
Contents
What is functional abdominal pain?
Functional abdominal pain also called centrally mediated abdominal pain syndrome (CAPS) or functional abdominal pain syndrome is pain occurring in your abdomen (belly) that cannot be fully explained by another medical condition and when no cause can be found after a thorough physical examination and appropriate investigations 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20.
Functional abdominal pain is belly pain that 6, 1:
- has been checked by a gastroenterologist (a specialist in gastrointestinal diseases) and does not have a clear cause
- happens at least 4 times per month
- has lasted for at least 2 months
- episodic or continuous abdominal pain that does not occur solely during physiologic events
- usually doesn’t last longer than 1 hour
- isn’t related to anything in particular (such as eating, activity, or bowel movements)
- happens in a child who is growing normally and has not lost weight
- can be triggered by stress or anxiety
In addition the main symptom of abdominal pain, children might have:
- nausea (feeling sick to the stomach)
- headache
- dizziness
- tiredness
Functional abdominal pain is one of the most common complaints of children and adolescents who are seen by gastroenterologists (specialists in gastrointestinal diseases) who care for young patients. Almost 25 percent of all children seen for stomach or intestinal complaints have functional abdominal pain 12.
Most young children will point to the belly button (umbilicus) when asked to describe the location of the abdominal pain. However, pain centered around the belly button could be due to a number of causes that should be considered when evaluating a child with chronic abdominal pain (abdominal pain that is present for more than 3 months either continuously or intermittently ). Some of those causes are not very serious while other causes require close and long term care. Possible causes that should be considered based on the history, physical examination and testing, are acid reflux, constipation, lactose intolerance, parasitic infections of the small and large intestines, infections of the stomach with a germ called Helicobacter pylori (that is associated with ulcers in the first portion of the small bowel), inflammatory bowel disease (IBD) such as Crohn’s disease and ulcerative colitis, celiac disease which is a sensitivity to cereal grains, food allergies, food sensitivity, inflammation of the liver (hepatitis), gall bladder problems, an inflamed pancreas (pancreatitis), an intestinal obstruction (blockage), appendicitis, and many more rare disorders. It must be emphasized that typically, none of these more severe problems cause abdominal pain in most children with chronic or recurrent bellyaches. Instead, the pain is usually “functional” 12.
Functional abdominal pain can be intermittent (recurrent abdominal pain) or continuous. Although the exact cause of functional abdominal pain is not known, nerve signals or chemicals secreted by the gut or brain, may cause the gut to be more sensitive to triggers that normally do not cause significant pain such as stretching or gas bloating 12. Because of this change in bowel function, this type of abdominal pain is often referred to as “functional abdominal pain.”
To diagnose functional abdominal pain, gastroenterologists:
- Ask about your child symptoms and make sure your child doesn’t have problems like weight loss, poor growth, fever, rash, vomiting, or arthritis.
- Do a physical exam.
- Do blood tests and tests for blood in the stool (poop).
- Ask about stressors such as recent changes at home or problems at school or work.
Many children undergo numerous diagnostic tests and sometimes painful procedures before the diagnosis functional abdominal pain is made. After appropriate evaluation, the abdominal pain cannot be fully explained by another medical condition 6, 1.
Doctors will only diagnose functional abdominal pain after excluding for other functional abdominal pain disorders in children and adolescents such as irritable bowel syndrome (IBS), functional dyspepsia, or abdominal migraine 21, 1.
Children with no serious symptoms and normal blood test and stool test results usually don’t need other tests.
The good new is that most children with functional abdominal pain get better within a few weeks to months with no lasting problems.
Doctors treat functional abdominal pain with some or all of the following:
- Diet changes such as avoiding foods that cause gas (like broccoli and cauliflower), fried foods, carbonated drinks (like soda), and spicy foods
- Medicines that help with cramping or lower the amount of acid in the stomach
- Pain medicine
- Cognitive-behavioral therapy (CBT) or relaxation techniques
Figure 1. Functional abdominal pain causes (The Microbiome-Gut-Brain Axis)
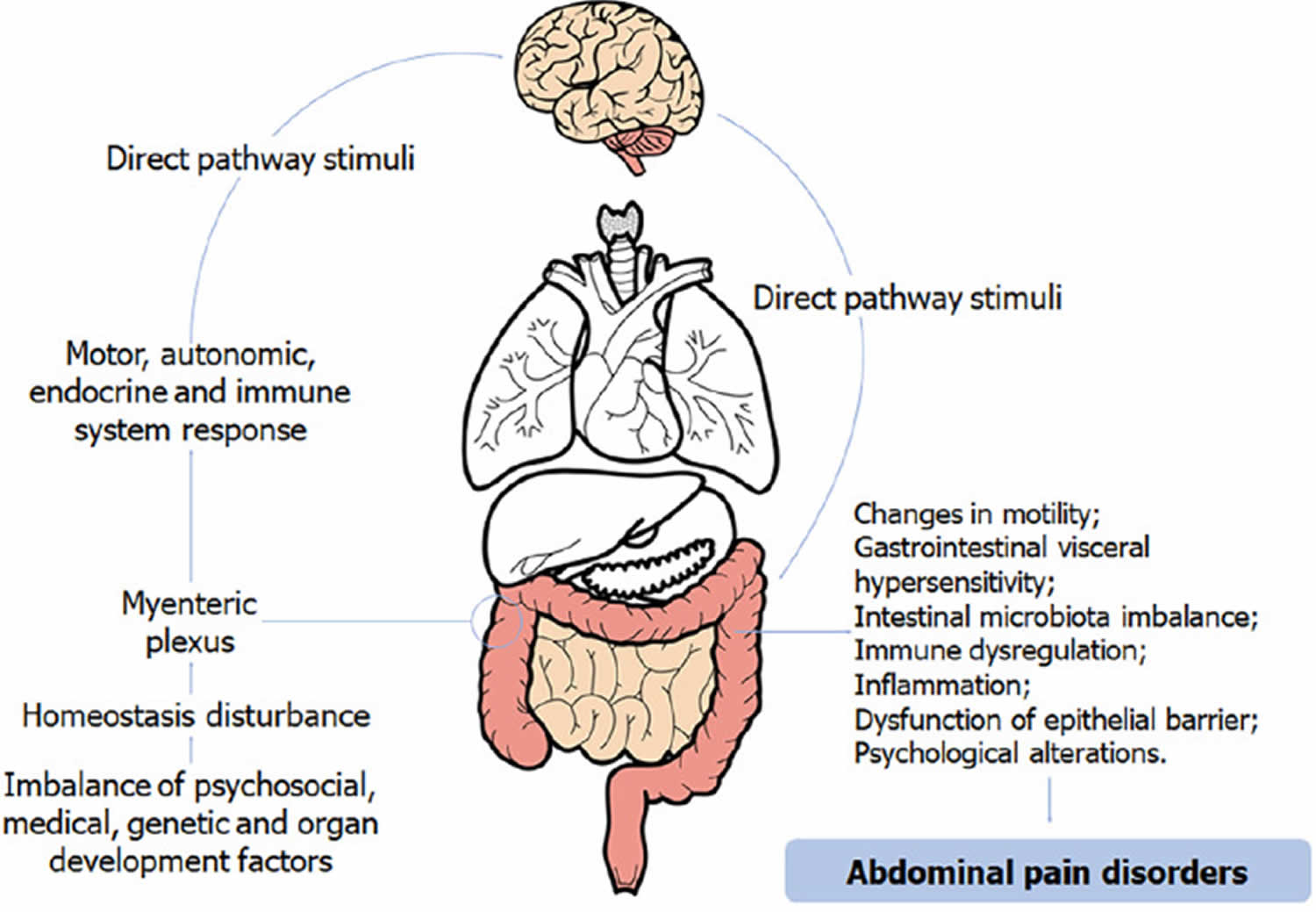
Footnote: Image of the Microbiome-Gut-Brain Axis in the pathogenesis of functional abdominal pain in children.
[Source 22 ]See a doctor if your child has functional abdominal pain and develops:
- blood in the poop
- diarrhea that lasts more than 2 days
- vomiting that lasts more than 2 days
- vomit with blood in it
- belly pain that lasts longer than 1 hour or gets worse
- a fever
- loss of appetite
- pain when peeing
- constipation
Also see a doctor if your child has:
- family history of inflammatory bowel disease (IBD), celiac disease, or peptic ulcer disease;
- persistent right upper or right lower quadrant pain;
- difficulty swallowing (dysphagia);
- painful swallowing (odynophagia);
- persistent vomiting;
- gastrointestinal blood loss;
- nighttime diarrhea;
- arthritis;
- perirectal disease;
- involuntary weight loss;
- deceleration of linear growth;
- delayed puberty and unexplained fever.
Functional abdominal pain causes
Doctors don’t know exactly what causes functional abdominal pain 23, 24. Functional abdominal pain may be related to nerve signals from the brain or gut that make someone more sensitive to pain 25, 26. Nerve signals or chemicals secreted by the gut or brain, may cause the gut to be more sensitive to triggers that normally do not cause significant pain such as stretching or gas bloating. The nerve signals may be set off by stretching of the stomach or rectum. Because of this change in bowel function, this type of abdominal pain is often referred to as “functional abdominal pain.”
Functional abdominal pain usually happens in children 4 to 16 years old. Sometimes, it happens after a gastrointestinal infection. It can be associated with a stressful event like a move or divorce.
Risk factors for functional abdominal pain
In some cases, children previously suffering from anxiety, depression and other psychiatric disorders may show an exaggerated pain response. Sometimes, the parent and the child may not be consciously aware of any stress or emotional disturbances. Other possible risk factors are thought to be physically or emotionally traumatic experiences, and preceding gastrointestinal infections. Parents and children need to be reassured that functional abdominal pain is not life threatening. However, functional abdominal pain may have negative effects on the child’s physical and psychological state. The pain may interfere with school attendance, participation in sports and other extra-curricular activities. Infrequently, it may affect appetite and sleep. The changes in the daily routine may affect the child’s mood and emotions, and in turn cause depression and anxiety.
Functional abdominal pain pathophysiology
The pathophysiology of functional abdominal pain disorders in children is not well understood. However, it has currently been observed that the microbiota-intestine-brain axis plays an important role in these diseases, as pathophysiological development seems to be linked to changes in its integrity and/or functionality 25. This neuroanatomical axis has an integrated and complex circuit that processes information about the emotional, sensory, and cognitive situation. The Microbiome-Gut-Brain Axis is represented graphically in Figure 1 above. There are direct connections from the central nervous system (brain and spinal cord) and the gastrointestinal tract with myenteric plexus act on the individual’s motor, autonomic, endocrine and immune system 26. The influence of this neuronal circuit has a direct reflex on the central nervous system (brain and spinal cord) and can trigger responses that result in changes in motility, gastrointestinal visceral hypersensitivity, intestinal microbiota, immune dysregulation, inflammation, and dysfunction of barriers 8. This is the most accepted hypothesis in the biopsychosocial model of functional abdominal pain disorders in children, and is linked to psychosocial, medical, genetic, and developmental factors of the organs and circuits involved in this axis. Disturbances on these systems and their homeostasis may result in some disorders.
A study with patients with irritable bowel syndrome (IBS) demonstrated that gastrointestinal motility problems are linked to delayed gastric emptying and increased intestinal transit 27. In another study conducted in Texas, USA, impaired myoelectric activity in the gastric environment was observed in patients with functional dyspepsia. The result of measuring myoelectric activity suggested a decrease in normal slow waves and an excessive amount of arrhythmic waves, resulting in impaired coordination of gastric slow waves 28. Riezzo et al 29 evaluated 52 children with non-ulcer dyspepsia and 114 healthy children, and changes in the electrical activity of the gastric environment and delayed gastric emptying were also observed. In addition, serotonin receptors and transporters may play an important role in this integrated response relationship of the gut-brain axis 30. Further studies on this topic are needed, since there are still few publications on the contribution of altered gastric motility in children with these functional disorders, and most of these are with adult patients.
Gastrointestinal visceral hypersensitivity is the most widespread and accepted mechanism of abdominal pain in the literature 31. The perceptual response of hyperalgesia is characterized by changes in the signal processing of the primary neurons afferent from the enteric nervous system to the central nervous system (brain and spinal cord), which interprets this stimulus as abdominal pain and triggers a series of reflexes that are recognized as pain 31, 32. Therefore, visceral sensitivity is also regulated at various levels of the microbiota-intestine-brain axis, such as the enteric mucosa and submucosa, medulla, thalamus, and cerebral cortex 32, which demonstrates an integrated sensory response throughout this axis. In a study of 51 children, a decrease in sensory threshold was observed in patients with functional gastrointestinal disorders (FGIDs) when compared to children with organic diseases 33, which indicates that this decreased sensory threshold associated with changes in neuronal stimuli is possibly the explanation of visceral hypersensitivity in functional gastrointestinal disorders (FGIDs).
Evidence shows that the microbiota of patients with functional gastrointestinal disorders differs from healthy people 34. In a recent systematic review with patients with irritable bowel syndrome (IBS), with three studies included with children, a significant increase in the bacterial population of the family Enterobacteriaceae and Lactobacillaceae and genus Bacteroides in patients with irritable bowel syndrome (IBS) when compared with the control group was observed. In addition, there was a decrease in bacterial colonization of Bifidobacterium spp., Faecalibacterium spp., and Faecalibacterium prausnitzii 35, which plays an important role in the balance of the immune system in the intestine 36. However, the role of the microbiota in relation to functional diseases in children is not well established. Most studies evaluated fecal samples from adult patients with irritable bowel syndrome (IBS) and have limitations in relation to sample collection, and diet and medication used by the patient. More studies would be important in order to understand the influence that the way of delivery, metabolome and other microorganisms have on the intestinal microbiota of these children.
Homeostasis of the microbiota-intestine-brain axis is essential to maintain the integrity of the immune system, and disturbances in this balance can generate uncontrolled inflammation in the gastrointestinal mucosa. Interestingly, infiltration of mast cells, eosinophils, and lymphocytes has been observed in intestinal environment of patients with functional disorders. In particular, mast cell recruitment is involved in epithelial and neuromuscular dysfunction 37. These inflammatory cells are close to neurosensorial fibers of the gastrointestinal tract mucosa and have a relevant role in altering neurogenic inflammatory pathways and in perception of pain in response to harmful stimuli 38. In addition, the degree of inflammation in the gastrointestinal tract mucosa can cause injuries and, consequently, a rupture of barriers that restrict bacterial colonization under normal conditions. As a result, bacterial overgrowth can be observed, which can culminate in functional gastrointestinal disorders (FGIDs) 32, 39.
High self-perceived prevalence of food intolerances has been reported in children with IBS 40. These symptoms are associated with nutritional behavioral changes and children’s diet 41; however, the knowledge about how nutritional factors influence functional gastrointestinal diseases is still unclear. Therefore, greater knowledge about a possible adequate nutritional pattern for maintaining the balance of the microbiota-intestine-brain axis may be ideal for a better understanding of the relationship between food and the intestinal microbiota in that axis.
The psychological factors and their relationship to intestinal motility are well understood. Some studies have already demonstrated the physiological effects on the gastrointestinal tract, triggered by anger, fear, and anxiety 32. In a recent review, the authors concluded that although it is still unclear whether functional gastrointestinal disorders (FGIDs) may have psychological factors as their etiology, there is strong evidence that these factors exacerbate and contribute to maintenance of pain 42. An interesting correlational study found a decrease in the symptoms of functional disorders in children in summer, when compared to spring 43. The authors correlated this improvement to the vacation period when they are exposed to fewer stressors, but were unable to distinguish what is the cause and what is the effect of decreasing symptoms 43. Also, the hypothalamus-pituitary-adrenal axis may have an interaction with the microbiota-intestine-brain axis, releasing cortisol and corticotropin, which stimulate metabolic stress and cause a release of mast cells and pro-inflammatory cytokines 25. Stress factors can also deregulate the balance of the intestinal microbiota, increasing the permeability of epithelial tissue, and facilitating the entry of pathogens that can create an inflammatory environment. In addition, the release of cytokines such as IFNγ, IL-1, and IL-6 can stimulate an immune response in the central nervous system (brain and spinal cord) and reflect an exacerbation of psychological symptoms 44. With this, it becomes increasingly important that children with symptoms related to functional gastrointestinal disorders (FGIDs) receive the integration of the psychological examination in their care 45.
Functional abdominal pain symptoms
Functional abdominal pain is belly pain that:
- has been checked by a gastroenterologist (a specialist in gastrointestinal diseases) and does not have a clear cause
- happens 4 times a month or more
- has lasted for at least 2 months
- usually doesn’t last longer than 1 hour
- isn’t related to anything in particular (such as eating, activity, or bowel movements)
- happens in a child who is growing normally and has not lost weight
- can be triggered by stress or anxiety
In addition the main symptom of abdominal pain, children might have:
- nausea (feeling sick to the stomach)
- headache
- dizziness
- tiredness
Usually, the functional abdominal pain is located around the umbilicus (belly button), however the pattern or location of abdominal pain is not always predictable. The pain may occur suddenly or slowly increase in severity. The pain may be constant or may increase and decrease in severity.
Some children with functional abdominal pain may experience indigestion (dyspepsia described as burning sensation, stomach ache, bloating or a feeling of fullness during and after meals), or upper abdominal pain associated with nausea, vomiting, and/or a feeling of fullness after just a few bites (early satiety). Others may experience abdominal pain with bowel movements. Pain that is usually relieved by bowel movements, or associated with changes in bowel movement habits (mainly constipation, diarrhea, or constipation alternating with diarrhea) is the classic irritable bowel syndrome (IBS).
Functional abdominal pain complications
As functional abdominal pain does not have an underlying organic pathology, complications based on the disease process itself are not expected. Complications may arise due to the impact of chronic pain on social functioning and school performance or may be related to comorbid depression and anxiety compounded by the persistence of symptoms 10. A supportive and understanding environment at home and school is important to keep the child physically and mentally healthy.
Functional abdominal pain diagnosis
A gastroenterologist will diagnose functional abdominal pain based on a careful history, a physical exam, and the pattern of your symptoms. There are no abnormal x-rays or laboratory findings to explain the pain.
The diagnosis of abdominal pain has five components depending on your age. The five components include medical history, a physical examination, laboratory testing, results of imaging studies and response to empiric therapy:
- Medical History. To diagnose abdominal pain, doctors and healthcare professionals are likely to ask you the following questions:
- Location, intensity, character and duration of the pain, time of day or night that pain occurs
- Appetite, diet, satiety, nausea, reflux, vomiting
- Stool pattern, consistency, completeness of evacuation
- Review of systems: weight loss, growth or pubertal delay, fever, rash
- Medications and nutritional interventions
- Family history,
- Travel history,
- Interference with school, work, play, peer relations and family dynamics
- Physical examination
- Weight, height, growth velocity, pubertal stage, blood pressure
- Complete physical examination
- Objective abdominal findings: location, rebound, mass, psoas sign
- Liver, spleen and renal size, ascites, flank pain
- A rectal exam to check for hidden blood or other problems
- A check of the penis and scrotum
- A pelvic exam to check for problems in the womb (uterus), fallopian tubes and ovaries, and a pregnancy test
- Stool testing for occult blood
- Laboratory tests. If tests are needed, these may include:
- Complete blood count with differential, erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP)
- Urinalysis and urine culture to look for a urine infection or blood (if there is a kidney stone)
- Laboratory tests individualized according to indication
- Stool testing and culture for polymorphonuclear leukocytes, parasites, Giardia antigen
- Serum chemistry profile, serum amylase and serum lipase level
- Pregnancy test, cultures for sexually transmitted diseases
- Breath hydrogen test: lactose, fructose
- Serologic testing for amebae, Helicobacter pylori
- An ECG (an electrical tracing of the heart) to rule out a heart attack
- Imaging studies individualized according to indication
- Abdominal and pelvic sonography
- Upper gastrointestinal contrast study with small bowel testing, abdominal computed tomography
- Upper endoscopy – an examination where a flexible tube with a light and video camera at the tip is used to examine some internal organs without the need for surgery. Different names are used depending on which organ is being looked at for examples, small-bowel capsule endoscopy, video capsule endoscopy, colonoscopy and laparoscopy
- Empiric interventions
- Patient and parent education
- Symptom diary of pain, bowel pattern, diet and associated features, response to intervention
- Constipation investigated as a factor
- Dietary interventions, including adjusted fiber intake, reduced lactose intake, reduced juice intake
- Trial of peptic management.
The diagnosis of functional abdominal pain is often based on the report of your symptoms and normal physical examination. It is also quite possible that your doctor may do some tests. The reason for these tests is to look for signs of any serious disease. These screening tests may initially include blood and stool tests. The results of screening tests often guide your doctor in deciding whether further tests are needed or whether a trial of diet changes, stress management or medication may be started. Testing should be limited if the history is typical for functional abdominal pain and the child’s physical examination is normal. In that case, many doctors prefer to treat without testing in order to avoid the discomfort of testing or the slight risk associated with testing. Of course, if the history, the physical examination, or the results of screening tests are abnormal, further testing may be required. This further testing may include a test to confirm lactose intolerance, ultrasound of the abdomen, a CT of the abdomen, and upper gastrointestinal series (radiology test), and possibly an endoscopy (scope). The scope allows the doctor to use a special camera on the scope to look at the inner lining of the food pipe, stomach, first and last portion of the small intestine and the large intestine. At the time of the endoscopy, biopsies (small pinches of the lining) are also obtained and examined under the microscope for signs of certain infections and disorders like inflammatory bowel disease (IBD) and celiac disease. Normal test results in a child without alarm signs or red flags strongly suggest recurrent abdominal pain or one of the other types of functional abdominal pain, such as irritable bowel syndrome (IBS) or functional dyspepsia (also called nonulcer dyspepsia is a term for recurring symptoms of an upset stomach that have no obvious cause).
Functional abdominal pain diagnostic criteria
The ROME IV (4) criteria were developed to avoid unnecessary diagnostic tests and help facilitate the diagnosis of functional abdominal pain 1. Functional abdominal pain is one of several categories of gastrointestinal disorders classified by the Rome IV criteria, with the other categories including functional nausea and vomiting or functional defecation disorders 1.
The Rome IV criteria, published in 2016, allow for clinical diagnosis of functional abdominal pain and related functional conditions (irritable bowel syndrome, functional dyspepsia, abdominal migraine). As a change from the prior Rome III criteria, functional abdominal pain can be diagnosed based on symptoms “after appropriate medical evaluation the symptoms cannot be attributed to another medical condition” rather than the previous criteria’s requirement that there “is no evidence for organic disease” 1.
The diagnostic Rome IV criteria for functional abdominal pain must be fulfilled for at least 2 months before diagnosis, must be met at least 4 times per month, and include all of the following 1:
- Episodic or continuous abdominal pain that does not occur solely during physiological events such as eating and menses
- Insufficient criteria for other functional gastrointestinal disorders including irritable bowel syndrome, functional dyspepsia, or abdominal migraine
- After appropriate evaluation, the abdominal pain cannot be fully explained by another medical condition.
Functional abdominal pain treatment
Functional abdominal pain (centrally mediated abdominal pain syndrome) can be a challenging condition to manage. It is important that you work with a gastroenterologist who demonstrates empathy toward you and an understanding of the symptoms of functional abdominal pain. Functional abdominal pain syndrome or centrally mediated abdominal pain syndrome is a disorder where treatment requires the participation of both you and your doctor. Treatments for functional abdominal pain are most effective when the patient and the doctor work as a team, each having a role. Your doctor has the responsibility to educate you about functional abdominal pain. He or she should answer your questions and provide you with an understanding of what your symptoms are about and what your treatment options are.
You need to express your views about your treatment goals, work with your doctor to develop the treatment plan, and work toward putting the plan into action. If you follow the treatment plan closely, you and your doctor will be better able to track your results. This will allow you to achieve the best possible relief of abdominal pain.
Functional abdominal pain treatment is to help you gain control over your symptoms and improve daily function. It usually is not possible to totally eliminate your symptoms. Because the brain has such a strong influence on the sensation of pain, psychological treatments can relieve symptoms of functional abdominal pain (centrally mediated abdominal pain syndrome) by sending signals that close the gate. Therapeutic interventions such as relaxation techniques, guided imagery, hypnotherapy, and cognitive-behavioral therapy (CBT) can be effective in alleviating pain by facilitating the transmission of signals that help to reduce pain sensations. These interventions teach individuals how to modify their own pain perception and provide relief from discomfort.
- Stress management (i.e., relaxation techniques, meditation, yoga): Teaches you how to focus attention on something other than the pain. Yoga has been shown to be an exercise that provides several benefits for children, including improvements in the emotional control, anxiety, and depression 46, 47. A study carried out by Brands et al 48 evaluated Yoga practice in 20 children (age range: 8-18 years) with inflammatory bowel syndrome or abdominal pain. The children participated in 10 Yoga sessions, lasting 1.5 hour each, being observed that the exercises reduced the severity and frequency of abdominal pain immediately after the classes. Moreover, after 3 months of continued exercises at home, the children continued to report improvements; however, the status of the preexisting conditions was not modified 48. A recent study enrolling adolescents aged from 14 to 17 years with inflammatory bowel disease demonstrated that the use of Yoga for 6 week resulted in an improvement of abdominal pain, sleep, and visceral hypersensitivity among responding participants 49. A study by Evans et al 50 showed that an intervention with Yoga as a complementary treatment benefits young adults with inflammatory bowel disease with a reduction of symptoms. In addition, the findings of this systematic review suggest that yoga might be a feasible and safe adjunctive treatment for people with irritable bowel syndrome (IBS) 51.
- Exercise: Boradyn et al 52 carried out a study including 25 children aged from 5 to 11 years to evaluate the impact of exercise (physical activity) in children diagnosed with functional abdominal pain. The results showed that the practice of physical activities might increase stool frequency among children; however, the data regarding the relationship between exercises and abdominal pain were not statistically significant 52. A recent study observed an association between the practice of physical activities and the development of constipation among children and identified that children who often exercises had a lower odds of acquiring the disorder than sedentary individuals 53. A study that evaluated the effectiveness of alternative complementary medicine for functional abdominal pain observed that 49% of the patients enrolled used to practice exercises to improve their symptoms. Moreover, individuals who rated their condition as severe tend to practice exercises more often than those who rate their disorders as mild or moderate 54. Kichline et al 55 recently observed that children with chronic abdominal pain did not do physical activities 60 min per day. In addition, another study evaluated socioeconomic factors involved in the probability of occurrence of gastrointestinal disorders related to abdominal pain and concluded that the low practice of exercises is positively associated with the disorder 56.
- Acupuncture: Acupuncture is an ancient medical procedure that has been practiced in China and other East Asian countries. The technique involves the placement of small needles at various locations in the body and related therapies include electroacupuncture, acupressure, moxibustion (i.e., burning of an herb near an acupoint to create local warming), laser stimulation of acupoints, and non-invasive stimulation of acupoints utilizing a transcutaneous electrical nerve stimulator 57. A systematic review of randomized controlled trials on the use of acupuncture in infantile colic shows that acupuncture appears to be effective in alleviating the symptoms of colic, including crying and feeding and stooling problems 58. However, due to the small sample sizes of the included studies, more randomized clinical trials are necessary 58. Another case series study found that minimal acupuncture in infantile colic is an effective and easy treatment procedure 59.
- Therapeutic massage. Therapeutic massage has been associated with a significant improvement among children with chronic pain due to several diseases, including abdominal disturbances 60, 61, 62, 63, 64. In a recently published study, Al Qahtani and Ahmed 65 recommended the development of educational programs aiming to teach abdominal massage and feet reflexology techniques for parents, since it is an effective way to improve abdominal colic in babies.
- Hypnosis (hypnotherapy): Helps you focus attention away from the pain. Positive suggestion can change ways you think or react.
- Cognitive-behavioral therapy (CBT): Teaches you how to change non-helpful thoughts, perceptions, and behaviors to control symptoms. Cognitive-behavioral therapy (CBT) involves the teaching of coping and distraction strategies and relaxation techniques; identification and change of pain-related thoughts; and modification of family responses to pain. This method can involve the family itself or may focus only on the child, as well as be performed face-to-face or remotely 66, 67. Family approach seeks to alter environmental factors that might reinforce the child’s pain behavior within the family and to identify and treat factors that may precipitate in it 67. Multiple components are typically used in CBT, such as education about the pain, increasing self-confidence[60], cognitive restructuring of maladaptive thoughts, exposure exercises, relaxation, and parent management techniques 68. In exposure-based CBT for functional abdominal pain syndrome, the patients gradually expose themselves to symptom-provoking stimuli (such as eating pizza) and approach situations in which symptoms are perceived as intolerable (such as being in school). This approach is hypothesized to decrease fear and avoidance related to symptoms and thereby enables symptom reduction 69.
- Spinal manipulation (chiropractic care): The relationship between spinal manipulation and improvement of symptoms related to abdominal disorders is controversial. Some studies have indicated that the therapy may be associated with an improvement of abdominal pain among children 70, 71. On the other hand, a systematic review of clinical trials was not able to conclude that the spinal manipulation is an effective therapeutic practice against infant colic, and the author stated that the low quality of the studies contributes to the lack of consistent recommendations on that issue 72.
A fearful, anxious, or depressed child however should be fully assessed by a psychiatrist or psychologist. Some psychological treatments that help children cope with functional abdominal pain and other stressors, include cognitive-behavioral therapy (CBT), relaxation exercises and hypnosis. It is very important that the physician, parents, and school encourage the child resume a normal routine.
Functional abdominal pain diet
Your child may benefit from certain dietary changes depending on his/her history. These are recommended on a case-by-case basis. Your child’s doctor may advise avoidance of greasy and spicy foods, caffeine, juices, and carbonated drinks. Eliminating lactose (a natural sugar in milk and other dairy products) from the diet may benefit those who suffer from lactose intolerance in addition to functional abdominal pain. Some children with abdominal pain who also experience “gas” may improve by eating food slowly and by avoiding carbonated drinks, and gas forming foods such as cabbage, or beans. In addition, fruit drinks, sugar-free chewing gum, and sugar free candy sweetened with an alcohol called sorbitol should be avoided. Sorbitol, which tastes sweet, cannot be properly digested, and when taken in large amounts, it can cause cramping, bloating, and even diarrhea.
In patients who report bloating, dietary measures may be effective such as utilizing a low-fermentable oligosaccharides, disaccharides, monosaccharides, and polyols (FODMAPs) diet to exclude foods with certain classes of carbohydrates including wheat, various fruits, lactose, fructose, and some artificial sweeteners.
Boradyn et al 52 carried out a study including 25 children aged from 5 to 11 years to evaluate the impact of insufficient intake of fiber, showed children with lower fiber intake had higher abdominal pain intensity than children with adequate fiber intake.
Functional abdominal pain medication
The published literature on treatments for functional abdominal pain is still scarce, and the effectiveness of pharmacological therapy lacks studies that provide quality scientific evidence 70. Although there are a large number of studies indicating medication effectiveness in relation to placebo, most studies that analyze pharmacological intervention have a small sample size, are uncontrolled or non-randomized, and even present controversial or incomplete results. In addition, most studies have methodological flaws that prevent authors from drawing significant conclusions about effectiveness 73, 74, 75, 76. Therefore, the current functional abdominal pain guidelines and studies recommend that the initial approach to children with functional abdominal pain disorders should be managed without the use of medication and only use medication if functional abdominal pain is significantly limiting the daily routine, while observing for possible side effects 77. Potential medications for functional abdominal pain disorders (FAPDs) have been identified based on the gut-brain axis, mainly including antispasmodics, antidepressants, secretagogues, antihistamines, anti-reflux agents, calcium channel blockers, serotonin antagonists, laxatives, antibiotics, and hormone therapy 78.
Some children may be candidates for medications, if functional abdominal pain is significantly limiting the daily routine. These medications include anti-spasmodic medicines (drugs that reduce intestinal contraction e.g., hyoscyamine or dicyclomine) for those with crampy pain in relation to bowel movements, laxatives for those with constipation, and acid-suppressing medicines for those with pain and indigestion (dyspepsia). If the child does not respond to any of these treatments, he or she may benefit from low doses of medicines called antidepressants (medications used to treat depression). Specifically, your doctor may suggest a low dose antidepressant for continuous or severe abdominal pain. It’s important to keep in mind that these medications are not solely for the treatment of depression. An antidepressant can act as pain relievers (central analgesics) at lower doses than those typically used for depression or for the treatment of other painful conditions. Antidepressant medications can help stimulate the brain in such a way that it increases the signals that block pain messages from the abdomen to the brain. It may take several weeks before a difference is noticed. It’s important to be patient as it may take several weeks before you start to notice any difference in your symptoms. However, with the right medication and treatment plan in place, it is possible to manage functional abdominal pain (centrally mediated abdominal pain syndrome) and improve your overall quality of life.
Some people will experience side effects from antidepressant medications. Usually, the side effects will go away after a few days so it is important to stay with the medication until treatment benefit is obtained. The tricyclic antidepressants (TCAs) can cause dry mouth and drowsiness. Another group of antidepressants is called selective serotonin-norepinephrine reuptake inhibitors (SNRIs). These can cause side effects like nausea. Both of these classes of antidepressants are helpful for treating pain.
Lastly, it is becoming increasingly common to use combinations of treatments like a medication for the bowel and an antidepressant or two types of medications to affect the brain’s pain control or a behavioral treatment like cognitive behavioral therapy (CBT) with an antidepressant. These combinations can improve the pain benefit while keeping side effects at a minimum.
It is important to realize that Opioids are not indicated and can even be harmful and need to be avoided in treating chronic abdominal pain. Over long periods of time, Opioids may produce more pain causing a condition called “Opioid Induced Constipation” or “Narcotic Bowel Syndrome”.
Functional abdominal pain prognosis
Functional abdominal pain has a good prognosis and a chronic course with almost half of these children getting better on their own or with treatment within a few weeks to months 10. Though there is a lack of underlying organic pathology, continued abdominal pain can impact school performance and social relationships, causing distress and disability. A supportive and understanding environment at home and school is important to keep the child physically and mentally healthy.
Longitudinal studies suggest many children have persistent abdominal pain years after original diagnosis. Historical studies indicate that adults with irritable bowel syndrome (IBS) are more likely to have had symptoms consistent with a functional gastrointestinal disorder as a child. Research suggests that comorbid features such as anxiety or depression or extraintestinal features such as headaches are a more significant determinant of long-term prognosis than the diagnosis alone 21, 79.
- Hyams JS, Di Lorenzo C, Saps M, Shulman RJ, Staiano A, van Tilburg M. Functional Disorders: Children and Adolescents. Gastroenterology. 2016 Feb 15:S0016-5085(16)00181-5. doi: 10.1053/j.gastro.2016.02.015[↩][↩][↩][↩][↩][↩][↩][↩]
- Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, Spiller RC. Functional bowel disorders. Gastroenterology. 2006 Apr;130(5):1480-91. doi: 10.1053/j.gastro.2005.11.061. Erratum in: Gastroenterology. 2006 Aug;131(2):688.[↩]
- Matthews PJ, Aziz Q. Functional abdominal pain. Postgrad Med J. 2005 Jul;81(957):448-55. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1743310/pdf/v081p00448.pdf[↩]
- Thompson WG, Longstreth GF, Drossman DA, Heaton KW, Irvine EJ, Müller-Lissner SA. Functional bowel disorders and functional abdominal pain. Gut. 1999 Sep;45 Suppl 2(Suppl 2):II43-7. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1766683/pdf/v045p0II43.pdf[↩]
- Farmer AD, Aziz Q. Mechanisms and management of functional abdominal pain. J R Soc Med. 2014 Sep;107(9):347-54. doi: 10.1177/0141076814540880[↩]
- Rasquin A, Di Lorenzo C, Forbes D, Guiraldes E, Hyams JS, Staiano A, Walker LS. Childhood functional gastrointestinal disorders: child/adolescent. Gastroenterology. 2006 Apr;130(5):1527-37. doi: 10.1053/j.gastro.2005.08.063[↩][↩][↩]
- Schmulson M, Drossman D. Rome IV Functional Gastrointestinal Disorders: Disorders of gut-brain interaction. 4 edition. Rome Foundation, Inc, May 2017.[↩]
- Drossman DA. Functional Gastrointestinal Disorders: History, Pathophysiology, Clinical Features and Rome IV. Gastroenterology. 2016 Feb 19:S0016-5085(16)00223-7. doi: 10.1053/j.gastro.2016.02.032[↩][↩]
- Drossman DA. The functional gastrointestinal disorders and the Rome III process. Gastroenterology. 2006 Apr;130(5):1377-90. doi: 10.1053/j.gastro.2006.03.008[↩]
- McClellan N, Ahlawat R. Functional Abdominal Pain in Children. [Updated 2023 Jun 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537298[↩][↩][↩]
- Wallace C, Gordon M, Sinopoulou V, Akobeng AK. Probiotics for management of functional abdominal pain disorders in children. Cochrane Database Syst Rev. 2023 Feb 17;2(2):CD012849. doi: 10.1002/14651858.CD012849.pub2[↩]
- Functional Abdominal Pain in Children. https://gi.org/topics/functional-abdominal-pain-in-children[↩][↩][↩][↩]
- Clouse RE, Mayer EA, Aziz Q, Drossman DA, Dumitrascu DL, Mönnikes H, Naliboff BD. Functional abdominal pain syndrome. Gastroenterology. 2006 Apr;130(5):1492-7. doi: 10.1053/j.gastro.2005.11.062[↩]
- Banez GA. Chronic abdominal pain in children: what to do following the medical evaluation. Curr Opin Pediatr. 2008 Oct;20(5):571-5. doi: 10.1097/MOP.0b013e32830c6ef1[↩]
- Grover M, Drossman DA. Functional abdominal pain. Curr Gastroenterol Rep. 2010 Oct;12(5):391-8. doi: 10.1007/s11894-010-0125-0[↩]
- Posovszky C, Roesler V, Becker S, Iven E, Hudert C, Ebinger F, Calvano C, Warschburger P. Roles of Lactose and Fructose Malabsorption and Dietary Outcomes in Children Presenting with Chronic Abdominal Pain. Nutrients. 2019 Dec 16;11(12):3063. doi: 10.3390/nu11123063[↩]
- Xue M, Chen X, Shi L, Si J, Wang L, Chen S. Small-bowel capsule endoscopy in patients with unexplained chronic abdominal pain: a systematic review. Gastrointest Endosc. 2015 Jan;81(1):186-93. https://doi.org/10.1016/j.gie.2014.04.062[↩]
- Kim W, Lee B, Yoo A, Kim S, Joo M, Park JJ. Predictors of Positive Video Capsule Endoscopy Findings for Chronic Unexplained Abdominal Pain: Single-Center Retrospective Study and Meta-Analysis. Diagnostics (Basel). 2021 Nov 16;11(11):2123. doi: 10.3390/diagnostics11112123[↩]
- Gijsbers CF, Benninga MA, Schweizer JJ, Kneepkens CM, Vergouwe Y, Büller HA. Validation of the Rome III criteria and alarm symptoms for recurrent abdominal pain in children. J Pediatr Gastroenterol Nutr. 2014 Jun;58(6):779-85. doi: 10.1097/MPG.0000000000000319[↩]
- Helgeland H, Flagstad G, Grøtta J, Vandvik PO, Kristensen H, Markestad T. Diagnosing pediatric functional abdominal pain in children (4-15 years old) according to the Rome III Criteria: results from a Norwegian prospective study. J Pediatr Gastroenterol Nutr. 2009 Sep;49(3):309-15. doi: 10.1097/MPG.0b013e31818de3ab[↩]
- Korterink J, Devanarayana NM, Rajindrajith S, Vlieger A, Benninga MA. Childhood functional abdominal pain: mechanisms and management. Nat Rev Gastroenterol Hepatol. 2015 Mar;12(3):159-71. doi: 10.1038/nrgastro.2015.21[↩][↩]
- Cordeiro Santos ML, da Silva Júnior RT, de Brito BB, França da Silva FA, Santos Marques H, Lima de Souza Gonçalves V, Costa Dos Santos T, Ladeia Cirne C, Silva NOE, Oliveira MV, de Melo FF. Non-pharmacological management of pediatric functional abdominal pain disorders: Current evidence and future perspectives. World J Clin Pediatr. 2022 Mar 9;11(2):105-119. doi: 10.5409/wjcp.v11.i2.105[↩]
- Hyams JS, Di Lorenzo C, Saps M, Shulman RJ, Staiano A, van Tilburg M. Functional disorders: children and adolescents. Gastroenterology. 2016;150:1456–1468. e2. doi: 10.1053/j.gastro.2016.02.015[↩]
- Schmulson MJ, Drossman DA. What is new in rome IV. J Neurogastroenterol Motil. 2017;23:151–163. doi: 10.5056/jnm16214[↩]
- Thapar N, Benninga MA, Crowell MD, Di Lorenzo C, Mack I, Nurko S, Saps M, Shulman RJ, Szajewska H, van Tilburg MAL, Enck P. Paediatric functional abdominal pain disorders. Nat Rev Dis Primers. 2020 Nov 5;6(1):89. doi: 10.1038/s41572-020-00222-5[↩][↩][↩]
- Jones MP, Dilley JB, Drossman D, Crowell MD. Brain-gut connections in functional GI disorders: anatomic and physiologic relationships. Neurogastroenterol Motil. 2006 Feb;18(2):91-103. doi: 10.1111/j.1365-2982.2005.00730.x[↩][↩]
- DuPont AW, Jiang ZD, Harold SA, Snyder N, Galler GW, Garcia-Torres F, DuPont HL. Motility abnormalities in irritable bowel syndrome. Digestion. 2014;89(2):119-23. doi: 10.1159/000356314[↩]
- Sha W, Pasricha PJ, Chen JD. Rhythmic and spatial abnormalities of gastric slow waves in patients with functional dyspepsia. J Clin Gastroenterol. 2009 Feb;43(2):123-9. doi: 10.1097/MCG.0b013e318157187a[↩]
- Riezzo G, Chiloiro M, Guerra V, Borrelli O, Salvia G, Cucchiara S. Comparison of gastric electrical activity and gastric emptying in healthy and dyspeptic children. Dig Dis Sci. 2000 Mar;45(3):517-24. doi: 10.1023/a:1005493123557[↩]
- Gershon MD. Review article: serotonin receptors and transporters — roles in normal and abnormal gastrointestinal motility. Aliment Pharmacol Ther. 2004 Nov;20 Suppl 7:3-14. doi: 10.1111/j.1365-2036.2004.02180.x[↩]
- Bueno L, Fioramonti J. Visceral perception: inflammatory and non-inflammatory mediators. Gut. 2002;51 Suppl 1:i19–i23. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1867723/pdf/v051p00i19.pdf[↩][↩]
- Karantanos T, Markoutsaki T, Gazouli M, Anagnou NP, Karamanolis DG. Current insights in to the pathophysiology of Irritable Bowel Syndrome. Gut Pathog. 2010 May 13;2(1):3. doi: 10.1186/1757-4749-2-3[↩][↩][↩][↩]
- Halac U, Noble A, Faure C. Rectal sensory threshold for pain is a diagnostic marker of irritable bowel syndrome and functional abdominal pain in children. J Pediatr. 2010 Jan;156(1):60-65.e1. doi: 10.1016/j.jpeds.2009.06.062[↩]
- Enck P, Mazurak N. Dysbiosis in Functional Bowel Disorders. Ann Nutr Metab. 2018;72(4):296-306. doi: 10.1159/000488773[↩]
- Pittayanon R, Lau JT, Yuan Y, Leontiadis GI, Tse F, Surette M, Moayyedi P. Gut Microbiota in Patients With Irritable Bowel Syndrome-A Systematic Review. Gastroenterology. 2019 Jul;157(1):97-108. doi: 10.1053/j.gastro.2019.03.049[↩]
- Miquel S, Martín R, Rossi O, Bermúdez-Humarán LG, Chatel JM, Sokol H, Thomas M, Wells JM, Langella P. Faecalibacterium prausnitzii and human intestinal health. Curr Opin Microbiol. 2013 Jun;16(3):255-61. doi: 10.1016/j.mib.2013.06.003[↩]
- Santos J, Alonso C, Guilarte M, Vicario M, Malagelada JR. Targeting mast cells in the treatment of functional gastrointestinal disorders. Curr Opin Pharmacol. 2006 Dec;6(6):541-6. doi: 10.1016/j.coph.2006.08.001[↩]
- Wouters MM, Vicario M, Santos J. The role of mast cells in functional GI disorders. Gut. 2016 Jan;65(1):155-68. doi: 10.1136/gutjnl-2015-309151[↩]
- Husebye E. The pathogenesis of gastrointestinal bacterial overgrowth. Chemotherapy. 2005;51 Suppl 1:1-22. doi: 10.1159/000081988[↩]
- Chumpitazi BP, Weidler EM, Lu DY, Tsai CM, Shulman RJ. Self-Perceived Food Intolerances Are Common and Associated with Clinical Severity in Childhood Irritable Bowel Syndrome. J Acad Nutr Diet. 2016 Sep;116(9):1458-1464. doi: 10.1016/j.jand.2016.04.017[↩]
- Reed-Knight B, Squires M, Chitkara DK, van Tilburg MA. Adolescents with irritable bowel syndrome report increased eating-associated symptoms, changes in dietary composition, and altered eating behaviors: a pilot comparison study to healthy adolescents. Neurogastroenterol Motil. 2016 Dec;28(12):1915-1920. doi: 10.1111/nmo.12894[↩]
- Newton E, Schosheim A, Patel S, Chitkara DK, van Tilburg MAL. The role of psychological factors in pediatric functional abdominal pain disorders. Neurogastroenterol Motil. 2019 Jun;31(6):e13538. doi: 10.1111/nmo.13538[↩]
- Pollard KL, Campbell C, Squires M, Palsson O, van Tilburg MAL. Seasonal Association of Pediatric Functional Abdominal Pain Disorders and Anxiety. J Pediatr Gastroenterol Nutr. 2018 Jul;67(1):18-22. doi: 10.1097/MPG.0000000000001886[↩][↩]
- Dinan TG, Cryan JF. The Microbiome-Gut-Brain Axis in Health and Disease. Gastroenterol Clin North Am. 2017 Mar;46(1):77-89. doi: 10.1016/j.gtc.2016.09.007[↩]
- Cunningham NR, Moorman E, Brown CM, Mallon D, Chundi PK, Mara CA, Pentiuk S, Lynch-Jordan AM, Dykes DMH, Elfers J, Farrell MK. Integrating Psychological Screening Into Medical Care for Youth With Abdominal Pain. Pediatrics. 2018 Aug;142(2):e20172876. doi: 10.1542/peds.2017-2876[↩]
- Nanthakumar C. The benefits of yoga in children. J Integr Med. 2018 Jan;16(1):14-19. doi: 10.1016/j.joim.2017.12.008[↩]
- Reindl D, Hamm A, Lewis R, Gellar L. Elementary student and teacher perceptions of a mindfulness and yoga-based program in school: A qualitative evaluation. Explore (NY). 2020 Mar-Apr;16(2):90-93. doi: 10.1016/j.explore.2019.07.009[↩]
- Brands MM, Purperhart H, Deckers-Kocken JM. A pilot study of yoga treatment in children with functional abdominal pain and irritable bowel syndrome. Complement Ther Med. 2011 Jun;19(3):109-14. doi: 10.1016/j.ctim.2011.05.004[↩][↩]
- Evans S, Seidman LC, Lung K, Sternlieb B, Zeltzer LK. Yoga for Teens With Irritable Bowel Syndrome: Results From a Mixed-Methods Pilot Study. Holist Nurs Pract. 2018 Sep/Oct;32(5):253-260. doi: 10.1097/HNP.0000000000000288[↩]
- Evans S, Lung KC, Seidman LC, Sternlieb B, Zeltzer LK, Tsao JC. Iyengar yoga for adolescents and young adults with irritable bowel syndrome. J Pediatr Gastroenterol Nutr. 2014 Aug;59(2):244-53. doi: 10.1097/MPG.0000000000000366[↩]
- Schumann D, Anheyer D, Lauche R, Dobos G, Langhorst J, Cramer H. Effect of Yoga in the Therapy of Irritable Bowel Syndrome: A Systematic Review. Clin Gastroenterol Hepatol. 2016 Dec;14(12):1720-1731. doi: 10.1016/j.cgh.2016.04.026[↩]
- Boradyn KM, Przybyłowicz KE, Jarocka-Cyrta E. The role of selected dietary and lifestyle factors in the occurrence of symptoms in children with functional abdominal pain – a pilot study. Acta Sci Pol Technol Aliment. 2020 Jul-Sep;19(3):291-300. doi: 10.17306/J.AFS.0833[↩][↩][↩]
- Seidenfaden S, Ormarsson OT, Lund SH, Bjornsson ES. Physical activity may decrease the likelihood of children developing constipation. Acta Paediatr. 2018 Jan;107(1):151-155. doi: 10.1111/apa.14067[↩]
- Ciciora SL, Yildiz VO, Jin WY, Zhao B, Saps M. Complementary and Alternative Medicine Use in Pediatric Functional Abdominal Pain Disorders at a Large Academic Center. J Pediatr. 2020 Dec;227:53-59.e1. doi: 10.1016/j.jpeds.2020.08.027[↩]
- Kichline T, Cushing CC, Ortega A, Friesen C, Schurman JV. Associations Between Physical Activity and Chronic Pain Severity in Youth With Chronic Abdominal Pain. Clin J Pain. 2019 Jul;35(7):618-624. doi: 10.1097/AJP.0000000000000716[↩]
- Chouliaras G, Kondyli C, Bouzios I, Spyropoulos N, Chrousos GP, Roma-Giannikou E. Dietary Habits and Abdominal Pain-related Functional Gastrointestinal Disorders: A School-based, Cross-sectional Analysis in Greek Children and Adolescents. J Neurogastroenterol Motil. 2019 Jan 31;25(1):113-122. doi: 10.5056/jnm17113[↩]
- Wren AA, Ross AC, D’Souza G, Almgren C, Feinstein A, Marshall A, Golianu B. Multidisciplinary Pain Management for Pediatric Patients with Acute and Chronic Pain: A Foundational Treatment Approach When Prescribing Opioids. Children (Basel). 2019 Feb 21;6(2):33. doi: 10.3390/children6020033[↩]
- Lee D, Lee H, Kim J, Kim T, Sung S, Leem J, Kim TH. Acupuncture for Infantile Colic: A Systematic Review of Randomised Controlled Trials. Evid Based Complement Alternat Med. 2018 Oct 24;2018:7526234. doi: 10.1155/2018/7526234[↩][↩]
- Reinthal M, Lund I, Ullman D, Lundeberg T. Gastrointestinal symptoms of infantile colic and their change after light needling of acupuncture: a case series study of 913 infants. Chin Med. 2011 Aug 11;6:28. doi: 10.1186/1749-8546-6-28[↩]
- Suresh S, Wang S, Porfyris S, Kamasinski-Sol R, Steinhorn DM. Massage therapy in outpatient pediatric chronic pain patients: do they facilitate significant reductions in levels of distress, pain, tension, discomfort, and mood alterations? Paediatr Anaesth. 2008 Sep;18(9):884-7. doi: 10.1111/j.1460-9592.2008.02638.x[↩]
- Nam MJ, Bang YIe, Kim TI. [Effects of abdominal meridian massage with aroma oils on relief of constipation among hospitalized children with brain related disabilities]. J Korean Acad Nurs. 2013 Apr;43(2):247-55. Korean. doi: 10.4040/jkan.2013.43.2.247[↩]
- Silva CA, Motta ME. The use of abdominal muscle training, breathing exercises and abdominal massage to treat paediatric chronic functional constipation. Colorectal Dis. 2013 May;15(5):e250-5. doi: 10.1111/codi.12160[↩]
- Karkhaneh M, Zorzela L, Jou H, Funabashi M, Dryden T, Vohra S. Adverse events associated with paediatric massage therapy: a systematic review. BMJ Paediatr Open. 2020 Aug 20;4(1):e000584. doi: 10.1136/bmjpo-2019-000584[↩]
- Çetinkaya B, Başbakkal Z. The effectiveness of aromatherapy massage using lavender oil as a treatment for infantile colic. Int J Nurs Pract. 2012 Apr;18(2):164-9. doi: 10.1111/j.1440-172X.2012.02015.x[↩]
- Al Qahtani AM, Ahmed HM. The Effect of Educational Program for New Mothers about Infant Abdominal Massage and Foot Reflexology for Decreasing Colic at Najran City. Compr Child Adolesc Nurs. 2021 Mar;44(1):63-78. doi: 10.1080/24694193.2020.1740827[↩]
- Groß M, Warschburger P. Evaluation of a cognitive-behavioral pain management program for children with chronic abdominal pain: a randomized controlled study. Int J Behav Med. 2013 Sep;20(3):434-43. doi: 10.1007/s12529-012-9228-3[↩]
- Abbott RA, Martin AE, Newlove-Delgado TV, Bethel A, Thompson-Coon J, Whear R, Logan S. Psychosocial interventions for recurrent abdominal pain in childhood. Cochrane Database Syst Rev. 2017 Jan 10;1(1):CD010971. doi: 10.1002/14651858.CD010971.pub2[↩][↩]
- Hermann C. Psychological interventions for chronic pediatric pain: state of the art, current developments and open questions. Pain Manag. 2011 Sep;1(5):473-83. doi: 10.2217/pmt.11.48[↩]
- Lalouni M, Hesser H, Bonnert M, Hedman-Lagerlöf E, Serlachius E, Olén O, Ljótsson B. Breaking the vicious circle of fear and avoidance in children with abdominal pain: A mediation analysis. J Psychosom Res. 2021 Jan;140:110287. doi: 10.1016/j.jpsychores.2020.110287[↩]
- Santucci NR, Saps M, van Tilburg MA. New advances in the treatment of paediatric functional abdominal pain disorders. Lancet Gastroenterol Hepatol. 2020 Mar;5(3):316-328. doi: 10.1016/S2468-1253(19)30256-0[↩][↩]
- Dobson D, Lucassen PL, Miller JJ, Vlieger AM, Prescott P, Lewith G. Manipulative therapies for infantile colic. Cochrane Database Syst Rev. 2012 Dec 12;12:CD004796. doi: 10.1002/14651858.CD004796.pub2[↩]
- Ernst E. Chiropractic spinal manipulation for infant colic: a systematic review of randomised clinical trials. Int J Clin Pract. 2009 Sep;63(9):1351-3. doi: 10.1111/j.1742-1241.2009.02133.x[↩]
- Sadeghian M, Farahmand F, Fallahi GH, Abbasi A. Cyproheptadine for the treatment of functional abdominal pain in childhood: a double-blinded randomized placebo-controlled trial. Minerva Pediatr. 2008 Dec;60(6):1367-74.[↩]
- Bahar RJ, Collins BS, Steinmetz B, Ament ME. Double-blind placebo-controlled trial of amitriptyline for the treatment of irritable bowel syndrome in adolescents. J Pediatr. 2008 May;152(5):685-9. doi: 10.1016/j.jpeds.2007.10.012[↩]
- Saps M, Youssef N, Miranda A, Nurko S, Hyman P, Cocjin J, Di Lorenzo C. Multicenter, randomized, placebo-controlled trial of amitriptyline in children with functional gastrointestinal disorders. Gastroenterology. 2009 Oct;137(4):1261-9. doi: 10.1053/j.gastro.2009.06.060[↩]
- Collins BS, Lin HC. Double-blind, placebo-controlled antibiotic treatment study of small intestinal bacterial overgrowth in children with chronic abdominal pain. J Pediatr Gastroenterol Nutr. 2011 Apr;52(4):382-6. doi: 10.1097/MPG.0b013e3181effa3b[↩]
- Tack J, Camilleri M. New developments in the treatment of gastroparesis and functional dyspepsia. Curr Opin Pharmacol. 2018 Dec;43:111-117. doi: 10.1016/j.coph.2018.08.015[↩]
- Chiou E, Nurko S. Management of functional abdominal pain and irritable bowel syndrome in children and adolescents. Expert Rev Gastroenterol Hepatol. 2010 Jun;4(3):293-304. doi: 10.1586/egh.10.28[↩]
- Horst S, Shelby G, Anderson J, Acra S, Polk DB, Saville BR, Garber J, Walker LS. Predicting persistence of functional abdominal pain from childhood into young adulthood. Clin Gastroenterol Hepatol. 2014 Dec;12(12):2026-32. doi: 10.1016/j.cgh.2014.03.034[↩]





{kind=link}