Contents
What is flat feet
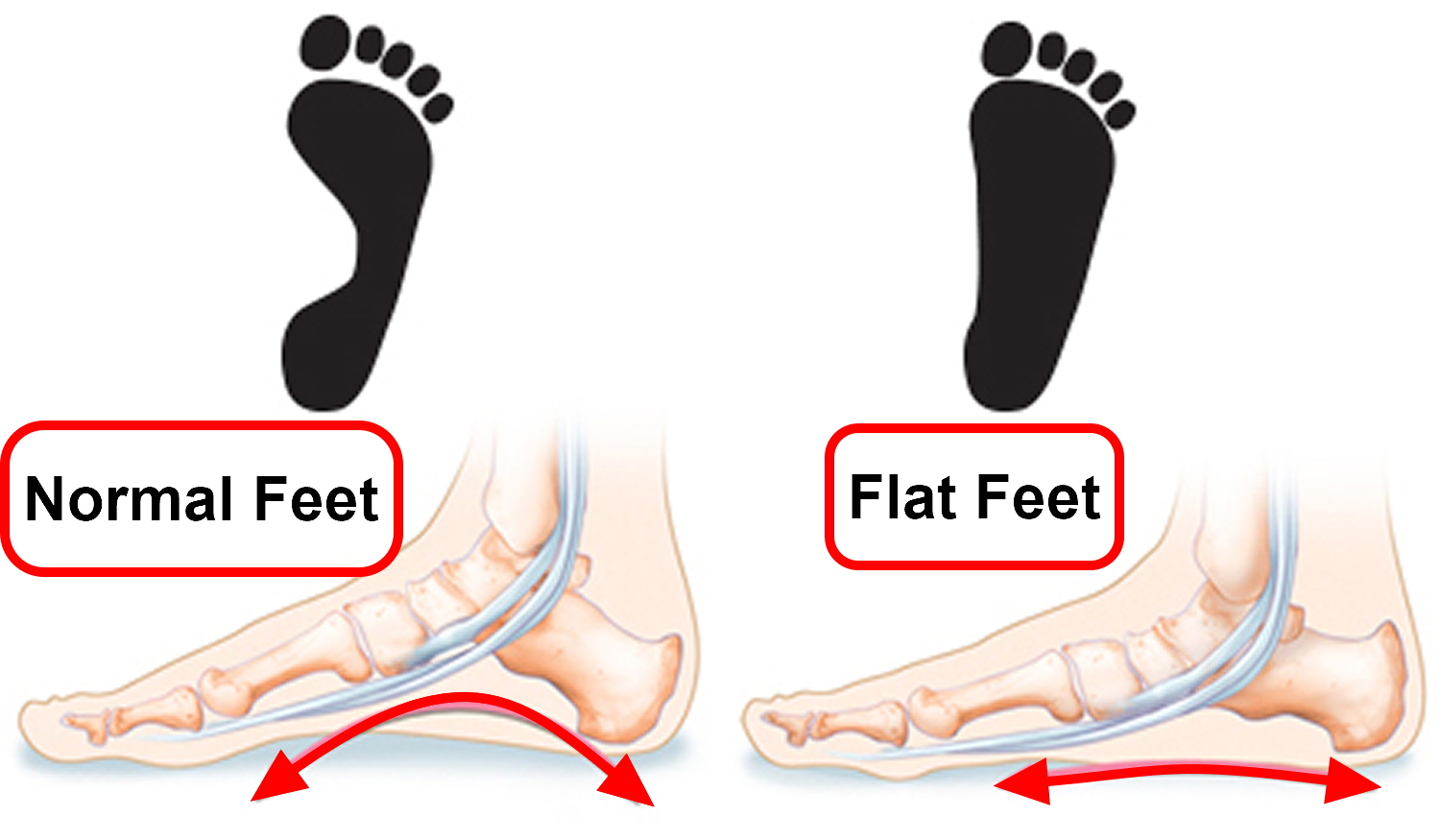
Flat feet or fallen arches means that your feet have low or no arches and press almost completely flat against the ground when you stand up. The arch or instep, is the middle part of the foot that’s usually raised off the ground when you stand, while the rest of the foot remains flat on the ground.
In young children, this arch isn’t always visible because of the baby fat and soft tissue in their feet. It usually develops and appears as they get older.
But some people never really develop this arch. Sometimes this is because they inherited flat feet from their parents.
Flat feet (fallen arches) is a common and usually painless condition, flatfeet can occur when the arches don’t develop during childhood. In other cases, flatfeet develop after an injury or from the simple wear-and-tear stresses of age.
Flatfeet can sometimes contribute to problems in your ankles and knees because the condition can alter the alignment of your legs. If you aren’t having pain, no treatment is usually necessary for flatfeet.
Figure 1. Flat feet

Are flat feet a problem?
Flat feet are usually nothing to worry about. Many people with flat feet don’t have any associated problems, so treatment isn’t necessary.
But flat feet can sometimes be associated with:
- pain in the feet, ankles, lower legs, knees, hips or lower back
- the feet rolling inwards too much (overpronation) – this can cause shoes to wear out quickly and lead to injuries
- an underlying problem with the bones, muscles or connective tissues in and around the feet
Treatment may be recommended if you have any of these problems.
Consider seeing your doctor if you have flat feet and your:
- feet are painful, even when wearing supportive, well-fitting shoes
- shoes wear out very quickly
- feet appear to be getting flatter
- feet are weak, numb or stiff
Your doctor will examine your foot and may be able to advise you about treatments that can help.
If necessary, they may be able to refer you to a podiatrist (a specialist in foot problems) or orthopedic surgeon to discuss possible treatments.
You can also contact a podiatrist or orthopedic surgeon directly if you’re considering private treatment.
Flat Feet Outlook (Prognosis)
Most cases of flat feet are painless and do not cause any problems. They will not need treatment.
Some causes of painful flat feet can be treated without surgery. If other treatments do not work, surgery may be needed to relieve pain in some cases.
Surgery often improves pain and foot function for people who need it.
What causes flat feet
Many people simply inherit flat feet from their parents.
Occasionally, flat feet can be the result of:
- the feet bones not forming properly in the womb
- loose connective tissue throughout the body, such as in Ehlers-Danlos syndrome or joint hypermobility syndrome
- a condition affecting the muscles and nerves, such as cerebral palsy, spina bifida or muscular dystrophy
- the connective tissue in the foot becoming stretched and inflamed – possibly as a result of overuse, unsupportive footwear, an injury, increasing age, obesity or rheumatoid arthritis.
Risk factors for flat feet
Factors that can increase your risk of flatfeet include:
- Obesity
- Injury to your foot or ankle
- Rheumatoid arthritis
- Aging
- Diabetes
Adult Acquired Flat Feet
Arthritis
Inflammatory arthritis, such as rheumatoid arthritis, can cause a painful flatfoot. This type of arthritis attacks not only the cartilage in the joints, but also the ligaments that support the foot. Inflammatory arthritis not only causes pain, but also causes the foot to change shape and become flat.
The arthritis can affect the back of the foot or the middle of foot, both of which can result in a fallen arch.
Rheumatoid Arthritis of the Foot and Ankle
Rheumatoid arthritis affects approximately 1% of the population. Women are affected more often than men, with a ratio of up to 3 to 1. Symptoms most commonly develop between the ages of 40 and 60.
The joints of your body are covered with a lining — called synovium — that lubricates the joint and makes it easier to move. Rheumatoid arthritis causes an overactivity of this lining. It swells and becomes inflamed, destroying the joint, as well as the ligaments and other tissues that support it. Weakened ligaments can cause joint deformities — such as claw toe or hammer toe. Softening of the bone (osteopenia) can result in stress fractures and collapse of bone.
Rheumatoid arthritis is not an isolated disease of the bones and joints. It affects tissues throughout the body, causing damage to the blood vessels, nerves, and tendons. Deformities of the hands and feet are the more obvious signs of rheumatoid arthritis. In about 20% of patients, foot and ankle symptoms are the first signs of the disease.
Rheumatoid arthritis cause
The exact cause of rheumatoid arthritis is not known. There may be a genetic reason — some people may be more likely to develop the disease because of family heredity. However, doctors suspect that it takes a chemical or environmental “trigger” to activate the disease in people who inherit rheumatoid arthritis.
Rheumatoid arthritis symptoms
The most common symptoms are pain, swelling, and stiffness. Unlike osteoarthritis, which typically affects one specific joint, symptoms of rheumatoid arthritis usually appear in both feet, affecting the same joints on each foot.
Rheumatoid arthritis Nonsurgical Treatment
Although there is no cure for rheumatoid arthritis, there are many treatment options available to help people manage pain, stay active, and live fulfilling lives.
Rheumatoid arthritis is often treated by a team of healthcare professionals. These professionals may include rheumatologists, physical and occupational therapists, social workers, rehabilitation specialists, and orthopedic surgeons.
Although orthopedic treatment may relieve symptoms, it will not stop the progression of the disease. Specific medicines called disease-modifying anti-rheumatic drugs are designed to stop the immune system from destroying the joints. The appropriate use of these medications is directed by a rheumatologist.
Orthopedic treatment of rheumatoid arthritis depends on the location of the pain and the extent of cartilage damage. Many patients will have some symptom relief with appropriate nonsurgical treatment.
- Rest
Limiting or stopping activities that make the pain worse is the first step in minimizing the pain. Biking, elliptical training machines, or swimming are exercise activities that allow patients to maintain their health without placing a large impact load on the foot.
- Ice
Placing ice on the most painful area of the foot for 20 minutes is effective. This can be done 3 or 4 times a day. Ice application is best done right after you are done with a physical activity. Do not apply ice directly to your skin.
- Nonsteroidal Anti-inflammatory Medication
Drugs, such as ibuprofen or naproxen, reduce pain and inflammation. In patients with rheumatoid arthritis, the use of these types of medications should be reviewed with your rheumatologist or medical doctor.
- Orthotics
An orthotic (shoe insert) is a very effective tool to minimize the pressure from prominent bones in the foot. The orthotic will not be able to correct the shape of your foot. The primary goal is to minimize the pressure and decrease the pain and callous formation. This is more effective for deformity in the front and middle of the foot.
For people with rheumatoid arthritis, hard or rigid orthotics generally cause too much pressure on the bone prominences, creating more pain. A custom orthotic is generally made of softer material and relieves pressure on the foot.
- Braces
A lace-up ankle brace can be an effective treatment for mild to moderate pain in the back of the foot and the ankle. The brace supports the joints of the back of the foot and ankle. In patients with a severe flatfoot or a very stiff arthritic ankle, a custom-molded plastic or leather brace is needed. The brace can be a very effective device for some patients, allowing them to avoid surgery.
- Steroid Injection
An injection of cortisone into the affected joint can help in the early stages of the disease. In many cases, a rheumatologist or medical doctor may also perform these injections. The steroid helps to reduce inflammation within the joint. The steroid injection is normally a temporary measure and will not stop the progression of the disease.
- Surgical Treatment
Your doctor may recommend surgery depending upon the extent of cartilage damage and your response to nonsurgical options.
Preparing for Surgery
Many of the medications that help with rheumatoid arthritis also affect the ability of the body to heal wounds and fight infection. Your surgeon will work with your rheumatologist or medical doctor to review which of your medications will need to be stopped prior to surgery. Once the wounds are healed, the medication is typically resumed.
This period of time can be very difficult for patients with other areas of the body that are affected by rheumatoid arthritis. Many fusions require at least 6 weeks of time where no pressure can be placed on the foot. Making appropriate preparations to ensure you have help at home is crucial for success after surgery.
- Fusion. Fusion of the affected joints is the most common type of surgery performed for rheumatoid arthritis. Fusion takes the two bones that form a joint and fuses them together to make one bone. During the surgery, the joints are exposed and the remaining cartilage is removed. The two bones are then held together with screws or a combination of screws and plates. This prevents the bones from moving. Because the joint is no longer intact, this surgery does limit joint motion. Limited joint motion may not be felt by the patient, depending on the joints fused. The midfoot joints often do not have much motion to begin with, and fusing them does not create increased stiffness. The ankle joint normally does have a lot of motion, and fusing it will be noticeable to the patient. By limiting motion, fusion reduces the pain. Fusion can be a successful technique. However, because patients with rheumatoid arthritis also show damaged cartilage and loose ligaments, the success rate of this type of surgery is lower in patients with rheumatoid arthritis than in patients without rheumatoid arthritis. The use of newer generation medication can slow the progression of the disease and impact the type of surgeries that can be performed successfully.
- Other surgeries. The front of the foot is where there are more surgical options for some patients. Surgeons can now perform joint sparing operations to correct the bunion and hammertoes in some patients. Your surgeon will review the most appropriate options for your case.
Midfoot (Middle of the Foot)
Fusion is the most reliable surgical method to treat rheumatoid arthritis of the midfoot joints. If the shape of the foot is not normal, surgery is designed to help restore the arch and minimize the prominences on the foot.
There are joint replacement implants available for joints on the outside of the midfoot. This may preserve some midfoot motion. However, the use of these implants is at the surgeon’s discretion. These implants are not available for the joints on the inside of the midfoot.
Although the foot cannot be returned to a normal shape, the goals are to reduce pain in the foot and improve the potential for the patient to wear more normal shoes.
Injury
An injury to the ligaments in the foot can cause the joints to fall out of alignment. The ligaments support the bones and prevent them from moving. If the ligaments are torn, the foot will become flat and painful. This more commonly occurs in the middle of the foot (Lisfranc injury), but can also occur in the back of the foot.
In addition to ligament injuries, fractures and dislocations of the bones in the midfoot can also lead to a flatfoot deformity.
Lisfranc (Midfoot) Injury
Lisfranc (midfoot) injuries result if bones in the midfoot are broken or ligaments that support the midfoot are torn. The severity of the injury can vary from simple to complex, involving many joints and bones in the midfoot.
A Lisfranc injury is often mistaken for a simple sprain, especially if the injury is a result of a straightforward twist and fall. However, injury to the Lisfranc joint is not a simple sprain that should be simply “walked off.” It is a severe injury that may take many months to heal and may require surgery to treat.
Figure 2. Bones of foot (right foot)
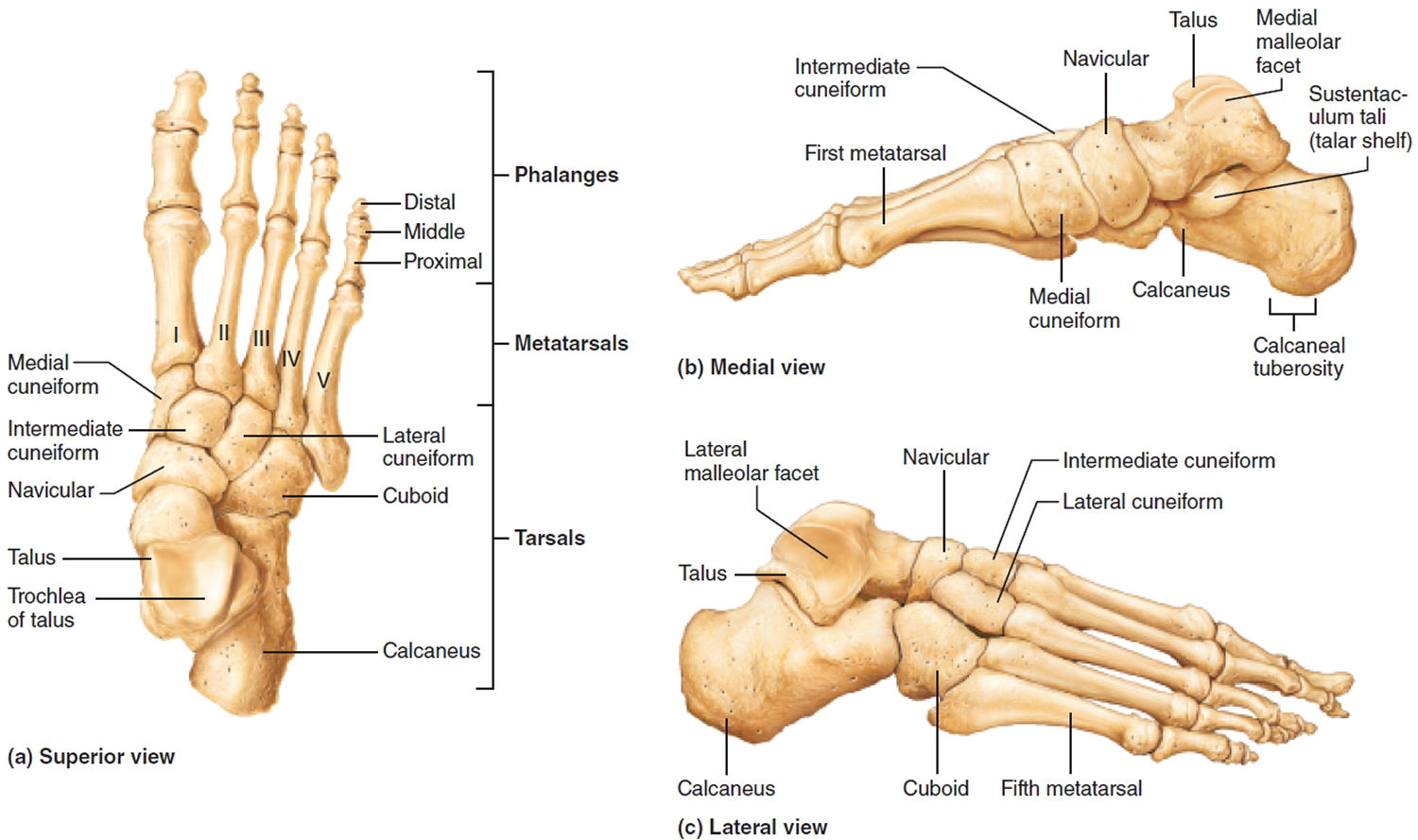
The foot has three arches: the medial and lateral longitudinal arches and the transverse arch. These arches are maintained by the interlocking shapes of the foot bones, by strong ligaments, and by the pull of some tendons during muscle activity; the ligaments and tendons also provide resilience. As a result, the arches “give” when weight is applied to the foot, then spring back when the weight is removed.
- The medial longitudinal arch curves well above the ground. The talus, near the talonavicular joint, is the keystone of this arch which originates at the
calcaneus, rises to the talus, and then descends to the three medial metatarsals. - The lateral longitudinal arch is very low. It elevates the lateral edge of the foot just enough to redistribute some of the body weight to the calcaneus and some to the head of the fifth metatarsal (that is, to the two ends of the arch). The cuboid bone is the keystone of this lateral arch.
- The two longitudinal arches serve as pillars for the transverse arch, which runs obliquely from one side of the foot to the other, following the line of the joints between the tarsals and metatarsals. Together, the three arches form a half dome that distributes approximately half of a person’s standing and walking weight to the heel bones and half to the heads of the metatarsals.
Anatomy
The midfoot is the middle region of the foot, where a cluster of small bones forms an arch on the top of the foot. From this cluster, five long bones (metatarsals) extend to the toes. The bones are held in place by connective tissues (ligaments) that stretch both across and down the foot. However, there is no connective tissue holding the first metatarsal to the second metatarsal. A twisting fall can break or shift (dislocate) these bones out of place.
The midfoot is critical in stabilizing the arch and in walking (gait). During walking, the midfoot transfers the forces generated by the calf muscles to the front of the foot.
The midfoot joint complex is also called the Lisfranc joint. It is named after French surgeon Jacques Lisfranc de St. Martin, who served in the Napoleonic army in the 1800s.
The Lisfranc joint complex has a specialized bony and ligamentous structure, providing stability to this joint.
The Lisfranc joint complex includes the bones and ligaments that connect the midfoot and forefoot. Lisfranc injuries include ligament strains and tears, as well as fractures and dislocations of bone.
The midfoot will be affected if the bones are broken (fractured) or the ligaments are torn (ruptured). Injuries can vary, from a simple injury that affects only a single joint to a complex injury that disrupts multiple different joints and includes multiple fractures.
Lisfranc injuries tend to damage the cartilage of the midfoot joints. Cartilage covers the ends of bones in the joints, allowing the joints to move smoothly. If severe midfoot injuries are not treated with surgery, then damage to the cartilage and increased stress at the midfoot joints will result in both collapse of the arch and arthritis, which require complex surgery to correct. Even with successful surgery for the Lisfranc injury, arthritis can still develop in later life.
Figure 3. Lisfranc midfoot injuries
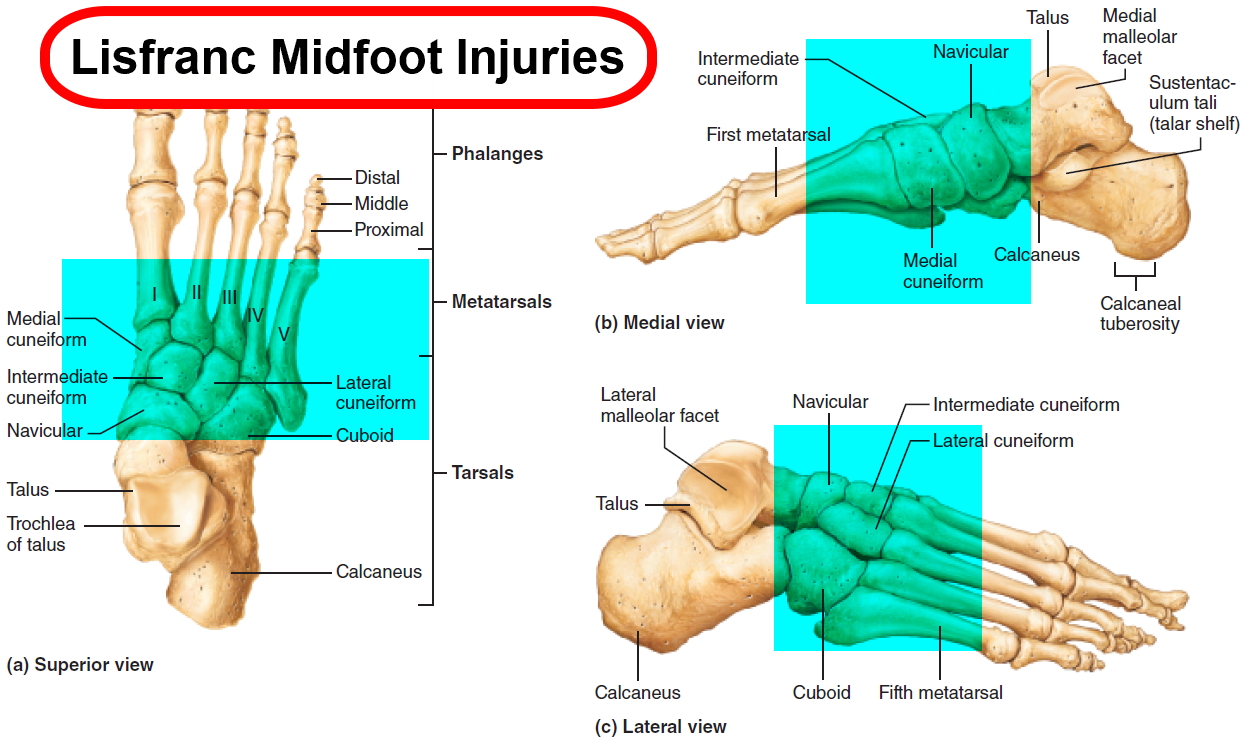 Figure 4. Lisfranc midfoot injuries (X-ray)
Figure 4. Lisfranc midfoot injuries (X-ray)
Note: (Left) A subtle injury to the midfoot with widening between the first and second metatarsals (circle), compared with the normal foot on the left. (Center) A fracture of the second metatarsal (arrow) and a fracture of the cuboid (circle). (Right) A very severe injury of the foot from a high-energy event. It has resulted in a complete dislocation of the entire midfoot (box). Because no bones have been broken, a fusion may be recommended, given the high risk for future arthritis.
Lisfranc injuries cause
These injuries can happen with a simple twist and fall. This is a low-energy injury. It is commonly seen in football and soccer players. It is often seen when someone stumbles over the top of a foot flexed downwards.
More severe injuries occur from direct trauma, such as a fall from a height. These high-energy injuries can result in multiple fractures and dislocations of the joints.
Lisfranc injuries symptoms
The most common symptoms of Lisfranc injury include:
- The top of foot may be swollen and painful.
- There may be bruising on both the top and bottom of the foot. Bruising on the bottom of the foot is highly suggestive of a Lisfranc injury.
- Pain that worsens with standing, walking or attempting to push off on the affected foot. The pain can be so severe that crutches may be required.
If standard treatment for a sprain (rest, ice, elevation) does not relieve pain and swelling, you should seek care from an orthopedic surgeon.
Lisfranc (midfoot) injuries treatment
Treatment for a Lisfranc injury depends on how severe the injury is.
- Nonsurgical Treatment
If there are no fractures or dislocations in the joint and the ligaments are not completely torn, nonsurgical treatment may be all that is necessary for healing. A nonsurgical treatment plan includes wearing a non-weightbearing cast or boot for 6 weeks. You must be very strict about not putting weight on your injured foot during this period. This then progresses to weightbearing in a removable cast boot or an orthotic.
Your doctor will want to follow up with you regularly and take additional x-rays to make sure your foot is healing well. In the course of follow up, if there is any evidence that the bones in the injured joint have moved, then surgery will be needed to put the bones back in place.
- Surgical Treatment
Surgery is recommended for all injuries with a fracture in the joints of the midfoot or with abnormal positioning (subluxation) of the joints. The goal of surgical treatment is to realign the joints and return the broken (fractured) bone fragments to a normal position.
Internal fixation. In this procedure, the bones are positioned correctly (reduced) and held in place with plates or screws. Because the plates or screws will be placed across joints that normally have some motion, some or all of this hardware may be removed at a later date. This can vary from 3 to 5 months after surgery, and is at the surgeon’s discretion.
Occasionally, the hardware may break before it is removed. This is not unusual when screws or plates span bones that have some movement. Metal can fatigue and fail under these conditions, just as a paperclip will fail if bent repeatedly. Most often surgery is successful even if some of the hardware fails.
Fusion. If the injury is severe and has damage that cannot be repaired, fusion may be recommended as the initial surgical procedure. A fusion is essentially a “welding” process. The basic idea is to fuse together the damaged bones so that they heal into a single, solid piece.
The joints in the midfoot have very little motion and mainly transfer stress to the front of the foot. Therefore, patients who do require fusion surgery can still have a relatively normal gait.
Lisfranc injuries that may require fusion include joints that cannot be repaired with screws or plates or when the ligaments are severely ruptured. The hardware will not need to be removed because the joints are fused and will not move after they heal.
Rehabilitation. After either surgery (reduction or fusion), a period of non-weightbearing for 6 to 8 weeks is recommended in a cast or cast boot. Weight bearing is started while the patient is in the boot if the x-rays look appropriate after 6 to 8 weeks. The amount of weight a patient can put on their foot, as well as the distance the patient is allowed to walk, is at the surgeon’s discretion.
If the patient has had internal fixation (not a fusion), impact activities, such as running and jumping, should be avoided until the hardware has been removed.
Lisfranc injuries recovery
Some athletes never return to their pre-injury levels of sport after these injuries. Despite excellent surgical reduction and fixation, arthritis may occur from the damage to the cartilage. This may result in chronic pain and may require fusion in the future.
Posterior Tibial Tendon Dysfunction
Damage to the posterior tibial tendon (tibialis posterior tendon) is the most common cause of adult acquired flatfoot.
The posterior tibial tendon is one of the most important tendons of the leg. It starts at a muscle in the calf, travels down the inside of the lower leg and attaches to the bones on the inside of the foot.
Women and people over 40 are more likely to develop problems with the posterior tibial (tibialis posterior) tendon. Other risk factors include obesity, diabetes, and hypertension. Having flat feet since childhood increases the risk of developing a tear in the posterior tibial tendon. In addition, people who are involved in high impact sports, such as basketball, tennis, or soccer, may have tears of the tendon from repetitive use.
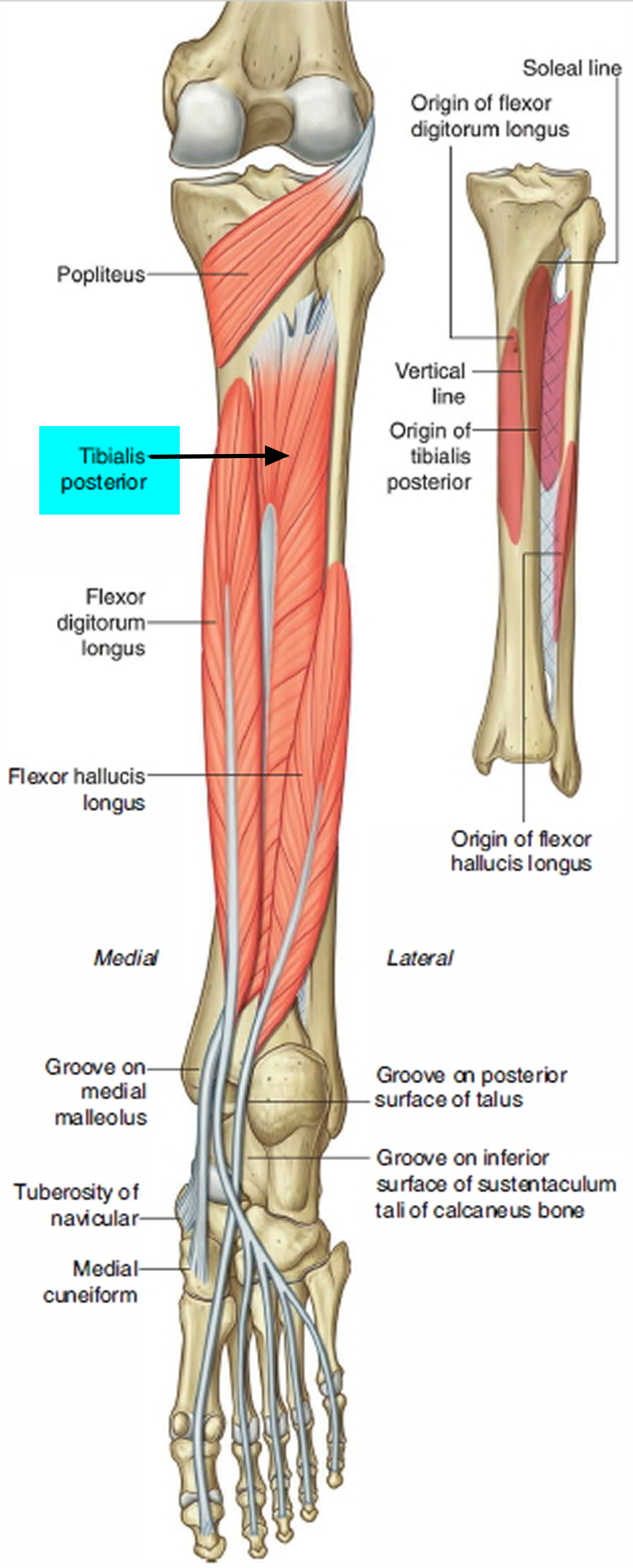
Tibialis posterior muscle and tendon
- Origin: Proximal tibia, fibula, and interosseous membrane.
- Insertion: Metatarsals II–IV; navicular; and all three cuneiforms.
- Action: Plantar flexes foot at ankle joint and inverts (supinates) foot at intertarsal joints. The main function of the tibialis posterior tendon is to hold up the medial arch of foot and support the foot when walking.
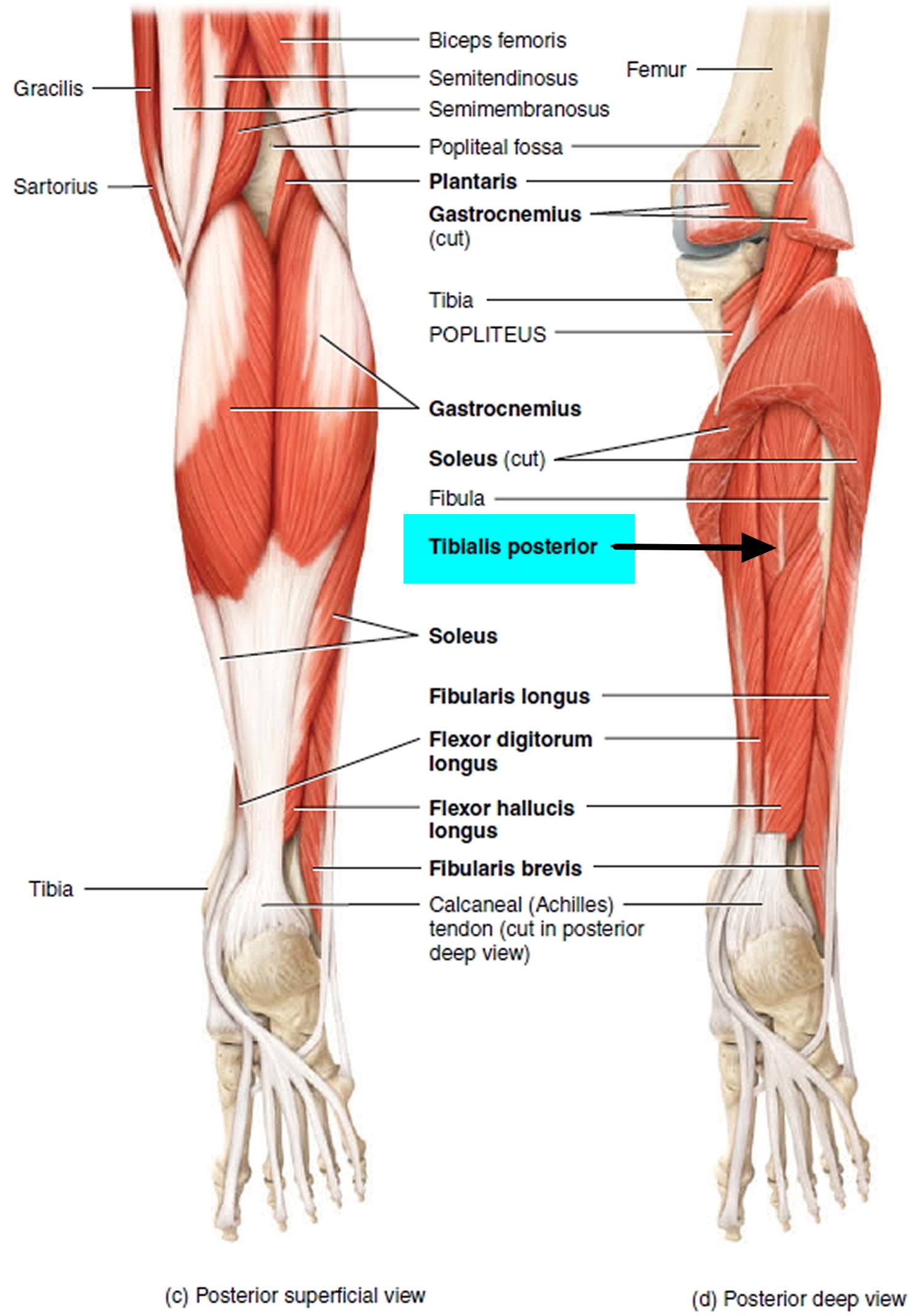
Figure 6. Tibialis posterior muscle and tendon
 Posterior Tibial Tendon DysfunctionPosterior tibial tendon dysfunction is one of the most common problems of the foot and ankle. It occurs when the posterior tibial tendon becomes inflamed or torn. As a result, the tendon may not be able to provide stability and support for the arch of the foot, resulting in flatfoot.Most patients can be treated without surgery, using orthotics and braces. If orthotics and braces do not provide relief, surgery can be an effective way to help with the pain. Surgery might be as simple as removing the inflamed tissue or repairing a simple tear. However, more often than not, surgery is very involved, and many patients will notice some limitation in activity after surgery.
Posterior Tibial Tendon DysfunctionPosterior tibial tendon dysfunction is one of the most common problems of the foot and ankle. It occurs when the posterior tibial tendon becomes inflamed or torn. As a result, the tendon may not be able to provide stability and support for the arch of the foot, resulting in flatfoot.Most patients can be treated without surgery, using orthotics and braces. If orthotics and braces do not provide relief, surgery can be an effective way to help with the pain. Surgery might be as simple as removing the inflamed tissue or repairing a simple tear. However, more often than not, surgery is very involved, and many patients will notice some limitation in activity after surgery.Posterior tibial tendon dysfunction cause
An acute injury, such as from a fall, can tear the posterior tibial tendon or cause it to become inflamed. The tendon can also tear due to overuse. For example, people who do high-impact sports, such as basketball, tennis, or soccer, may have tears of the tendon from repetitive use. Once the tendon becomes inflamed or torn, the arch will slowly fall (collapse) over time.
Posterior tibial tendon dysfunction is more common in women and in people older than 40 years of age. Additional risk factors include obesity, diabetes, and hypertension.
Posterior tibial tendon dysfunction symptoms
- Pain along the inside of the foot and ankle, where the tendon lies. This may or may not be associated with swelling in the area.
- Pain that is worse with activity. High-intensity or high-impact activities, such as running, can be very difficult. Some patients can have trouble walking or standing for a long time.
- Pain on the outside of the ankle. When the foot collapses, the heel bone may shift to a new position outwards. This can put pressure on the outside ankle bone. The same type of pain is found in arthritis in the back of the foot.
Posterior tibial tendon dysfunction treatment
Nonsurgical Treatment
Symptoms will be relieved in most patients with appropriate nonsurgical treatment. Pain may last longer than 3 months even with early treatment. For patients who have had pain for many months, it is not uncommon for the pain to last another 6 months after treatment starts.
- Rest
Decreasing or even stopping activities that worsen the pain is the first step. Switching to low-impact exercise is helpful. Biking, elliptical machines, or swimming do not put a large impact load on the foot, and are generally tolerated by most patients.
- Ice
Apply cold packs on the most painful area of the posterior tibial tendon for 20 minutes at a time, 3 or 4 times a day to keep down swelling. Do not apply ice directly to the skin. Placing ice over the tendon immediately after completing an exercise helps to decrease the inflammation around the tendon.
- Nonsteroidal Anti-inflammatory Medication
Drugs, such as ibuprofen or naproxen, reduce pain and inflammation. Taking such medications about a half of an hour before an exercise activity helps to limit inflammation around the tendon. The thickening of the tendon that is present is degenerated tendon. It will not go away with medication. Talk with your primary care doctor if the medication is used for more than 1 month.
- Immobilization
A short leg cast or walking boot may be used for 6 to 8 weeks. This allows the tendon to rest and the swelling to go down. However, a cast causes the other muscles of the leg to atrophy (decrease in strength) and thus is only used if no other conservative treatment works.
- Orthotics
Most people can be helped with orthotics and braces. An orthotic is a shoe insert. It is the most common nonsurgical treatment for a flatfoot. An over-the-counter orthotic may be enough for patients with a mild change in the shape of the foot. A custom orthotic is required in patients who have moderate to severe changes in the shape of the foot. The custom orthotic is more costly, but it allows the doctor to better control the position the foot.
- Braces
A lace-up ankle brace may help mild to moderate flatfoot. The brace would support the joints of the back of the foot and take tension off of the tendon. A custom-molded leather brace is needed in severe flatfoot that is stiff or arthritic. The brace can help some patients avoid surgery.
- Physical Therapy
Physical therapy that strengthens the tendon can help patients with mild to moderate disease of the posterior tibial tendon.
- Steroid Injection
Cortisone is a very powerful anti-inflammatory medicine that your doctor may consider injecting around the tendon. A cortisone injection into the posterior tibial tendon is not normally done. It carries a risk of tendon rupture. Discuss this risk with your doctor before getting an injection.
Surgical Treatment
Surgery should only be done if the pain does not get better after 6 months of appropriate treatment. The type of surgery depends on where tendonitis is located and how much the tendon is damaged. Surgical reconstruction can be extremely complex. The following is a list of the more commonly used operations. Additional procedures may also be required.
- Gastrocnemius Recession or Lengthening of the Achilles Tendon
This is a surgical lengthening of the calf muscles. It is useful in patients who have limited ability to move the ankle up. This surgery can help prevent flatfoot from returning, but does create some weakness with pushing off and climbing stairs. Complication rates are low but can include nerve damage and weakness. This surgery is typically performed together with other techniques for treating flatfoot.
- Tenosynovectomy (Cleaning the Tendon)
This surgery is used when there is very mild disease, the shape of the foot has not changed, and there is pain and swelling over the tendon. The surgeon will clean away and remove the inflamed tissue (synovium) surrounding the tendon. This can be performed alone or in addition to other procedures. The main risk of this surgery is that the tendon may continue to degenerate and the pain may return.
- Tendon Transfer
Tendon transfer can be done in flexible flatfoot to recreate the function of the damaged posterior tibial tendon. In this procedure, the diseased posterior tibial tendon is removed and replaced with another tendon from the foot, or, if the disease is not too significant in the posterior tibial tendon, the transferred tendon is attached to the preserved (not removed) posterior tibial tendon.
One of two possible tendons are commonly used to replace the posterior tibial tendon. One tendon helps the big toe point down and the other one helps the little toes move down. After the transfer, the toes will still be able to move and most patients will not notice a change in how they walk.
Although the transferred tendon can substitute for the posterior tibial tendon, the foot still is not normal. Some people may not be able to run or return to competitive sports after surgery. Patients who need tendon transfer surgery are typically not able to participate in many sports activities before surgery because of pain and tendon disease.
- Osteotomy (Cutting and Shifting Bones)
An osteotomy can change the shape of a flexible flatfoot to recreate a more “normal” arch shape. One or two bone cuts may be required, typically of the heel bone (calcaneus).
If flatfoot is severe, a bone graft may be needed. The bone graft will lengthen the outside of the foot. Other bones in the middle of the foot also may be involved. They may be cut or fused to help support the arch and prevent the flatfoot from returning. Screws or plates hold the bones in places while they heal.
- Fusion
Sometimes flatfoot is stiff or there is also arthritis in the back of the foot. In these cases, the foot will not be flexible enough to be treated successfully with bone cuts and tendon transfers. Fusion (arthrodesis) of a joint or joints in the back of the foot is used to realign the foot and make it more “normal” shaped and remove any arthritis. Fusion involves removing any remaining cartilage in the joint. Over time, this lets the body “glue” the joints together so that they become one large bone without a joint, which eliminates joint pain. Screws or plates hold the bones in places while they heal.
Side-to-side motion is lost after this operation. Patients who typically need this surgery do not have a lot of motion and will see an improvement in the way they walk. The pain they may experience on the outside of the ankle joint will be gone due to permanent realignment of the foot. The up and down motion of the ankle is not greatly affected. With any fusion, the body may fail to “glue” the bones together. This may require another operation.
Surgery Complications
The most common complication is that pain is not completely relieved. Nonunion (failure of the body to “glue” the bones together) can be a complication with both osteotomies and fusions. Wound infection is a possible complication, as well.
Surgical Outcome
Most patients have good results from surgery. The main factors that determine surgical outcome are the amount of motion possible before surgery and the severity of the flatfoot. The more severe the problem, the longer the recovery time and the less likely a patient will be able to return to sports. In many patients, it may be 12 months before there is any great improvement in pain.
Diabetic Collapse (Charcot Foot)
People with diabetes or with a nerve problem that limits normal feeling in the feet, can have arch collapse.
This type of arch collapse is typically more severe than that seen in patients with normal feeling in their feet. This is because patients do not feel pain as the arch collapses. In addition to the ligaments not holding the bones in place, the bones themselves can sometimes fracture and disintegrate – without the patient feeling any pain. This may result in a severely deformed foot that is very challenging to correct with surgery. Special shoes or braces are the best method for dealing with this problem.
Diabetes is a condition of elevated blood sugar that affects about 6 percent of the population in the United States, or about 16 million people. Diabetic foot problems are a major health concern and are a common cause of hospitalization.
Most foot problems that people with diabetes face arise from two serious complications of the disease:
- Nerve damage and
- Poor circulation.
Nerve damage (neuropathy) is a complication of diabetes that leads to a loss of sensation in the feet. Some people with diabetes can no longer feel when something has irritated or even punctured the skin. A wound as small as a blister can progress to a serious infection in a matter of days.
Diabetes also damages blood vessels, decreasing the blood flow to the feet. Poor circulation weakens bone, and can cause disintegration of the bones and joints in the foot and ankle. As a result, people with diabetes are at a high risk for breaking bones in the feet.
When a diabetic fractures a bone in the foot, he or she may not realize it because of nerve damage. Continuing to walk on the injured foot results in more severe fractures and joint dislocations. Sharp edges of broken bone within the foot can point downward toward the ground, increasing the risk of chronic foot sores from the abnormal pressure.
Figure 7. Diabetic Foot Collapse – Charcot Foot

The combination of bone disintegration and trauma can warp and deform the shape of the foot. This condition is called Charcot arthropathy, and is one of the most serious foot problems that diabetics face.
There are treatment options for the wide range of diabetic foot problems. The most effective treatment, however, is prevention. For people with diabetes, careful, daily inspection of the feet is essential to overall health and the prevention of damaging foot problems.
Charcot Foot Symptoms
Although a patient with Charcot arthropathy typically will not have much pain, they may have other symptoms.
- The most sensitive sign of early Charcot foot is swelling of the foot. This can occur without an obvious injury.
- Redness of the foot can also occur in the early stages.
- The swelling, redness, and changes to the bone that are seen on x-ray may be confused for a bone infection. A bone infection is very unlikely if the skin is intact and there is no ulcer present.
Charcot Foot Treatment
The goal of treatment for Charcot arthropathy is to heal the broken bones, as well as prevent further deformity and joint destruction.
Nonsurgical Treatment
Casting. The early stages of Charcot are usually treated with a cast or cast boot to protect the foot and ankle. The use of a cast is very effective in reducing the swelling and protecting the bones.
Casting requires that the patient not put weight on the foot until the bones begin to heal. Crutches, a knee-walker device, or a wheelchair are usually necessary. Healing can sometimes take 3 months or more. The cast will usually be changed every week or two to make sure that it continues to “fit” the leg as the swelling goes down.
Custom shoes. After the initial swelling has decreased and the bones begin to fuse back together, a specialized custom walking boot or diabetic shoe may be recommended. The specialized shoe is designed to decrease the risk of ulcers (sores that do not heal). Some diabetics may not be able to wear regular, over-the-counter shoes because they do not fit the deformed foot correctly.
Figure 8. Charcot Foot custom walking boot

Surgical Treatment
Surgery may be recommended if the foot deformity puts the patient at a high risk for ulcers, or if protective shoewear is not effective. Unstable fractures and dislocations also require surgery to heal.
- Mild deformity with tightness at the heel. In some cases, the deformity is mild and associated with tightness at the back of the heel. Ulcers in the front of the foot that do not respond to a period of casting and protective shoewear, may be treated through Achilles tendon lengthening. Surgically lengthening the tendon that runs down the back of the leg and attaches to the back of the heel decreases the pressure on the midfoot and front of the foot. This allows the ulcer to heal and reduces the chance that it will return.
- Bony prominence on the bottom of the foot. A more severe deformity is the appearance of a very large bony bump on the bottom of the foot. If this cannot be addressed with shoe modification, it requires surgery. The type of surgery depends on the stability of the bones and joints in the foot.
- Stable deformity. Surgery involves a simple removal of the prominent bone by shaving it off.
- Unstable deformity. When the bones are too loose at the sight of the prominence, a simple removal of the bump will not be effective. The loose bones will simply move and a new prominence will develop. In this situation, fusion and repositioning of the bones is needed.
Fractures that occur in the softer bone of diabetics are typically more complex. Operations to fix them generally involve more hardware (plates and screws) than would normally be required in people without diabetes. The screws and plates may even be placed across normal joints to provide added stability.
This operation is extremely difficult to perform and carries a higher risk of wound complications, infections, and amputation, compared to routine foot and ankle fracture surgery.
Figure 9. Charcot Foot surgery (for unstable deformity)

Note: (Top) In this x-ray taken from the side, the patient has unstable Charcot of the back of the foot (hindfoot). The dislocation of the joints is seen where the two bones in the back of the foot do not line up (arrowhead). (Bottom) A complex realignment and fusion was performed to prevent the patient from developing a prominence and ulceration.
After this type of operation, there is typically a period of no weight on the foot for at least 3 months. Placing weight on the foot early and failing to follow the doctor’s instructions will likely lead to complications, such as the return of the deformity or even worsening of the deformity.
Ankle deformity. Charcot of the ankle is difficult to treat simply with a brace or shoe and commonly requires surgical fusion of both the ankle and the joint below the ankle (subtalar) to hold the foot straight. Given the amount of destruction of the bone and the poor quality of the soft tissue, the risk that the bone will not heal and the risk of infection are very high. Amputation may be required, either as the first operation or to salvage a fusion that has not healed or has became infected.
To ensure the best outcome from treatment, it is essential that the patient follows doctor’s instructions regarding when it is safe to put weight on the injured foot. In addition, the sooner Charcot arthropathy is diagnosed and treated, the better the final outcome. Patients must carefully inspect both feet everyday and control their blood sugar levels. Both responsibilities are important in recognizing Charcot foot early, and in avoiding future complications.
Flexible Flat Feet in Children
A flat foot is normal in infants and toddlers, because the foot’s arch hasn’t yet developed. Most people’s arches develop throughout childhood, but some people never develop arches. This is a normal variation in foot type, and people without arches may or may not have problems.
Babies are often born with flat feet, which may persist well into their childhood. This occurs because children’s bones and joints are flexible, causing their feet to flatten when they stand. Young babies also have a fat pad on the inner border of their feet that hides the arch. You still can see the arch if you lift your baby up on the tips of the toes, but it disappears when he’s standing normally.
Some children have flexible flatfoot, in which the arch is visible when the child is sitting or standing on tiptoes, but disappears when the child stands. Although called “flexible flatfoot,” this condition always affects both feet.
A flexible flat feet is considered to be a variation of a normal foot. The muscles and joints of a flexible flatfoot function normally.
Most children are born with very little arch in the feet. As they grow and walk, the soft tissues along the bottom of the feet tighten, which gradually shapes the arches of the feet.
Children with flexible flatfeet often do not begin to develop an arch until the age of 5 years or older. Some children never develop an arch.
Normally, flat feet disappear by age six as the feet become less flexible and the arches develop. Only about 1 or 2 out of every 10 children will continue to have flat feet into adulthood. For children who do not develop an arch, treatment is not recommended unless the foot is stiff or painful. Shoe inserts won’t help your child develop an arch, and may cause more problems than the flat feet themselves.
If flexible flatfeet continues into adolescence, a child may experience aching pain along the bottom of the foot. A doctor should be consulted if a child’s flatfeet cause pain. For instance, a child may have tightness of the heel cord (Achilles tendon) that limits the motion of his foot. This tightness can result in a flat foot, but it usually can be treated with special stretching exercises to lengthen the heel cord. Rarely, a child will have truly rigid flat feet, a condition that can cause problems. These children have difficulty moving the foot up and down or side to side at the ankle. The rigid foot can cause pain and, if left untreated, can lead to arthritis. This rigid type of flat foot is seldom seen in an infant or very young child. (More often, rigid flat feet develop during the teen years and should be evaluated by your child’s pediatrician.)
Symptoms that should be checked by a pediatrician include foot pain, sores or pressure areas on the inner side of the foot, a stiff foot, limited side-to-side foot motion, or limited up-and-down ankle motion. For further treatment you should see a pediatric orthopedic surgeon or podiatrist experienced in childhood foot conditions.
Flexible Flat Feet in Children Treatment
Nonsurgical Treatment
Treatment for flexible flatfoot is required only if the child is experiencing discomfort from the condition.
Stretching exercises. If your child has activity-related pain or tiredness in the foot, ankle, or leg, your doctor may recommend stretching exercises for the heel cord.
- Heel Cord Stretch: Lean forward against a wall with one leg in front of the other. Straighten your back leg and press your heel into the floor. Your front knee is bent. Hold for 15 to 30 seconds. Keep both heels flat on the floor. Point the toes of your back foot toward the heel of your front foot.
Figure 10. Heel cord stretch

Shoe inserts. If discomfort continues, your doctor may recommend shoe inserts. Soft-, firm-, and hard-molded arch supports may relieve your child’s foot pain and fatigue. They can also extend the life of your child’s shoes, which may otherwise wear unevenly.
Additional treatment. Your doctor may prescribe physical therapy or casting if your child has flexible flatfoot with tight heel cords.
Surgical Treatment
Occasionally, surgical treatment will be necessary for an adolescent with persistent pain. In a small number of children, flexible flatfeet become rigid instead of correcting with growth. These cases may need further medical evaluation.
Flat feet symptoms
Most people have no signs or symptoms associated with flatfeet. But some adults with flatfeet experience foot pain, particularly in the heel or arch area. Pain may worsen with activity. Symptoms in adults may include tired or achy feet after long periods of standing or playing sports. Swelling along the inside of the ankle can also occur.
Children may have foot pain, ankle pain, or lower leg pain. They should be evaluated by a health care provider if this occurs.
Flat feet diagnosis
To view the mechanics of your feet, your doctor will observe your feet from the front and back and ask you to stand on your toes.
To diagnose the problem, the health care provider will ask you to stand on your toes. If an arch forms,the flat foot is called flexible. You will not need any more tests or treatment.
He or she might also look at the wear pattern on your shoes.
Imaging tests
If you’re having a lot of pain in your feet and if the arch does not form with toe-standing (called rigid flat feet), other tests may be needed, including:
- X-rays. A simple X-ray uses a small amount of radiation to produce images of the bones and joints in your feet. It’s particularly useful in detecting arthritis.
- CT scan. This test takes X-rays of your foot from different angles and provides much more detail than a standard X-ray.
- Ultrasound. If your doctor suspects an injured tendon, he or she may request this test, which uses sound waves to produce detailed images of soft tissues within the body.
- MRI. Using radio waves and a strong magnet, MRIs provide excellent detail of both hard and soft tissues.
Flat feet treatment
No treatment is necessary for flatfeet if they don’t cause pain.
Flat feet only need to be treated if you have an associated problem, such as pain, overpronation or an underlying health condition.
Non-surgical treatments are often recommended first, although surgery may be needed in some cases.
Flat feet in a child do not need treatment if they are not causing pain or walking problems.
- Your child’s feet will grow and develop the same, whether special shoes, shoe inserts, heel cups, or wedges are used.
- Your child may walk barefoot, run or jump, or do any other activity without making the flat feet worse.
In older children and adults, flexible flat feet that do not cause pain or walking problems do not need further treatment.
If you have pain due to flexible flat feet, the following may help:
- An arch-support (orthotic) that you put in your shoe. You can buy this at the store or have it custom-made.
- Special shoes
Rigid or painful flat feet need to be checked by a health care provider. The treatment depends on the cause of the flat feet.
For tarsal coalition, treatment starts with rest and possibly a cast. Surgery may be needed if pain does not improve.
In more severe cases, surgery may be needed to:
- Clean or repair the tendon
- Fuse joints in the foot into a corrected position
Flat feet in older adults can be treated with pain relievers, orthotics, and sometimes surgery.
Non-surgical treatments
Your doctor or podiatrist may recommend:
- wearing supportive shoes that fit well
- wearing specially made insoles (orthotics) inside your shoes to support your feet and stop them rolling inwards
- taking painkillers if you have any discomfort
- losing weight if you’re overweight
- stretching the muscles and connective tissues in your lower legs to help stop your foot rolling over
- you may be referred to a physiotherapist, who can recommend some exercises to try
These treatments won’t change the shape of the feet, but may help relieve some of the problems associated with flat feet.
- Arch supports (orthotic devices). Over-the-counter arch supports may help relieve the pain caused by flatfeet. Or your doctor might suggest custom-designed arch supports, which are molded to the contours of your feet. Arch supports won’t cure flatfeet, but they often reduce symptoms.
- Stretching exercises. Some people with flatfeet also have a shortened Achilles tendon. Exercises to stretch this tendon may help.
- Supportive shoes. A structurally supportive shoe might be more comfortable than sandals or shoes with minimal support.
- Physical therapy. Flatfeet may contribute to overuse injuries in some runners. A physical therapist can do a video analysis of how you run to help you improve your form and technique.
If these measures don’t help, you may be referred to an orthopedic surgeon to discuss whether surgery is an option.
Lifestyle and home remedies
If your flatfeet cause you minor pain, you might want to try:
- Rest. Avoid activities that aggravate your condition. Participate in low-impact activities — such as walking, biking or swimming — rather than jumping and running activities.
- Arch supports. Over-the-counter arch supports might increase your comfort.
- Medications. Over-the-counter pain relievers might help.
- Weight loss. Losing weight can reduce stress on your feet.
Flat feet surgery
Surgery is normally only considered if the treatments above haven’t helped or you have an underlying problem that can be corrected with an operation, such as abnormally developed bones in the feet or tendon tear or rupture.
The surgical procedure recommended for you will depend on the cause of your flat feet.
For example, bones that are abnormally shaped or joined together may need to be straightened or separated, while flat feet caused by a problem with your connective tissues may be treated by lengthening or repairing the affected tissues.
Your surgeon will talk to you about the operation you may need and what this involves.
Flat Feet Possible Complications
Possible problems after surgery include:
- Failure of the fused bones to heal
- Foot deformity that does not go away
- Infection
- Loss of ankle movement
- Pain that does not go away.





{kind=link}