Contents
- What is electrolyte imbalance
- Body Fluid Compartments and Fluid Homeostasis
- Sources of Body Water Gain and Loss
- Regulation of Electrolyte and Water Loss
- Disorders of Fluid Balance
- What causes electrolyte imbalance
- Dehydration
- Illness
- Sweating
- Alcohol
- Diabetes
- Increased urination
- Who Is at Risk of Dehydration ?
- What are symptoms and signs of dehydration ?
- Table 3. Signs of dehydration in Adults
- Some of the early warning signs of dehydration in adults include 16, 17, 18:
- Signs of severe dehydration in adults 16:
- A baby or a young child may be dehydrated if they 16, 17, 18:
- Table 4. Symptoms and signs of clinical dehydration and shock in Children (Under 5 years)
- Electrolyte imbalance treatment
- Complications of Dehydration
- What is Diabetes insipidus
- Dehydration
What is electrolyte imbalance
Electrolytes are minerals in your body that have an electric charge. They are in your blood, urine, tissues, and other body fluids. Electrolytes are important because they help
- Balance the amount of water in your body
- Balance your body’s acid/base (pH) level
- Move nutrients into your cells
- Move wastes out of your cells
- Make sure that your nerves, muscles, the heart, and the brain work the way they should
Sodium, calcium, potassium, chlorine, phosphate, and magnesium are all electrolytes. You get them from the foods you eat and the fluids you drink.
The levels of electrolytes in your body can become too low or too high. This can happen when the amount of water in your body changes. The amount of water that you take in should equal the amount you lose. If something upsets this balance, you may have too little water (dehydration) or too much water (overhydration). Some medicines, vomiting, diarrhea, sweating, and liver or kidney problems can all upset your water balance.
Treatment helps you to manage the imbalance. It also involves identifying and treating what caused the imbalance.
Body Fluid Compartments and Fluid Homeostasis
A body fluid is usually a liquid that is produced by the body and consists of water and dissolved solutes. In lean adults, body fluids constitute between 55% and 60% of total body mass in females and males, respectively (Figure 1).
Body fluids are present in two main “compartments”—inside cells and outside cells.
Body Fluid Composition
- Intracellular fluid (ICF): About two-thirds of body fluid is intracellular fluid (intra- = within) or cytosol, the fluid within cells has high concentrations of potassium, phosphate, and magnesium ions. It includes a greater concentration of sulfate ions and lesser concentrations of sodium, chloride, calcium, and bicarbonate ions than does extracellular fluid. Intracellular fluid also has a greater concentration of protein than does plasma. Figure 3 shows these relative concentrations.
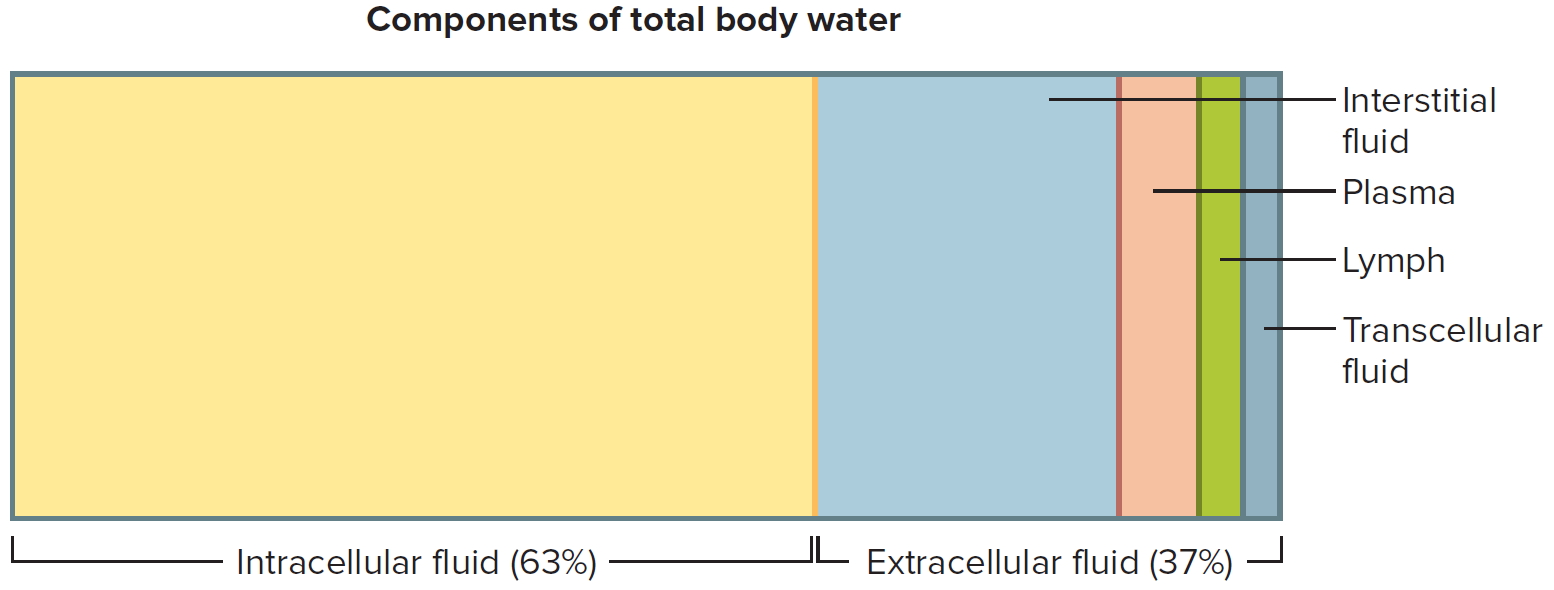
- Extracellular fluids (ECF): The other third, called extracellular fluid (ECF) (extra- = outside), is outside cells and includes all other body fluids. Extracellular fluid (ECF) generally are similar in composition, including high concentrations of sodium, chloride, calcium, and bicarbonate ions and lesser concentrations of potassium, magnesium, phosphate, and sulfate ions. The blood plasma portion of extracellular fluid has considerably more protein than does either interstitial fluid or lymph. About 80% of the ECF is interstitial fluid (inter- =between), which occupies the microscopic spaces between tissue cells, and 20% of the extracellular fluid (ECF) is blood plasma, the liquid portion of the blood. Other extracellular fluids that are grouped with interstitial fluid include lymph in lymphatic vessels; cerebrospinal fluid in the nervous system; synovial fluid in joints; aqueous humor and vitreous body in the eyes; endolymph and perilymph in the ears; and pleural, pericardial, and peritoneal fluids between serous membranes.
Figure 1. Body fluid compartments
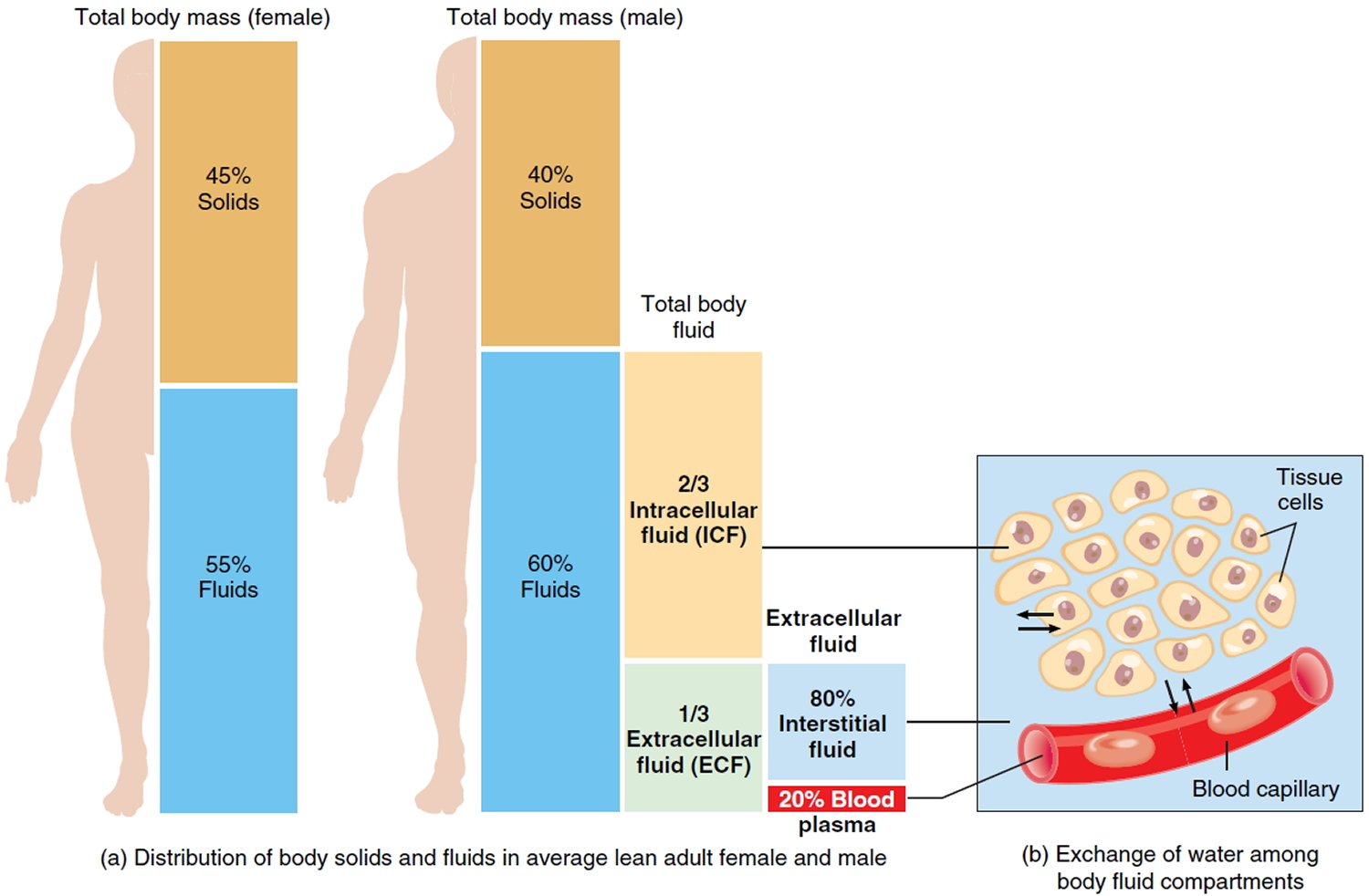
Figure 2. Components of total body water
Two general “barriers” separate intracellular fluid, interstitial fluid, and blood plasma.
- The plasma membrane of individual cells separates intracellular fluid from the surrounding interstitial fluid. The plasma membrane is a selectively permeable barrier: It allows some substances to cross but blocks the movement of other substances. In addition, active transport pumps work continuously to maintain different concentrations of certain ions in the cytosol and interstitial fluid.
- Blood vessel walls divide the interstitial fluid from blood plasma. Only in capillaries, the smallest blood vessels, are the walls thin enough and leaky enough to permit the exchange of water and solutes between blood plasma and interstitial fluid.
The body is in fluid balance when the required amounts of water and electrolytes are present and are correctly proportioned among the various compartments. Water is by far the largest single component of the body, making up 45–75% of total body mass, depending on age, gender, and the amount of adipose tissue (fat) present in the body. Obese people have proportionally less water than leaner people because water comprises less than 20% of the mass of adipose tissue. Skeletal muscle tissue, by contrast, is about 65% water. Infants have the highest percentage of water, up to 75% of body mass. The percentage of body mass that is water decreases until about 2 years of age. Until puberty, water accounts for about 60% of body mass in boys and girls. In lean adult males, water still accounts for about 60% of body mass. However, lean adult females have more subcutaneous fat than do lean adult males. Thus, their percentage of total body water is lower, accounting for about 55% of body mass.
Figure 3. Intracellular (ICF) and Extracellular (ECF) fluid electrolyte concentrations
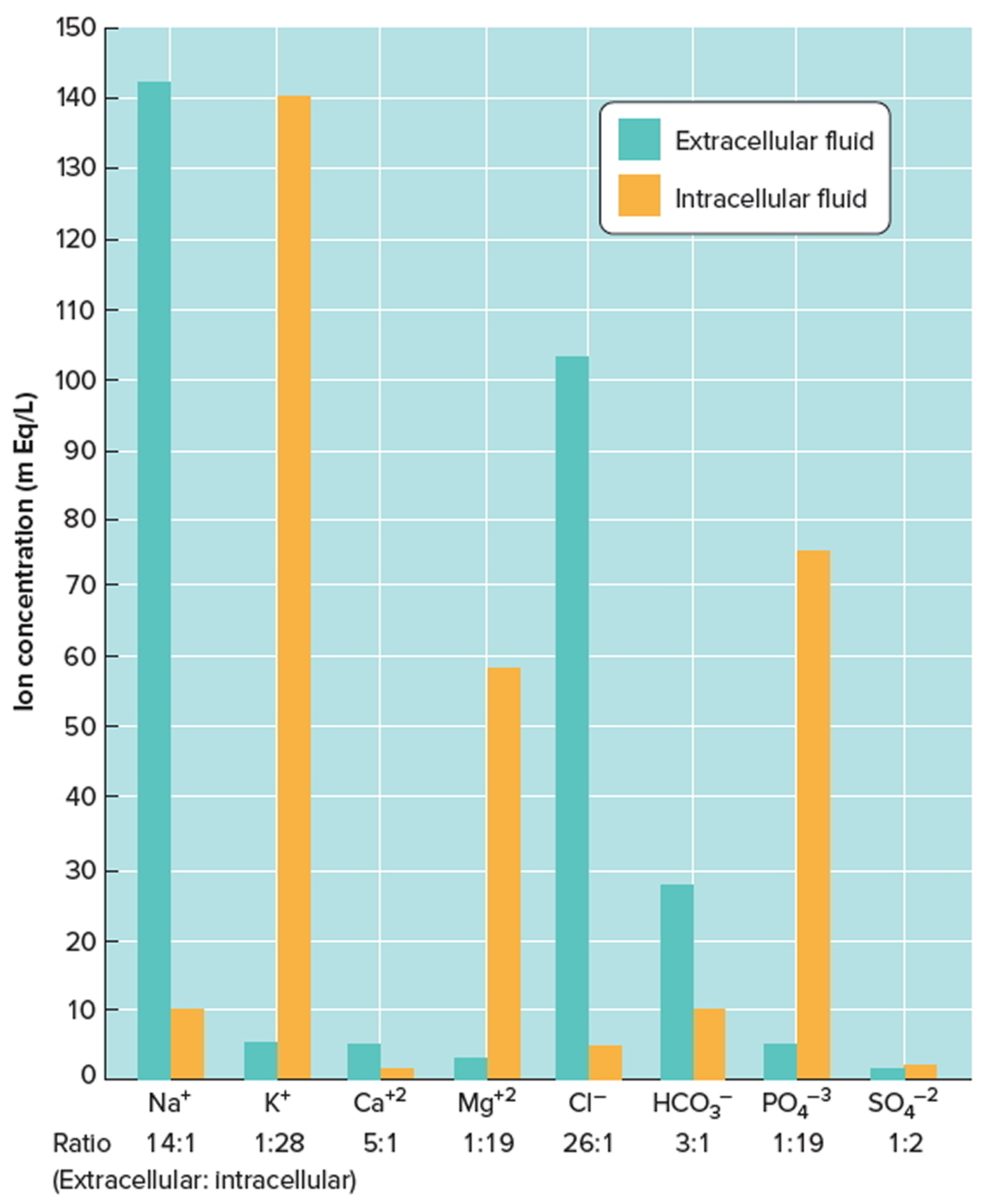
Note: Extracellular fluids have relatively high concentrations of sodium (Na+), calcium (Ca+2), chloride (Cl−), and bicarbonate (HCO3−) ions. Intracellular fluid has relatively high concentrations of potassium (K+), magnesium (Mg+2), phosphate (PO4−3), and sulfate (SO4−2) ions.
[Source 1]The processes of filtration, reabsorption, diffusion, and osmosis allow continual exchange of water and solutes among body fluid compartments. Yet the volume of fluid in each compartment remains remarkably stable. The pressures that promote filtration of fluid from blood capillaries and reabsorption of fluid back into capillaries. Because osmosis is the primary means of water movement between intracellular fluid and interstitial fluid, the concentration of solutes in these fluids determines the direction of water movement. Because most solutes in body fluids are electrolytes, inorganic compounds that dissociate into ions, fluid balance is closely related to electrolyte balance. Because intake of water and electrolytes rarely occurs in exactly the same proportions as their presence in body fluids, the ability of the kidneys to excrete excess water by producing dilute urine, or to excrete excess electrolytes by producing concentrated urine, is of utmost importance in the maintenance of homeostasis.
Sources of Body Water Gain and Loss
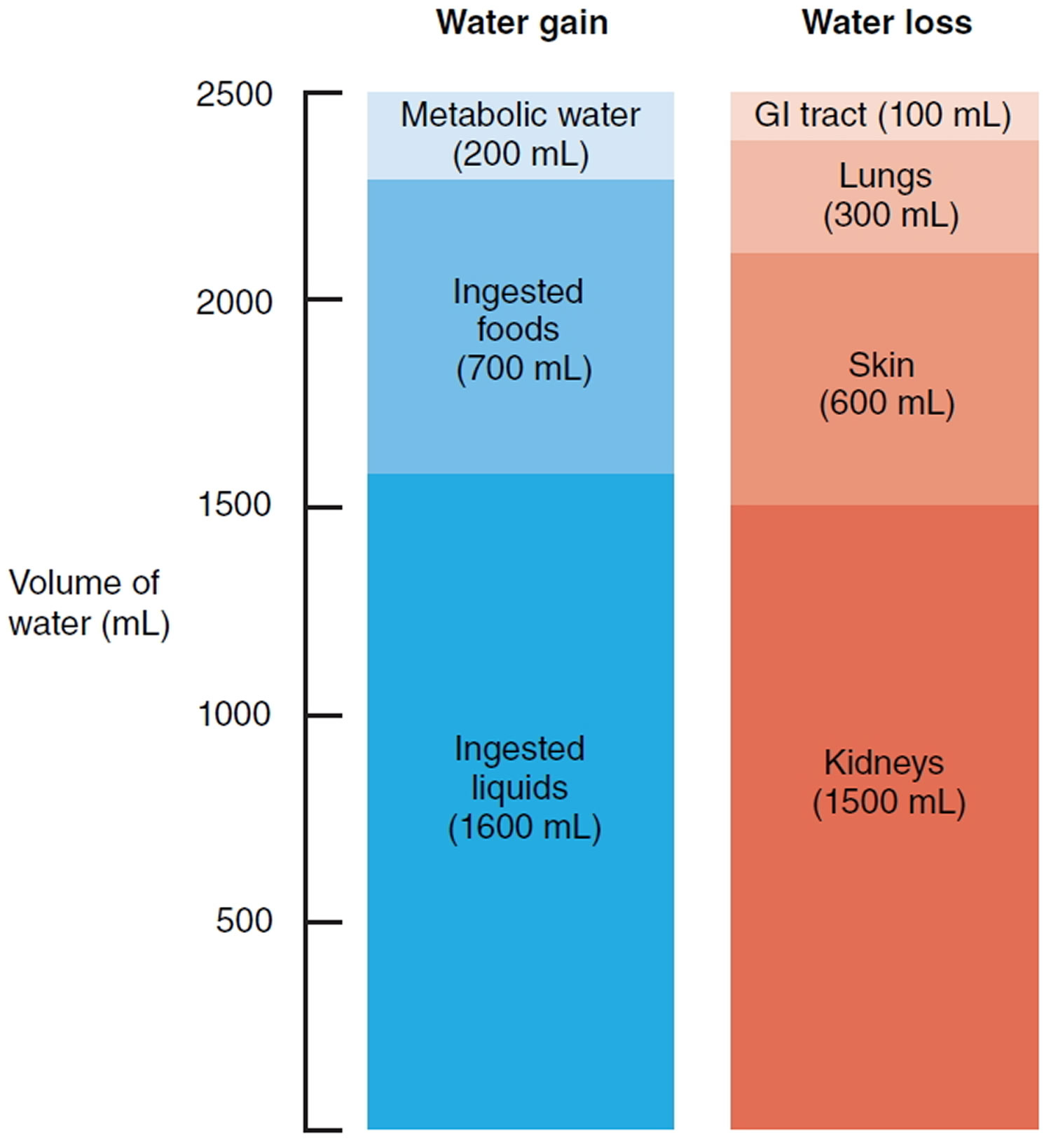
The body can gain water by ingestion and by metabolic synthesis (Figure 4). The main sources of body water are ingested liquids (about 1600 mL) and moist foods (about 700 mL) absorbed from the gastrointestinal (GI) tract, which total about 2300 mL/day. The other source of water is metabolic water that is produced in the body mainly when electrons are accepted by oxygen during aerobic respiration and to a smaller extent during dehydration synthesis reactions. Metabolic water gain accounts for only 200 mL/day. Daily water gain from these two sources totals about 2500 mL.
Normally, body fluid volume remains constant because water loss equals water gain. Water loss occurs in four ways. Each day the kidneys excrete about 1500 mL in urine, the skin evaporates about 600 mL (400 mL through insensible perspiration— sweat that evaporates before it is perceived as moisture—and 200 mL as sweat), the lungs exhale about 300 mL as water vapor, and the gastrointestinal tract eliminates about 100 mL in feces. In women of reproductive age, additional water is lost in menstrual flow. On average, daily water loss totals about 2500 mL. The amount of water lost by a given route can vary considerably over time. For example, water may literally pour from the skin in the form of sweat during strenuous exertion. In other cases, water may be lost in diarrhea during a GI tract infection.
Figure 4. Sources of daily water gain and loss under normal conditions. Numbers are average volumes for adults.
Regulation of Body Water Gain
The volume of metabolic water formed in the body depends entirely on the level of aerobic respiration, which reflects the demand for ATP (Adenosine triphosphate is the energy packets in your cells that is essential for life and your body to function) in body cells. When more ATP is produced, more water is formed. Body water gain is regulated mainly by the volume of water intake or how much fluid you drink. An area in the hypothalamus known as the thirst center governs the urge to drink.
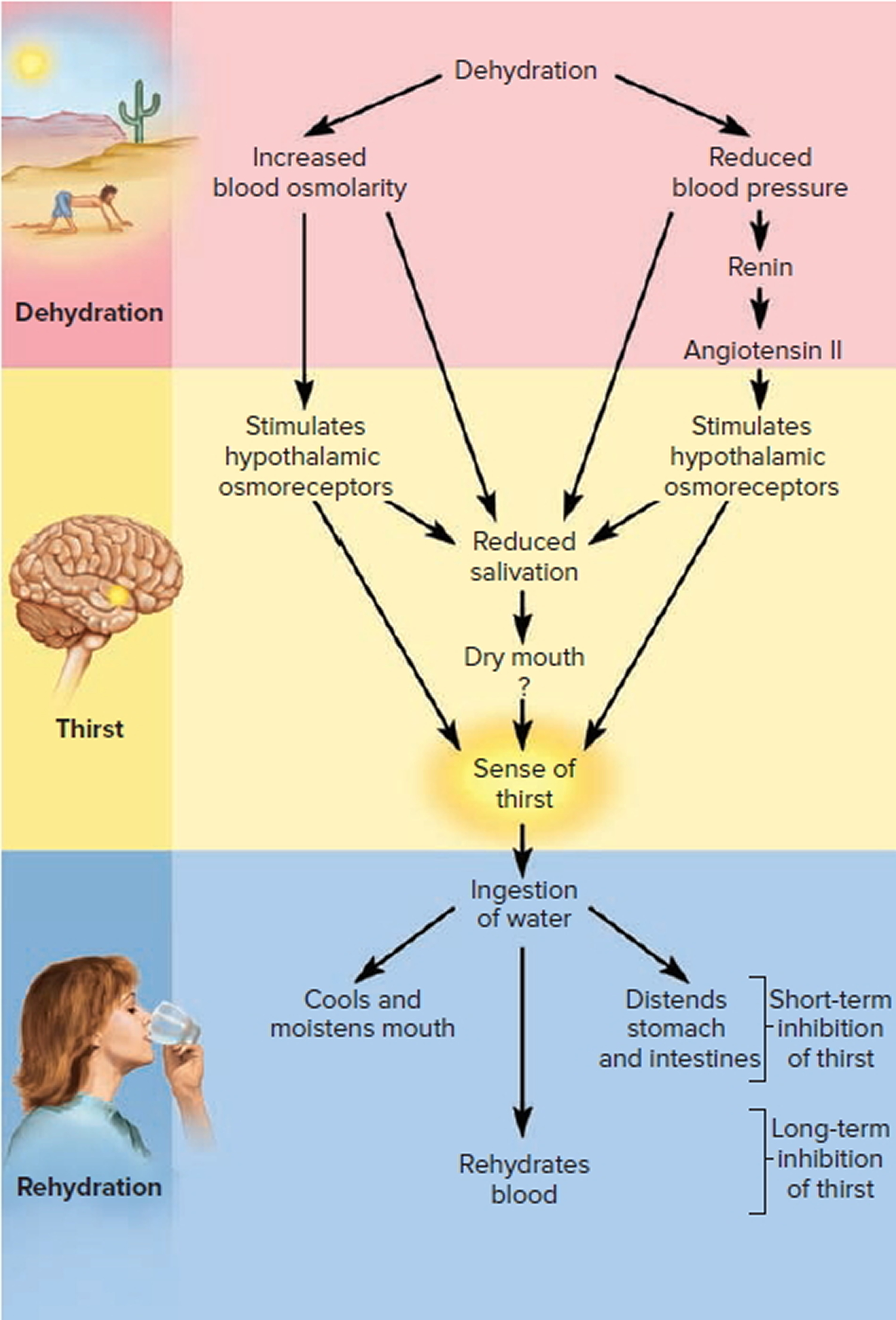
When water loss is greater than water gain, dehydration—a decrease in volume and an increase in osmolarity of body fluids— occurs. A decrease in blood volume causes blood pressure to fall. Increased activity from osmoreceptors in the hypothalamus, triggered by increased blood osmolarity, stimulates the thirst center in the hypothalamus (Figure 5).
Other signals that stimulate the thirst center come from:
- Volume receptors in the atria that detect the decrease in blood volume,
- Baroreceptors in blood vessels that detect the decrease in blood pressure,
- Angiotensin II that is formed due to activation of the renin-angiotensin-aldosterone pathway by the decrease in blood pressure, and
- Neurons in the mouth that detect dryness due to a decreased flow of saliva. As a result of these stimuli, the sensation of thirst increases, which usually leads to increased fluid intake (as long as fluids are available) and restoration of normal fluid volume.
Overall, fluid gain balances fluid loss. Sometimes, however, the sensation of thirst does not occur quickly enough or access to fluids is restricted, and significant dehydration ensues. This happens most oft en in elderly people, in infants, and in those who are in a confused mental state. When heavy sweating or fluid loss from diarrhea or vomiting occurs, it is wise to start replacing body fluids by drinking fluids even before the sensation of thirst occurs.
Figure 5. Regulation of water intake
Regulation of Electrolyte and Water Loss
Even though the loss of water and electrolytes through sweating and exhalation increases during exercise, elimination of excess body water or electrolytes occurs mainly by control of their loss in urine. The extent of urinary salt (NaCl) loss is the main factor that determines body fluid volume. The reason for this is that “water follows electrolytes” in osmosis, and the two main electrolytes in extracellular fluid (and in urine) are sodium ions (Na+) and chloride ions (Cl−). In a similar way, the main factor that determines body fluid osmolarity is the extent of urinary water loss.
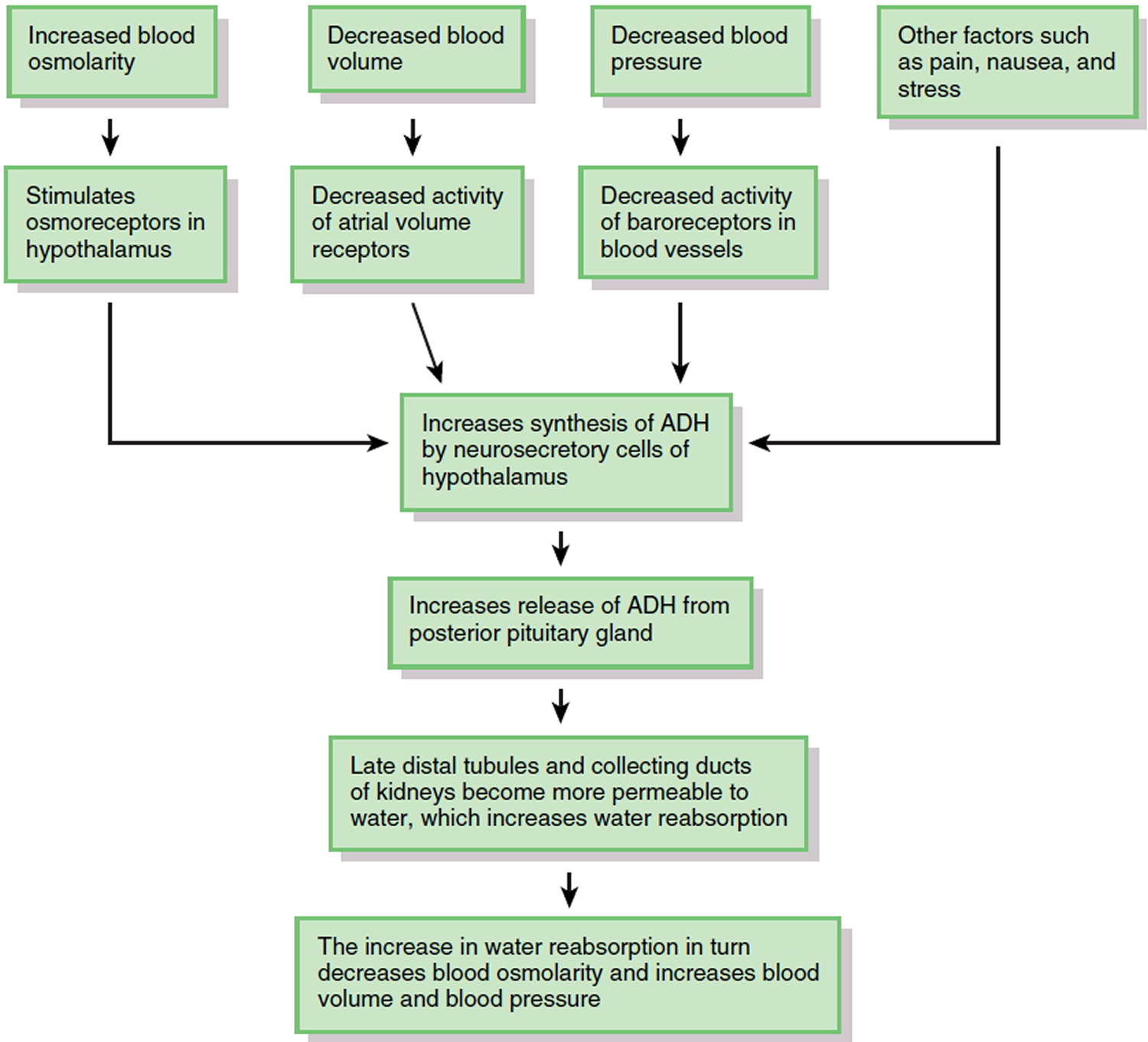
The major hormone that regulates water loss is antidiuretic hormone (ADH). This hormone, also known as vasopressin, is produced by neurosecretory cells in the hypothalamus and stored in the posterior pituitary gland. When the osmolarity of body fluids increases, osmoreceptors in the hypothalamus not only stimulate thirst; they also increase the synthesis and release of ADH (Figure 6). ADH promotes the insertion of water-channel proteins (aquaporin-2) into the apical membranes of principal cells in the late distal tubules and collecting ducts of the kidneys. As a result, the permeability of these cells to water increases. Water molecules move by osmosis from the renal tubular fluid into the cells and then from the cells into the bloodstream. This results in a decrease in blood osmolarity, an increase in blood volume and blood pressure, and the production of a small volume of concentrated urine. Once the body has adequate water, the ADH level in the bloodstream decreases. As the amount of ADH in the blood declines, some of the aquaporin-2 channels are removed from the apical membrane via endocytosis. Consequently, the water permeability of the principal cells decreases and more water is lost in the urine.
Factors other than blood osmolarity influence ADH secretion (Figure 6). A decrease in blood volume or blood pressure also stimulates ADH release. Atrial volume receptors detect the decrease in blood volume, and baroreceptors in blood vessels detect the decrease in blood pressure. ADH release is also stimulated by factors that are unrelated to water balance, such as pain, nausea, and stress. Secretion of ADH is inhibited by alcohol, which is why consumption of alcoholic beverages promotes diuresis (voiding large amounts of urine).
Figure 6. Role of Antidiuretic Hormone (ADH) in water balance
Because your daily diet contains a highly variable amount of NaCl (salt), urinary excretion of Na+ and Cl− must also vary to maintain homeostasis. Hormones regulate the urinary loss of Na+ ions, Cl− ions usually follow Na+ ions because of electrical attraction or because they are transported along with Na+ ions via symporters. The two most important hormones that regulate the extent of renal Na+ reabsorption (and thus how much is lost in the urine) are aldosterone and atrial natriuretic peptide.
- Aldosterone. When there is a decrease in blood pressure, which occurs in response to a decrease in blood volume, or when there is a deficiency of Na+ in the plasma, the kidneys release renin, which activates the renin-angiotensin-aldosterone pathway. Once aldosterone is formed, it increases Na+ reabsorption in the late distal tubules and collecting ducts of the kidneys, which relieves the Na+ deficiency in the plasma. Because antidiuretic hormone (ADH) is also released when blood pressure is low, water reabsorption accompanies Na+ reabsorption via osmosis. This conserves the volume of body fluids by reducing urinary loss of water.
- Atrial natriuretic peptide. An increase in blood volume, as might occur after you finish one or more supersized drinks, stretches the atria of the heart and promotes release of atrial natriuretic peptide (ANP). ANP promotes natriuresis, elevated excretion of Na+ into the urine. The osmotic consequence of excreting more Na+ is loss of more water in urine, which decreases blood volume and blood pressure. In addition to stimulating the release of ANP, an increase in blood volume also slows the release of renin from the kidneys. When the renin level declines, less aldosterone is formed, which causes reabsorption of filtered Na+ to slow in the late distal tubules and collecting ducts of the kidneys. More filtered Na+ and water (due to osmosis) thus remain in the tubular fluid to be excreted in the urine.
Table 1. Summary of Factors That Maintain Body Water Balance
FACTOR | MECHANISM | EFFECT |
| Thirst center in hypothalamus | Stimulates desire to drink fluids. | Water gained if thirst is quenched. |
| Antidiuretic hormone (ADH), also known as vasopressin | Promotes insertion of water-channel proteins (aquaporin-2) into apical membranes of principal cells in collecting ducts of kidneys. As a result, water permeability of these cells increases and more water is reabsorbed. | Reduces loss of water in urine. |
| Aldosterone | By promoting urinary reabsorption of Na+, increases water reabsorption via osmosis. | Reduces loss of water in urine. |
| Atrial natriuretic peptide (ANP) | Promotes natriuresis, elevated urinary excretion of Na+, accompanied by water. | Increases loss of water in urine. |
Disorders of Fluid Balance
The body is in a state of fluid imbalance if there is an abnormality of total volume, concentration, or distribution of water among the compartments.
Fluid Deficiency
Fluid deficiency arises when output exceeds intake over a long enough period of time. The two kinds of deficiency—volume depletion and dehydration—differ in the relative loss of water and electrolytes and the resulting osmolarity of the extracellular fluid (ECF). This important distinction calls for different strategies of fluid replacement therapy.
Volume depletion (hypovolemia) occurs when proportionate amounts of water and sodium are lost without replacement. Total body water declines but osmolarity remains normal. Volume depletion occurs in cases of hemorrhage, severe burns, and chronic vomiting or diarrhea. A less common cause is aldosterone hyposecretion (Addison disease), which results in inadequate sodium and water reabsorption by the kidneys.
Dehydration (negative water balance) occurs when the body eliminates significantly more water than sodium, so the extracellular fluid (ECF) osmolarity rises. The simplest cause of dehydration is a lack of drinking water—for example, when stranded in a desert or at sea. It can be a serious problem for elderly and bed ridden people who depend on others to provide them with water, especially for those who cannot express their need or whose caretakers are insensitive to it. Diabetes mellitus, ADH hyposecretion (diabetes insipidus), profuse sweating and overuse of diuretics are additional causes of dehydration. Cold weather can dehydrate a person just as much as hot weather.
For three reasons, infants are more vulnerable to dehydration than adults: (1) Their high metabolic rate produces toxic metabolites faster, and they excrete more water to eliminate them. (2) Their kidneys are not fully mature and cannot concentrate urine as effectively. (3) They have a greater ratio of body surface to volume; consequently, compared with adults, they lose twice as much water per kilogram of body weight by evaporation.
Dehydration affects all fluid compartments. Suppose, for example, that you play a strenuous tennis match on a hot summer day and lose a liter of sweat. Where does this fluid come from ? Most of it filters out of the bloodstream through the capillaries of the sweat glands. In principle, 1 L of sweat would amount to about one-third of the blood plasma. However, as the blood loses water, its osmolarity rises and water from the tissue fluid enters the bloodstream to balance the loss. This raises the osmolarity of the tissue fluid, so water moves out of the cells to balance that. Ultimately, all three fluid compartments (the ICF, blood, and tissue fluid) lose water. To excrete 1 L of sweat, about 300 mL of water would come from the tissue fluid and 700 mL from the ICF. Immoderate exercise without fluid replacement can lead to losses greater than 1 L per hour.
The most serious effects of fluid deficiency are circulatory shock due to loss of blood volume and neurological dysfunction due to dehydration of brain cells. Volume depletion by diarrhea is a major cause of infant mortality, especially under unsanitary conditions that lead to intestinal infections such as cholera.
Fluid Excess
Fluid excess is less common than fluid deficiency because the kidneys are highly effective at compensating for excessive intake by excreting more urine. Renal failure and other causes, however, can lead to excess fluid retention.
Fluid excesses are of two types called:
- Volume excess and
- Hypotonic hydration.
In volume excess, both sodium and water are retained and the extracellular fluid (ECF) remains isotonic. This can result from aldosterone hypersecretion or renal failure. In hypotonic hydration (also called water intoxication or positive water balance), more water than sodium is retained or ingested and the extracellular fluid (ECF) becomes hypotonic. This can occur if you lose a large amount of water and salt through urine and sweat and you replace it by drinking plain water. Without a proportionate intake of electrolytes, water dilutes the extracellular fluid (ECF), makes it hypotonic, and causes cellular swelling. ADH hypersecretion can cause hypotonic hydration by stimulating excessive water retention as sodium continues to be excreted. Among the most serious effects of either type of fluid excess are pulmonary and cerebral edema and death.
The four preceding forms of fluid imbalance are summarized and compared in table 2.
Table 2. Forms of Fluid Imbalance
Form | Total Body Water | Osmolarity |
| Fluid Deficiency | ||
| Volume depletion (hypovolemia) | Reduced | Isotonic (normal) |
| Dehydration (negative water balance) | Reduced | Hypertonic (elevated) |
| Fluid Excess | ||
| Volume excess | Elevated | Isotonic (normal) |
| Hypotonic hydration (positive water balance, water intoxication) | Elevated | Hypotonic (reduced) |
What causes electrolyte imbalance
Dehydration
Dehydration is usually caused by not drinking enough fluid to replace what you lose. The climate, the amount of physical exercise you are doing (particularly in hot weather) and your diet can contribute to dehydration 2. You can also become dehydrated as a result of an illness, such as persistent vomiting and diarrhea, or sweating from a fever.
Your body may lose a lot of fluid from:
- Sweating too much, for example, from exercising in hot weather
- Fever
- Vomiting or diarrhea
- Urinating too much (uncontrolled diabetes or some medications, like diuretics, can cause you to urinate a lot)
You might not drink enough fluids because:
- You do not feel like eating or drinking because you are sick
- You are nauseated
- You have a sore throat or mouth sores
Older adults and people with certain diseases, such as diabetes, are also at higher risk for dehydration.
Illness
- Diarrhea, vomiting. Severe, acute diarrhea — that is, diarrhea that comes on suddenly and violently — can cause a tremendous loss of water and electrolytes in a short amount of time. If you have vomiting along with diarrhea, you lose even more fluids and minerals.
- Fever. In general, the higher your fever, the more dehydrated you may become. The problem worsens if you have a fever in addition to diarrhea and vomiting.
Sweating
You can also become dehydrated if you sweat excessively after a fever, exercise, or carrying out heavy, manual work in hot and humid weather conditions.
In these situations, it’s important to drink regularly to replace lost fluids. It doesn’t necessarily need to be hot for you to lose a significant amount of fluid from sweating.
Children and teenagers are particularly at risk because they may ignore the symptoms of dehydration, or not know how to recognise and treat them.
Alcohol
Dehydration can also occur as a result of drinking too much alcohol. Alcohol is a diuretic, which means it makes you wee more.
The headache associated with a hangover indicates that your body is dehydrated. You should try to drink plenty of water when you have been drinking alcohol.
Diabetes
If you have diabetes, you’re at risk of becoming dehydrated because you have high levels of glucose in your bloodstream. Your kidneys will try to get rid of the glucose by creating more urine, so your body becomes dehydrated from going to the toilet more frequently.
Increased urination
This may be due to undiagnosed or uncontrolled diabetes. Certain medications, such as diuretics and some blood pressure medications, also can lead to dehydration, generally because they cause you to urinate more.
Who Is at Risk of Dehydration ?
Anyone can become dehydrated, but certain people are at greater risk:
- Infants and children. The most likely group to experience severe diarrhea and vomiting, infants and children are especially vulnerable to dehydration. Having a higher surface area to volume area, they also lose a higher proportion of their fluids from a high fever or burns. Young children often can’t tell you that they’re thirsty, nor can they get a drink for themselves.
- Older adults. As you age, your body’s fluid reserve becomes smaller, your ability to conserve water is reduced and your thirst sense becomes less acute. These problems are compounded by chronic illnesses such as diabetes and dementia, and by the use of certain medications. Older adults also may have mobility problems that limit their ability to obtain water for themselves.
- People with chronic illnesses. Having uncontrolled or untreated diabetes puts you at high risk of dehydration. Kidney disease also increases your risk, as do medications that increase urination. Even having a cold or sore throat makes you more susceptible to dehydration because you’re less likely to feel like eating or drinking when you’re sick.
- People who work or exercise outside. When it’s hot and humid, your risk of dehydration and heat illness increases. That’s because when the air is humid, sweat can’t evaporate and cool you as quickly as it normally does, and this can lead to an increased body temperature and the need for more fluids.
That’s why it’s important to increase water intake during hot weather or when you’re ill.
What are symptoms and signs of dehydration ?
Clinical symptoms and signs of dehydration generally have poor sensitivity and specificity 3. Nevertheless, factors that have a sensitivity >80% are dry mucous membranes in the mouth and nose and longitudinal furrows on the tongue. Some other factors have good specificity (>80%): speech incoherence, extremity weakness, dry axilla and sunken eyes.
Dehydration can be mild, moderate or severe, depending on how much of your body weight is lost through fluids 4. Signs of mild-to-moderate and severe dehydration are listed in Table 2 5. More recently, it has been shown that mild dehydration corresponding to only 1–2% of body weight loss in adults can lead to a significant impairment in both cognitive function (alertness, concentration, short-term memory) and physical performance (endurance, sports skills) 6, 7. Populations at particular risk of dehydration include the very young and the elderly.
Two early signs of dehydration are thirst and dark-colored urine. This is the body’s way of trying to increase water intake and decrease water loss. However, thirst isn’t always a reliable early indicator of the body’s need for water. Many people, particularly older adults, don’t feel thirsty until they’re already dehydrated. From a recent dehydration in the elderly review 8 only two tests showed any ability to diagnose water‐loss dehydration in the elderly (including both impending and current water‐loss dehydration) as stand‐alone tests. expressing fatigue and missing drinks between meals were shown to be sensitive and specific to diagnose dehydration in the elderly. Furthermore, fluid intake, urine specific gravity, urine color, urine volume, heart rate, dry mouth, feeling thirsty and bioelectrical impedance analysis (BIA) assessment of intracellular water or extracellular water are not useful, and should not be relied on individually as ways of assessing presence or absence of dehydration in older people 8.
Heat- and exercise-induced moderate acute dehydration resulted in a significant impairment of specific cognitive-motor functions such as short-term memory, working memory, perceptive discrimination, and visual-motor function 9, 10. The critical level of acute water deficit causing a decrease in cognitive performance occurred at a level of 2% or more 10. Adverse effects of acute moderate dehydration induced by heat or exercise were identical 11.
In contrast, reduced drinking in the presence of physiological needs may be particularly important in predisposing to subacute and chronic dehydration in the general population 12, 13. Water deprivation for 24 hours can induce a comparable level of water deficit, as acute heat or exercise testing during 0.5–2 hours 14, 15.
That’s why it’s important to increase water intake during hot weather or when you’re ill.
Table 3. Signs of dehydration in Adults
| Signs of mild-to-moderate dehydration | Signs of severe dehydration |
|---|---|
| Dry, sticky mouth | Extreme thirst |
| Sleepiness or tiredness | Extreme fussiness or sleepiness in infants and children; irritability and confusion in adults |
| Thirst | Very dry mouth, skin and mucous membranes |
| Decreased urine output | Lack of sweating |
| Few or no tears when crying | Little or no urination—any urine that is produced will be dark yellow or amber |
| Muscle weakness | Sunken eyes |
| Headache | Shrivelled and dry skin that lacks elasticity and does not ‘bounce back’ when pinched into a fold |
| Dizziness or light-headedness | In infants, sunken fontanels—the soft spots on the top of a baby’s head |
| Skin goes back slowly when pinched | Low blood pressure |
| Rapid heartbeat | |
| Fever | |
| Delirium or unconsciousness |
Some of the early warning signs of dehydration in adults include 16, 17, 18:
- A dry mouth, lips and eyes
- Feeling thirsty and lightheaded
- Urinating less often than usual (less than three or four times a day)
- Passing small amounts of urine infrequently
- Dark-colored urine, strong-smelling urine
- Dry cool skin
- Feeling tired
- Headache
- Confusion
- Muscle cramps
- Dizziness, light-headedness and fainting.
Signs of severe dehydration in adults 16:
- Not urinating, or very dark yellow or amber-colored urine
- Dry, shriveled skin
- Irritability or confusion
- Dizziness or light-headedness
- Rapid heartbeat
- Rapid breathing
- Sunken eyes
- Listlessness
- Shock (not enough blood flow through the body)
- Unconsciousness or delirium
Dehydration can also lead to a loss of strength and stamina. It’s a main cause of heat exhaustion.
The body is affected even when you lose a small amount of fluid.
You should be able to reverse dehydration at this stage by drinking more fluids.
If dehydration is ongoing (chronic), it can affect your kidney function and increase the risk of kidney stones. It can also lead to muscle damage and constipation.
A baby or a young child may be dehydrated if they 16, 17, 18:
- have a sunken soft spot (fontanelle) on their head
- dry mouth and tongue
- sunken eyes, cheeks
- Listlessness or irritability
- no wet diapers for 3 hours or more
- have few or no tears when crying
- have fewer wet nappies (nappies will feel lighter)
- are drowsy
- a high fever
- unusually sleepy or drowsy.
Table 4. Symptoms and signs of clinical dehydration and shock in Children (Under 5 years)
| Increasing severity of dehydration | |||
|---|---|---|---|
| No clinically detectable dehydration | Clinical dehydration | Clinical shock | |
| Symptoms (remote and face-to-face assessments) | Appears well | – | |
| Alert and responsive | Decreased level of consciousness | ||
| Normal urine output | Decreased urine output | – | |
| Skin colour unchanged | Skin colour unchanged | Pale or mottled skin | |
| Warm extremities | Warm extremities | Cold extremities | |
| Signs (face-to-face assessments) | Alert and responsive | Decreased level of consciousness | |
| Skin colour unchanged | Skin colour unchanged | Pale or mottled skin | |
| Warm extremities | Warm extremities | Cold extremities | |
| Eyes not sunken | – | ||
| Moist mucous membranes (except after a drink) | Dry mucous membranes (except for ‘mouth breather’) | – | |
| Normal heart rate | Tachycardia | ||
| Normal breathing pattern | Tachypnoea | ||
| Normal peripheral pulses | Normal peripheral pulses | Weak peripheral pulses | |
| Normal capillary refill time | Normal capillary refill time | Prolonged capillary refill time | |
| Normal skin turgor | – | ||
| Normal blood pressure | Normal blood pressure | Hypotension (decompensated shock) | |
Patients would merely be classified as follows: ‘no clinically detectable dehydration’, ‘clinical dehydration’ and ‘clinical shock’. With this assessment scheme the clinician would have to recognise the presence of clinical dehydration. This simplified scheme does not imply that the degree of dehydration is uniform, but rather acknowledges the difficulties in accurately assessing dehydration severity. The Guideline Development Group 19 recognised that experienced clinicians could distinguish marked differences in the severity of dehydration. They also considered that clinical signs were likely to be more pronounced and numerous in those with severe dehydration. However, firm recommendations linking clinical symptoms and signs with specific varying levels of dehydration were impossible. The crucial point however, is that the scheme (Table 3) is all that is required to guide fluid management 19.
Electrolyte imbalance treatment
Dehydration Treatment
- Children and adults who are severely dehydrated should be treated by emergency personnel arriving in an ambulance or in a hospital emergency room. Salts and fluids delivered through a vein (intravenously) are absorbed quickly and speed recovery.
Example in Hospital Emergency Room
A 7-mo-old infant has diarrhea for 3 days with weight loss from 10 kg to 9 kg. The infant is currently producing 1 diarrheal stool every 3 h and refusing to drink. Clinical findings of dry mucous membranes, poor skin turgor, markedly decreased urine output, and tachycardia with normal BP and capillary refill suggest 10% fluid deficit. Rectal temperature is 37° C; serum Na, 136 mEq/L; K, 4 mEq/L; Cl, 104 mEq/L; and HCO3, 20 mEq/L.
Fluid volume is estimated by deficits, ongoing losses, and maintenance requirements.
- The total fluid deficit given 1 kg wt loss = 1 L.
- Ongoing diarrheal losses are measured as they occur by weighing the infant’s diaper before application and after the diarrheal stool.
- Baseline maintenance requirements by the weight-based Holliday-Segar method are 100 mL/kg × 10 kg = 1000 mL/day = 1000/24 or 40 mL/h.
Electrolyte losses resulting from diarrhea in a eunatremic patient are an estimated 80 mEq of Na and 80 mEq of K.
IV Fluid Resuscitation
The patient is given an initial bolus of lactated Ringer solution 200 mL (20 mL/kg × 10 kg) over 30 min. This amount replaces 26 mEq of the estimated 80 mEq Na (sodium) deficit.
Deficits
- Residual fluid deficit is 800 mL (1000 initial − 200 mL resuscitation), and Na deficit is 54 mEq (80 − 26 mEq). This residual amount is given over the next 24 h. Typically, half (400 mL) is given over the first 8 h (400 ÷ 8 = 50 mL/h) and the other half is given over the next 16 h (25 mL/h). The fluid used is 5% dextrose/0.45% saline. This amount replaces the Na deficit (0.8 L × 77 mEq Na/L =62 mEq Na). When urine output is established, K is added at a concentration of 20 mEq/L (for safety reasons, no attempt is made to replace complete K deficit acutely).
Ongoing losses
Five percent dextrose/0.45% saline also is used to replace ongoing losses; volume and rate are determined by the amount of diarrhea.
Switch from intravenous hydration to oral rehydration solution once hydration is improved and the patient can drink. This will conserve IV fluids and reduce the risk of phlebitis and other complications.
Nasogastric tubes can be used to administer oral rehydration solution if patient is alert but unable to drink sufficient quantities independently.
Maintenance fluid
Five percent dextrose/0.2% or 0.45% saline is given at 40 mL/h with 20 mEq/L of K added when urine output is established. Alternatively, the deficit could be replaced during the initial 8 h followed by the entire day’s maintenance fluid in the next 16 h (ie, 60 mL/h); 24 h of maintenance fluid given in 16 h reduces mathematically to a rate of 1.5 times the usual maintenance rate and obviates the need for simultaneous infusions (which may require 2 rate-controlling pumps).
World Health Organization (WHO) Fluid Replacement or Treatment Recommendations
| No dehydration | Oral rehydration salts | |||
|---|---|---|---|---|
| Age | Volume of ORS (Oral Rehydration Solution) | |||
| <2 years | 50–100 ml, up to 500 mL/day | |||
| 2–9 years | 100–200 ml, up to 1000 mL/day | |||
| ≥10 years | As much as wanted, up to 2000 mL/day | |||
| Some dehydration | Oral rehydration salts | |||
| Age | Weight | Volume of ORS (Oral Rehydration Solution) | ||
| <4 months | <5 kg | 200–400 mL | ||
| 4–11 months | 5–7.9 kg | 400–600 mL | ||
| 1–2 years | 8–10.9 kg | 600–800 mL | ||
| 2–4 years | 11–15.9 kg | 800–1200 mL | ||
| 5–14 years | 16–29.9 kg | 1200–2200 mL | ||
| ≥15 years | 30 kg or more | 2200–4000 mL | ||
| Severe dehydration | Intravenous Ringer’s Lactate or, if not available, normal saline and oral rehydration salts as outlined above. Do not give plain glucose or dextrose solution. | |||
| Age< 12 months | ||||
| Timeframe | Total volume | |||
| 0–30 min | 30 ml/kg* | |||
| 30 min–6 h | 70 ml/kg | |||
| 6 h–24 h | 100 ml/kg | |||
| Age≥ 1 year | ||||
| Timeframe | Total volume | |||
| 0–30 min | 30 ml/kg* | |||
| 30 min–3 h | 70 ml/kg | |||
| 3 h–24 h | 100 ml/kg | |||
*Repeat once if radial pulse is still very weak or not detectable
[Source 20]Treatment of Dehydration at Home
A well-conducted systematic review did not find any significant difference in the incidences of hyponatraemia, hypernatraemia, the mean duration of diarrhoea, weight gain or total fluid intake in children treated with oral rehydration solution therapy compared with intravenous therapy 21. Although oral rehydration solution therapy was associated with a 4% higher risk of rehydration failure, when the analysis was conducted using a homogeneous definition of rehydration failure, no statistically significant difference was seen. Dehydrated children treated with oral rehydration solution therapy had a significantly shorter stay in hospital and those receiving intravenous therapy had a higher risk of phlebitis (vein inflammation) but no statistically significant differences were found between the oral rehydration solution therapy and intravenous therapy groups for the other complications – hypernatraemia, paralytic ileus, abdominal distension, peri-orbital oedema or seizures 21. Methodologically, there was great variation between the trials with regard to the study population characteristics, composition of oral rehydration solution solution and the modes of administration of oral rehydration solution solution.
The only effective treatment for dehydration is to replace lost fluids and lost electrolytes. The best approach to dehydration treatment depends on age, the severity of dehydration and its cause.
- Oral rehydration solution should contain complex carbohydrate or 2% glucose and 50 to 90 mEq/L of Na 22. Sports drinks, sodas, juices, and similar drinks do not meet these criteria and should not be used. They generally have too little Na and too much carbohydrate to take advantage of Na/glucose cotransport, and the osmotic effect of the excess carbohydrate may result in additional fluid loss. The Na/glucose cotransport in the gut is optimized with an Na:glucose ratio of 1:1.
Oral rehydration solution is recommended by the World Health Organization and is widely available in the US without prescription. Most solutions come as powders that are mixed with tap water.
An oral rehydration solution packet is dissolved in 1 Liter of water to produce a solution containing glucose 111, sodium 90, potassium 20, chloride 80 and bicarbonate 30, all in 311 mmol/l (standard WHO ORS with high 311 mmol/l with sodium:glucose ratio 1:3) 23 or sodium 75, potassium 20, chloride 65, citrate 10, and glucose 75 (WHO reduced-osmolarity ORS with 245 mmol/l low sodium:glucose ratio 1:1) 23. There is evidence from one high-quality systematic review indicating a significant reduction in the need for unscheduled IV fluids for the treatment of dehydration in children with diarrhoea when using low-osmolarity ORS solution (sodium 75, potassium 20, chloride 65, citrate 10, and glucose 75 (WHO reduced-osmolarity ORS with 245 mmol/l low sodium:glucose ratio 1:1)) compared with the previously recommended high-osmolarity WHO ORS solution (glucose 111, sodium 90, potassium 20, chloride 80 and bicarbonate 30, all in 311 mmol/l (standard WHO ORS with high 311 mmol/l with sodium:glucose ratio 1:3)). Moreover, the results suggest that low-osmolarity ORS solution leads to a greater reduction in stool output and vomiting. No difference was seen in the incidence of hyponatraemia. The other systematic review reported no statistically significant difference between oral rehydration solutions with different sodium contents in terms of treatment failure (need for IVT) in well-nourished children with gastroenteritis and dehydration 23. It also failed to show any consistent trend in favour of either high- or low-sodium ORS solution for rehydration 21.
In conclusion, oral rehydration solution of reduced osmolarity (<270 mOsm/l) is preferable to solutions with a high osmolarity (>311 mOsm/l). Reduced osmolarity oral rehydration solution solution was associated with a lower incidence of failure to rehydrate and also a greater reduction in stool output.
Evidence from a well-conducted systematic review found no statistically significant differences in stool output or duration of diarrhoea when children with non-cholera diarrhoea were treated with rice-based oral rehydration solution solution compared with the traditional glucose-based oral rehydration solution solution. However, in children with cholera, rice-based oral rehydration solution solution was associated with a reduction in stool output and duration of diarrhoea 23.
Administration
Generally, 50 mL/kg is given over 4 h for mild dehydration and 100 mL/kg for moderate. For each diarrheal stool, an additional 10 mL/kg (up to 240 mL) is given. After 4 h, the patient is reassessed. If signs of dehydration persist, the same volume is repeated. Patients with diarrhea may require many liters of fluid/day.
- Or the approximate amount of oral rehydration solution (in milliliters) needed can also be calculated by multiplying the patient’s weight in kg by 75 20.
- A rough estimate of oral rehydration rate for older children and adults is 100 ml oral rehydration solution every five minutes, until the patient stabilizes 20.
- During the initial stages of therapy, while still dehydrated, adults can consume as much as 1000 ml of oral rehydration solution per hour, if necessary, and children as much as 20 ml/kg body weight per hour.
- The volumes and time shown are guidelines based on usual needs. If necessary, amount and frequency can be increased, or the oral rehydration solution can be given at the same rate for a longer period to achieve adequate rehydration. Similarly, the amount of fluid can be decreased if hydration is achieved earlier than expected.
- If the patient requests more than the prescribed oral rehydration solution solution, give more.
- Patients should continue to eat a normal diet or resume a normal diet once vomiting stops.
Vomiting usually should not deter oral rehydration (unless there is bowel obstruction or other contraindication) because vomiting typically abates over time. Small, frequent amounts are used, starting with 5 mL every 5 min and increasing gradually as tolerated. The calculated volume required over a 4-h period can be divided into 4 separate portions. These 4 aliquots can then be divided into 12 smaller aliquots and given every 5 min over the course of an hour with a syringe if needed.
In children with diarrhea, oral intake often precipitates a diarrheal stool, so the same volume should be given in fewer aliquots.
Once the deficit has been replaced, an oral maintenance solution containing less Na should be used. Children should eat an age-appropriate diet as soon as they have been rehydrated and are not vomiting. Infants may resume breastfeeding or formula.
Signs of Adequate Rehydration
- Skin goes back normally when pinched
- Thirst has subsided
- Urine has been passed
- Pulse is strong
Infants and children
For infants and children who have become dehydrated from diarrhea, vomiting or fever, use an oral rehydration solution such as Pedialyte or Hydralyte. These solutions contain water and salts in specific proportions to replenish both fluids and electrolytes.
Babies
Start with about a teaspoon (5 milliliters) every one to five minutes and increase as tolerated. It may be easier to use a syringe for very young children.
Giving your baby regular sips (a few times an hour) of oral rehydration solution in addition to their usual feed (breastmilk, formula milk and water) will help to replace lost fluids, salts and sugars.
Avoid giving your baby fruit juice, particularly if they have diarrhoea and vomiting, because it can make it worse.
In a case–control study from Bangladesh 24, children aged between 1 and 35 months were selected for study inclusion if they had watery diarrhoea for 6 days or less at first presentation and had been breastfeeding up to the time of onset of diarrhoea. All were assessed for dehydration and were classified as ‘cases’ (with moderate to severe dehydration if there was a definite decrease in skin elasticity and presence of one or more of following signs: sunken eyes, failure to urinate for 6 hours, sunken anterior fontanelle, rapid and weak pulse) or as ‘controls’ (with no dehydration or mild dehydration if they did not fulfil those clinical criteria). Home oral rehydration solution therapy use was defined as giving either pre-packaged oral rehydration solution or home-made salt and sugar solution. There were 285 cases and 728 controls. After controlling for confounding factors (lack of maternal education, history of vomiting, high stool frequency, young age and infection with Vibrio cholerae), the risk of dehydration was five times higher in infants whose mothers stopped breastfeeding compared with infants whose mothers continued to breastfeed following the onset of diarrhoea 24. Similarly, the risk of dehydration was 1.5 times higher in infants who did not receive any oral rehydration solution therapy at home compared with those who received plentiful oral rehydration solution therapy (total volume ≥ 250 ml). Infants receiving smaller amounts of oral rehydration solution therapy (≤ 250 ml) before admission had an 18% higher risk of dehydration compared with those receiving plentiful oral rehydration solution therapy, but the risk was not statistically significant. Evidence from a case–control study indicated that cessation of breastfeeding in children with gastroenteritis was associated with an increased risk of dehydration. This study also suggested that oral fluid supplementation begun at home and given in good quantity was associated with a reduced risk of dehydration 21.
In children with gastroenteritis but without clinical dehydration:
- continue breastfeeding and other milk feeds.
- encourage fluid intake.
- discourage the drinking of fruit juices and carbonated drinks, especially in those at increased risk of dehydration.
- offer oral rehydration salt (ORS) solution as supplemental fluid to those at increased risk of dehydration.
Children
Children who are dehydrated should also take an oral rehydration solution such as Pedialyte or Hydralyte. These solutions contain water and salts in specific proportions to replenish both fluids and electrolytes.
If your child is finding it difficult to hold down fluids because of vomiting, give them smaller amounts more frequently. You may find it easier to use a spoon or a syringe.
Recommendation on oral rehydration therapy in children 21
In children with clinical dehydration, including hypernatraemic dehydration:
- use low-osmolarity ORS solution (240–250 mOsm/l)* for oral rehydration therapy
- give 50 ml/kg for fluid deficit replacement over 4 hours as well as maintenance fluid
- give the ORS solution frequently and in small amounts
- consider supplementation with their usual fluids (including milk feeds or water, but not fruit juices or carbonated drinks) if they refuse to take sufficient
- quantities of ORS solution and do not have red flag symptoms or signs (see Table 3)
- consider giving the ORS solution via a nasogastric tube if they are unable to drink it or if they vomit persistently
- monitor the response to oral rehydration therapy by regular clinical assessment.
However, some children may not tolerate oral rehydration therapy, either because they are unable to drink oral rehydration solution solution in adequate quantities or because they persistently vomit. In such cases, oral rehydration solution solution could be administered via a nasogastric tube, rather than changing to intravenous fluid therapy. This overcomes the problem of oral rehydration solution refusal. Continuous infusion of oral rehydration solution via a nasogastric tube might reduce the risk of vomiting.
Adults
- Most adults with mild to moderate dehydration from diarrhea, vomiting or fever can improve their condition by drinking more water or other liquids. Diarrhea may be worsened by full-strength fruit juice and soft drinks.
If you work or exercise outdoors during hot or humid weather, cool water is your best bet. Sports drinks containing electrolytes and a carbohydrate solution also may be helpful.
- Sports drink for exercise or working outdoors during hot and humid weather 25:
Sports drinks make an excellent fuel and hydration choice because they are a mix of carbohydrates and water. For exercise lasting anywhere from 60 minutes to
several hours, drinking carbohydrate beverages significantly boosts endurance performance compared to drinking water. According to some research, you can
expect an improvement in endurance of about 20 percent or more in workouts lasting over 90 minutes.
- Most commercial sports drinks supply a blend of sugars: four to nine percent solution, or 13 to 19 grams of carbs, per eight ounces.
- Drinking one-and-a-half to four cups per hour (more if you have heavy sweat losses) will provide you with both the fluid and carbs you need for endurance.
- Choose a beverage flavor you enjoy to encourage you to drink appropriate amounts.
- Fitness waters do not provide enough carbohydrate to boost endurance, but they can keep you hydrated.
- Drinking before and after exercise is also an important factor in maintaining proper hydration levels.
When you have diarrhea or gastroenteritis
Diarrhea is the passage of loose or watery stool 26. For some, diarrhea is mild and will go away within a few days 27. For others, it may last longer. It can make you lose too much fluid (dehydrated) and feel weak. It can also lead to unhealthy weight loss.
The stomach flu (viral gastroenteritis) is a common cause of diarrhea 28. Medical treatments, such as antibiotics and some cancer treatments can also cause diarrhea.
How to Relieve Diarrhea
These things may help you feel better if you have diarrhea:
- Drink 8 to 10 glasses of clear fluids every day. Water is best.
- Drink at least 1 cup (240 milliliters) of liquid every time you have a loose bowel movement.
- Eat small meals throughout the day, instead of 3 big meals.
- Eat some salty foods, such as pretzels, soup, and sports drinks.
- Eat some high potassium foods, such as bananas, potatoes without the skin, and fruit juices.
Your provider may also recommend a special medicine for diarrhea. Take this medicine as you have been told to take it.
Eating When you Have Diarrhea
You can bake or broil beef, pork, chicken, fish, or turkey. Cooked eggs are also OK. Use low-fat milk, cheese, or yogurt.
If you have very severe diarrhea, you may need to stop eating or drinking dairy products for a few days.
Eat bread products made from refined, white flour. Pasta, white rice, and cereals such as cream of wheat, farina, oatmeal, and cornflakes are OK. You may also try pancakes and waffles made with white flour, and cornbread. But don’t add too much honey or syrup.
You should eat vegetables, including carrots, green beans, mushrooms, beets, asparagus tips, acorn squash, and peeled zucchini. Cook them first. Baked potatoes are OK. In general, removing seeds and skins is best.
Some desserts and snacks to try include fruit-flavored gelatin, fruit-flavored ice pops, cakes, cookies, or sherbet.
Things you Should Avoid Eating or Drinking
You should avoid certain kinds of foods when you have diarrhea, including fried foods and greasy foods.
Avoid fruits and vegetables that can cause gas, such as broccoli, peppers, beans, peas, berries, prunes, chickpeas, green leafy vegetables, and corn.
Avoid caffeine, alcohol, and carbonated drinks.
Limit or cut out milk and other dairy products if they are making your diarrhea worse or causing gas and bloating.
When to See a Doctor
See your health care provider if you have:
- The diarrhea gets worse or does not get better in 2 days for an infant or child, or 5 days for adults
- Stools with an unusual odor or color
- Nausea or vomiting
- Blood or mucus in your stool
- A fever that does not go away
- Stomach pain
Complications of Dehydration
Dehydration can lead to serious complications, including:
Permanent brain damage.
Death.
Heat Injury or Heatstroke
If you don’t drink enough fluids when you’re exercising vigorously and perspiring heavily, you may end up with a heat injury, ranging in severity from mild heat cramps to heat exhaustion or potentially life-threatening heatstroke 29.
Heat injuries (heatstroke) can occur due to high temperatures and humidity 29. Heat exhaustion or heatstroke can develop quickly over a few minutes, or gradually over several hours or days. You are more likely to feel the effects of heat sooner if:
- You are not used to high temperatures or high humidity.
- You are a child or an older adult.
- You are already ill from another cause (such as diabetes or a heart or lung condition) and dehydrated (e.g. gastro diarhhea) or have been injured.
- You are obese.
- You are doing strenuous exercise for long periods, such as military soldiers, athletes, hikers and manual workers. Even a person who is in good shape can suffer heat illness if warning signs are ignored.
You’re more likely to experience problems if you’re dehydrated, there’s little breeze or ventilation, or you’re wearing tight, restrictive clothing.
Certain medications can also increase your risk of developing heat exhaustion or heatstroke, including diuretics, antihistamines, beta-blockers, antipsychotics and recreational drugs, such as amphetamines and ecstasy.
The following make it harder for the body to regulate its temperature, and make a heat emergency more likely:
- Drinking alcohol before or during exposure to heat or high humidity
- Not drinking enough fluids when you’re active on warmer or hot days
- Heart disease
- Certain medicines: Examples are beta-blockers, water pills or diuretics, some medicines used to treat depression, psychosis, or ADHD
- Sweat gland problems
- Wearing too much clothing
Symptoms of Heatstroke
Heat cramps are the first stage of heat illness. If these symptoms are not treated, it can lead to heat exhaustion and then heat stroke.
Heat stroke occurs when the body is no longer able to regulate its temperature, and it keeps rising. Heat stroke can cause shock, brain damage, organ failure, and even death.
The early symptoms of heat cramps include:
- Muscle cramps and pains that most often occur in the legs or abdomen
- Very heavy sweating
- Fatigue
- Thirst
Later symptoms of heat exhaustion include:
- Headache
- Dizziness, lightheadedness
- Weakness
- Nausea and vomiting
- Cool, moist skin
- Dark urine
The symptoms of heatstroke include (call your local emergency number right away):
- Fever — temperature above 104°F (40°C)
- Irrational behavior
- Extreme confusion
- Dry, hot, and red skin
- Rapid, shallow breathing
- Rapid, weak pulse
- Seizures
- Unconsciousness
First Aid for Heatstroke
If you think a person may have heatstroke or heat emergency:
- Have the person lie down in a cool place. Raise the person’s feet about 12 inches (30 centimeters).
- Remove any unnecessary clothing to expose as much of their skin as possible.
- Apply cool, wet cloths (or cool water directly) to the person’s skin and use a fan to lower body temperature. Place cold compresses on the person’s neck, groin, and armpits.
- Fan their skin while it’s moist – this will help the water to evaporate, which will help their skin cool down.
- If alert, give the person a beverage to sip (such as a sports drink or water), or make a salted drink by adding a teaspoon (6 grams) of salt per quart (1 liter) of water.
- Give a half cup (120 milliliters) every 15 minutes. Cool water will do if salt beverages are not available.
- For muscle cramps, give beverages as noted above and massage affected muscles gently, but firmly, until they relax.
- If the person shows signs of shock (bluish lips and fingernails and decreased alertness), starts having seizures, or loses consciousness, call 911 and give first aid as needed.
Stay with the person until they’re feeling better. Most people should start to recover within 30 minutes.
If the person is unconscious, you should follow the steps above and place the person in the recovery position until help arrives (see below). If they have a seizure, move nearby objects out of the way to prevent injury.
Follow these precautions:
- DO NOT give the person medications that are used to treat fever (such as aspirin or acetaminophen). They will not help, and they may be harmful.
- DO NOT give the person salt tablets.
- DO NOT give the person liquids that contain alcohol or caffeine. They will make it harder for the body to control its internal temperature.
- DO NOT use alcohol rubs on the person’s skin.
- DO NOT give the person anything by mouth (not even salted drinks) if the person is vomiting or unconscious.
Prevention of Heatstroke
Heat exhaustion and heatstroke can often be prevented by taking sensible precautions when it’s very hot.
During the summer, check for heatwave warnings, so you’re aware when there’s a potential danger. The government uses a system called Heat-Health Watch to warn people about the chances of a heatwave. This is a system of four different warning levels based on the expected temperature.
The first step in preventing heat illnesses is thinking ahead.
- Find out what the temperature will be for the whole day when you will be outdoors.
- Think about how you have dealt with heat in the past.
- Make sure you will have plenty of fluids to drink.
- Find out if there is shade available where you are going.
- Learn the early signs of heat illness.
To help prevent heat illnesses:
- Wear loose-fitting, lightweight and light-colored clothing in hot weather.
- Rest often and seek shade when possible.
- Avoid exercise or heavy physical activity outdoors during hot or humid weather.
- Drink plenty of fluids every day. Drink more fluids before, during, and after physical activity.
- Be very careful to avoid overheating if you are taking drugs that impair heat regulation, or if you are overweight or elderly.
- Be careful of hot cars in the summer. Allow the car to cool off before getting in.
- NEVER leave a child sitting in a car exposed to the hot sun, even after opening windows.
Stay out of the heat
- Keep out of the sun between 11am and 3pm.
- If you have to go out in the heat, walk in the shade, apply sunscreen and wear a hat and light scarf.
- Avoid extreme physical exertion.
- Wear light, loose-fitting cotton clothes.
If you’re travelling to a hot country, be particularly careful for at least the first few days, until you get used to the temperature.
Cool yourself down
- Have plenty of cold drinks, and avoid excess alcohol, caffeine and hot drinks.
- Eat cold foods, particularly salads and fruit with a high water content.
- Take a cool shower or bath.
- Sprinkle water over your skin or clothing, or keep a damp cloth on the back of your neck.
If you’re not urinating frequently or your urine is dark, it’s a sign that you’re becoming dehydrated and need to drink more.
Keep your environment cool
- Keep windows and curtains that are exposed to the sun closed during the day, but open windows at night when the temperature has dropped.
- If possible, move into a cooler room, especially for sleeping.
- Electric fans may provide some relief.
- Turn off non-essential lights and electrical equipment, as they generate heat.
- Keep indoor plants and bowls of water in the house, as these can cool the air.
In the longer term, it can help to have your loft and cavity walls insulated, as this will keep the heat in when it’s cold and keep it out when it’s hot. Using light-colored, reflective external paint on your house may also be useful.
Look out for others
- Keep an eye on isolated, elderly, ill or very young people and make sure they are able to keep cool.
- Ensure that babies, children or elderly people are not left alone in stationary cars.
- Check on elderly or sick neighbours, family or friends every day during a heatwave.
- Be alert and call a doctor or social services if someone is unwell or further help is needed.
Urinary and kidney problems
- Prolonged or repeated bouts of dehydration can cause urinary tract infections, kidney stones and even kidney failure.
Seizures
- Electrolytes — such as potassium and sodium — help carry electrical signals from cell to cell. If your electrolytes are out of balance, the normal electrical messages can become mixed up, which can lead to involuntary muscle contractions and sometimes to a loss of consciousness.
Low blood volume shock (hypovolemic shock)
- This is one of the most serious, and sometimes life-threatening, complications of dehydration. It occurs when low blood volume causes a drop in blood pressure and a drop in the amount of oxygen in your body.
What is Diabetes insipidus
Diabetes insipidus is an uncommon disorder that causes an imbalance of water in the body. This imbalance leads to intense thirst even after drinking fluids (polydipsia), and excretion of large amounts of urine (polyuria). Diabetes insipidus causes frequent urination. You become extremely thirsty, so you drink. Then you urinate. This cycle can keep you from sleeping or even make you wet the bed. Your body produces lots of urine that is almost all water.
While the names diabetes insipidus and diabetes mellitus sound similar, they’re not related. Diabetes mellitus — which can occur as type 1 or type 2 — is the more common form of diabetes.
There’s no cure for diabetes insipidus, but treatments are available to relieve your thirst and normalize your urine output.
Symptoms of Diabetes insipidus
The most common signs and symptoms of diabetes insipidus are:
- Extreme thirst
- Excretion of an excessive amount of diluted urine
Depending on the severity of the condition, urine output can be as much as 16 quarts (about 15 liters) a day if you’re drinking a lot of fluids. Normally, a healthy adult will urinate an average of less than 3 quarts (about 3 liters) a day.
Other signs may include needing to get up at night to urinate (nocturia) and bed-wetting.
Infants and young children who have diabetes insipidus may have the following signs and symptoms:
- Unexplained fussiness or inconsolable crying
- Trouble sleeping
- Fever
- Vomiting
- Diarrhea
- Delayed growth
- Weight loss
When to see a doctor
See your doctor immediately if you notice the two most common signs of diabetes insipidus: excessive urination and extreme thirst.
Causes of Diabetes insipidus
Diabetes insipidus occurs when your body can’t regulate how it handles fluids. Normally, your kidneys remove excess body fluids from your bloodstream. This fluid waste is temporarily stored in your bladder as urine, before you urinate.
When your fluid regulation system is working properly, your kidneys conserve fluid and make less urine when your body water is decreased, such as through perspiration.
The volume and composition of your body fluids remain balanced through a combination of oral intake and excretion by the kidneys. The rate of fluid intake is largely governed by thirst, although your habits can increase your intake far above the amount necessary. The rate of fluid excreted by your kidneys is greatly influenced by the production of anti-diuretic hormone (ADH), also known as vasopressin.
Your body makes ADH in the hypothalamus and stores the hormone in your pituitary gland, a small gland located in the base of your brain. ADH is released into your bloodstream when your body starts to become dehydrated. ADH then concentrates the urine by triggering the kidney tubules to release water back into your bloodstream rather than excreting as much water into your urine.
The way in which your system is disrupted determines which form of diabetes insipidus you have:
- Central diabetes insipidus. The cause of central diabetes insipidus in adults is usually damage to the pituitary gland or hypothalamus. This damage disrupts the normal production, storage and release of ADH.
The damage is commonly due to surgery, a tumor, an illness (such as meningitis), inflammation or a head injury. For children, the cause may be an inherited genetic disorder. In some cases the cause is unknown.
- Nephrogenic diabetes insipidus. Nephrogenic diabetes insipidus occurs when there’s a defect in the kidney tubules — the structures in your kidneys that cause water to be excreted or reabsorbed. This defect makes your kidneys unable to properly respond to ADH.
The defect may be due to an inherited (genetic) disorder or a chronic kidney disorder. Certain drugs, such as lithium or the antiviral medications cidofovir and foscarnet (Foscavir), also can cause nephrogenic diabetes insipidus.
- Gestational diabetes insipidus. Gestational diabetes insipidus is rare and occurs only during pregnancy and when an enzyme made by the placenta — the system of blood vessels and other tissue that allows the exchange of nutrients and waste products between a mother and her baby — destroys ADH in the mother.
- Primary polydipsia. This condition — also known as dipsogenic diabetes insipidus or psychogenic polydipsia — can cause excretion of large volumes of dilute urine. Rather than a problem with ADH production or damage, the underlying cause is intake of excessive fluids.
Prolonged excessive water intake by itself can damage the kidneys and suppress ADH, making your body unable to concentrate urine. Primary polydipsia can be the result of abnormal thirst caused by damage to the thirst-regulating mechanism, situated in the hypothalamus. Primary polydipsia has also been linked to mental illness.
In some cases of diabetes insipidus, doctors never determine a cause.
Risk factors for diabetes insipidus
Nephrogenic diabetes insipidus that’s present at or shortly after birth usually has a genetic cause that permanently alters the kidneys’ ability to concentrate the urine. Nephrogenic diabetes insipidus usually affects males, though women can pass the gene on to their children.
Complications of diabetes insipidus
Dehydration
Except for primary polydipsia, which causes you to retain too much water, diabetes insipidus can cause your body to retain too little water to function properly, and you can become dehydrated. Dehydration can cause:
- Dry mouth
- Changes in skin elasticity
- Low blood pressure (hypotension)
- Elevated blood sodium (hypernatremia)
- Fever
- Headache
- Rapid heart rate
- Weight loss
Electrolyte imbalance
Diabetes insipidus can also cause an electrolyte imbalance. Electrolytes are minerals in your blood — such as sodium and potassium — that maintain the balance of fluids in your body. Electrolyte imbalance can cause symptoms, such as:
- Fatigue or lethargy
- Nausea
- Loss of appetite
- Muscle cramps
- Confusion
Diagnosis of diabetes insipidus
Since the signs and symptoms of diabetes insipidus can be caused by other conditions, your doctor will perform a number of tests. If your doctor determines you have diabetes insipidus, he or she will need to determine which type of diabetes insipidus you have, because the treatment is different for each form of the disease.
Some of the tests doctors commonly use to diagnose and determine the type of diabetes insipidus and in some cases, its cause, include:
Water deprivation test. This test confirms the diagnosis and helps determine the cause of diabetes insipidus. Under medical supervision, you’ll be asked to stop drinking fluids for a time so that your doctor can measure changes in your body weight, urine output and the concentration of your urine and blood when fluids are withheld.
Your doctor may also measure blood levels of ADH or administer synthetic ADH during this test. The water deprivation test is performed under close supervision in children and pregnant women to make sure no more than 5 percent of body weight is lost during the test.
Urinalysis. Urinalysis is the physical and chemical examination of urine. If your urine is less concentrated — meaning the amount of water is high relative to other excreted substances — it could be due to diabetes insipidus.
Magnetic resonance imaging (MRI). An MRI of the head is a noninvasive procedure that uses a powerful magnetic field and radio waves to construct detailed pictures of brain tissues. Your doctor may want to perform an MRI to look for abnormalities in or near the pituitary gland.
Genetic screening
If your doctor suspects an inherited form of diabetes insipidus, he or she will look at your family history of polyuria and may suggest genetic screening.
Treatment of diabetes insipidus
Treatment of diabetes insipidus depends on what form of the condition you have. Treatment options for the most common types of diabetes insipidus include:
Central diabetes insipidus. Because the cause of this form of diabetes insipidus is a lack of anti-diuretic hormone (ADH), treatment is usually with a synthetic hormone called desmopressin. You can take desmopressin as a nasal spray, as oral tablets or by injection.
The synthetic hormone will eliminate the increase in urination. For most people with this form of the condition, desmopressin is safe and effective. If the condition is caused by an abnormality in the pituitary gland or hypothalamus (such as a tumor), your doctor will first treat the abnormality.
Desmopressin should be considered a medication you take as needed. This is because in most people, the deficiency of ADH is not complete, and the amount made by the body can vary day to day.
Taking more desmopressin than needed can result in too much water retention and low sodium levels in the blood. Symptoms of low sodium include lethargy, headache, nausea and, in severe cases, seizures.
In mild cases of central diabetes insipidus, you may need only to increase your water intake.
Nephrogenic diabetes insipidus. This condition is the result of your kidneys not properly responding to ADH, so desmopressin is not a treatment option. Instead, your doctor may prescribe a low-salt diet to help reduce the amount of urine your kidneys make. You’ll also need to drink enough water to avoid dehydration.
The drug hydrochlorothiazide, used alone or with other medications, may improve symptoms. Although hydrochlorothiazide is a diuretic (usually used to increase urine output), in some cases it can reduce urine output for people with nephrogenic diabetes insipidus.
If symptoms from nephrogenic diabetes insipidus are due to medications you’re taking, stopping these medicines may help; however, don’t stop taking any medication without first talking to your doctor.
Gestational diabetes insipidus. Treatment for most cases of gestational diabetes insipidus is with the synthetic hormone desmopressin. In rare cases, this form of the condition is caused by an abnormality in the thirst mechanism. In these rare cases, doctors don’t prescribe desmopressin.
Primary polydipsia. There is no specific treatment for this form of diabetes insipidus, other than decreasing the amount of fluid intake. However, if the condition is caused by mental illness, treating the mental illness may relieve the symptoms.
Lifestyle and home remedies for diabetes insipidus
If you have diabetes insipidus:
- Prevent dehydration. As long as you take your medication and have access to water when the medication’s effects wear off, you’ll prevent serious problems. Plan ahead by carrying water with you wherever you go, and keep a supply of medication in your travel bag, at work or at school.
- Wear a medical alert bracelet or carry a medical alert card in your wallet. If you have a medical emergency, a health care professional will recognize immediately your need for special treatment.
- Hole’s Essentials of Human Anatomy and Physiology 13th edition. Published by McGraw-Hill Education, 2 Penn Plaza, New York, NY 10121.[↩]
- NHS. Causes of dehydration. http://www.nhs.uk/Conditions/Dehydration/Pages/Causes.aspx[↩]
- Thomas DR, Cote TR, Lawhorne L, Levenson SA, Rubestein LZ, Smith DA et al. (2008). Understanding clinical dehydration and its treatment. J Am Med Dir Assoc 9, 292–301. https://www.ncbi.nlm.nih.gov/pubmed/18519109[↩]
- NHS. Dehydration – Symptoms. http://www.nhs.uk/Conditions/Dehydration/Pages/Symptoms.aspx[↩]
- Mayo Foundation for Medical Education and Research. Dehydration. http://www.mayoclinic.org/diseases-conditions/dehydration/home/ovc-20261061[↩][↩]
- Ritz P, Berrut G (2005). The importance of good hydration for day-to-day health. Nutr Rev 63, S6–S13. https://www.ncbi.nlm.nih.gov/pubmed/16028567[↩]
- Shirreffs SM (2005). The importance of good hydration for work and exercise performance. Nutr Rev 63, S14–S21. https://www.ncbi.nlm.nih.gov/pubmed/16028568[↩]
- Roncal-Jimenez C, Lanaspa M, A, Jensen T, Sanchez-Lozada L, G, Johnson R, J, Mechanisms by Which Dehydration May Lead to Chronic Kidney Disease. Ann Nutr Metab 2015;66(suppl 3):10-13. https://www.karger.com/Article/FullText/381239[↩][↩]
- Sharma VM, Sridharan K, Pichan G, and Panwar MR. Influence of heat stress-induced dehydration on mental functions. Ergonomics 29: 791–799, 1986. https://www.ncbi.nlm.nih.gov/pubmed/3743537[↩]
- Gopinathan PM, Pichan G, and Sharma VM. Role of dehydration in heat stress-induced variations in mental performance. Arch Environ Health 43: 15–17, 1988. https://www.ncbi.nlm.nih.gov/pubmed/3355239[↩][↩]
- Cian C, Barraud PA, Melin B, and Raphel C. Effects of fluid ingestion on cognitive function after heat stress or exercise-induced dehydration. Int J Psychophysiol 42: 243–251, 2001. https://www.ncbi.nlm.nih.gov/pubmed/11812391[↩]
- Kayser-Jones J, Schell ES, Porter C, Barbaccia JC, and Shaw H. Factors contributing to dehydration in nursing homes: inadequate staffing and lack of professional supervision. J Am Geriatr Soc 47: 1187–1194, 1999. https://www.ncbi.nlm.nih.gov/pubmed/10522951[↩]
- Kleiner SM. Water: an essential but overlooked nutrient. J Am Diet Assoc 99: 200–206, 1999. https://www.ncbi.nlm.nih.gov/pubmed/9972188[↩]
- Phillips PA, Bretherton M, Risvanis J, Casley D, Johnston C, and Gray L. Effects of drinking on thirst and vasopressin in dehydrated elderly men. Am J Physiol Regul Integr Comp Physiol 264: R877–R881, 1993. http://ajpregu.physiology.org/content/ajpregu/264/5/R877.full.pdf[↩]
- Phillips PA, Rolls BJ, Ledingham JGG, Forsling ML, Morton JJ, Crowe MB, and Wollner L. Reduced thirst after water deprivation in healthy elderly men. N Engl J Med 311: 753–759, 1984. https://www.ncbi.nlm.nih.gov/pubmed/6472364[↩]
- U.S. National Library of Medicine. Dehydration. https://medlineplus.gov/dehydration.html[↩][↩][↩]
- Mayo Foundation for Medical Education and Research. Dehydration – Symptoms and causes. http://www.mayoclinic.org/diseases-conditions/dehydration/symptoms-causes/dxc-20261072[↩][↩]
- NHS. Symptoms of dehydration. http://www.nhs.uk/Conditions/Dehydration/Pages/Symptoms.aspx[↩][↩]
- National Collaborating Centre for Women’s and Children’s Health (UK). Diarrhoea and Vomiting Caused by Gastroenteritis: Diagnosis, Assessment and Management in Children Younger than 5 Years. London: RCOG Press; 2009 Apr. (NICE Clinical Guidelines, No. 84.) 4, Assessing dehydration and shock. Available from: https://www.ncbi.nlm.nih.gov/books/NBK63845/[↩][↩][↩]
- Centers for Disease Control and Prevention. Rehydration Therapy. https://www.cdc.gov/cholera/treatment/rehydration-therapy.html[↩][↩][↩]
- National Collaborating Centre for Women’s and Children’s Health (UK). Diarrhoea and Vomiting Caused by Gastroenteritis: Diagnosis, Assessment and Management in Children Younger than 5 Years. London: RCOG Press; 2009 Apr. (NICE Clinical Guidelines, No. 84.) 5, Fluid management. Available from: https://www.ncbi.nlm.nih.gov/books/NBK63837/[↩][↩][↩][↩][↩]
- Merck Sharp & Dohme Corp. Dehydration and Fluid Therapy in Children. https://www.merckmanuals.com/professional/pediatrics/dehydration-and-fluid-therapy-in-children/oral-rehydration[↩]
- National Collaborating Centre for Women’s and Children’s Health (UK). Diarrhoea and Vomiting Caused by Gastroenteritis: Diagnosis, Assessment and Management in Children Younger than 5 Years. London: RCOG Press; 2009 Apr. (NICE Clinical Guidelines, No. 84.) 5, Fluid management. Available from: https://www.ncbi.nlm.nih.gov/books/NBK63837/ [↩][↩][↩][↩]
- Faruque AS, Mahalanabi D, Islam A, et al. Breast feeding and oral rehydration at home during diarrhoea to prevent dehydration. Archives of Disease in Childhood. 1992;67:1027–9. https://www.ncbi.nlm.nih.gov/pubmed/1520006[↩][↩]
- American College of Sports Medicine. Selecting and Effectively Using Sports Drinks, Carbohydrate Gels and Energy Bars. http://www.acsm.org/docs/brochures/selecting-and-effectively-using-sports-drinks-carbohydrate-gels-and-energy-bars.pdf[↩]
- Shiller LR, Sellin JH. Diarrhea. In: Feldman M, Friedman LS, Brandt LJ, eds. Sleisenger & Fordtran’s Gastrointestinal and Liver Disease. 10th ed. Philadelphia, PA: Elsevier Saunders; 2016:chap 16.[↩]
- U.S. National Library of Medicine. Medline Plus. When you have diarrhea. https://medlineplus.gov/ency/patientinstructions/000121.htm[↩]
- U.S. National Library of Medicine. Medline Plus. Viral gastroenteritis (stomach flu). https://medlineplus.gov/ency/article/000252.htm[↩]
- U.S. National Library of Medicine. Heat emergencies. https://medlineplus.gov/ency/article/000056.htm[↩][↩]





{kind=link}