
Contents
What is erysipelas
Erysipelas is a superficial form of cellulitis, a potentially serious bacterial infection affecting your skin. Erysipelas affects the outermost layer of your skin and the local lymph nodes. Erysipelas affects the upper dermis and extends into the superficial cutaneous lymphatics. Erysipelas is also known as St. Anthony’s fire, with reference to the intense rash associated with it.
Erysipelas rash is normally one-sided, except on the face where it is occasionally bilateral. Compared to cellulitis the edge is more well-demarcated. The skin is red, hot and tender
Erysipelas most often affects infants and the elderly, but can affect anyone in any age group.
The typical erysipelas symptom is a painful and shiny light-red swelling of a quite clearly defined area of skin. Red streaks leading from that area may be a sign that the infection has started to spread along the lymph vessels too 1). In more severe cases, blisters may form as well. Nearby lymph nodes sometimes swell up and become more sensitive to pressure. People usually have a fever and generally feel unwell right from the start of the infection, when the skin first turns red.
Risk factors are similar to those for other forms of cellulitis.
Factors that increase the risk of developing erysipelas infection include:
- Previous episode(s) of erysipelas
- Breaks in the skin barrier due insect bites, ulcers and chronic skin conditions such as psoriasis, athlete’s foot and eczema
- Skin wounds
- Current or prior injury (e.g., trauma, surgical wounds, radiotherapy)
- In newborns, exposure of the umbilical cord and vaccination site injury
- Nasopharyngeal infection
- Venous disease (e.g., gravitational eczema, leg ulceration)
- Poor circulation in the legs (peripheral vascular disease)
- Lymphedema
- Chronic lower leg swelling (edema)
- Immune deficiency or weakened immune system due to underlying illness or medication, such as:
- Diabetes
- Alcoholism
- Obesity
- Human immunodeficiency virus (HIV)
- Nephrotic syndrome
- Pregnancy
- Athlete’s foot (tinea pedis)
- Bites from insects, animals, or other humans
- Intravenous drug abuse
Erysipelas treatment
An oral antibiotic (taken by mouth) must be given as early as possible and continued until the recommended course is completed. The antibiotic given to you will depend on your local trusts antimicrobial guidelines. If the condition is not improving, higher doses and longer courses may be required. More severe cellulitis and erysipelas are likely to need antibiotic injections or infusions in hospital.
Most people are treated with a form of penicillin, so it is extremely important that you tell your doctor if you are allergic to penicillin.
As long as the affected area is red, swollen and hot, it should be rested. In cellulitis or erysipelas of the leg, the foot should be rested higher than the hip to allow gravity to reduce the swelling.
Failure to improve to appropriate treatment may lead your doctor to seek a specialist opinion as sometimes this condition can mimic others.
It is important that any breaks in the skin, for example due to athlete’s foot or eczema, are treated to prevent repeated episodes of cellulitis. Your doctor may prescribe topical medication (in a cream) for this. Any leg swelling after the skin infection has settled should be treated with compression stockings until the swelling has gone completely.
If there are repeated episodes of cellulitis or erysipelas, the doctor may suggest long-term preventative antibiotic treatment.
Figure 1. Skin structure

Figure 2. Structure and skin cells of the Epidermis
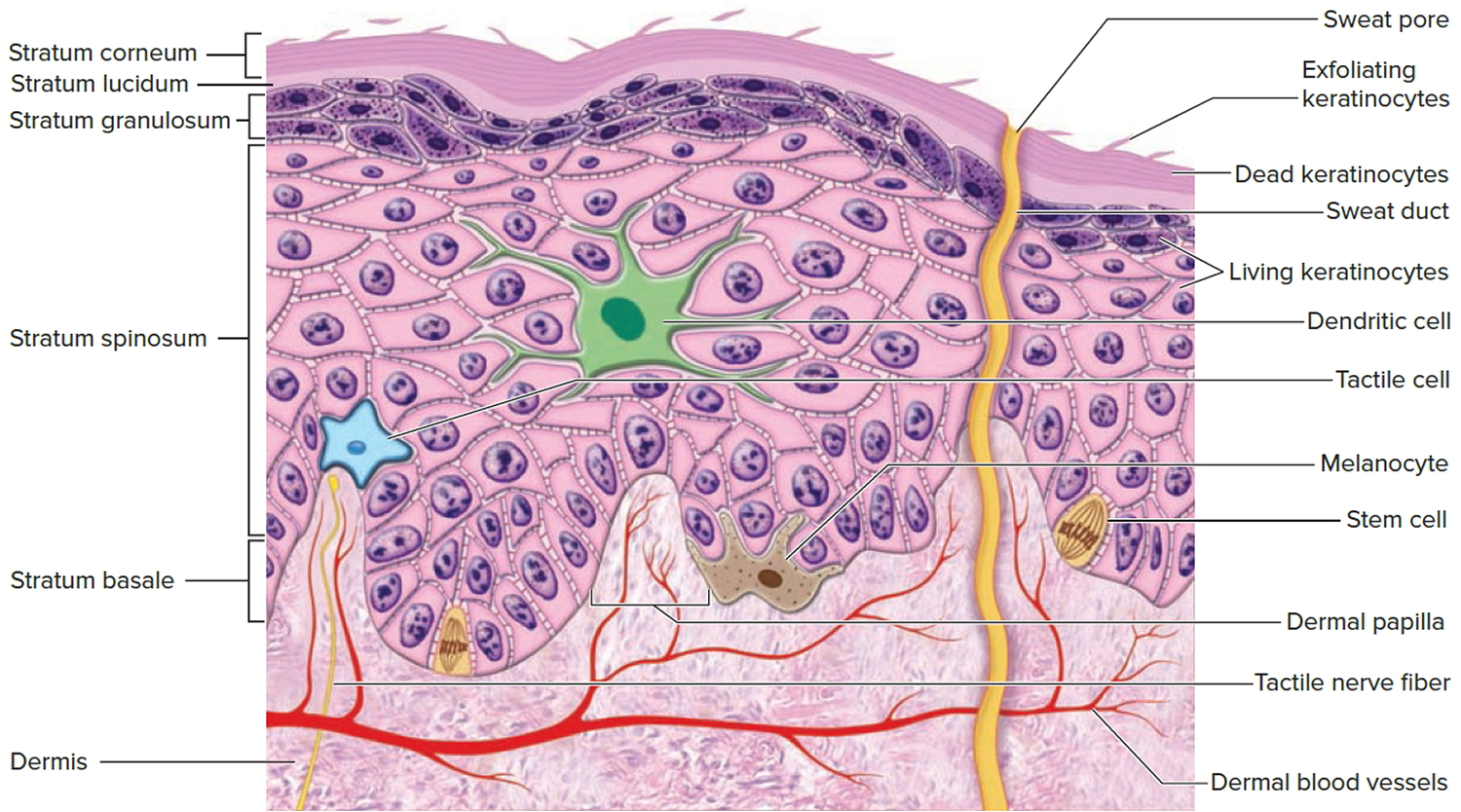
Figure 3. Erysipelas face

Figure 4. Erysipelas cheek

Is erysipelas contagious?
No. because erysipelas and cellulitis affect the deeper layers of the skin. Erysipelas and cellulitis are different from impetigo (see below), which is a superficial infection and is easily passed to other people.
Factors that increase the risk of developing erysipelas infection include:
- Previous episode(s) of erysipelas
- Breaks in the skin barrier due insect bites, ulcers and chronic skin conditions such as psoriasis, athlete’s foot and eczema
- Skin wounds
- Current or prior injury (e.g., trauma, surgical wounds, radiotherapy)
- In newborns, exposure of the umbilical cord and vaccination site injury
- Nasopharyngeal infection
- Venous disease (e.g., gravitational eczema, leg ulceration)
- Poor circulation in the legs (peripheral vascular disease)
- Lymphedema
- Chronic lower leg swelling (edema)
- Immune deficiency or weakened immune system due to underlying illness or medication, such as:
- Diabetes
- Alcoholism
- Obesity
- Human immunodeficiency virus (HIV)
- Nephrotic syndrome
- Pregnancy
- Athlete’s foot (tinea pedis)
- Bites from insects, animals, or other humans
- Intravenous drug abuse
Can cellulitis and erysipelas be cured?
Yes, and treatment with antibiotics at an early stage is important to prevent the spread of infection and the complications listed below.
Erysipelas vs Cellulitis
Erysipelas is a form of cellulitis with marked superficial skin inflammation, typically affecting the lower limbs and the face. Erysipelas affects the upper layers of the skin. Erysipelas and cellulitis are skin infections that can develop if bacteria enter your skin through cuts or sores. Both infections make your skin swell, become red and tender. Erysipelas usually only affects the uppermost layers of skin, while cellulitis typically reaches deeper layers of tissue. Provided the right treatment is started early enough, these infections usually clear up without any lasting effects. Left untreated, they sometimes lead to serious complications.
If the infection is left untreated for too long, cellulitis can result in pockets of pus (abscesses) or the spread of bacteria into the bloodstream (bacteremia). However, most cases of cellulitis resolve with appropriate antibiotic therapy.
Cellulitis is a common bacterial infection of the lower dermis and subcutaneous tissue that is characterized by redness, pain, and lymphangitis. Cellulitis is most often caused by the bacteria Streptococcus or Staphylococcus aureus. These bacteria are able to enter the skin through small cracks (fissures), causing the sudden appearance of redness, swelling, and warmth in the skin.
Cellulitis results in a localized area of red, painful, swollen skin, and systemic symptoms. Up to 40% of people with cellulitis have systemic illness such as fever, chills, and general fatigue 2). Similar symptoms are experienced with the more superficial infection, such as erysipelas, so cellulitis and erysipelas are often considered together.
In cellulitis, the reddened skin is less clearly defined than it is in erysipelas, and it is often dark-red or slightly purplish. Unlike erysipelas, the infection caused by cellulitis reaches the lower layers of skin and the tissue beneath it. The infection can spread along tendons and muscles, and pus may form.
Both infections are most common on the feet or lower legs, but they may also affect other parts of the body. Erysipelas can develop on the face, and cellulitis may also occur on the palm of the hand, for instance. There it can spread in a V-shape in the tendon sheaths between the thumb, wrist and little finger.
Cellulitis and erysipelas can result in local necrosis and abscess formation. Around a quarter of people have more than one episode of cellulitis within 3 years.
Erysipelas and cellulitis are among the most common skin conditions, but it’s not known exactly how often they occur. According to some studies, 2 out of 10,000 people are affected each year. Other research suggests that more than 250 out of 10,000 people are affected 3).
Cellulitis affects people of all ages and races. Predispositions to cellulitis include:
- Previous episode(s) of cellulitis
- Fissuring of toes or heels, eg due to athlete’s foot, tinea pedis or cracked heels
- Venous disease, e.g., gravitational eczema, leg ulceration, and/or lymphedema
- Current or prior injury, e.g., trauma, surgical wounds, radiotherapy
- Immunodeficiency, e.g., human immunodeficiency virus infection (HIV)
- Immune suppressive medications
- Diabetes
- Chronic kidney disease
- Chronic liver disease
- Obesity
- Pregnancy
- Alcoholism
Many people falsely attribute an episode of cellulitis to an unseen spider bite. Documented spider bites have not led to cellulitis.
Figure 5. Cellulitis

Causes and risk factors of cellulitis
Erysipelas is often caused by streptococcus bacteria, while cellulitis is typically caused by staphylococcus bacteria. Both types of bacteria may cause either erysipelas or cellulitis, though.
Bacterial skin infections are more likely to arise if the surface of your skin is damaged, making it easier for bacteria to enter. Because of this, the risk factors include skin problems such as eczema, impetigo, fungal infections such as athlete’s foot, or wounds and ulcers. Erysipelas or cellulitis can also develop following injuries, pin pricks, and insect or animal bites, or if germs get into the wound during an operation.
The risk of infection is particularly high if you have a weakened immune system. The immune system may become weaker due to things like taking certain medications. These include some cancer drugs, corticosteroids and medication commonly used following organ transplants to suppress the body’s immune response.
The risk is also higher in people who are overweight or have diabetes, problems with the circulation of lymph or blood, or have venous insufficiency. Previous erysipelas or cellulitis is considered to be a risk factor too.
Erysipelas vs Impetigo
Impetigo is a contagious bacterial infection of the superficial skin, predominantly occurring in children. There are two forms, the more common non-bullous impetigo, often referred to simply as impetigo, and bullous impetigo.
- Nonbullous impetigo: In nonbullous impetigo, staphylococci and/or streptococci invade a site of minor trauma where exposed proteins allow the bacteria to adhere.
- Bullous impetigo: Bullous impetigo is due to staphylococcal exfoliative toxins (exfoliatin A–D), which target desmoglein 1 (a desmosomal adhesion glycoprotein), and cleave off the superficial epidermis through the granular layer. No trauma is required, as the bacteria can infect intact skin.
Impetigo is characterized by pustules and honey-colored crusted erosions (“school sores”). Impetigo is most often caused by Staphylococcus aureus. Non-bullous impetigo can also be caused by group A beta-hemolytic streptococcus (Streptococcus pyogenes).
Impetigo may be passed on from an infected individual, or arise with no clear source of infection. It often enters the skin at the site of a minor skin injury, or secondarily to another skin condition such as chickenpox.
Impetigo is most common in children (especially boys), but may also affect adults if they have low immunity to the bacteria. It is prevalent worldwide. Peak onset is during summer and it is more prevalent in developing countries.
The following factors predispose to impetigo:
- Atopic dermatitis or eczema
- Scabies
- Skin trauma: chickenpox, insect bite, abrasion, laceration, thermal burn, dermatitis, surgical wound
Management of impetigo
Step 1: General measures
- Cover affected areas where possible
- Wash hands regularly
- Use separate towels and flannels
- Avoid school until the lesions are healed or crusted over, or 48 hours after antibiotics are started
The following steps are used to treat impetigo 4).
- Cleanse the wound; use moist soaks to gently remove crusts
- Apply antiseptic 2–3 times daily for 5 days (povidone iodine, hydrogen peroxide 1% cream, chlorhexidine, superoxidised solution and others)
- First-line treatment is topical fusidic acid for 7-10 days. In cases of fusidic acid resistance use topical mupirocin
- Cover the affected areas.
- Oral antibiotics are recommended if:
- Symptoms are significant or severe (fever, malaise)
- There are more than 3 lesions
- There is a high risk of complications
- The infection is not resolving or is unlikely to resolve.
Suitable oral antibiotics are flucloxacillin 500 mg four times daily for 5 days (adult dose), and in case of allergy or bacterial resistance, trimethoprim + sulphamethoxazole 960 mg, twice daily, for five days (adult dose), erythromycin 800 mg twice daily for 5 days or cephalexin 1 g twice daily for 5 days.
To prevent recurrence:
- Treat carrier sites: apply antiseptic ointment to nostrils
- Wash daily with antibacterial soap or soak in a bleach bath
- Cut nails and keep hands clean
- Identify and treat the source of re-infection, usually another infected person or carrier in the household.
To reduce the chance of passing the infection to another person:
- Avoid close contact with others
- Children must stay away from school until crusts have dried out or for 24 hours after starting oral antibiotics
- Use separate towels and flannels
- Change and launder clothes and linen daily.
Figure 6. Impetigo face

Erysipelas causes
Unlike cellulitis, almost all erysipelas is caused by Group A beta hemolytic streptococci (Streptococcus pyogenes). Staphylococcus aureus, including methicillin resistant strains (MRSA), Streptococcus pneumoniae, Klebsiella pneumoniae, Yersinia enterocolitica, and Haemophilus influenzae have also been found rarely to cause erysipelas.
Some conditions that can lead to erysipelas are:
- A cut in the skin
- Problems with drainage through the veins or lymph system
- Skin sores (ulcers)
Risk factors for developing erysipelas
Factors that increase the risk of developing erysipelas infection include:
- Previous episode(s) of erysipelas
- Breaks in the skin barrier due insect bites, ulcers and chronic skin conditions such as psoriasis, athlete’s foot and eczema
- Skin wounds
- Current or prior injury (e.g., trauma, surgical wounds, radiotherapy)
- In newborns, exposure of the umbilical cord and vaccination site injury
- Nasopharyngeal infection
- Venous disease (e.g., gravitational eczema, leg ulceration)
- Poor circulation in the legs (peripheral vascular disease)
- Lymphedema
- Chronic lower leg swelling (edema)
- Immune deficiency or weakened immune system due to underlying illness or medication, such as:
- Diabetes
- Alcoholism
- Obesity
- Human immunodeficiency virus (HIV)
- Nephrotic syndrome
- Pregnancy
- Athlete’s foot (tinea pedis)
- Bites from insects, animals, or other humans
- Intravenous drug abuse
Erysipelas prevention
Keep your skin healthy by avoiding dry skin and preventing cuts and scrapes. This may reduce the risk for erysipelas. People who have had erysipelas or cellulitis are quite likely to develop the same kind of infection again after completing successful treatment. About one third of people who have had an erysipelas infection get it again.
There are various ways to stop this from happening. If a skin condition like athlete’s foot or eczema made it easier for the infection to occur in the first place, it is important to treat this cause first. Also, it’s important for people who have an increased risk of infection due to diabetes or circulation problems to pay attention to maintaining good foot hygiene.
If bacterial skin infections keep occurring, preventive treatment with antibiotics may be considered. When used for this purpose, the antibiotics need to be taken daily over the course of several months.
Erysipelas symptoms
Symptoms and signs of erysipelas are usually abrupt in onset and often accompanied by fevers, chills and shivering.
Erysipelas predominantly affects the skin of the lower limbs, but when it involves the face it can have a characteristic butterfly distribution on the cheeks and across the bridge of the nose.
- The affected skin has a very sharp, raised border.
- It is bright red, firm and swollen. It may be finely dimpled (like an orange skin).
- It may be blistered, and in severe cases may become necrotic.
- Bleeding into the skin may cause purpura.
- Cellulitis does not usually exhibit such marked swelling, but shares other features with erysipelas, such as pain and increased warmth of affected skin.
- In infants, it often occurs in the umbilicus or diaper/napkin region.
- Bullous erysipelas can be due to streptococcal infection or co-infection with Staphylococcus aureus (including MRSA).
What are the complications of erysipelas?
Sometimes the bacteria that cause erysipelas may travel to the blood. This results in a condition called bacteremia. When this happens, the infection may spread to the heart valves, joints, and bones.
Life-threatening complications are rare. If bacteria enter the bloodstream, they may cause blood poisoning (septicemia). In rare cases, a bacterial skin infection on the face can cause meningitis (inflammation of the membranes covering the brain and spinal cord) or a blood clot in one of the blood vessels in the brain (cerebral venous thrombosis).
If there are complications, only fast treatment can prevent more major damage.
Signs of a more severe infection include the following:
- Severe pain
- Fever, cold sweats, pale skin
- Nausea
- Faster rate of breathing or a racing heart
- Drowsiness, confusion, or other problems with consciousness or awareness
If you notice any of these symptoms, it is important to call the emergency services immediately.
Erysipelas recurs in up to one third of patients due to:
- Persistence of risk factors
- Lymphatic damage (hence impaired drainage of toxins)
Complications are rare but can include:
- Abscess
- Gangrene
- Thrombophlebitis
- Chronic leg swelling
- Infections distant to the site of erysipelas:
- Infective endocarditis (heart valves)
- Septic arthritis
- Bursitis
- Tendonitis
- Post-streptococcal glomerulonephritis (a kidney condition affecting children)
- Cavernous sinus thrombosis (dangerous blood clots that can spread to the brain)
- Streptococcal toxic shock syndrome or septic shock (rare).
Untreated bacterial skin infections can cause various complications. These include the following:
- The spread of pus-producing infection and abscesses: Especially in cellulitis, an infection with pus can spread to deeper tissue (such as muscle tissue). Sometimes the pus builds up in natural spaces or gaps between tissue. An abscess is a sealed, pus-filled space that can develop as a result of various bacterial skin infections. It is mostly made up of dead germs, tissue cells, and immune system cells.
- Lymphedema: Parts of the infected lymphatic vessels may be destroyed following an erysipelas infection. This blocks the flow of lymph (the fluid in the lymphatic system), causing it to build up. That results in permanent swelling and poorer circulation in the tissue, increasing the risk of developing further bacterial skin infections.
Erysipelas prognosis
Prognosis depends on many factors, such as severity of initial infection and any complications and comorbidities which may hinder recovery.
While signs of general illness resolve within a day or two, the skin changes may take some weeks to resolve completely. No scarring occurs.
Cellulitis and erysipelas can become a recurrent, chronic problem and identifying underlying risk factors is essential. If recurrence at the same site is a problem despite prevention strategies, long-term low-dose penicillin can be tried for a couple of years.
Erysipelas recurs in up to one third of patients due to persistence of risk factors and also because erysipelas itself can cause lymphatic damage (hence impaired drainage of toxins) in involved skin which predisposes to further attacks.
Long term preventive treatment with penicillin is often required for recurrent attacks of erysipelas.
How is erysipelas diagnosed?
Doctors can usually tell whether an infection is erysipelas or cellulitis based on the typical symptoms and the appearance of the skin. Your medical history or recent injuries often help to diagnose the problem too.
Further tests aren’t usually needed. It can sometimes help to test fluid from the wound for germs. This is done when doctors think there may be a specific germ causing the infection, for instance because someone’s skin became infected after they were bitten by an animal.
Tests may reveal:
- Raised white cell count
- Raised C-reactive protein (CRP)
- Positive blood culture identifying the organism
MRI and CT are undertaken in case of deep infection.
Erysipelas treatment
Erysipelas and cellulitis are both treated with antibiotics. The medication is delivered directly into a vein using a drip. In milder cases, tablets are enough. People who go to the hospital for treatment usually have to stay for about a week.
The exact type of antibiotic will depend on several factors, such as what type of bacteria doctors think you have. To check the progress of the treatment, the infected area of skin is outlined with a special marker pen. This makes it possible to see whether the antibiotics are having an effect and the infection and redness are going away.
It is also recommended that you cool the swelling and apply moist antiseptic wraps. Anti-inflammatory painkillers like ibuprofen can be used to relieve pain and fever.
If the skin on your face is infected, it’s better to speak or chew as little as possible. If the skin on a leg or foot is infected, it can help to elevate that leg. Bed rest is even recommended in many cases. People are then given injections to prevent thrombosis.
In more severe cellulitis, surgery may be needed to remove pus and dead tissue.
General
- Cold packs and analgesics to relieve local discomfort
- Elevation of an infected limb to reduce local swelling
- Compression stockings
- Wound care with saline dressings that are frequently changed
Antibiotics
- Oral or intravenous penicillin is the antibiotic of first choice.
- Erythromycin, roxithromycin or pristinamycin may be used in patients with penicillin allergy.
- Vancomycin is used for facial erysipelas caused by MRSA
- Treatment is usually for 10–14 days
References [ + ]





{kind=link}