child’s hands — at least 70% of people have had hand eczema at some time in their life. Redness and itchy patches behind your child’s ears, on their feet or scalp, may also be a sign of atopic dermatitis. But these could also be symptoms of another condition, like seborrheic dermatitis, which can exist with eczema.
What triggers my child’s eczema or causes it to get worse?
Some of the most common eczema triggers include:
- Dry skin
- Irritants
- Heat and sweating
- Infection
- Allergens such as pet dander, pollen or dust
Your child’s eczema may be worse in the winter when the air is dry. Saliva from drooling can also cause irritation on your baby’s cheeks, chin and neck.
The best way to manage your child’s eczema is by getting to know their symptoms and triggers so that you can help keep it under control.
Figure 1. Eczema rash

Eczema Herpeticum
Eczema herpeticum is a disseminated viral infection characterized by fever and clusters of itchy blisters or punched-out erosions 2. The vast majority of eczema herpeticum cases are caused by herpes simplex virus type 1 (HSV 1) and herpes simplex virus type 2 (HSV 2) and most often seen as a complication of atopic dermatitis/eczema 3. However, Cocksackie virus A16 and vaccinia virus have been implicated also in eczema herpeticum 4. Multiple skin disorders have been associated with eczema herpeticum including, pemphigus foliaceous, Darier disease, pemphigus vulgaris, pityriasis rubra pilaris, Hailey-Hailey disease, irritant contact dermatitis, cutaneous T-cell lymphoma, seborrheic dermatitis, psoriasis, Wiskott-Aldrich syndrome, congenital icthyosiform erythroderma, and Sezary syndrome 5, 6. Viral infection is believed to occur as a result of auto-inoculation in a host with a latent infection, or from an infected contact 3.
Eczema herpeticum is also known as Kaposi varicelliform eruption because it was initially described by Kaposi in 1887, who thought it resembled chickenpox/varicella zoster 7.
Figure 2. Eczema herpeticum


What is the cause of eczema herpeticum?
Most cases of eczema herpeticum are due to Herpes simplex virus type 1 (HSV 1) or 2 (HSV 2).
Eczema herpeticum usually arises during a first episode of Herpes simplex infection (primary herpes). Signs appear 5 to 12 days after contact with an infected individual, who may or may not have visible cold sores.
Eczema herpeticum may also complicate recurrent herpes. However, repeated episodes of eczema herpeticum are unusual.
Eczema herpeticum can affect males and females of all ages but is more commonly seen in infants and children with atopic dermatitis. Atopics appear to have reduced immunity to herpes infection. The dermatitis can be mild to severe, active or inactive.
Eczema herpeticum can also occur when there are other reasons for breakdown of the skin barrier, including:
- Thermal burns
- Pemphigus vulgaris
- Darier disease
- Cutaneous T-cell lymphoma / mycosis fungoides
- Ichthyosis.
Other viruses may occasionally be responsible, such as coxsackievirus A16 (the cause of hand foot and mouth disease).
As smallpox has been eliminated, disseminated vaccinia as a consequence of smallpox vaccination is now very rare. It was reported to be very severe, with mortality of up to 50%.
Clinical features of Eczema herpeticum
Eczema herpeticum starts with clusters of itchy and/or painful blisters. It may affect any site but is most often seen on face and neck. Blisters can occur in normal skin or in sites actively or previously affected by atopic dermatitis or other skin disease. New patches form and spread over a period of 7 to 10 days and may rarely be widely disseminated throughout the body.
The patient is unwell, with fever and swollen local lymph nodes.
- The blisters are monomorphic, i.e. they all appear similar to each other.
- They may be filled with clear yellow fluid or thick purulent material.
- They are often blood-stained i.e., red, purple or black in color.
- New blisters have central dimples (umbilication).
- They may weep or bleed.
- Older blisters crust over and form sores (erosions)
- Lesions heal over a period of 2-6 weeks.
- In severe cases where the skin has been destroyed by infection, small white scars may persist long term.
Secondary bacterial infection with staphylococci or streptococci may lead to impetigo and/or cellulitis.
Severe eczema herpeticum may affect multiple organs, including the eyes, brain, lung, and liver. It can rarely be fatal.
Eczema herpeticum diagnosis
Viral infection can be confirmed by viral swabs taken by scraping the base of a fresh blister. Several tests are available.
- Viral culture
- Direct fluorescent antibody stain
- PCR (Polymerase Chain Reaction) sequencing
- Tzank smear showing epithelial multinucleated giant cells and acantholysis (cell separation)
Bacterial swabs should also be taken for microscopy and culture as eczema herpeticum may resemble impetigo and it can be complicated by bacterial infection.
Skin biopsy reveals distinctive pathological changes.
Treatment of Eczema herpeticum
Eczema herpeticum is considered as one of the few dermatological emergencies. Prompt treatment with antiviral medication should eliminate the need for hospital admission.
Oral aciclovir 400 to 800 mg 5 times daily, or, if available, valaciclovir 1 g twice daily, for 10 to 14 days or until lesions heal. Intravenous aciclovir is prescribed if the patient is too sick to take tablets, or if the infection is deteriorating despite treatment.
Secondary bacterial skin infection is treated with systemic antibiotics.
Topical steroids are not generally recommended, but may be necessary to treat active atopic dermatitis.
Consult an ophthalmologist when eyelid or eye involvement is seen or suspected.
Dyshidrotic eczema
Dyshidrotic eczema also called pompholyx, is a form of hand/foot eczema characterized by vesicles or bullae (blisters) 8. It is a form of vesicular dermatitis of hands and feet, also called vesicular endogenous eczema and may be the same condition as dyshidrotic eczema 9. It is sometimes subclassified as cheiropompholyx (hands) and pedopompholyx (feet) 10.
Outlook (prognosis) for dyshidrotic eczema (pompholyx)?
Dyshidrotic eczema generally gradually subsides and resolves spontaneously. It may recur in hot weather or after a period of stress, and in some patients is recalcitrant.
Complications of dyshidrotic eczema (pompholyx)?
Secondary bacterial infection with Staphylococcus aureus and/or Streptococcus pyogenes is common in pompholyx, and results in pain, swelling and pustules on the hands and feet.
Figure 3. Dyshidrotic eczema


Dyshidrotic eczema (Pompholyx) most often affects young adults.
- It is more common in females than males.
- Many of them report palmoplantar hyperhidrosis.
- There is a personal or family history of atopic eczema in 50%.
What causes dyshidrotic eczema?
Dyshidrotic eczema is multifactorial. In many cases it appears to be related to sweating, as flares often occur during hot weather, humid conditions, or following emotional upset. Other contributing factors include:
- Genetics
- Contact with irritants such as water, detergents, solvents and friction
- Association with contact allergy to nickel and other allergens
- Inflammatory dermatophyte (tinea) infections (when it is known as a dermatophytid)
- Adverse reaction to drugs, most often immunoglobulin therapy
What are the clinical features of dyshidrotic eczema?
Dyshidrotic eczema (pompholyx) presents as recurrent crops of deep-seated blisters on the palms and soles. They cause intense itch and/or a burning sensation. The blisters peel off and the skin then appears red, dry and has painful fissures (cracks).
When involving the distal finger adjacent or proximal to the nail fold, it can result in paronychia (nail fold swelling) and nail dystrophy with irregular pitting and ridges.
Dyshidrotic eczema (pompholyx) diagnosis
The clinical presentation is typical.
- If suspicious of a fungal infection (tinea pedis), skin scrapings should be taken for mycology.
- Patch testing is indicated in chronic or atypical cases.
- Skin biopsy is rarely necessary. It shows spongiotic eczema.
Aggravating factors of dyshidrotic eczema (pompholyx)
As in other forms of hand dermatitis, pompholyx is aggravated by contact with irritants such as water, detergents and solvents. Contact with them must be avoided as much as possible and protective gloves worn to prevent additional irritant contact dermatitis.
People with pompholyx that are found to be allergic to nickel must try to avoid touching nickel items.
Dyshidrotic eczema (pompholyx) treatment
Dyshidrotic eczema is challenging to treat. Topical therapy is relatively ineffective because of the thick horny layer of skin of palms and soles.
General measures:
- Wet dressings to dry up blisters, using dilute potassium permanganate, aluminium acetate or acetic acid
- Cold packs
- Soothing emollient lotions and creams
- Potent antiperspirants applied to palms and soles at night
- Protective gloves should be worn when doing wet or dirty work
- Well-fitting footwear, with 2 pairs of socks to absorb sweat and reduce friction
Prescription medicines
- Ultrapotent topical corticosteroid creams applied to new blisters under occlusion, and ointments applied during the inflamed dry phase
- Short courses of systemic corticosteroids, eg prednisone or prednisolone, for flare-ups
- Oral antistaphylococcal antibiotics for secondary infection
- Topical and oral antifungal agents for confirmed dermatophyte infection
- In patients with hyperhidrosis, probanthine or oxybutynin is worth trying.
- In severe cases, immune modulating medicines are indicated. These include: methotrexate, mycophenolate mofetil, azathioprine and ciclosporin.
- Where available, alitretinoin is used for resistant chronic disease.
Other options
- Superficial radiotherapy
- Botulinum toxin injections (to prevent sweating)
- Phototherapy and photochemotherapy (PUVA) therapy
Nummular eczema
Nummular eczema is also called discoid eczema, is a common type of eczema/dermatitis, in which there are scattered, roundish patches of eczema. They can be intensely itchy.
Who gets nummular eczema?
Nummular eczema can affect children and adults. It is slightly more prevalent in adult males than females. In males over the age of 50 years, there is an association with chronic alcoholism.
Nummular eczema can occur in atopic eczema, eczema craquelé and secondary eczematisation.
Figure 4. Nummular eczema



What is the cause of nummular eczema?
The cause of nummular eczema is unknown. Some cases are associated with Staphylococcus aureus infection.
The eruption can be precipitated by:
- Localized injury such as scratch, insect bite or thermal burn
- Impetigo or wound infection
- Contact dermatitis
- Dry skin
- Varicose veins (varicose eczema)
- Another skin problem
What are the clinical features of nummular eczema?
There are two forms of nummular eczema:
- Exudative acute nummular eczema: oozy papules, blisters and plaques
- Dry nummular eczema: subacute or chronic erythematous, dry plaques
Both forms of nummular eczema are usually more prevalent on the limbs than the trunk, but the rash may be widespread. Although often bilateral, the distribution is often asymmetrical.
Individual plaques are well circumscribed, mostly 1–3 cm in diameter, and inflamed. The majority of patches are round or oval, hence the name ‘discoid‘ or ‘nummular’ (coin shape). The plaques are usually very itchy but sometimes don’t itch at all. The skin between the patches is usually normal, but may be dry and irritable.
Severe discoid eczema may generalise, with numerous small to large itchy lesions appearing all over the body due to autoeczematisation reaction.
The patches may clear up without leaving a sign. However, in darker skins, marks may persist for months. These may be dark brown (postinflammatory hyperpigmentation) or paler than surrounding skin (postinflammatory hypopigmentation).
Nummular eczema diagnosis
In most cases, the appearance of nummular eczema is quite characteristic.
- Bacterial swabs may reveal Staphylococcus aureus colonisation or infection.
- Scrapings are commonly taken for mycology, as nummular eczema can look very similar to tinea corporis (ringworm infection).
- Patch testing is sometimes arranged to see whether there could be a contact allergy responsible for the dermatitis. In most cases no specific allergy can be found.
Nummular eczema treatment
As nummular eczema is associated with loss of skin barrier function, it is important to:
- Protect the skin from injury. As this type of dermatitis often starts off as minor skin injuries, protect all your skin carefully. If the hands are affected, use gloves and tools to make sure the skin is not irritated by friction, detergents, solvents, other chemicals or excessive water.
- Apply emollients frequently. Emollients include bath oils, soap substitutes and moisturizing creams. They can be applied to the dermatitis as frequently as required to relieve itching, scaling and dryness. Emollients should also be used on the unaffected skin to reduce dryness. It may be necessary to try several different products to find one that suits. Many people find one or more of the following helpful: sorbolene, glycerine and cetomacrogol cream, white soft paraffin/liquid paraffin mixed, fatty cream, wool fat lotions.
Anti-inflammatory treatments include:
- Topical steroids
Topical steroids are anti-inflammatory creams or ointments available on prescription which may clear the dermatitis and reduce irritation. The stronger products are applied to the patches just once or twice daily for 2–4 weeks. They are repeated from time to time. Mild ones such as hydrocortisone are safe for daily use if necessary.
- Antibiotics
Antibiotics (most often flucloxacillin) are often prescribed if the dermatitis is blistered, sticky or crusted. Sometimes discoid eczema clears completely on oral antibiotics, only to recur when they are discontinued.
Other treatments sometimes prescribed for severe nummular eczema include:
- Oral antihistamines
Antihistamine pills may reduce the itching, and are particularly helpful at night-time. They do not clear the dermatitis. Non-sedating antihistamines appear less useful for discoid eczema than first-generation antihistamines taken at night to help sleep.
Ultraviolet radiation (UV) treatment
Phototherapy several times weekly for 6–12 weeks can reduce extent and severity of nummular eczema.
Steroid injections
Intralesional steroids are sometimes injected into one or two particularly stubborn areas of nummular eczema. This treatment is unsuitable for multiple lesions.
Oral steroids
Systemic steroids are reserved for severe and extensive cases of nummular eczema. They are usually prescribed for a few weeks, while continuing steroid creams and emollients on residual dermatitis.
Other oral treatments
Persistent and troublesome nummular eczema is occasionally treated with methotrexate, azathioprine or ciclosporin. These medicines have important risks and side effects and require careful monitoring by a specialist dermatologist. They may be more suitable in many cases than long-term steroids.
Nummular eczema can usually be controlled with the above measures, although it has a tendency to recur when the treatment has been stopped. In most patients the dermatitis eventually clears up completely.
Eczema on hands
Hand eczema is also known as hand dermatitis, is a common group of acute and chronic eczematous disorders that affect the dorsal and palmar aspects of the hand.
Hand eczema affects about 10% of the U.S. population. Both genetics and contact allergens and irritating substances play a role in “triggering” this form of eczema. It often affects people who work in cleaning, catering, hairdressing, healthcare and mechanical jobs where they may come into contact with chemicals and other irritants.
Hand eczema isn’t contagious. You cannot “catch” it from another person, or give it to someone else. Even so, the symptoms of hand eczema can impact a person’s self-esteem and their ability to perform on the job.
Hand eczema can range from an acute, extremely itchy or painful eruption, characterized by minute, “tapioca” vesicles (dyshidrotic eczema, pompholyx), to the chronic hand eczema commonly seen in those in at-risk occupations. For therapeutic purposes, hand eczema can be classified into vesiculobullous types (acute and chronic) and hyperkeratotic hand eczema (no vesicles in any phase of the eruption). Persons who are predisposed to atopic dermatitis are at particular risk of developing hand eczema. The therapeutic strategy is to eliminate any external cause and to control the cutaneous inflammatory reaction.
Who gets hand eczema?
Hand eczema is common (especially in young adult females) and accounts for 20–35% of all eczema. It may occur at any age, including during childhood. It is particularly prevalent in people with a history of atopic eczema.
Hand eczema is particularly common in industries involving cleaning, catering, metalwork, hairdressing, healthcare, housework, painting and mechanical work. This is mainly due to the contact with irritants, but specific contact allergies can contribute.
Complications of hand eczema
- Bacterial infection (staphylococci and/or streptococci) can result in pustules, crusting and pain.
- Eczema at the ends of the fingers may result in deformed nails.
- Eczema can spread to affect other sites, particularly the forearms and feet.
Figure 5. Hand eczema (hand dermatitis)


Hand eczema causes
Hand eczema often results from a combination of causes, including:
- Genetic and unknown factors (constitutional hand eczema)
- Injury (contact irritant eczema)
- Immune reactions (contact allergic eczema).
Hand eczema is frequently caused or aggravated by work, when it is known as occupational eczema.
Irritants include water, detergents, solvents, acids, alkalis, cold, heat and friction. These damage the outer stratum corneum, removing lipids and disturbing the skin’s barrier function. Water loss and inflammation lead to further impairment of barrier function.
Contact allergy is a delayed hypersensitivity reaction with elicitation and memory phases involving T lymphocytes and release of cytokines.
What does hand eczema look like?
Hand eczema may affect the backs of the hands, the palms or both. It can be very itchy, often burns, and is sometimes painful. It has acute, relapsing and chronic phases.
Acute hand eczema presents with:
- Red macules, papules and plaques
- Itching
- Pain
- Swelling
- Blistering and weeping
- Fissuring or cracks.
Features of chronic hand eczema include:
- Dryness to the point of peeling and flaking
- Lichenification (skin has become thickened and leathery).
There are various causes and clinical presentations of hand eczema.
All types of eczema cause itching and redness of the skin. But some, like hand eczema, look and act slightly different than others.
There is another specific type of hand eczema called pompholyx or dyshidrotic eczema (see dyshidrotic eczema description above), which causes small, itchy blisters to appear on the palms of the hands. Dyshidrotic eczema tends to affect women more than men. If you think that you might have dyshidrotic eczema, make an appointment with your doctor.
Types hand eczema
Atopic hand eczema
Atopic hand eczema depends on constitutional weakness of the skin barrier function and is triggered by contact with irritants. It may affect one or both dorsal hands and palms. It may manifest as a discoid pattern of eczema. Patients may also have eczema in other sites including feet, hands, flexures.
Nummular eczema
Nummular eczema or discoid eczema tends to affect the dorsal surfaces of the hands and fingers as circumscribed plaques. Other sites of the body may or may not be affected.
Vesicular hand eczema
Vesicular hand eczema is also known as pompholyx, cheiropompholyx and dyshidrotic eczema. Intensely itchy crops of skin-coloured blisters arise on the palms and the sides of the hands and fingers. Similar symptoms often affect the feet. It is likely this form of eczema is triggered by emotional stresses via sweating (hyperhidrosis).
Chronic relapsing vesiculosquamous eczema
Chronic relapsing vesiculosquamous eczema is a common pattern of palmar and finger eczema, in which episodes of acute vesicular eczema are followed by chronic scaling and fissuring.
Hyperkeratotic hand eczema
Hyperkeratotic hand eczema is a chronic, dry, non-inflammatory palmar eczema. It can appear similar to palmar psoriasis, but is less red and less well circumscribed.
Fingertip eczema
Fingertip eczema can be isolated to one or several fingers.
Irritant contact eczema
The hands are the most common site for irritant contact eczema, and is often due to wet work and repeated exposure to low-grade irritants. The finger-webs are the first place to be affected, but inflammation can extend to fingers, the backs of the hands and the wrists. Irritant contact eczema often spares the palms.
Acute irritant eczema is due to injury by potent irritants such as acids and alkalis, often in an occupational setting.
Repeated exposure to low-grade irritants such as water, soaps, and detergents leads to chronic cumulative irritant eczema.
Allergic contact eczema
Allergic contact eczema may be difficult to distinguish from constitutional forms of hand eczema and irritant contact eczema. There are about 30 common allergens and innumerable uncommon or rare ones. Common allergens include nickel, fragrances, rubber accelerators (in gloves) and p-phenylenediamine (permanent hair-dye). Clues to contact allergy depend on the allergen, but may include:
- Periodic flare-ups associated with certain tasks or places hours to days earlier
- Irregular, asymmetrical distribution of rash
- Sharp border to the rash (eg, at wrist corresponding with cuff of rubber glove).
Hand eczema diagnosis
Hand eczema is usually straight forward to diagnose and classify by history and examination, considering:
- Acute, relapsing or chronic course
- Past history of skin disease
- Eczema on other sites.
Differential diagnosis includes:
- Contact urticaria — for example, to latex gloves (immediate redness, itching and swelling that resolves within an hour)
- Protein contact eczema, most often affecting caterers (combination of urticaria and eczema induced by reactions to meat)
- Psoriasis (symmetrical, well circumscribed, red, scaly plaques)
- Tinea manuum (unlilateral or asymmetrical, peripheral scale).
Patients with chronic hand eczema may have patch tests to detect contact allergens.
Hand eczema treatment
The best treatment for hand eczema is avoiding what caused it.
Knowing which substances trigger your hand eczema and protecting your hands at home and at work, can help guard your skin against further irritation. The most important thing to remember is to be consistent — a daily routine for care and control is the best defense.
If you believe that a substance at home or at work is causing your hand eczema, your doctor can do a “patch test” to see which allergens or irritants may be the problem. Your doctor can also help pinpoint behaviors or practices that may be contributing to your hand eczema and help you find ways to modify or avoid them.
Patients with all forms of hand eczema should be most particular to:
- Minimise contact with irritants — even water
- Use non-soap cleanser when washing hands, rinse carefully, and ensure hands are completely dry afterwards
- Completely avoid touching allergens that have been identified by patch testing
- Wear task-appropriate protective gloves
- Apply thick emollients before work/school and reapply after washing or when the skin dries out (this may be 10–20 times in a day).
Vinyl gloves are less likely than rubber gloves to cause allergic reactions.
- They must be scrupulously clean and should have no holes.
- They should not be worn for long periods.
- Sweating under the gloves aggravates eczema.
- Lined gloves or inner cotton gloves improve comfort.
Topical steroids reduce inflammation.
- Use a potent topical steroid on eczema on the backs of the hands and an ultrapotent topical steroid on palms.
- Cream formulation is usually best for vesicular hand eczema, and ointment for chronic eczema.
- They should be applied to areas of active eczema once or twice daily for several weeks, then discontinued or frequency/potency reduced.
- Short-term occlusion increases potency and is warranted if standard applications have not been effective.
Secondary infection may require oral antibiotic, usually flucloxacillin.
Severe acute flares of hand eczema are treated with prednisone (systemic steroids) for 2–4 weeks.
With careful management, hand dermatitis usually recovers completely. A few days off work may be helpful. When occupational dermatitis is severe, it may not be possible to work for weeks or months. Occasionally a change of occupation is necessary.
Chronic intractable hand eczema may be treated with secondline agents such as azathioprine, methotrexate, ciclosporin, alitretinoin or phototherapy.
Home remedies to help control hand eczema
- If you need to clean your hands, wash them with lukewarm (not hot) water and fragrance-free cleanser.
- Gently blot hands dry, and apply a moisturizer immediately after you wash your hands.
- Apply thick emollients before work/school and reapply after washing or when the skin dries out (this may be 10–20 times in a day).
- The most effective moisturizers are the ones with a higher oil content (like ointments and creams). Keep one near every sink in your home, so you don’t forget to apply it after washing your hands.
- If sanitizing your hands isn’t necessary, try a waterless hand washing method: use the same cleanser, but without any water and then gently blot off any excess cleanser when you’re done.
- Avoid waterless, antibacterial cleansers, which often contain ingredients like alcohol and solvents that are very hard on your hands (especially during flare-ups).
- Keep cotton gloves around the house to protect your hands while you do chores, like folding the laundry. When the gloves become dirty, be sure to wash them using fragrance-free, dye-free detergent.
- If your fingertips aren’t affected by eczema, you can cut the tips off of your cotton gloves so that they’re more comfortable to wear in warm weather.
- Use a combination of vinyl gloves and cotton liners when doing work that involves getting your hands wet. Afterward, be sure to wash your gloves inside out, and let them air dry. If water gets into your glove, take it off immediately, blot hands dry and replace with a new glove.
- If you’re doing work with foods like potatoes, onions, peppers, meat, or acidic fruits (like tomatoes, or citrus), use disposable gloves that you can throw away once you’re finished.
- Ask someone else to shampoo your hair, or shampoo it yourself while wearing protective gloves (waterproof vinyl with cotton liners). Use rubber bands around your forearms to help keep water from rolling down your arm, and into your gloves.
- Remove rings from your fingers while doing housework and before washing and drying your hands, as irritants can get trapped beneath. Clean your rings often.
- Do not wash dishes or clothes by hand. Instead, use a dishwasher and washing machine. If you can’t avoid washing by hand, do so under running water and use a long-handled scrubber to prevent hot water from damaging your skin.
- Once your eczema clears, your doctor may want you to use petroleum jelly on your hands, overnight, with gloves. Use the same gloves over and over, so that they continue to absorb the product and lock moisture in while you wear them.
Some basic things you can do at work to help control your hand eczema
- Avoid allergens or irritating substances in products you use on the job — like industrial hand cleansers or waterless, antibacterial cleansers that may trigger your hand eczema, or make it worse. These often contain ingredients like alcohol and solvents, that are very hard on your hands, especially during flare-ups.
- Protect your hands at work with a combination of heavy-duty vinyl or neoprene gloves and cotton glove liners. Regularly wash cotton liners and vinyl gloves if they aren’t disposable.
- Always carry your own hand cleanser, moisturizer and medication with you, wherever you go.
- Keep your clothes, protective gear, tools and work surfaces clean and free of residue from irritating substances.
- Treat wounds on your hands (even minor ones) and bandage them in order to avoid irritation from allergens or chemical substances.
Your doctor may also prescribe a barrier repair cream, or topical steroid to help speed up healing.
What type of moisturizer is good for hand eczema?
The more water there is in a lotion or moisturizer, the more likely it is to worsen your hand eczema. Moisturizers usually contain more water than oil, and when the water evaporates it can dry out the skin. The best moisturizer for hand eczema is a greasy ointment, such as petroleum jelly. Be sure to read the label to determine which moisturizer has the least amount of water.
Apply the moisturizer to your hands immediately after you bathe and each time you wash your hands.
Remember that it can take a few months for a flare-up to clear. Even if your hands appear eczema-free, you will sometimes need to take special care with them to avoid a return of symptoms.
What are emollients and moisturizers?
Emollients are products used to soften skin. Moisturizers are products used to add moisture to the skin. There are numerous emollients and moisturisers on sale at general stores and pharmacies. Options include:
- Oils
- Lotions
- Creams
- Ointments
Emollients and moisturizers are most effective when applied immediately after bathing but can also be applied at other times
Why use emollients and moisturizers?
Uses of emollients and moisturizers include:
- To relieve dryness and scaling of the skin
- To disguise fine lines and wrinkles
- To treat mild irritant contact dermatitis
- As a base for make-up
What do emollients and moisturizers contain?
Active ingredients of emollients and moisturizers are occlusives and humectants. They often include other ingredients such as surfactants (non-soap cleansers), fragrances and preservatives.
Occlusive moisturizers
Occlusives are oils of non-human origin, often mixed with water and an emulsifier to form a lotion or cream. They provide a layer of oil on the surface of the skin to reduce water loss from the stratum corneum.
- Bath oil deposits a thin layer of oil on the skin upon rising from the water.
- Lotions are more occlusive than oils.
- Creams are more occlusive again. Thicker barrier creams containing dimeticone are particularly useful for hand dermatitis.
- Ointments are the most occlusive, and include pure oil preparations such as equal parts of white soft and liquid paraffin or petroleum jelly.
The choice of occlusive emollient depends upon the area of the body and the degree of dryness and scaling of the skin.
- Lotions are used for the scalp and other hairy areas and for mild dryness elsewhere
- Creams are used when more emollience is required.
- Ointments are prescribed for dry, thick, scaly areas, but many patients find them too greasy.
Sorbolene cream is general-purpose moisturizer that is non-greasy, cheap and available in bulk without prescription.
The minimum quantity for an occlusive emollient is 250 g (or ml) and often 500 g or 1 kg is needed: liberal and regular usage is to be encouraged. How frequently it is applied depends on how dry the skin is: very dry skin may benefit from a greasy emollient every couple of hours, but slightly dry skin may only need a light moisturizer at night.
Humectants
Humectants increase the water holding capacity of the stratum corneum. They include:
- Glycerine
- Urea
- Alpha hydroxy acids such as lactic acid or glycolic acid.
- Salicylic acid
Urea and the acidic preparations often sting if applied to scratched or fissured skin. They are also keratolytic, that is they have a descaling or peeling effect, important in management of ichthyosis.
Adverse reactions to emollients
Irritant reactions
People with sensitive skin associated with atopic dermatitis or rosacea often describe irritant reactions to emollients and moisturisers such as burning and stinging. If irritation is transient, the product can continue to be used. It should be discontinued if contact dermatitis appears.
Contact allergy
Contact allergy to moisturisers and emollients is rare. Suspected contact allergy to preservative, fragrance or vehicle can be investigated by patch testing.
Folliculitis
Occlusive emollients can cause or aggravate acne, perioral dermatitis, folliculitis and boils.
Thermal burns
Thermal burns from paraffin-containing ointments on the skin, clothing or bedding, can be dangerous and may occur if exposed to cigarettes or a lighted fire.
Eczema on scalp
Eczema on scalp or seborrheic dermatitis is a common, chronic or relapsing form of eczema/dermatitis that mainly affects the sebaceous, gland-rich regions of the scalp, face, and trunk .
There are infantile and adult forms of seborrhoeic dermatitis. It is sometimes associated with psoriasis (sebopsoriasis). Seborrhoeic dermatitis is also known as seborrhoeic eczema.
Dandruff (also called ‘pityriasis capitis’) is an uninflamed form of seborrhoeic dermatitis. Dandruff presents as bran-like scaly patches scattered within hair-bearing areas of the scalp.
Figure 6. Seborrhoeic dermatitis

Figure 7. Seborrheic dermatitis on baby scalp (cradle cap)

Figure 8. Seborrheic dermatitis on eyelid
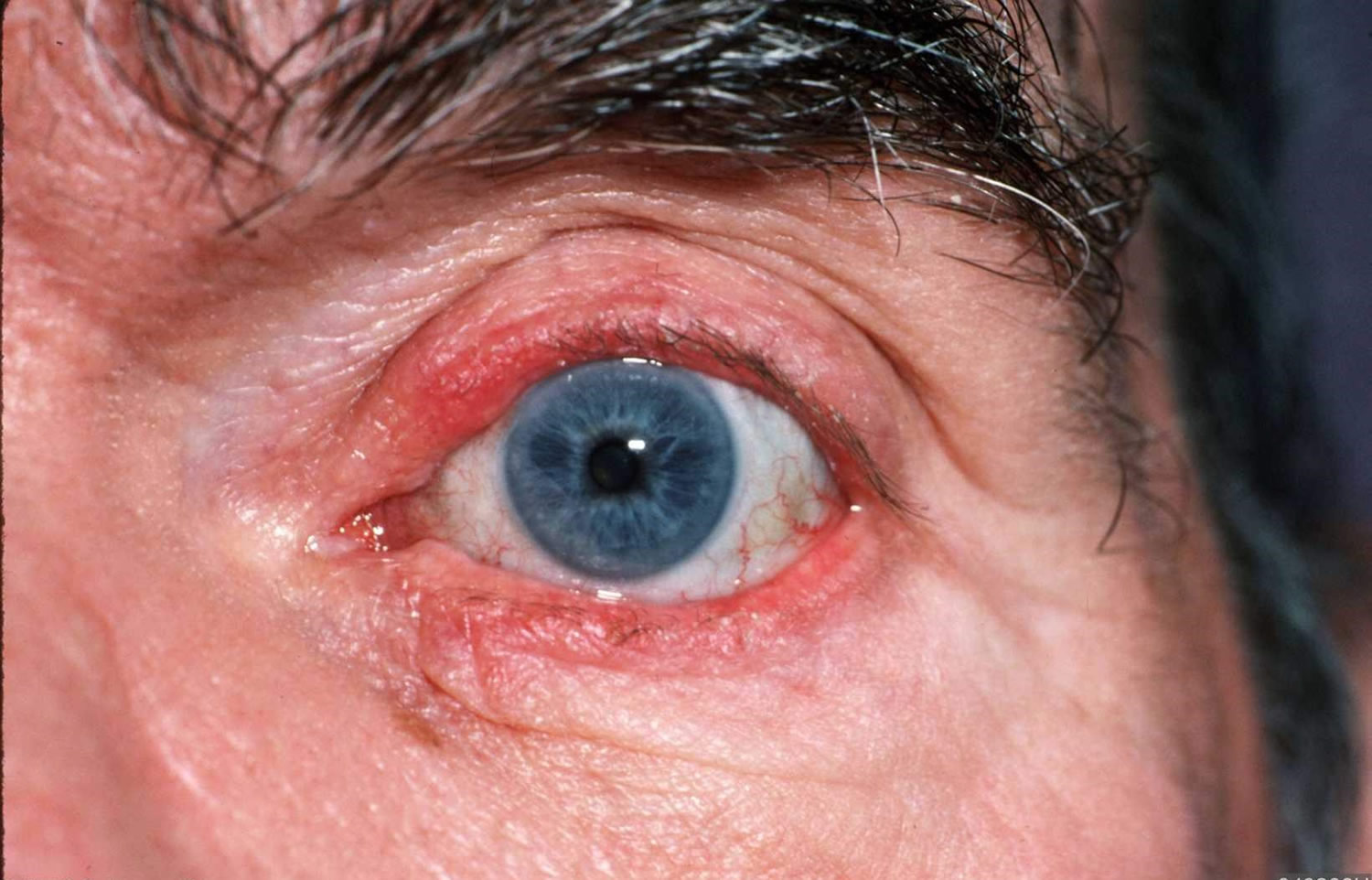
What causes eczema on scalp (seborrhoeic dermatitis)?
The cause of seborrhoeic dermatitis is not completely understood. It is associated with proliferation of various species of the skin commensal Malassezia, in its yeast (non-pathogenic) form. Its metabolites (such as the fatty acids oleic acid, malssezin, and indole-3-carbaldehyde) may cause an inflammatory reaction. Differences in skin barrier lipid content and function may account for individual presentations.
Who gets eczema on scalp (seborrhoeic dermatitis)?
Infantile seborrhoeic dermatitis affects babies under the age of 3 months and usually resolves by 6–12 months of age.
Adult seborrhoeic dermatitis tends to begin in late adolescence. Prevalence is greatest in young adults and in the elderly. It is more common in males than in females.
The following factors are sometimes associated with severe adult seborrhoeic dermatitis:
- Oily skin (seborrhoea)
- Familial tendency to seborrhoeic dermatitis or a family history of psoriasis
- Immunosuppression: organ transplant recipient, human immunodeficiency virus (HIV) infection and patients with lymphoma
- Neurological and psychiatric diseases: Parkinson disease, tardive dyskinesia, depression, epilepsy, facial nerve palsy, spinal cord injury and congenital disorders such as Down syndrome
- Treatment for psoriasis with psoralen and ultraviolet A (PUVA) therapy
- Lack of sleep, and stressful events.
What are the clinical features of eczema on scalp (seborrhoeic dermatitis)?
Infantile seborrhoeic dermatitis
Infantile seborrhoeic dermatitis causes cradle cap (diffuse, greasy scaling on scalp). The rash may spread to affect armpit and groin folds (a type of napkin dermatitis).
- There are salmon-pink patches that may flake or peel.
- It is not especially itchy, so the baby often appears undisturbed by the rash, even when generalized.
Adult seborrhoeic dermatitis
Seborrhoeic dermatitis affects scalp, face (creases around the nose, behind ears, within eyebrows) and upper trunk.
Typical features include:
Winter flares, improving in summer following sun exposure
Minimal itch most of the time
Combination oily and dry mid-facial skin
Ill-defined localised scaly patches or diffuse scale in the scalp
Blepharitis: scaly red eyelid margins
Salmon-pink, thin, scaly, and ill-defined plaques in skin folds on both sides of the face
Petal or ring-shaped flaky patches on hair-line and on anterior chest
Rash in armpits, under the breasts, in the groin folds and genital creases
Superficial folliculitis (inflamed hair follicles) on cheeks and upper trunk
Extensive seborrhoeic dermatitis affecting scalp, neck and trunk is sometimes called pityriasiform seborrhoeide.
How is eczema on scalp (seborrhoeic dermatitis) diagnosed?
Seborrhoeic dermatitis is diagnosed by its clinical appearance and behaviour. As malassezia are a normal component of skin flora, their presence on microscopy of skin scrapings is not diagnostic.
Skin biopsy may be helpful but is rarely indicated. Histological findings specific to seborrhoeic dermatitis are superficial perivascular and perifollicular inflammatory infiltrates, psoriasiform hyperplasia, and parakeratosis around follicular openings.
Eczema on scalp (seborrhoeic dermatitis) treatment
Treatment of seborrhoeic dermatitis often involves several of the following options.
- Keratolytics can be used to remove scale when necessary, eg salicylic acid, lactic acid, urea, propylene glycol
- Topical antifungal agents are applied to reduce malassezia eg ketoconazole, or ciclopirox shampoo or and/or cream. Note, some strains of malassezia are resistant to azole antifungals. Try zinc pyrithione or selenium sulphide
- Mild topical corticosteroids are prescribed for 1–3 weeks to reduce the inflammation of an acute flare
- Topical calcineurin inhibitors (pimecrolimus cream, tacrolimus ointment) are indicated if topical corticosteroids are often needed, as they have fewer adverse effects on facial skin.
In resistant cases in adults, oral itraconazole, tetracycline antibiotics or phototherapy may be recommended. Low dose oral isotretinoin has also been shown to be effective for severe or moderate seborrhoeic dermatitis.
Scalp treatment
- Medicated shampoos containing ketoconazole, ciclopirox, selenium sulfide, zinc pyrithione, coal tar, and salicylic acid, used twice weekly for at least a month and if necessary, indefinitely.
- Steroid scalp applications reduce itching, and should be applied daily for a few days every so often.
- Calcineurin inhibitors such as tacrolimus can be used as steroid alternatives.
- Coal tar cream can be applied to scaling areas and removed several hours later by shampooing.
- Combination therapy is often advisable.
Face, ears, chest and back
- Cleanse the affected skin thoroughly once or twice each day using a non-soap cleanser.
- Apply ketoconazole or ciclopirox cream once daily for 2 to 4 weeks, repeated as necessary.
- Hydrocortisone cream can also be used, applied up to twice daily for 1 or 2 weeks. Occasionally a more potent topical steroid may be prescribed.
- Topical calcineurin inhibitors such as pimecrolimus cream or tacrolimus ointment may be used instead of topical steroids.
- A variety of herbal remedies are commonly used, but their efficacy is uncertain.
Management in infants
Regular washing of the scalp with baby shampoo or aqueous cream is followed by gentle brushing to clear the scales.
- White petrolatum may be useful.
- Topical antifungals are often prescribed, depending on the extent of the rash.
Allergic eczema
Allergic contact dermatitis is a form of dermatitis/eczema caused by an allergic reaction to a material, called an allergen, in contact with the skin. The allergen is harmless to people that are not allergic to it. Allergic contact dermatitis is also called contact allergy.
Who gets allergic contact dermatitis?
Allergic contact dermatitis is common in the general population and in specific employment groups.
- It is more common in women than men, mainly due to nickel allergy and, recently, to acrylate allergy associated with nail cosmetics.
- Many young children are also allergic to nickel.
- Contact allergy to topical antibiotics is common in patients over the age of 70 years old.
- Allergic contact dermatitis is especially common in metal workers, hairdressers, beauticians, health care workers, cleaners, painters and florists.
What causes allergic contact dermatitis?
Allergic contact dermatitis is a type 4 or delayed hypersensitivity reaction and occurs 48–72 hours after exposure to the allergen. The mechanism involves CD4+ T-lymphocytes, which recognise an antigen on the skin surface, releasing cytokines that activate the immune system and cause the dermatitis. Note:
- Contact allergy occurs predominantly from an allergen on the skin rather than from internal sources or food.
- Only a small number of people react to the specific allergen, which is harmless to those who are not allergic to it.
- They may have been in contact with the allergen for years without it causing dermatitis.
- Contact with tiny quantities of an allergen can induce dermatitis.
- Patients with impaired barrier function of the skin are more prone to allergic contact dermatitis, eg patients with leg ulcers, perianal dermatitis, or chronic irritant contact dermatitis.
- Patients with atopic dermatitis associated with defective filaggrin (a structural protein in the stratum corneum) have a high risk of also developing allergic contact dermatitis.
What are the clinical features of allergic contact dermatitis?
Allergic contact dermatitis arises some hours after contact with the responsible material. It settles down over some days providing the skin is no longer in contact with the allergen.
Allergic contact dermatitis is generally confined to the site of contact with the allergen, but it may extend outside the contact area or become generalised.
- Transmission from the fingers can lead to dermatitis on the eyelids and genitals.
- Dermatitis is unlikely to be due to a specific allergen if the area of skin most in contact with that allergen is unaffected.
- The affected skin may be red and itchy, swollen and blistered, or dry and bumpy.
Some typical examples of allergic contact dermatitis include:
- Eczema in skin in contact with jewellery items, due to contact allergy to nickel
- Reactions to fragrances in perfumes and household items
- Eczema under adhesive plaster, due to contact allergy to rosin
- Swelling and blistering of face and neck in reaction to permanent hair dye, due to allergy to paraphenylene diamine
- Hand dermatitis caused by rubber accelerator chemicals used in the manufacture of rubber gloves
- Itchy red face due to contact with methylisothiazolinone, a preservative in wash-off hair products and baby wipes
- Fingertip dermatitis due to acrylates used in hair extensions and nail cosmetics.
- Reactions after dental implants containing acrylates
- Localised blistering at the site of topical medications such as antibiotics
- Swelling and blistering on exposed sites (eg face and hands) due to contact with plants such as poison ivy or, in New Zealand, the Japanese wax tree
- Toxicodendron succedanium
There is a very long list of materials that have caused contact allergy in a small number of individuals.
What is the differential diagnosis of allergic contact dermatitis?
Allergic contact dermatitis should be distinguished from:
- Irritant contact dermatitis, which is due to irritation or repetitive injury to the skin.Irritants include water, soaps, detergents, solvents, acids, alkalis, and friction. Irritant contact dermatitis may affect anyone, providing they have had enough exposure to the irritant, but those with atopic dermatitis are particularly sensitive. Most cases of hand dermatitis are due to contact with irritants. Irritant contact dermatitis can occur immediately after a single injury or develop slowly after repeated exposure to an irritant.
- Other forms of dermatitis, which may mimic allergic contact dermatitis.
- Contact urticaria, in which a rash appears within minutes of exposure and fades away within minutes to hours. The allergic reaction to latex is the best known example of allergic contact urticaria.
- Fungal infections; tinea corporis may present as a unilateral rash.
What are the complications of allergic contact dermatitis?
Allergic contact dermatitis starts as a localised reaction to an allergen in contact with the skin, but severe reactions may generalise due to autoeczematisation, and can lead to erythroderma.
Ingestion of a contact allergen may rarely may lead to baboon syndrome or generalised systemic contact dermatitis.
Photoallergy
Sometimes contact allergy arises only after the skin has been exposed to ultraviolet light. The rash is confined to sun exposed areas even though the allergen may have been in contact with covered areas. This is called photocontact dermatitis.
Examples of photoallergy include:
- Dermatitis due to a sunscreen chemical, affecting the top but not the under surface of the arm
- Dermatitis of face, neck, arms and hands due to antibacterial soap.
How is allergic contact dermatitis diagnosed?
Sometimes it is easy to recognise contact allergy and no specific tests are necessary. Taking a very good history including information on work environment, hobbies, products in use at home and work and sun exposure will enhance the chances of finding a diagnosis. The rash usually (but not always) completely clears up if the allergen is no longer in contact with the skin, but recurs even with slight contact with it again.
The open application test is used to confirm contact allergy to a cosmetic, such as a moisturiser. The product under suspicion is applied several times daily for several days to a small area of sensitive skin. The inner aspect of the upper arm is suitable. Contact allergy is likely if dermatitis arises in the treated area.
Dermatologists will perform patch tests in patients with suspected contact allergy, particularly if the reaction is severe, recurrent or chronic. The tests can identify the specific allergen causing the rash.
Fungal scrapings of skin for microscopy and culture can exclude a fungal infection.
Dimethylgloxime test is available to ‘spot test’ if a product contains nickel.
What is the treatment for allergic contact dermatitis?
It is important to recognise how you are in contact with the responsible substance so that, where possible, you can avoid it.
- Find out precisely what you are allergic to by having comprehensive patch tests.
- Identify where the allergen is found, thus read labels of all products before use.
- Carefully study your environment to locate the allergen. Note: many chemicals have several names, and cross-reactions to similar chemicals with different names are common.
- Wear appropriate gloves to protect hands from touching materials to which you react and remove gloves in the appropriate way. Some chemicals will penetrate certain gloves; seek a safety expert’s advice.
- Ask your dermatologist to help.
Active dermatitis is usually treated with the following:
- Emollient creams
- Topical steroids
- Topical or oral antibiotics for secondary infection
- Oral steroids, usually short courses, for severe cases
- Phototherapy or photochemotherapy.
- Azathioprine, ciclosporin or other immunosuppressive agent.
- Tacrolimus ointment and pimecrolimus cream are immune modulating drugs that inhibit calcineurin and may prove helpful for allergic contact dermatitis.
What is the outcome for allergic contact dermatitis?
Contact allergy often persists lifelong so it is essential to identify the allergen and avoid touching it. Dermatitis may recur on re-exposure to the allergen.
Some allergens are more difficult to avoid than others, with airborne allergens being a particular problem (eg epoxy resin, compositae pollen).
The longer a person suffers from severe allergic contact dermatitis, the longer it will take to clear after the diagnosis is made and the cause detected.
The dermatitis may clear up on avoidance of contact with the allergen, but sometimes it persists indefinitely, eg chromate allergy.
Prognosis depends on patient education and compliance in avoiding allergens and appropriate skin care.
- Eczema. https://medlineplus.gov/eczema.html[↩]
- Wollenberg A, Zoch C, Wetzel S, Plewig G, Przybilla B. Predisposing factors and clinical features of eczema herpeticum: a retrospective analysis of 100 cases. J Am Acad Dermatol 2003;49(2):198-205.[↩]
- Braun-Falco, O., Plewig, G., Wolff, H.H., & Burgdorf, W.H.C. (2000). Dermatology (2nd ed.). Berlin: Springer.[↩][↩]
- Kaposi varicelliform eruption. McKenna J, Krusinski P. 2002. Available from: www.emedicine.com/derm/topic204.htm[↩]
- Fitzpatrick JE, Aeling JL. (2001) Dermatology Secrets in Color (2nd ed.). Philadelphia: Hanley & Belfus.[↩]
- Wollenberg A, Zoch C, Wetzel S, Plewig G, Przybilla B. Predisposing factors and clinical features of eczema herpeticum-a retrospective analysis of 100 cases. J Amer Acad Dermatol 2003; 49:198-205.[↩]
- Kaposi varicelliform eruption (eczema herpeticum). https://escholarship.org/uc/item/9dr4c02z[↩]
- Stanley JR. Pemphigus. In : Wolff K, Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell D J, editors. Fitzpatrick’s Dermatology in General Medicine. 7th ed. New York: McGraw-Hill publications; 2008. 459-67[↩]
- Miller JL, Hurley HJ. Diseases of the Eccrine and Apocrine Sweat Glands. In: Bolognia JL, Jorizzo JL, Rapini RP, editors. Dermatology. 2nd ed. Spain : Mosby Elsvier limited; 2008.[↩]
- Doshi DN, Kimball AB. Vescicular palmoplantar eczema. In : Wolff K, Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell D J, editors. Fitzpatrick’s Dermatology in General Medicine. 7th ed. New York: McGraw-Hill publications; 2008. 162-6 [↩]





{kind=link}