Contents
- What is an embolic stroke
- Embolic vs Thrombotic stroke
- Causes of embolic stroke
- What causes embolic stroke
- How to prevent embolic stroke
- Embolic stroke symptoms
- Stroke diagnosis
- Embolic stroke treatment
- Stroke recovery
What is an embolic stroke
An embolic stroke is a type of ischemic stroke that occurs if an artery that supplies oxygen-rich blood to the brain becomes blocked by blood clots (emboli) that have come from another part of the body — commonly in your heart and large arteries of the upper chest and neck.
A second important cause of embolism is an irregular heartbeat, known as atrial fibrillation. It creates conditions where clots can form in the heart, dislodge and travel to the brain.
A stroke is a serious life-threatening medical condition that occurs when the blood supply to part of the brain is cut off. Within minutes, brain cells begin to die. If brain cells die or are damaged because of a stroke, symptoms occur in the parts of the body that these brain cells control. Examples of stroke symptoms include sudden weakness; paralysis or numbness of the face, arms, or legs (paralysis is an inability to move); trouble speaking or understanding speech; and trouble seeing.
- Strokes are a medical emergency and urgent treatment is essential.
- A stroke can cause lasting brain damage, long-term disability, or even death.
- Stroke is the no. 5 cause of death and a leading cause of disability in the United States.
The sooner a person receives treatment for a stroke, the less damage is likely to happen.
If you suspect that you or someone else is having a stroke, call your local emergency number immediately and ask for an ambulance.
The main symptoms of stroke can be remembered with the word F.A.S.T.:
- Face – the face may have dropped on one side, the person may not be able to smile, or their mouth or eye may have dropped.
- Arms – the person with suspected stroke may not be able to lift both arms and keep them there because of weakness or numbness in one arm.
- Speech – their speech may be slurred or garbled, or the person may not be able to talk at all despite appearing to be awake.
- Time – it’s time to dial your local emergency number immediately if you see any of these signs or symptoms.
If you have any of these symptoms or if you suspect someone else is having a stroke, you must get to a hospital quickly to begin treatment. Acute stroke therapies try to stop a stroke while it is happening by quickly dissolving the blood clot or by stopping the bleeding.
Post-stroke rehabilitation helps individuals overcome disabilities that result from stroke damage. Drug therapy with blood thinners is the most common treatment for stroke.
Embolic vs Thrombotic stroke
Thrombosis occurs when a blood clot forms either in a vein or an artery even though you are not bleeding. The clot is known as a thrombus. Normally, blood clots only occur when you bleed. The blood gets thicker so that the bleeding stops. If you did not get blood clots, you would bleed to death.
A thrombotic stroke occurs when a blood clot (thrombus) forms in one of the arteries that supply blood to your brain. A clot may be caused by fatty deposits (plaque) that build up in arteries and cause reduced blood flow (atherosclerosis) or other artery conditions.
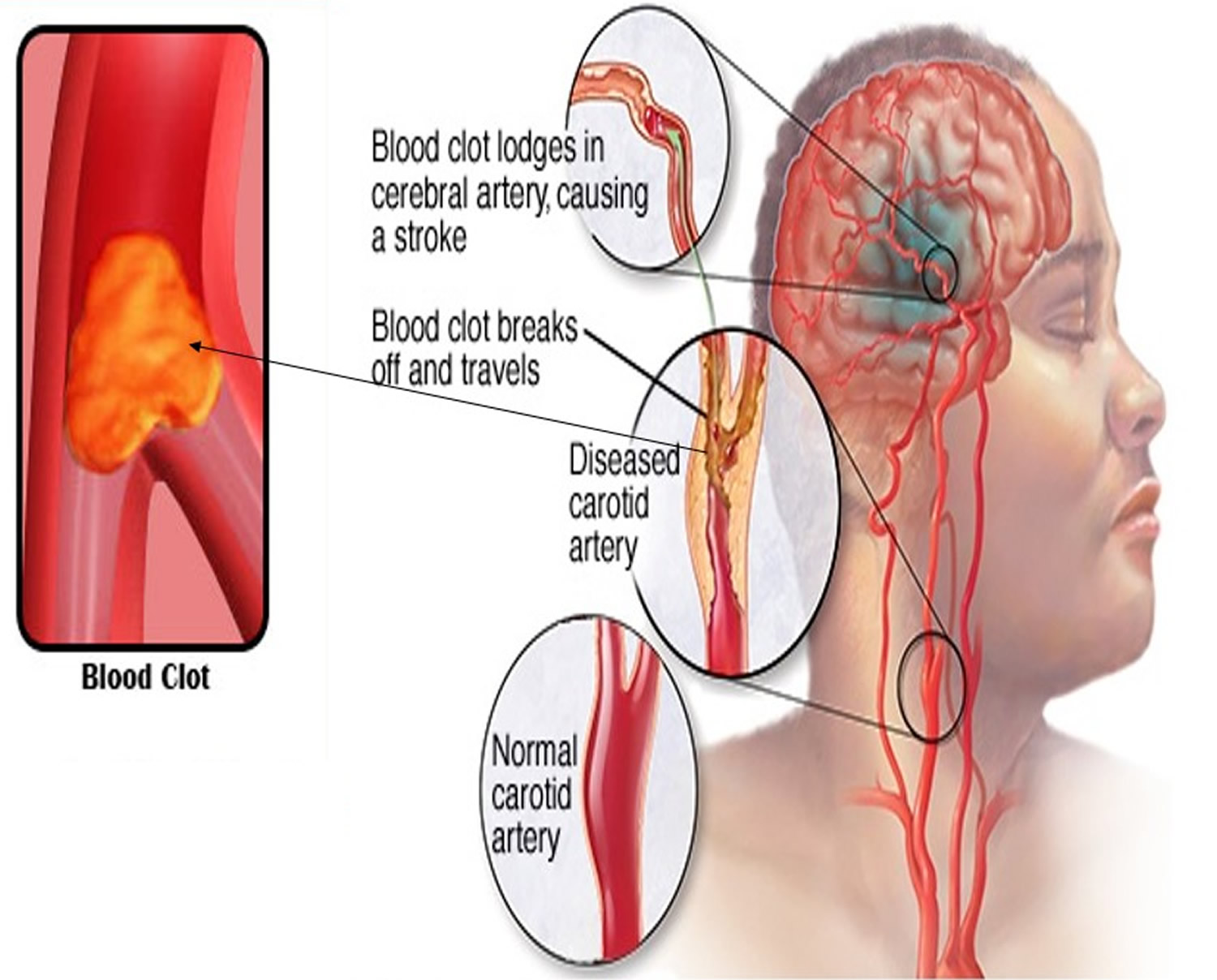
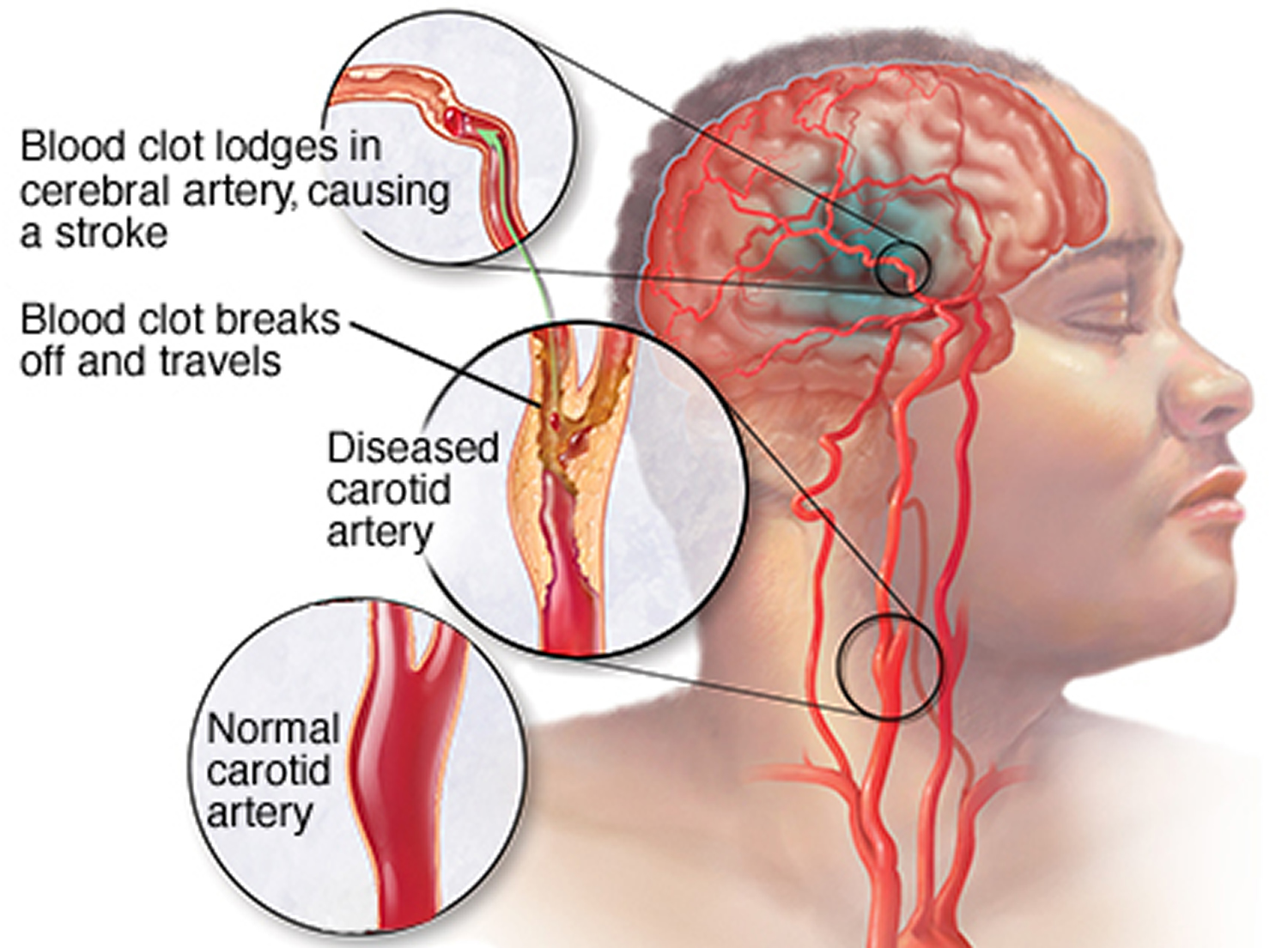
Embolic stroke is caused by a piece of plaque or clot floating in the bloodstream that lodges in one of the blood vessels that supplies the brain.
Figure 1. Embolic stroke
Causes of embolic stroke
An “embolus” is a blood clot or a piece of plaque that acts like a clot. The word “emboli” means there is more than one clot or piece of plaque. When the clot travels from the site where it formed to another location in the body, it is called an embolism.
An arterial embolism may be caused by one or more clots. The clots can get stuck in an artery and block blood flow. The blockage starves tissues of blood and oxygen. This can result in damage or tissue death (necrosis).
An embolic stroke occurs when a blood clot or other debris forms away from your brain — commonly in your heart — and is swept through your bloodstream to lodge in narrower brain arteries. This type of blood clot is called an embolus. Emboli that occur in the brain cause a stroke. Ones that occur in the heart cause a heart attack. Less common sites include the kidneys, intestines, and eyes.
What causes embolic stroke
A stroke occurs when the blood supply to your brain is interrupted or reduced. This deprives your brain of oxygen and nutrients, which can cause your brain cells to die.
A stroke may be caused by a blocked artery (ischemic stroke) or the leaking or bursting of a blood vessel (hemorrhagic stroke). Some people may experience only a temporary disruption of blood flow to their brain (transient ischemic attack, or TIA). This causes what’s known as a mini-stroke, often lasting between a few minutes and several hours. TIAs should be treated urgently, as they’re often a warning sign you’re at risk of having a full stroke in the near future. Seek medical advice as soon as possible, even if your symptoms resolve.
Risk factors for embolic stroke
Many factors can increase your risk of a stroke. Some factors can also increase your chances of having a heart attack. Potentially treatable stroke risk factors include:
Lifestyle risk factors
- Being overweight or obese
- Physical inactivity
- Heavy or binge drinking
- Use of illicit drugs such as cocaine and methamphetamines
Medical risk factors
- High blood pressure (hypertension) — the risk of stroke begins to increase at blood pressure readings higher than 120/80 millimeters of mercury (mm Hg). Your doctor will help you decide on a target blood pressure based on your age, whether you have diabetes and other factors.
- Cigarette smoking or exposure to secondhand smoke.
- High cholesterol.
- Diabetes.
- Obstructive sleep apnea — a sleep disorder in which the oxygen level intermittently drops during the night.
- Cardiovascular disease, including heart failure, heart defects, heart infection or abnormal heart rhythm (atrial fibrillation).
Other factors associated with a higher risk of stroke include:
- Personal or family history of stroke, heart attack or transient ischemic attack.
- Being age 55 or older.
- Race — African-Americans have a higher risk of stroke than do people of other races.
- Gender — Men have a higher risk of stroke than women. Women are usually older when they have strokes, and they’re more likely to die of strokes than are men. Also, they may have some risk from some birth control pills or hormone therapies that include estrogen, as well as from pregnancy and childbirth.
How to prevent embolic stroke
Knowing your stroke risk factors, following your doctor’s recommendations and adopting a healthy lifestyle are the best steps you can take to prevent a stroke. If you’ve had a stroke or a transient ischemic attack (TIA), these measures may help you avoid having another stroke. The follow-up care you receive in the hospital and afterward may play a role as well.
Many stroke prevention strategies are the same as strategies to prevent heart disease. In general, healthy lifestyle recommendations include:
- Controlling high blood pressure (hypertension). One of the most important things you can do to reduce your stroke risk is to keep your blood pressure under control. If you’ve had a stroke, lowering your blood pressure can help prevent a subsequent transient ischemic attack or stroke.
Exercising, managing stress, maintaining a healthy weight, and limiting the amount of sodium and alcohol you eat and drink are all ways to keep high blood pressure in check.. In addition to recommending lifestyle changes, your doctor may prescribe medications to treat high blood pressure.
- Lowering the amount of cholesterol and saturated fat in your diet. Eating less cholesterol and fat, especially saturated fat and trans fats, may reduce the fatty deposits (plaques) in your arteries. If you can’t control your cholesterol through dietary changes alone, your doctor may prescribe a cholesterol-lowering medication.
- Quitting smoking. Smoking raises the risk of stroke for smokers and nonsmokers exposed to secondhand smoke. Quitting tobacco use reduces your risk of stroke.
- Controlling diabetes. You can manage diabetes with diet, exercise, weight control and medication.
- Maintaining a healthy weight. Being overweight contributes to other stroke risk factors, such as high blood pressure, cardiovascular disease and diabetes. Weight loss of as little as 10 pounds may lower your blood pressure and improve your cholesterol levels.
- Eating a diet rich in fruits and vegetables. A diet containing five or more daily servings of fruits or vegetables may reduce your risk of stroke. Following the Mediterranean diet, which emphasizes olive oil, fruit, nuts, vegetables and whole grains, may be helpful.
- Exercising regularly. Aerobic or “cardio” exercise reduces your risk of stroke in many ways. Exercise can lower your blood pressure, increase your level of high-density lipoprotein cholesterol, and improve the overall health of your blood vessels and heart. It also helps you lose weight, control diabetes and reduce stress. Gradually work up to 30 minutes of activity — such as walking, jogging, swimming or bicycling — on most, if not all, days of the week.
- Drinking alcohol in moderation, if at all. Alcohol can be both a risk factor and a protective measure for stroke. Heavy alcohol consumption increases your risk of high blood pressure, ischemic strokes and hemorrhagic strokes. However, drinking small to moderate amounts of alcohol, such as one drink a day, may help prevent ischemic stroke and decrease your blood’s clotting tendency. Alcohol may also interact with other drugs you’re taking. Talk to your doctor about what’s appropriate for you.
- Treating obstructive sleep apnea, if present. Your doctor may recommend an overnight oxygen assessment to screen for obstructive sleep apnea (OSA). If obstructive sleep apnea is detected, it may be treated by giving you oxygen at night or having you wear a small device in your mouth.
- Avoiding illicit drugs. Certain street drugs, such as cocaine and methamphetamines, are established risk factors for a TIA or a stroke. Cocaine reduces blood flow and can cause narrowing of arteries.
Preventive medications
If you’ve had an ischemic stroke or TIA, your doctor may recommend medications to help reduce your risk of having another stroke. These include:
- Anti-platelet drugs. Platelets are cells in your blood that initiate clots. Anti-platelet drugs make these cells less sticky and less likely to clot. The most commonly used anti-platelet medication is aspirin. Your doctor can help you determine the right dose of aspirin for you. Your doctor may also consider prescribing Aggrenox, a combination of low-dose aspirin and the anti-platelet drug dipyridamole, to reduce the risk of blood clotting. If aspirin doesn’t prevent your TIA or stroke, or if you can’t take aspirin, your doctor may instead prescribe an anti-platelet drug such as clopidogrel (Plavix).
- Anticoagulants. These drugs, which include heparin and warfarin (Coumadin), reduce blood clotting. Heparin is fast-acting and may be used over a short period of time in the hospital. Slower acting warfarin may be used over a longer term. Warfarin is a powerful blood-thinning drug, so you’ll need to take it exactly as directed and watch for side effects. Your doctor may prescribe these drugs if you have certain blood-clotting disorders, certain arterial abnormalities, an abnormal heart rhythm or other heart problems. Other newer blood thinners may be used if your TIA or stroke was caused by an abnormal heart rhythm.
Embolic stroke symptoms
The signs and symptoms of a stroke vary from person to person, but usually begin suddenly.
As different parts of your brain control different parts of your body, your symptoms will depend on the part of your brain affected and the extent of the damage.
The main stroke symptoms can be remembered with the word F.A.S.T.:
- Face – the face may have dropped on one side, the person may not be able to smile, or their mouth or eye may have drooped.
- Arms – the person with suspected stroke may not be able to lift both arms and keep them there because of weakness or numbness in one arm.
- Speech – their speech may be slurred or garbled, or the person may not be able to talk at all despite appearing to be awake.
- Time – it’s time to dial your local emergency immediately if you notice any of these signs or symptoms.
It’s important for everyone to be aware of these signs and symptoms, particularly if you live with or care for somebody in a high-risk group, such as someone who is elderly or has diabetes or high blood pressure.
Other possible symptoms
Symptoms in the F.A.S.T. test identify most strokes, but occasionally a stroke can cause different symptoms.
Other symptoms and signs may include:
- Sudden numbness, paralysis or weakness of the face, arm or leg (especially on one side of the body)
- Sudden loss or blurring of vision in one or both eyes
- Dizziness
- Sudden trouble walking, dizziness, loss of balance or coordination
- Sudden confusion, trouble speaking or understanding speech
- Difficulty understanding what others are saying
- Problems with balance and co-ordination
- Difficulty swallowing (dysphagia)
- Sudden and very severe headache resulting in a blinding pain unlike anything experienced before
- Loss of consciousness
However, there may be other causes for these symptoms.
Transient ischemic attack (TIA)
The symptoms of a TIA, also known as a mini-stroke, are the same as a stroke, but tend to only last between a few minutes and a few hours before disappearing completely.
Although the symptoms do improve, a TIA should never be ignored as it’s a serious warning sign of a problem with the blood supply to your brain. It means you’re at an increased risk of having a stroke in the near future.
Stroke diagnosis
To determine the most appropriate treatment for your stroke, your emergency team needs to evaluate the type of stroke you’re having and the areas of your brain affected by the stroke. They also need to rule out other possible causes of your symptoms, such as a brain tumor or a drug reaction. Your doctor may use several tests to determine your risk of stroke, including:
Physical examination. Your doctor will ask you or a family member what symptoms you’ve been having, when they started and what you were doing when they began. Your doctor then will evaluate whether these symptoms are still present. Your doctor will want to know what medications you take and whether you have experienced any head injuries. You’ll be asked about your personal and family history of heart disease, transient ischemic attack or stroke.
Your doctor will check your blood pressure and use a stethoscope to listen to your heart and to listen for a whooshing sound (bruit) over your neck (carotid) arteries, which may indicate atherosclerosis. Your doctor may also use an ophthalmoscope to check for signs of tiny cholesterol crystals or clots in the blood vessels at the back of your eyes.
- Blood tests. You may have several blood tests, which tell your care team how fast your blood clots, whether your blood sugar is abnormally high or low, whether critical blood chemicals are out of balance, or whether you may have an infection. Managing your blood’s clotting time and levels of sugar and other key chemicals will be part of your stroke care.
- Computerized tomography (CT) scan. A CT scan uses a series of X-rays to create a detailed image of your brain. A CT scan can show a hemorrhage, tumor, stroke and other conditions. Doctors may inject a dye into your bloodstream to view your blood vessels in your neck and brain in greater detail (computerized tomography angiography).
- Magnetic resonance imaging (MRI). An MRI uses powerful radio waves and magnets to create a detailed view of your brain. An MRI can detect brain tissue damaged by an ischemic stroke and brain hemorrhages. Your doctor may inject a dye into a blood vessel to view the arteries and veins and highlight blood flow (magnetic resonance angiography, or magnetic resonance venography).
- Carotid ultrasound. In this test, sound waves create detailed images of the inside of the carotid arteries in your neck. This test shows buildup of fatty deposits (plaques) and blood flow in your carotid arteries.
- Cerebral angiogram. In this test, your doctor inserts a thin, flexible tube (catheter) through a small incision, usually in your groin, and guides it through your major arteries and into your carotid or vertebral artery. Then your doctor injects a dye into your blood vessels to make them visible under X-ray imaging. This procedure gives a detailed view of arteries in your brain and neck.
- Echocardiogram. An echocardiogram uses sound waves to create detailed images of your heart. An echocardiogram can find a source of clots in your heart that may have traveled from your heart to your brain and caused your stroke. You may have a transesophageal echocardiogram. In this test, your doctor inserts a flexible tube with a small device (transducer) attached into your throat and down into the tube that connects the back of your mouth to your stomach (esophagus). Because your esophagus is directly behind your heart, a transesophageal echocardiogram can create clear, detailed ultrasound images of your heart and any blood clots.
Embolic stroke treatment
Emergency treatment for stroke depends on whether you’re having an ischemic stroke blocking an artery — the most common kind — or a hemorrhagic stroke that involves bleeding into the brain.
Ischemic stroke
To treat an ischemic stroke, doctors must quickly restore blood flow to your brain.
Emergency treatment with medications
Therapy with clot-busting drugs must start within 3 hours if they are given into the vein — and the sooner, the better. Quick treatment not only improves your chances of survival but also may reduce complications. You may be given:
- Aspirin. Aspirin is an immediate treatment given in the emergency room to reduce the likelihood of having another stroke. Aspirin prevents blood clots from forming.
- Intravenous injection of tissue plasminogen activator (TPA). Some people can benefit from an injection of a recombinant tissue plasminogen activator (TPA), also called alteplase. An injection of TPA is usually given through a vein in the arm. This potent clot-busting drug needs to be given within 4.5 hours after stroke symptoms begin if it’s given in the vein. TPA restores blood flow by dissolving the blood clot causing your stroke, and it may help people who have had strokes recover more fully. Your doctor will consider certain risks, such as potential bleeding in the brain, to determine if TPA is appropriate for you.
Emergency procedures
Doctors sometimes treat ischemic strokes with procedures that must be performed as soon as possible, depending on features of the blood clot:
- Medications delivered directly to the brain. Doctors may insert a long, thin tube (catheter) through an artery in your groin and thread it to your brain to deliver TPA directly into the area where the stroke is occurring. The time window for this treatment is somewhat longer than for intravenous TPA but is still limited.
- Mechanical clot removal. Doctors may use a catheter to maneuver a tiny device into your brain to physically break up or grab and remove the clot.
However, recent studies suggest that for most people, delivering medication directly to the brain (intra-arterial thrombolysis) or using a device to break up or remove clots (mechanical thrombectomy) may not be beneficial. Researchers are working to determine who might benefit from this procedure.
Other procedures to decrease your risk of having another stroke
To decrease your risk of having another stroke or transient ischemic attack, your doctor may recommend a procedure to open up an artery that’s narrowed by fatty deposits (plaques). Doctors sometimes recommend the following procedures to prevent a stroke.
Options will vary depending on your situation:
- Carotid endarterectomy. In a carotid endarterectomy, a surgeon removes plaques from arteries that run along each side of your neck to your brain (carotid arteries). In this procedure, your surgeon makes an incision along the front of your neck, opens your carotid artery and removes plaques that block the carotid artery. Your surgeon then repairs the artery with stitches or a patch made from a vein or artificial material (graft). The procedure may reduce your risk of ischemic stroke. However, a carotid endarterectomy also involves risks, especially for people with heart disease or other medical conditions.
- Angioplasty and stents. In an angioplasty, a surgeon gains access to your carotid arteries most often through an artery in your groin. Here, he or she can gently and safely navigate to the carotid arteries in your neck. A balloon is then used to expand the narrowed artery. Then a stent can be inserted to support the opened artery.
Stroke recovery
Following emergency treatment, stroke care focuses on helping you regain your strength, recover as much function as possible and return to independent living. The impact of your stroke depends on the area of the brain involved and the amount of tissue damaged.
If your stroke affected the right side of your brain, your movement and sensation on the left side of your body may be affected. If your stroke damaged the brain tissue on the left side of your brain, your movement and sensation on the right side of your body may be affected. Brain damage to the left side of your brain may cause speech and language disorders.
In addition, if you’ve had a stroke, you may have problems with breathing, swallowing, balancing and vision.
People who survive a stroke are often left with long-term problems caused by injury to their brain.
Some people need a long period of rehabilitation before they can recover their former independence, while many never fully recover and need support adjusting to living with the effects of their stroke.
Most stroke survivors receive treatment in a rehabilitation program. Your doctor will recommend the most rigorous therapy program you can handle based on your age, overall health and your degree of disability from your stroke. Your doctor will take into consideration your lifestyle, interests and priorities, and the availability of family members or other caregivers.
Your rehabilitation program may begin before you leave the hospital. It may continue in a rehabilitation unit of the same hospital, another rehabilitation unit or skilled nursing facility, an outpatient unit, or your home.
Every person’s stroke recovery is different. Depending on your condition, your treatment team may include:
- Doctor trained in brain conditions (neurologist)
- Rehabilitation doctor (physiatrist)
- Nurse
- Dietitian
- Physical therapist
- Occupational therapist
- Recreational therapist
- Speech therapist
- Social worker
- Case manager
- Psychologist or psychiatrist
- Chaplain
Psychological impact
Two of the most common psychological problems that can affect people after a stroke are:
- Depression – many people experience intense bouts of crying, and feel hopeless and withdrawn from social activities
- Anxiety – where people experience general feelings of fear and anxiety, sometimes punctuated by intense, uncontrolled feelings of anxiety (anxiety attacks)
Feelings of anger, frustration and bewilderment are also common.
You’ll receive a psychological assessment from a member of your healthcare team soon after your stroke to check if you’re experiencing any emotional problems.
Advice should be given to help deal with the psychological impact of stroke. This includes the impact on relationships with other family members and any sexual relationship.
There should also be a regular review of any problems of depression and anxiety, and psychological and emotional symptoms generally.
These problems may settle down over time, but if they are severe or last a long time, doctors can refer people for expert healthcare from a psychiatrist or clinical psychologist.
For some people, medicines and psychological therapies, such as counselling or cognitive behavioral therapy (CBT), can help. Cognitive behavioral therapy (CBT) is a therapy that aims to change the way you think about things to produce a more positive state of mind.
Cognitive impact
Cognitive is a term used by scientists to refer to the many processes and functions our brain uses to process information.
One or more cognitive functions can be disrupted by a stroke, including:
- Communication – both verbal and written
- Spatial awareness – having a natural awareness of where your body is in relation to your immediate environment
- Memory
- Concentration
- Executive function – the ability to plan, solve problems and reason about situations
- Praxis – the ability to carry out skilled physical activities, such as getting dressed or making a cup of tea
As part of your treatment, each one of your cognitive functions will be assessed and a treatment and rehabilitation plan will be created.
You can be taught a wide range of techniques that can help you relearn disrupted cognitive functions, such as recovering your communication skills through speech and language therapy.
There are many ways to compensate for any loss of cognitive function, such as using memory aids, diaries and routines to help plan daily tasks.
Most cognitive functions will return after time and rehabilitation, but you may find they don’t return to the way they were before.
The damage a stroke causes to your brain also increases the risk of developing vascular dementia. This may happen immediately after a stroke or may develop some time after the stroke occurred.
Movement problems
Strokes can cause weakness or paralysis on one side of the body, and can result in problems with co-ordination and balance.
Many people also experience extreme tiredness (fatigue) in the first few weeks after a stroke, and may also have difficulty sleeping, making them even more tired.
As part of your rehabilitation, you should be seen by a physiotherapist, who will assess the extent of any physical disability before drawing up a treatment plan.
Physiotherapy will often involve several sessions a week, focusing on areas such as exercises to improve your muscle strength and overcome any walking difficulties.
The physiotherapist will work with you by setting goals. At first, these may be simple goals, such as picking up an object. As your condition improves, more demanding long-term goals, such as standing or walking, will be set.
A careworker or carer, such as a member of your family, will be encouraged to become involved in your physiotherapy. The physiotherapist can teach you both simple exercises you can carry out at home.
If you have problems with movement and certain activities, such as getting washed and dressed, you may also receive help from an occupational therapist. They can find ways to manage any difficulties.
Occupational therapy may involve adapting your home or using equipment to make everyday activities easier, and finding alternative ways of carrying out tasks you have problems with.
Communication problems
After having a stroke, many people experience problems with speaking and understanding, as well as reading and writing.
If the parts of the brain responsible for language are damaged, this is called aphasia, or dysphasia. If there is weakness in the muscles involved in speech as a result of brain damage, this is known as dysarthria.
You should see a speech and language therapist as soon as possible for an assessment and to start therapy to help you with your communication.
This may involve:
- exercises to improve your control over your speech muscles
- using communication aids – such as letter charts and electronic aids
- using alternative methods of communication – such as gestures or writing
Swallowing problems
The damage caused by a stroke can interrupt your normal swallowing reflex, making it possible for small particles of food to enter your windpipe.
Problems with swallowing are known as dysphagia. Dysphagia can lead to damage to your lungs, which can trigger a lung infection (pneumonia).
You may need to be fed using a feeding tube during the initial phases of your recovery to prevent any complications from dysphagia.
The tube is usually put into your nose and passed into your stomach (nasogastric tube), or it may be directly connected to your stomach in a minor surgical procedure carried out using local anesthetic (percutaneous endoscopic gastrostomy, or PEG).
In the long term, you’ll usually see a speech and language therapist several times a week for treatment to manage your swallowing problems.
Treatment may involve tips to make swallowing easier, such as taking smaller bites of food and advice on posture, and exercises to improve control of the muscles involved in swallowing.
Visual problems
Stroke can sometimes damage the parts of the brain that receive, process and interpret information sent by the eyes.
This can result in losing half the field of vision – for example, only being able to see the left- or right hand side of what’s in front of you.
Strokes can also affect the control of the movement of the eye muscles. This can cause double vision.
If you have any problems with your vision after a stroke, you’ll be referred to an eye specialist called an orthoptist, who can assess your vision and suggest possible treatments.
For example, if you’ve lost part of your field of vision, you may be offered eye movement therapy. This involves exercises to help you look to the side with the reduced vision.
You may also be given advice about particular ways to perform tasks that can be difficult if your vision is reduced on one side, such as getting dressed.
Bladder and bowel control
Some strokes damage the part of the brain that controls bladder and bowel movements. This can result in urinary incontinence and difficulty with bowel control.
Some people may regain bladder and bowel control quite quickly, but if you still have problems after leaving hospital, help is available from the hospital, your GP, and specialist continence advisers.
Don’t be embarrassed – seek advice if you have a problem, as there are lots of treatments that can help.
These include:
- bladder retraining exercises
- medications
- pelvic floor exercises
- using incontinence products
Sex after a stroke
Having sex won’t put you at higher risk of having a stroke. There’s no guarantee you won’t have another stroke, but there’s no reason why it should happen while you’re having sex.
Even if you’ve been left with a severe disability, you can experiment with different positions and find new ways of being intimate with your partner.
Be aware that some medications can reduce your sex drive (libido), so make sure your doctor knows if you have a problem – there may be other medicines that can help.
Some men may experience erectile dysfunction after having a stroke. Speak to your GP or rehabilitation team if this is the case, as there are a number of treatments available that can help.
Driving after a stroke
If you’ve had a stroke or TIA, you can’t drive for one month. Whether you can return to driving depends on what long-term disabilities you may have and the type of vehicle you drive.
It’s often not physical problems that can make driving dangerous, but problems with concentration, vision, reaction time and awareness that can develop after a stroke.
Your doctor can advise you on whether you can start driving again a month after your stroke, or whether you need further assessment at a mobility center.
Preventing further strokes
If you’ve had a stroke, your chances of having another one are significantly increased.
You’ll usually require long-term treatment with medications aimed at improving the underlying risk factors for your stroke.
For example:
- medication – to help lower your blood pressure
- anticoagulants or antiplatelets – to reduce your risk of blood clots
- statins – to lower your cholesterol levels
You’ll also be encouraged to make lifestyle changes to improve your general health and lower your stroke risk, such as:
- eating a healthy diet
- exercising regularly
- stopping smoking if you smoke
- cutting down on the amount of alcohol you drink
Caring for someone who’s had a stroke
There are many ways you can provide support to a friend or relative who’s had a stroke to speed up their rehabilitation process.
These include:
- helping them practise physiotherapy exercises in between their sessions with the physiotherapist
- providing emotional support and reassurance their condition will improve with time
- helping motivate them to reach their long-term goals
- adapting to any needs they may have, such as speaking slowly if they have communication problems
Caring for somebody after a stroke can be a frustrating and lonely experience. The advice outlined below may help.
Be prepared for changed behavior
Someone who’s had a stroke can often seem as though they’ve had a change in personality and appear to act irrationally at times. This is the result of the psychological and cognitive impact of a stroke.
They may become angry or resentful towards you. Upsetting as it may be, try not to take it personally.
It’s important to remember they’ll often start to return to their old self as their rehabilitation and recovery progresses.
Try to remain patient and positive
Rehabilitation can be a slow and frustrating process, and there will be periods of time when it appears little progress has been made.
Encouraging and praising any progress, no matter how small it may appear, can help motivate someone who’s had a stroke to achieve their long-term goals.
Make time for yourself
If you’re caring for someone who’s had a stroke, it’s important not to neglect your own physical and psychological wellbeing. Socializing with friends or pursuing leisure interests will help you cope better with the situation.
Ask for help
There are a wide range of support services and resources available for people recovering from strokes, and their families and carers. This ranges from equipment that can help with mobility, to psychological support for carers and families.
The hospital staff involved with the rehabilitation process can provide advice and relevant contact information.





{kind=link}