
Contents
What is ehrlichiosis
Ehrlichiosis is the general name used to describe several bacterial diseases transmitted by ticks that affect animals and humans. The signs and symptoms of ehrlichiosis range from mild body aches to severe fever and usually appear within a week or two of a tick bite. If treated quickly with appropriate antibiotics, ehrlichiosis generally improves within a few days.
Human ehrlichiosisis a disease caused by at least three different ehrlichial species in the United States:
- Ehrlichia chaffeensis,
- Ehrlichia ewingii, and
- Ehrlichia species provisionally called Ehrlichia muris-like.
Ehrlichia bacteria are transmitted to humans by the bite of an infected tick. The lone star tick (Amblyomma americanum) is the primary vector of both Ehrlichia chaffeensis and Ehrlichia ewingii in the United States. Typical symptoms include: fever, headache, fatigue, and muscle aches. Usually, these symptoms occur within 1-2 weeks following a tick bite. The severity of ehrlichiosis may depend in part on the immune status of the patient. Persons with compromised immunity caused by immunosuppressive therapies (e.g., corticosteroids , cancer chemotherapy, or longterm immunosuppressive therapy following organ transplant), HIV infection, or splenectomy appear to develop more severe disease, and may also have higher case-fatality rates (i.e. the proportion of patients that die from infection). Because Ehrlichia organisms infect the white blood cells and circulate in the blood stream, these pathogens may pose a risk to be transmitted through blood transfusions. Ehrlichia chaffeensis has been shown to survive for more than a week in refrigerated blood. Several instances of suspected E. chaffeensis transmission through solid organ transplant have been investigated, although to date no cases have been confirmed that can be attributed to this route of transmission. Patients who develop ehrlichiosis within a month of receiving a blood transfusion or solid organ transplant should be reported to state health officials for prompt investigation. Use of leukoreduced blood products may theoretically decrease the risk of transfusion-associated transmission of these pathogens. However, the filtration process does not remove all leukocytes or bacteria not associated with leukocytes from leukoreduced blood; therefore, this process may not eliminate the risk completely.
Ehrlichios is diagnosed based on symptoms, clinical presentation, and later confirmed with specialized laboratory tests. The first line treatment for adults and children of all ages is doxycycline. Ehrlichiosis and other tickborne diseases can be prevented.
Ehrlichiosis is caused by bacteria that belong to the family called rickettsiae. Rickettsial bacteria cause a number of serious diseases worldwide, including Rocky Mountain spotted fever and typhus. All of these diseases are spread to humans by a tick, flea, or mite bite.
Scientists first described ehrlichiosis in 1986. There are two types of the disease in the United States:
- Human monocytic ehrlichiosis is caused by the rickettsial bacteria Ehrlichia chaffeensis.
- Human granulocytic ehrlichiosis is also called human granulocytic anaplasmosis (HGA). It is caused by the rickettsial bacteria called Anaplasma phagocytophilum
Ehrlichia chaffeensis bacteria can be carried by the:
- American dog tick
- Deer tick (Ixodes scapularis), which can also cause Lyme disease
- Lone Star tick
In the United States, human monocytic ehrlichiosis is found mainly in the southern central states and the Southeast. Human granulocytic ehrlichiosis is found mainly in the Northeast and upper Midwest.
Risk factors for ehrlichiosis include:
- Living near an area with a lot of ticks
- Owning a pet that may bring a tick home
- Walking or playing in high grasses
Ehrlichia chaffeensis, the cause of human monocytic ehrlichiosis, was described first in 1986 and is the most common agent of human ehrlichiosis. Ehrlichia ewingii was reported as a human pathogen in 1999 after being detected in peripheral blood leukocytes of four patients with illness during 1996–1998 1. Ehrlichia muris-like agent ehrlichiosis, first described in 2011, is the most recently recognized form of human ehrlichiosis in the United States and was detected originally in the blood of four patients from Minnesota and Wisconsin in 2009 2.
During 2008–2012, the average annual incidence of ehrlichiosis was 3.2 cases per million persons, which is more than twice the estimated incidence during 2000–2007 3. Cases have been reported from an increasing number of counties 3 (see Figure 1). Incidence generally increases with age, with the highest age-specific incidences occurring among persons aged 60–69 years (5,13,50). Case-fatality rates are highest among children aged <10 years and adults aged ≥70 years, and an increased risk for death has been documented among persons who are immunosuppressed 3. In areas where ehrlichiosis is endemic, the actual disease incidence is likely underrepresented in estimates that are based on passive surveillance 4.
Figure 1. Reported incidence rate* of Ehrlichia chaffeensis ehrlichiosis, by county — United States, 2000–2013 (* As reported through national surveillance, per 1,000,000 persons per year. Cases are reported by county of residence, which is not always where the infection was acquired)
Ehrlichia chaffeensis
Ehrlichia chaffeensis is transmitted to humans by the lone star tick, Amblyomma americanum (see Figures 4 and 5 below). The lone star tick is among the most commonly encountered ticks in the southeastern United States, with a range that extends into areas of the Midwest and New England states. Ehrlichiosis cases have been reported throughout the range of the lone star tick; states with the highest reported incidence rates include Arkansas, Delaware, Missouri, Oklahoma, Tennessee, and Virginia 3. The white-tailed deer is a major host of all stages of lone star ticks and is thought to be an important natural reservoir for Ehrlichia chaffeensis 5. Consequently, the lone star tick is found most commonly in woodland habitats that have white-tailed deer populations. The lone star tick feeds on a wide range of hosts, including humans, and has been implicated as the most common tick to bite humans in the southern United States 6. Although all stages of this tick feed on humans, only adult and nymphal ticks are known to be responsible for transmission of Ehrlichia chaffeensis to humans. Most cases of Ehrlichia chaffeensis ehrlichiosis occur during May–August.
Ehrlichia ewingii
Ehrlichia ewingii ehrlichiosis became a notifiable disease in 2008. During 2008–2012, cases were primarily reported from Missouri; however, cases also were reported from 10 other states within the distribution of the principal vector, the lone star tick, Amblyomma americanum 3 (see Figures 4 and 5 below). Although Ehrlichia ewingii ehrlichiosis initially was reported predominantly among persons who were immunosuppressed, passive surveillance data from 2008–2012 indicated that the majority of persons (74%) with reported Ehrlichia ewingii infection did not report immunosuppression 3. No fatal cases of Ehrlichia ewingii ehrlichiosis have been reported. The ecologic features of Ehrlichia ewingii are not completely known; however, dogs, goats, and deer have been infected naturally and experimentally 7.
Ehrlichia muris-Like Agent
In 2011, a new species of Ehrlichia referred to as the EML agent was described as a human pathogen after detection in the blood from four patients (three from Wisconsin and one from Minnesota) by using molecular testing techniques 2. The Ehrlichia muris-like agent subsequently was identified in blood specimens from 69 symptomatic patients who lived in or were exposed to ticks in Minnesota or Wisconsin during 2007‒2013 8. The blacklegged tick, Ixodes scapularis (Figure 3), is an efficient vector for the Ehrlichia muris-like agent in experimental studies 9, and DNA from the Ehrlichia muris-like agent has been detected from I. scapularis collected in Minnesota and Wisconsin but has not been detected in Ixodes scapularis from other states 10.
Ehrlichiosis long term effects
Without prompt treatment, ehrlichiosis can have serious effects on an otherwise healthy adult or child.
People with weakened immune systems are at an even higher risk of more-serious and potentially life-threatening consequences. Serious complications of untreated infection include:
- Kidney failure
- Respiratory failure
- Heart failure
- Seizures
- Coma
Figure 2. American dog tick (a male brown dog tick – Rhipicephalus sanguineus)

Figure 3. Deer tick (female Ixodes scapularis)

Figure 4. Lone Star tick (female Amblyomma americanum)

Figure 5. Lone Star tick (engorged female Amblyomma americanum) – An engorged female of this species can lay approximately 2000-2500 eggs.

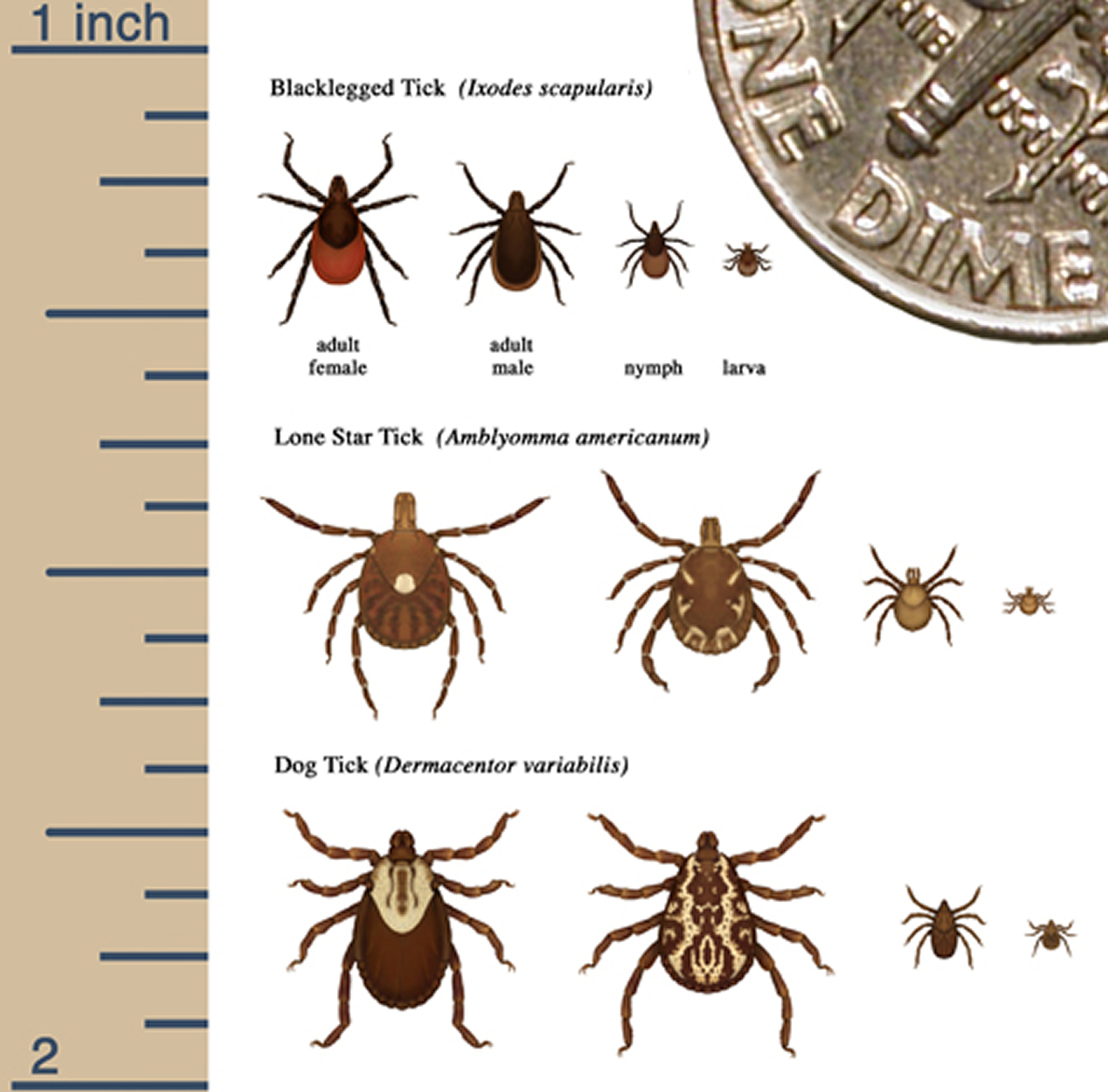
Figure 6. Relative sizes of several ticks at different life stages
Ehrlichiosis causes
Ehrlichiosis is caused by ehrlichia bacteria and is transmitted primarily by the Lone Star tick.
Ticks feed on blood, latching onto a host and feeding until they’re swollen to many times their normal size. During feeding, ticks that carry disease-producing bacteria can transmit the bacteria to a healthy host. Or they may pick up bacteria themselves if the host, such as a white-tailed deer or a coyote, is infected.
Usually, to get ehrlichiosis, you must be bitten by an infected tick. The bacteria enter your skin through the bite and eventually make their way into your bloodstream.
Before bacteria can be transmitted, a tick must be attached and feeding for at least 24 hours. An attached tick with a swollen appearance may have been feeding long enough to have transmitted bacteria. Removing ticks as soon as possible may prevent infection.
It’s also possible that ehrlichiosis may be transmitted through blood transfusions, from mother to fetus, and through direct contact with an infected, slaughtered animal.
Risk factors for ehrlichiosis
Ehrlichiosis spreads when an infected tick, primarily the Lone Star tick, bites you and feeds on you for 24 hours or longer. The following factors may increase your risk of getting tick-borne infections:
- Being outdoors in warm weather. Most cases of ehrlichiosis occur in the spring and summer months when populations of the Lone Star tick are at their peak, and people are outside more often.
- Living in or visiting an area with a high tick population. You are at greater risk if you are in an area with a high Lone Star tick population. In the United States, Lone Star ticks are most common in southeastern, eastern and south-central states.
- Being male. Ehrlichiosis infections are more common in males, possibly because of increased time outdoors for work and recreation.
Preventing tick bites
While it is a good idea to take preventive measures against ticks year-round, be extra cautious in warmer months (April-September) when ticks are most active and know which ticks are most common in your area.
Most ticks attach themselves to your lower legs and feet as you walk or work in grassy, wooded areas or overgrown fields. After a tick attaches to your body, it usually crawls upward to find a location to burrow into your skin. You may find a tick on the back of your knees, groin, underarms, ears, back of your neck and elsewhere.
If you remove a tick in the first 24 hours after attachment, you reduce your risk of infection. While you may not be able to avoid going into areas where ticks are present, the following tips can make it easier to discover and remove ticks before they attach to your skin.
How ticks survive
Most ticks go through four life stages: egg, six-legged larva, eight-legged nymph, and adult. After hatching from the eggs, ticks must eat blood at every stage to survive. Ticks that require this many hosts can take up to 3 years to complete their full life cycle, and most will die because they don’t find a host for their next feeding.
Although some tick species, like the brown dog tick, prefer to feed on the same host during all life stages. Ticks can feed on mammals, birds, reptiles, and amphibians. Most ticks prefer to have a different host animal at each stage of their life, as shown below:
Figure 7. Lifecyle of dog ticks
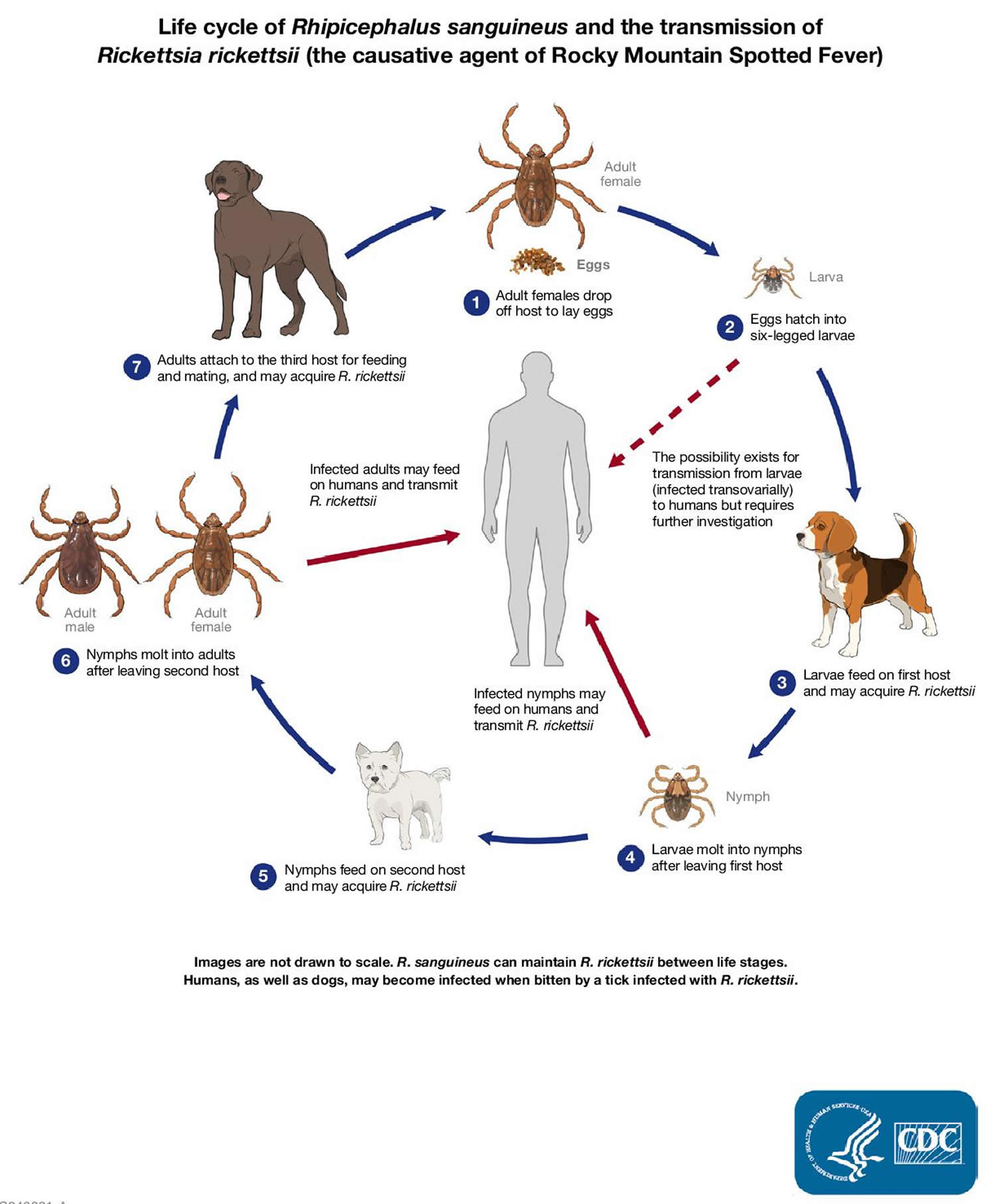
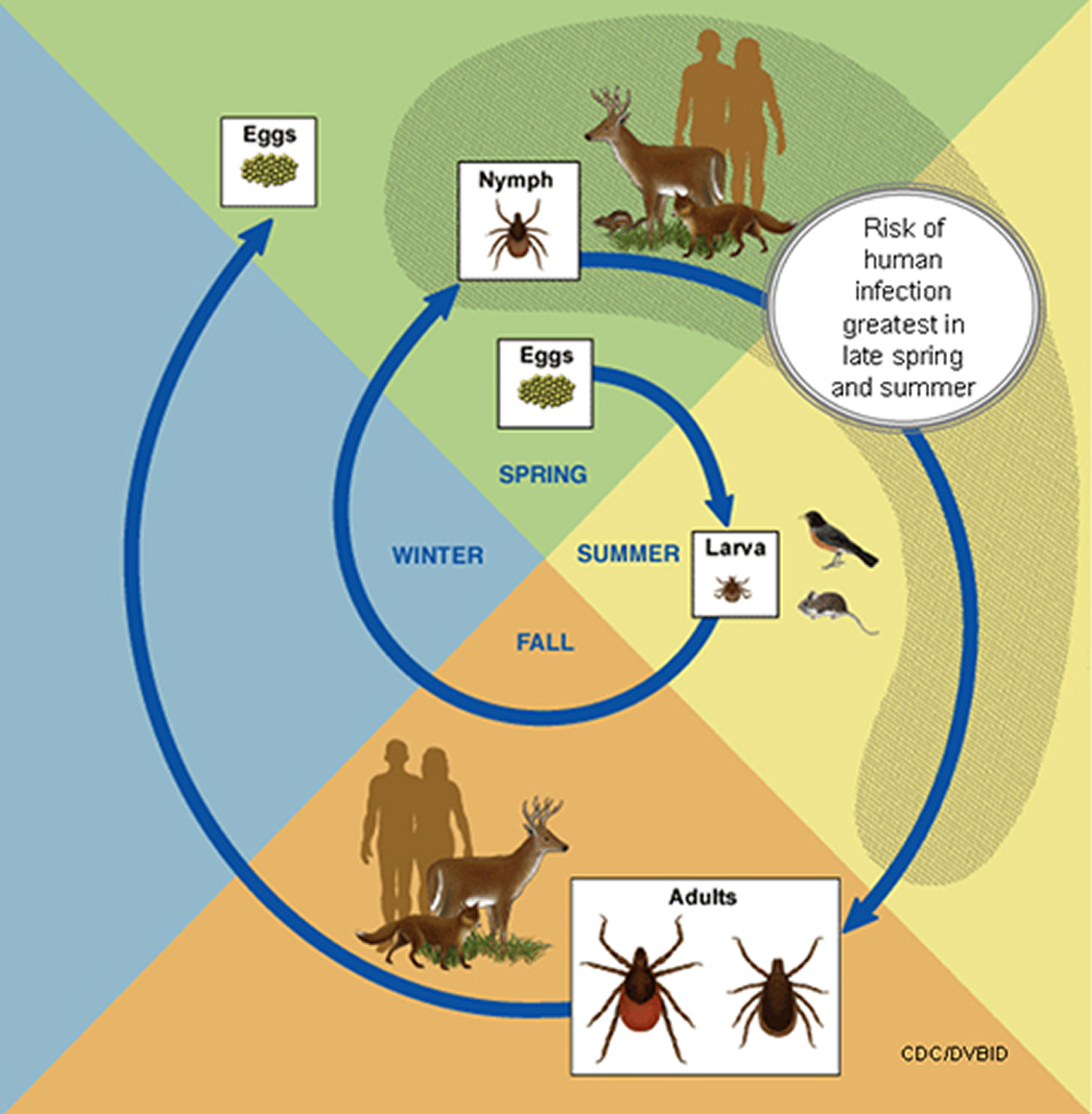
Figure 8. Life cycle of blacklegged ticks
How ticks find their hosts
Ticks find their hosts by detecting animals´ breath and body odors, or by sensing body heat, moisture, and vibrations. Some species can even recognize a shadow. In addition, ticks pick a place to wait by identifying well-used paths. Then they wait for a host, resting on the tips of grasses and shrubs. Ticks can’t fly or jump, but many tick species wait in a position known as “questing”.
While questing, ticks hold onto leaves and grass by their third and fourth pair of legs. They hold the first pair of legs outstretched, waiting to climb on to the host. When a host brushes the spot where a tick is waiting, it quickly climbs aboard. Some ticks will attach quickly and others will wander, looking for places like the ear, or other areas where the skin is thinner.
How ticks spread disease
Ticks transmit pathogens that cause disease through the process of feeding.
- Depending on the tick species and its stage of life, preparing to feed can take from 10 minutes to 2 hours. When the tick finds a feeding spot, it grasps the skin and cuts into the surface.
- The tick then inserts its feeding tube. Many species also secrete a cement-like substance that keeps them firmly attached during the meal. The feeding tube can have barbs which help keep the tick in place.
- Ticks also can secrete small amounts of saliva with anesthetic properties so that the animal or person can’t feel that the tick has attached itself. If the tick is in a sheltered spot, it can go unnoticed.
- A tick will suck the blood slowly for several days. If the host animal has a bloodborne infection, the tick will ingest the pathogens with the blood.
- Small amounts of saliva from the tick may also enter the skin of the host animal during the feeding process. If the tick contains a pathogen, the organism may be transmitted to the host animal in this way.
- After feeding, most ticks will drop off and prepare for the next life stage. At its next feeding, it can then transmit an acquired disease to the new host.
Avoid Direct Contact with Ticks
- Avoid wooded and brushy areas with high grass and leaf litter.
- Walk in the center of trails.
Repel Ticks on Skin and Clothing
- Use repellent that contains 20 percent or more DEET, picaridin, or IR3535 on exposed skin for protection that lasts several hours.
- Always follow product instructions. Parents should apply this product to their children, avoiding hands, eyes, and mouth.
- Use products that contain permethrin on clothing. Treat clothing and gear, such as boots, pants, socks and tents with products containing 0.5% permethrin. It remains protective through several washings. Pre-treated clothing is available and may be protective longer.
- The Environmental Protection Agency (EPA) has an online tool (https://www.epa.gov/insect-repellents/find-repellent-right-you) to help you select the repellent that is best for you and your family.
- Wear light-colored clothing. Ticks are dark-colored. Light clothing helps you and others notice ticks on your clothing before they can attach themselves to your skin.
- Avoid open-toed shoes or sandals. Ticks generally live in grassy areas or fields and can attach themselves to your feet and legs when you brush by. Wearing open-toed shoes or sandals increases the risk of a tick attaching to your bare skin and working its way under your clothes, out of sight from detection.
- Wear long pants and a long-sleeved shirt. The less skin you expose, the less area a tick has to bite. For added protection, wear shirts, pants and socks with permethrin impregnated in the fabric.
- Tuck your shirt into your pants and your pants into your socks. By doing this, ticks will be less able to crawl onto exposed skin. However, be aware that if ticks get on your clothing, they’ll climb upward until they reach exposed skin. Check your clothing often while you’re outdoors.
- Stay on clear trails whenever possible. Ticks prefer grassy areas and may be less common on well-beaten paths.
- Inspect your body. Do a complete visual inspection of your body. Be sure to check your head and neck because ticks will continue to climb upward until they find a suitable burrowing site. Use your hands to feel through your hair and in areas you can’t see when you return from your outing or garden. Ticks can be as small as a strawberry seed, and they usually attach to hidden skin. Be sure to check all the possibilities. A shower alone will rarely dislodge attached ticks from your head and body.
- Inspect your clothes and gear. Check your clothes, backpacks and other gear when you get home to look for ticks that hitched a ride. Spinning your clothes in the dryer for about an hour will kill any ticks you missed.
- Don’t forget your pets. Do a daily inspection for ticks on any pet that spends time outdoors.
Find and Remove Ticks from Your Body
- Bathe or shower as soon as possible after coming indoors (preferably within two hours) to wash off and more easily find ticks that are crawling on you.
- Conduct a full-body tick check using a hand-held or full-length mirror to view all parts of your body upon return from tick-infested areas. Parents should check their children for ticks under the arms, in and around the ears, inside the belly button, behind the knees, between the legs, around the waist, and especially in their hair.
- Examine gear and pets. Ticks can ride into the home on clothing and pets, then attach to a person later, so carefully examine pets, coats, and day packs.
- Tumble dry clothes in a dryer on high heat for 10 minutes to kill ticks on dry clothing after you come indoors.
- If the clothes are damp, additional time may be needed.
- If the clothes require washing first, hot water is recommended. Cold and medium temperature water will not kill ticks effectively. If the clothes cannot be washed in hot water, tumble dry on low heat for 90 minutes or high heat for 60 minutes. The clothes should be warm and completely dry.
Tick Removal
If you find a tick attached to your skin, there’s no need to panic. There are several tick removal devices on the market, but a plain set of fine-tipped tweezers will remove a tick quite effectively.
If you develop a rash or fever within several weeks of removing a tick, see your doctor. Be sure to tell the doctor about your recent tick bite, when the bite occurred, and where you most likely acquired the tick.
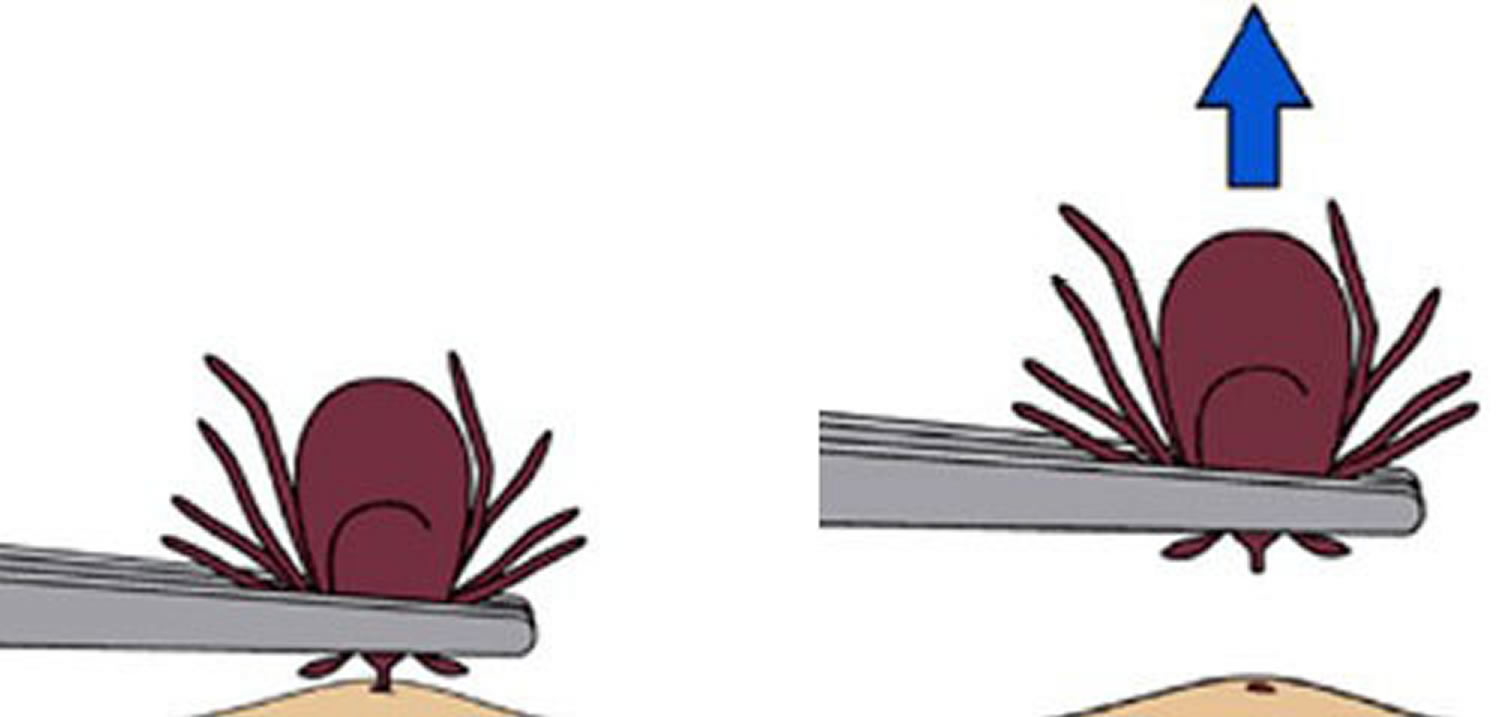
How to remove a tick
- Use fine-tipped tweezers to grasp the tick as close to the skin’s surface as possible.
- Pull upward with steady, even pressure. Don’t twist or jerk the tick; this can cause the mouth-parts to break off and remain in the skin. If this happens, remove the mouth-parts with tweezers. If you are unable to remove the mouth easily with clean tweezers, leave it alone and let the skin heal.
- After removing the tick, thoroughly clean the bite area and your hands with rubbing alcohol, an iodine scrub, or soap and water.
- Dispose of a live tick by submersing it in alcohol, placing it in a sealed bag/container, wrapping it tightly in tape, or flushing it down the toilet. Never crush a tick with your fingers.
- AVOID folklore remedies such as “painting” the tick with nail polish or petroleum jelly, or using heat to make the tick detach from the skin. Your goal is to remove the tick as quickly as possible–not waiting for it to detach.
Figure 9. How to remove a tick
Ehrlichiosis symptoms
In the United States, the term “ehrlichiosis” may be broadly applied to several different infections. Ehrlichia chaffeensis and Ehrlichia ewingii are transmitted by the lonestar tick in the southeastern and southcentral United States. In addition, a third Ehrlichia species provisionally called Ehrlichia muris-like has been identified in a small number of patients residing in or traveling to Minnesota and Wisconsin; a tick vector for the Ehrlichia muris-like organism has not yet been established.
If a tick carrying the bacterium that causes ehrlichiosis has been feeding on you for at least 24 hours, the following flu-like signs and symptoms may appear — usually within seven to 14 days of the bite. The tick bite is usually painless, and about half of the people who develop ehrlichiosis may not even remember being bitten by a tick.
Some people infected with ehrlichiosis may have symptoms so mild that they never seek medical attention, and the body fights off the illness on its own. But untreated ehrlichiosis with persistent symptoms can result in an illness serious enough to require hospitalization.
The following is a list of symptoms commonly seen with this disease, however, it is important to note that the combination of symptoms varies greatly from person to person.
- Mild fever
- Fatigue
- Loss of appetite
- Joint pain
- Confusion
- Cough
- Headache
- Chills
- Malaise
- Muscle pain
- Nausea / Vomiting / Diarrhea
- Confusion
- Conjunctival injection (red eyes)
- Rash (in up to 60% of children, less than 30% of adults)
Ehrlichiosis is a serious illness that can be fatal if not treated correctly, even in previously healthy people. Severe clinical presentations may include difficulty breathing, or bleeding disorders. The estimated case fatality rate (i.e. the proportion of persons who die as a result of their infection) is 1.8%. Patients who are treated early may recover quickly on outpatient medication, while those who experience a more severe course may require intravenous antibiotics, prolonged hospitalization or intensive care.
Ehrlichiosis rash
Skin rash is not considered a common feature of ehrlichiosis, and should not be used to rule in or rule out an infection. The rash appears from day 0 to day 13 of the illness. Ehrlichia chaffeensis infection can cause a rash in up to 60% of children, but is reported in fewer than 30% of adults (skin rash varies between 20 to 88% of cases). When present, the rash takes various forms. Rash is not commonly reported in patients infected with Ehrlichia ewingii or the Ehrlichia muris-like organism. The rash associated with Ehrlichia chaffeensis infection may range from maculopapular (macular = flat discolorations; papular = small lumps) to petechial (small red or purple spots due to bleeding into the skin) in nature, and is usually not pruritic (itchy). Less commonly, lesions are described as blistering, nodular (larger solid lumps), vasculitic, purpuric, mottled, blotchy, crusted, or ulcerated. The rash usually spares the face, but in some cases may spread to the palms and soles. A type of rash called erythroderma may develop in some patients. Erythroderma is a type of rash that resembles a sunburn and consists of widespread reddening of the skin that may peel after several days. In severe cases, a widespread rash and desquamation (shedding of the skin in scales) can fit criteria for toxic shock syndrome. Some patients may develop a rash that resembles the rash of Rocky Mountain spotted fever making these two diseases difficult to differentiate on the basis of clinical signs alone.
Figure 10. Ehrlichiosis rash (erythematous maculopapular rash without distinct margins)

Figure 11. Ehrlichiosis rash (multiple erythematous papules on a 51-year-old woman seen 5 days after her exposure to wooded area)

Ehrlichiosis diagnosis
The diagnosis of ehrlichiosis must be made based on clinical signs and symptoms, and can later be confirmed using specialized confirmatory laboratory tests. Treatment should never be delayed pending the receipt of laboratory test results, or be withheld on the basis of an initial negative laboratory result.
Clinical Diagnosis
There are several aspects of ehrlichiosis that make it challenging for healthcare providers to diagnose and treat. The symptoms vary from patient to patient and can be difficult to distinguish from other diseases. Treatment is more likely to be effective if started early in the course of disease. Diagnostic tests based on the detection of antibodies will frequently be negative in the first 7-10 days of illness.
For this reason, healthcare providers must use their judgment to treat patients based on clinical suspicion alone. Healthcare providers may find important information in the patient’s history and physical examination that may aid clinical suspicion. Information such as recent tick bites, exposure to areas where ticks are likely to be found, or history of recent travel to areas where ehrlichiosis is endemic can be helpful in making the diagnosis. The healthcare provider should also look at routine blood tests, such as a complete blood cell count or a chemistry panel. Clues such as a low platelet count (thrombocytopenia), low white blood cell count (leukopenia), or elevated liver enzyme levels are helpful predictors of ehrlichiosis, but may not be present in all patients depending on the course of the disease. After a suspect diagnosis is made on clinical suspicion and treatment has begun, specialized laboratory testing should be used to confirm the diagnosis of ehrlichiosis.
Laboratory Detection
During the acute phase of illness, a sample of whole blood can be tested by polymerase chain reaction (PCR) assay to determine if a patient has ehrlichiosis. This method is most sensitive in the first week of illness, and quickly decreases in sensitivity following the administration of appropriate antibiotics. Although a positive polymerase chain reaction (PCR) result is helpful, a negative result does not completely rule out the diagnosis.
During the first week of illness a microscopic examination of blood smears (known as a peripheral blood smear) may reveal morulae (microcolonies of ehrlichiae) in the cytoplasm of white blood cells in up to 20% of patients.
The type of blood cell in which morulae are observed may provide insight into the infecting species: E. chaffeensis most commonly infects monocytes, whereas E. ewingii more commonly infect granulocytes. However, the observance of morulae in a particular cell type cannot conclusively identify the infecting species. Culture isolation of Ehrlichia is only available at specialized laboratories; routine hospital blood cultures cannot detect Ehrlichia.
When a person develops ehrlichiosis, their immune system produces antibodies to the Ehrlichia, with detectable antibody titers usually observed by 7-10 days after illness onset. It is important to note that antibodies are not detectable in the first week of illness in 85% of patients, and a negative test during this time does not rule out ehrlichiosis as a cause of illness.
The gold standard serologic test for diagnosis of ehrlichiosis is the indirect immunofluorescence assay (IFA) using Ehrlichia chaffeensis antigen, performed on paired serum samples to demonstrate a significant (four-fold) rise in antibody titers. The first sample should be taken as early in the disease as possible, preferably in the first week of symptoms, and the second sample should be taken 2 to 4 weeks later. In most cases of ehrlichiosis, the first IgG immunofluorescence assay titer is typically low, or “negative,” and the second typically shows a significant (four-fold) increase in IgG antibody levels. IgM antibodies usually rise at the same time as IgG near the end of the first week of illness and remain elevated for months or longer. Also, IgM antibodies are less specific than IgG antibodies and more likely to result in a false positive. For these reasons, physicians requesting IgM serologic titers should also request a concurrent IgG titer.
Serologic tests based on enzyme immunoassay (EIA) technology are available from some commercial laboratories. However, enzyme immunoassay (EIA) tests are qualitative rather than quantitative, meaning they only provide a positive/negative result, and are less useful to measure changes in antibody titers between paired specimens. Furthermore, some enzyme immunoassay assays rely on the evaluation of IgM antibody alone, which may have a higher frequency of false positive results.
Antibodies to Ehrlichia chaffeensis may remain elevated for months or longer after the disease has resolved, or may be detected in persons who were previously exposed to antigenically related organisms. Up to 12% of currently healthy people in some areas may have elevated antibody titers due to past exposure to Ehrlichia species or similar organisms. Therefore, if only one sample is tested it can be difficult to interpret, while paired samples taken weeks apart demonstrating a significant (four-fold) rise in antibody titer provides the best evidence for a correct diagnosis of ehrlichiosis.
Ehrlichiosis treatment
Doxycycline is the first line treatment for adults and children of all ages and should be initiated immediately whenever ehrlichiosis is suspected.
Use of antibiotics other than doxycycline and other tetracyclines is associated with a higher risk of fatal outcome for some rickettsial infections. Doxycycline is most effective at preventing severe complications from developing if it is started early in the course of disease. Therefore, treatment must be based on clinical suspicion alone and should always begin before laboratory results return.
If the patient is treated within the first 5 days of the disease, fever generally subsides within 24-72 hours. In fact, failure to respond to doxycycline suggests that the patient’s condition might not be due to ehrlichiosis. Severely ill patients may require longer periods before their fever resolves. Resistance to doxcycline or relapses in symptoms after the completion of the recommended course have not been documented.
Recommended Dosage
Doxycycline is the first line treatment for adults and children of all ages:
- Adults: 100 mg every 12 hours
- Children under 45 kg (100 lbs): 2.2 mg/kg body weight given twice a day
Patients should be treated for at least 3 days after the fever subsides and until there is evidence of clinical improvement. Standard duration of treatment is 7 to 14 days. Some patients may continue to experience headache, weakness and malaise for weeks after adequate treatment.
Treating children
The use of doxycycline to treat suspected ehrlichiosis in children is standard practice recommended by both Centers for Disease Control and Prevention (CDC) and the American Academy of Pediatrics Committee on Infectious Diseases. Unlike older generations of tetracyclines, the recommended dose and duration of medication needed to treat ehrlichiosis has not been shown to cause staining of permanent teeth, even when five courses are given before the age of eight. Healthcare providers should use doxycycline as the first-line treatment for suspected ehrlichiosis in patients of all ages.
Other Treatments
In cases of life threatening allergies to doxycycline and in some pregnant patients for whom the clinical course of ehrlichiosis appears mild, physicians may need to consider alternate antibiotics. Although recommended as a second-line therapeutic alternative to treat Rocky Mountain spotted fever, chloramphenicol is not recommended for the treatment of either ehrlichiosis or anaplasmosis, as studies have shown a lack of efficacy. Rifampin appears effective against Ehrlichia in laboratory settings. However, rifampin is not effective in treating Rocky Mountain spotted fever, a disease that may be confused with ehrlichiosis. Healthcare providers should be cautious when exploring treatments other than doxycycline, which is highly effective in treating both. Other antibiotics, including broad spectrum antibiotics are not considered highly effective against ehrlichiosis, and the use of sulfa drugs during acute illness may worsen the severity of infection.
Prophylaxis (Preventive Treatment)
Antibiotic treatment following a tick bite is not recommended as a means to prevent ehrlichiosis. There is no evidence this practice is effective, and this may simply delay onset of disease. Instead, persons who experience a tick bite should be alert for symptoms suggestive of tickborne illness and consult a physician if fever, rash, or other symptoms of concern develop.
Home remedies
If you find a tick on your body, don’t be alarmed. If you remove the tick within 24 hours of its attachment, it’s unlikely you’ll get ehrlichiosis or other tick-borne illnesses. Follow these steps for safe removal of ticks:
- Use tweezers if possible. Use a pair of flat-tipped tweezers or cover your hand with a tissue or glove to remove a tick. A tick’s saliva and bodily fluids can carry the same bacterium that’s found in its mouth and the bacterium can enter your body through cuts or mucous membranes in your skin. Remove the tick slowly. Grab the tick by its mouth parts where it has attached to your skin. Pull it up and out of your skin steadily and slowly without jerking or twisting it. If you pull too quickly or grab the tick by its body, the tick will likely separate, leaving the mouth parts in your skin. If the tick’s mouth parts do break off in your skin, remove them with tweezers. Petroleum jelly and hot matches are not effective treatments for removing ticks or tick parts from your skin. These methods may make matters worse by triggering the tick to release more of its bodily fluids, and that could cause further infection.
- Kill the tick. Once you have successfully removed the tick, kill it by placing it in a container with rubbing alcohol in it. Don’t crush the tick in your hands or with your fingernails because the fluids it releases may contain infected bacteria. If you want to save the tick for testing in the event you become ill, put it in a plastic bag or a jar, date the container and place it in the freezer.
- Clean the bite site. Wash the bite site thoroughly with hand antiseptic or soap and water. And, thoroughly wash your hands.
- Monitor the bite site. In the following days and weeks, watch the bite site for a rash and pay close attention to any signs and symptoms that develop such as fever, muscle aches or joint pain. If you notice anything out of the ordinary, see your doctor. If possible, bring the tick with you to your appointment.
- Buller RS, Arens M, Hmiel SP, et al. Ehrlichia ewingii, a newly recognized agent of human ehrlichiosis. N Engl J Med 1999;341:148–55. http://www.nejm.org/doi/10.1056/NEJM199907153410303[↩]
- Pritt BS, Sloan LM, Johnson DK, et al. Emergence of a new pathogenic Ehrlichia species, Wisconsin and Minnesota, 2009. N Engl J Med 2011;365:422–9. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3319926/[↩][↩]
- Nichols KH, Dahlgren FS, Drexler NA, Massung RF, Behravesh CB. Increasing incidence of ehrlichiosis in the United States: a summary of national surveillance of Ehrlichia chaffeensis and Ehrlichia ewingii infections in the United States, 2008–2012. Am J Trop Med Hyg 2016;94:52–60. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4710445/[↩][↩][↩][↩][↩][↩]
- Olano JP, Masters E, Hogrefe W, Walker DH. Human monocytotropic ehrlichiosis, Missouri. Emerg Infect Dis 2003;9:1579–86. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3034327/[↩]
- Paddock CD, Yabsley MJ. Ecological havoc, the rise of white-tailed deer, and the emergence of Amblyomma americanum-associated zoonoses in the United States. Curr Top Microbiol Immunol 2007;315:289–324. https://www.ncbi.nlm.nih.gov/pubmed/17848069[↩]
- Merten HA, Durden LA. A state-by-state survey of ticks recorded from humans in the United States. J Vector Ecol 2000;25:102–13. https://www.ncbi.nlm.nih.gov/pubmed/10925803[↩]
- Loftis AD, Levin ML, Spurlock JP. Two USA Ehrlichia spp. cause febrile illness in goats. Vet Microbiol 2008;130:398–402. https://www.ncbi.nlm.nih.gov/pubmed/18328644[↩]
- Johnson DKH, Schiffman EK, Davis JP, et al. Human infection with Ehrlichia muris-like pathogen, United States, 2007–2013. Emerg Infect Dis 2015;21:1794–9. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4593436/[↩]
- Karpathy SE, Allerdice MEJ, Sheth M, Dasch GA, Levin ML. Co-feeding transmission of the Ehrlichia muris-like agent (EMLA) to mice (Mus musculus). Vector Borne Zoonotic Dis 2016;16:145–50 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4809518/[↩]
- Stromdahl E, Hamer S, Jenkins S, et al. Comparison of phenology and pathogen prevalence, including infection with the Ehrlichia muris-like (EML) agent, of Ixodes scapularis removed from soldiers in the Midwestern and the northeastern United States over a 15 year period (1997–2012). Parasit Vectors 2014;7:553. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4265324/[↩]





{kind=link}