Contents
What is fecal incontinence
Fecal incontinence or bowel incontinence is a term used to describe leakage from the bowel due to poor bowel control. You may also find you have excessive wind or experience staining of your underwear. Poor bowel control can be caused or made worse by a number of things including certain health conditions or medicines taken for other problems.
Incontinence is a term that describes any accidental or involuntary loss of bowel motion, feces or wind from the bowel (fecal or bowel incontinence) or urine from the bladder (urinary incontinence). Incontinence is a widespread condition that ranges in severity from ‘just a small leak’ to complete loss of bladder or bowel control.
The experience of bowel incontinence can vary from person to person. Some people feel a sudden need to go to the toilet but are unable to reach a toilet in time. This is known as urge bowel incontinence.
Other people experience no sensation before soiling themselves, known as passive incontinence or passive soiling, or there might be slight soiling when passing wind.
Some people experience fecal incontinence on a daily basis, whereas for others it only happens from time to time.
It’s thought one in 10 people will be affected by it at some point in their life. It can affect people of any age, although it’s more common in elderly people. It’s also more common in women than men.
- Fecal incontinence or bowel incontinence impacts the lives of more than 18 million Americans.
- Between 2% and 8% of adults have fecal incontinence.
- An estimated 15 percent of people age 70 and older are affected.
- Although fecal incontinence is more common in middle-aged and older adults, it isn’t an inevitable part of aging. It’s often the result of another treatable medical issue or can be a warning sign of a more serious problem.
It’s important to remember that:
- Bowel incontinence isn’t something to be ashamed of – it’s simply a medical problem that’s no different from diabetes or asthma.
- It can be treated – there’s a wide range of successful treatments.
- Bowel incontinence isn’t a normal part of ageing.
- It won’t usually go away on its own – most people need treatment for the condition.
Fecal incontinence can be upsetting and hard to cope with, but it can be treated and managed. In many cases fecal incontinence can also be cured, so make sure you see your doctor.
See your doctor if you or your child develops fecal incontinence. Often, new mothers and other adults are reluctant to tell their doctors about fecal incontinence. But treatments are available, and the sooner you are evaluated, the sooner you may find some relief from your symptoms.
Why bowel incontinence happens?
Bowel incontinence is a symptom of an underlying problem or medical condition.
Many cases are caused by diarrhea, constipation, or weakening of the muscle that controls the opening of the anus.
It can also be caused by long-term conditions such as diabetes, multiple sclerosis and dementia.
The Rectum and Anus
Your rectum and anus are at the end of your large intestine (Figure 1). Normally, the muscles and nerves in and around these two structures sense the presence of waste, allow storage in the rectum, and then move and eliminate stool. Changes in the function of this complex system can interfere with normal stool elimination.
The rectum forms the last 15 cm (6 in.) of the large intestine. The rectum is an expandable organ for the temporary storage of feces. The rectum lies next to the sacrum and generally follows its curvature. The peritoneum firmly attaches the rectum to the sacrum. The rectum ends about 5 centimeters below the tip of the coccyx, where it becomes the anal canal.
The anal canal is the continuation of the large intestine inferior to the rectum. The anal canal is about 3 cm long, it begins where the rectum passes through the levator ani, the muscle that forms the pelvic floor. At its distal end, the anal canal opens to the outside as the anus. Two sphincter muscles guard the anus—an internal anal sphincter muscle, composed of smooth muscle under involuntary control, and an external anal sphincter muscle, composed of skeletal muscle under voluntary control. A portion of the levator ani is responsible for maintaining the anorectal angle, an acute angle between the anus and the rectum that contributes to fecal continence. The anal canal lies entirely external to the abdominopelvic cavity in the perineum.
Internally, the superior half of the anal canal contains longitudinal folds of mucosa, the anal columns. These columns contain the terminal portions of the superior rectal artery and vein (the hemorrhoidal vessels) (see Figure 2). Neighboring anal columns join each other inferiorly at crescent-shaped transverse folds called anal valves. The pockets just superior to these valves are anal sinuses, which release mucus when they are compressed by feces, providing lubrication that eases fecal passage during defecation. The horizontal line along which the anal valves lie is called the pectinate (“comb-shaped”) line. Because the mucosa superior to this line is innervated by visceral sensory fibers, it is relatively insensitive to pain. Inferior to the pectinate line, however, the mucosa is sensitive to pain because it is innervated by somatic nerves.
The wall of the anal canal contains two sphincter muscles: an internal anal sphincter of smooth muscle and an external anal sphincter of skeletal muscle (see Figure 2). The former is a thickening of the circular layer of the muscularis, whereas the latter is a distinct muscle. The external sphincter contracts voluntarily to inhibit defecation, whereas the internal sphincter contracts involuntarily, both to prevent feces from leaking from the anus between defecations and to inhibit defecation during emotional stress. During toilet training, children learn to control the external anal sphincter.
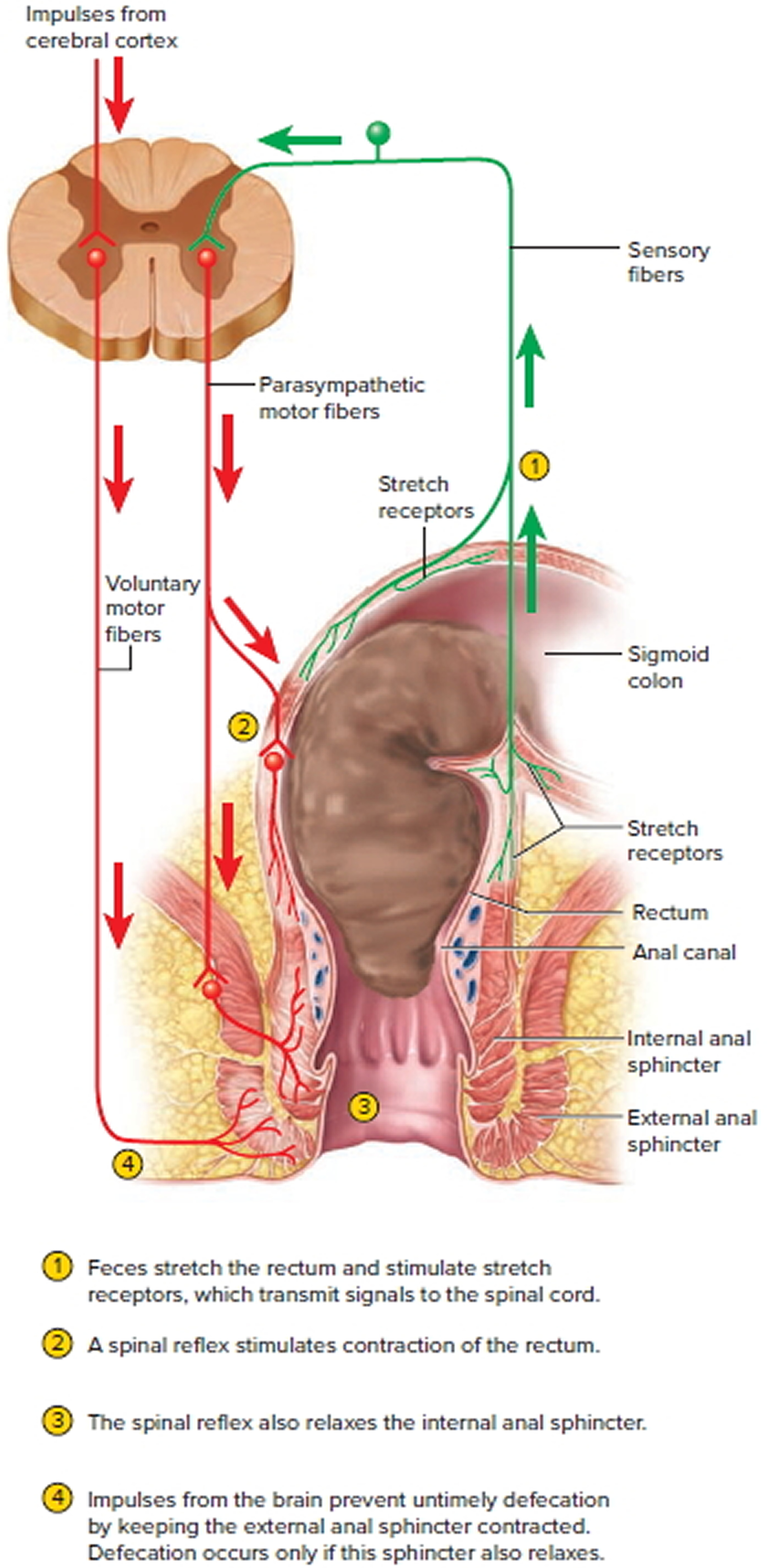
The rectum is usually empty and the anal sphincters contracted. When feces are squeezed into the rectum by mass peristaltic movements, the stretching of the rectal wall initiates the defecation reflex, which account for the urge to defecate that is often felt soon after a meal (Figure 3).
The defecation reflexes involve two reflexes:
- The intrinsic defecation reflex. This reflex is mediated entirely by the myenteric plexus. Stretch signals travel through the plexus to the muscularis of the descending and sigmoid colon and the rectum. This activates a peristaltic wave that drives feces downward, and it relaxes the internal anal sphincter. This reflex is relatively weak, however, and usually requires the cooperative action of the following reflex.
- The parasympathetic defecation reflex. This is a spinal reflex. Its principal events are that stretch signals are transmitted to the spinal cord; motor signals return by way of the pelvic nerves; and these signals intensify peristalsis in the descending and sigmoid colon and rectum while they relax the internal anal sphincter. These reflexes are involuntary and are the sole means of controlling defecation in infants and some people with transecting spinal cord injuries. However, the external anal sphincter is under voluntary control, enabling one to limit defecation to appropriate circumstances.
Voluntary retention of feces is also aided by the puborectalis muscle, which loops around the rectum like a sling and creates a sharp anorectal angle that blocks the passage of feces. Defecation normally occurs only when the external anal sphincter and puborectalis muscle are voluntarily relaxed. The kink in the rectum then straightens out and the sphincter opens to allow the feces to fall away. Defecation is also aided by the voluntary Valsalva maneuver, in which a breath hold and contraction of the abdominal muscles increase abdominal pressure, compress the rectum, and squeeze the feces from it. This maneuver can also initiate the defecation reflex by forcing feces from the descending colon into the rectum. The external anal sphincter and external urethral sphincter are controlled together by inhibitory signals from the brainstem, so as this inhibition is released, defecation is usually accompanied by urination.
Some spinal cord injuries and diseases abolish the voluntary control of the external anal sphincter. The resulting inability to voluntarily retain the feces is called fecal incontinence. If the defecation urge is suppressed, contractions cease in a few minutes and the rectum relaxes. The defecation reflexes reoccur a few hours later or when another mass movement propels more feces into the rectum.
Figure 1. Rectum
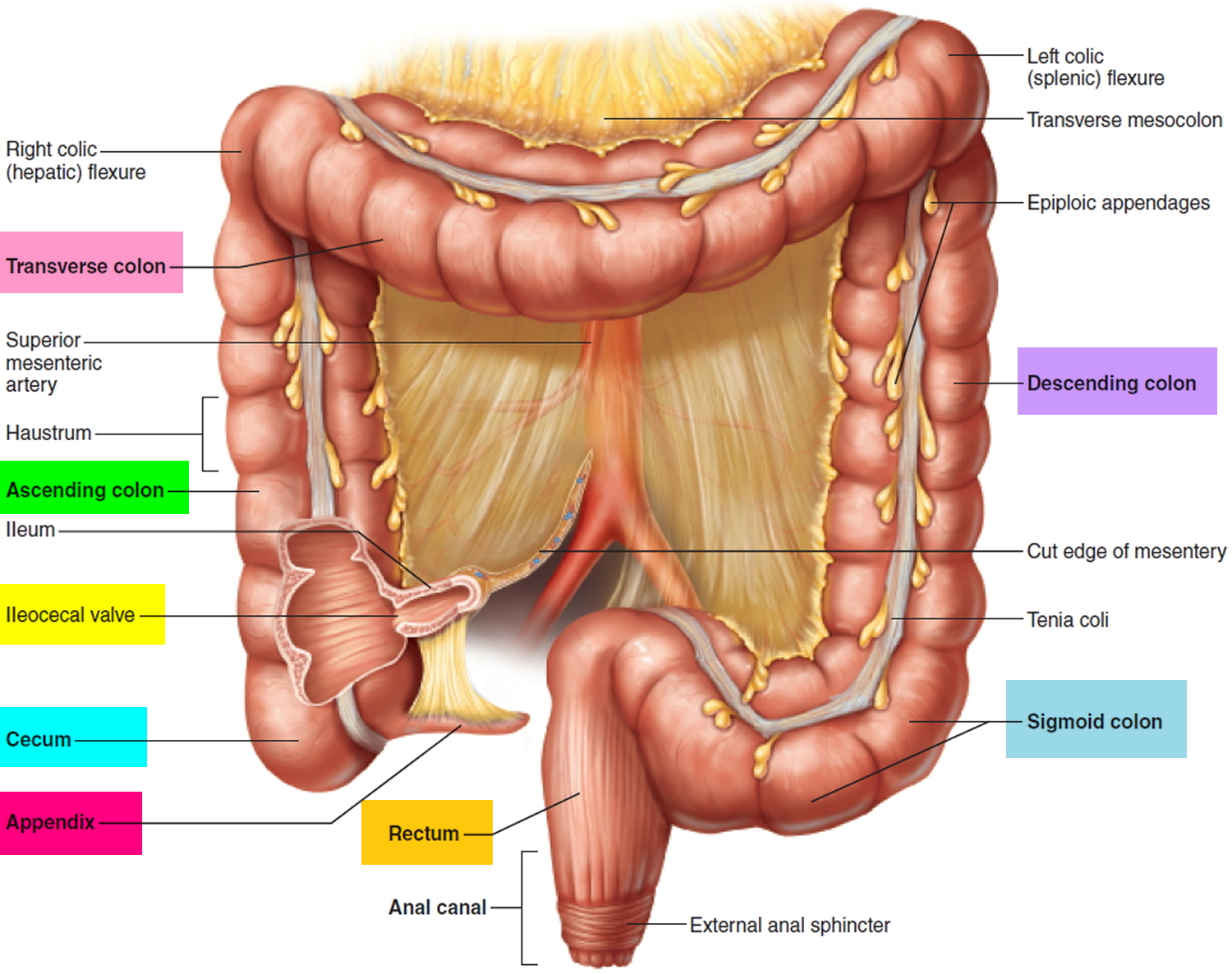
Figure 2. Rectum anatomy and Anus (anal canal)
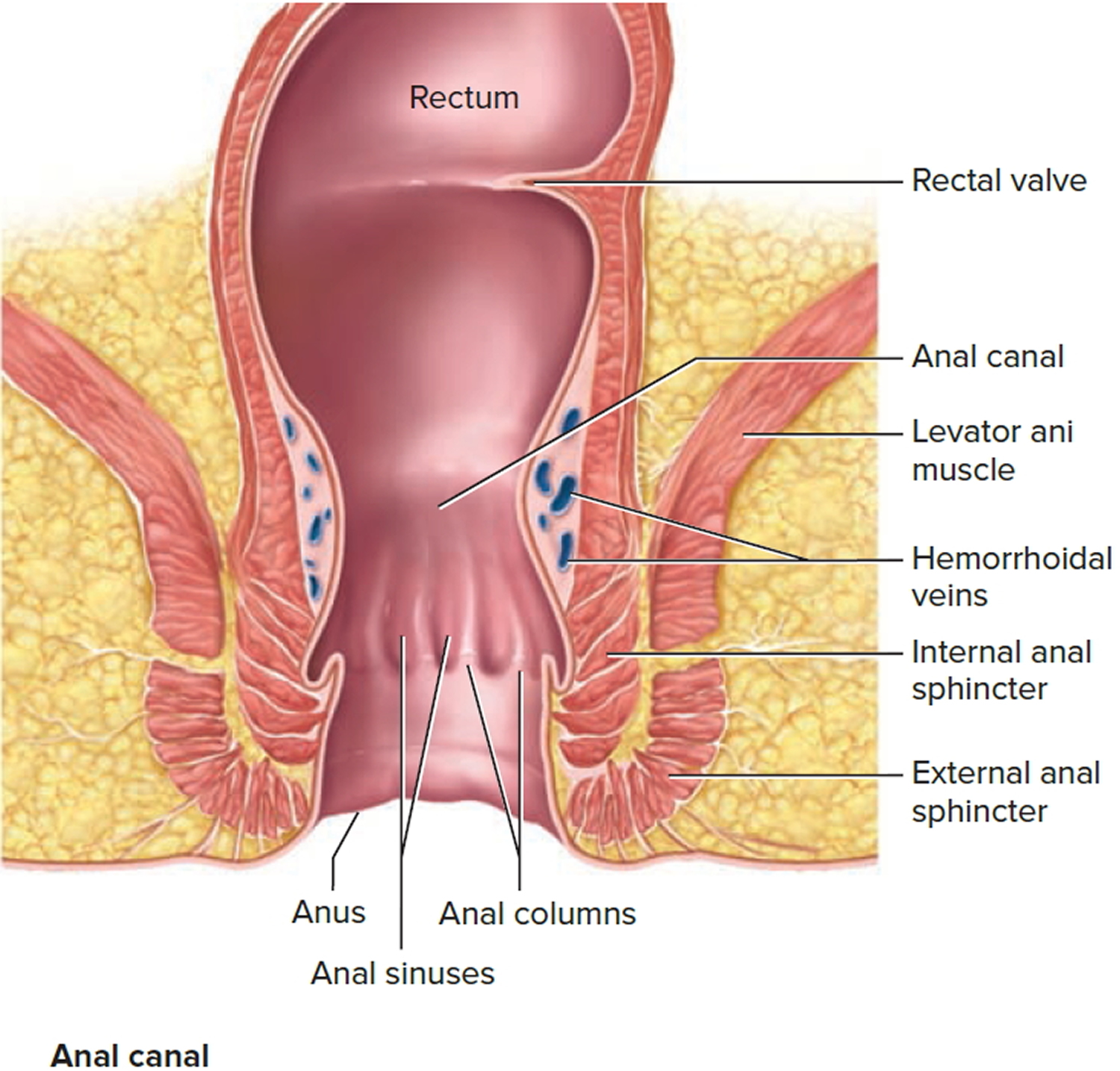
Figure 3. Rectum function and neural control of defecation
Damage to these muscles or nerves are potential causes of fecal incontinence. It may be difficult to hold stool back if muscles at the end of the rectum are damaged during childbirth, or hemorrhoid or cancer surgery. Weak or improperly functioning pelvic floor muscles (which support the organs in the lower abdomen and pelvis) also can contribute to fecal incontinence, as can injury to nerves that sense stool in the rectum or that control the anal sphincters. Childbirth, a habit of straining to pass stool, a spinal cord injury, a stroke and even certain diseases (such as diabetes and multiple sclerosis) can affect these nerves.
Chronic constipation or diarrhea also can result in fecal incontinence. Ongoing constipation can lead to a hard, dry stool in the rectum that’s too hard to pass. As a result, muscles in the rectum and intestines stretch, weakening and allowing watery stool from farther up to leak out around the hard mass. It can also cause nerves in the anus and rectum to become less responsive to the presence of stool. Diarrhea can cause or make fecal incontinence worse, since it’s easier to retain solid stool in the rectum than loose stool.
In addition, changes in the rectum wall that cause the rectum to stiffen (from radiation treatment, rectal surgery or inflammatory bowel disease) may reduce its capacity to hold stool.
Once fecal incontinence is diagnosed and the likely cause is identified, your doctor can discuss treatment options that may be best suited to your situation. It’s not unusual to use multiple approaches to treat fecal incontinence.
What you eat and drink affects stool consistency and how fast it passes through your digestive system. If constipation is causing fecal incontinence, your doctor may recommend drinking plenty of fluids and gradually increasing your intake of fiber-rich foods. Getting adequate fiber can help with diarrhea, too. Avoid beverages with caffeine, alcohol, milk and carbonation if they trigger diarrhea. Artificial sweeteners and high fructose corn syrup also can produce diarrhea.
Sometimes, medications you’re taking for other conditions can contribute to fecal incontinence. If that’s the case, your doctor can make appropriate medication changes to help reduce aggravation of fecal incontinence. It’s important that your doctor is aware of all prescription and nonprescription drugs and supplements you’re taking.
Other possible treatments may include pelvic floor exercises, biofeedback, and bowel training (determining a specific time of day to have a bowel movement). A relatively new treatment —electrical stimulation of the sacral nerves — may be considered if more conservative measures aren’t successful.
Surgical treatments for fecal incontinence may be necessary when the cause is related to pelvic floor damage or muscle injuries that affect the anal sphincter. Surgery also may be done to repair protrusion of the rectum through the anus (rectal prolapse) or through the vagina (rectocele), or for hemorrhoids that interfere with bowel function. If damage to the anal sphincter is severe, a new sphincter may be constructed.
Fecal incontinence complications
Complications of fecal incontinence may include:
- Emotional distress. The loss of dignity associated with losing control over one’s bodily functions can lead to embarrassment, shame, frustration, anger and depression. It’s common for people with fecal incontinence to try to hide the problem or to avoid social engagements.
- Skin irritation. The skin around the anus is delicate and sensitive. Repeated contact with stool can lead to pain and itching, and potentially to sores (ulcers) that require medical treatment.
Fecal incontinence causes
Bowel incontinence is a result of poor bowel control. Factors that can lead to loss of bowel control include:
- long term straining
- medications, e.g. antibiotics, drugs for arthritis and diabetes
- lifestyle, e.g. heavy lifting leading to weak pelvic floor muscles
- weak back passage muscles due to having babies, getting older, some types of surgery, or radiation therapy
- diabetes
- bowel disease, e.g. Celiac disease, Crohn’s disease
- nerve disorders resulting from MS (multiple sclerosis) and Parkinson’s
- severe diarrhea, or
- constipation.
Problems with the rectum
Constipation
Constipation is a leading cause of bowel incontinence.
In cases of severe constipation, a large, solid stool can become stuck in the rectum. This is known as fecal impaction. The stool then begins to stretch the muscles of the rectum, weakening them.
Watery stools can leak around the stool and out of the bottom, causing bowel incontinence. This is called overflow incontinence and happens most commonly in elderly people.
Repeated straining caused by constipation or fecal impaction can also lead to rectal prolapse, when part of your lower intestine falls out of place and protrudes from your bottom. Rectal prolapse may also lead to bowel incontinence.
Diarrhea
It’s difficult for the rectum to hold liquid stools (diarrhea), so people with diarrhea (particularly recurring diarrhea) can develop bowel incontinence.
Conditions that can cause recurring diarrhea include:
- Crohn’s disease – inflammation of the digestive system
- Irritable bowel syndrome (IBS) – a condition that causes a range of digestive problems, such as diarrhea and bloating
- Ulcerative colitis – inflammation of the large bowel
These conditions can also cause scarring of the rectum, which can lead to bowel incontinence.
Hemorrhoids
Hemorrhoids (piles) are enlarged blood vessels inside or around the bottom (the rectum and anus). Symptoms include discomfort, itching, bleeding or a lump hanging down outside of the anus.
In severe cases, hemorrhoids may lead to bowel incontinence.
Problems with the sphincter muscles
The sphincter muscles at the bottom of the rectum control the bowel. Bowel incontinence happens if these muscles become weakened or damaged.
Childbirth is a common cause of damage to the sphincter muscles and a leading cause of bowel incontinence. During a vaginal birth, the sphincter muscles can become stretched and damaged, particularly as a result of a forceps delivery. Other causes include a large baby, the baby being born with the back of their head facing the mother’s back (occipitoposterior position) and a long labor.
Sphincter muscles can also become damaged through injury, or damage from bowel or rectal surgery.
Nerve damage
Bowel incontinence can also be caused by a problem with the nerves connecting the brain and the rectum. A nerve problem can mean your body is unaware of stools in your rectum, and may make it difficult for you to control your sphincter muscles.
Damage to these nerves is related to a number of conditions, including:
- Diabetes
- Multiple sclerosis (a condition of the central nervous system)
- Stroke
- Spina bifida (birth defects that affect the development of the spine and nervous system)
An injury to these nerves, such as a spinal injury, can also lead to bowel incontinence.
Other health conditions
In some cases, bowel incontinence may result from a health condition such as dementia or a severe learning disability that causes the person to lose bowel control.
A physical disability can also make it difficult to get to the toilet in time.
For many people, there is more than one cause of fecal incontinence. Causes can include:
- Muscle damage. Injury to the rings of muscle at the end of the rectum (anal sphincter) may make it difficult to hold stool back properly. This kind of damage can occur during childbirth, especially if you have an episiotomy or forceps are used during delivery.
- Nerve damage. Injury to the nerves that sense stool in the rectum or those that control the anal sphincter can lead to fecal incontinence. The nerve damage can be caused by childbirth, constant straining during bowel movements, spinal cord injury or stroke. Some diseases, such as diabetes and multiple sclerosis (MS), also can affect these nerves and cause damage that leads to fecal incontinence.
- Constipation. Chronic constipation may lead to a mass of dry, hard stool in the rectum (impacted stool) that is too large to pass. The muscles of the rectum and intestines stretch and eventually weaken, allowing watery stool from farther up the digestive tract to move around the impacted stool and leak out. Chronic constipation may also cause nerve damage that leads to fecal incontinence.
- Diarrhea. Solid stool is easier to retain in the rectum than is loose stool, so the loose stools of diarrhea can cause or worsen fecal incontinence.
- Loss of storage capacity in the rectum. Normally, the rectum stretches to accommodate stool. If your rectum is scarred or your rectal walls have stiffened from surgery, radiation treatment or inflammatory bowel disease, the rectum can’t stretch as much as it needs to, and excess stool can leak out.
- Surgery. Surgery to treat enlarged veins in the rectum or anus (hemorrhoids), as well as more complex operations involving the rectum and anus, can cause muscle and nerve damage that leads to fecal incontinence.
- Rectal prolapse. Fecal incontinence can result if the rectum drops down into the anus.
- Rectocele. In women, fecal incontinence can occur if the rectum protrudes through the vagina.
Risk factors for fecal incontinence
A risk factor for fecal incontinence is urinary incontinence. Other risk factors are similar to those of urinary incontinence, but also include:
- Chronic diarrhea
- Age. Although fecal incontinence can occur at any age, it’s more common in middle-aged and older adults.
- Being female. Fecal incontinence is slightly more common in women. One reason may be that fecal incontinence can be a complication of childbirth. But most women with fecal incontinence develop it after age 40, so the connection with pelvic floor injury during childbirth is unclear. However, it’s possible that the injury doesn’t cause symptoms for many years.
- Nerve damage. People who have long-standing diabetes or multiple sclerosis — conditions that can damage nerves that help control defecation — may be at risk of fecal incontinence.
- Dementia. Fecal incontinence is often present in late-stage Alzheimer’s disease and dementia.
- Physical disability. Being physically disabled may make it difficult to reach a toilet in time. An injury that caused a physical disability also may cause rectal nerve damage, leading to fecal incontinence. Also, inactivity can lead to constipation, resulting in fecal incontinence.
Although there are many risk factors for incontinence, only a few have undergone rigorous testing. If you fall into one of these risk categories and are worried about poor bladder or bowel control (or experience symptoms of incontinence) speak to your doctor, a continence health professional or a continence nurse advisor.
If you are caring for someone with bladder or bowel problems, practical tips and advice are available to assist you with your care.
Fecal incontinence prevention
In many cases, incontinence can be prevented by adopting healthy diet and lifestyle habits. Here are some simple steps that can be incorporated into your daily life to help prevent urinary incontinence and fecal incontinence.
- Reduce constipation. Increase your exercise, eat more high-fiber foods and drink plenty of fluids.
- Control diarrhea. Treating or eliminating the cause of the diarrhea, such as an intestinal infection, may help you avoid fecal incontinence.
- Avoid straining. Straining during bowel movements can eventually weaken anal sphincter muscles or damage nerves, possibly leading to fecal incontinence.
Drink well
- aim to drink 6-8 cups (1.5 – 2 litres) of fluid per day, unless otherwise advised by your doctor
- spread your drinks evenly throughout the day
- drink more fluids (preferably water) if the weather is hot or if you are exercising, and
- cut down on alcohol, fizzy drinks and drinks that have caffeine in them as they irritate the bladder.
Tip: Don’t reduce your fluid intake if you have a bladder control problem, as this will concentrate your urine and make the problem worse.
Eat a healthy diet
- Eat plenty of fiber, which improves bowel function by absorbing water and adding bulk to your bowel motions (poo). Bulky stools keep things moving through your bowel to avoid constipation. Fiber is found in foods such as multi grain or whole grain breads, cereals and cereal products, fruit, vegetables, legumes, nuts and seeds, and
- Eat 2 servings of fruit, 5 servings of vegetables and 5 servings of cereals and breads each day.
Tip: A high fiber diet means you need to drink plenty of fluid as the fiber needs water in order to bulk up your bowel motions.
Lead a positive lifestyle
- Maintain an ideal body weight with a Body Mass Index (BMI) of 25 or less. Excess body fat strains the pelvic floor and can lead to bladder and bowel control problems. Speak to your doctor or qualified dietitian for more information about safe ways to lose weight, and
- Stop smoking. Chronic (long-term) coughing associated with smoking can weaken the muscles of your pelvic floor and lead to bladder and bowel control problems.
Tip: Talk to your doctor or pharmacist for information on quitting smoking and managing a chronic cough.
Get active
- Aim to exercise for 30 minutes most days. Exercise stimulates movement of the bowel, and even gentle exercise like walking helps, and
- Do your pelvic floor muscle exercises regularly. Obesity, pregnancy, childbirth, regular heavy lifting and a chronic cough can weaken the pelvic floor, but you can strengthen these muscles with specific exercises.
Practice good toilet habits
- go to the toilet when you get the urge to open your bowels, as this is the most effective time to completely empty your bowels. Most people get the urge first thing in the morning or following a meal when eating has stimulated the bowel.
- get into the correct sitting position on the toilet. Sit on the toilet, elbows on knees, lean forward and support feet with a footstool. This helps to fully relax your pelvic floor and sphincter muscles. Bulge out your tummy, relax your back passage and let go (don’t hold your breath or strain). When you have finished firmly draw up your back passage.
- avoid constipation as this affects bladder and bowel function. If you often strain to move your bowels, the pelvic floor stretches and weakens over time.
- don’t get into the habit of going to the toilet ‘just in case’ – only go when you need to, and
- visit your doctor as soon as you suspect a urinary tract infection.
Bowel incontinence signs and symptoms
Most adults who experience fecal incontinence do so only during an occasional bout of diarrhea. But some people have recurring or chronic fecal incontinence. They may be unable to resist the urge to defecate, which comes on so suddenly that they don’t make it to the toilet in time. This is called urge incontinence. Another type of fecal incontinence occurs in people are not aware of the need to pass stool. This is called passive incontinence.
Fecal incontinence may be accompanied by other bowel problems, such as:
- Diarrhea
- Constipation
- Gas and bloating
Fecal incontinence diagnosis
Your doctor will ask questions about your condition and perform a physical exam that usually includes a visual inspection of your anus. A probe may be used to examine this area for nerve damage. Normally, this touching causes your anal sphincter to contract and your anus to pucker.
Medical tests
A number of tests are available to help pinpoint the cause of fecal incontinence:
- Digital rectal exam. Your doctor inserts a gloved and lubricated finger into your rectum to evaluate the strength of your sphincter muscles and to check for any abnormalities in the rectal area. During the exam your doctor may ask you to bear down, to check for rectal prolapse.
- Balloon expulsion test. A small balloon is inserted into the rectum and filled with water. You are then asked to go to the toilet and expel the balloon. The length of time it takes to expel the balloon is recorded. A time of one minute or longer is usually considered a sign of a defecation disorder.
- Anal manometry. A narrow, flexible tube is inserted into the anus and rectum. A small balloon at the tip of the tube may be expanded. This test helps measure the tightness of your anal sphincter and the sensitivity and functioning of your rectum.
- Anorectal ultrasonography. A narrow, wand-like instrument is inserted into the anus and rectum. The instrument produces video images that allow your doctor to evaluate the structure of your sphincter.
- Proctography. X-ray video images are made while you have a bowel movement on a specially designed toilet. The test measures how much stool your rectum can hold and evaluates how well your body expels stool.
- Proctosigmoidoscopy. A flexible tube is inserted into your rectum to inspect the last two feet of the colon (sigmoid) for signs of inflammation, tumors or scar tissue that may cause fecal incontinence.
- Colonoscopy. A flexible tube is inserted into your rectum to inspect the entire colon.
- Magnetic resonance imaging (MRI). MRI can provide clear pictures of the sphincter to determine if the muscles are intact and can also provide images during defecation (defecography).
Fecal incontinence treatment
Bowel incontinence treatment depends on underlying cause and the pattern of your symptoms.
Trying the least intrusive treatments first, such as dietary changes and exercise programmes, is often recommended.
Medication and surgery are usually only considered if other treatments haven’t worked.
Continence products
You may find it helpful to use continence products until your bowel incontinence is better controlled.
Anal plugs are one way to prevent involuntary soiling. An anal plug is made of foam and designed to be inserted into your bottom. However, they can be uncomfortable and they’re not really a long term solution.
If the plug comes into contact with moisture from the bowel, it expands and prevents leakage or soiling. Anal plugs can be worn for up to 12 hours, after which time they are removed using an attached string.
Disposable body pads are contoured pads that soak up liquid stools and protect your skin. They can be used in cases of mild bowel incontinence.
Single-use silicone inserts, which form a seal around the rectum until your next bowel movement, are also being investigated as a treatment option for moderate to severe bowel incontinence.
Your local continence service can offer help and advice about continence products, and you don’t usually need a referral from your doctor to make an appointment. These clinics are staffed by nurses who specialize in continence treatment.
Dietary changes
Bowel incontinence associated with diarrhea or constipation can often be controlled by making changes to your diet.
It may be beneficial to keep a food diary to record the effect of your diet on your symptoms.
Diarrhea
The National Institute for Health and Care Excellence (NICE) has published dietary advice for managing diarrhoea in cases of irritable bowel syndrome 1. These guidelines can also be applied to people with diarrhoea associated with bowel incontinence.
The advice from NICE includes the following:
- limit fiber intake from wholegrain breads, bran, cereals, nuts and seeds (except golden linseeds)
- avoid skin, pips and pith from fruit and vegetables
- limit fresh and dried fruit to three portions a day and fruit juice to one small glass a day (make up the recommended ‘five a day’ with vegetables)
- limit how often you have fizzy drinks and drinks containing caffeine
- avoid foods high in fat, such as chips, fast foods and burgers
Constipation
A high-fiber diet is usually recommended for most people with constipation-associated bowel incontinence. Your doctor can tell you if a high-fiber diet is suitable for you. Fiber is predominately present in fruits, vegetables, and whole-grain breads and cereals. Aim for 20 to 30 grams of fiber a day, but don’t add it to your diet all at once. Too much fiber suddenly can cause uncomfortable bloating and gas.
Fiber can soften stools, making them easier to pass. Foods that are high in fiber include:
- fruit and vegetables
- beans
- wholegrain rice
- wholewheat pasta
- wholemeal bread
- seeds, nuts and oats
Drink plenty of fluids because this can help to soften your stools and make them easier to pass.
Bowel retraining
Bowel retraining is a type of treatment for people with reduced sensation in their rectum as a result of nerve damage, or for those who have recurring episodes of constipation.
There are three goals in bowel retraining:
- to improve the consistency of your stools
- to establish a regular time for you to empty your bowels
- to find ways of stimulating your bowels to empty themselves
Changes to your diet usually improve stool consistency (see above).
Establishing a regular time to empty your bowels means finding the most convenient time when you can go to the toilet without being rushed.
Ways to stimulate bowel movements can differ from person to person. Some people find a hot drink and meal can help. Others may need to stimulate their anus using their finger.
Biofeedback
Biofeedback is a type of bowel retraining exercise that involves placing a small electric probe into your bottom.
The sensor relays detailed information about the movement and pressure of the muscles in your rectum to an attached computer.
You’re then asked to perform a series of exercises designed to improve your bowel function. The sensor checks that you are performing the exercises in the right way.
Sacral nerve stimulation
The sacral nerves run from your spinal cord to muscles in your pelvis. These nerves regulate the sensation and strength of your rectal and anal sphincter muscles. Implanting a device that sends small electrical impulses continuously to the nerves can strengthen muscles in the bowel. This treatment is usually done only after other treatments are tried.
Sacral nerve stimulation is carried out in two stages.
- Stage 1: Insertion of the sacral nerve stimulation lead through a 1cm incision in the buttock and with x-ray assistance Electrical stimulation through a small hole in the sacrum called the ‘third sacral foramen’ along the path of the third sacral nerve. This is the nerve that mediates the control of bladder and bowel function from the brain and spinal cord. Once positioned, the lead is then tunneled to the flank or buttock, and connected to an external lead passing through the skin to a temporary nerve stimulator. At first, the pulse generator is located outside your body. If the treatment is effective, the pulse generator will be implanted deep under the skin in your back.
- Stage 2: If the patient experiences a significant improvement in the first 1-2 weeks after surgery, stage 2 involves removal of the external lead and insertion of the pulse generator.
Success rates
The recently published INSITE* trial has confirmed an overall success rate of 70 per cent. When successful, the procedure is usually life changing with patients reporting a 3-5 times improvement in quality of life over standard medical treatments, with 45% reporting complete continence.
How long does sacral nerve stimulation last?
The INSITE trial has shown, a long-term success rate of more than 80% at 5 years.
Current pulse generators have a battery life of up to 5 years and soon rechargeable implantable pulse generators will be available with projected battery life of more than 10 years.
What is the recovery time following sacral nerve stimulation?
An important factor in recovery is to minimize the risk of the lead moving. Because the greatest risk for this is in the first few weeks after surgery, patients are advised to avoid strenuous exercise, especially twisting and bending movements for at least two weeks after surgery. The surgery itself is relatively minor and often not associated with much pain.
Risks and complications of sacral nerve stimulation
Every surgical procedure and medical treatment has potential issues and adverse events. The INSITE trial reported no unanticipated adverse events, with typical adverse experiences including, lead movement, infection – 3% [mostly in diabetics], lead fracture – 1%, high impedance in the lead, electrical ‘shorting’ of the lead and pain at implantable pulse generator site – 5%. These adverse events are easily corrected.
Posterior tibial nerve stimulation
Tibial nerve stimulation is a fairly new treatment for bowel incontinence.
A fine needle is inserted into the tibial nerve just above the ankle and an electrode is placed on the foot. A mild electric current is passed through the needle to stimulate the tibial nerve. It’s not known exactly how this treatment works, but it’s thought to work in a similar way to sacral nerve stimulation.
This minimally invasive treatment may be helpful for some people with fecal incontinence, but more studies are needed.
Vaginal balloon (Eclipse System)
This is a pump-type device inserted in the vagina. The inflated balloon results in pressure on the rectal area, leading to a decrease in the number of episodes of fecal incontinence. Results for women have been promising, but more data are needed.
Injectable bulking agents
Bulking agents, such as collagen or silicone, can be injected into the muscles of the sphincter and rectum to strengthen them.
The use of bulking agents in this way is a fairly new technique, so there’s little information about their long-term effectiveness and safety.
You should discuss the possible advantages and disadvantages of this type of treatment in full with your treatment team before deciding whether to proceed.
Endoscopic heat therapy
Endoscopic radiofrequency (heat) therapy is a fairly new treatment for bowel incontinence.
Heat energy is applied to the sphincter muscles through a thin probe, to encourage scarring of the tissue. This helps tighten the muscles and helps to control bowel movements.
The National Institute for Health and Care Excellence (NICE) recently produced guidelines on this procedure. NICE concluded that the procedure appears to be safe, although there are still uncertainties about how well it works 2.
As well as the uncertainties surrounding this procedure, it is also expensive.
Medications
Depending on the cause of fecal incontinence, options include:
- Anti-diarrheal drugs such as loperamide hydrochloride (Imodium) and diphenoxylate and atropine sulfate (Lomotil). Loperamide is a medicine widely used to treat diarrhoea. It works by slowing down the movement of stools through the digestive system, allowing more water to be absorbed from the stools. Loperamide can be prescribed in low doses to be taken regularly over a long period of time.
- Bulk laxatives such as methylcellulose (Citrucel) and psyllium (Metamucil), if chronic constipation is causing your incontinence
- Injectable bulking agents such as Dextranomer Microspheres/Hyaluronate Sodium in 0.9 % Nacl (Solesta) are injected directly into the anal canal.
- Rectal irrigation or enemas are used when bowel incontinence is caused by fecal impaction and other treatments have failed to remove the impacted stool from the rectum. These procedures involve a small tube that is placed into your anus. A special solution is then used to wash out your rectum.
Surgery
Surgery is usually only recommended after all other treatment options have been tried. Surgery may be required to correct an underlying problem, such as rectal prolapse or sphincter damage caused by childbirth.
The options include:
- Sphincteroplasty. This procedure repairs a damaged or weakened anal sphincter. Doctors identify an injured area of muscle and free its edges from the surrounding tissue. They then bring the muscle edges back together and sew them in an overlapping fashion, strengthening the muscle and tightening the sphincter. The procedure is used for people who have fecal incontinence right after childbirth.
- Treating rectal prolapse, a rectocele or hemorrhoids. Surgical correction of these problems will likely reduce or eliminate fecal incontinence.
- Sphincter replacement. A damaged anal sphincter can be replaced with an artificial anal sphincter. The device is essentially an inflatable cuff, which is implanted around your anal canal. When inflated, the device keeps your anal sphincter shut tight until you’re ready to defecate. To go to the toilet, you use a small external pump to deflate the device and allow stool to be released. The device then reinflates itself.
- Sphincter repair (dynamic graciloplasty). In this surgery doctors take a muscle from the inner thigh and wrap it around the sphincter, restoring muscle tone to the sphincter.
- Colostomy (bowel diversion). This surgery diverts stool through an opening in the abdomen. Doctors attach a special bag to this opening to collect the stool. Colostomy is generally considered only after other treatments have been tried.
Artificial sphincter
An artificial sphincter may be implanted if you have bowel incontinence caused by a problem with your sphincter muscles.
This operation involves placing a circular cuff under the skin around the anus. The cuff is filled with fluid and sits tightly around the anus, keeping it closed.
A tube is placed under the skin from the cuff to a control pump. In men, the pump is placed near the testicles, in women it’s placed near the vagina. A special balloon is placed into the tummy, and this is connected to the control pump by tubing that runs under the skin.
The pump is activated by pressing a button located under the skin. This drains the fluid from the cuff into the balloon, so your anus opens and you can pass stools. When you are finished, the fluid slowly refills the cuff and the anus closes.
The use of an artificial sphincter is a relatively new procedure, so there isn’t much good-quality information about its long-term effectiveness and safety.
Possible problems include infection, injury during surgery and the cuff becoming dislodged. In some cases, further surgery is required to correct problems.
Living with incontinence
Follow our tips on how to cope with the daily challenges of living with incontinence.
Do daily pelvic floor exercises (Kegel exercises)
Pelvic floor exercises can be really effective at reducing leakage, but it’s important to do them properly.
Pelvic floor exercises strengthen the muscles around your bladder, vagina or penis, and back passage. Strengthening your pelvic floor muscles can help stop incontinence, treat prolapse, and make sex better, too.
Both men and women can benefit from doing pelvic floor exercises.
Kegel Pelvic floor muscle training exercises
Pelvic floor muscle training exercises are a series of exercises designed to strengthen the muscles of the pelvic floor.
Pelvic floor muscle training exercises are recommended for:
- Women with urinary stress incontinence
- Men with urinary stress incontinence after prostate surgery
- People who have fecal incontinence
Pelvic floor muscle training exercises can help strengthen the muscles under the uterus, bladder, and bowel (large intestine). They can help both men and women who have problems with urine leakage or bowel control.
To perform Kegel exercises:
- Begin by emptying your bladder.
- Tighten (contract) your pelvic floor muscles as though you were trying to prevent urinating or passing gas.
- Hold the contraction for five seconds, and then relax for five seconds. If this is too difficult, start by holding for two seconds and relaxing for three seconds.
- Work up to holding the contractions for 10 seconds at a time.
- Aim for at least three to five sets of 10 repetitions each day (morning, afternoon, and night).
Because these muscles control the bladder, rectum, and vagina, the following tips may help:
- Insert a finger into your vagina. Tighten the muscles as if you are holding in your urine, then let go. You should feel the muscles tighten and move up and down.
It is very important that you keep the following muscles relaxed while doing pelvic floor muscle training exercises:
- Abdominal
- Buttocks (the deeper, anal sphincter muscle should contract)
- Thigh
A pelvic floor muscle training exercise is like pretending that you have to urinate, and then holding it. You relax and tighten the muscles that control urine flow. It is important to find the right muscles to tighten.
The next time you have to urinate, start to go and then stop. Feel the muscles in your vagina, bladder, or anus get tight and move up. These are the pelvic floor muscles. If you feel them tighten, you have done the exercise right.
You can do these exercises at any time and place. Most people prefer to do the exercises while lying down or sitting in a chair. After 4 to 6 weeks, most people notice some improvement. It may take as long as 3 months to see a major change.
After a couple of weeks, you can also try doing a single pelvic floor contraction at times when you are likely to leak (for example, while getting out of a chair).
- A word of caution: Some people feel that they can speed up the progress by increasing the number of repetitions and the frequency of exercises. However, over-exercising can instead cause muscle fatigue and increase urine leakage.
If you feel any discomfort in your abdomen or back while doing these exercises, you are probably doing them wrong. Breathe deeply and relax your body when you do these exercises. Make sure you are not tightening your stomach, thigh, buttock, or chest muscles.
When done the right way, pelvic floor muscle exercises have been shown to be very effective at improving urinary continence.
If you are still not sure whether you are tightening the right muscles, keep in mind that all of the muscles of the pelvic floor relax and contract at the same time.
A woman can also strengthen these muscles by using a vaginal cone, which is a weighted device that is inserted into the vagina. Then you try to tighten the pelvic floor muscles to hold the device in place.
Kegel exercises may be most successful when they’re taught by a physical therapist and reinforced with biofeedback. If you are unsure whether you are doing the pelvic floor muscle training correctly, you can use biofeedback and electrical stimulation to help find the correct muscle group to work.
- Biofeedback is a method of positive reinforcement. Electrodes are placed on the abdomen and along the anal area. Some therapists place a sensor in the vagina in women or anus in men to monitor the contraction of pelvic floor muscles.
- A monitor will display a graph showing which muscles are contracting and which are at rest. The therapist can help find the right muscles for performing pelvic floor muscle training exercises.
There are physical therapists specially trained in pelvic floor muscle training. Many people benefit from formal physical therapy.
Enjoy good sex despite incontinence
Worries about embarrassing leaks during sex can mean you avoid intimate contact. This puts strain on relationships and damages your self-esteem and self-confidence.
There’s no reason why anyone with bladder or bowel weakness can’t enjoy intimate relationships.
If you empty your bladder and bowel and don’t drink too much fluid before having sex, any leak probably won’t be serious. Sex involves all sorts of bodily fluids, so a small leak probably won’t even be noticed.
It can give you peace of mind to protect the bed. Bed pads, which absorb moisture and have a stay-dry cover, may be the most comfortable choice.
Skin care
You can help avoid further discomfort from fecal incontinence by keeping the skin around your anus as clean and dry as possible. To relieve anal discomfort and eliminate any possible odor associated with fecal incontinence:
- Wash with water. Gently wash the area with water after each bowel movement. Showering or soaking in a bath also may help. Soap can dry and irritate the skin. So can rubbing with dry toilet paper. Premoistened, alcohol-free, perfume-free towelettes or wipes may be a good alternative for cleaning the area.
- Dry thoroughly. Allow the area to air-dry, if possible. If you’re short on time, you can gently pat the area dry with toilet paper or a clean washcloth.
- Apply a cream or powder. Moisture-barrier creams help keep irritated skin from having direct contact with feces. Be sure the area is clean and dry before you apply any cream. Nonmedicated talcum powder or cornstarch also may help relieve anal discomfort.
- Wear cotton underwear and loose clothing. Tight clothing can restrict airflow, making skin problems worse. Change soiled underwear quickly.
When medical treatments can’t completely eliminate incontinence, products such as absorbent pads and disposable underwear can help you manage the problem. If you use pads or adult diapers, be sure they have an absorbent wicking layer on top, to help keep moisture away from your skin.
Constant dampness can make your skin irritated, but you can avoid this by following a simple routine.
Wash using a cotton cloth or disposable wipes (flannels and sponges can be too harsh). Use products that cleanse without drying. These are available as non-aerosol sprays, foams and disposable wipes.
Don’t use soap as it makes the skin dry. And check that disposable wipes are alcohol-free to avoid skin irritation.
After cleansing, always moisturize and use a non-greasy barrier cream. This forms a protective layer to block out unwanted moisture.
What to take on holiday
Incontinence shouldn’t stop you going on holiday or staying with friends. The key is to plan ahead.
When you’re out — wear trousers or skirts that are easy to undo and have elasticated waistbands rather than buttons.
Take enough of all the products you use with you. Include a small bag containing your clean-up kit. This could contain a change of clothes, pads, handwash, wet wipes and plastic bags.
If you intend to do your own laundry, find out where you can wash and dry items in private, if necessary. A portable washing line and pegs can be useful.
If you’re flying, pre-book an aisle seat near the toilet and wear loose-fitting clothes, as they’re more comfortable and make changing easier.
Finally, pack a deodorizing spray, which will remove odors, rather than just masking them.
Fight depression with talking therapy
Incontinence can affect you mentally as well as physically. The negative effect on your self-esteem, dignity and independence can lead to isolation, distress and depression.
According to continence nurses, up to 70% of people with incontinence are affected by depressive illnesses.
It helps to talk to people you trust, so tell your friends and family how you’re feeling.
Or ask your doctor to refer you for counseling or other talking therapy.
Treat constipation promptly
Straining to empty your bowels weakens your pelvic floor muscles and makes leakage worse.
Never delay the urge to empty your bowels. If you have constipation, it may help to change your diet and lifestyle.
Eating more fibre and taking more exercise can help. It may also help if you change the way you sit and use your muscles to empty your bowels. A specialist physiotherapist can advise you on this.
Lifestyle Changes
The following can help you control your symptoms:
- Lose weight if you are obese.
- Avoid heavy lifting or straining.
- Get treated for a chronic cough. If you cough is due to smoking, try to quit.
Lose weight
Being overweight can weaken your pelvic floor muscles and can cause incontinence, because of the pressure of fatty tissue on the bladder.
Your symptoms may improve, and could clear up completely, if you lose the excess weight.
Quit smoking
If you smoke, you put yourself at risk of incontinence, because coughing puts strain on your pelvic floor muscles.
Advice to help you stop smoking is available from your doctor or pharmacist.
Avoid lifting
Lifting puts strain on your pelvic floor muscles, so avoid it wherever you can.
When you do need to lift something, like picking up children or shopping bags, tighten your pelvic floor muscles before and during the lift.
Cut down on caffeine
Caffeine irritates the bladder and can make incontinence worse.
Coffee has the biggest effect, so stop drinking it or switch to decaffeinated.
Fizzy drinks, tea, green tea, energy drinks and hot chocolate also contain caffeine, so cut down on these too and replace them with water and herbal or fruit teas.
Cut down on alcohol to improve incontinence
Alcohol is a diuretic, which makes you urinate more often. Cutting down may help your incontinence symptoms.





{kind=link}