Contents
What is ferritin
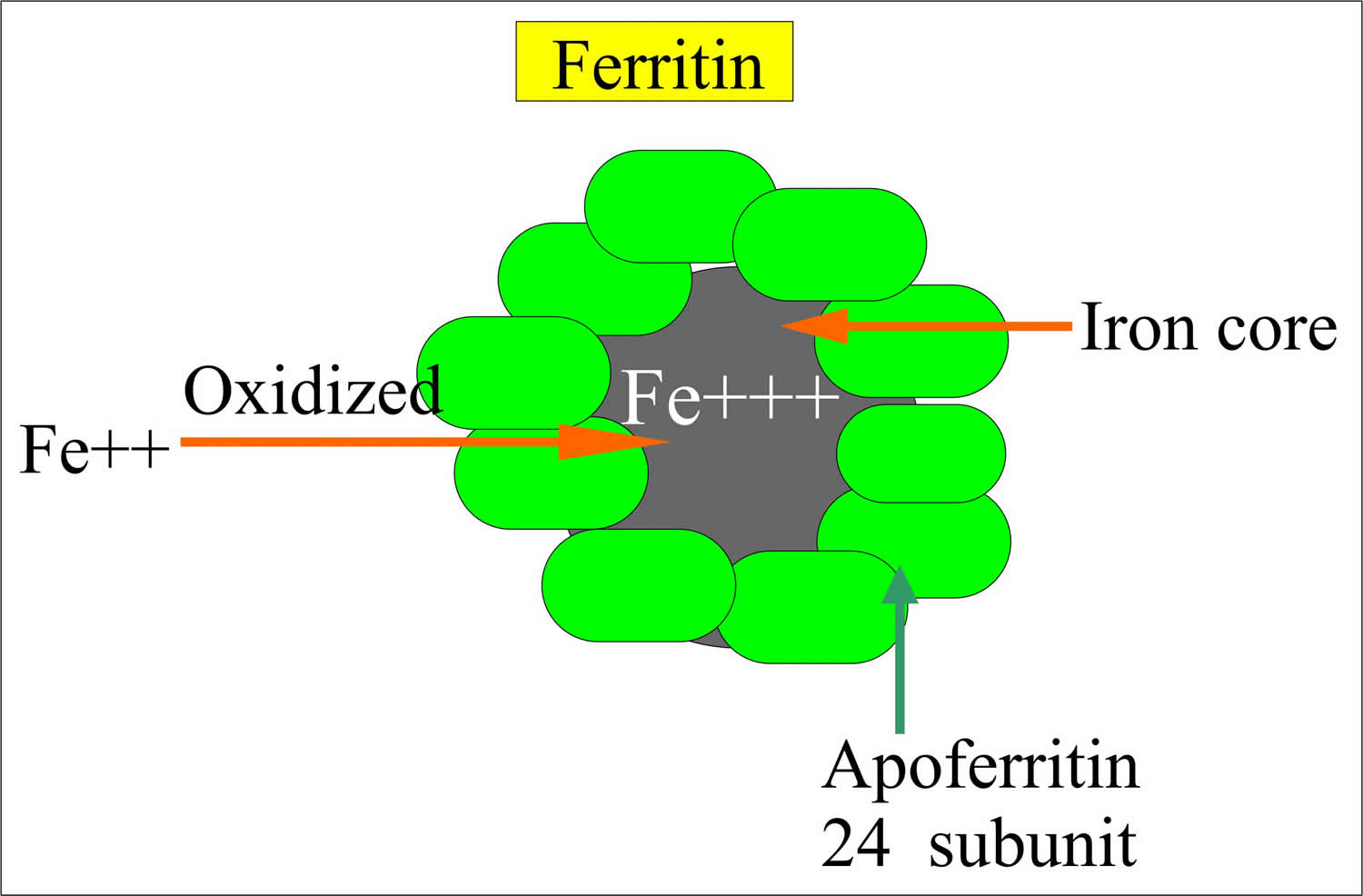
Ferritin is a large spherical protein consisting of 24 noncovalently linked subunits with a molecular weight of approximately 450,000 daltons. The subunits form a shell surrounding a central core containing variable amounts of ferric hydroxyphosphate. One molecule of ferritin is capable of binding between 4,000 and 5,000 atoms of iron, making ferritin the major iron storage protein for the body.
Ferritin is found chiefly in the cytoplasm of cells of the reticuloendothelial system and is a constituent of normal human serum. The concentration of ferritin is directly proportional to the total iron stores in the body. The small amount of ferritin that is released and circulates in the blood is a reflection of the total amount of iron stored in the body and the serum ferritin concentrations become a common diagnostic tool in the evaluation of iron status.
The concentration of ferritin in serum correlates well with the amount of storage iron as proven by phlebotomy trials. Hence, serum ferritin is a good marker of total body iron stores. A low serum ferritin is almost only seen in iron deficiency.
In most normal adults, serum ferritin concentrations vary with age and sex. There is a sharp rise in serum ferritin concentrations in the first month of life, coinciding with the depression of bone marrow erythropoiesis. Within 2 or 3 months, erythropoiesis becomes reactivated and there is a drop in the concentration of serum ferritin. By 6 months, the concentration is reduced to fairly low levels where they remain throughout childhood. There is no sex difference until the onset of puberty, at which time ferritin concentrations rise, particularly in males. There is a significant positive correlation between age and serum ferritin concentrations in females, but not in males.
Patients with iron deficiency anemia have serum ferritin concentration approximately one-tenth of normal subjects, while patients with iron overload (hemochromatosis, hemosiderosis) have serum ferritin concentrations much higher than normal. Studies also suggest that serum ferritin provides a sensitive means of detecting iron deficiency at an early stage. Serum ferritin concentrations may serve as a tool to monitor the effects of iron therapy, but results should be interpreted with caution, as these cases may not always reflect the true state of iron stores. Ferritin is a positive acute phase reactant in both adults and children, whereby chronic inflammation results in a disproportionate increase in ferritin in relation to iron reserves. Elevated ferritin is also observed in acute and chronic liver disease, chronic renal failure, and in some types of neoplastic disease.
In the presence of conditions such as inflammation, infection, malignancy (hematological and solid tumors), or liver or kidney disease, serum ferritin concentrations do not reflect iron stores alone and are typically higher than otherwise expected.
In addition, higher ferritin levels are seen with increasing BMI (body mass index) and post-menopause. In all these settings, a normal or elevated serum ferritin level does not exclude iron deficiency nor diagnose iron overload.
Ferritin normal range:
Levels are age and gender dependent with method-related upper reference limits.
- Adult female (premenopausal): 20-220 µg/L.
- Adult female (postmenopausal): 30-370 µg/L.
- Adult male: 30-620 µg/L.
Iron is an essential trace element and nutrient that, among other functions, is necessary for the production of healthy red blood cells (RBCs). The body cannot produce iron and must absorb it from the foods we eat or from supplements.
In healthy people, most of the iron absorbed by the body is incorporated into the hemoglobin of red blood cells. Most of the remaining is stored as ferritin or as hemosiderin, with additional small amounts used to produce other proteins such as myoglobin and some enzymes. Ferritin and hemosiderin are present primarily in the liver but also in the bone marrow, spleen, and skeletal muscles.
When the level of iron is insufficient to meet the body’s needs, the level of iron in the blood drops, iron stores are depleted and ferritin levels decrease. This may occur because:
- Not enough iron is consumed (either foods or supplements)
- The body is unable to absorb iron from the foods eaten in conditions such as celiac disease
- There is an increased need for iron such as during pregnancy or childhood, or due to a condition that causes chronic blood loss (e.g., peptic ulcer, colon cancer).
Insufficient levels of circulating and stored iron may eventually lead to iron deficiency anemia (decreased hemoglobin). In the early stage of iron deficiency, no physical effects are usually seen and the amount of iron stored may be significantly depleted before any signs or symptoms of iron deficiency develop. If a person is otherwise healthy and anemia develops over a long period of time, symptoms seldom appear before the hemoglobin in the blood drops below the lower limit of normal.
However, as the iron-deficiency progresses, symptoms eventually begin to appear. The most common symptoms of iron deficiency anemia include fatigue, weakness, dizziness, headaches and pale skin.
Conversely, iron storage and ferritin levels increase when more iron is absorbed than the body needs. Absorbing too much iron over time can lead to the progressive buildup of iron compounds in organs and may eventually cause their dysfunction and failure. An example of this is hemochromatosis, a rare genetic disease in which the body absorbs too much iron, even on a normal diet. Additionally, iron overload can occur when a person undergoes repeated blood transfusions.
Iron homeostasis
Iron is an essential element for many living organisms. In humans iron is required for oxygen transportation (in hemoglobin and myoglobin) and electron transfer reactions.
Approximately two-thirds of your body’s iron is found in red blood cells and a further 15% is in muscle and cellular enzymes. The remaining iron is excess to needs and stored primarily as ferritin or hemosiderin in the liver and within macrophages in the reticuloendothelial system. Iron recycling through the mobilization of these stores means that most human diets can account for minor daily losses from the sloughing of epithelial cells or insignificant blood losses.
Absorption of iron from the small intestine and its release from macrophages is tightly controlled, as free iron has the potential to cause tissue damage through
the production of reactive oxygen species (ROS). Maintaining low levels of free iron also aids resistance to infection, as bacteria constantly scavenge for iron from their environment for growth.
Hepcidin, a 25 amino acid peptide produced by the liver, is the principal iron-regulatory hormone providing the link between iron metabolism and innate immunity 1).
Hepcidin production is stimulated by both iron loading and infection/inflammation — conditions where the body aims to limit the uptake of iron and its availability to invading organisms.
Hepcidin acts by binding ferroportin, a transmembrane protein involved in exporting iron from macrophages, red blood cells (erythrocytes) and enterocytes.
This interaction leads to ferroportin degradation. This in turn leads to decreased dietary iron absorption, sequestration of iron into macrophages and decreased circulating iron concentrations. Stimulated production of hepcidin is also seen in the anemia of chronic disease, where body iron stores are not deficient but
simply not available for red cell production.
Conversely, in response to increased iron demand (iron deficiency, hypoxia and hemorrhagic or hemolytic anemias), hepcidin production is suppressed, resulting
in a release of stored iron and increased dietary iron absorption.
In hereditary iron overload syndromes (e.g., hereditary hemochromatosis), mutations in genes such as HFE cause a deficiency in hepcidin. It is likely that the liver, although exporting iron, has a greater ability to take up the increased plasma iron resulting in liver iron deposition 2).
Who should take iron supplements?
The people who typically need iron supplements are pregnant women and those with documented iron deficiency. Young women who become anemic due to poor dietary intake and have chronic and/or excessive loss of blood during their menstrual cycle may require iron supplements. People should not take iron supplements before talking to their healthcare practitioner as excess iron can cause chronic iron overload. An overdose of iron pills can be toxic, especially to children.
Ferritin blood test
The ferritin test is used to assess a person’s iron stores in the body. The ferritin test is often ordered along with an iron level and Total Iron Binding Capacity (TIBC) and the calculation of transferrin saturation (calculated based on blood level of transferrin) to detect a low iron level (iron deficiency) or too much iron in the body (iron overload) as well as to assess the severity of these conditions.
Serum iron studies are usually requested to diagnose iron deficiency or iron overload, but interpretation can be difficult because of the relationship shared by iron metabolism and inflammation. Serum iron concentration is a poor measure of iron status in the body. In an individual, levels fluctuate significantly due to diurnal variation and fasting status. Even when blood collection is standardized to morning samples in fasting patients, iron is an acute phase reactant and low levels may be seen as a consequence of acute inflammation.
In the presence of conditions such as inflammation, infection, malignancy (hematological and solid tumors), or liver or kidney disease, serum ferritin concentrations do not reflect iron stores alone and are typically higher than otherwise expected.
In addition, higher ferritin levels are seen with increasing BMI (body mass index) and post-menopause. In all these settings, a normal or elevated serum ferritin level does not exclude iron deficiency nor diagnose iron overload.
Transferrin is often referred to as the circulating carrier protein for iron. In fact, this describes apotransferrin, which, when bound to either one or two atoms of iron, is then named transferrin.
Monoferric or diferric transferrin has high affinity for the transferrin receptor allowing cellular uptake by endocytosis. Iron is then utilised or stored by the cell and apotransferrin returned to the circulation.
Liver synthesis further contributes to apotransferrin levels so that high serum transferrin concentrations may be induced in iron deficiency or high estrogen states (e.g, pregnancy, oral contraceptive pill use).
Low levels may be in response to iron loading or due to liver disease with poor synthetic function. Like serum iron, transferrin is also a negative acute phase
reactant.
Transferrin saturation is a calculated ratio between serum iron and total iron binding capacity (TIBC). Because of this, it is influenced by the analytical, physiological and pathological factors that affect these components.
Total Iron Binding Capacity (TIBC) may be measured directly or derived from measuring unsaturated iron binding capacity (UIBC) or transferrin. Measuring transferrin is generally more expensive for laboratories compared with total iron binding capacity (TIBC) or unsaturated iron binding capacity (UIBC), but there is less variation in results between different assays.
Hepcidin, despite its importance in iron metabolism, is yet to have an established role in diagnostic testing and is not routinely available.
When is ferritin test ordered?
The ferritin test may be ordered, along with other iron tests, when a routine complete blood count (CBC) shows that a person’s hemoglobin and hematocrit are low and their red blood cells are smaller and paler than normal (microcytic and hypochromic), suggesting iron deficiency anemia even though other clinical symptoms may not have developed yet.
A ferritin test as well as other iron-related tests may be ordered when a person develops signs and symptoms of iron-deficiency anemia such as:
- Chronic fatigue/tiredness
- Weakness
- Dizziness
- Headaches
- Pale skin (pallor)
A ferritin level may also be ordered when iron overload is suspected. Signs and symptoms of iron overload will vary from person to person and tend to worsen over time. They are due to iron accumulation in the blood and tissues. They may include:
- Joint pain
- Fatigue, weakness
- Weight loss
- Lack of energy
- Abdominal pain
- Loss of sex drive
- Organ damage, such as in the heart and liver
To confirm the presence of iron overload, other iron tests (iron, total iron binding capacity) and a genetic test for hereditary hemochromatosis may be ordered as well.
Ferritin level chart
Ferritin levels are often evaluated in conjunction with other iron tests. A summary of the changes in iron tests seen in various diseases of iron status is shown in the chart below.
The transferrin test, total iron-binding capacity (TIBC), unsaturated iron-binding capacity (UIBC), and transferrin saturation, along with other iron tests, help evaluate the amount of iron in the body by measuring several substances in the blood. These tests are often ordered at the same time and the results interpreted together to help diagnose and/or monitor iron deficiency or iron overload.
| Disease | Iron | TIBC/Transferrin | UIBC | %Transferrin Saturation | Ferritin |
| Iron Deficiency | Low | High | High | Low | Low |
| Hemochromatosis/Hemosiderosis | High | Low | Low | High | High |
| Chronic Illness | Low | Low/Normal | Low/Normal | Low/Normal | High/Normal |
| Hemolytic Anemia | High | Normal/Low | Low/Normal | High | High |
| Sideroblastic Anemia | Normal/High | Normal/Low | Low/Normal | High | High |
| Iron Poisoning | High | Normal | Low | High | Normal |
Abbreviations: TIBC = total iron binding capacity; UIBC = unsaturated iron-binding capacity
Note: Though total iron-binding capacity is a reflection of the amount of transferrin available, total iron-binding capacity and transferrin are not synonymous.
- Serum iron test—measures the total amount of iron in the liquid portion of the blood, nearly all of which is bound to transferrin.
- Transferrin test—directly measures the level of transferrin in the blood. The level depends upon liver function and a person’s nutritional status. Transferrin is a protein that may decrease during any inflammatory process and is referred to as a negative acute phase reactant.
- TIBC (total iron-binding capacity)—measures the total amount of iron that can be bound by proteins in the blood. Since transferrin is the primary iron-binding protein, the total iron-binding capacity (TIBC) test is a good indirect measurement of transferrin availability—the amount of transferrin that is available to bind to iron.
- UIBC (unsaturated iron-binding capacity)—this test determines the reserve capacity of transferrin, i.e., the portion of transferrin that has not yet been saturated with iron.
- Transferrin saturation— dividing the iron concentration by the total iron-binding capacity (TIBC) produces an estimate of how many of transferrin iron-binding sites are occupied; this is called the transferrin saturation. Under normal conditions, transferrin is typically one-third saturated with iron. This means that about two-thirds of its capacity is held in reserve. (Less commonly, the iron concentration may be divided by the transferrin concentration, not the total iron-binding capacity (TIBC). This similar estimate is usually called the transferrin index.)
- Ferritin—measures the level of ferritin, a protein made by almost all cells in response to increased iron. The ferritin level reflects the total body iron. It will be low when there is iron deficiency and high when there is an excess of iron in the body.
Iron overload
If the iron level and transferrin saturation are high, the total iron-binding capacity (TIBC), unsaturated iron-binding capacity (UIBC) and ferritin are normal and the person has a clinical history consistent with iron overdose, then it is likely that the person has iron poisoning. Iron poisoning occurs when a large dose of iron is taken all at once or over a short period of time. Iron poisoning in children is almost always acute, occurring in children who ingest their parents’ iron supplements. In some cases, acute iron poisoning can be fatal.
In the absence of excessive dietary iron or supplements, raised transferrin saturation may be the earliest indicator of hereditary hemochromatosis, an autosomal recessive condition of progressive iron overload. Men with hereditary hemochromatosis may present with symptoms as early as the fourth decade of life depending on the severity of disease. Women are generally diagnosed after menopause when menstruation and pregnancy can no longer offer protection against iron overload. Elevations in transferrin saturation typically precede a rise in serum ferritin, with levels greater than or equal to 45% being a sensitive marker of early disease.
In patients with chronic iron overload, ferritin levels increase.
A person who has mutations in the HFE gene is diagnosed with hereditary hemochromatosis. However, while many people who have hemochromatosis will have no symptoms for their entire life, others will start to develop symptoms such as joint pain, abdominal pain, and weakness in their 30’s or 40’s. Men are affected more often than women because women lose blood during their reproductive years through menstruation. Early diagnosis and treatment are important in hereditary hemochromatosis in order to avoid organ damage from iron overload and maintain normal life expectancy. It is one of the few conditions where genetic testing of asymptomatic individuals is suggested. Currently, general genetic testing for hereditary hemochromatosis only encompasses detection of mutations in the HFE gene, specifically C282Y and H63D.
Iron overload may also occur in people who have hemosiderosis and in those who have had repeated transfusions. This may occur with sickle cell anemia, thalassemia major, or other forms of transfusion-dependent anemia. The iron from each transfused unit of blood stays in the body, eventually causing a large buildup in the tissues. Some persons with alcoholism and with chronic liver disease also develop iron overload.
Normally, most ferritin is found inside of cells with only a small amount in the blood. Patients with iron overload have high ferritin levels. However, ferritin levels can become elevated under certain condition (e.g., acute illness) even though the total amount of iron in the body is normal.
What other conditions may increase my ferritin levels?
Increased ferritin levels may be seen in alcohol abuse, acute hepatitis, and infections.
Is there any way to cure iron overload?
If it is due to a temporary condition or ingestion of iron supplements, then it will likely resolve on its own once the condition is resolved or supplement ingestion is stopped. If it is due to hemochromatosis or to a chronic disease, then it cannot be cured; careful management by your healthcare practitioner is required. In severe cases, periodic removal of a prescribed amount of blood, also known as therapeutic phlebotomy, may be necessary.
What is hemochromatosis?
Hemochromatosis is an iron metabolism disorder that may be inherited or acquired. People with hemochromatosis accumulate more iron than their body needs. As the body does not have a way to excrete excess iron, there is a progressive buildup of iron in tissues and organs.
Eventually, the iron overload can lead to dysfunction and failure of several organs, notably the heart, liver, and endocrine portion of the pancreas. Complications include arthritis, diabetes, liver cirrhosis, heart arrhythmias and heart failure, and an increase in skin pigmentation called “bronzing.”
There are two types of hemochromatosis: primary hemochromatosis, an inherited form that is passed from one generation to the next, and secondary hemochromatosis, which is caused by some other disease or underlying condition.
Primary or Hereditary Hemochromatosis
Hereditary hemochromatosis, also called primary hemochromatosis, is one of the most common genetic disorders in the U.S., affecting about one million people, most of them Caucasians. The disease is usually caused by a mutation in the HFE gene. Everyone has two copies of the HFE gene – one inherited from their mother and one inherited from their father.
The mutations lead to changes in the building blocks of proteins, termed amino acids, and they are commonly referred to by the changes they induce in these amino acids. For example, the most common mutation involves changing from an amino acid called cysteine (C) to one called tyrosine (Y) in the 282nd amino acid of the protein made by the HFE gene; this mutation is called C282Y.
There are several mutations in the HFE gene that can cause hemochromatosis. The probability of developing iron overload depends on the combination of genes inherited.
Secondary or Acquired Hemochromatosis
Secondary hemochromatosis is an acquired iron overload that can be due to a variety of other diseases and conditions. Examples include:
- Chronic liver disease, such as chronic hepatitis C infection, alcoholic liver disease, or nonalcoholic steatohepatitis (NASH)
- Alcohol abuse
- Some forms of anemia
- Multiple blood transfusions
- Rarely, oral iron supplementation
Hemochromatosis signs and symptoms
According to the National Heart, Lung and Blood Institute, not everyone who has hemochromatosis will have signs and symptoms, and though estimates vary, as many as half of those with the disease may not have any initial symptoms. Signs and symptoms tend to emerge and increase in severity over a long period of time and can be similar to those of other conditions.
Typically, men will not become symptomatic until they are 30-50 years old. Most women with hemochromatosis will not experience symptoms until several years after their period stops due to menopause (around age 50).
Signs and symptoms will vary from person to person and may include:
- Fatigue, weakness
- Abdominal pain
- Joint pain
- Increased blood glucose levels and diabetes
- Liver dysfunction and/or abnormal liver blood tests
- Decreased sex drive, impotence in men
- Lack of menstruation in women
- Hypothyroidism
- Changes in skin color, turning grey or bronze
Hemochromatosis diagnosis and tests
The tests below are used to detect and diagnose hemochromatosis and evaluate body organs for the severity of iron overload. They may also be used to monitor the effectiveness of treatment. Genetic testing may be used to confirm a diagnosis, but since many people who have genetic mutations associated with the disease never develop symptoms, blood tests are considered the most reliable form of diagnosis.
Laboratory tests
Laboratory testing typically includes:
- Serum iron — used to check iron levels in the blood
- Total iron-binding capacity (TIBC) — measures the total amount of iron that can be bound by proteins in the blood; transferrin is the primary iron-binding protein and the TIBC test is a good indirect measurement of transferrin availability.
- Transferrin saturation — a calculation using the iron and total iron-binding capacity (TIBC) test results, representing the percentage of the transferrin that is saturated with iron; it is elevated with hereditary hemochromatosis but is not specific for it.
- Serum ferritin — used to evaluate the body’s iron stores; it may be elevated with hereditary hemochromatosis but is not specific for it. In those who have hereditary hemochromatosis genes, normal levels mean low risk for developing organ damage.
- Liver panel — a group of tests used to evaluate liver function
- Genetic testing — can be used to help confirm a diagnosis of hereditary hemochromatosis. Most cases of hereditary hemochromatosis, about 80-90%, are caused by two copies of a C282Y mutation in the HFE gene. The presence of the C282Y mutation does not necessarily mean that a person will develop the disorder but does indicate an increased risk, and men are more likely to be affected than women. The largest population study found about a 25% risk among men and 1% risk among women. Sometimes an H63D or S65C mutation of the HFE gene or paired combinations of the three may cause hereditary hemochromatosis. Rarely, the condition may be due to another genetic abnormality.
- Liver biopsy — in rare cases, the diagnosis is confirmed by examination of a liver biopsy specimen for iron accumulation and liver damage.
Non-laboratory tests
An MRI (magnetic resonance imaging) test may be used to help evaluate the amount of iron in the liver.
The HFE Gene
The following lists possible gene combinations for the HFE gene:
- Two copies of C282Y or a copy of C282Y together with a copy of H63D or S55C mutant genes places a person at the highest risk for hereditary hemochromatosis.
- Two copies of H63D, S55C, or one copy each of H63D and S55C puts a person in the low risk category and is only rarely associated with hereditary hemochromatosis.
- A single copy of C282Y, H63D or S65C means that the person is a carrier. Carriers do not develop the disease, but they can pass it on to their offspring if they have children with someone who is also a carrier.
Of course, other genes besides the HFE gene can affect a person’s ability to metabolize iron, so no combination of genes guarantees that someone will or will not develop the disease. For example, it is estimated that only about 25% of men and about 1% of women who have two copies of the C282Y mutation will ever develop organ damage related to excess iron.
Hereditary hemochromatosis affects more men than women, and symptoms of the disorder emerge at an earlier age for men, typically at about 30 to 50 years old. Two other rare forms of inherited hemochromatosis, neonatal and juvenile hemochromatosis, can cause severe iron overload in children and young adults. These disorders are caused by mutations in a different gene, one called hemojuvelin. In fact, a small percentage of cases of hereditary hemochromatosis are due to mutations in genes coding for other proteins, including hemojuvelin as well as transferrin-receptor 2, ferroportin and hepcidin. Tests for these mutations are not widely available, however.
Hemochromatosis treatment
The goals of hemochromatosis treatment are to reduce the amount of iron in the body and maintain it at near normal concentrations, to minimize permanent organ damage, and to address complications. If a person has secondary hemochromatosis, then treatment should also address the underlying disorder or condition. Because not all individuals who have the genetic changes need treatment, only those who have organ damage from excess iron are generally treated.
Hemochromatosis is usually treated with phlebotomy therapy, which typically involves the removal of a unit of blood. The frequency and length of treatment depend on the cause and degree of iron overload; for example, in those with severe iron overload, phlebotomy may initially be done once or twice a week, but after the excess iron is removed, phlebotomy may only be done a few times a year with the aim of keeping serum ferritin below 50μg/L.
There is no cure for hereditary hemochromatosis, but it can be successfully managed over a person’s lifetime.
Someone who has secondary hemochromatosis may not require long-term blood removal treatment if the underlying condition can be resolved, and if their iron overload is due to many transfusions, it may not be possible to do phlebotomy if the need for transfusions is still present. There are also drugs that bind iron and allow it to be excreted in the urine, and these may be used for people who cannot safely have phlebotomy performed.
The U.S. Food and Drug Administration has approved the use of blood from hemochromatosis patients as donor blood.
Iron deficiency
Iron deficiency is the most common nutritional deficiency worldwide, with anemia only one part of the clinical spectrum.
It is now recognized that iron deficiency without overt anemia is common, and can adversely affect growth, cognitive performance and behavior in children and
adolescents. Iron deficiency can also reduce immunity to infections, and decrease work capacity and performance in all age groups.
During pregnancy, iron deficiency with anemia is associated with increased risk of maternal and infant mortality 3).
In industrialized nations where poor nutrition and parasitic infestations are uncommon, the diagnosis of iron-deficiency anemia in adult males and postmenopausal females warrants further investigation for a source of blood loss, particularly gastrointestinal malignancy.
Traditionally, serum ferritin concentrations less than or equal to 10-15μg/L have been used to diagnose iron deficiency based on high specificity for strict definitions of iron deficiency anemia, but at the expense of poor sensitivity. Using a cut-off of less than or equal to 30μg/L has been shown to greatly improve sensitivity without much loss in specificity and using a cut-off of 50μg/L has been proposed to reduce the number of false negatives in the investigation of anemic patients for colon cancer 4).
Further support for a higher ferritin cut-off includes observations that levels of 30-50μg/L correlate well with iron deficiency by other measures such as bone marrow iron stores, hepcidin and soluble transferrin receptors, and increasing recognition that low level inflammation may be present in the general community 5).
When interpreting serum ferritin results, one should suspect iron deficiency in adults (including pregnant women) with values less than 30μg/L and in children with values less than 20μg/L.
The diagnosis of iron deficiency in the presence of inflammation is difficult. Even recognising inflammation is not straightforward because markers like C-reactive protein (CRP) are not always elevated, particularly in mild cases. In these situations, measurement of soluble transferrin receptors (sTfR) in serum may prove useful. High levels of soluble transferrin receptors (sTfR) are a sensitive indicator of iron deficiency.
The early stage of iron deficiency is the slow depletion of iron stores. This means there is still enough iron to make red cells but the stores are being used up without adequate replacement. The serum iron level may be normal in this stage, but the ferritin level will be low.
As iron deficiency continues, all of the stored iron is used and the body tries to compensate by producing more transferrin to increase iron transport. The serum iron level continues to decrease and transferrin and total iron-binding capacity (TIBC) and unsaturated iron-binding capacity (UIBC) increase. As this stage progresses, fewer and smaller red blood cells are produced, eventually resulting in iron deficiency anemia. Transferrin saturation is decreased with iron deficiency.
The expression of transferrin receptors on cell membranes is up-regulated when body iron needs are increased such as in iron deficiency or in conditions of increased erythropoiesis such as polycythemia rubra vera. Serum concentrations of transferrin receptors are proportional to membrane-associated levels and are not an acute phase reactant.
Iron deficiency treatment
There is now a greater appreciation for the spectrum of clinical iron deficiency and that supplementation, especially in children and adolescents, may reverse declines in outcomes such as cognitive functioning and physical performance.
The management recommendations for iron deficiency is to commence iron supplementation and explore the possible causes for the iron deficiency.
- Oral preparations (3-6mg/kg elemental iron per day for children) are usually sufficient as first-line management of iron deficiency 6).
- Intravenous iron may be considered in selected patients, especially in the presence of iron deficiency anemia, including those with demonstrated malabsorption or intolerance to oral iron, and where there is a clinical
need for rapid iron supply 7).
In infants and children, contributing factors to iron deficiency may include insufficient dietary intake, prematurity, increased requirements during periods of rapid growth, malabsorption (eg, celiac disease) and blood loss.
Response to therapy should be assessed clinically and by re-measuring serum ferritin in six weeks.
My iron level is normal, but my ferritin level is low. Why is that?
The development of iron deficiency anemia is a gradual process. If your body is not taking in enough iron, your body first uses the iron that is stored in tissues (i.e., ferritin) and blood levels of ferritin will begin to decrease. If not corrected, the stored iron begins to be depleted as it is used in the production of red blood cells. In the early stages of iron-deficiency, blood levels of iron can be normal while stored iron, and therefore ferritin levels, will begin to decrease.
Will eating foods high in iron or taking iron supplements increase my iron level, and also increase my ferritin level?
Yes. Taking in more iron will increase the level of iron in your body. If the level of iron in your body increases and is more than your body requires, then your body will begin to store more iron in the form of ferritin.
High ferritin
A raised serum ferritin is not an uncommon finding in the general community and although most cases are not due to hereditary haemochromatosis, it is reasonable to consider genetic testing for HFE gene mutations (i.e., hereditary hemochromatosis) in persistent high ferritin cases. Inflammation, infection, malignancy, hepatic and renal disease may all account for ferritin elevations. They often occur in combination, for example, in addition to the inflammation associated with chronic hepatitis infection, virus-damaged hepatocytes may leak ferritin into the circulation.
Alcohol abuse can also raise serum ferritin levels with beer having a greater effect than spirits or wine with an equivalent amount of alcohol 8).
Elevated serum ferritin can also be seen with fatty liver, metabolic syndrome, obesity and diabetes mellitus.
Serum ferritin also rises in women after menopause with the cessation of menstruation.
It is unclear whether there are any long-term health implications from persistently high ferritin levels due to, for example, chronic inflammation, and therapeutic venesection may be considered.
How to reduce high ferritin levels
Hemochromatosis is usually treated with phlebotomy therapy, which typically involves the removal of a unit of blood. The frequency and length of treatment depend on the cause and degree of iron overload; for example, in those with severe iron overload, phlebotomy may initially be done once or twice a week, but after the excess iron is removed, phlebotomy may only be done a few times a year with the aim of keeping serum ferritin below 50μg/L.
There is no cure for hereditary hemochromatosis, but it can be successfully managed over a person’s lifetime.
Someone who has secondary hemochromatosis may not require long-term blood removal treatment if the underlying condition can be resolved, and if their iron overload is due to many transfusions, it may not be possible to do phlebotomy if the need for transfusions is still present. There are also drugs that bind iron and allow it to be excreted in the urine, and these may be used for people who cannot safely have phlebotomy performed.
The U.S. Food and Drug Administration has approved the use of blood from hemochromatosis patients as donor blood.
Low ferritin
A serum ferritin concentration less than 30μg/L in an adult or 20μg/L in a child indicates iron deficiency. The cause of the iron deficiency should be identified, and is particularly important in men and post-menopausal women, where this might be the first sign of bowel cancer.
Iron deficiency is the most common nutritional deficiency worldwide, with anemia only one part of the clinical spectrum.
It is now recognized that iron deficiency without overt anemia is common, and can adversely affect growth, cognitive performance and behavior in children and
adolescents. Iron deficiency can also reduce immunity to infections, and decrease work capacity and performance in all age groups.
During pregnancy, iron deficiency with anemia is associated with increased risk of maternal and infant mortality 9).
In industrialized nations where poor nutrition and parasitic infestations are uncommon, the diagnosis of iron-deficiency anemia in adult males and postmenopausal females warrants further investigation for a source of blood loss, particularly gastrointestinal malignancy.
Traditionally, serum ferritin concentrations less than or equal to 10-15μg/L have been used to diagnose iron deficiency based on high specificity for strict definitions of iron deficiency anemia, but at the expense of poor sensitivity. Using a cut-off of less than or equal to 30μg/L has been shown to greatly improve sensitivity without much loss in specificity and using a cut-off of 50μg/L has been proposed to reduce the number of false negatives in the investigation of anemic patients for colon cancer 10).
Further support for a higher ferritin cut-off includes observations that levels of 30-50μg/L correlate well with iron deficiency by other measures such as bone marrow iron stores, hepcidin and soluble transferrin receptors, and increasing recognition that low level inflammation may be present in the general community 11).
When interpreting serum ferritin results, one should suspect iron deficiency in adults (including pregnant women) with values less than 30μg/L and in children with values less than 20μg/L.
The diagnosis of iron deficiency in the presence of inflammation is difficult. Even recognising inflammation is not straightforward because markers like C-reactive protein (CRP) are not always elevated, particularly in mild cases. In these situations, measurement of soluble transferrin receptors (sTfR) in serum
may prove useful. High levels of soluble transferrin receptors (sTfR) are a sensitive indicator of iron deficiency.
The early stage of iron deficiency is the slow depletion of iron stores. This means there is still enough iron to make red cells but the stores are being used up without adequate replacement. The serum iron level may be normal in this stage, but the ferritin level will be low.
As iron deficiency continues, all of the stored iron is used and the body tries to compensate by producing more transferrin to increase iron transport. The serum iron level continues to decrease and transferrin and total iron-binding capacity (TIBC) and unsaturated iron-binding capacity (UIBC) increase. As this stage progresses, fewer and smaller red blood cells are produced, eventually resulting in iron deficiency anemia. Transferrin saturation is decreased with iron deficiency.
The expression of transferrin receptors on cell membranes is up-regulated when body iron needs are increased such as in iron deficiency or in conditions of increased erythropoiesis such as polycythemia rubra vera. Serum concentrations of transferrin receptors are proportional to membrane-associated levels and are not an acute phase reactant.
Iron deficiency treatment
There is now a greater appreciation for the spectrum of clinical iron deficiency and that supplementation, especially in children and adolescents, may reverse declines in outcomes such as cognitive functioning and physical performance.
The management recommendations for iron deficiency is to commence iron supplementation and explore the possible causes for the iron deficiency.
- Oral preparations (3-6mg/kg elemental iron per day for children) are usually sufficient as first-line management of iron deficiency 12).
- Intravenous iron may be considered in selected patients, especially in the presence of iron deficiency anemia, including those with demonstrated malabsorption or intolerance to oral iron, and where there is a clinical
need for rapid iron supply 13).
In infants and children, contributing factors to iron deficiency may include insufficient dietary intake, prematurity, increased requirements during periods of rapid growth, malabsorption (eg, celiac disease) and blood loss.
Response to therapy should be assessed clinically and by re-measuring serum ferritin in six weeks.
Low ferritin symptoms
Initially, iron deficiency anemia can be so mild that it goes unnoticed. But as the body becomes more deficient in iron and anemia worsens, the signs and symptoms intensify.
Iron deficiency anemia signs and symptoms may include:
- Extreme fatigue
- Tiredness and lack of energy
- Weakness
- Pale skin
- Chest pain, fast heartbeat or shortness of breath
- Shortness of breath
- Noticeable heartbeats (heart palpitations)
- Headache, dizziness or lightheadedness
- Cold hands and feet
- Inflammation or soreness of your tongue
- Brittle nails
- Unusual cravings for non-nutritive substances, such as ice, dirt or starch
- Poor appetite, especially in infants and children with iron deficiency anemia
Less common symptoms of iron deficiency anemia (that are not usually connected to pregnancy) include:
- headache
- hearing ringing, buzzing or hissing noises inside your head (tinnitus)
- food tasting strange
- feeling itchy
- a sore tongue
- hair loss – you notice more hair coming out when brushing or washing it
- wanting to eat non-food items (for example, paper or ice) – called pica
- finding it hard to swallow (dysphagia)
- painful open sores (ulcers) in the corners of your mouth
- spoon-shaped nails
- restless legs syndrome
Low ferritin causes
Iron deficiency anemia occurs when your body doesn’t have enough iron to produce hemoglobin. Hemoglobin is the part of red blood cells that gives blood its red color and enables the red blood cells to carry oxygenated blood throughout your body.
If you aren’t consuming enough iron, or if you’re losing too much iron, your body can’t produce enough hemoglobin, and iron deficiency anemia will eventually develop.
Causes of iron deficiency anemia include:
- Blood loss. Blood contains iron within red blood cells. So if you lose blood, you lose some iron. Women with heavy periods are at risk of iron deficiency anemia because they lose blood during menstruation. Slow, chronic blood loss within the body — such as from a peptic ulcer, a hiatal hernia, a colon polyp or colorectal cancer — can cause iron deficiency anemia. Gastrointestinal bleeding can result from regular use of some over-the-counter pain relievers, especially aspirin.
- A lack of iron in your diet. Your body regularly gets iron from the foods you eat. If you consume too little iron, over time your body can become iron deficient. Examples of iron-rich foods include meat, eggs, leafy green vegetables and iron-fortified foods. For proper growth and development, infants and children need iron from their diets, too.
- An inability to absorb iron. Iron from food is absorbed into your bloodstream in your small intestine. An intestinal disorder, such as celiac disease, which affects your intestine’s ability to absorb nutrients from digested food, can lead to iron deficiency anemia. If part of your small intestine has been bypassed or removed surgically, that may affect your ability to absorb iron and other nutrients.
- Pregnancy. Without iron supplementation, iron deficiency anemia occurs in many pregnant women because their iron stores need to serve their own increased blood volume as well as be a source of hemoglobin for the growing fetus.
Risk factors for developing iron deficiency anemia
These groups of people may have an increased risk of iron deficiency anemia:
- Women. Because women lose blood during menstruation, women in general are at greater risk of iron deficiency anemia.
- Infants and children. Infants, especially those who were low birth weight or born prematurely, who don’t get enough iron from breast milk or formula may be at risk of iron deficiency. Children need extra iron during growth spurts. If your child isn’t eating a healthy, varied diet, he or she may be at risk of anemia.
- Vegetarians. People who don’t eat meat may have a greater risk of iron deficiency anemia if they don’t eat other iron-rich foods.
- Frequent blood donors. People who routinely donate blood may have an increased risk of iron deficiency anemia since blood donation can deplete iron stores. Low hemoglobin related to blood donation may be a temporary problem remedied by eating more iron-rich foods. If you’re told that you can’t donate blood because of low hemoglobin, ask your doctor whether you should be concerned.
Complications of iron deficiency anemia
Mild iron deficiency anemia usually doesn’t cause complications. However, left untreated, iron deficiency anemia can become severe and lead to health problems, including the following:
- Heart problems. Iron deficiency anemia may lead to a rapid or irregular heartbeat. Your heart must pump more blood to compensate for the lack of oxygen carried in your blood when you’re anemic. This can lead to an enlarged heart or heart failure.
- Problems during pregnancy. In pregnant women, severe iron deficiency anemia has been linked to premature births and low birth weight babies. But the condition is preventable in pregnant women who receive iron supplements as part of their prenatal care.
- Growth problems. In infants and children, severe iron deficiency can lead to anemia as well as delayed growth and development.
- Iron deficiency anemia is associated with an increased susceptibility to infections and illness – a lack of iron affects the immune system
Prevention of iron deficiency
You can reduce your risk of iron deficiency anemia by choosing iron-rich foods.
Choose iron-rich foods
Foods rich in iron include:
- Red meat, pork and poultry
- Seafood
- Beans
- Dark green leafy vegetables, such as spinach
- Dried fruit, such as raisins and apricots
- Iron-fortified cereals, breads and pastas
- Peas
Your body absorbs more iron from meat than it does from other sources. If you choose to not eat meat, you may need to increase your intake of iron-rich, plant-based foods to absorb the same amount of iron as does someone who eats meat.
Choose foods containing vitamin C to enhance iron absorption
You can enhance your body’s absorption of iron by drinking citrus juice or eating other foods rich in vitamin C at the same time that you eat high-iron foods. Vitamin C in citrus juices, like orange juice, helps your body to better absorb dietary iron.
Vitamin C is also found in:
- Broccoli
- Grapefruit
- Kiwi
- Leafy greens
- Melons
- Oranges
- Peppers
- Strawberries
- Tangerines
- Tomatoes
Preventing iron deficiency anemia in infants
To prevent iron deficiency anemia in infants, feed your baby breast milk or iron-fortified formula for the first year. Cow’s milk isn’t a good source of iron for babies and isn’t recommended for infants under 1 year. After age 6 months, start feeding your baby iron-fortified cereals or pureed meats at least twice a day to boost iron intake. After one year, be sure children don’t drink more than 20 ounces (591 milliliters) of milk a day. Too much milk often takes the place of other foods, including those that are rich in iron.
Iron deficiency anemia diagnosis and tests
To diagnose iron deficiency anemia, your doctor may run tests to look for:
- Red blood cell size and color. With iron deficiency anemia, red blood cells are smaller and paler in color than normal.
- Hematocrit. This is the percentage of your blood volume made up by red blood cells. Normal levels are generally between 34.9 and 44.5 percent for adult women and 38.8 to 50 percent for adult men. These values may change depending on your age.
- Hemoglobin. Lower than normal hemoglobin levels indicate anemia. The normal hemoglobin range is generally defined as 13.5 to 17.5 grams (g) of hemoglobin per deciliter (dL) of blood for men and 12.0 to 15.5 g/dL for women. The normal ranges for children vary depending on the child’s age and sex.
- Ferritin. This protein helps store iron in your body, and a low level of ferritin usually indicates a low level of stored iron.
Additional diagnostic tests
If your blood work indicates iron deficiency anemia, your doctor may order additional tests to identify an underlying cause, such as:
- Endoscopy. Doctors often check for bleeding from a hiatal hernia, an ulcer or the stomach with the aid of endoscopy. In this procedure, a thin, lighted tube equipped with a video camera is passed down your throat to your stomach. This allows your doctor to view the tube that runs from your mouth to your stomach (esophagus) and your stomach to look for sources of bleeding.
- Colonoscopy. To rule out lower intestinal sources of bleeding, your doctor may recommend a procedure called a colonoscopy. A thin, flexible tube equipped with a video camera is inserted into the rectum and guided to your colon. You’re usually sedated during this test. A colonoscopy allows your doctor to view inside some or all of your colon and rectum to look for internal bleeding.
- Ultrasound. Women may also have a pelvic ultrasound to look for the cause of excess menstrual bleeding, such as uterine fibroids.
Your doctor may order these or other tests after a trial period of treatment with iron supplementation.
How to increase ferritin
To treat iron deficiency anemia, your doctor may recommend that you take iron supplements. Your doctor will also treat the underlying cause of your iron deficiency, if necessary.
Iron supplements
Your doctor may recommend over-the-counter iron tablets to replenish the iron stores in your body. Your doctor will let you know the correct dose for you. Iron is also available in liquid form for infants and children. To improve the chances that your body will absorb the iron in the tablets, you may be instructed to:
- Take iron tablets on an empty stomach. If possible, take your iron tablets when your stomach is empty. However, because iron tablets can upset your stomach, you may need to take your iron tablets with meals.
- Don’t take iron with antacids. Medications that immediately relieve heartburn symptoms can interfere with the absorption of iron. Take iron two hours before or four hours after you take antacids.
- Take iron tablets with vitamin C. Vitamin C improves the absorption of iron. Your doctor might recommend taking your iron tablets with a glass of orange juice or with a vitamin C supplement.
Iron supplements can cause constipation, so your doctor may also recommend a stool softener. Iron may turn your stools black, which is a harmless side effect.
Iron deficiency can’t be corrected overnight. You may need to take iron supplements for several months or longer to replenish your iron reserves. Generally, you’ll start to feel better after a week or so of treatment. Ask your doctor when to have your blood rechecked to measure your iron levels. To be sure that your iron reserves are replenished, you may need to take iron supplements for a year or more.
Treating underlying causes of iron deficiency
If iron supplements don’t increase your blood-iron levels, it’s likely the anemia is due to a source of bleeding or an iron-absorption problem that your doctor will need to investigate and treat. Depending on the cause, iron deficiency anemia treatment may involve:
- Medications, such as oral contraceptives to lighten heavy menstrual flow
- Antibiotics and other medications to treat peptic ulcers
- Surgery to remove a bleeding polyp, a tumor or a fibroid
If iron deficiency anemia is severe, you may need iron given intravenously or you may need blood transfusions to help replace iron and hemoglobin quickly.
References [ + ]





{kind=link}